
Abstract
Professionals are expected to justify their actions to clients, disciplinary committees and courts in multiple accountability systems. Although developed to reflect professional standards, is it possible that these systems induce proactive behaviours that counteract their goals and instead serve to protect the professional? This article examines the types of stimuli professionals acquire from the public and professional accountability contexts and how these stimuli motivate engagement in specific proactive behaviours. An interpretive grounded theory study was conducted; it included 31 in-depth interviews with physicians from eight hospitals. The study revealed that accountability systems trigger and motivate professionals to engage in self-serving, proactive job-crafting behaviours. Professionals simultaneously manage their perceived accountability pressures and their personal interests. Context-specific factors that motivate individuals to craft their jobs are identified, and we reveal four distinct stimuli–motivation–job-crafting patterns that are linked to specific performance episodes (i.e. work stages). Our findings emphasize the importance of taking specific work contexts (i.e. accountability) and work stages into account when studying job-crafting behaviours. This study contributes to understanding professionals’ motivations and behaviours in the context of accountability, which is essential, as the quality and safety of their work are matters of public concern.
Introduction
Professionals, such as healthcare workers, lawyers and accountants, have the discretion to make decisions relatively independently within their professional domains owing to their lengthy professional education. There are, however, protocols and control mechanisms in place through which professionals are subject to critical evaluation and can be held accountable for their actions (Bovens, 2007; Frink et al., 2008; Hall et al., 2017). Clients who experience service delivery failures or are harmed (Mulgan, 2000; Rasche and Esser, 2006; Schillemans, 2008) and external institutions, such as courts and disciplinary committees (Frink et al., 2008; Mulgan, 2000; Pas et al., 2021), can ask professionals to justify their behaviour. Autonomy in professional decision making will be preserved only if professionals are subject to critical evaluation and can be held accountable for their behaviours and actions (Hoogland and Jochemsen, 2000).
In the last two decades, professionals have had to cope with increasingly complicated accountability demands that have created stress and tension (Evetts, 2011; Noordegraaf, 2011, 2016) for two main reasons. First, this stress is created by the potential loss of social status and group membership (Dekker, 2012), and second the ‘many-hands-problem’ (Thompson, 1980, 2017). Individual liability can be hard to determine in practice when there is intensive collaboration and collective responsibility. Despite this, in such situations, the legal and public systems often focus on the faults of individuals rather than the underlying cause of an incident or adverse event (Thompson, 2017). This raises questions regarding the fairness of sanctioning the individual professional (Dekker, 2012). Taken together, the perceived accountability that stems from professional institutions, courts and the public encourages compliance with expected behaviours such as fulfilling obligations (Freeman et al., 2009) and following guidelines (Hwang and Han, 2017). However, it also generates negative emotions and thoughts such as stress, tension, fear of being blamed and dissatisfaction (Brees et al., 2020; Frink et al., 2008; Hall et al., 2003, 2017; Renkema et al., 2014). Furthermore, it can lead to increased stereotyping (Gordon et al., 1989; Tetlock, 1992), distorted performance appraisal ratings (Levy and Williams, 2004; Mero et al., 2007), wasted resources (Adelberg and Batson, 1978) and cognitive bias in decision making (Tetlock et al., 1989), aspects that are referred to as the ‘dark side’ of accountability (Frink and Klimoski, 2004; Rofcanin et al., 2019).
Although several conceptual studies have reported on the negative impact of accountability systems on professionals’ individual behaviour (Frink et al., 2008; Hall et al., 2017), empirical research that examines how the accountability context motivates professionals’ actions is limited. A study by Hall et al. (2003) suggested that felt accountability is related to increased work involvement, emotional labour, job tension and citizenship behaviour. It has also been suggested that the dark side of accountability might induce professionals to engage in coping behaviours to mitigate their own negative feelings (Tetlock, 2002), such as by reducing the risk of litigation or minimizing personal responsibility (Markman and Tetlock, 2000; Schlenker et al., 1994). These coping behaviours can be proactive in nature (Hall et al., 2017; Schillemans, 2015). As such, accountability has also been classified as a social influence variable that spurs the use of social influence tactics to increase positive personal accountability outcomes and reduce negative personal accountability outcomes (Hall et al., 2016). However, empirical evidence for these stimuli and behaviours is scarce despite insights into stimuli–motivation–action links helping to provide an understanding of behaviours that are not aligned with the positive intentions of the accountability systems (Hall et al., 2017). Consequently, we ask the following: how do professionals proactively address public and professional accountability contexts?
To answer this question, an interpretive grounded theory study (Charmaz, 2014; Corbin and Strauss, 2015; Gehman et al., 2018) in the healthcare sector provided us with the opportunity to capture how physicians, living the experience of accountability, give meaning to it and to adequately theorizing about this experience (Foley and Timonen, 2015; Gioia et al., 2012). The sanctioning powers of accountability contexts are often particularly severe in healthcare, as they can result in the loss of one’s professional licence. Furthermore, following an increased focus on incidents and failures in the debate on quality and safety in medicine (Classen et al., 2011), healthcare professionals are increasingly called upon to be open about incidents and to justify their actions (Iedema et al., 2011). Moreover, accountability is obviously salient in that healthcare professionals are very aware that their mistakes might have harmful outcomes for their patients and have impacts beyond the organization (Hall et al., 2007). As such, this profession seems particularly appropriate for investigating the stimuli that professionals experience from accountability contexts and how these stimuli might encourage various proactive coping behaviours.
During the initial rounds of coding our interview data, several proactive behaviours showed similarities to job-crafting behaviours. Job crafting comprises individuals’ proactive behaviours to modify aspects of their work, resulting in relatively permanent changes in the way they work (Wrzesniewski and Dutton, 2001). Job crafting is an individually initiated strategy to optimize the work environment and achieve personal, self-serving work goals or outcomes (Bruning and Campion, 2018; De Bloom et al., 2020; Tims and Bakker, 2010). Accountability studies have examined proactive coping behaviours to address accountability demands (e.g. Schillemans, 2015). However, as already outlined by Frink and Klimoski (2004: 10), it is more likely that ‘the terms of accountability are negotiated’, rather than accountability dictating how an individual will behave. Here, Frink and Klimoski refer to an integration of the focal ideas of role theory and accountability theory and, as such, discuss the importance of individuals’ expectations surrounding potential accountability evaluations. In organizations, these expectations are captured in norms that guide individuals to behave according to rules defining appropriate behaviours. However, individuals should not be regarded only as ‘role takers’, who act according to role expectations, but also as ‘role makers’, where they proactively shape their work and influence role expectations and interactions and thus also their accountability (see also Frink et al., 2008; Hall and Ferris, 2011). Role theory has also been applied in job-crafting studies (e.g. Bizzi, 2017) to show that employees in a work environment can act as role senders who influence the extent to which their colleagues can craft their own jobs. Despite these theoretical linkages between accountability and job-crafting theories, studies exploring how the accountability context influences how individuals craft their job tasks to address potential accountability pressures are scarce. By revealing the role of job crafting in relation to felt accountability, we show that individuals proactively address accountability pressures while simultaneously managing their personal interests.
Our analysis contributes to both the accountability and job-crafting literatures. The first contribution to the accountability literature centres on the finding that the accountability context fuels various stimuli that motivate professionals to enact self-serving proactive job-crafting behaviours. Moreover, we traced self-initiated changes that would not be expected from a professional based on their work role or conflicted with the established professional norms and the original purposes of the accountability systems. In addition, within this specific work context, various phases (i.e. examination, post-treatment and call-to-account stages) were identified to exert unique influences on physicians’ perceptions of the accountability risks that ultimately informed their job-crafting behaviours.
Second, we contribute to the job-crafting literature by shifting the focus from factors that facilitate job-crafting behaviours, for example as specific work characteristics, such as autonomy (e.g. Slemp et al., 2015), workload (e.g. Kuijpers et al., 2020) and social contexts (e.g. Wang et al., 2017), to context-specific factors that generate motivations for job-crafting behaviours. Explicitly considering that the work environment may pose accountability threats enriches the job-crafting perspective by illustrating how accountability may give rise to additional motivations for, and subsequent forms of, job crafting beyond those that have been acknowledged thus far. Specifically, we identified job-crafting motivations beyond the often-mentioned motivations of increasing person–job fit (e.g. Kooij et al., 2017) and satisfying psychological needs (De Bloom et al., 2020; Wrzesniewski and Dutton, 2001), namely, motivations to decrease or contain accountability risks. In turn, these motivations inform specific job-crafting behaviours, indicating that the high-stakes context in which physicians operate gives rise to self-protecting motives that influence their work behaviours.
Theoretical background
Felt accountability
Individuals may be called upon to explain and justify their behaviour (Schillemans, 2008; Schlenker et al., 1994) to various audiences, such as a board of directors, colleagues, clients, an audit office, a court and journalists (Mulgan, 2000). Some refer to a ‘web of accountabilities’ (Frink and Klimoski, 1998; Hall et al., 2017) when individuals ‘bear multiple accountabilities to multiple sources’ (Hall et al., 2007: 408). This web creates interpersonal expectations that influence what an individual thinks (Tetlock, 1985) and how the individual behaves (Frink and Klimoski, 2004). An audience can interrogate individuals about their behaviour, pass judgement, impose sanctions or invoke negative consequences (Cummings and Anton, 1990; Dekker, 2012). Felt accountability is based on an individual’s perceptions of what and to whom one is accountable (Frink and Klimoski, 1998; Hall et al., 2017) and can be induced even if it is not certain that an event will occur (Frink and Klimoski, 1998).
Many individuals work within a system of ‘bureaucratic’ or ‘hierarchical’ accountability (Fuller et al., 2006; Hochwarter et al., 2007; Schillemans et al., 2020) that consists of legitimate hierarchical relationships between superiors and subordinates in which the subordinates are empowered, instructed and monitored by their superiors (Romzek and Dubnick, 1987). Professionals, like physicians, experience less strict hierarchical or even non-hierarchical relationships with others in their organization. They usually work in professional and public accountability systems that include the possibility of having to account for one’s actions to both professional and public institutions (Bovens, 2007). Professional accountability systems consist of codes of conduct, protocols and professional standards set by professional associations and disciplinary committees. Often, these codes, protocols and standards provide only general guidance since professional work is complex and ambiguous, such that the appropriate handling of the divers options depends on the situation. Hence, the output quality of professional work is difficult to understand for non-experts (Von Nordenflycht, 2010). Because establishing unambiguous rules and procedures for directing professional work is difficult, professionals have discretion to make relatively independent decisions within their professional domains. This decision-making autonomy is granted by their own professional groups, based on an often long-term professional education. However, professional autonomy can be preserved only if professionals are subject to critical evaluations by their professional group and if they can be called upon by courts to explain their behaviour (Rasche and Esser, 2006; Schillemans, 2008). The latter refers to a second public accountability system: in the event of disputes or incidents, professionals may also be called to civil or criminal courts that will assess whether they have acted according to the law. This accountability is ‘public’ in the sense that, first, it is transparent and open to the public and, second, it addresses an issue of public interest (Bovens et al., 2014). In our study, the overarching issue is the quality of healthcare in society, one where healthcare providers are obliged to provide an account of how they meet their public responsibilities.
Professional and public audiences might invoke various types of accountability (Dubnick, 2003), which may cause stress among professionals. One stress-raising factor is that professionals might lose their professional group membership and/or their social status within society (Harris and Byhoff, 2017) if their account is perceived as unacceptable and they are blamed; that is, ‘accountability-as-blameworthiness’. Being involved in a disciplinary or legal case might cause reputational damage (Keren-Paz, 2010; Noordegraaf, 2011), even if one is cleared of any wrongdoing. This accountability also creates an obligation to provide answers upon request about one’s actions, labelled ‘accountability-as-answerability’, which might be uncomfortable for professionals when it involves non-experts or emotional clients. A second stress-raising factor is the risk of being held responsible for actions (Renkema et al., 2019), referred to as ‘accountability-as-liability’, even when the actions resulted from teamwork. Increasingly, such ‘sanctioning’ of individual professionals is considered unjust (Renkema et al., 2019) owing to the many hands involved (Thompson, 2017).
To preserve their social identity and self-image, people regulate their behaviours based on their felt accountability (Frink et al., 2008; Lerner and Tetlock, 1999). Conceptual studies have argued that felt accountability drives individuals’ behaviours because being accountable to an audience provides individuals with a strong motivation to manage demands (Hall et al., 2017). Moreover, the severity of possible sanctions, the salience of accountability and the experience of a ‘web of accountabilities’ might induce proactive behavioural strategies to prevent negative individual outcomes such as stress or litigation. Tetlock (1991, 2002) refers to coping strategies of ‘pre-emptive self-criticism’ (i.e. the pre-decisional strategy of anticipating potential objections by accountability audiences and taking these objections into account when deciding how to act), the ‘acceptability heuristic’ (i.e. the pre-decisional strategy of making socially acceptable decisions) and ‘defensive bolstering’ (i.e. the post-decisional strategy to justify one’s action afterwards). Other strategies that can be invoked to cope with or manage professional and public accountability include determining the interests of stakeholders upfront and what to prioritize in terms of accountability obligations (Hwang and Han, 2017; Schillemans, 2015), following guidelines (Hwang and Han, 2017) and proactively collecting data to be able to provide an account if required (Schillemans, 2015). Although all these strategies are applied to manage one’s accountability, they do not shed light on the specific kinds of stimuli that professionals experience in the multiple accountability contexts in which they must act and how these inducements motivate them to act in specific ways. Such insights could help provide an understanding of how to preserve the positive impact of accountability systems while reducing professionals’ stress levels. In the initial stages of our data analysis, these proactive behaviours were found to resemble job-crafting behaviours in many ways.
Job crafting
The way individuals behave at work is shaped by many factors, such as the interactions they have with others, how these interactions are interpreted by the individual (Cooley, 1902; Katz and Kahn, 1978; Mead, 1934) and formal and informal role expectations (Salancik and Pfeffer, 1978). Furthermore, an individual’s efforts to shape the interactions, tasks and cognitions they have with regard to their work role are also recognized (Frink and Klimoski, 2004; Wrzesniewski and Dutton, 2001). The latter behaviour is referred to as job crafting, which allows individuals to change the meaning of their work and their work identity (Wrzesniewski and Dutton, 2001). As such, job crafting is an activity that primarily serves the employee and could be either beneficial or harmful to others (Tims and Parker, 2020; Wrzesniewski and Dutton, 2001). For example, although healthcare professionals should conform to the technical and ethical standards of their profession, they may be more focused on their own well-being or protecting their image and thus show job-crafting behaviours that go against expected professional behaviours. Furthermore, job crafting involves self-initiated changes that are not specifically expected of an employee’s work role (Wrzesniewski and Dutton, 2001) and may even conflict with established professional norms and protocols. Although job crafting can take many forms, we focus on instances that are self-serving and proactive and result in a relatively permanent change in a job (Bruning and Campion, 2018), such as adding a task or avoiding an aspect of work that is associated with a high litigation risk.
Recent research has distinguished approach and avoidance orientations in job crafting (Bruning and Campion, 2018; De Bloom et al., 2020; Zhang and Parker, 2019; and see Lichtenthaler and Fischbach, 2019 for a similar reasoning related to promotion and prevention job crafting). Approach crafting is job-crafting behaviour that is directed towards solving problems, improving the work situation, and accepting and interpreting stressors in a positive way. Avoidance crafting seeks to reduce or eliminate aspects of the job to prevent the emergence of negative outcomes. Zhang and Parker (2019) argued that approach and avoidance orientations can be further distinguished by whether an individual makes behavioural or cognitive changes in the job (i.e. changing the way they work or think about aspects of the job) and whether job demands (i.e. aspects of the job that require sustained physical and/or psychological effort or skills; LePine et al., 2005) or job resources (i.e. aspects of the job that help achieve work goals or stimulate personal growth, learning and development; Bakker and Demerouti, 2007) are changed. Zhang and Parker (2019) distinguish eight conceptual types of job crafting, such as approach behavioural resources crafting or avoidance cognitive demands crafting.
Wrzesniewski and Dutton (2001) argue that basic human needs motivate job crafting. That is, when the need for control over one’s environment, the need for a positive self-image or the need to have meaningful relationships with others is thwarted, individuals may be motivated to restore or fulfil these needs by job crafting. Similarly, De Bloom et al. (2020) propose that individuals craft when they experience a psychological need discrepancy. Moreover, when crafting is successful, individuals experience their psychological needs as satisfied. Although qualitative and quantitative syntheses of the literature have identified many antecedents of job crafting (see Lazazzara et al., 2020; Rudolph et al., 2017; Zhang and Parker, 2019), these antecedents comprise specific job (e.g. autonomy), personal (e.g. proactive personality) and social characteristics (e.g. leadership style) while neglecting the role of specific work contexts. In the present study, we address this gap by focusing on the broader accountability context, which has been found to generate specific stimuli (Hall et al., 2017) that might influence an individual’s motivations and subsequent job-crafting behaviours.
Method
The interpretive grounded theory study reported here is an extension to a larger study that examined physicians’ attitudes towards incidents, litigation and patient complaints. In this extension, our aim was to elaborate specifically on accountability theory and to empirically investigate how physicians’ experienced accountability impacts their daily work behaviour. The interpretive grounded theory approach is particularly strong for giving voice to informants and how they experience and act upon a phenomenon of theoretical interest (here: how experienced accountability impacts daily work behaviour) while also trying to surface concepts and relationships ‘grounded up’ from the data, describing these findings in theoretically relevant terms and to build substantive theory (here: theory on how accountability systems trigger and motivate professionals to engage in self-serving, proactive job-crafting behaviours) (Corbin and Strauss, 2015; Foley and Timonen, 2015; Merriam and Tisdell, 2015; Sebastian, 2019).
Organization and participant selection
We carried out in-depth semi-structured interviews with 31 physicians working in eight hospitals in the Netherlands. We initially approached a mixture of 12 academic and general hospitals that were geographically spread across the Netherlands. Three hospitals declined because they considered their staff to have insufficient time or perceived the topic to be too sensitive, and one hospital did not respond to our request. The other eight hospitals granted approval for the interviews through hospital management and the medical staff. On our behalf, the medical staff director, the head of the quality department or the hospital director approached physicians to determine whether they were willing to be interviewed. Participants from five different specialties with varying degrees of medical experience were approached. These five specialties were known for generating patient complaints and facing litigation. Initially, 54 physicians were asked to participate; of these, 17 declined without giving reasons, and five did not respond. We further cancelled one interview after the interviewee requested payment. Consequently, 21 male and 10 female physicians were interviewed, of whom 18 had personal experience with litigation. The interviews were voluntary, and the interviewees were informed about the topic before the interviews took place and gave consent to use the information contained in the interviews anonymously. The Dutch Law on Medical Research Involving Human Subjects (WMO) did not require us to seek ethical approval, as the research would not contribute to clinical medical knowledge and no participation by patients or use of patient data was involved. We further obtained confirmation that our research complied with the ethical guidelines of the Vrije Universiteit Amsterdam (reference number SBE10/21/2020mts790).
Data collection
The first author conducted the interviews using a semi-structured interview protocol (see online Appendix 1) aimed at gathering occupational narratives and real-life accounts of how the physicians addressed the professional and public accountability contexts in their daily work. We were concerned that physicians would find it difficult to talk about their behaviours in relation to the ‘web of accountabilities’ and be reluctant to express behaviours that may not align with the formal goals of the accountability systems, since medical errors increasingly receive considerable media attention and have high reputational risks. We therefore adopted semi-structured interviewing and asked our questions in a neutral, non-leading way to encourage physicians to talk about these delicate issues and to share their own experiences. In framing the interviews, professional and public accountability was construed as being ‘felt’ and as arising from possible investigations into whether a physician had been negligent in his or her medical actions and the possibility of litigation through the Medical Disciplinary Committee of the disciplinary court, the Health Inspectorate or a civil or criminal court. These are professional and public institutions to which patients in the Netherlands can file formal complaints about a physician in the event of an incident or adverse outcome. To examine the participants’ awareness of litigation, each interview began by asking the participants about their knowledge and perception of litigation and their experiences thereof. We asked the physicians about their thoughts and emotions regarding the personal consequences of litigation to encourage them to share their experiences on this delicate topic (Cunningham and Wilson, 2011; Pereira et al., 2014). A general question was posed regarding the participants’ own behaviour: how does knowing you work in a professional and public accountability context influence your behaviour? The interviewees were invited to give concrete examples of the behaviours they described to expose ‘the why’ of their behaviours. In the final part of each interview, the focus shifted to actual incidents and adverse outcomes that had occurred. The interviews lasted between 35 and 120 minutes, with an average of 75 minutes.
Data analysis
The interviews were audio recorded, transcribed using a text editor and checked for accuracy by one of the researchers. The interviews were conducted in Dutch, and we continued in Dutch, the native language of all the authors and interviewees, when analysing the data. During the preparation of the manuscript, the codes and the quotes were translated to English and edited by a native speaker from an English editing agency to ensure that subtleties and nuances were retained. The authors further checked whether the translations were accurate by discussing them alongside the original Dutch quotes until full agreement was reached to ensure the richness of the original quotes remained intact. The transcripts consisted of 638 pages, amounting to 353,865 words, with an average of 11,415 words per interview. For the content analysis, we used ATLAS.ti version 7.5.12, a computer program designed for this purpose. Consistent with our interpretive grounded theory approach, in the coding process, we draw heavily on the constant comparative method of data analysis (Charmaz, 2014; Glaser and Strauss, 1967; Merriam and Tisdell, 2015). We moved back and forth several times between the collected data and their analysis, as well as between the emergent findings and the literature. When we planned the interviews, we estimated that we needed a sample of around 30 interviews to reach enough information power. It was only after having completed the analysis of all interviews that we could conclude that we reached data saturation after having conducted 18 interviews. The additional interviews provided us with a rich pool of data from which we were able to use the quotes as included in this article (Corbin and Strauss, 2015).
Analysis step 1
We started the iterative process by inductively coding proactive behaviours that physicians described as being triggered by their accountability contexts. The first author started the process by adding in vivo codes to four interviews, which were subsequently discussed with the second and third authors. Once we had agreed on these first codes, the second and third authors each also coded four interviews. Once again, the codes were compared and discussed. After agreeing on the full list of in vivo codes (see online Appendix 2, step 1), we discussed several approaches for labelling the proactive behaviours. Ultimately, we concluded that an approach based on their strong similarities with job-crafting behaviours was the most credible. We then consulted an expert on job crafting and discussed our in vivo coded material, and this expert then became a member of our research team. Consequently, we decided to focus on behaviours that constituted a relatively permanent change in the physician’s job (Bruning and Campion, 2018) and that were self-serving (Wrzesniewski and Dutton, 2001) in the sense of aiming to achieve or optimize a personal work goal (Tims and Bakker, 2010). As such, we then ignored behaviours that could be seen as expected based on the profession. For example, although ordering an ECG scan as part of a patient’s diagnosis is part of a physician’s work and in the interest of the patient, if a physician regularly orders unnecessary ECG scans to provide juridical evidence for decisions made, it constitutes proactive behaviour with a self-serving aim. The next step was to inductively attribute in vivo codes to stimuli, reflecting what respondents mentioned as elements that required addressing in the accountability context and the motivations that led the physicians to adopt specific job-crafting behaviours. We applied the same procedure as before to code these triggers and motivations: the first author started by coding four interviews, and subsequently, the other authors became involved in the coding process.
Having decided to adopt a job-crafting perspective, we went back and forth between our list of in vivo codes and a list of eight job-crafting behaviours (second-order themes) based on the categories of job-crafting behaviours outlined by Zhang and Parker (2019). Subsequently, we tried to match these second-order themes to the in vivo codes (see online Appendix 2, step 2).
This back-and-forth process between our data and the literature resulted in a list of 13 in vivo codes and four second-order themes for job-crafting behaviours, six in vivo codes for stimuli and six in vivo codes for motivations (see online Appendix 2). All the researchers then used this list to independently code six interviews (20% of the coded text blocks), and a subsequent comparison demonstrated high interrater reliability (Krippendorff, 2004) for the coding (α > 0.80). The first author then coded the remaining interviews.
Analysis step 2: Stimuli–motivation–job-crafting patterns by work stage
After the coding process, we investigated the relationships between the stimuli, motivations and behaviours to understand how the accountability context triggered and motivated physicians to enact specific forms of job crafting. We included only behaviours that had been identified in the work of at least three physicians (Tippmann et al., 2012). By returning to the full transcripts of the interviews and the coded text blocks linked to each distinct stimulus, motivation and behaviour, we were able to link the specific stimuli and motivations to the behaviours. The analysis revealed two things. First, we observed that the work of physicians went through various stages. Second, we saw that ‘stimuli–motivation–job-crafting’ patterns in each stage could be grouped into four aggregated patterns. To verify the consistency of the analysis, all the researchers used these four patterns to independently code the job-crafting patterns of two interviews, and high interrater reliability (α = 0.83) was achieved.
Results
The impact of accountability
During the analysis of the interview transcripts, three relevant work stages were identified that induce their own specific context-related accountability stimuli for physicians, and were labelled the ‘examination’, ‘post-treatment’ and ‘call-to-account’ stages. The ‘examination’ stage is where physicians examine their patients, provide treatment or medicine or refer them to other physicians. In this stage, physicians described three specific stimuli they experience in relation to their accountability: perceived patient pressure; uncertainty or fear about one’s patient handling; and the perception that some procedures are high risk. Examples of these stimuli can be found in Table 1. The ‘post-treatment’ stage is the period after patient treatment during which physicians are faced with the outcomes and consequences of any adverse incidents that may have occurred during treatment. During this stage, physicians experience stimuli based on emotional pressure and/or doubts that surface about their handling that led to unintended outcomes. The third and final ‘call-to-account’ stage is characterized by physicians’ expectations, or the possibility, of having to account for one’s actions. In this stage, physicians fear being pursued; that is, ‘the perceived threat of litigation’. In each work stage, the various stimuli induce specific motivations in physicians to craft their job to deal with their accountability salience. These motivations are described below along with the specific stimuli–motivation–job-crafting patterns that were identified (Figure 1).
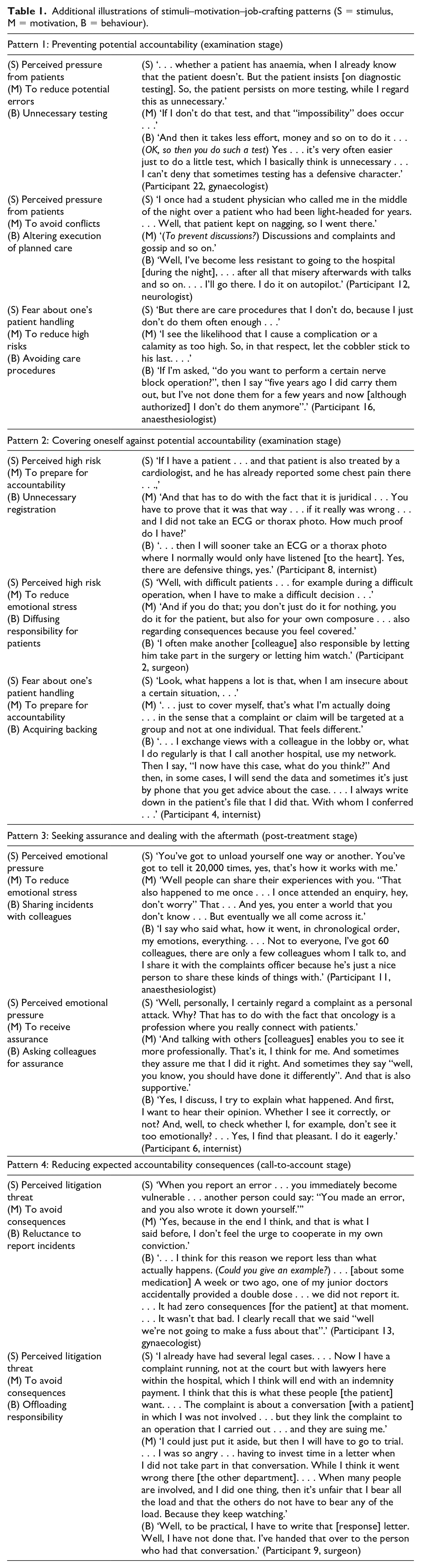
Additional illustrations of stimuli–motivation–job-crafting patterns (S = stimulus, M = motivation, B = behaviour).
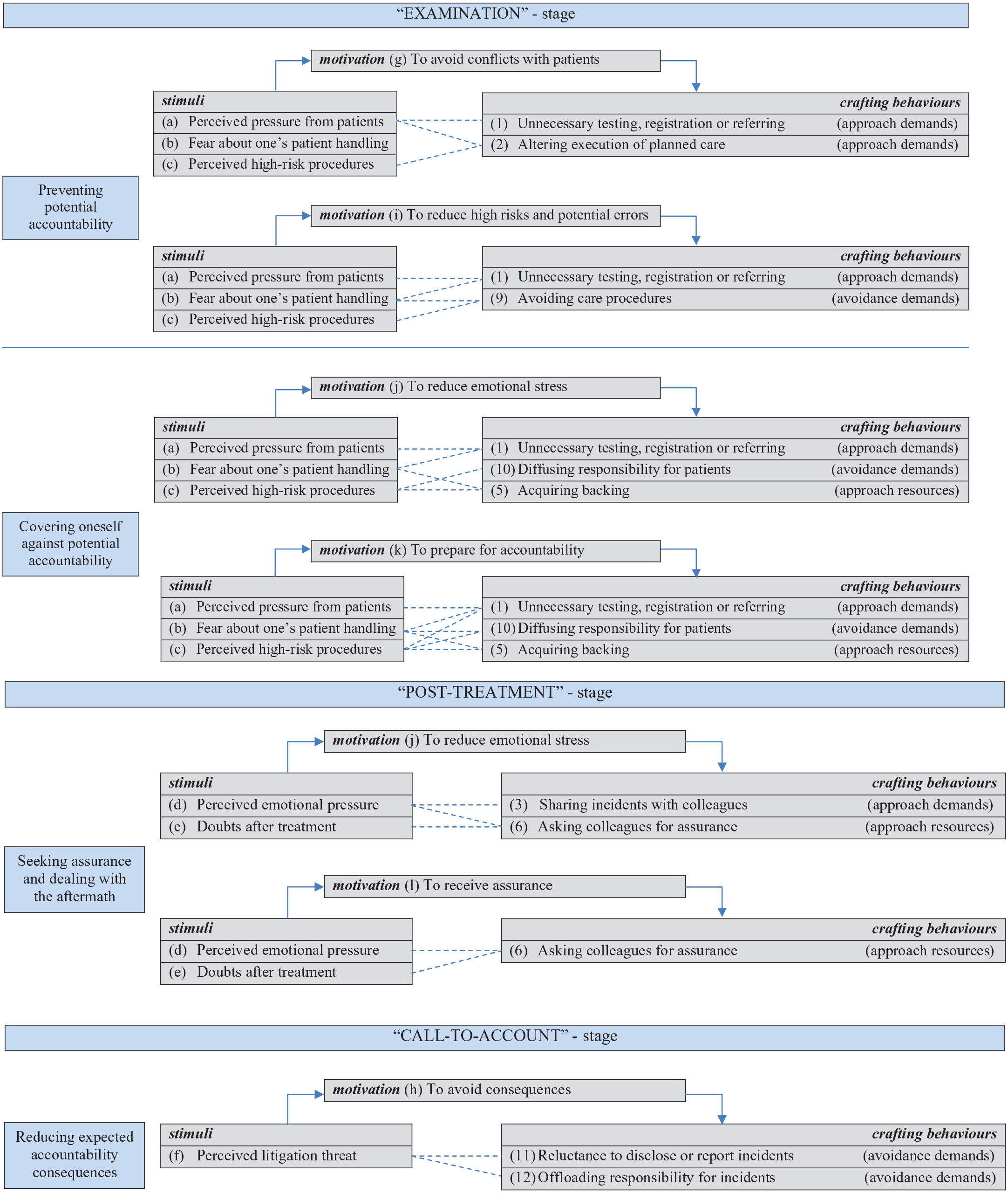
Data structuring of stimuli–motivation–job-crafting patterns by work stage.
The stimuli–motivation–job-crafting patterns
The data revealed four forms of job crafting. Physicians most often referred to what amounted to approach demands crafting (behavioural) and avoidance demands crafting (behavioural) in the forms of altering their tasks or interactions with patients and colleagues to resolve or avoid hindering job demands that stem from the accountability contexts. The physicians also alluded to approach resources crafting (behavioural) through acquiring additional job resources in the form of backing or assurance from their colleagues. Avoiding job activities that lack positive job resources (i.e. avoidance resources crafting (behavioural)) was not mentioned. In terms of cognitive crafting, only avoidance demands crafting (cognitive) was identified and involved changing how one views the provision of care, accountability and litigation. Combined with the context-related stimuli, the motivations and behaviours resulted in four aggregated job-crafting patterns. Table 1 summarizes the various stimuli, motivations and job-crafting behaviours (first column) and provides illustrative examples of the patterns found – relating ‘stimuli’, through ‘motivations’, to ‘job-crafting behaviour’ (second column). We describe these patterns in more detail below in the sequence of the three work stages.
Job crafting during the examination stage
The stimuli in this stage initiate two distinct job-crafting patterns: ‘preventing potential accountability’ and ‘covering oneself against potential accountability’. In the first pattern, ‘preventing potential accountability’, physicians are motivated to craft their jobs ‘to avoid conflicts with patients’ and ‘to reduce high risks and potential errors’. In addressing the motivation ‘to avoid conflicts with patients’, physicians sometimes mentioned carrying out unnecessary testing, as illustrated in the following quote: Occasionally I order an MRI scan for a patient, even if I know that it’s of no use. . . . Also, because the patient actually nags about it. Then, I think, nagging is one thing, but then next you’ll see . . .. So, actually, I do it, well yes, to put the patient at ease but also to calm the patient down so that the patient, shall we say, does not start complaining about it [i.e. not having an MRI]. (Participant 15, anaesthesiologist)
The quote above illustrates how this physician sometimes perceives patients as applying pressure for an examination. To avoid potential complaints that could lead to litigation, this physician crafts his job by ordering unnecessary MRIs and other examinations that are of little use. The physicians also mentioned that ‘altering the execution of planned care’ is triggered by perceived patient pressure and perceived high-risk procedures. The latter was described as follows by an anaesthesiologist: I would not give an epidural to a patient who, because of a hernia, has sensitivity problems in his legs . . .. I would not give them an epidural because their problem could naturally get worse, but they will always relate it to that epidural. They will always get full narcosis from me because I fear that if their back problem gets worse, so their symptoms worsen, that they will say: ‘You see that was caused by that epidural.’ (Participant 23, anaesthesiologist)
The second motivation that was identified in the pattern of ‘preventing potential accountability’ is ‘to reduce high risks and potential errors’. Here, physicians also mentioned the stimulus of perceived patient pressure leading them to carry out unnecessary testing, registration or referring. However, here, unnecessary testing was also triggered by their own fear about patient handling, as one physician described: Well look, it’s often more difficult to exclude something [a disease] than to prove it. And, sometimes you want to exclude something, based on your own thoughts . . .. That you exclude something with 100% certainty. And, yes, that can be a reason to ask for a medical examination that proves useless . . .. And, my thoughts about this come down to, what I just said, I am not going to be frugal. (Participant 1, neurologist)
The stimulus of fear regarding one’s patient handling and the motivation ‘to reduce high risks’ could even lead to job crafting in the form of ‘avoiding care procedures’. Moreover, physicians noted that this motivation, leading to ‘avoiding care procedures’, could be stimulated by the perception that some procedures are considered high risk, as described by one physician: ‘Certain pain-reducing injections in the neck area. That we have agreed on, that we don’t do that anymore. Because there is a 1%, 2% chance that it goes wrong, and we don’t want that’ (Participant 1, neurologist).
The second pattern, ‘covering oneself against potential accountability’, has the same stimuli, but here, it leads to different motivations: ‘to reduce emotional stress’ and ‘to prepare for accountability’. Emotional stress can be triggered by perceived pressure from patients leading to the application of unnecessary care actions: Well, yes, we do a lot of diagnostics ourselves, so you sometimes look with an extra echo, of which you think, yes now I am covering myself . . .. Yes, it’s a mixture of your own composure, assuring the patient and, yes, maybe in the back of our minds, if we look at things many times, then no one can say that we did not do it right . . .. There are surely, a couple of times a year, patients of whom I think, when I notice during a consultation that it doesn’t go well, a little bit that the patient distrusts me. There is something going on. What is it? And, you do extra things you can think of, to really cover yourself. (Participant 18, gynaecologist)
In addition to the application of unnecessary care actions, the fear and consequent motivation to reduce emotional stress can lead to acquiring backing, as one physician describes: The first time that I again performed a gallbladder operation, I arranged back-up. So, I said upfront, you know, I’m going to do that gallbladder, I find it more stressful because of that disciplinary case, so can you be my back-up . . .. And, I also have operated once together with someone, so I could say ‘What would you do, if this or that would happen’ or ‘How do you see this? What do you look for?’ . . . Like a focused additional training. (Participant 9, surgeon)
Furthermore, the stimulus of perceived high-risk procedures and the motivation to reduce one’s stress could lead to diffusing one’s responsibility. The second motivation identified within the pattern of ‘covering oneself against potential accountability’ is that physicians prepare themselves for potential accountability (i.e. addressing a need for control) by proactively diverting patient responsibility onto colleagues. As one physician described: If I have a patient and I feel things are going in the wrong direction, then it is good, I think, for the patient but also, and I won’t deny it, for me as a physician, to divert it away from me, and move to collective responsibility. If I think ‘it is going wrong with this patient’, then it pays to send that patient to other colleagues, so you do not have to stand alone . . .. It’s a kind of protection mechanism, to already think upfront: hey, through my antenna I sense this is going wrong. Then, the protection mechanism is diffusing: to diffuse the responsibility. (Participant 7, internist)
The motivation to prepare oneself for accountability is also triggered by perceived high-risk procedures. A surgeon mentioned how he acquired backing for his decision not to perform a risky colon operation and thereby covered himself: We are more and more looking at the boundaries of operating on colon cancer . . .. Colon operations are dangerous and have a mortality rate of around 4–5% . . . the chances that you develop metastases are around 5–10% . . .. Well, you can imagine that a random professor, who was trained 30 years ago, and now at the end of his career is being used for his expertise [as a witness in a court case] says ‘But, you always have to remove this colon’ . . .. That’s what I feared, how did I cover myself? Because that’s what it is, covering oneself . . . I discussed it with a doctor, who I think has the most expertise worldwide in this treatment . . .. He let me know he had submitted an article [to a scientific journal] about their experiences that supported my decision, which the patient agreed with, not to operate. (Participant 2, surgeon)
Job crafting during the post-treatment stage
In the post-treatment stage, we identified a job-crafting pattern that we labelled ‘seeking assurance and dealing with the aftermath’. The pattern starts with two context-specific stimuli: emotional pressure and/or doubts that surface about their handling of a patient after an action that did not have the intended result or led to patient dissatisfaction. These stimuli lead to two specific motivations for physicians to craft their job during this stage: ‘to reduce emotional stress’ and ‘to receive assurance’. When physicians perceive emotional pressure, they can be motivated to reduce stress by sharing incidents with their colleagues. A surgeon described this pattern as follows: I must say that it is not a regular thing here, that we report to each other ‘Oh, did someone experience something [an incident] here.’ It’s a reasonably open culture, but it’s not obligatory to report to each other . . .. I discuss it mostly with one or two [colleagues] with whom I have a certain contact . . . but it’s more a case of unloading emotional pressure. . . . There is always something suboptimal happening [about an incident], and unfortunately, in this case, it led to a financial claim. Then, if someone [a colleague] says to me ‘you are unfortunate, that you were confronted with just that patient’ . . . then it is nice that my colleagues are in the first instance supportive, and do not give me additional criticism. (Participant 3, surgeon)
An anaesthesiologist mentioned how personal doubts after treatment and the motivation to reduce stress can also lead to asking colleagues for assurance about one’s handling: Well, often one is, let’s put it this way, with things that are not going well there is always a certain doubt, ‘Could I have done it differently? Would it have gone better that way?’ . . . [about an incident that happened] But, in the end, it’s a relief, no matter how severe it was, and it ended well. A narrow escape. But, it feels like a relief because my colleagues say ‘Well you did that, and did not do it another way, yes that’s also a possibility.’ So, you are also checking it with the professional standards that way. In addition, if it is in line with what my colleagues say, then I feel relieved, because then you think, oh it’s less threatening because, if a judge asks that same question, then I give that answer. (Participant 15, anaesthesiologist)
However, ‘to receive assurance’ can also act as a motivation in itself. Perceived emotional pressure or doubts after treatment can trigger a motivation to receive assurance. A surgeon described how, after having received a complaint, doubt about a certain treatment triggered the motivation to receive assurance and to ask colleagues for it: Mostly you see it coming, and there is already a difficult consideration, and if I then get a complaint, then I discuss it, yes. But, for me, it was eventually also the ultimate proof that I had done it right because, I told myself, and the colleagues with whom I had spoken, they all said, don’t worry, you didn’t do anything wrong. Nevertheless, the fact is that there was a debate about it in the whole room, . . . that there were diverse ways of doing things, at least that we make different choices, and that everybody found these decisions difficult. Well, from that, I saw how difficult it was, and that I really had thought thoroughly about which steps to take. Thus, there, I only saw confirmation that, well, I had done my utmost best, what can reasonably be expected from a reasonable doctor. . . . So, that was, for me, so to say, vindication. (Participant 9, surgeon)
Job crafting during the call-to-account stage
One job-crafting pattern was revealed during the call-to-account stage, which we labelled ‘reducing expected accountability consequences’. The stimulus for physicians in this stage is ‘the perceived threat of litigation’. This perceived threat triggers the motivation ‘to avoid consequences’ of accountability and results in two forms of job crafting: ‘reluctance to disclose or report incidents’ and ‘offloading responsibility for incidents’ onto colleagues. A gynaecologist explained the reluctance to discuss or report incidents as follows: There’s a group of patients that wants to sue us . . . who, if we give an inch, take a mile. The very idea that somebody wants to profit from the situation. That’s the word: profiteer . . .. I once made a severe error during a curettage, but it all ended well, at least I hope so . . .. However, there were so many consequences that were caused by it, that I thought ‘Oh, I have to explain it really carefully to this partner [of the patient]’, because otherwise there’s only one thing he will remember and that is ‘There’s been a mistake’ . . .. (OK, and how did you explain it then?) Restrained, more factual, I could almost say more objectively . . . ‘Yes, this happens with these treatments. You just had bad luck that it happened to you.’ (Participant 22, gynaecologist)
The second form of job crafting, stimulated by a perceived litigation threat and the motivation to keep a positive self-image, is the offloading of responsibilities for an incident onto colleagues: If I am one of four neurologists involved with a patient that I admitted [to the hospital], but otherwise did not have anything to do with, and something goes wrong, then I do not feel that I am part of that. Then, I find it annoying that my name is listed . . .. It happens occasionally that patients are admitted during my shift – then my name appears at the foot of the bed ‘Dr (my name) is in charge of this department.’ Then, once my shift is long finished, something happens with that patient, and people [colleagues] think: ‘Hey, it says Doctor (my name) on the plate. Something went wrong [with the patient], so that’s handy!’ Strictly speaking, it is my patient, but I didn’t have anything to do with the complaint. Then, I also try, as much as I can, to ensure that I do not have to get involved with that case. (Participant 17, neurologist)
Discussion
This interpretive grounded theory study among physicians shows how they proactively craft their jobs to deal with specific accountability threats and identifies the stimuli and motivations for their specific job-crafting behaviours. The contributions of the study are elaborated below in detail.
Job crafting as a strategy to manage accountability outcomes
Previous studies on accountability and work behaviour have reported individuals taking action to improve the professional quality of their work (Fuller et al., 2006; Hochwarter et al., 2007; Mero et al., 2006). In the present study, we contribute to this theorizing by empirically showing that professionals are also inclined to reduce the negative outcomes of their felt accountability and do so in several ways. Specifically, four ‘stimuli–motivation–job-crafting’ patterns were identified, and they illustrate how physicians’ work contexts and, specifically, the accountability systems that are part of this context influence the actions they take at work to protect their own self-image and retain their individual, self-perceived control. Moreover, we identified self-initiated changes that were not specifically expected from the professionals based on their work roles and even conflicted with the established professional norms and the original purposes of accountability systems.
The first job-crafting pattern we identified was labelled ‘preventing potential accountability’. Facing pressure from patients, uncertainty or fear about one’s patient handling and the high-risk procedures in which professionals are involved motivate physicians to avoid conflicts with patients and to avoid high-risk situations and potential errors, which drives their crafting behaviours. The avoidance of care procedures that are viewed as inherently risky and requesting unnecessary testing are in sharp contrast with the original aims of the accountability systems: to monitor and improve service delivery. These findings indicate that physicians not only fill their expected care-taking roles (Frink and Klimoski, 2004) but also act as their own gatekeepers by crafting job demands by proactively selecting patients and situations that reduce the likelihood of being held accountable. The detailed description of this job-crafting pattern provides a more profound interpretation of the ‘person as intuitive politician’ metaphor (Green et al., 2000; Tetlock, 1985, 2002). This metaphor underlines how people try to maintain a desired social identity towards relevant audiences by proactively applying various coping strategies, such as avoiding situations that present risks (Tetlock, 2002). Furthermore, the findings of this study support the claim made by Hall et al. (2016) that people with a high reputation tend to take the least risky path in resolving issues in their workplace. The second job-crafting pattern, ‘covering oneself against potential accountability’, is evoked by the same stimuli to those that evoke the first pattern and driven by the motivation of physicians to reduce emotional stress and be prepared for possible accountability. These motivations invoke behavioural crafting in the form of unnecessary testing and registration, through which they deliberately collect evidence that could be later used to support their decisions. Physicians know that their audiences (courts, patients) will accept these tests, medical images and registrations as validation of their decisions. This relates to Tetlock’s (1991) ‘acceptability heuristic’ metaphor, which recognizes that people try to make decisions that they believe will be accepted by those who might hold them accountable.
The motivations also induce them to spread the responsibility for patients and seek backing in the form of supportive opinions from colleagues to cover themselves. This proactive behaviour relates to Tetlock’s (2002) pre-decisional strategy of ‘pre-emptive self-criticism’, where people take potential objections or conflicting views into account. By including colleagues in decision making and collecting supportive opinions, physicians try to address the complexities in healthcare and the potentially conflicting views on how to act that exist, even among medical experts, in court cases.
In the third job-crafting pattern, ‘seeking assurance and dealing with the aftermath’, physicians experience emotional pressure and doubts after carrying out treatments and are motivated to reduce stress and to receive assurance for their actions. They proactively reach out to their colleagues by sharing information about incidents with them and seeking their reassurance. Here, they are trying to understand their own behaviour and justify it to themselves, which can be viewed as an operationalization of Tetlock’s post-decisional strategy of ‘defensive bolstering’ in coping with accountability. Defensive bolstering is the process of self-justification by finding reasons why one is right, and others are wrong (Tetlock, 2002).
The final job-crafting pattern ‘reducing expected accountability consequences’ takes place when a physician perceives a litigation threat, and it reflects the physician’s motivation to avoid consequences. This results in two forms of behavioural avoidance demands crafting: a reluctance to disclose and report incidents and, occasionally, an attempt to offload responsibility onto colleagues. Such behaviours are poorly aligned with the aims of the accountability system. They can also be seen as behavioural outcomes of Tetlock’s (2002) defensive bolstering strategy. Physicians believe that taking responsibility for an incident can have negative personal consequences and thus try to reduce these consequences by keeping quiet or offloading responsibility onto colleagues. Physicians use these job-crafting behaviours to weaken the link between incidents that occurred and their personal responsibility (Schlenker et al., 1994).
Job crafting in relation to context, stimuli and specific self-serving motivations
To date, job-crafting research has given little weight to the specific context in which it is investigated or the concrete and specific motivations that lead to job crafting. Our study reveals that physicians’ motivations for crafting their jobs are stimulated by perceived patient pressures, the necessity of applying high-risk procedures, emotional pressures, doubts after treatment and the perceived threat of litigation. These stimuli originate within a context of public and professional accountability in which professionals face heightened risks for a variety of reasons, including media attention given to incidents (Noordegraaf, 2011). Thus, although job crafting is a proactive activity in the sense that it is initiated by an individual to satisfy a personal need (De Bloom et al., 2020; Parker and Collins, 2010), we show that work contexts create specific stimuli that motivate people to craft their job to protect themselves from potentially negative future consequences, such as litigation.
We further revealed physicians’ specific, self-serving motivations, which were triggered by the accountability context and led to job-crafting behaviours. The combination of these motivations and behaviours shows that accountability and job crafting are connected through social influence tactics. Social influence tactics are the behavioural strategies of a person to influence others towards maximizing positive outcomes for oneself and minimizing negative outcomes (Ferris et al., 2002; Hall et al., 2016). The motivations found in this study could be considered general, higher-level, personal motivations. The motivations to avoid conflicts with patients and to avoid the consequences of litigation can be viewed as reflecting a ‘need for a positive self-image’ (Wrzesniewski and Dutton, 2001: 182) and a desire to protect one’s reputation (see also Frink et al., 2008). To positively influence their self-image and reputation, the physicians in this study applied their social influence directly through job-crafting behaviours such as unnecessary testing and altering the execution of care. Indirectly, physicians try to influence people who might potentially investigate and judge their behaviour if a formal case develops by crafting their jobs by being reluctant to disclose or report incidents, seeking cover by involving others and offloading their responsibility. These attempts could be regarded as forms of impression management (Frink and Ferris, 1998; Frink and Klimoski, 1998) or self-presentation (Ferris et al., 2002).
Reducing risks and preparing oneself for the possibility of being held accountable result in a motivation for a ‘need to control’ (Wrzesniewski and Dutton, 2001: 182) potential accountability, whereas receiving assurance can be interpreted as a form of Wrzesniewski and Dutton’s (2001: 182) motivation for a ‘need for human connection with others’. In addition, physicians craft their jobs to reflect a motivation to reduce the emotional stress of accountability pressures and thereby protect their well-being (Bruning and Campion, 2018). This motivation reflects Frink et al.’s (2008) assertion that accountability is a workplace stressor. To control this workplace stressor, physicians apply their influence tactics via interpersonal relationships (Ferris et al., 2002; Frink and Klimoski, 1998) with their colleagues. They craft their jobs by sharing incidents with colleagues, asking for their assurance and acquiring their backing. In this way, they try to reduce their stress levels and protect their well-being.
Combined, the motivations identified in this study show that the accountability context generates specific motivations to craft work with the aim of defending one’s individual needs and that physicians connect accountability with job crafting through social influence tactics.
Job crafting in different work stages
The third contribution of this study is the finding that job crafting differs by work stage (see Figure 1). To date, some scholars have investigated job crafting on a daily basis, considering day-level job performance (Demerouti et al., 2015) and day-level work engagement (Petrou et al., 2012), and over longer time periods (e.g. several months; Tims et al., 2013). However, our study indicates that job crafting seems to vary with performance episodes (i.e. work stages). While it is known that behavioural actions before an accountability event differ from those after the event (Schlenker et al., 1994; Tetlock, 2002), we have been able to generate a more detailed description of these behaviours and their motivations by considering specific work stages. The work of professionals other than physicians may similarly contain distinct activities that resemble ‘assessment’, ‘action’ and ‘after-service’ stages. Therefore, when identifying job-crafting behaviours, researchers should investigate whether the context they are addressing similarly involves different work stages, which may have distinct stimuli and motivations that induce different job-crafting behaviours.
Strengths and limitations
Given that public and professional accountability is increasingly an attribute of professional work, the stimuli and motivations that we identified are likely to be generalizable to other professional groups, although further research needs to be conducted to support this claim. As an illustration, rather than patient pressure, service-providing employees might experience customer pressure that could motivate them to proactively diverge from expected work practices. Similarly, politicians or scientists might not be willing to disclose or report mistakes made in fear of the public’s response and the negative impact on their future careers.
As with all studies, this research has limitations. First, as we gathered the data from the participants themselves, the behaviours assessed were self-declared, and the responses could suffer from a social desirability bias. In the interviews, we tried to avoid socially desirable answers by probing and asking about real-life events (Patton, 1999). Furthermore, there is no obvious and more reliable approach for measuring the relationship between litigation and job crafting, although data from other sources, such as colleagues, could have added value to our findings by providing greater insight into the group and organizational dynamics in which job crafting occurs. Additionally, social desirability bias does not explain why so many physicians reported trying to reduce hindering job demands since such job crafting would be seen as less socially desirable than increasing job resources and job challenges (e.g. Tims et al., 2013).
Another limitation might be using an interpretive grounded theory approach instead of conducting hypothesis-driven research. Although both the accountability and job-crafting literatures can be considered to have reached a ‘mature’ stage, no previous study has related accountability theory and job-crafting. Furthermore, how this accountability context might trigger job crafting has not yet been considered. We invite future scholars to research the motivations and job-crafting patterns that we identified through, for example, hypothesis testing.
A final limitation is that the litigation context is determined by country-specific laws (e.g. Mello et al., 2006); therefore, other behaviours might be seen in other countries. Our study took place in the Netherlands, a country with a modest litigation climate, where physicians can face reputational damage but are seldom exposed to large financial risks. However, even in this context, how physicians dealt with their work and acted was impacted by their accountability perceptions. We would therefore expect that in countries in which the litigation climate is much stronger (e.g. the USA), studies would reveal similar behaviours and potentially even more avoidance crafting behaviours.
Future research
Our findings offer several useful contributions for researchers interested in studying accountability and job-crafting behaviours. First, investigating job-crafting behaviours in a range of accountability contexts would provide a better understanding of how accountability is experienced and influences people at work. Researchers could, for example, investigate job-crafting behaviour in the context of corporate governance (Huse, 2005) or accountability to a range of stakeholders (beneficiaries, customers) of an organization (Rasche and Esser, 2006) and determine the extent to which the offloading of responsibility and the avoidance of risky situations by organizational leaders are apparent in these contexts.
Furthermore, the job-crafting patterns we identified suggest that investigating job crafting in relation to specific stimuli and self-serving motivations would be a fruitful avenue for future research and increase our understanding of the reasoning behind job crafting. The self-serving motivation of saving one’s reputation could be a topic for job-crafting research, as little is known about this. Additionally, the patterns that we identified contain job-crafting behaviours that contribute to a professional’s individual self-serving goals but also seem to run counter to the original aims of the accountability system (i.e. quality assurance and promoting improvements). As such, it would be interesting to investigate how personal goals and system aims influence each other over time by using a longitudinal multilevel study (e.g. physicians in a range of country-specific systems).
Another key area for future research is to examine the way job-crafting behaviour is influenced during specific performance episodes. Research to date has mostly looked at job crafting at a general or day level, while our study shows that job crafting can differ depending on the specific work stage a professional is in. It would be useful to determine whether this finding is replicated in other contexts.
Practical implications
The professionals interviewed referred to the need to interact and obtain backing for their actions, assurance and emotional support from each other because of the risks associated with public and professional accountability. Those who manage such professionals can create circumstances in which this need to interact and receive support can be fulfilled. They may also discourage professionals from employing certain behaviours, such as offloading responsibility onto others and being reluctant to report incidents that have negative consequences for colleagues, clients and for the organization or that go against the aims of the public and professional accountability systems. As such, our findings indicate that professionals should be treated in a way that creates working conditions that lead to quality work and safety for clients.
We also saw that professionals emphasized engaging in certain tasks, such as carrying out unnecessary testing, for defensive reasons. This may counteract an organization’s goal of reducing unnecessary care and contradict the aims of the public and professional accountability system itself. Aligning the behaviour of professionals with organizational goals is another challenge facing leaders in the context of public and professional accountability (Von Nordenflycht, 2010).
Conclusions
We have examined the proactive behaviours that professionals engage in within a context of public and professional accountability. Professionals simultaneously manage the perceived accountability pressures and their personal interests. Our findings emphasize the importance of taking specific work contexts (i.e. the associated accountability) and work situations (i.e. work stage) into account when studying proactive job-crafting behaviours. Acknowledging this interrelatedness between context and job-crafting behaviours helps us understand why employees craft their jobs in certain ways even though doing so may go against organizational or public interests.
Supplemental Material
sj-pdf-1-hum-10.1177_00187267221104011 – Supplemental material for Working around: Job crafting in the context of public and professional accountability
Supplemental material, sj-pdf-1-hum-10.1177_00187267221104011 for Working around: Job crafting in the context of public and professional accountability by Erik Renkema, Manda Broekhuis, Maria Tims and Kees Ahaus in Human Relations
Supplemental Material
sj-pdf-2-hum-10.1177_00187267221104011 – Supplemental material for Working around: Job crafting in the context of public and professional accountability
Supplemental material, sj-pdf-2-hum-10.1177_00187267221104011 for Working around: Job crafting in the context of public and professional accountability by Erik Renkema, Manda Broekhuis, Maria Tims and Kees Ahaus in Human Relations
Footnotes
Acknowledgements
The authors wish to thank all the physicians for their participation in this study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.