
Abstract
Menopause is one of the most distinctive and individualised aspects of health-related gendered ageing at work, which is important as more women than ever before are working through their entire menopause cycle. We turn to the life-span development model of Selection, Optimisation and Compensation (SOC), which has great potential to provide a more nuanced review of adaptive behavioural strategies for potential work-related resource loss owing to menopause. In this article, we provide evidence from two studies: study 1 was an inductive analysis of 21 interviews; study 2 tested a number of hypotheses emergent from study 1 on two survey samples (N = 381). We found that women with severe menopause symptoms were adversely affected at work; however, the use of SOC alongside supervisory and female peer support, ameliorated the negative impact of physical menopause symptoms on work performance. We also identified that SOC use was actually detrimental to work performance when used to manage psychological menopause symptoms. Our findings advance the understanding of gendered ageing at work, specifically managing menopause at work, through the lens of SOC theory. We show how engaging in agentic adaptive behaviours can be both beneficial and detrimental for differentially managing physical and psychological menopause symptoms at work.
Introduction
Affecting a significant majority of cisgender women and trans men 1 at some point in their lives, menopause transition is one of the most distinctive and individualised aspects of health-related gendered ageing at work and is currently receiving greater attention in human relations, organisation studies and management literatures. This is important as more women than ever before are working through their entire menopause cycle (Hardy et al., 2018; Jack et al., 2016). In the UK, 67% of women aged 50–59 are in paid employment (Goldman, 2010) and around 80% of women between the ages of 40 and 55 experience menopause symptoms (Office for National Statistics (ONS), 2016). Menopause symptoms can last up to 10 years (STUC, 2018), where 25% of women suffer ‘severe’ symptoms that adversely impact their performance at work (ONS, 2016).
However, for many women, menopause remains a ‘taboo topic’ at work (Atkinson et al., 2021; Grandey et al., 2020; Jack et al., 2019; Steffan, 2021). This way of thinking is clearly detrimental to women’s identity where male-dominated or gender-neutral work structures do not allow for the undisciplined body to be displayed (Putnam and Bochantin, 2009; Trethewey, 1999). The extent of the effect of menopause symptoms on work-related outcomes is hidden owing to high presenteeism as many women continue to work despite suffering from menopause-related ill-health (Whiteley et al., 2013). An ONS survey reported that 14 million working days were lost to physical and psychological menopause symptoms, 370,000 working women aged between 50 and 64 either left or were planning to leave work and one in 10 women had passed up a more demanding position owing to menopause symptoms (ONS, 2016). As the Organisation for Economic Co-operation and Development (OECD) countries prioritise women in mid- to later life at work within their labour market policies (Hickey et al., 2017) and considering the UK Government’s emphasis on retaining women in mid- to later career in work (Altmann, 2015), it is important for organisations to better understand the impact of menopause on workplace outcomes such as performance and retention. More research is also needed to understand how women could best be supported to manage or cope with their menopause symptoms at work (Atkinson et al., 2021; Grandey et al., 2020; Steffan, 2021). To address this gap, we aim to explore how women manage their physical and psychological menopause symptoms at work and how these symptoms affect their performance and retention via two studies. In study 1, we conducted a qualitative, exploratory investigation to gain a better understanding of how women experience menopause symptoms and how these affect their work. In study 2, we conducted a quantitative survey to test the hypotheses derived from the results of our inductive study and predominantly qualitative research on this topic. Throughout this article, we use the generic term ‘menopause’ and ‘menopause symptoms’ as those symptoms experienced during the ‘peri-menopause’ phase of the ‘menopause’ cycle (Grandey et al., 2020).
To address these aims, we turn specifically to the adaptive, life-span development model of Selection, Optimisation and Compensation (SOC) (Baltes, 1997). This framework has great potential to provide a more nuanced review of agentic mechanisms and strategies that women can use to cope with transient resource loss owing to experiencing menopause symptoms, which can significantly negatively impact their job performance and retention. As a life-span development model, the SOC framework suggests that age-related changes in individual potential can be conceptualised in terms of maximisation of gains and minimisation of losses, which can be achieved by engaging in strategies such as prioritising one’s goals (i.e. selection), and improving and obtaining resources (i.e. optimisation) or using alternative ways (i.e. compensation) in order to achieve one’s goals (Baltes, 1997). We use the SOC model to further conceptualise how women deal with their menopause experience in order to maintain their potential and regulate the menopause-related loss of their resources, which in turn could protect their performance and retention.
Our contribution to the gendered ageing at work literature is twofold. First, we unpack the process of how women experience menopause and how they cope with its impact on their workplace-related attitudes and outcomes. Although some previous qualitative research has looked at these questions, we provide a more nuanced view of specific coping mechanisms that women might use to manage their menopause symptoms at work drawing from the SOC framework (Baltes, 1997). In so doing, we elaborate on and show the effects of these different coping strategies for offsetting the negative effects of different menopause symptoms on two key behavioural outcomes, such as performance and retention. Second, we provide a deeper understanding of how the work context shapes women’s experience of menopause at work. Given that women often feel embarrassed or ashamed of their gendered biological experiences in the workplace (Putnam and Bochantin, 2009; Trethewey, 1999), workplace social support might play a fundamental role in how women successfully manage to overcome the stigma associated with menopause at work. To this end, we differentiate between supervisory and female peer support as two contextual resources that women could draw from for managing their menopause symptoms.
On the whole, our findings demonstrate how different workplace resources and agentic adaptive behaviours play a key role in coping with physical and psychological menopause symptoms at work. We enrich the gendered ageing at work literature by conceptualising menopause coping strategies using the SOC behaviours that women might use, in conjunction with drawing from workplace social support, to maintain their performance and stay in the workforce for longer. Our research also provides practical solutions to how employers can help their employees who experience menopause symptoms at work through gendered social support structures.
Background and literature review
Menopause is a workplace issue
The impact of menopause symptoms at work is gaining attention owing to the growing number of women in mid- to later life at work (Grandey et al., 2020; Hardy et al., 2018). Menopause symptoms are an under-reported potential cause of disruption to the career trajectory of women, in addition to previously identified gendered factors including maternity leave, childcare and caring for elderly relatives (Fan and Potočnik, 2021; Loretto and Vickerstaff, 2015). The potential disruption caused by menopause symptoms challenges the overly simplified linear depiction of women’s work lives (Putnam and Bochantin, 2009), for example Mainiero and Sullivan’s (2005) outline of the mid- to late career phase of the ideal worker as a leader, agentic and socially skilled, appears controlled and confident. Similarly, an ‘ideal’ menopausal woman is one who ‘takes control of her symptoms’ (Butler, 2020: 4). This agentic view of ageing where individuals are encouraged, even expected, to ‘take care of themselves’ and cope with losses in physical health (Truxillo et al., 2015), pushes women to maintain or even mask the effects of bodily ageing in response to gendered work structures (Putnam and Bochantin, 2009; Trethewey, 1999), presenting the ideal older worker as someone who has not actually aged at all (Rowe and Kahn, 1998, 2015). This presents an incongruence between what is expected as the ‘ideal’ worker and the potential challenges brought about through experiences of menopause symptoms to female employees. It should be noted that not all women experience work-related interruption from menopause symptoms; however, research suggests that, for those who do, support is limited.
Menopause symptoms, including anxiety, irritability, hot flushes and poor concentration, can be perceived as problematic, embarrassing and shameful in the workplace (Griffiths et al., 2013; Hardy et al., 2018). Indeed, frequent hot flushes and night sweats alone were associated with reduced work engagement, greater intention to quit (Joffe et al., 2016) and impaired work productivity (Steffan, 2021; Whiteley et al., 2013) for many women. Just eight years ago, the first large-scale survey into menopause at work, comprising a sample of 900 women from 10 different organisations, was conducted in the UK (Griffiths et al., 2013). The limited number of studies that have reported empirical evidence on the impact of menopause symptoms on women’s workplace attitudes have been relatively exploratory in nature and have insufficiently considered the organisational context, which is surprising as the workplace has been reported to both intensify symptoms and provide crucial support to alleviate them (Brewis et al., 2017; Grandey et al., 2020; Hardy et al., 2018; Jack et al., 2019). For example, Griffiths et al. (2013) found that women used coping mechanisms including psychological (e.g. distraction and making light of matters) and social (e.g. asking advice from those who had experienced menopause) adaptive behaviours to conceal performance decline; however, findings were presented in a rather descriptive way, without reporting the strength of their association with work outcomes. Within a gendered ageing at work focus, these studies suggest that workplace factors can exacerbate adverse work outcomes owing to insufficiently supporting women with managing their menopause symptoms.
The majority of studies on the impact of menopause symptoms at work refer to menopause symptoms collectively (Atkinson et al., 2021; Hardy et al., 2018; Hickey et al., 2017) or highlight a specific symptom (Butler, 2020; Jack et al., 2016). Indeed, Brewis et al. (2017) stated that very few studies have explored specific symptoms separately. Some studies have addressed this lack of categorisation of menopause symptoms by reporting on ‘physical’ symptoms such as sleep, hot flushes, night sweats and migraines and ‘psychological’ symptoms, such as decision making, concentration and memory (citing Mishra and Kuh, 2006; Griffiths et al., 2013), irritability, mood swings and emotional outbursts (citing Mishra and Kuh, 2006; Kittell et al., 1998); and depression (citing Wagner et al., 2011). Our research makes an important contribution to the gendered ageing at work literature by simultaneously studying a number of different physical and psychological symptoms, making a distinction in how these symptoms are managed and coped with by women at work.
Coping with menopause symptoms in the workplace
Organisational structures reinforce how older women are able to manage their ‘undisciplined’ bodies through a form of subtle gendered ageism (Trethewey, 1999), specifically where symptoms of menopause are considered taboo (Grandey et al., 2020). Work is at the core of how women experience menopause, having the capacity to ‘generate, exacerbate, even relieve’ menopause symptoms (Jack et al., 2019: 129), yet scarce qualitative research has suggested that menopause symptoms can severely and adversely impact work performance (Griffiths et al., 2013). Interestingly, these findings were attributed to women failing to seek help and advice (Goldman, 2010). Brewis et al. (2017) reported that only limited and exclusively qualitative research studied what coping strategies women use to manage their symptoms at work, which were mainly of avoidance type, such as hiding and denying symptoms. These coping strategies appeared to be overwhelmingly motivated by the avoidance of age and gender stereotypes about mid-life women. Further, arguing that women can self-manage the menopause symptom of fluctuating emotions at work was posited as counter-productive as psychological symptoms are often not manageable (Kittell et al., 1998).
While Butler’s (2020) study focused on the body and physical menopause symptoms, she found that the same-gender peer-group support of ‘real women’, who were not only not ashamed of their menopausal bodies but used their bodily distinction as a psychological coping mechanism, was one of their key sources of support that helped them cope. This speaks to Trethewey’s (1999: 437) findings that professional women’s bodies are not only performative, but are positioned as ‘excessively sexual’. Trethewey (1999) also referred to the female professional body as being undisciplined and excessive, albeit not referring to the menopause directly. Coping with menopause, therefore, is also coping with the performative older female body. In Griffiths et al. (2013), women reported a wide range of coping strategies for managing their menopause symptoms at work, such as psychological, social, informational, practical, organisational and changing health behaviours. Our literature review shows only a few empirical studies that consider how women develop coping strategies to manage the seemingly mysterious and hidden world of physical and psychological menopause symptoms at work. This is especially surprising as studies suggest that women are expected to cope with, manage, even mask menopause symptoms at work (Butler, 2020; Hardy et al., 2018).
One framework that could help us conceptualise how women manage their menopause symptoms at work is SOC theory, which focuses on how individuals gain resources and minimise resource loss (Freund and Baltes, 2002). SOC is a life-span development theory, which is well established in the study of how health-related changes can impact how individuals engage with work (Baltes and Baltes, 1990; Moghimi et al., 2017; Zacher and Frese, 2011). Specifically, life-span development theory that underpins SOC represents the function of growth, the function of maintenance (including resilience) and the regulation of loss. As such, drawing from this framework in the study of menopause has the potential to extend SOC theory in relation to how women cope with and manage their menopause symptoms, which are inevitable for most women as they age. SOC seeks to understand how individuals cope with their everyday demands (Rowe and Kahn, 2015) and focuses on ‘doing the best with what one has’ (Strawbridge et al., 2002). SOC was designed to explore future potential and age-related changes of human development (Baltes, 1997). In focusing on specific strategies that women might use to adapt their behaviours (Freund and Baltes, 2002), we expect that the use of SOC strategies will have an impact on such potential through performance and retention of women who experience menopause symptoms.
Specifically, selection involves prioritising ‘some goals over others, either to achieve a desired state (elective selection) or in response to a loss of resources needed for goal achievement (loss-based selection)’ (Moghimi et al., 2017: 247). Optimisation focuses on obtaining, refining and using resources for achieving one’s goals and compensation entails the acquisition and use of new or alternative resources for goal-achievement to compensate for declining resources. Specifically, compensation draws on the use of external resources; for example, an older worker might compensate for a loss in physical strength by asking others for help (Moghimi et al., 2017). The SOC model would suggest that individuals who can adapt their behaviours using these three strategies would be able to deal with their multiple demands and pursuing multiple goals more successfully than those who do not use such strategies. Moghimi et al.’s (2017) meta-analysis shows that the use of SOC strategies leads to positive outcomes and that these strategies are particularly effective when demands are high and resources are low. Indeed, SOC strategy use is particularly effective when external resources provided by the work environment (e.g. supervisor support, family-friendly policies) are low (Zacher and Frese, 2011). This suggests that SOC strategies should, in principle, be effective for coping with both physical and psychological health demands of menopause. However, it should be noted that research has also shown a potential of SOC to deliver less positive outcomes. For example, when individual resources are ample for the job, or in a situation in which a goal is no longer achievable, SOC use could lead to an unnecessary restriction of goals, which may be maladaptive in the long run (Moghimi et al., 2017). Furthermore, SOC use requiring investment of resources to achieve a goal may be resource consuming in itself and eventually lead to the depletion of resources and feelings of fatigue.
Most empirical evidence on the use of SOC is done through the physical body or performative actions that can be seen and commented upon and much less is known around later life development, the ageing body and the impact of SOC strategies on psychological health (Moghimi et al., 2017). Zhang and Radhakrishan (2018) conducted a systematic literature review on chronic conditions and the use of SOC. While the majority of studies measured physical health, they identified a few studies on depression, anxiety and cognitive impairment. They found that the use of SOC was associated with improvement in these conditions and in ability to perform daily activities. Despite its broad application in ageing literature, SOC has not, to the best of our knowledge, been used to study how women manage their menopause symptoms at work.
Our research draws from SOC theory by using its life-span approach to consider the impact of resources over women’s career trajectories during their experience of menopause and thus, we respond to the call for research on ‘critical points’ of when resources are needed the most (Halbesleben et al., 2014b). Specifically, we explore how women seeking new mechanisms of support to cope with new health challenges of menopause can draw on SOC strategies as a resource. We contribute to the gendered ageing at work literature by combining an investigation of SOC strategy use with women’s management of menopause, and in so doing, we focus on resources that are deemed particularly salient to women who experience age-related health symptoms. By addressing the joint role of the use of SOC strategies and workplace social support in coping with menopause symptoms at work, we contribute to the emerging research on how environmental or contextual resources interact with individual agentic and adaptive behaviours (Zacher and Frese, 2011), to protect women against any potential menopause-related decline in their performance and retention. Specifically, Moghimi et al. (2017) found that overall self-reported job performance is an established outcome of SOC use, as are attitudes around workplace retention. To this end, we have first conducted an in-depth inductive study to explore what resources women use to manage their menopause symptoms at work and how the experience of menopause symptoms affects their workplace attitudes and outcomes. We then tested hypotheses derived from this study to explore the strength of the effects different resources have on offsetting the negative impact of symptoms on women’s performance and retention.
Study 1
Method
Participants and procedure
An open-ended approach was taken to collect and analyse the data in our first study, which was part of a larger project on bodily ageing at work. Data were collected from workers in mid- to later life around their gendered experiences of bodily ageing at work and associated appearance bias at work (Langlois et al., 2000). As such, it was their own perceptions of themselves as ‘older workers’ that constructed their individual narratives within their specific organisational contexts that was relevant to our study. We used life grids, presented as columns for life domains and rows as time (Nico, 2016) in conjunction with semi-structured interviews with open-ended questions (Parry et al., 1999), which allowed for life-course events to be understood with the elasticity of a non-linear narrative. This approach was designed to capture not only current working practices and attitudes, but also historical aspects of self, such as educational attainment, employment trajectory, family events and health issues (Tulle, 2008).
Interview questions were designed to gain an understanding of the context of work and personal life trajectories in line with qualitative studies of the life course (Tulle, 2008). The interviews began with a simple question asking all participants: can you tell me about your job and what it entails on a weekly basis? Participants were then asked to describe how their work had changed during their lives in order to capture the life-course aspect of a changing nature of work for the individual within structural factors. They were then asked what the term ‘successful ageing’ meant to them as workers, which prompted participants to discuss aspects of ‘healthy ageing’. At this point, the majority of women raised the subject of menopause symptoms at work. The question of successful ageing was motivated by extensive recent work within organisation studies on and around ageing (Zacher et al., 2015).
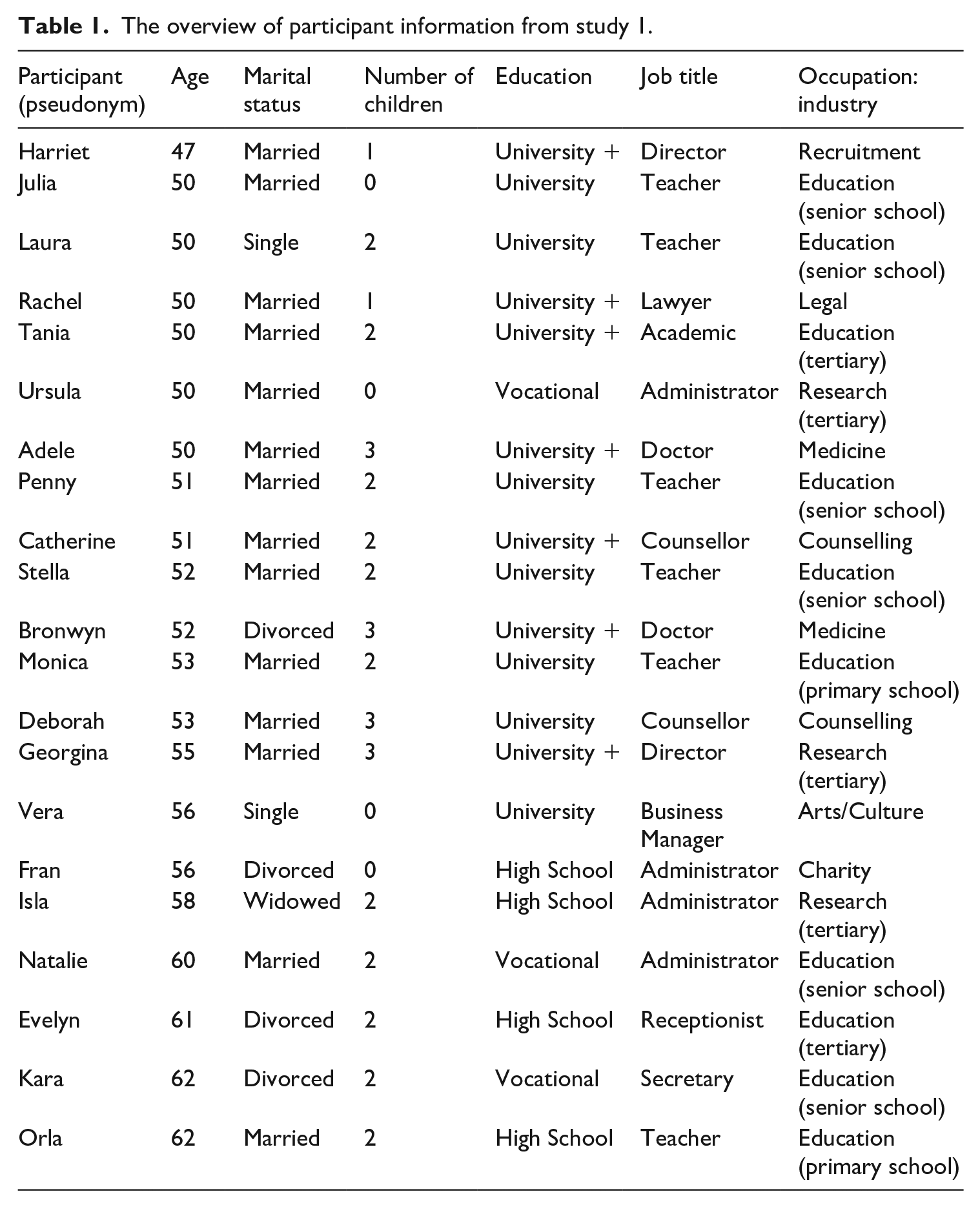
Our sample consisted of 21 women working in the UK. All participants were over 47 years of age and in paid professional employment, with a broad range of job and industry types, educational attainment and personal income. Unlike previous research on menopause at work, this heterogeneity of sample for this exploratory study 1 did not limit findings to specific professions. Interviewees were recruited through indirect advertising of the project, and through word of mouth, or snowballing. The first author conducted all interviews over the period of 18 months from May 2018 to December 2019. None of the participants was directly asked about the menopause during their interview; the menopause was only discussed if the subject was raised by the participant herself. In fact, 16 out of 21 participants voluntarily raised the issue of menopause as something of significance to the appearance of bodily ageing at work. However, when raised, the interviewer (i.e. the lead author) asked probing questions to gain greater insight into participant experience thus generating this rich seam of data on menopause experience. Table 1 shows the overview of our sample in study 1.
The overview of participant information from study 1.
Results
Coping with menopause symptoms at work
Data revealed that participants were struggling to cope with menopause symptoms at work and very few sought assistance from external sources. Further, there was a clear acknowledgement from women in this study of a detrimental impact on work performance owing to a range of physical and psychological menopause symptoms, as exemplified by: I’m seriously struggling with the menopause . . . the fatigue and everything that’s impacting on everything. (Ursula, 50, Administrator ) . . . you are working all day in a very demanding job, physically . . . everything is timed [long pause] an awful lot of energy required for that . . . I’m an older woman, I’m into my 50s, peri-menopausal, I’m not able for a lot of that. (Laura, 50, teacher) I’m having really bad sweats . . . very exhausted a lot of the time, not sleeping well. (Fran, 56, Administrator)
In addition to an awareness of menopause symptoms adversely impacting actual performance, participants also acknowledged a perception around job performance decline, exemplified by Tania, a 50-year-old university professor, who had recently been offered counselling at work to cope with perceived work performance concerns: . . . just not being able to perform and being resilient . . . have I just given a poor perception of someone that can’t function but yet you know I’m [examples of recent professional acclaim] . . . menopause is changing how you act . . . your behaviour.
There was an overwhelming narrative of coping, or trying to cope. Through a narrative of resilience, menopause symptoms were described as something to be endured, put up with, something women had to learn to live with. Women felt that the onus was on them personally to cope with menopause symptoms, without drawing attention to themselves at work. Harriet (47, director) exemplified this concept with her assertion that she needed to get her body under control: ‘I’m going through the change . . . one day I’ll be like down here and the next day I’m up here . . . so I need to get that under control.’ Very few participants sought help from support systems at work instead choosing to downplay or even hide the severity of symptoms.
The variability of support at work
Data revealed the importance of effective and appropriate supervisory support to help women cope with menopause symptoms. Overwhelmingly, however, participants’ experience of support from their organisations was largely non-existent. For example, Vera (56, business manager) spoke about how her senior managers, all of whom were male, were reluctant to approach the issue of the menopause at work; however, she was complicit in this lack of engagement assuming that her male managers could not ‘cope’ with managing the menopause: ‘we’ve not even opened that Pandora’s box . . . because they can’t cope with it.’
Participants with male managers addressed concern over their perceived reluctance to manage menopause symptoms, which created a barrier to workplace supervisory support relationships as illustrated by the following selected quotes: He’s a man, he’s an older man . . . So, I went to [other manager] ’cause . . . she kind of has ultimate responsibility. (Ursula, 50, Administrator) . . . it’s very difficult when you’re standing in front of a class and perhaps you have to go to the loo . . . and that’s hard when you’re a teacher, ’cause you can’t just run off and leave your class . . . It can be very embarrassing with male staff . . . can be very awkward . . . I don’t think they need to know the finer points of what’s happening to a woman’s body, but they do need to be aware that you can have anxiety and all sorts of different things can manifest themselves. (Penny, 51, teacher)
There was a sense that women wanted to discuss how menopause symptoms impact their work ability within their organisations, although very few felt that they had supervisory or social support networks to facilitate this discussion. One of the few examples of workplace support was generated by the participant herself. Julia, a 50-year-old teacher, began informally discussing menopause at work within her peer group, actively looking for support: ‘I’m talking to more and more women at work about menopausal symptoms, just small things, we get tired in the evening, we’re on our feet from 8 a.m. in the day until the evening and we get tired.’ Further, there was a desire to ‘legitimise’ the effect of menopause symptoms at work as a genuine workplace health issue, for example: It’s quite an individual thing, but it needs to be somehow legitimised, so if I say legitimately that I suffer from age-related fatigue . . . it’s an actual medical fact that didn’t affect me two to three years ago . . . but it’s a critical six years, between your early mid-40s and your early 50s, there’s a phenomenal change. (Laura, 50, teacher)
By legitimising the taboo subject of the menopause at work, participants felt that supervisory support would increase from greater awareness of the impact of the menopause at work. However, the desire for overt workplace support was not unanimous. For example, Georgina, a 55-year-old director, expressed her desire to keep the menopause out of her world of work. Her fears were around being seen as ‘an older woman’ and attributed the menopause as a signpost of gendered ageing at work: ‘Yesterday one of my colleagues started saying, Menopause! Menopause! in the office. We’re meant to talk about menopause at work. . . . Is that helpful?’
Discussion
Menopause is a workplace issue causing substantial disruption to the working life of women in mid- to later life (Grandey et al., 2020). Our findings from exploratory study 1 clearly show that our participants felt a personal, individual responsibility to manage or cope with their menopause symptoms at work, often choosing to hide the impact of menopause symptoms on job performance, reinforcing the taboo nature of this subject (Grandey et al., 2020; Jack et al., 2019). Gender of supervisor or human relations manager emerged as an important factor in how women felt that they were able to cope with menopause symptoms at work. In line with previous work, embarrassment around male supervisors reinforced the shameful and taboo nature of menopause at work (Griffiths et al., 2013; Hardy et al., 2018), even to the extent that women perceived that they had done something wrong (Grandey et al., 2020; citing High and Marcellino, 1994), or are part of a ‘problem group’ (Bochantin, 2014).
Further, some women actively hid menopause symptoms to avoid their impact at work; however, this arguably reinforces the need for organisations to better support managing menopause. Some women, conforming to an ‘ideal’ menopausal woman as one who ‘takes control of her symptoms’ (Butler, 2020: 4), agentically acted to circumvent traditional supervisory support where that supervisor was a man to instead find an empathetic peer-aged female elsewhere in the business to act as a surrogate supervisor. This finding sheds some light on previous research that women ‘fail’ to seek help and advice (Goldman, 2010). Rather than failing to find support, the support available to women in our study was deemed ineffective, inappropriate or unavailable and they were forced, through agentic adaptive behaviours to find alternatives, such as the use of SOC strategies (e.g. using optimisation through seeking help from a female manager rather than her male supervisor).
The relationship with supervisor appears specifically important, where male supervision can lead to an awkward situation for the reporting of menopause symptoms, an empathetic older female supervisor can create an accommodating arrangement without drawing upon broader human resource (HR) policy. These findings support Hickey et al.’s (2017) suggestion that, rather than a supervisor, there should be a dedicated HR professional for concerns around the menopause and that women should also seek social support from peers ‘who got each other’ to managing their menopause symptoms at work (Butler, 2020). Abernethy (2018) posited that how a woman decides to manage menopause symptoms at work was a matter of personal choice of behaviours, which of course assumes that women are resilient and can engage in active coping behaviours as well as have access to resources including social support (Smith et al., 2008). Our findings suggest that women struggled to cope with menopause at work through inappropriate and insufficient supervisory and/or social support at work. Our findings reinforce Whiteley et al.’s (2013) constellation of symptoms, suggesting that future studies should consider the impact of a wider range of physical and psychological menopause symptoms at work. Our findings show the heterogeneous and individual nature of the menopause, highlighting the challenge for organisations. We further unpack these findings in our second study.
Study 2
Hypotheses development
Study 2 sought to test a number of hypotheses derived from our findings from study 1. First, we aim to explore the strength of the associations between the severity of physical and psychological menopause symptoms and workplace outcomes that were found particularly salient in our inductive study, such as job performance and retention. Second, we further unpack the role of SOC strategies and supervisory and female peer social support, respectively, in how women manage their menopause symptoms at work, as these have surfaced from our in-depth data as key individual and contextual resources for women to manage their symptoms at work. Following Halbesleben et al. (2014a: 1338), we define a resource as ‘anything perceived by the individual to help attain his or her goals’. Based on this definition, the use of SOC strategies falls in the category of individual or personal resources, whereas supervisory and female peer support are part of contextual resources.
Although the menopause experience varies in terms of type of symptoms and their severity, we expect that the more severe the physical and psychological menopause symptoms are, the more adversely they affect women in the workplace (Atkinson et al., 2021; Grandey et al., 2020). Women’s narratives from our first study support this argument as well as other qualitative research that showed how women experiencing menopause might suffer from poorer job performance (Brewis et al., 2017; Griffiths et al., 2006; Kleinman et al., 2013) and retention (Atkinson et al., 2021; Brewis et al., 2017; Griffiths et al., 2010; Jack et al., 2014). The experience of physical and psychological menopause symptoms is likely to create difficulties for women in the workplace, such as reduced ability to pay attention to details, concentrate and stay focused and learn as well as poorer memory and cognitive processing ability (Atkinson et al., 2021; Brewis et al., 2017). The more significant health-related demands that the menopause symptoms impose on women, the more significantly they may affect their performance and retention. Therefore, differentiating between physical and psychological menopause symptoms, we propose the following hypothesis:
Hypothesis 1: The severity of physical and psychological menopause symptoms is negatively related with job performance and retention, respectively.
As observed in our first study, women felt that it was their responsibility to manage their menopausal bodies in the workplace through the use of agentic adaptive behaviours to maintain their performance and stay in the workplace. These findings resonate with the arguments of SOC theory (Baltes, 1997; Freund and Baltes, 2002) in that women who are more likely to use the SOC strategies are able to better adapt to physical and psychological effects of their menopause symptoms, which could translate into them exhibiting improved performance and higher retention compared with those women who are less likely to use SOC strategies. According to the SOC literature, there are various mechanisms that can explain the effectiveness of SOC behaviours (Freund and Baltes, 2002; Zacher and Frese, 2011). For instance, the use of SOC behaviours should enhance the effective allocation of personal resources as well as adaptation to the loss of resources to carry on performing despite the menopause-related challenges. The use of SOC strategies should also help women to more effectively adapt to their external, contextual demands in their workplace, which should lead to better performance and retention. Finally, women who use SOC strategies are expected to set goals for themselves more flexibly and adapt them to their external demands better than women who do not use such strategies. Although they did not draw from the SOC framework as such, we found two studies that identified the use of agentic behaviours similar to SOC in managing the experience of menopause. Griffiths et al. (2013: 158) observed that one-third of their respondents reported that their performance would be negatively affected if ‘they did not work hard to compensate for the difficulties their symptoms presented’. Im and Meleis (2001) in their qualitative study observed that menopausal women, rather than changing their working hours or employer, worked harder to compensate for the negative impact of their symptoms on work outcomes. Therefore, we would expect that the use of SOC strategies should help women cope with their menopause-related physical and psychological health demands in terms of protecting their performance and retention.
However, in addition to using agentic adaptive strategies to cope with menopause symptoms, study 1 revealed that working in a supportive context helps offset the negative impact of symptoms on work outcomes. Women acknowledged the importance of supervisory support to help them cope with menopause symptoms, although oftentimes supervisory support was ineffective or lacking. This resonates with Jack et al. (2014) who argued that women feel relief if they are able to talk about their menopause experience with their supervisors and colleagues, which could significantly buffer the negative impact of menopause symptoms on their performance and career opportunities. An interesting finding from our first study was that women felt particularly supported by their female colleagues, who were more likely to ‘feel their pain’. Based on this evidence, in our second study we focused on female peer and supervisory social support as two contextual resources that could help women cope with their menopause symptoms. Social support has been extensively studied as a buffer in previous research (Bavik et al., 2020). When individuals’ demands exceed their resources, the perceived stress is expected to trigger coping, whereby higher levels of social support increase coping resources, which in turn should ameliorate the negative effects of demands on individual outcomes. Menopause symptoms can be considered as a type of individual health demand and as such, we could expect that higher levels of female peer and supervisory social support would buffer the negative effects of symptoms on performance and retention. Taken together, our inductive study showed that women use individual agentic behaviours, such as SOC strategies, to cope with their symptoms as well as they appreciate having a supportive context that normalises the experience of menopause in the workplace. Therefore, in our second set of hypotheses, we test the joint buffering effect of the use of SOC strategies and female peer and supervisory social support, respectively, and predict the following:
Hypothesis 2a: The use of SOC strategies and female peer support moderate the negative relationships between the severity of physical and psychological menopause symptoms and job performance and retention, respectively, such that these relationships are weaker when both the use of SOC and female peer support are high.
Hypothesis 2b: The use of SOC strategies and supervisory support moderate the negative relationships between the severity of physical and psychological menopause symptoms and job performance and retention, respectively, such that these relationships are weaker when both the use of SOC and supervisory support are high.
Method
Participants
We used two samples in the second study. Sample 1 was recruited via Prolific and was composed of 239 women (the average age: M = 51.11 years; SD = 4.22). We used this sample to validate our measures of the severity of menopause symptoms, retention, supervisory support and female peer support that we developed specifically for the purposes of this study. The majority of participants (55.6%) were in full-time employment, followed by 26.8% who were employed part-time, 15.1% who were self-employed and 2.5% who indicated another type of employment, such as casual agency workers. In terms of type of jobs, the majority (25.1%) worked in administrative and clerical roles, followed by 19.7% who worked in professional services, 10.9% had managerial roles, 10% were in teaching jobs, 7.1% had manual jobs, 6.2% had retail jobs, 3.8% had research and academic jobs and 17.2% were in other jobs. In terms of industry, 30.2% worked in public services, including healthcare and administration, followed by 23.0% who worked in teaching and education-related industries. Most of them (57.3%) had a female supervisor. The majority of their supervisors were 50 to 59 years old (36.4%), followed by those who were 40 to 49 years old (33.9%).
We recruited participants for our sample 2, which was used for testing the hypotheses, via networks of women who provide social and emotional support to those experiencing menopause. We created an online survey and used a snowballing technique to reach our participants. After sending the survey link to our contacts from different menopause support networks, we also invited our personal contacts to complete the survey and asked them to send it onto any woman who was going through the menopause at the time of the data collection. This sample was composed of 142 women with the average age of 51.15 years (SD = 4.74). The majority of them (59.2%) were in full-time employment, followed by 25.4% who were employed part-time, 5.6% who were self-employed and 3.5% who indicated another type of employment, such as having zero hours contract or a combination of part-time and freelance employment. A total of 6.3% of the participants did not answer this question. The majority (21.8%) worked in managerial roles, followed by 21.1% who worked in professional services, 20.4% who had administrative and clerical roles, 8.5% worked in teaching jobs, 6.3% had research and academic jobs, 2.8% worked in manual jobs, 1.4% worked in retail and 17.6% who had other type of jobs. In terms of industry, 33.1% worked in public services, including healthcare and administration, followed by 19.7% who worked in teaching and education-related industries. Most of them (59.9%) had a female supervisor. The majority of their supervisors were 50 to 59 years old (37.7%), followed by those who were 40 to 49 years old (33.1%).
Procedure
For the purpose of this study, we first had to develop four measures that captured very specific aspects of women’s experience at work that were derived from our study 1. Specifically, these measures were the severity of menopause symptoms, retention, supervisory support and female peer support. To ensure the validity of these newly developed measures, a two-step approach was followed. We first conducted a pilot study to test the survey for face validity and confirm that all the items were meaningful before rolling out the survey comprising these newly developed measures on our first sample. Six women who either were academics in the field of gender research or had themselves experienced menopause at work have read through the survey. Based on their suggestions, we made minor modifications to the wording of some items and response scales. We then recruited our first sample to provide a psychometric assessment of the four measures that we developed. Once these measures were validated, we collected the data on our second sample using revised measures of menopause symptoms, supervisory support, female peer support and retention. On this sample, in addition to these revised measures, we also measured the use of SOC, job performance and trait resilience by means of already established scales with minor modifications to adjust these to the context of our study. There were no significant differences between sample 1 and sample 2 in terms of the participants’ age, employment status, gender and age of their supervisors, and industry. Before proceeding with the hypotheses testing, we conducted a set of confirmatory factor analyses of all measures using our sample 2 to provide a final test of the validity of our measures.
Measures designed for the purpose of this study to be validated on sample 1
Menopause symptoms
Our measure of severity of menopause symptoms was largely inspired by the Menopause Rating Scale (Heinemann et al., 2004). This has been one of the most often used scales to assess menopause symptoms and has showed good psychometric characteristics in previous research (Hickey et al., 2017). We have taken nine symptoms from the original scale that have also been reported by our participants in study 1, as follows: hot flushes, heart discomfort, sleep problems, depressive mood, irritability, anxiety, physical and mental exhaustion, bladder problems, and joint and muscular discomfort. We added seven further symptoms that were reported by women in our study 1 to this list, such as fatigue, weight increase, itchy skin, hair loss, menstrual flooding, lowered resilience and reduced confidence. Participants rated the severity of each symptom using a five-point response scale, ranging from 1 (none) to 5 (very severe).
Female peer support
Two items were developed to assess the extent of social support women receive from female peers to manage their menopause at work (e.g. ‘My female colleagues are a key source of support for managing my menopause symptoms’). A five-point response scale, ranging from 1 (strongly disagree) to 5 (strongly agree) was used.
Supervisory support
We used eight items to assess supervisory support. Four items (e.g. ‘My line manager cares about my opinions’) were adapted from the scale developed by Rhoades et al. (2001) and four were developed for the purpose of the current study to measure the supervisory support specifically in relation to the experience of menopause (e.g. ‘My line manager wants to better understand how the menopause impacts me and my work’). A five-point response scale, ranging from 1 (strongly disagree) to 5 (strongly agree) was used.
Retention
We developed five items to measure the impact of the menopause symptoms on retention and intention to stay in the current organisation based on our findings from study 1 (e.g. ‘Due to menopause symptoms, I have not sought promotion’). We reversed the items that were worded in a way that suggested negative impact of menopause symptoms, so that the higher score on this scale indicated higher retention. Participants replied to each item using a five-point response scale, ranging from 1 (never) to 5 (always).
The results of the exploratory factor analysis
We submitted the 31 items that we developed to measure the severity of the menopause symptoms, female peer support, supervisory support and retention to the exploratory factor analysis using principal components and varimax rotation. This analysis yielded eight factors, explaining 66.58% of the variance. In addition to eigenvalues, we also conducted the parallel analysis and minimum average partial test (MAP) to strengthen our decision making of how many factors we should extract (O’Connor, 2000). These two methods suggested that we should extract between four and five factors, respectively. Next, we explored the factor loadings across the first four and five factors. With the exception of three items from the menopause symptoms scale referring to itchy skin, hair loss and menstrual flooding and one item from the retention scale, the remaining 26 items loaded across the first five factors as suggested by the MAP test. 2 Specifically, four items of retention loaded on one factor (Cronbach α = .83; CR = .80), both items referring to female peer support loaded on a separate factor (Cronbach α = .85; CR = .85) and eight items of supervisory support loaded on its own factor (Cronbach α = .91; CR = .89). A closer examination of the remaining two factors showed clear support for two types of menopause symptoms, namely psychological symptoms (seven items; Cronbach α = .87; CR = .83) and physical symptoms (six items; Cronbach α = .73; CR = .71). We decided to keep these 26 items in our further analysis and data collection using sample 2.
Measures for the hypotheses testing using sample 2
Menopause symptoms
Based on the exploratory factor analysis on sample 1, we used a revised measure of menopause symptoms, comprising seven items referring to psychological symptoms (i.e. depressive mood, irritability, anxiety, lowered resilience, sleep problems, physical and mental exhaustion, and reduced confidence) and six items referring to physical symptoms (i.e. hot flushes, heart discomfort, fatigue, weight increase, bladder problems, and joint and muscular discomfort). We used the same response scale as on sample 1.
Female peer support
We used the same two items and response scale as on sample 1 to measure female peer support since the exploratory factor analysis supported the validity of our initial measure.
Supervisory support
We used the same eight items and response scale as on sample 1 to measure supervisory support since the exploratory factor analysis supported the validity of our initial measure.
Selection, optimisation and compensation
SOC strategies were measured with 12 items that were adapted from Zacher and Frese (2011). We have slightly modified each item to fit the context of our study (e.g. ‘At work, when experiencing menopausal symptoms, I concentrate all my energy on few things’). Participants rated each item using a five-point response scale, ranging from 1 (strongly disagree) to 5 (strongly agree).
Retention
We used a revised measure of retention consisting of four rather than five items based on our exploratory factor analysis. We used the same response scale as on sample 1.
Job performance
We assessed job performance by means of a seven-item scale (e.g. ‘I adequately complete the assigned duties’) by Williams and Anderson (1991). Participants replied to each item using a five-point response scale, ranging from 1 (never) to 5 (always).
Control variables
Because the focus of our study was on menopause at work, we adjusted our results for number of days working from home in a usual week. We also controlled for trait resilience, because trait resilience can explain how individuals can inherently maintain vigour and commitment to important life tasks, despite external challenges such as experiencing poor health (Hobfoll, 2010). Also, our study 1 findings suggested that women who were inherently more effective at coping with stressful events, might be better at managing their symptoms. Finally, one of the psychological health-related symptoms in our measure refers to lowered resilience. Taken together, we controlled for trait resilience to eliminate its confounding effects from our main findings. We assessed trait resilience by means of six items (e.g. ‘I tend to bounce back quickly after hard times’) from Smith et al. (2008), using a five-point response scale, ranging from 1 (strongly disagree) to 5 (strongly agree). We also controlled for the supervisor’s gender and age as previous research (Griffiths et al., 2013; Hickey et al., 2017) and our study 1 findings suggested that women were less likely to disclose their menopause symptoms to male and younger supervisors.
The results of the confirmatory factor analyses
We carried out a set of confirmatory factor analyses to confirm the convergent and discriminant validity of all our measures to be used in hypotheses testing, including trait resilience as our control variable. As shown in Table 2, our theoretical measurement model comprising eight latent constructs (i.e. psychological symptoms, physical symptoms, SOC strategies, female peer support, supervisory support, performance, retention and trait resilience) yielded acceptable fit to the data. All items significantly loaded on their predicted factors and the fit of our measurement model was significantly better compared with all other alternative models, supporting the convergent and discriminant validity of our study measures. Further, we assessed the extent to which our results might be inflated by the common-method bias by means of Herman single factor test and unmeasured latent method factor technique (Podsakoff et al., 2003). Our results in Table 2 show that our measurement model showed a significantly better fit than the single factor model (Δ χ2 (Δdf) = 1539.31 (28), p < .01). Next, the fit of the nine-factor model, including our predicted eight factors and a common latent method factor (χ2 = 1587.64, df = 1162, p < .01; CFI = .90; TLI = .88; SRMR = .08) was not superior to our measurement model (Δ χ2 (Δdf) = 64.02 (51), p > .05). These results give us confidence that the common-method bias was not an issue in our study.
Confirmatory factor analysis fit indices to confirm the construct validity of our measures on our main sample.
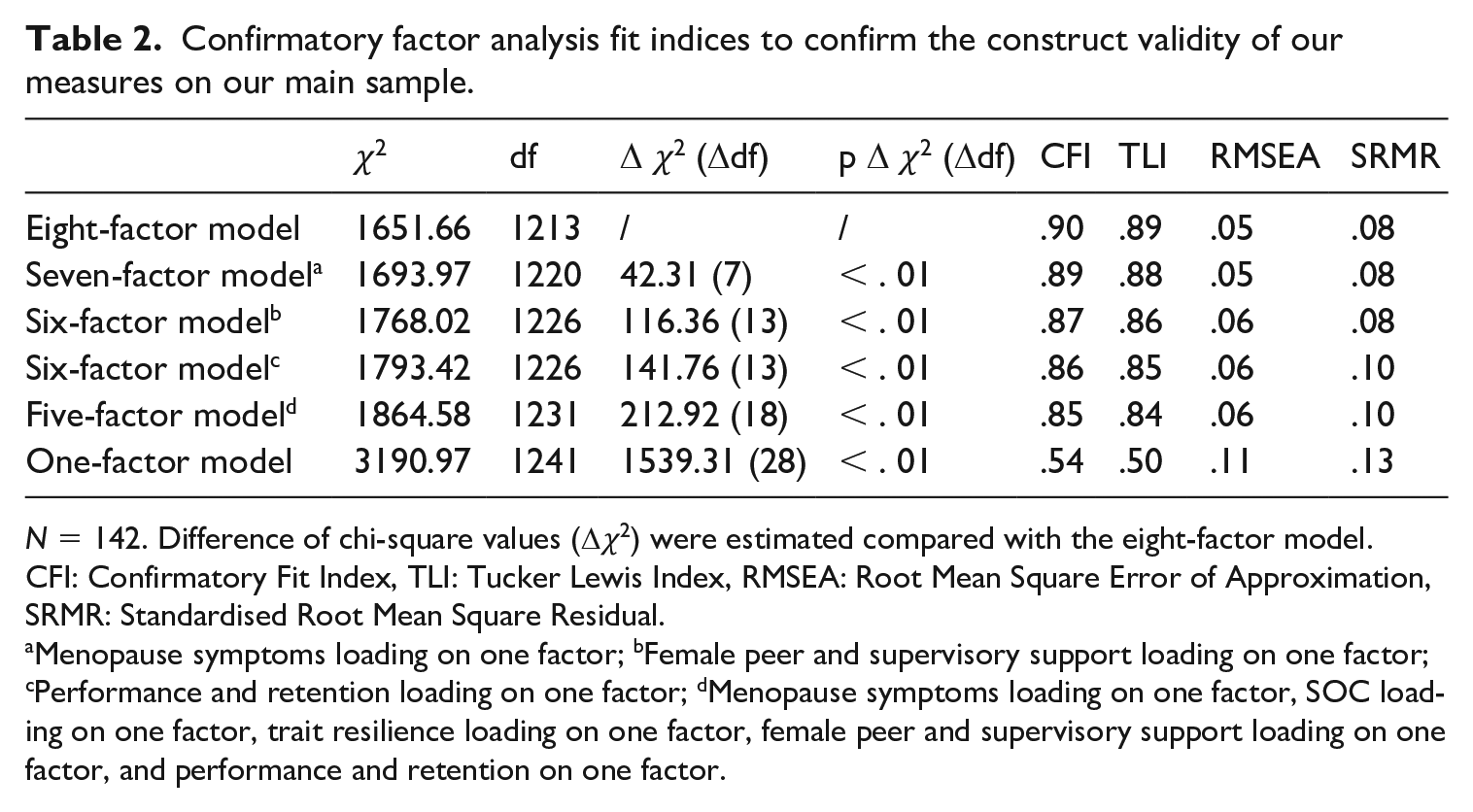
N = 142. Difference of chi-square values (Δχ2) were estimated compared with the eight-factor model. CFI: Confirmatory Fit Index, TLI: Tucker Lewis Index, RMSEA: Root Mean Square Error of Approximation, SRMR: Standardised Root Mean Square Residual.
Menopause symptoms loading on one factor; bFemale peer and supervisory support loading on one factor; cPerformance and retention loading on one factor; dMenopause symptoms loading on one factor, SOC loading on one factor, trait resilience loading on one factor, female peer and supervisory support loading on one factor, and performance and retention on one factor.
Results
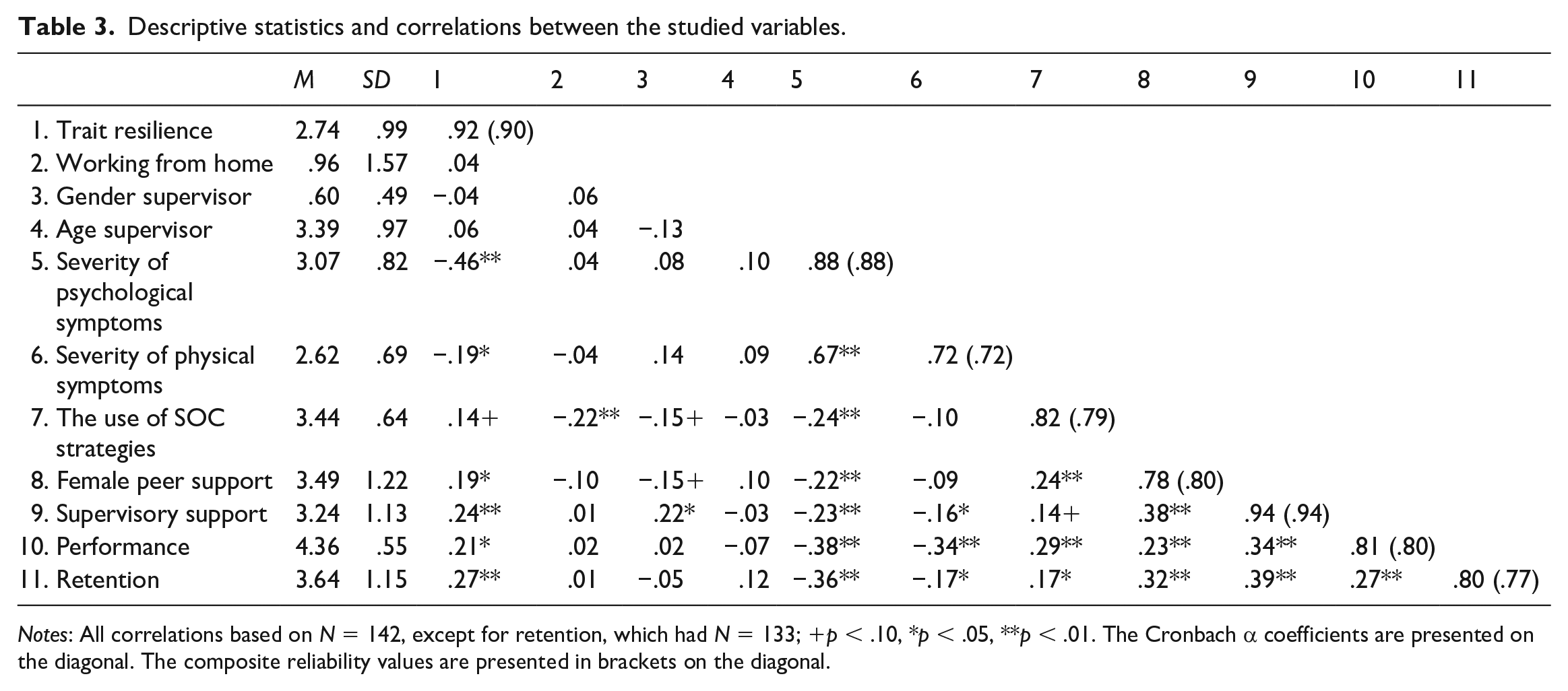
Table 3 shows descriptive statistics and correlations among the studied variables. These results show preliminary support for our hypotheses.
Descriptive statistics and correlations between the studied variables.
We tested our hypotheses by means of hierarchical regression analyses, whereby we introduced the control variables in the first step, followed by the severity of both types of menopause symptoms, the use of SOC strategies, female peer support and supervisory support, respectively, in the second step, all two-way interactions in the third step and finally the three-way interactions between each dimension of menopause symptoms, the use of SOC strategies, and female peer support and supervisory support, respectively, in step four.
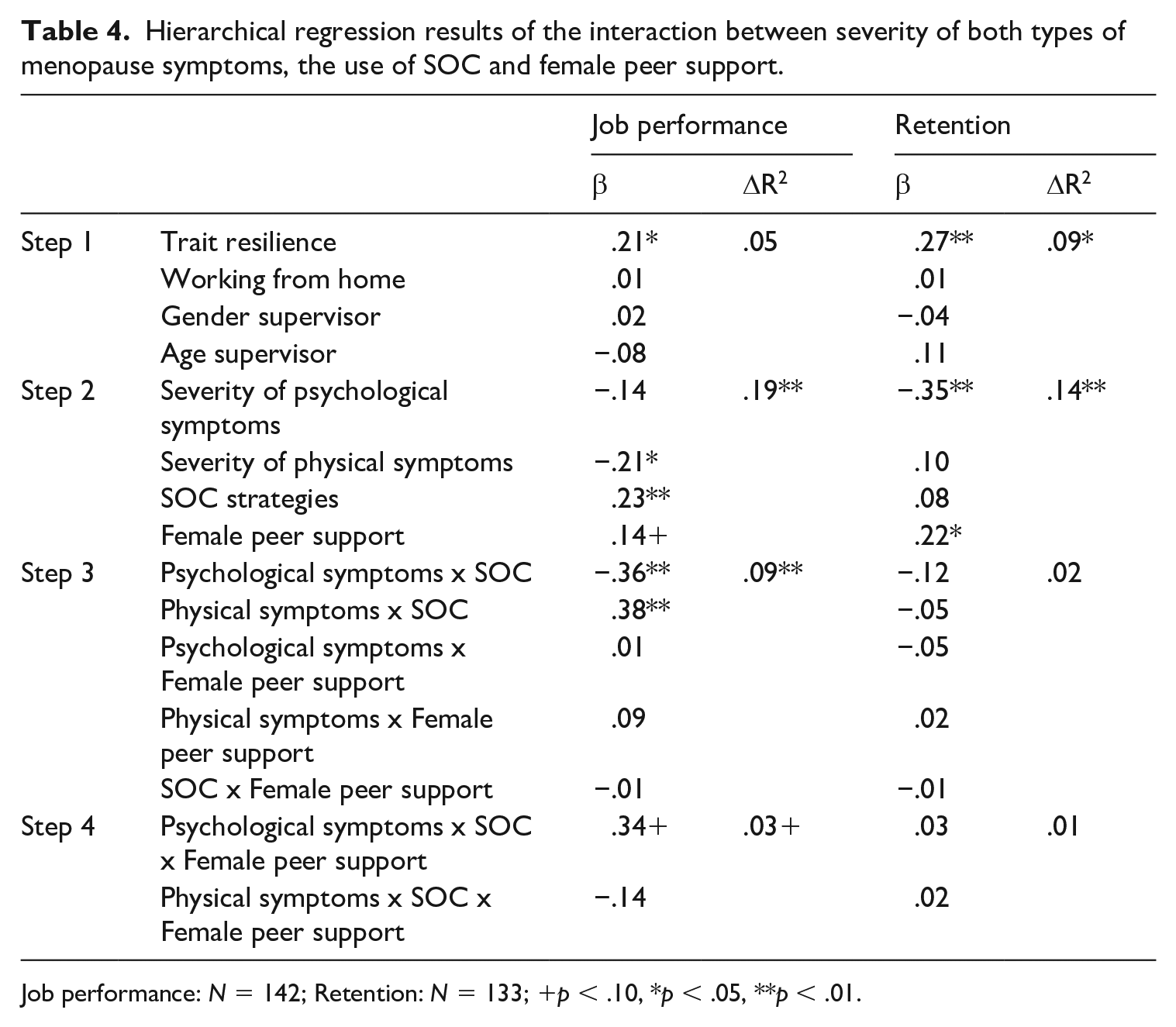
Tables 4 and 5 show the summary of hierarchical regression results. We found significant negative relationships between physical symptoms and job performance (β = −.21, p < .05 when regressing SOC and female peer support and β = −.17, p < .10 when regressing SOC and supervisory support). We also observed a significant negative relationship between psychological symptoms and retention (β = −.35, p < .01 when regressing SOC and female peer support and β = −.36, p < .01 when regressing SOC and supervisory support). These results partially support Hypothesis 1.
Hierarchical regression results of the interaction between severity of both types of menopause symptoms, the use of SOC and female peer support.
Hierarchical regression results of the interaction between severity of both types of menopause symptoms, the use of SOC and supervisory support.
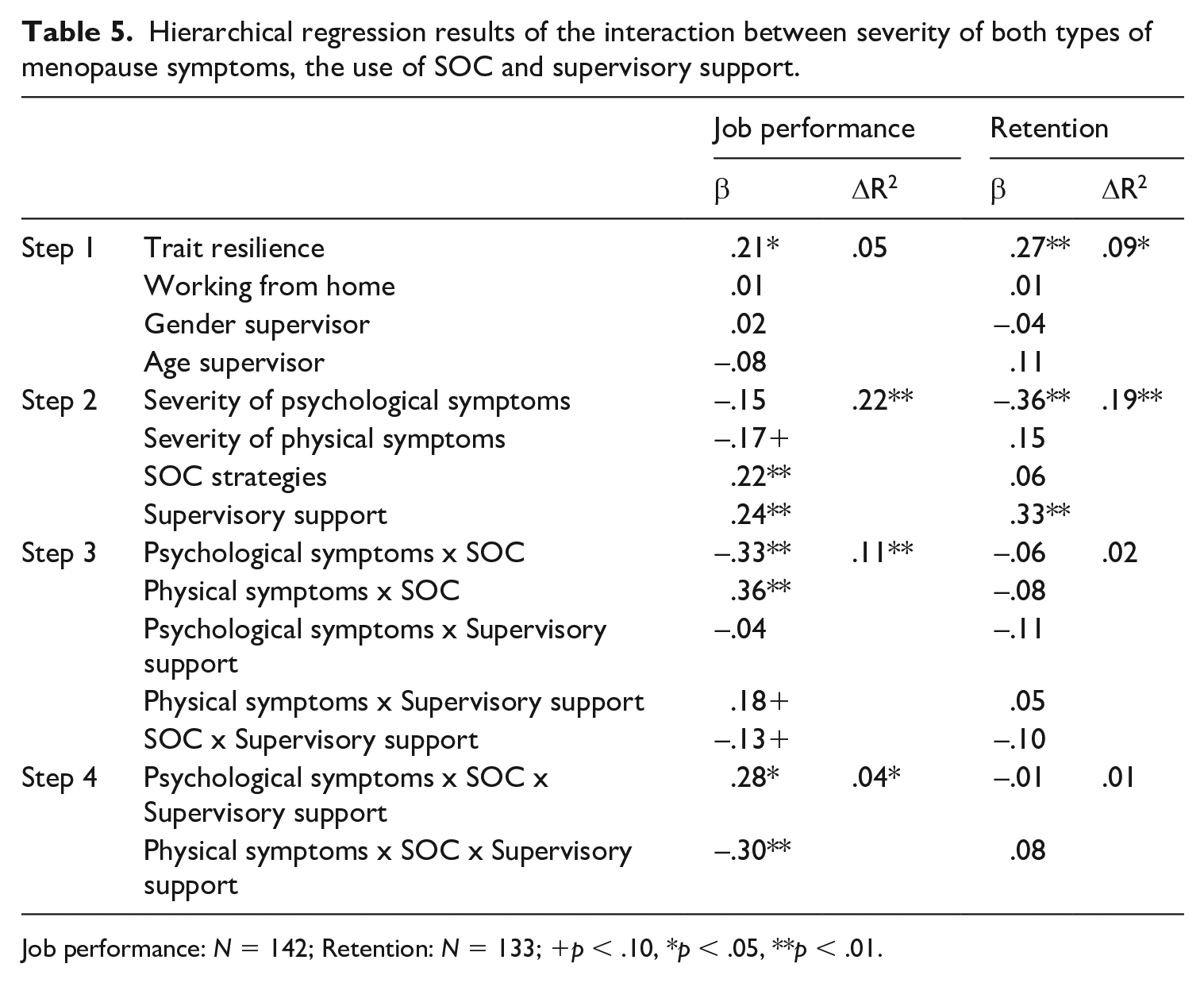
Job performance: N = 142; Retention: N = 133; +p < .10, *p < .05, **p < .01.
In relation to the moderating role of SOC and female peer support, we found a marginally significant interaction effect between the severity of psychological symptoms, female peer support and the use of SOC strategies on job performance (β = .34, p < .10). We depict this interaction effect in Figure 1 at 1 SD below and above the mean of the severity of menopause symptoms and SOC strategies and female peer support. Our results show that the relationship between the severity of psychological symptoms and performance was negative in women who perceived low female peer support, although their use of SOC strategies was high (slope 2: t = −2.54, p < .05). The relationship between psychological symptoms and performance in groups with other combination of SOC and female peer support was not significant, although we should note that slope 2 was significantly different from slope 4 representing those women who reported low female peer support and low use of SOC (t = −3.32, p < .01). These results do not support Hypothesis 2a, since the use of SOC was found to aggravate rather than alleviate the effects of psychological symptoms on performance. Also, the interaction effect between the use of SOC, female peer support and the menopause symptoms on retention was not significant.
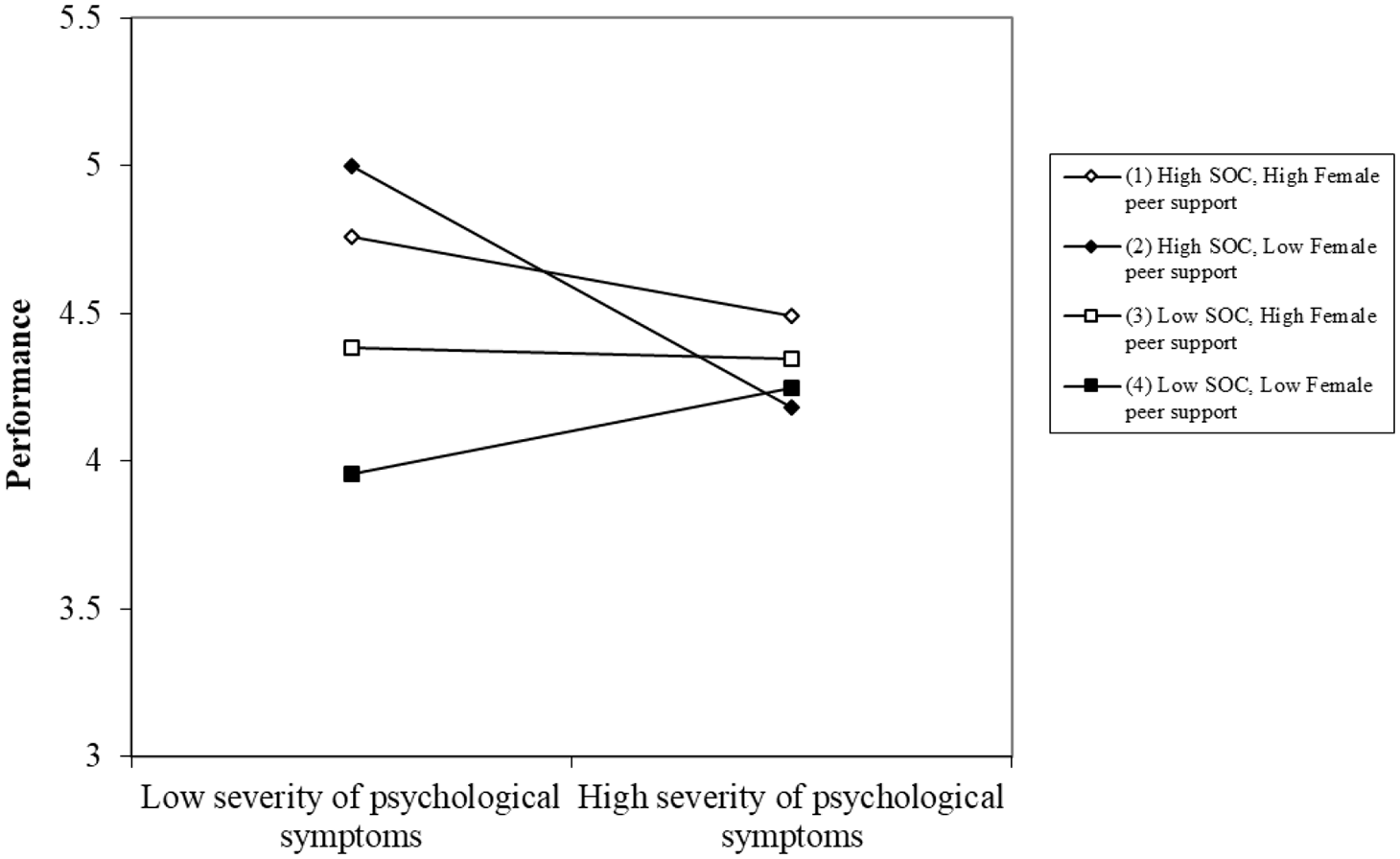
The interaction effect between the severity of psychological symptoms, the use of SOC strategies and female colleagues support on job performance.
Furthermore, we found significant interaction effects between psychological and physical symptoms, respectively, and the use of SOC and supervisory support on job performance. We depict these effects in Figures 2 and 3, respectively.
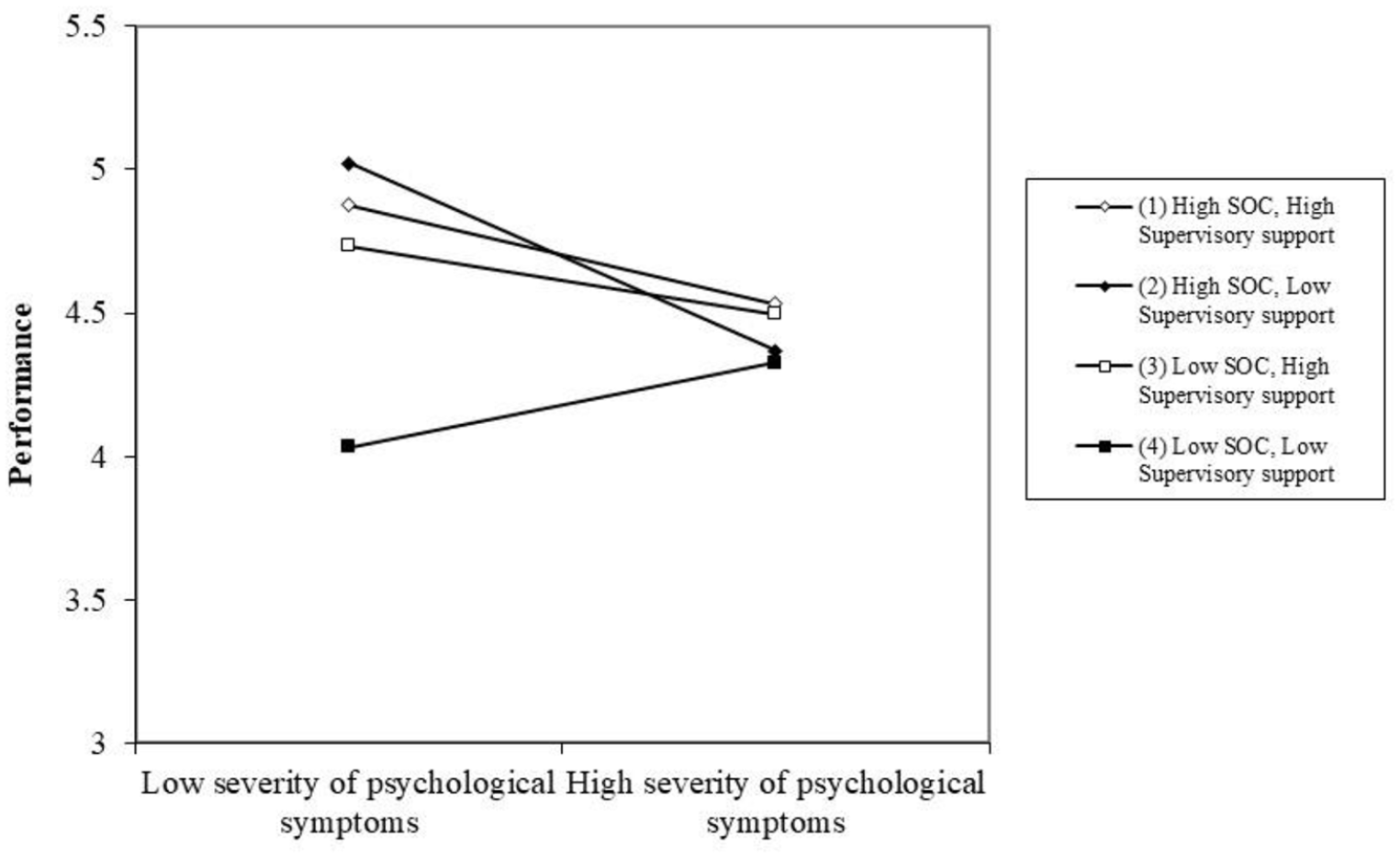
The interaction effect between the severity of psychological symptoms, the use of SOC strategies and supervisory support on job performance.
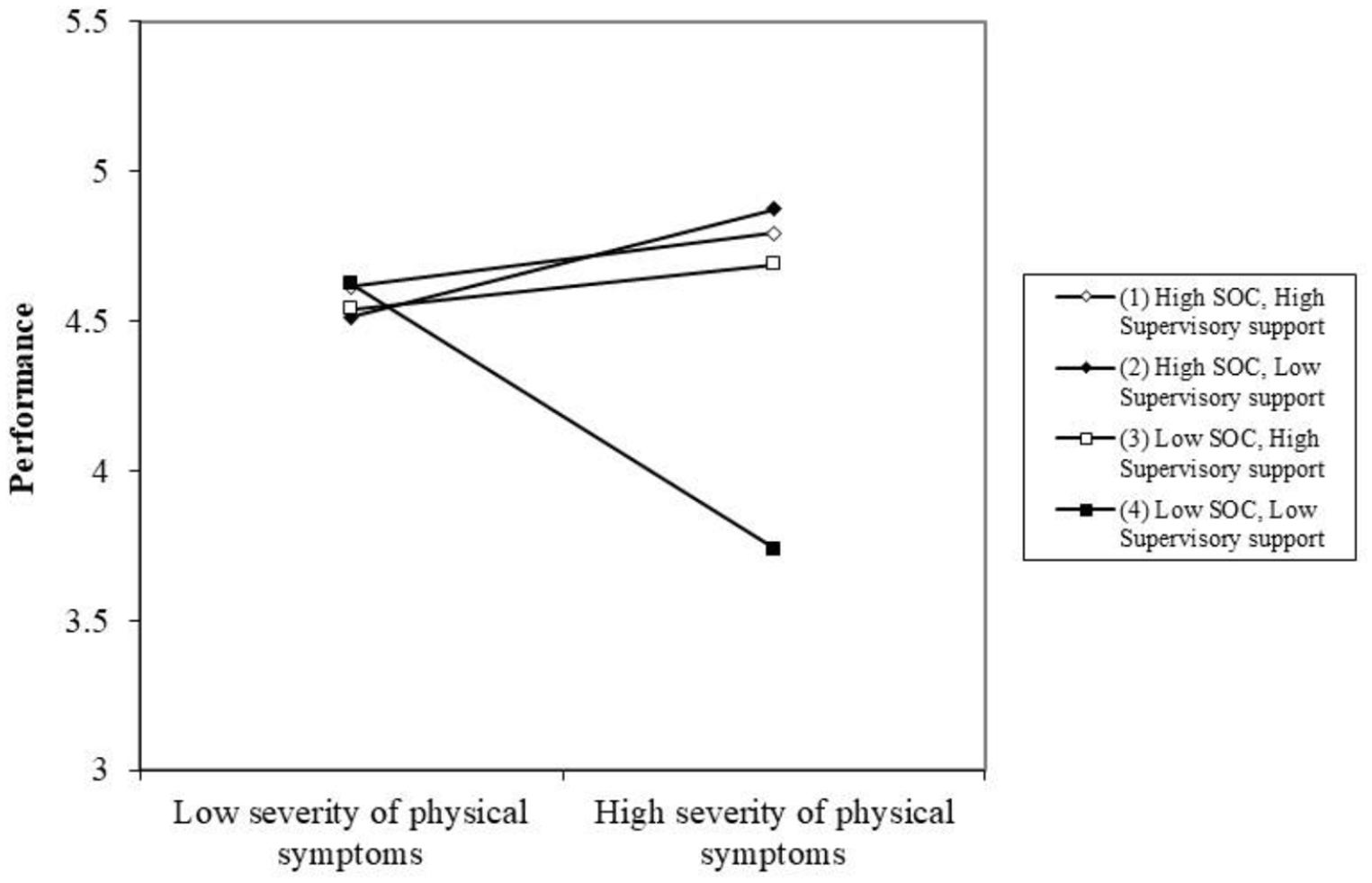
The interaction effect between the severity of physical symptoms, the use of SOC strategies and supervisory support on job performance.
Our results showed that the relationship between the severity of psychological symptoms and performance was negative in women who reported having low supervisory support, but high use of SOC (slope 2: t = −2.76, p < .01). The relationship between psychological symptoms and performance in groups with other combinations of SOC and supervisory support was not significant, although slope 2 was significantly different from slope 4, which refers to those women who experienced low supervisory support and low use of SOC (t = −3.35, p < .01). Also in this case, our results suggest a potentially detrimental effect of the use of SOC strategies on performance when women experience severe psychological symptoms. Further, our results show that the relationship between physical symptoms and performance is strongly significant and negative in those women who experienced low supervisory support and low use of SOC (slope 4: t = −14.01, p < .01). This group of women experienced significantly lower performance as their severity of physical symptoms increased, compared with those who experienced high supervisory support and high use of SOC (slope 1 vs 4: t = 3.76, p < .01), as well as those who experienced either high use of SOC, but low supervisory support (slope 2 vs 4: t = 9.84, p < .01) or low use of SOC, but high supervisory support (slope 3 vs 4: t = 5.79, p < .01). These results partially support Hypothesis 2b showing that when experiencing severe physical symptoms, the use of SOC strategies and having supervisory support is beneficial for buffering the negative effects of menopause on job performance; however, the use of SOC was detrimental when women experienced severe psychological symptoms.
Supplementary analysis
Owing to the cross-sectional nature of our research design in study 2, we could not establish the temporal ordering between our core variables. In order to address this issue, we analysed supplementary data that were obtained from 78 participants (55%) from our second sample – that is, the sample that was used for hypotheses testing – who shared their experiences of how menopause symptoms had influenced their work by means of qualitative answers at the end of the survey. Deductive analysis of these data provides a temporal structure for how participants experienced menopause symptoms at work, how this had influenced their work ability and performance (compared with pre-menopause) and the adaptive behaviours they used to cope with menopause symptoms at work. We provide here participant’s age, industry and gender of supervisor (i.e. F or M) following each quote.
Women in our study spoke about the temporal nature of menopause symptoms, crucially the change in their performance from the pre-menopause to menopause. There was a clear sense of distinction between their current experiences and of their pre-menopause experiences at work, as exemplified by: I used to be enthusiastic and ‘on the ball’ about work but now I have just lost interest and seem to be ploughing through a heavy field. (54, Third sector, F) I had to leave a well-paid position due to no support. I lost my house, my confidence and my self-worth. I felt like a failure. (55, Teaching, F) The menopause has made me question every aspect of the requirements . . . [of] my job effectively. I have lost all confidence in my abilities. (57, Healthcare, M) I resigned from my job that I really loved. I was fortunate to be taken back on once I spoke more openly about the menopause. It’s life changing I had coped and even enjoyed [job] for seven years until peri-menopause started. I had no choice but to leave. I sought a job with a team, decent terms and conditions and am blessed to have a supportive manager. (53, HR, F) I was fired in 2017 from my high-level job . . . I worked for the company for 19 years. Menopause was horrible, I had zero support even after reporting it, my manager drove me to burnout, and my HR manager said, ‘Maybe we should put a man in your job next time!’ And they did. (55, Energy/utilities, M) . (49, Teaching, F)
. (49, Teaching, F)
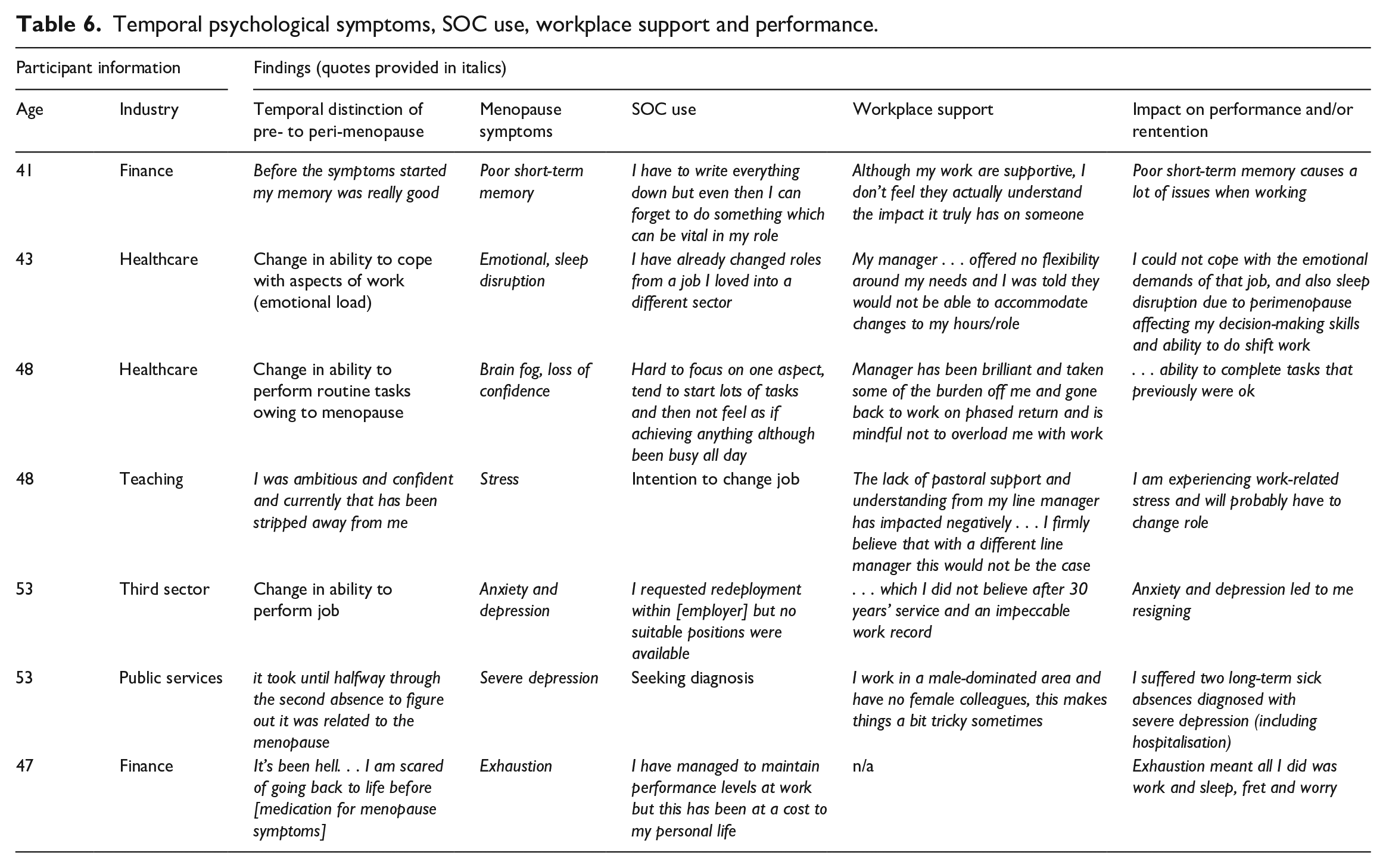
The following tables provide examples of quotes relating to psychological (Table 6) and physical (Table 7) menopause symptoms, their temporality, evidence of SOC use, workplace support, performance and retention outcomes. These experiences are in direct response to the impactful and changing nature of managing menopause symptoms at work.
Temporal psychological symptoms, SOC use, workplace support and performance.
Temporal physical symptoms, SOC use, workplace support and performance.
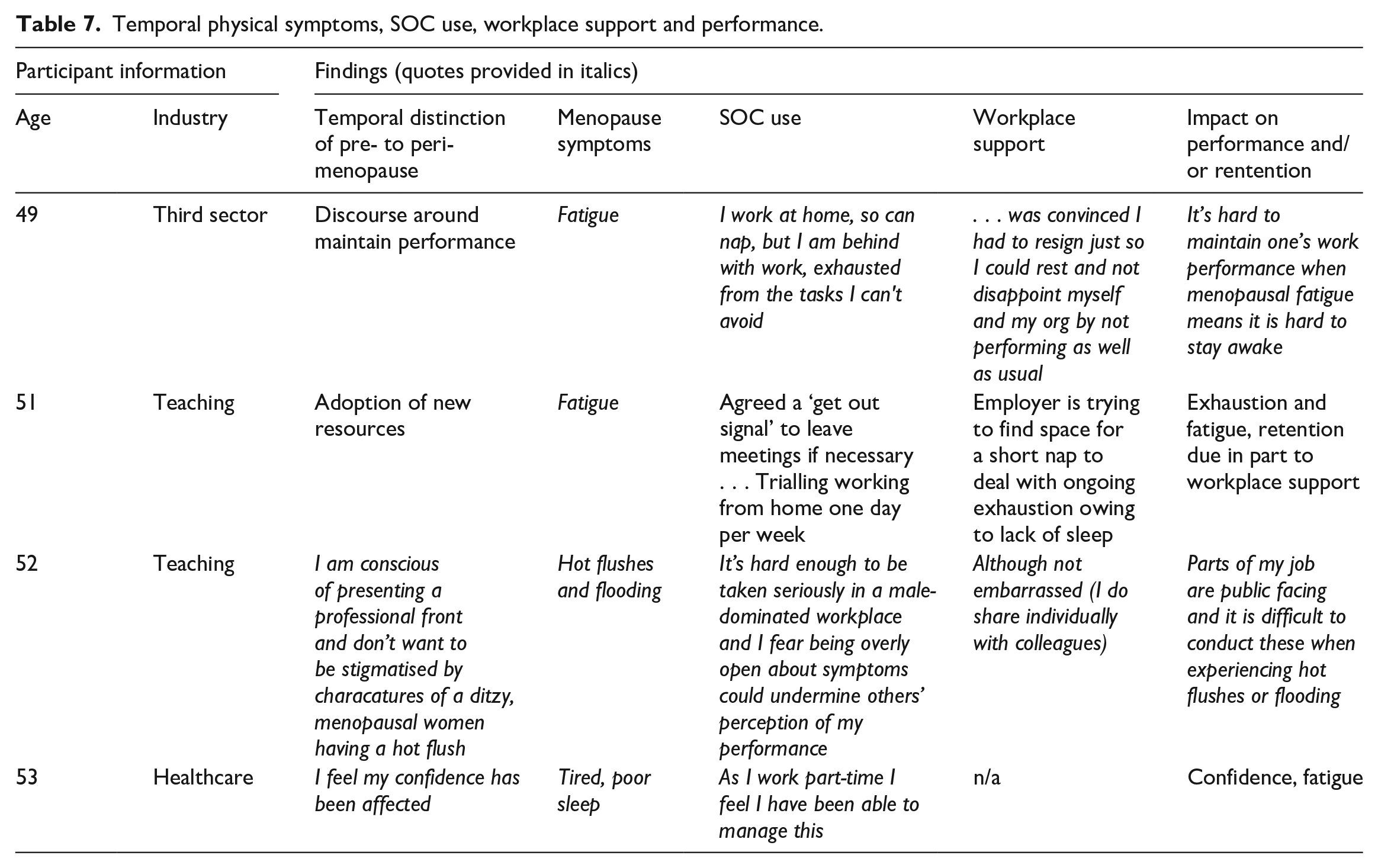
Although we could not use a longitudinal research design in our study, these data are situated in a temporal space whereby women speak about their pre-menopause performance and ability at work compared with their menopause-affected performance and how the use of SOC strategies during the menopause phase are adopted. These quotes also demonstrate the outcome of the temporal, changing nature of menopause and the relative efficacy of SOC use on menopause symptoms, providing a more explicit practical contribution of our findings. These findings provide further insight into the value of SOC as a theoretical framework by explicitly linking the challenges presented by menopause symptoms at work and corresponding coping strategies of personal and organisational resources.
Discussion
The main aim of our second study was to test two sets of hypotheses that we derived from our inductive study 1 to test the effects of physical and psychological menopause symptoms on job performance and retention. We also explored the joint role of SOC strategies and supervisory and female peer support, respectively, as pertinent individual and contextual resources to alleviate the negative effects of menopause symptoms on performance and retention. Our results showed that higher severity of physical menopause symptoms was related with poorer job performance, whereas higher severity of psychological symptoms was related with poorer retention. These findings resonate with previous research that observed connections between the menopause and poorer performance (Atkinson et al., 2021; Griffiths et al., 2013; Kleinman et al., 2013) and problems with retention (Atkinson et al., 2021; Brewis et al., 2017; Griffiths et al., 2010). Our findings also provide further support for studying different symptoms simultaneously owing to their differential relationship with employment outcomes.
The differential effect of psychological and physical symptoms on study outcomes was also observed when exploring the moderating role of SOC and social support. Unexpectedly, we found that when women suffered from severe psychological symptoms, the use of SOC strategies was detrimental rather than beneficial for their performance. It was female peer and supervisory support that buffered the negative effects of psychological symptoms on performance. Essentially, our findings suggest that women with severe psychological symptoms who were able to adapt their behaviours by means of prioritising their goals, obtaining additional and/or alternative resources to compensate for any loss of previously held resources, necessary to achieve their goals in the workplace, exhibited lower performance than women who did not use such SOC strategies. These findings do not only make a significant contribution to the literature on gendered ageing at work, but also to SOC theory by showing how using SOC strategies might in fact be damaging when women attempt to cope with psychological menopause symptoms, such as anxiety and depression.
However, SOC does not have such a detrimental effect when women experience severe physical symptoms. In this case, the use of SOC was strongly beneficial for offsetting the negative effects of physical symptoms on performance, suggesting that women who use SOC strategies are better able to adapt to the physical health-related demands that menopause imposes on women and as a result, they might be better at sustaining their performance in the workplace (Moghimi et al., 2017). Both types of social support buffered the negative impact of physical and psychological symptoms on performance, such that the relationship between symptoms and performance was not significant when women perceived having high female peer and supervisory support. These findings confirm that the work context plays a significant role in how women manage their menopause at work.
General discussion
Drawing from the scarce menopause at work literature and SOC theory, we aimed to explore how women experience menopause in the workplace and how this biological process affects their work outcomes. This is an important question because women in mid- to late careers derive considerable social support from their employment and it is therefore imperative that women are able to work for as long as they wish (Atkinson et al., 2021). Across both studies we found that women who experienced more severe symptoms were adversely affected in terms of their job performance and retention. Differentiating between two types of symptoms, our second study showed that the severity of physical menopause symptoms was particularly detrimental for job performance, whereas the severity of psychological symptoms adversely affected job retention. Both studies showed that women experiencing menopause successfully coped with their symptoms by drawing from the support from their supervisors and female colleagues. Both types of support were particularly important for coping with psychological symptoms for which engaging in action regulation strategies, such as SOC (Baltes and Baltes, 1990; Moghimi et al., 2017) was in fact counterproductive, as seen in study 2. We turn to the implications of these results next.
Theoretical contributions
Our research makes several theoretical contributions to the gendered ageing at work literature (Loretto and Vickerstaff, 2015; Trethewey, 1999) more broadly and to the management of menopause at work (Atkinson et al., 2021; Grandey et al., 2020; Steffan, 2021) more specifically. First, our findings show how women experience different menopause symptoms at work and how this constellation of symptoms might adversely affect their performance and retention (Atkinson et al., 2021; Grandey et al., 2020; Whiteley et al., 2013). Although women commonly experience these symptoms during their menopause, their impact on women’s work outcomes remains underexplored in academic literature (Griffiths et al., 2013; Jack et al., 2019). Specifically, our findings provide support for differentiating between two categories of symptoms, physical and psychological and, unlike previous research on menopause in the workplace (Griffiths et al., 2013; Hickey et al., 2017; Jack et al., 2019), we provide evidence on the strength of the association of the menopause experience with work outcomes: the severity of physical symptoms was significantly related with poorer performance, whereas the severity of psychological symptoms was significantly related with poorer retention. Women appeared to agentically support a broader narrative where being older was associated with the threat of economic redundancy; however, rather than age being the limiting factor (Trethewey, 1999), it was menopause symptoms and structural issues of support that go with it. These findings contribute to our understanding of gendered ageing at work suggesting that women’s inevitable biological process of menopause represents a temporary, but reversible age-related decline in their physical and mental health, which can ultimately lead to impaired work-related outcomes in women at the peak of their careers.
Second, we contribute nuanced effects of the supervisory support and female peer support and show how both are two key resources that women draw from to cope with their menopause symptoms. Our findings are in agreement with Beck et al. (2021) who noted that having support mechanisms at work would help women cope with their menopause symptoms in the workplace and would benefit them in terms of experiencing less severe outcomes. We could argue that by sharing their experience of menopause with other women in their workplace who might be going through the same experience or are perceived to understand the ‘secret world of menopause’ better than their male peers, women feel relief and perceive less stigma. By talking about their menopause experience with their supervisors and female colleagues, women contribute to normalising menopause in the workplace. As such, our findings contribute to the diversity and disclosure theoretical paradigm (Grandey et al., 2020) by showing that it pays off to offer education around the issues of menopause as part of the diversity and inclusion initiatives for women to feel that they have ‘allies’ in their workplaces. Indeed, as Atkinson et al. (2021) posit, having social support at work to manage menopause is key to creating inclusive workplaces in which employees of all ages and genders can work together effectively.
Third, we bring SOC, a well-established life-span development framework, to the gendered ageing at work literature by showing how the use of adaptive behavioural strategies might be instrumental for women to cope with the adverse effects of menopause symptoms at work. Building on Baltes’ (1997: 13) claim that ‘the future is not something we simply enter, the future is something that we help to create’, we found that women’s use of SOC did influence how menopause symptoms affected their world of work. Unlike most previous research that universally assumes how SOC strategies result in positive outcomes (Moghimi et al., 2017), we make a further contribution to this literature by showing how SOC might be maladaptive in certain situations. To the best of our knowledge, the use of SOC strategies to cope with menopause symptoms remains unexplored. We found that the use of SOC was effective for offsetting the negative effects of physical symptoms on job performance. These findings are aligned with Moghimi et al. (2017: 251) who reported that ‘employees who use SOC strategies should perform better on the job because they adapt to high demands and deliberately invest their limited resources in an optimal way to achieve work goals’. In other words, women who focus on goal-seeking behaviours, in line with SOC theory (Baltes and Baltes, 1990; Zacher and Frese, 2011), are better able to harness their personal resources, which helps them manage physical health-related symptoms in a way that their performance does not suffer despite their experience of menopause.
However, our findings also showed that the use of SOC was detrimental for buffering the negative effects of psychological symptoms, such as depressive mood, anxiety or irritability, on performance. These results show how agentic, active behaviours such as prioritising one’s goals, obtaining and refining the resources as well as acquiring new resources to cope with psychological health-related decline owing to menopause are counterproductive and in fact worsen women’s job performance. We could explain these unexpected results with the argument that psychological symptoms are more difficult to manage with agentic behaviours (Kittell et al., 1998), which, ultimately, rather than helping them cope make them feel frustrated and hopeless. We could also argue that actively trying to adjust one’s goals and seek new or refine current resources to cope with symptoms such as anxiety can further exacerbate the feelings of incompetence as they see how the use of SOC strategies does not work to protect their performance. Further, the investment of resources including attention and effort for goal attainment might consume resources through the act itself and thus lead to a depletion of resources and feelings of fatigue, which might further exacerbate the negative effects of psychological symptoms on performance. Indeed, this has been identified as an under-researched avenue in the area of SOC strategy use and employment outcomes (Moghimi et al., 2017).
As the experience of menopause is inevitable for the vast majority of women, our findings on the effectiveness of SOC strategies for women to cope with their work demands and manage their physical health-related menopause symptoms are promising. Our research adds further support to the effectiveness of SOC strategies for successful ageing (Moghimi et al., 2017; Zacher and Frese, 2011); however, future research should explore the usefulness of SOC strategies for dealing with mental health or psychological health-related outcomes.
Practical implications
It is key for women in their mid- to late career stages who are experiencing menopause to carry on working given that some might have experienced earlier career breaks owing to motherhood and other caring responsibilities (Grandey et al., 2020) and therefore will probably be penalised by realising lower salaries and pensions compared with their male counterparts. Ensuring menopausal women feel supported by their supervisors and peers is crucial in achieving fair and inclusive workplaces for women in mid- to late career stages to thrive and feel accomplished (Atkinson et al., 2021; Grandey et al., 2020). Our findings highlight that peer social support and supervisory support can help women cope with their menopause symptoms at work. Coping with menopause symptoms benefits both employers and women themselves through protection of job performance and retention. We suggest that there is an opportunity for both female employees who are either approaching or experiencing menopause and employers who employ women to better understand the menopause.
Our findings support recent work that, for many women, managing menopause symptoms at work appears to involve hiding or minimising their symptoms (Jack et al., 2019). However, we argue that this personal strategy is potentially detrimental to the continued labour force participation of women struggling with menopause symptoms at work. Specifically, our study shows that women themselves would benefit from seeking support through informal workplace support systems or through supervisory support, where possible. In this way, successful ageing at work can be operationalised, potentially protecting job performance and encouraging labour force participation through retention. Our study shows that if formal workplace support structures are not present then women, rather than hiding their symptoms, should create informal support structures, which are likely to help them cope with the practical impact of menopause symptoms on employment outcomes.
Our findings also highlight the unambiguous requirement of a more proactive employer role in helping women cope with menopause at work. It is widely recognised that processes of gendered ageing more broadly and the menopause specifically are poorly understood by personnel managers (Atkinson et al., 2021; Grandey et al., 2020). It is time that the menopause is not only noticed, but actively managed within organisations. Findings from study 1 highlight that women are not likely to ask for help with symptoms owing to perceived punitive actions; however, for many women, there was a desire for the menopause to be recognised as a genuine workplace issue. This would be a useful starting point for employers who as yet do not have a formal menopause policy within their organisations. An education programme for women and personnel managers could be developed to increase the awareness and reduce the taboo nature of menopause (Brewis et al., 2017; Grandey et al., 2020), which could support the introduction of such policies. Also, menopause, while affecting most women in mid- to later life in some way, is very individualised. As such, employers, while creating their menopause policies are warned that a one blanket approach is likely to be insufficient (Steffan, 2021). While studies have shown that individual interventions can alleviate symptoms, such as desk fans, breathable uniforms and exercise programmes (Brewis et al., 2017; Hickey et al., 2017), they ultimately place the onus on the individual to highlight that the woman is ‘menopausal’, which might not be an acceptable approach for all women.
Strengths, limitations and recommendations for future research
Our study highlights the impact of menopause symptoms at work, an under-researched topic affecting labour force participation of a significant population in the labour market, that is, women in mid- to later life. Although research is starting to reveal the impact of menopause, our research adds value to this emerging conversation by revealing the extent to which supervisory and female peer support contribute to improved employment outcomes. However, our results might not be generalisable to all women of menopause age owing to the relatively small samples used in both studies. Both studies were also drawn from a relatively homogenous occupation type and therefore future research should explore how occupational factors, such as occupation type, sex-dominated occupations and industry type could influence the experience of menopause at work. We envisage that a deeper qualitative and quantitative investigation into job and industry type from a larger sample of women would yield insightful results on the importance of working in a male- versus female-dominated environment. This approach should also consider the individual nature of the desire to disclose (or not) menopause symptoms at work. As we saw in study 1, a director working in a male-dominated environment did not want her menopause symptoms to be acknowledged at work, preferring to be viewed as gender-neutral. Future studies could explore why some women prefer the taboo nature of menopause to not be challenged in the workplace.
While Freund and Baltes (2002: 643) view SOC as a ‘co-ordinated ensemble of contextualised processes’ that should be considered together, a potential limitation of study 2 was that we did not analyse SOC strategies separately. Future research would benefit from a more nuanced understanding of how women engage with both individual and combined use of SOC strategies (Zacher and Frese, 2011). For example, combined SOC might be more important when considering overall behaviour adaptation (Freund and Baltes, 2002), while compensation might be more relevant to study how women of menopause age choose to compensate based on physical performative decline (Griffiths et al., 2013).
Another potential direction for future research is to understand how women can develop their coping behaviours around menopause symptoms to improve job performance, and other employment outcomes, such as workplace retention and seeking promotion. For instance, drawing from the conversation of resources theory (Hobfoll, 2010), future research could employ longitudinal designs and explore how different resources help women cope with their menopause symptoms through resource depletion, resource accumulation and resource investment mechanisms. One specific resource that future longitudinal research could explore is resilience as a state rather than trait, which could explain how women both cope and adapt to changing circumstances at work owing to their experience of menopause (Wilson et al., 2021). 3 Also, behaviour adaptation through SOC use can be trained (Zacher et al., 2015), which is important to keep in mind as the use of SOC was found useful for offsetting the negative impact of physical symptoms. Women in our study were shown to demonstrate high personal responsibility when managing their symptoms at work. As such, we suggest that future research should include a longitudinal intervention study whereby a sample of women within a specific organisation or industry are taught targeted and optimal combined use of SOC strategies. In turn, the effectiveness of any such learned strategies can be examined by comparing the effects of menopause on women’s outcomes before and after the intervention.
There has been an increasing awareness of the impact of menopause on working women. We found evidence that menopause symptoms adversely impacted women’s performance and retention, but having access to social support was found to ameliorate the negative effects of menopause on women’s outcomes. We suggest that there is a clear role for the employer to play in offering social support to help them cope with their menopause in the workplace. In so doing, employers could provide more inclusive workplaces for women who would like to, or who need to actively participate in the labour force while experiencing menopause.
Footnotes
Acknowledgements
We would like to thank the participants who were interviewed (study 1) and to those who took the time to respond to our survey. We also thank those women who spread the word to friends and family to engage in our research in the early stages of data collection for study 2, and to those colleagues who took part in the pilot study to help us develop our survey. We would also like to thank the anonymous reviewers for their very helpful and constructive comments, along with the handling editor, Professor Chidiebere Ogbonnaya, all of whom contributed to bringing this article to fruition.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.