
Abstract
Background
Chronic Neck Pain (CNP) among rotary-wing aircrew is thought to stem from night vision goggles (NVG) and counterweight (CW) systems which displace the centre of mass of the head. This investigation aimed to quantify the loads acting on the neck as a function of movement magnitude (MM), helmet conditions, and movement axes in rapid movements.
Methods
Cervical spine kinematics during rapid head repositioning tasks for flexion-extension (FE) and axial rotation (AR) movements were measured from 15 males and 15 females. Participants moved in either a 35° (Near MM) or 70° arc (Far MM), while donning a helmet, helmet with NVG, helmet with NVG and a typical CW, and a CW Liner (CWL). Measured EMG from three muscles bilaterally and used to drive a biomechanical model to quantify the compression and shear acting at the C5-C6 joint.
Results
In AR, the NVGs were associated with the largest compression magnitudes, 252 (24) N. CW conditions decreased the maximum compression to 249 (53) N. For FE, the compression was 340 N for the Far MM trials and 246 N for Near MMs. Changing the helmet configuration only modestly influenced these magnitudes in FE.
Conclusion
Every 30° of MM increased compression by 57 to 105 N. The reduction of the moment of inertia by 16% in the CWL did not reduce reaction forces. Joint loads scaled proportionately with head-supported weight by a factor of 2.05. The magnitudes of loads suggest a cumulative loading pathway for CNP development.
Introduction
The cockpit of a military helicopter represents a potential perfect storm of risk factors for the development of musculoskeletal disorders (MSDs), particularly chronic neck pain (CNP). Pilots and flight engineers are exposed to vibration, frequently adopt awkward postures, and fly for extended periods (Farrell et al., 2020; Forde et al., 2011; Xiao & Farrell, 2016), all while wearing a helmet which dramatically changes the inertial parameters of the head. It is no surprise that reports of chronic neck pain in helicopter personnel are endemic; in the Royal Canadian Air Force (RCAF), for example, up to 75% of helicopter pilots report CNP (Chafé & Farrell, 2016).
Despite these alarming statistics and the development of mathematical models of cervical spines to quantify these issues (Hoek van Dijke et al., 1993; Snijders et al., 1991), only a few investigations have explored the relationship between helmet mass, the moment of inertia, and neck loads (Bandou et al., 2020; Farrell et al., 2018). Night-vision goggles (NVGs) worn by aircrew induce a flexor moment throughout the cervical spine (Harrison et al., 2007; Thuresson et al., 2005). A counterweight (CW) is sometimes placed opposite the NVGs on the helmet to negate the gravitational moment. The premise is that the compression decrease from the reduced muscle activity needed to balance the gravitational moment of the NVGs exceeds the CW’s weight (Harrison et al., 2007). However, both the NVGs and CW increase the moments of inertia about all three axes. Since dynamic head-repositioning tasks are commonplace for aircrew, an increased moment of inertia would increase the muscle demands needed to initiate and terminate these movements.
In addition, the NVGs constrain peripheral vision from 140° to 40° (Brickner, 1989; Isbell & Estrera, 2003). This deficit is compensated for by increasing the cervical spine’s motion magnitude (MM) (Forde et al., 2011). Postures that deviate from neutral are typically associated with greater muscular demands (Peolsson et al., 2014; Straker et al., 2008) and decreased tissue tolerances (Gallagher et al., 2005). These competing factors, none of which are mutually exclusive, have been explored through EMG and inverse dynamics analyses. However, few investigations have aimed to quantify the resulting joint loads with the inclusion of active muscle contributions (Farrell et al., 2020).
The purpose of this investigation was to document the joint loads on the cervical spine during rapid movements in participants donning a helicopter helmet for Griffon CH-146 flight crew, in addition to NVGs and two versions of CW. A standard CW and a counterweight-liner (CWL). The CWL is based on the same design philosophy as the standard CW but is moulded to the helmet’s interior to reduce its moment of inertia. The objective of this study was to quantify the compression and shear acting at C5-C6 for each of these helmet configurations during rapid head repositioning tasks at two discrete levels of MM.
Methods
Participants
Thirty participants (age: 25.5 ± 4 years; height: 174.7 ± 7.0 cm; body mass: 79.5 ± 16.3 kg) were recruited from a healthy university population. Participants were excluded if they had colour blindness or a history of low back, neck, or shoulder pain. They provided informed consent, and the institutional review board approved the experimental protocol.
Helmet Conditions
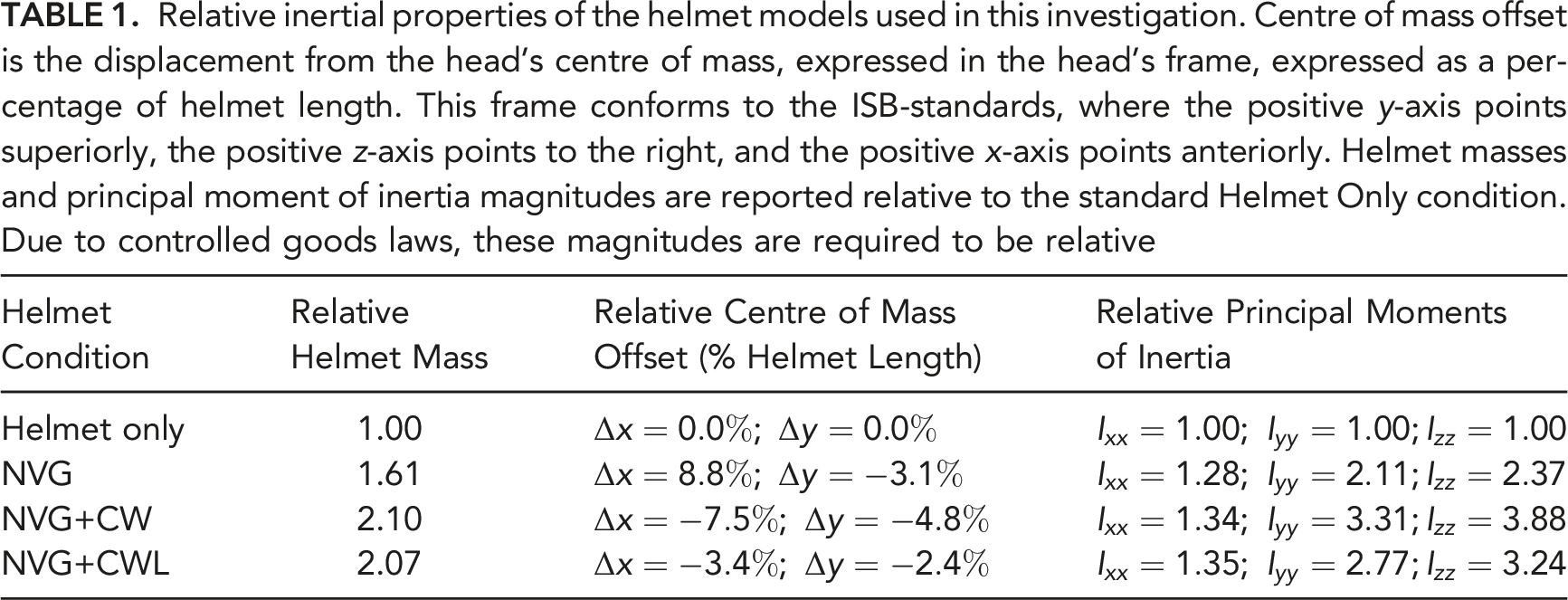
Relative inertial properties of the helmet models used in this investigation. Centre of mass offset is the displacement from the head’s centre of mass, expressed in the head’s frame, expressed as a percentage of helmet length. This frame conforms to the ISB-standards, where the positive y-axis points superiorly, the positive z-axis points to the right, and the positive x-axis points anteriorly. Helmet masses and principal moment of inertia magnitudes are reported relative to the standard Helmet Only condition. Due to controlled goods laws, these magnitudes are required to be relative
Movement Trials
While sitting, participants performed a rapid scanning head-repositioning task on a 3D visual target acquisition system (VTAS) based on Fitts’ Law (Derouin & Fischer, 2019; Fitts, 1954). This task involved a circular array of round solar panels (6V 100 mA, 100 mm diameter, Sundance Solar, Hopkinton NH) behind a 20 mm aperture, with multi-coloured LEDs. A single LED emitted a red signal to the participant to indicate which target they were instructed to acquire. The participant then aligned the image from a laser pointer attached to the helmet just above the NVGs, with the indicated solar panel. Upon contact with the solar panel, the LED would shift from red to blue, then to green after the participant held a 300 ms dwell time. The cycle then repeated with another target presented to the participant.
Targets were paired symmetrically so that the participants were required to either move from left to right and vice-versa in Axial Rotation (AR) or Flexion-Extension (FE). Further, two movement magnitude (MM) conditions were used, consisting of arcs of either 35° (Near) or 70° (Far), based on typical day and night flight movements, respectively (Forde et al., 2011). Each trial consisted of 30 seconds. Participants alternated between two targets under the instruction to “acquire as many targets as possible within 20 seconds,” with an extra five seconds on either side of the data collection. The order of the helmet conditions was block randomized, with each MM or movement axis condition being fully randomized within each helmet block. This yielded a full factorial repeated measures design (Helmet
Kinematics
Trunk and head kinematics were recorded with a passive optoelectric motion capture system, sampled at 80 Hz, using twelve cameras (Vicon, Centennial, CO, USA). Specifically, trunk kinematics were recorded from six reflective motion capture markers over bony landmarks (suprasternal notch, xiphoid process, left and right acromion, and the C7 and T10 spinous processes). A rigid body consisting of three non-collinear markers was also placed over the sternum to allow for landmark reconstruction in the event of marker occlusion (Della Croce et al., 2005). Five passive markers were attached to the helmet to allow for the construction of a frame. Markers were attached to the head over the ears, top of helmet, anterior and posterior helmet. Both the head and trunk local coordinate systems and the Euler Angles between these two frames were defined per International Society of Biomechanics (ISB) standards (Wu et al., 2002). Before the calculation of Euler Angles, gaps in the marker trajectories were interpolated (Nexus 2.0, Centennial, CO, USA), and a 6 Hz low-pass zero-phase second-order (effectively fourth-order with the dual-pass) Butterworth filter was applied to smooth the data (Winter, 2009). A neutral posture was defined by having the participant aim at the centre solar panel in the VTAS array.
Electromyography
Surface EMG (Trigno mini series, Delsys, Natick, MA) were recorded from bipolar electrodes placed over the muscle belly of three muscles bilaterally: the sternocleidomastoid, upper trapezius, and splenius capitis (upper neck extensor). These six channels of EMG were sampled at 2000 Hz using a 16-bit analog to digital converter. A 30 Hz high-pass filter was used to reduce the effects of heart-rate contamination (Drake & Callaghan, 2006) before full-wave rectification and application of a digital 4 Hz low-pass single-pass Butterworth filter (Lu & Bishop, 1996). The impulse response of the single-pass filter induces a delay in the linear envelope representative of the electromechanical delay of the cervical musculature (Almosnino et al., 2009; Milner-Brown et al., 1973; Winter, 1976). The resulting linear envelope signals were normalized to the maximum activation recorded during maximal voluntary exertions (MVEs). During MVE trials, manual resistance was provided against neck flexion, extension, and shoulder elevation at both 45° and 90° of lateral shoulder flexion (Essendrop et al., 2001; Harms-Ringdahl et al., 1986; Murray et al., 2016).
Kinetics
Subject kinematics and EMG were used with an EMG-driven cervical spine model based on a 50th percentile anthropometry to calculate joint loads (Figure 1) (Barrett et al., 2021). Each helmet condition was added to the model with a weld-joint so that the centre-of-mass of the base-helmet was coincident with the centre of mass of the head (inertial parameters in Table 1). The three-dimensional head-trunk Euler Angles from kinematics analysis were partitioned among the intervertebral joints in proportion to their range-of-motion (ROM) (Anderst et al., 2015a; Ordway et al., 1999). Inverse dynamics were used to calculate the net-joint moments acting at each of the 24 degrees-of-freedom (DOF) in the model, the three rotational DOFs in each of the eight gimbal joints representing C0–C1 to C7–T1. Muscle forces were first estimated from surface EMG using a Hill-type approach and then adjusted using an EMG-assisted optimization routine (Cholewicki & McGill, 1994; Gagnon et al., 2011). Muscles that were not driven with EMG were optimized with the classical sum of squared activations (Crowninshield & Brand, 1981). The muscle forces obtained from this step were used to calculate the net joint compression and shear forces acting at the C5–C6 joint level, which was used for statistical analysis. Cervical spine model with a visual representation of the (A) CW condition, (B) Helmet Only condition, and (C) NVG condition. Muscle activation is calculated from EMG, then adjusted based on an EMG-assisted optimization routine. Muscles too deep to collect surface EMG, or otherwise inaccessible, had their muscle activations calculated with the classical sum of squared activations. The CWL liner condition looked similar to (C) since the CWL is not visible from the exterior of the helmet.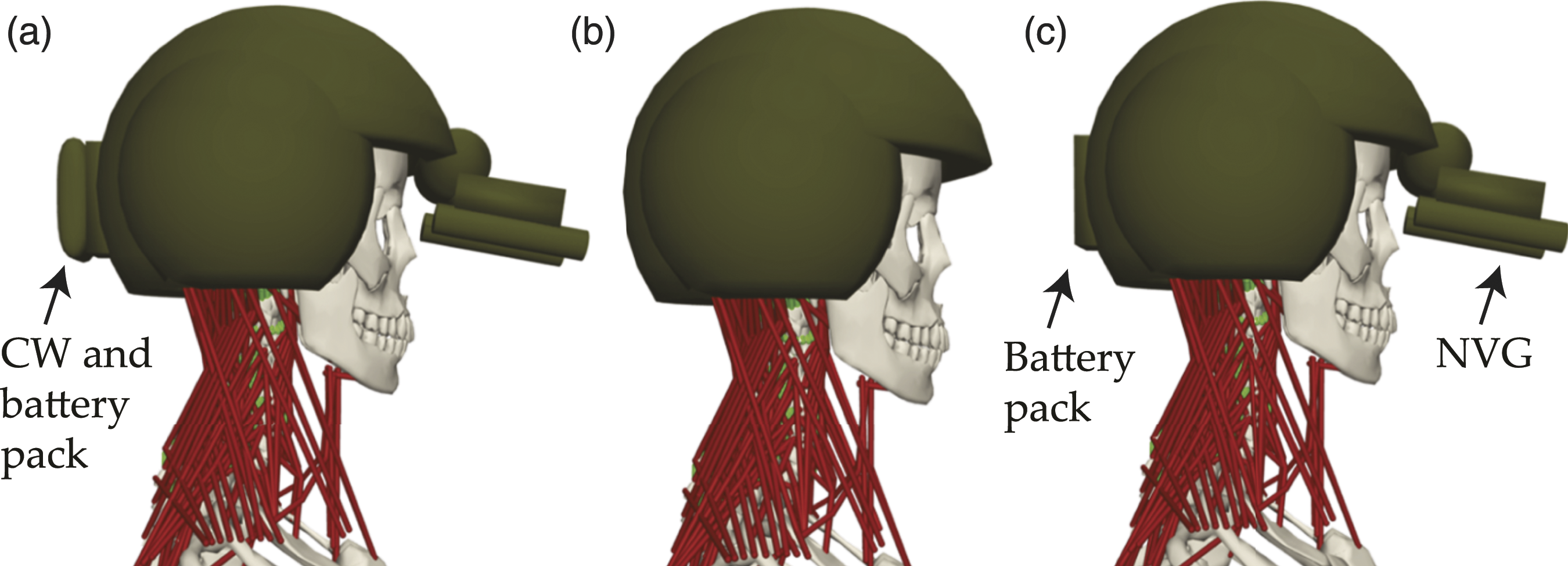
Outcome Measures
The cervical spine model yields time histories of joint reaction moments and forces. Maximum compression (maximum compression) and anteroposterior (AP) shear magnitudes (maximum AP shear) acting at the C5–C6 joint were averaged across all cycles for each of the helmet and MM trials for statistical analysis (Figure 2). In addition, we quantified ensemble average curves for the neck angles, torques at C5–C6, compression and shear across all helmet configurations and MMs, which we have made available as supplemental material. Sample curves from a typical flexion-extension movement trial demonstrating the outcome variables for the analysis. The top panel depicts the total head-trunk flexion angle, with positive angles indicating extension as per ISB convention. The cycles are depicted as shaded regions, with pips indicating the start and end of each cycle. The second panel is the internal flexion moment (positive indicating an extensor moment), which can be seen encountering extrema during the initiation of movement. Finally, the bottom two panels depict the compression and AP shear at C5-C6, respectively, calculated from the joint torques (second panel) using the EMG-driven model. Thus, there is a strong relationship between the joint torque and shear. Positive values of AP shear indicate a posteriorly directed force on the superior vertebra with respect to the inferior one (shown on plot). These maxima were averaged over each of these cycles.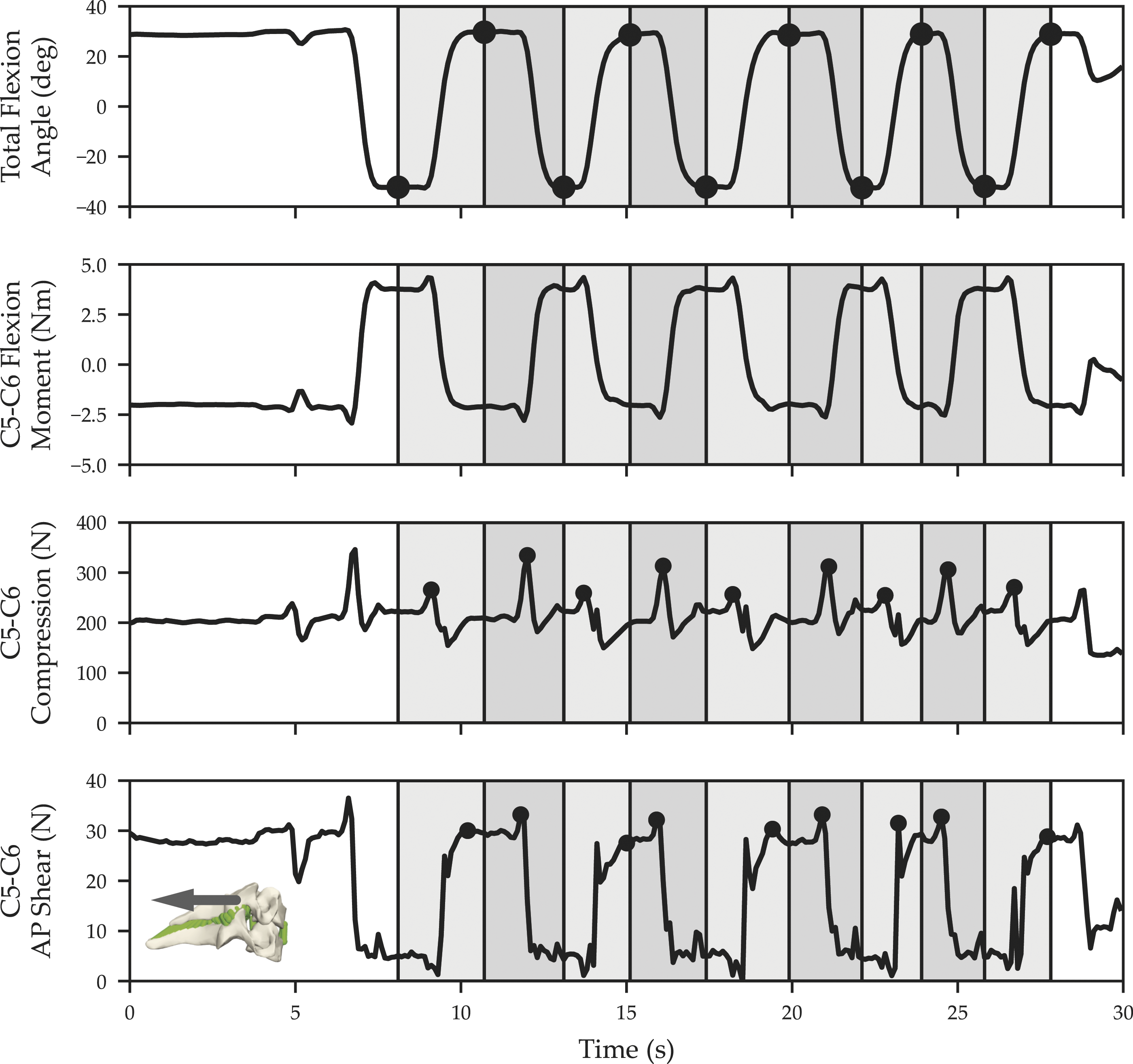
Statistics
A two-way repeated-measures analysis of variance (ANOVA) (MM
Results
Compression
For AR movements, there were significant main effects for both helmet (Figure 3A) and MM (Figure 3B) conditions on the resulting maximum compression, with no interaction effects (p = .41). The increased MM was associated with a significant increase of 59 ± 35 N (mean ± standard deviation) of compression when averaged across all helmet conditions (p < .05), which amounted to an average increase of 31.7%. The NVG condition during the Far MM trials was associated with the most considerable magnitude of compression: 252 ± 24 N, which was a significant 19 ± 39 N increase over the Helmet Only condition (p < .05). Both counterweight conditions decreased the maximum compression to 249 ± 53 N, which was statistically significant compared to the NVG (p < .05). The CW condition was significantly more compression than the Helmet Only condition (p = .020), whereas the CWL condition was not (p = .086). Maximum compression results for both the AR (panels A and B) and FE (panels C and D) trials in this investigation. (A) For AR-trials, there was a main effect of helmet condition for maximum compression. The Helmet Only was generally associated with the smallest compression, which increased when both the CW and NVG were donned. (B) AR trials also had a main effect of range-of-motion, where the Far condition was associated with higher magnitudes of compression. (C) In FE, the maximum compression also exhibited a main effect of helmet condition. Like the AR-trials, the Helmet Only condition was associated with the lowest magnitudes of compression, which increased significantly with NVG, CW+NVG and CWL+NVG. Also, like AR-trials, there was a significant main effect of MM (D) on the maximum compression in FE trials. The null hypothesis was retained if two bars have common letters in their annotation. For example, in (A), the Helmet Only condition was significantly different from the NVG and CW+NVG conditions (no common letters), but not the CWL+NVG condition.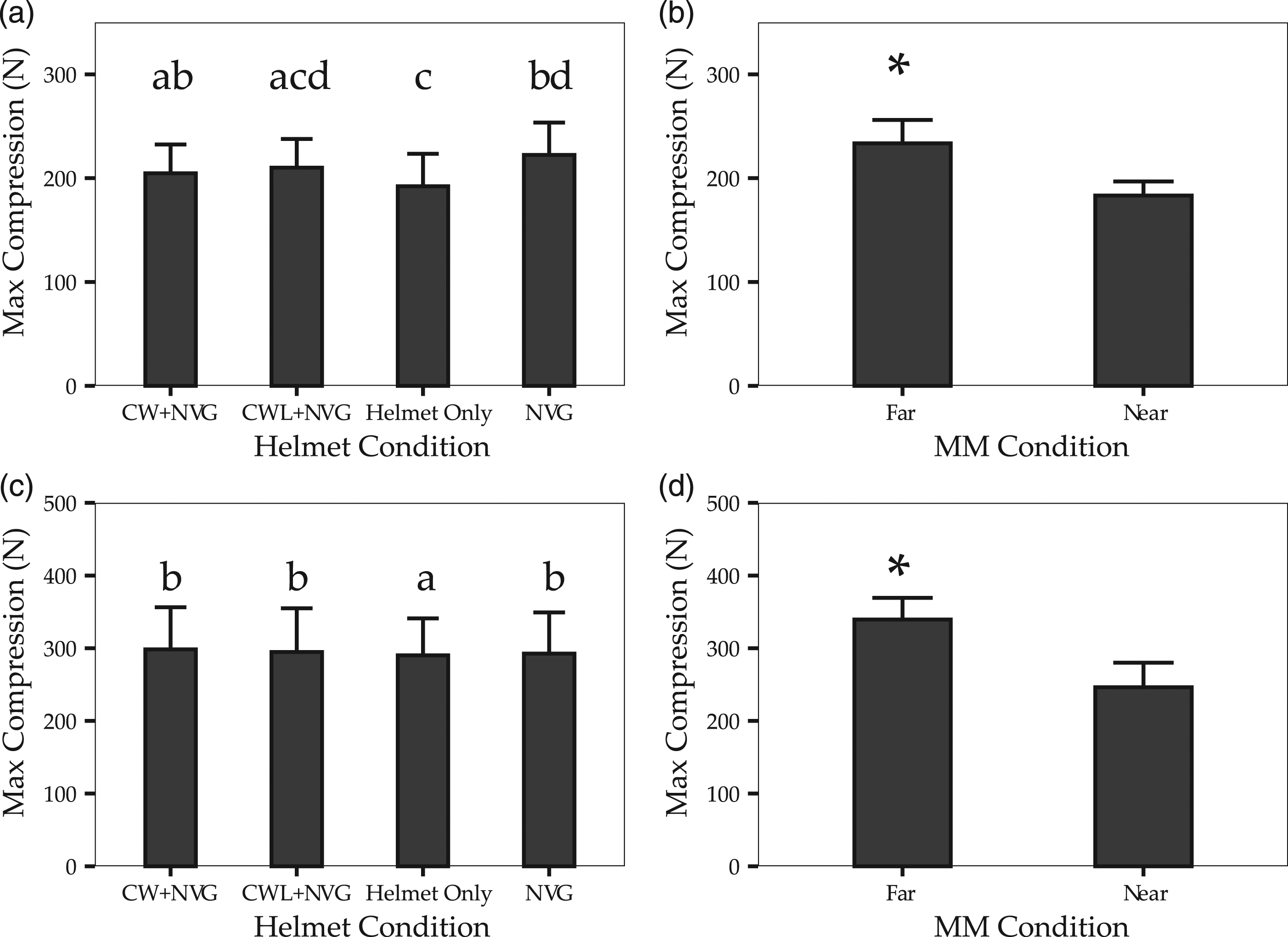
For FE trials, both helmet (Figure 3C) and MM (Figure 3D) conditions also had significant main effects on compression (p < .05) with no interaction (p = .314). In particular, the Far MM trials incurred a significantly increased maximum compression over the Near condition by 94 ± 31 N, representing an average increase of 38.3% (Figure 3D). Donning NVGs, CW, or CWL significantly increased compression by 18 ± 31 N over the standard Helmet Only condition (p < .05). Despite the trend that the change in compression between helmet conditions was more pronounced for the Far-trials than Near trials—9.3% and 2.6% increase, respectively—this result did not achieve statistical significance (p = .314).
Anteroposterior Shear
There were main effects of helmet (Figure 4A) and MM (Figure 4B) on AP shear in the AR trials. Posterior shear of the superior vertebra on the inferior one was significantly greater for all the Far conditions compared to Near (Figure 4B). A constant AP shear of 13 ± 5 N was observed in the near condition. This contrasted with the Far distance trials, which produced twice as much AP shear in the CW, CWL, and Helmet Only condition, on average 24 ± 16 N, with slightly less in the NVG group: 19 ± 8 N (p < .05). The effects of helmet and MM conditions on the resulting anteroposterior shear. (A) There was a main effect of helmet condition on the resulting AP shear for AR-trials, where the Helmet Only and NVG conditions produced the least AP shear, which increased with the addition of the CW or CWL. (B) The main effect of MM on the resulting AP shear for AR-trials, where the Far condition was associated with significantly more shear. (C) Interaction effect between helmet condition and AP shear for the FE-movement trials. For Far trials, the magnitude of AP shear was lowest with either the Helmet Only or NVG conditions and increased with the inclusion of a counterweight system. Conversely, for the Near condition, the magnitude of AP shear for the helmet was more like the counterweights. The null hypothesis was retained if two bars have common letters in their annotation.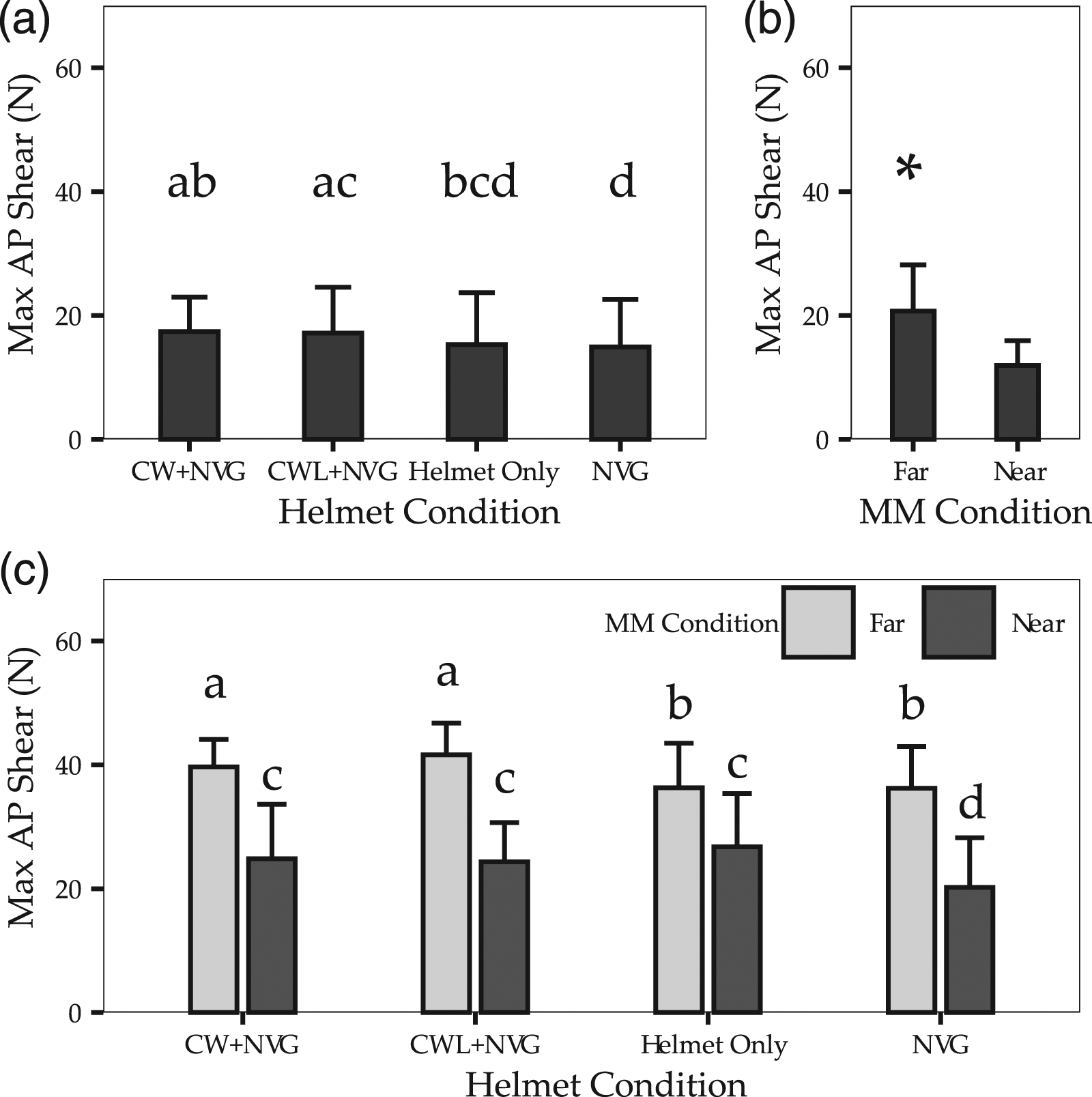
There was a significant interaction between helmet condition and MM on AP shear in the FE trials (Figure 4C). The more extensive range-of-motion trials produced an average of 14 ± 7 N more AP shear than the Near trials. There was also a slight but significant increase in AP shear in both the CW and CWL helmet conditions compared to the Helmet Only or NVG conditions in the Far MM trials. The counterweights were associated with 4.0 ± 6.0 N more AP shear.
Discussion
This study used an EMG-Driven cervical spine model to quantify the compression and shear in the middle cervical spine during rapid head repositioning tasks where participants donned a helmet, NVGs, and CW systems. These results highlight the role of MM while also delineating the impact of head-supported mass and moment of inertia on the resulting loads in the cervical spine. Every 30° of MM corresponded to an increase in maximum compression by 105 N and 57 N for FE and AR trials, respectively. Further, there was a twofold amplification of joint compression with head-supported weight through muscle activity.
Movement magnitude was significant for both the AR and FE movement axes on maximum compression. The increased MM invited larger magnitudes of angular acceleration from participants, which naturally increased the inertial moment generated in these trials. On the other hand, the larger movement amplitude displaced the centre of mass of the head and helmet relative to the C5-C6 joint centre, inducing a more substantial gravitational moment, especially in the FE movement axis. The increase in maximum compression with MM supports the hypothesis that the reduced peripheral vision from NVGs may increase neck joint loads, which in turn may lead to neck troubles (Healey et al., 2021). To this point, other occupations where operators exploit the mobility of the neck also demonstrate a heightened prevalence of chronic neck pain. For instance, mining operators reversing large machinery deep underground often adopt deviated cervical spine postures when checking the blind spots of their vehicles (Godwin et al., 2010; LeClair et al., 2018; Lloyd et al., 1986). Agricultural workers also adopt similar postures as they operate large machinery, with an accompanying increase in reports of chronic neck pain (Rosecrance et al., 2006). These reports, combined with our finding that MM is associated with increased joint loads, suggest that MM may also contribute to a pain generation in these occupations. Tissue models routinely find that more deviated postures are associated with reduced tolerance, both in terms of flexion-extension (Gunning et al., 2001) and axial rotation (Drake et al., 2005; Veres et al., 2010). Of course, our experimental design simulated helicopter pilot exposures who typically don more head-supported mass than these other occupations (LeClair et al., 2018). The combination of increased MM with increased magnitudes of head-supported mass may partially explain why CNP prevalence among helicopter personnel is so high. Overall, every 30° of MM increased the maximum compression by 105 N for FE, and 57 N for AR trials; this suggests that the limited field of view may contribute to the onset of CNP in this population.
The reduced moment of inertia in the counterweight liner condition brought compressive loading closer to the helmet-only condition. Still, it did not produce a statistically significant difference from NVGs or the standard counterweight. The 16% lower axial rotation moment of inertia tended to correspond with a 5.2% reduction in the axial-rotation moment compared to the CW condition. However, this did not translate into any detectable change in the magnitude of compression at C5-C6, implying that the CWL was not superior to the CW for load reduction. In a smaller follow-up analysis, we found that gravitational moments from the head and helmet account for most of the net joint moments, dwarfing those arising from inertia (Supplemental Material). Gravitational moments may partially explain why altering the helmet moment of inertia did not lead to downstream joint load reductions.
For FE trials, donning any additional head-supported mass increased the magnitude of compression by 18 ± 31 N, an average percent increase of only 5.9%. This difference tended to be more pronounced for the Far versus Near MM trials, 9.3% versus 2.6%, respectively; however, the interaction was not significant. This result is consistent with the moment and EMG activities reported by Thuresson et al. (2005). They observed substantial changes in these outcome variables with 20° of flexion, but not between NVG or CW conditions. The type of helmet design displaces the centre of mass of the head-helmet system relative to the C5–C6 joint centre by, at most, 22 mm. The same displacement is achieved by only 15° of flexion or extension, rendering the centre of mass repositioning of the helmet design somewhat inconsequential. The displaced COM is further evidenced by the substantial impact MM had on the resulting compression, increasing it by almost 40% (94 ± 31 N).
Similarly, Bandou et al. (2020) varied the centre of mass location, total helmet mass, and moment of inertia parameters of an experimental helmet in a fractional factorial design. The only two significant predictors in their regression equations for the sternocleidomastoid activity or mean extensor moment was the total mass and moment of inertia. The dramatic effect of MM observed in this experiment also suggests that a change in the flexion-extension posture of an individual can alter the function of the CW system from alleviating the flexor moment induced by the NVG to exacerbating it.
For sagittal plane movements, the moment of inertia about the C5–C6 flexion axis is not solely governed by the moment of inertia magnitudes of the helmet design. By the parallel axis theorem, the added mass of the helmet also contributes to the moment of inertia of the head-helmet system about the C5–C6 joint centre. For the base helmet model in a neutral posture, this added moment of inertia is 0.026 kg m2, roughly equivalent to the moment of inertia of the helmet alone. This added mass and moment of inertia increased the sagittal plane acting about the C5–C6 joint centre, which increased the compression acting at this joint. On average, due to added muscular demands, every 1 N of head-supported weight corresponded to a 2.05 N increase of C5–C6 joint compression: twice what would be expected from the weight of the NVG or CWs alone. This amplification is consistent withHoek van Dijke et al. (1993), whose simulations estimated a factor of 1.4. Overall, this investigation found evidence to support the hypothesis that the magnitude of head-supported mass may be a pivotal contributor to cervical spine loading during FE movements, both in terms of the added gravitational moment in some postures and its contribution to the inertial moment.
Comparison to in Vitro Tissue Tests
One advantage of in vitro biomechanical tests is that loads can be accurately and precisely applied to isolated tissue samples, which can then be closely examined for resulting damage or injury. This quality is unlike experimental studies with in vivo human volunteers, which can only estimate the loads borne by structures in the spine. Following this, in vitro tests apply loads to osteoligamentous functional spinal units (FSUs), consisting of two vertebrae and their intervening passive structures. A core observation in these studies is the presence of the neutral zone: a region on a moment-angle curve where a small applied moment elicits a large change in angle (Panjabi, 1992). Here, we compare our results to applicable in vitro data.
Few studies have explored complex loading of cervical FSUs under combined axial rotation and compression loads, as was found here. Drake et al. (2008) and Marshall and McGill (2010) demonstrated that axial rotation torque at moderate magnitudes accelerated the onset of disc herniation in isolated porcine cervical FSUs. McKinnon and Callaghan (2020) found that cervical FSUs exposed to compressive force (15% of ultimate compressive tolerance) combined with repetitive axial rotation could experience bony failure in the facet joints at magnitudes exceeding 22.7% of their total ROM. For comparison, the estimated entire ROM of the C5–C6 FSU on in vivo human volunteers is approximately 9.3 ± 1.4° (4.7 ± 0.7° on either side) (Anderst et al., 2015b). The model’s estimated maximum C5–C6 axial rotation angle (2.3°) is 48.6% of the total ROM, more than the 22.7% threshold hypothesized by McKinnon and Callaghan (2020). Notably, the laminar structure of the annulus fibrosis is not well suited for combined axial rotation and compressive loading. Only half of the annular layers are tensioned in axial rotation, which can contribute to the delamination of the annulus. These delaminated layers are hypothesized to facilitate the migration of nuclear tissue to the edge of the disc (Tampier et al., 2007). It is unclear if the load magnitudes observed here, typically around 7% of the failure tolerance of cervical FSUs in a neutral posture, when combined with the magnitudes of axial rotation, form the basis for annular damage.
The combination of flexion-extension postures with modest compression observed here may implicate a disc herniation mechanism. The maximum compressive forces (∼350 N) were around 10% of the ultimate compressive tolerance of the C5–C6 FSU (∼3.9 kN) (Pintar et al., 1998; Shea et al., 1991). Because of the well-documented decrease in the ultimate compressive tolerance of isolated FSUs with flexion (Gallagher et al., 2005; Gunning et al., 2001; Shea et al., 1991), it is essential to consider that this load is experienced when the joint is in a deviated posture. Specifically, maximum C5-C6 compression occurred at 2.2° of flexion or 1.4° of extension, depending on whether the cycle began in flexion and moved to extension or vice-versa. Using a porcine in vitro model, Parkinson and Callaghan (2009) demonstrated that repetitive flexion-extension cycles at loads lower than 30% of the predicted ultimate compressive tolerance can damage or injure the intervertebral disc. This result is in concordance with earlier work by Callaghan and McGill (2001), who observed that modest compressive loads could result in disc herniation provided enough flexion-extension cycles are endured.
Furthermore, in the FE trials, the maximum compression and the range of motion during the Far MM condition may implicate annular micro-damage. Gooyers et al. (2015) found little macroscopic evidence for injury (e.g. fracture or avulsion) in porcine cervical FSUs cyclically loaded at 10% of their estimated ultimate compressive tolerance, moving through their neutral-zone range for 5000 cycles. However, they observed histological evidence of micro-injury to the deep layers of the posterior-lateral annulus fibrosis, which worsened with the number of cycles applied per minute. Coincidentally, the maximum compression in this investigation occurs when the FSU is at 100% or 62% of the flexion or extension neutral zone lengths (defined using Thompson et al. (2003)), respectively, remarkably similar to that experimental condition. This result comes with the caveat that only the superficial layers of the annulus fibrosis tend to possess nociceptive sensory neurons (Bogduk et al., 1988). In light of these in vitro studies, we propose it is plausible that large movement magnitudes, coupled with increased head-supported mass, may implicate the intervertebral disc in a potential pain-generating pathway. Of course, we acknowledge that the porcine cervical spine models used in these investigations are more anatomically similar to the human lumbar spine (Oxland et al., 1991; Yingling et al., 1999). Unfortunately, there is no comparable data on either human cervical FSUs or another similar animal model to date.
Maximum AP shear magnitudes observed in this investigation were low relative to the ultimate shear tolerance of cervical spine FSUs, approximately 500 N (Pintar et al., 1998; Shea et al., 1991). The most substantial magnitudes of AP shear amounted to 41 N, below 10% of the expected tolerance of the C5-C6 FSU. Currently, there is no cyclic shear fatigue data published for the human middle cervical spine, especially at this low force magnitude. For instance, van Dieën et al. (2006) found that cyclic loads that varied between 20% and 80% of the estimated ultimate shear tolerance of isolated porcine lumbar specimens resulted in shear loading fatigue failure in 7 of 20 samples after 1500 cycles. Howarth and Callaghan (2013) conducted a more robust investigation into the cumulative shear fatigue properties of porcine cervical FSUs. Their reported weighting functions suggest that loads below 35.6% of the ultimate estimated shear tolerance of porcine FSUs do not result in substantive failures. Both investigations explored load magnitudes larger than what was estimated in the present study. Both observed bony failures in their FSUs that would be apparent on a sagittal plane radiograph of a CNP patient. Once again, it is worth noting that both investigations were attempting to simulate a lumbar exposure, in the latter case due to the anatomical similarities between the porcine cervical and human lumbar vertebrae (Yingling et al., 1999). A critical anatomical difference between the two species is the angles of the facet joint surfaces in the sagittal plane. This angle is approximately 45° to the transverse plane for human cervical vertebrae and 82° in the porcine model, which is more similar to the almost 90° in human lumbar vertebrae (Yingling et al., 1999). As the facet joints limit shear translations, this anatomical difference cannot be overlooked. While this result in isolation does not rule out a potential chronic soft-tissue injury from posterior shear-loading, it does suggest that the proper pain-generating pathway may culminate by other means.
Limitations
While this study presents results consistent with other reports (Bandou et al., 2020; Forde et al., 2011; Hoek van Dijke et al., 1993; Thuresson et al., 2005), there are still some limitations that need to be addressed. Arguably one of the most significant risk factors for CNP, vibration, was overlooked in this investigation (Ariëns et al., 2000; Charles et al., 2018). Intervertebral discs exposed to vibration show evidence of earlier injury initiation (Gregory and Callaghan, 2011, 2012), and their mechanical behaviour also interacts with the adopted posture (Barrett et al., 2016; Gooyers et al., 2012). At the same time, human volunteers exposed to vibration show marked changes in co-contraction (Thuresson et al., 2005), which would likely increase the compression acting on the neck. A second major limitation is that the musculoskeletal geometry used in this study was a 50th percentile adult human male. In contrast, the study data came from participants with various anthropometries. Scaling the model geometry would also require a valid scaling method for the passive tissue parameters, which we aim to explore in future investigations.
Using the same model to calculate all participant kinematics and kinetics would have likely decreased the variability in the calculated moments. However, the variability in predicted compression was considerable, stemming from the muscle activation strategies unique to each participant. Another avenue for future investigation may be to include lateral bending movements, as flight crew adopt these postures about as regularly as severely flexed or extended ones (Forde et al., 2011). For the current investigation, we focused on FE and AR movements.
There are also some limitations with the external validity of the VTAS task used in this investigation. While this was designed to mimic a scanning task aircrew commonly perform on missions, it is not a pure recreation of the cockpit environment. For one, it does not simulate exposures where those individuals are glancing around the cockpit with uncorrected vision, usually with NVGs in place. Secondly, there is likely an upper limit to the magnitude of extension permissible in the cockpit. MMs in this axis would probably not be distributed symmetrically around a neutral posture. Finally, participants may not have been true representatives of the aircrew population, as they were not excluded based on height or visual acuity. Nevertheless, the VTAS system represents a standardized task with a tightly controlled index of difficulty. The specific results regarding MM, head-supported mass, or moment of inertia, likely translate to real-world applications.
Finally, the CWL condition that was tested in this investigation is a theoretical construct not currently available for real-world deployment. This experimental condition tried to isolate the effects of changing the moment of inertia on joint kinetics. Overall, moving the counterweight closer to the head and reducing the moment of inertia did not reduce cervical joint loads.
Conclusion
The major findings in this investigation are fourfold. Firstly, for head-supported mass conditions, every 30° of MM resulted in increased compression by, on average, 105 N for FE and 57 N for AR movements. This result is taken as evidence supporting the hypothesis limited peripheral vision when wearing NVGs is one of several factors that may lead to CNP. Secondly, engineering reduction in the axial-twist moment of inertia by 16% does not generally translate into reduced compression. Thirdly, every 1 N of head-supported weight corresponded to a 2.05 N increase of C5-C6 joint compression, indicating that the magnitude of head-supported mass might not exchange favourably with the moment reduction from a counterweight. And finally, the low magnitudes of compression and shear—both approximately 10% of the estimated failure tolerance of isolated FSUs—combined with the effects of posture during rapid head repositioning tasks appear to implicate a soft tissue cumulative loading pathway.
Key Points
Every 30° of ROM utilized resulted in increased compression by, on average, 105 N for flexion-extension and 57 N for axial-rotation movements. The reduction of the axial-twist moment of inertia by 16% in the CWL did not translate into reduced compression. Increase in joint loads scaled proportionately with the magnitude of head-supported weight, with an amplification factor of 2.05. The low magnitudes of compression and shear—both approximately 10% of the estimated failure tolerance of isolated cervical functional spinal units—combined with the effects of posture during rapid head reposition tasks appeared to implicate a cumulative loading pathway for the development of CNP.
Supplemental Material
Supplemental Material - Cervical Spine Motion Requirements From Night Vision Goggles May Play a Greater Role in Chronic Neck Pain than Helmet Mass Properties
Supplemental Material for Cervical Spine Motion Requirements From Night Vision Goggles May Play a Greater Role in Chronic Neck Pain than Helmet Mass Properties by Jeff M. Barrett, Laura A. Healey, Steven L. Fischer and Jack P. Callaghan in Human Factors
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JPC is the Tier I Canada Research Chair in Spine Biomechanics and Injury Prevention. JMB was supported by a Natural Sciences and Engineering Council of Canada (NSERC) Post-Graduate Scholarship (PGS-D). We would like to thank Gentex for their graceful provision of the helmet systems used in this investigation; and Thumbprint Solutions (Stouffville, Ontario) for their contributions to calculating the inertial parameters of the helmet as well as Defense Research and Development Canada (DRDC) for their assistance.
Supplementary Material
The online supplemental material is available with the manuscript on the HF Web site.
Author Biographies
Jeff M. Barrett is a Ph.D. student in Kinesiology and Health Sciences at the University of Waterloo, where he completed a master’s degree in 2016 in Kinesiology.
Laura A. Healey completed her master’s degree in Kinesiology at the University of Waterloo in 2019. She is currently a Manager in Footwear innovations at PUMA.
Steven L. Fischer is an Associate Professor member in the Department of Kinesiology and Health Sciences at the University of Waterloo, where he completed his Ph.D. in Kinesiology in 2011.
Jack P. Callaghan is a Professor in the Department of Kinesiology and Health Sciences at the University of Waterloo. He completed his Ph.D. in Kinesiology from the University of Waterloo in 1999, specializing in low magnitude loading of the spine.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.