
Abstract
Objective
This study investigates how team cognition occurs in care transitions from operating room (OR) to intensive care unit (ICU). We then seek to understand how the sociotechnical system and team cognition are related.
Background
Effective handoffs are critical to ensuring patient safety and have been the subject of many improvement efforts. However, the types of team-level cognitive processing during handoffs have not been explored, nor is it clear how the sociotechnical system shapes team cognition.
Method
We conducted this study in an academic, Level 1 trauma center in the Midwestern United States. Twenty-eight physicians (surgery, anesthesia, pediatric critical care) and nurses (OR, ICU) participated in semi-structured interviews. We performed qualitative content analysis and epistemic network analysis to understand the relationships between system factors, team cognition in handoffs and outcomes.
Results
Participants described three team cognition functions in handoffs—(1) information exchange, (2) assessment, and (3) planning and decision making; information exchange was mentioned most. Work system factors influenced team cognition. Inter-professional handoffs facilitated information exchange but included large teams with diverse backgrounds communicating, which can be inefficient. Intra-professional handoffs decreased team size and role diversity, which may simplify communication but increase information loss. Participants in inter-professional handoffs reflected on outcomes significantly more in relation to system factors and team cognition (p < 0.001), while participants in intra-professional handoffs discussed handoffs as a task.
Conclusion
Handoffs include team cognition, which was influenced by work system design. Opportunities for handoff improvement include a flexibly standardized process and supportive tools/technologies. We recommend incorporating perspectives of the patient and family in future work.
Keywords
Handoff Communication Activities
We previously compared care transitions from the operating room (OR) to pediatric intensive care unit (PICU) or adult intensive care unit (ICU) (Wooldridge et al., 2022). We focused on pediatric and adult trauma patients because they are critical and unstable with complex care processes (Wooldridge, Carayon, Hoonakker, et al., 2019); trauma is also the leading cause of death in children and adults between 0 and 44years old (Stewart et al., 2003). We found care transitions include crucial work outside of handoff. The OR to ICU transition involved handoffs separated by profession (i.e., intra-professional handoff), where the OR to PICU transition included a handoff between the whole team (i.e., inter-professional handoff). Both types of handoffs are communication activities undertaken by two or more individuals interdependently, dynamically and adaptively, who share the goal of a safe transition—a team (Salas et al., 1992).
Team Cognition
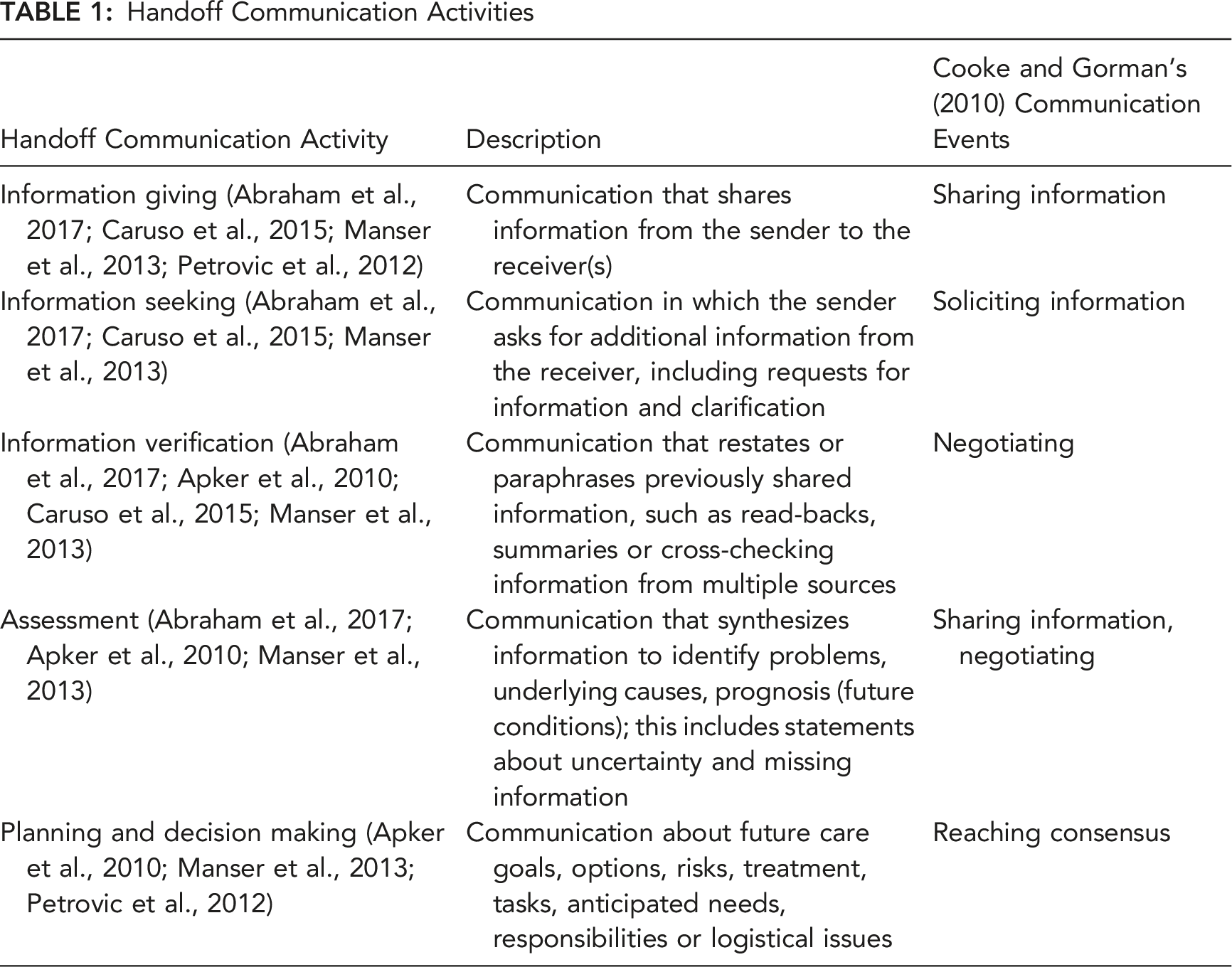
Improved team cognition results in more effective team performance (Cooke et al., 2013; DeChurch & Mesmer-Magnus, 2010). Two perspectives on team cognition have emerged: (1) shared team cognition and (2) interactive team cognition (ITC) (Cooke et al., 2013). The shared cognition perspective is heavily influenced by the information processing model of individual cognition (Parasuraman et al., 2000); team cognition is viewed as the aggregation of individual cognition. Cooke et al. (2013) described ITC as the explicit, observable communication and coordination interactions between team members, drawing on work by Hutchins (1995a, 1995b). Cooke and Gorman (2010) identify four types of communication events (i.e., team cognition functions) that are ITC: 1. Sharing information: team members share information with others. 2. Soliciting information: team members request information from others. 3. Negotiating: team members discuss information together. 4. Reaching consensus: team members decide next steps or agree.
In Table 1, we propose linkages between communication activities from handoff research and Cooke and Gorman’s (2010) team cognition functions.
Team cognition is tied to context. Many studies of ITC are conducted in simulated settings (Cooke, 2015; Cooke et al., 2007; Cooke & Gorman, 2009; Gorman et al., 2020), and, therefore, do not allow for the exploration of the impact of context on team cognition. Salas et al. (2008) called for the study of team cognition in natural settings, as team cognition is shaped by the sociotechnical system in which the team works, i.e., the context. We have yet to understand how the sociotechnical system impacts team cognition, which will help to design sociotechnical systems to support teams.
Sociotechnical Systems
Sociotechnical system theory focuses on the need to consider technical and social subsystems within a work environment and organization to jointly optimize performance (Clegg, 2000; Emery & Trist, 1965; Kleiner, 2008; Pasmore, 1988; Waterson et al., 2002). Carayon and Smith developed the work system model (Carayon, 2009; Smith & Carayon, 2001; Smith & Carayon-Sainfort, 1989) to describe and study sociotechnical systems; work system elements are the individuals, tasks, environment, tools and technologies, and organization. We must consider interactions between elements, which shape adaptive behavior and dynamic outcomes (Pew & Mavor, 2007). The work system model is integrated in the Systems Engineering Initiative for Patient Safety (SEIPS) 3.0 model, used to analyze, model and improve both patient and worker outcomes (Carayon et al., 2006, 2014, 2020). The SEIPS model includes feedback loops to support work system changes that may come about via local adaptations in real time and changes arising from a formal design process, both described by Hutchins (1991). Figure 1 shows an adaptation of SEIPS 3.0 as a system-process-outcome (S-P-O) framework to describe how the work system (system), team cognition functions (process), and outcomes are related in handoffs. System-process-outcome framework to describe handoffs based on SEIPS 3.0 (Carayon et al., 2006, 2014, 2020).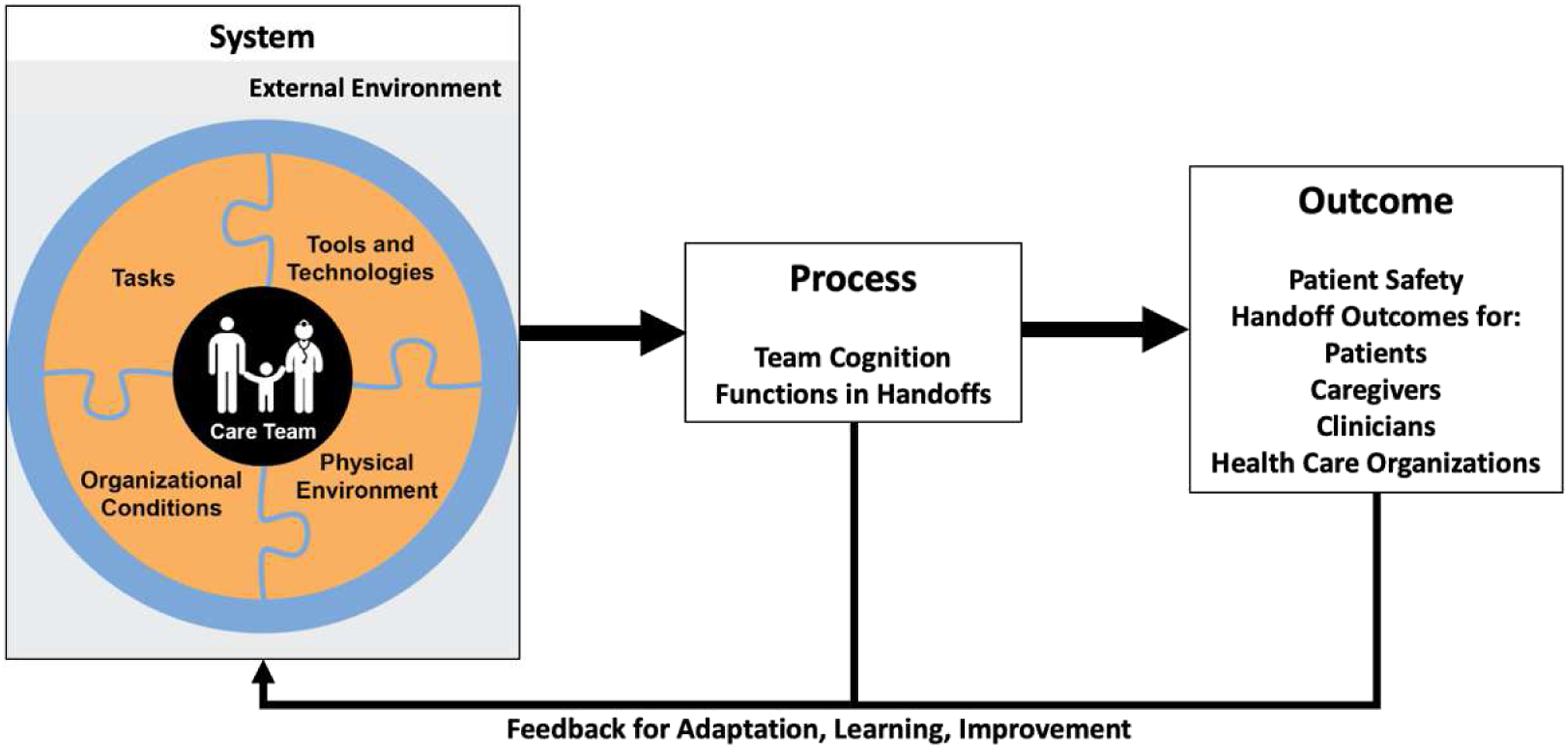
An important implication of ITC is that interactions between team members must occur for the team cognition to take place. The design of work systems likely influences these interactions, for example, increasing or limiting frequency or quality. Implementing inter-professional (i.e., team) handoffs might encourage interactions, improving team cognition and care transition outcomes. Studies of inter-professional handoffs comparing handoff quality before and after implementation of team handoffs find decreased information loss (Agarwal et al., 2012; Catchpole et al., 2007; Joy et al., 2011; Petrovic et al., 2012), improved clinical outcomes (Agarwal et al., 2012), error reduction (Catchpole et al., 2007; Joy et al., 2011) and improved clinician satisfaction (Petrovic et al., 2012). But these studies do not investigate how or why inter-professional handoffs result in improved outcomes versus intra-professional handoffs.
Study Objective
The goal of this study is to investigate team cognition in care transitions. We first determine the type(s) of team-level cognitive processing that occurs during handoffs. We then demonstrate how changes in work system design—inter-professional versus intra-professional handoffs—lead to perceived differences in team cognition; this allows us to gain insight into how the sociotechnical system and team cognition are related.
Methods
This study is part of a larger project to develop design requirements for health information technology (IT) for teamwork and care transitions in pediatric trauma care (http://cqpi.wisc.edu/teamwork-and-care-transitions-in-pediatric-trauma/). This research complied with the American Psychological Association Code of Ethics and was approved by the IRB at the University of Wisconsin-Madison and the IRB at the University of Illinois at Urbana-Champaign. Informed consent was obtained from each participant.
Setting and Sample
The participating health system with multiple hospitals is a level 1 trauma center for both pediatric and adult patients. The pediatric hospital has 111 beds, eight pediatric operating rooms, and a 21-bed PICU; the adult hospital has 505 beds, 27 operating rooms and multiple ICUs. This study focuses on the Trauma and Life Support Center (TLC), i.e., an ICU with 24 beds. In the PICU, pediatric intensivists and surgeons are involved in patient care; in the ICU, a critical care team, led by surgeons or critical care anesthesiologists, and surgeons are involved in patient care.
Participating Sample (N = 28)
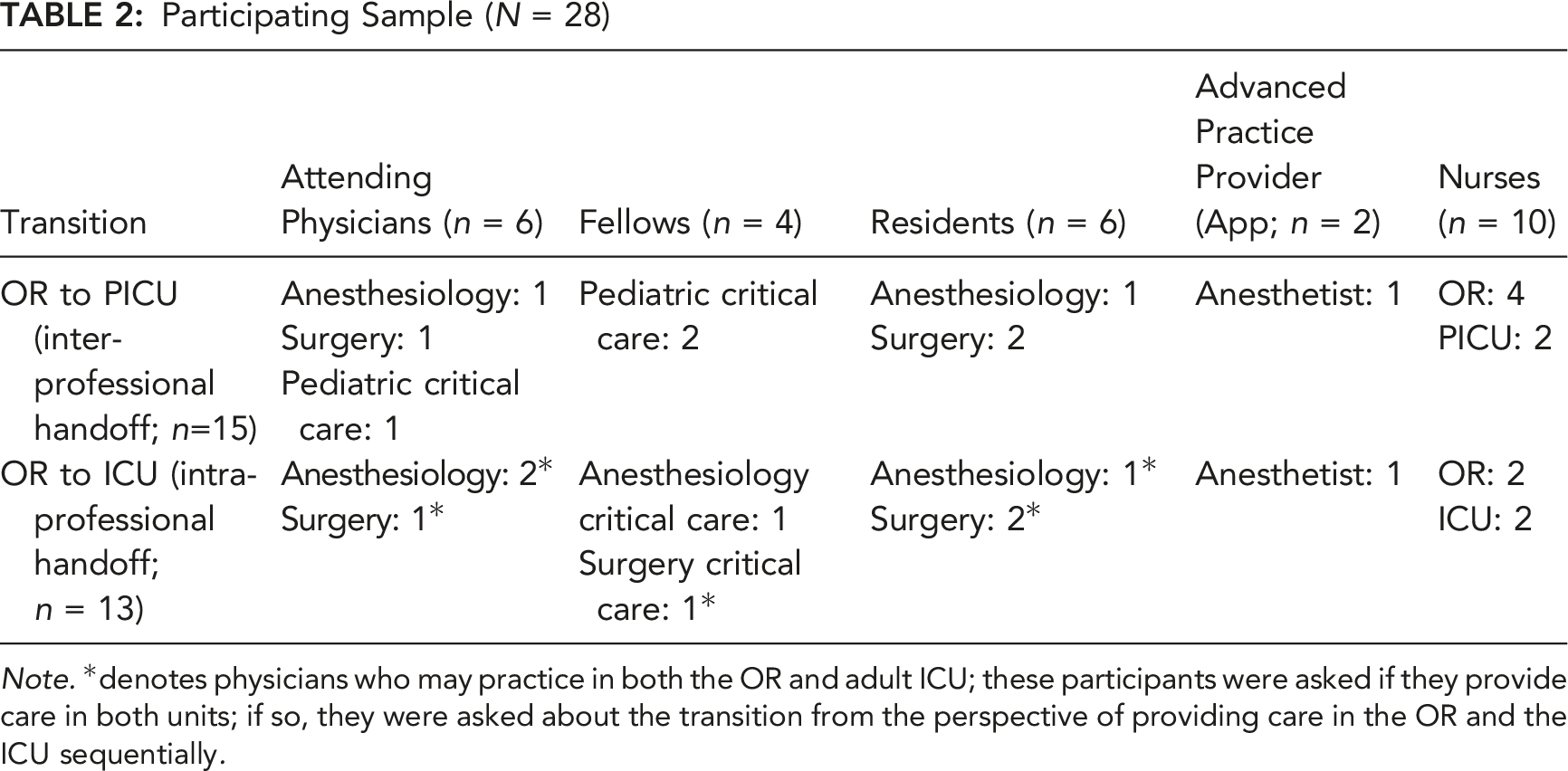
Note. *denotes physicians who may practice in both the OR and adult ICU; these participants were asked if they provide care in both units; if so, they were asked about the transition from the perspective of providing care in the OR and the ICU sequentially.
Data Collection
We conducted in person, semi-structured interviews to allow probing for detailed answers (Robson & McCartan, 2016). Each interview was conducted by one or two HFE researchers. The interview guide is available at: http://cqpi.wisc.edu/teamwork-and-care-transitions-in-pediatric-trauma/. We elicited detailed descriptions of the care transition process, i.e., all work system elements, examples of good care transitions (when care was not compromised and went well) and bad care transitions (when care was compromised and did not go well). Nearly 22 hours of interviews were conducted (average: 46 minutes, range: 24–65 minutes; N = 28 with two participants in one interview). All interviews were recorded and transcribed by a professional transcription service. After the first four interviews were conducted, we iterated between data collection and analysis, monitoring for saturation.
Data Analysis
Before analysis, all identifying information were removed from the transcripts. We conducted a qualitative content analysis (Graneheim & Lundman, 2004) of the interview transcripts and performed Epistemic Network Analysis (ENA) (Shaffer, 2017; Shaffer et al., 2016; Shaffer et al., 2009; Shaffer & Ruis, 2017; Wooldridge, Carayon, Shaffer, & Eagan, 2018) to understand the relationships in the inter- and intra-professional handoff groups.
Qualitative content analysis
Interactive Team Cognition Functions in Handoffs
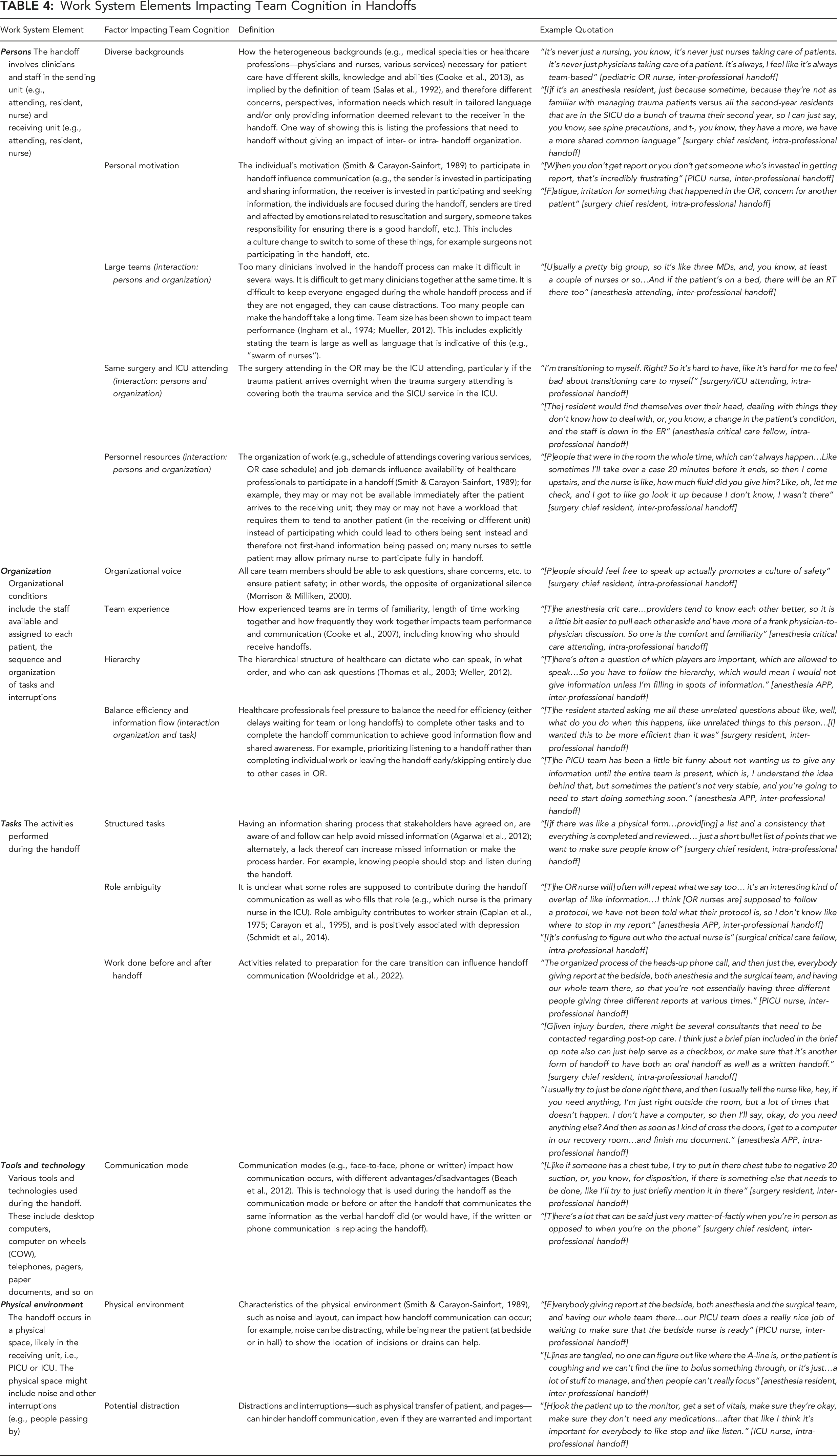
Work System Elements Impacting Team Cognition in Handoffs
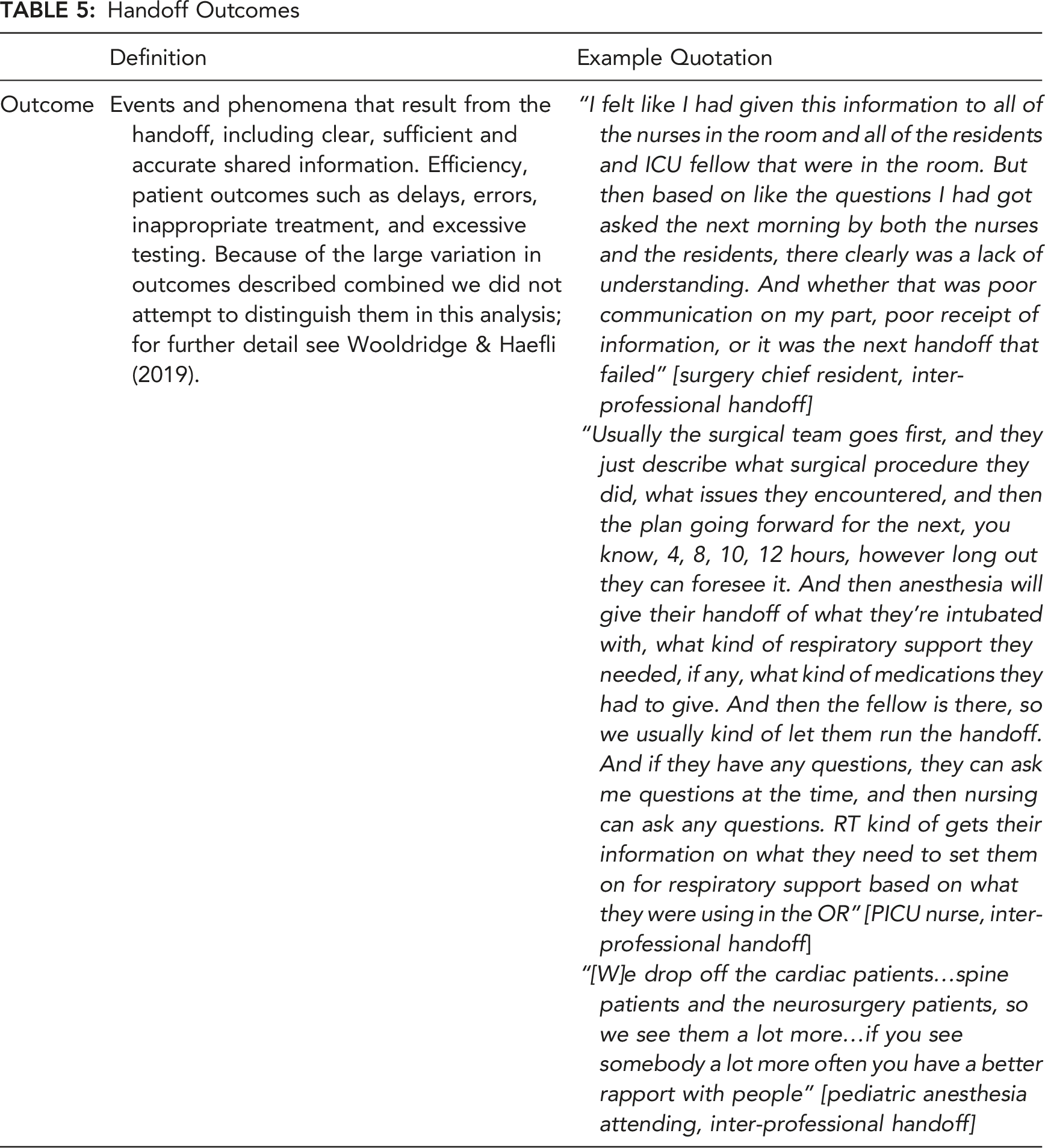
Handoff Outcomes
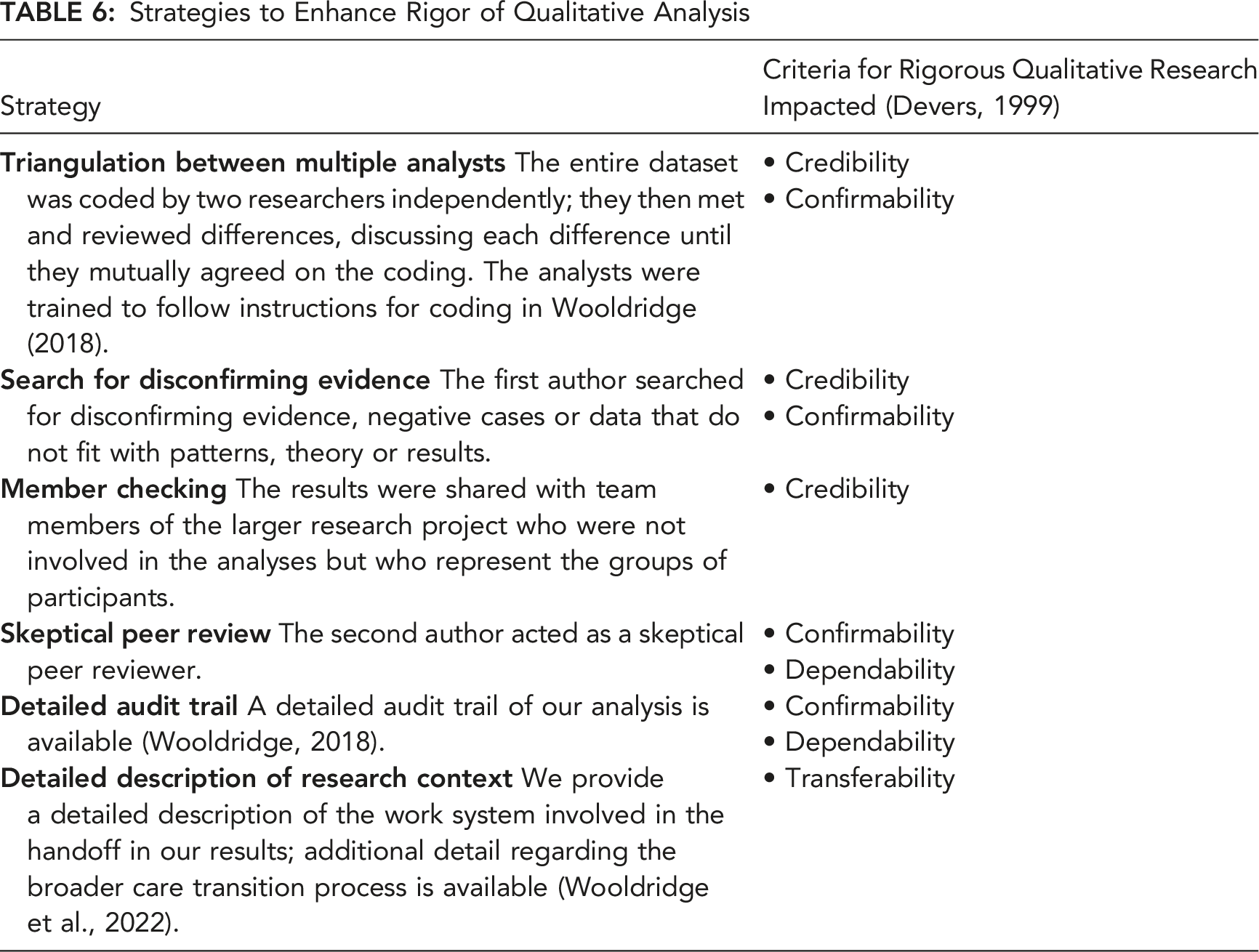
Strategies to Enhance Rigor of Qualitative Analysis
Epistemic network analysis
The underlying goal of ENA is to develop deep understandings of relationships between codes (Wooldridge, Carayon, Shaffer, & Eagan, 2018). ENA begins with high-quality qualitative data segmented according to principles of discourse analysis. We segmented our interview data by hand based on the interview guide, i.e., each numbered question on the interview guide, the response and subsequent probing questions and responses. We then uploaded the segmented data and codes to the ENA 1.7.0 Web Tool (Marquart et al., 2018). ENA uses code co-occurrence to infer relationships: ENA develops adjacency matrices of co-occurring codes, which are summed and plotted in a high-dimensional space. The vectors are normalized, and dimensions are reduced with single value decomposition, like a principal components analysis. The resulting networks are projected on a two-dimensional plot, where the x-axis accounts for the highest percentage of variance explained by a dimension and the y-axis is an orthogonal dimension that accounts for the next highest percentage of variance (Shaffer, 2017; Shaffer et al., 2009, 2016; Shaffer & Ruis, 2017).
We developed ENA models to compare networks of clinicians involved in inter-professional (OR to PICU) and intra-professional (OR to ICU) handoffs. Each line formed a complete stanza, and thus the relationships depicted in the resulting network graphs show connections between the codes applied to one segment. Our model had co-registration correlations of 0.98 (Pearson) and 0.98 (Spearman) for the first dimension and co-registration correlations of 0.99 (Pearson) and 0.99 (Spearman) for the second, indicating strong goodness of fit. We compared the average network graphs of the inter- and intra-professional handoffs, that is, clinicians participating in the OR to PICU and OR to ICU handoffs, respectively, and examined differences using the network graph of the difference (i.e., subtracted network). We also calculated the centroid of the average networks and 95% confidence interval of mean centroid locations. We conducted Mann–Whitney U tests on the location of the centroids of the inter- and intra-professional networks to quantify differences between the networks.
Results
The 28 interviews with clinicians who participate in care transitions of pediatric and adult trauma patients from the OR to PICU and ICU resulted in 201 quotations describing handoff communication; 188 quotations included work system elements, while 90 included outcomes.
Qualitative Content Analysis
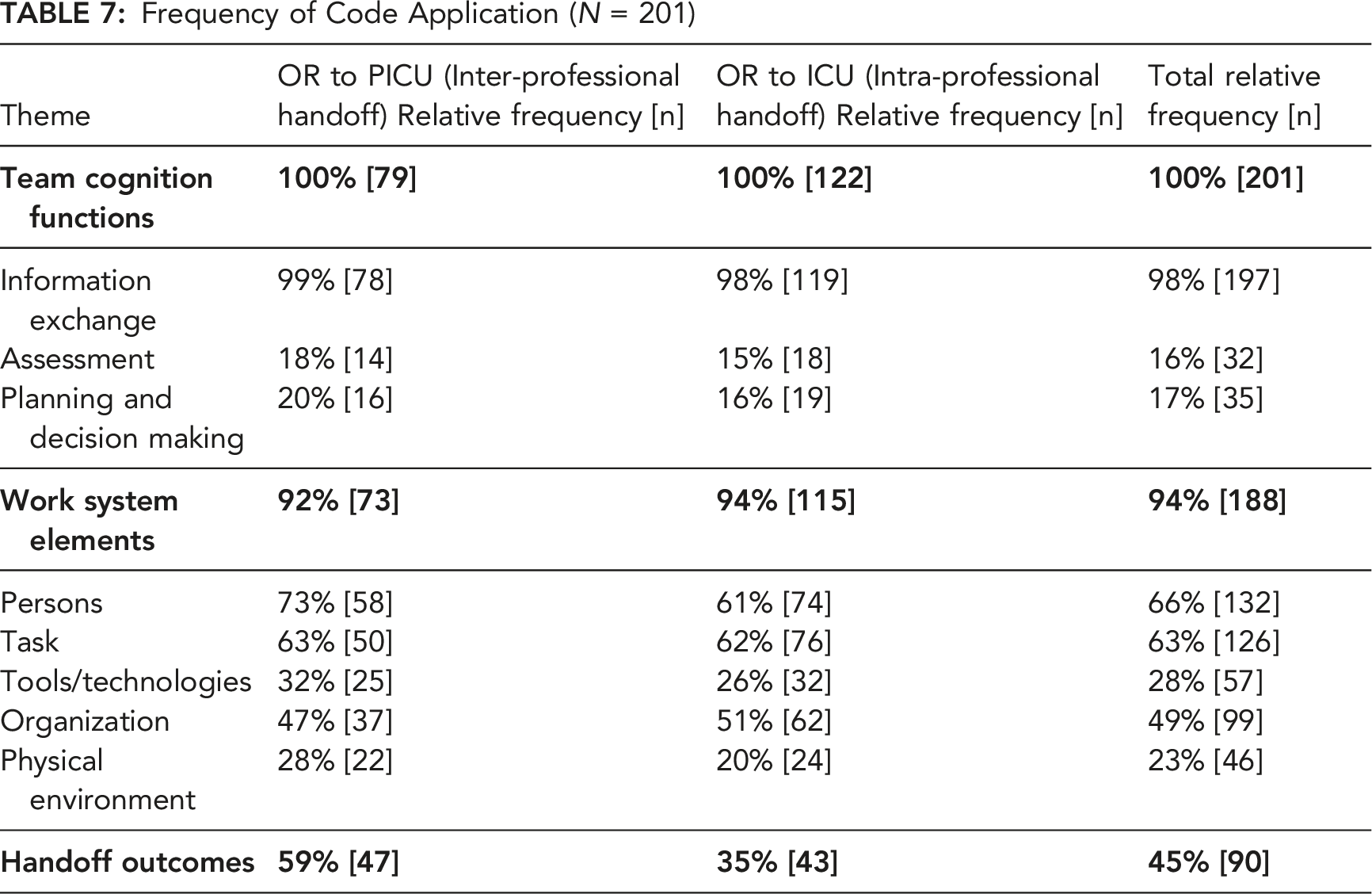
Tables 3–5 include example quotations. Table 7 shows the relative percentage and frequency of code application by handoff organization.
Team cognition functions
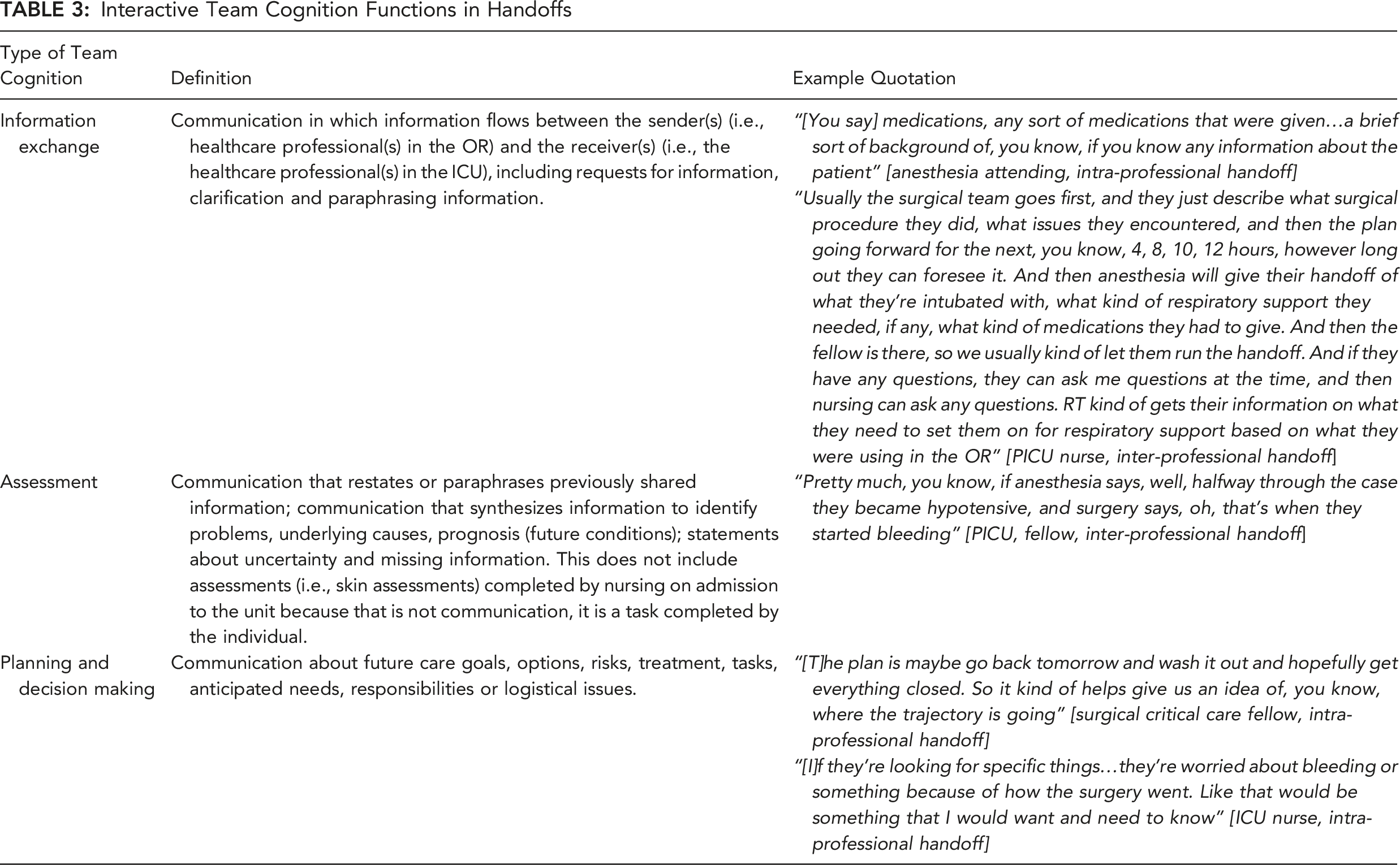
Participants in the inter-professional (OR to PICU) and intra-professional (OR to ICU) handoff talked about the three team cognition functions (see Table 3). Both groups mentioned the information exchange function most frequently. Many clinicians in the OR described the information they convey during the handoff. Information exchange also included the receiving PICU/ICU team requesting additional information or clarification.
Assessment was described the least by both groups. Assessment was typically described as the synthesis of information, for example, by identifying the underlying cause of events. A surgery chief resident in the intra-professional handoff echoed this when describing how understanding how the patient tolerated anesthesia in the OR helps the physician in the ICU “contextualize” the patient and provide better longitudinal care.
Planning and decision making was also described less often than information exchange. For example, the surgeon communicating the plan for future surgeries, particularly if there were open wounds, allowed the ICU team to better understand and anticipate how care of the patient would progress. The ICU nurses also pointed out that they needed to know what the physicians want to watch closely to better perform their job.
Work system elements
Table 4 describes the work system elements that influenced the various team cognition functions with selected quotes, and Table 7 shows the frequencies that each work system element was described with a team cognition function.
Frequency of Code Application (N = 201)
Two system factors were related to the interaction of the person and organization work system elements. In the OR to ICU handoff, the surgery attending is often the same attending staffing the ICU, eliminating a transition between physicians. However, it could be negative: they cover other services and may not be available at handoff. Participants in both handoffs noted there must be personnel resources to allow clinicians to participate in handoffs. Ideally, these clinicians would be those who provided care or who will provide care, rather than representatives, such as charge or floating nurses in the receiving PICU or ICU or an anesthesiologist who relieved the primary anesthesiologist involved in the surgery.
Participants in both handoffs talked about role ambiguity. Those involved in the OR to PICU handoff described the recent addition of another team member, the OR nurse, resulting in some confusion about who should report what. The OR to ICU handoff participants described not knowing who the primary bedside nurse was, since many nurses help settle the patient, but the primary nurse needed the handoff most.
Finally, both groups were sensitive to balancing the efficiency of the handoff with information flow, an interaction between the task and organization work system elements. A surgery chief resident expressed frustration when unrelated questions lengthened a handoff. Similarly, delays beginning handoff were frustrating, despite understanding the need to wait for all members to be present.
Handoff outcomes
Interviewees described a wide range of handoff outcomes (see Table 5). Participants in the inter-professional (OR to PICU) handoff talked about handoff outcomes more frequently than participants in the intra-professional (OR to ICU). The receiving team getting clear, sufficient and accurate information was a key outcome, as were efficiency and patient outcomes. For a more detailed analysis of the types of outcomes and differences between outcomes in the two groups, please see Wooldridge & Haefli (2019).
Results of the ENA
We used ENA to visualize, explore and compare relationships between work system elements, team cognition functions and outcomes. Figure 2 shows the average network for participants in the inter-professional handoff (OR to PICU), intra-professional handoff (OR to ICU) and the difference of these networks. The node size on the network graph represents the frequency of that code. The thickness of the lines between nodes represents the strength of the relationship between those codes, that is, frequency of co-occurrence. The squares are the centroids of the average networks, with dashed lines representing the 95% confidence interval of centroid location, while the circles are centroids of the network for individual interviews. The codes for the work system elements and team communication functions (i.e., processes) are generally to the left side of the graph, intertwined and inseparable. The outcome code is to the right side of the graph. Mean ENA Networks for (a) OR to PICU (inter-professional handoff), (b) OR to ICU (intra-professional handoff) and (c) Subtracted Mean (OR to PICU—OR to ICU). Note. Network centroids of interviewees participating in the inter-professional, OR to PICU handoff are significantly different along x-axis from the interviewees participating in the intra-professional, OR to ICU handoff (p < 0.001), but not significantly different along the y-axis (p = 0.72). Abbreviations are as follow. OR = Operating room. ICU = Intensive care unit. PICU = Pediatric intensive care unit. C.InfoExchange = Information exchange. C.Assess = Assessment. C.PlanDM = Planning and decision making. WS.Person = Persons work system element. WS.Task = Task work system element. WS.TT = Tools/technologies work system element. WS.Org = Organization work system element. WS.PE = Physical environment work system element. Outcome = Handoff outcome.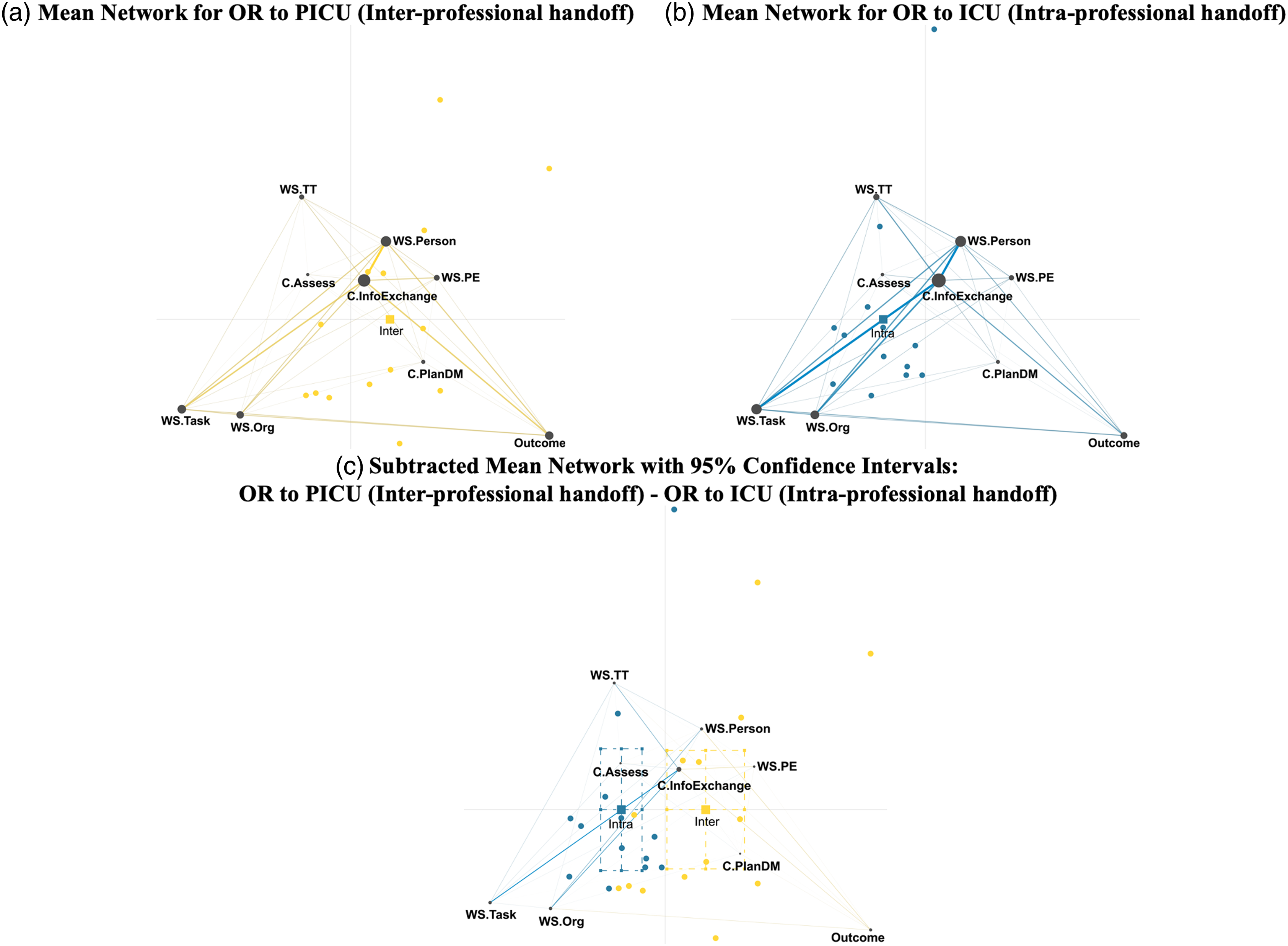
Information exchange is the largest node in both networks. The interprofessional handoff participants made strong connections between information exchange and outcome and person. An anesthesia resident in the inter-professional handoff described a repeating information (an outcome) caused by distractions (physical environment) and lack of focus (personal motivation) stemming from trouble untangling IV lines:
“
[I]t’s lines are tangled, no one can figure
out like where the
A-line
is, or the patient is coughing and we can’t find the line to bolus something through, or it’s just a lot of, like usually that happens
in situations where there’s like lots of lines and tubes and things going all over the place, and can just be a lot of stuff to manage, and then people can’t really focus on what they’re trying to tell each other.” [anesthesia resident,
inter-professional
handoff]
On the other hand, participants in the intra-professional handoff made less frequent connections between the system elements or processes and handoff outcomes. Instead, they focused on the influence of work system elements, particularly the person, task and organization, on information exchange. One of the ICU nurses described having worked with the surgical fellows (team experience) impacting whether the surgical fellow speaks to her. She goes on to describe the availability of the ICU resident (personnel resources) can result in a handoff outside the room after the initial discussion (work after handoff).
“
I will sometimes know a lot of like the like at least the surgical fellows, if they were in the case and stuff, if they come back with the patient like I know them. And so they like are, like I’m a familiar face…So sometimes like they’ll talk directly to me as well…sometimes the SICU resident isn’t even in the room right away because they didn’t even know the patient was coming at that time… they show up later, and then they’ll do like a brief overview” [ICU nurse,
intra-professional
handoff]
The subtracted network highlights the difference between the two groups, with the inter-professional handoff participants integrating handoff outcomes with work system and process codes. The Mann-Whitney U tests showed a significant difference in the location of the centroids of the networks along the first dimension (U=160.00, p<0.001) but not the second dimension (U=83.00, p=0.72). Participants in the intra-professional handoff made significantly stronger connections between work system elements, particularly task and organization, and information exchange; in other words, the handoff is something they do, with fewer reflections on outcomes, pulling their centroid in the negative direction.
Discussion
Team Cognition in Handoffs
Participants described three separate communication events in handoffs of pediatric and adult trauma patients from the OR to the PICU and ICU: (1) information exchange, (2) assessment and (3) planning and decision making. All three represent team-level cognitive processes, that is, team cognition. Information exchange, including OR clinicians giving report and PICU or ICU clinicians asking questions, was most reported. As argued in the literature, handoffs are not telegrams, and interactive, two-way communication for information exchange (i.e., asking questions) is a crucial part of handoffs (Cohen et al., 2012; Cohen & Hilligoss, 2009; Patterson & Wears, 2010). Our study further supports this argument, with two other crucial functions identified as follow. Assessment, e.g., synthesizing information from multiple sources to contextualize the patient, was reported less frequently, as was planning and decision making, e.g., developing care plans, deciding what to monitor. Frequency is not necessarily indicative of importance and training about handoffs as opportunities to transfer information may artificially inflate the prevalence of information exchange.
Impact of Work System on Team Cognition
This study suggests work system design influenced team cognition in handoffs. Participants in the inter-professional handoff described positive impacts of inter-professional handoffs on communication processes, e.g., information exchange, and outcomes: the inter-professional handoff facilitated interactions by bringing the team together to provide their unique perspective and role-specific information. However, this resulted in many people present, potential distractions and tension between efficiency and information flow; these were negative aspects of the work system. Negative impacts of intra-professional handoffs included missing information, but fewer people and distractions were involved. Intra-professional handoffs also facilitated tailoring information to the receiving clinicians as they were conducted separately for physicians and nurses. Role ambiguity, particularly identifying which nurse should receive handoff, was a challenge in the intra-professional handoff and could lead to the OR clinician delaying handoff or beginning too early.
The underlying tension between the benefits and shortcomings of inter-professional handoffs is due in part to limited education focused on interprofessional communication, professional silos and hierarchy (Weller et al., 2014). In this study, participants in the intra-professional handoff described “tailoring information” [Surgery/ICU attending, intra-professional handoff] based on the background of the person they were speaking to; for example, the surgeon might discuss wound care with the bedside ICU nurse but discuss the surgical procedure and plans in detail with the ICU attending. Tailoring information and language may represent a strategy to facilitate inter-professional communication in separate handoffs, but requires clear, shared understanding of what information is needed by whom to be effective. Without shared understanding, useful information maybe inadvertently withheld. Physicians and nurses described the importance of being able to ask questions in both handoffs, reflecting the importance of not allowing hierarchy to stifle organizational voice. Professional silos and hierarchy in health care may dictate who can ask what questions to whom, negatively impacting patient care and leaving key questions unasked. Alternate strategies to improve inter-professional communication, for example, enhanced inter-professional training and curriculum, could prove more effective than tailoring language in separate handoffs.
Work System-Based Interventions to Improve Team Cognition in Handoffs
Historically, recommendations for improving team cognition tend to focus on team training strategies or stable team membership. In this study we show how the design of work systems impacts team cognition. So, the question becomes how to design work systems to support team cognition. This could help to avoid the additional burden or workload of team training, which has not been robustly demonstrated to have long-term impact (Weaver et al., 2014). Stable or fixed team membership, another strategy to improve team cognition, does not adequately support the flexibility that health care requires. This study provides guidance for how to improve care transitions by redesigning the work system, as follows.
Participants in both handoffs described benefits of a well-understood process and the challenges of role ambiguity. Therefore, increasing organizational awareness, that is, awareness of how their roles fit in a thoughtfully-designed, understood process (Schultz et al., 2007), is an opportunity for improvement. Process mapping and process simulation are approaches that may increase organizational awareness and help design handoffs. Simulating the current process is a way for stakeholders to gain a more complete understanding of the process as it is actually done, not as it is imagined to be done (Barcellini et al., 2014). It also provides a useful opportunity to test and refine process redesigns in an iterative, participatory design approach (Barcellini et al., 2014). These strategies are in line with the meta-principles of sociotechnical system design proposed by Clegg (2000), specifically that design is a systemic, extended, contingent and socially-shaped process that involves making choices that should support the needs of the humans involved in the handoff. Further, embedded in our notion of process mapping and process design are all six process principles of Clegg (2000), augmented by ideas from participatory and constructive ergonomics (Falzon, 2014; Wilson et al., 2005). While we recommend process design that includes representations of the system (i.e., process maps), reflection and intentional implementation of changes but with participation of workers (i.e., insiders), the work system should also support adaptation of workers to emerging, unpredicted circumstances which may not include representations of work (Carayon et al., 2006, 2014, 2020; Holden et al., 2013; Hutchins, 1991). Future work could study the impact of participatory, constructive design practices on organizational awareness, in addition to linkages to process outcomes.
Another potential improvement identified by this study is developing tools and technologies to support clinicians during handoffs. Examples include simple, low-fidelity tools such as a laminated paper checklist of information to discuss, similar to that developed for multi-disciplinary rounds (Cox et al., 2017). The use of checklists in multi-disciplinary rounds addressed organizational voice issues by empowering the nurse through a leadership role in rounds; this could address the concerns voiced by the PICU nurse about the inter-professional handoff being less nurse friendly. Agarwal et al. (2012) found a structured handoff process improved perceived handoff quality, reduced information loss and improved four clinical outcomes: cardiopulmonary resuscitation, mediastinal reexploration, placement on extracorporeal membrane oxygenation and early extubations. However, care must be taken to avoid over-standardizing the process, which can have negative impacts (Patterson, 2008) and remove the ability of healthcare professionals to adapt as needed (Vincent & Amalberti, 2016), drawing on Clegg’s (2000) principle of flexible specification. While our participants did highlight the benefit of structured handoff process, seeming to conflict with the idea of flexible specification, the underlying benefit was from improved shared awareness discussed previously. Technology-based solutions, including information technology (IT), could also be developed to support handoffs (Bass et al., 2013; Flanagan et al., 2009; Van Eaton et al., 2004), particularly if they are designed to support teams, not individuals. For example, shared displays support situation awareness in resuscitations (Parush et al., 2017; Wu et al., 2017); similar displays could be developed to support care transitions. When implementing inter-professional handoffs, effort must be taken to support organizational voice, particularly of traditionally less powerful roles. Emphasizing and addressing inter-professional communication in the training of clinicians-to-be may decrease challenges in the future.
Summary of Recommendations to Improve Handoffs
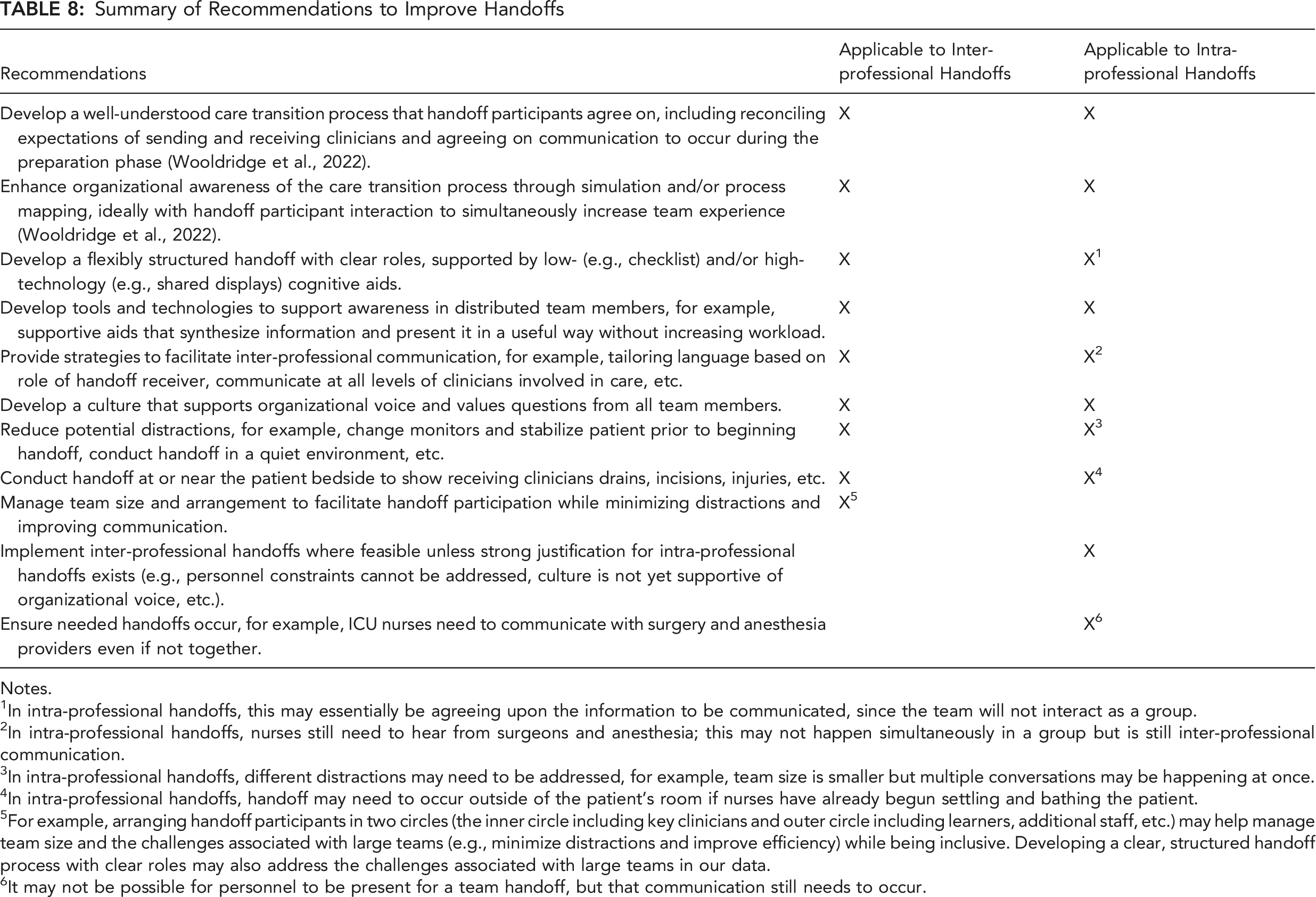
Notes.
1In intra-professional handoffs, this may essentially be agreeing upon the information to be communicated, since the team will not interact as a group.
2In intra-professional handoffs, nurses still need to hear from surgeons and anesthesia; this may not happen simultaneously in a group but is still inter-professional communication.
3In intra-professional handoffs, different distractions may need to be addressed, for example, team size is smaller but multiple conversations may be happening at once.
4In intra-professional handoffs, handoff may need to occur outside of the patient’s room if nurses have already begun settling and bathing the patient.
5For example, arranging handoff participants in two circles (the inner circle including key clinicians and outer circle including learners, additional staff, etc.) may help manage team size and the challenges associated with large teams (e.g., minimize distractions and improve efficiency) while being inclusive. Developing a clear, structured handoff process with clear roles may also address the challenges associated with large teams in our data.
6It may not be possible for personnel to be present for a team handoff, but that communication still needs to occur.
Limitations
This study was conducted in one healthcare system and compares only two cases (OR to adult ICU and OR to PICU care transitions), necessarily limiting generalizability. While this study represents a step toward conducting rigorous, situated field research on team cognition, it examines team cognition using interviews rather than observations. Interviews were useful to gain in-depth understanding of perspectives of clinicians and let us study transitions of trauma patients, which occur under time pressure and present logistical challenges to observe, but they may be subject to recall bias and under-emphasize assessment, planning and decision making. A more pressing limitation is that this study does not include the perspective of the patient or their family/caregiver. As health care progresses toward being more patient- and family-centered, it is increasingly important to include patients and their families (Valdez et al., 2015).
Conclusion
It is particularly important to study team cognition “in the wild” to learn how the sociotechnical (work) system can support improved team cognition with minimal added burdens. Using interviews, we examined team cognition and the sociotechnical system in which handoffs occurred. This is a unique approach to studying team cognition. Handoffs in care transitions constitute team cognition by the ITC definition (Cooke et al., 2013), with participants describing information exchange, assessment and planning and decision making as team-level cognitive processes involved in handoffs. Organization of handoffs (one work system element), that is, inter-professional versus intra-professional handoffs, impacted team cognition processes and outcomes. Inter-professional handoffs can enhance and hinder ITC. The presence of the inter-professional care team facilitated information exchange, improving perceived handoff outcomes; conversely, it hindered communication because the larger group of individuals resulted in logistic challenges and the diverse audience necessitate sometimes less precise communication strategies. We recommend future work investigate team cognition in the wild as it occurs during handoffs, leverage our findings to develop systems-based solutions to support team cognition in care transitions and develop methodologies to assess and predict the impact of changes to work system design on outcomes.
Footnotes
Acknowledgments
We thank the study participants, as our research would not be possible without them. We also thank Shannon Dean, Rima Rahal and Jennifer Hankwitz, who were instrumental in facilitating data collection. We appreciate the help provided by Madi Wall, RuthAnn Haefli and Maya Burgard, all undergraduate students who assisted with this work. Funding for this research was provided by the Agency for Healthcare Research and Quality (AHRQ) [Grant No. R01 HS023837]. The project described was supported by the Clinical and Translational Science Award (CTSA) program, through the National Institutes of Health (NIH) National Center for Advancing Translational Sciences (NCATS), [Grant UL1TR002373]. This work was funded in part by the National Science Foundation (DRL-0918409, DRL-0946372, DRL-1247262, DRL-1418288, DRL-1661036, DRL-1713110, DUE-0919347, DUE-1225885, EEC-1232656, EEC-1340402, REC-0347000), the MacArthur Foundation, the Spencer Foundation, the Wisconsin Alumni Research Foundation, and the Office of the Vice Chancellor for Research and Graduate Education at the University of Wisconsin-Madison. The opinions, findings, and conclusions do not reflect the views of the funding agencies, cooperating institutions, or other individuals. We also thank the original caretakers of the land where we performed this study. The University of Illinois at Urbana-Champaign occupies the lands of the Peoria, Kaskaskia, Piankashaw, Wea, Miami, Mascoutin, Odawa, Sauk, Mesquaki, Kickapoo, Potawatomi, Ojibwe, and Chickasaw Nations.
Key Points
• Care transitions, in particular handoffs, are characteristic examples of team cognition. • A change in sociotechnical system design—inter-professional handoffs versus intra-professional handoffs—influenced relationships between work system elements, team cognition, and outcomes. • Opportunities to improve care transition outcomes include changes to the organization of handoffs, increasing organizational awareness through simulation and participatory process analysis, and designing supportive tools and technology for teams.
ORCID iDs
Abigail R. Wooldridge is at The University of Illinois at Urbana-Champaign. Her highest degree is a PhD in Industrial Engineering specializing in Human Factors and Ergonomics, obtained in 2018 from The University of Wisconsin-Madison.
Pascale Carayon is at The University of Wisconsin-Madison. Her highest degree is a PhD in Industrial Engineering, obtained in 1988 from University of The University of Wisconsin-Madison.
Peter L. T. Hoonakker is at The University of Wisconsin-Madison. His highest degree is a PhD in Psychology, obtained in 2008 from University of Vienna Austria.
Bat-Zion Hose is at The University of Pennsylvania. Her highest degree is a PhD in Industrial Engineering, obtained in 2021 from the University of Wisconsin-Madison.
David Williamson Shaffer is at The University of Wisconsin-Madison. His highest degree is a PhD in Education, obtained in 1998 from Massachusetts Institute of Technology.
Tom Brazelton is at the University of Wisconsin School of Medicine and Public Health. His highest degree is a MD, obtained in 1994 from University of Tufts University School of Medicine.
Ben Eithun is at the University of Wisconsin School of Medicine and Public Health. His highest degree is a Master of Nursing, obtained in 2009 from University of Pennsylvania.
Deborah Rusy is at the University of Wisconsin School of Medicine and Public Health. Her highest degree is a MD followed by residency in Anesthesiology and fellowship in Neuroanesthesiology, obtained in 1997 from University of Wisconsin School of Medicine and Public Health.
Joshua Ross is at the University of Wisconsin School of Medicine and Public Health. His highest degree is a MD obtained in 2002 from The Ohio State University College of Medicine.
Jonathan Kohler is at the UC Davis School of Medicine. His highest degree is an MD in Medicine, obtained in 2005 from the University of Chicago Pritzker School of Medicine.
Michelle M. Kelly is at the University of Wisconsin School of Medicine and Public Health. Her highest degree is a MD, obtained in 2005 from Loyola University of Chicago Stritch School of Medicine.
Scott Springman is at the University of Wisconsin School of Medicine and Public Health. His highest degree is a Doctor of Medicine (MD), obtained in 1978 from the University of Wisconsin-Madison, WI.
Ayse P. Gurses is at the Johns Hopkins University and the Armstrong Institute Center for Health Care Human Factors. Her highest degree is a PhD in Industrial and Systems Engineering, obtained in 2005 from The University of Wisconsin-Madison