
Abstract
Objective
To investigate the effect of one’s sex and pedaling intensity on upper body muscle activation patterns during typing while cycling.
Background
Females are at a higher risk for computer work-related musculoskeletal disorders, and mobile workstations have been suggested to induce healthier muscular patterns compared with sitting. However, the neuromuscular characteristics of performing computer work in a cycling workstation have not been investigated.
Method
Twenty-two participants (10 females) completed a 60-min computer typing task while pedaling on a cycle ergometer at two different intensities (25%, 4% heart rate reserve). Surface electromyography (EMG) was recorded from seven muscles of the upper body. Effects of time, sex, and intensity were assessed for muscle activation (RMS), activation variability (CV), and normalized mutual information (NMI) via generalized estimating equations.
Results
With time, neck/shoulder CV increased in males during higher pedaling intensity, whereas in females it decreased during lower intensity. In females, RMS of neck/shoulder and NMI of neck/shoulder muscle pairs were lower, whereas forearm RMS was 34.2% higher with higher intensity cycling compared with lower intensity. Lower back RMS decreased 28.3% in the initial half of the task in females, but in males it increased 14.4% in the later half.
Conclusion and application
Cycling workstation showed a sex- and intensity-specific EMG response. These differing responses should be considered when implementing the use of cycling workstation and may be important for preventing/managing sex-specific muscle fatigue and musculoskeletal disorders.
Introduction
Concerns have been raised toward workforce becoming more computer based (Straker & Mathiassen, 2009) and with the associated increase in overall sedentarism (Brownson et al., 2005). Inadequate physical activity is a major preventable risk factor of various related negative health burdens (Dunstan et al., 2010). Prolonged sitting (e.g., traditional computer work) is linked to work-related musculoskeletal disorders (MSDs; World Health Organization, 2003), especially in the neck/shoulder and lower back area (Ardahan & Simsek, 2016).
One feasible countermeasure tool to address occupational sedentarism and reduce MSD symptoms is dynamic workstations (Carr et al., 2012; McAlpine et al., 2007; Thompson et al., 2008). For example, in a study by Thompson et al. (2008), subjects with back pain reported that using a treadmill workstation reduced their back pain. Furthermore, Fedorowich et al. (2015) reported that walking (compared with sitting) while performing a computer task was associated with less upper limb discomfort and muscle activation patterns that resembled more those of healthy, as opposed to fatigued or injured individuals. These positive results may be due to the different back and upper limb posture between walking and sitting, as previous studies have suggested that seated position may be associated with higher low back strain (Wilke et al., 2001). However, the effect could also be due to the dynamic component of the mobile workstation, as exercise increases muscle blood flow and oxygenation, and thus prevents fatigue development. Amongst the different workstations, cycling workstations provide an interesting solution in that they have shown less detrimental effects on computer typing performance such as typing speed than the walking workstation, when compared with traditional sitting (Elmer & Martin, 2014; Straker, Levine, et al., 2009). However, despite this better computer performance with the cycling workstation, its effect on neuromuscular measures have not been investigated.
There are sex-specific risk factors of MSDs, where females report more neck/shoulder symptoms and males suffer more lower back injuries (Hooftman et al., 2009). This could be, at least in part, related to the sex-specific neuromuscular response to fatigue, as muscle fatigue may be a critical physical precursor of work-related MSDs (van der Windt et al., 2000). Muscle fatigue is characterized by increased muscle activation (Vøllestad, 1997), activation variability (Srinivasan et al., 2016), and mutual information (i.e., shared connectivity between muscle pairs; Madeleine et al., 2011). Increased muscle activation variability may indicate that the neuromuscular system is searching for new motor patterns to maintain task performance as muscles fatigue (Côté, 2014). Decreased mutual information may represent a strategy to prevent the spread of fatigue across other muscles (Fedorowich et al., 2013). Low mutual information (i.e., low functional connectivity) may be associated with musculoskeletal symptoms of the neck/shoulder area (Madeleine et al., 2016).
It has been suggested that muscle activation patterns, including variability and mutual information, are associated with sex-specific fatigue and injury mechanisms (Fedorowich et al., 2013). Accordingly, studies have shown sex-specific muscle activation responses to fatigue. For example, during a fatiguing repetitive task, males showed higher upper trapezius activation variability than females (Srinivasan et al., 2016), and while connectivity of upper and lower trapezius muscles decreased in males, females showed no change (Fedorowich et al., 2013). As per research with computer work, Cui et al. (2020) reported that females had higher deltoid activation compared with males during a seated computer task. These suggest that males may possess a better muscle activation patterns during repetitive tasks and computer work. As mobile workstation has shown improvement in discomfort and activation patterns than sitting, and there is sex-specific neuromuscular response to fatigue, it is possible that mobile workstation may elicit different activation pattern response between females and males. Therefore, sex-specific muscular response to dynamic workstations was investigated in the present study.
Exercising at higher intensities is associated with greater energy expenditure and systemic cardiovascular health benefits, although prolonged tasks that lead to neuromuscular fatigue have been associated with the development of MSDs (Côté, 2014). Moreover, the intensity at which individuals should cycle or walk to gain positive physical effects but avoid negative impact on work performance has not been established. Previously, cycling at 25% and 40% heart rate reserve (HRR) has shown no difference in typing performance compared with sitting (Commissaris et al., 2014). We recently found that compared with cycling at 25% HRR, the 40% HRR session was associated with greater blood flow to the neck/shoulder and wrist muscles, and faster typing speed without a difference in typing error (Yoon et al., 2019). Further, there were differences in time-course changes across sexes and pedaling intensities (25%, 40% HRR) in typing accuracy and error, but not in blood flow (Yoon et al., 2019). In that paper, we reported the typing performances and the discomfort, vascular, and analgesic characteristics of the neck and upper limb during a computer task performed on a cycle ergometer, but the electromyographic data were not reported (Yoon et al., 2019).
To our knowledge, the specific guidelines of pedaling intensity and duration of these cycling workstation have not been established and the neuromuscular parameters during computer work in a cycling workstation have not been investigated. Hence, the objective of the present study was to examine the sex-specific time-course of upper body neuromuscular patterns during a 60-min simulated computer work task performed while pedaling at two different intensities on a cycle ergometer. We hypothesized that muscle activity characteristics (amplitude, coefficient of variation, functional connectivity) would show different: (1) time-course changes across sexes and pedaling intensities, (2) pedaling intensity-dependencies across sexes, and (3) time-course changes across sexes.
Methodology
We completed an experimental study of adult female and male participants while they pedaled at a computer workstation at two different pedaling intensities (25%, 40% HRR) for 60 min each. During this time, we continuously measured the activity of seven muscles for 30 s every 10 min, including: five neck and shoulder muscles, a forearm muscle that extends the wrist, and a low back extensor muscle. For each second within these 30-s epochs, we calculated the amplitude of the muscle activity. From these 30 amplitudes, we calculated the average amplitude and the coefficient of variation within each muscle for each 30-s epoch. In addition, we calculated the functional connectivity across the muscles for each 30-s epoch. We then compared these metrics across time (six levels), pedaling intensities (two levels), and sexes (two levels).
Participants
A convenience sample of 12 males and 10 females volunteered to participate in this study. Inclusion criteria were to be aged between 18 and 30 years, computer use for at least 40 hr per week, and free of any neurological, cardiorespiratory, or musculoskeletal injuries of neck/shoulder and any other health concerns provided by the Physical Activity Readiness Questionnaire (CSEP Expert Advisory Committee, 2002). The experiment took place in the Occupational Biomechanics and Ergonomics Laboratory (OBEL) of the McGill University in Montreal, Quebec. All participants provided written informed consent prior to testing. This research compiled with the American Psychological Association Code of Ethics and was approved by the Research Ethics Board of the Center for Interdisciplinary Research in Rehabilitation (CRIR) of Greater Montreal.
Session 1 (Familiarization, Determination of Maximal Heart Rate Reserve)
The participant attended three sessions. The first session comprised of an incremental maximal cycling test to determine one’s maximal heart rate. The cycle ergometer (Monark 814E, Sweden) seat was adjusted to provide 10–15° knee flexion at the most extended position and a heart rate monitor (Polar T61-coded) was placed with the sensor aligned to the xiphoid process. The maximal heart rate test involved the participant pedaling at 70 revolutions per minute starting with 1 kg resistance then .25 kg of resistance being added each subsequent minute concurrently with obtaining the Borg rating. The participant continued until they either reached a rating of 20 on the Borg general (6–20) rating scale (Borg, 1970), could not pedal over 60 revolutions per minute, or voluntarily stopped. The participant was not aware of the stoppage criteria. The peak heart rate was obtained as the highest value recorded on the heart rate monitor throughout the test. Following the test, familiarization of the computer typing task while pedaling on the cycle ergometer, called the Bike-and-Type task (Figure 1), was performed for 5 min. The set-up included desk height being set to provide a 90° elbow flexion when the hands are placed on the laptop keyboard, and the typing task involved reproduction of predetermined article text displayed on the laptop’s 15-inch display.
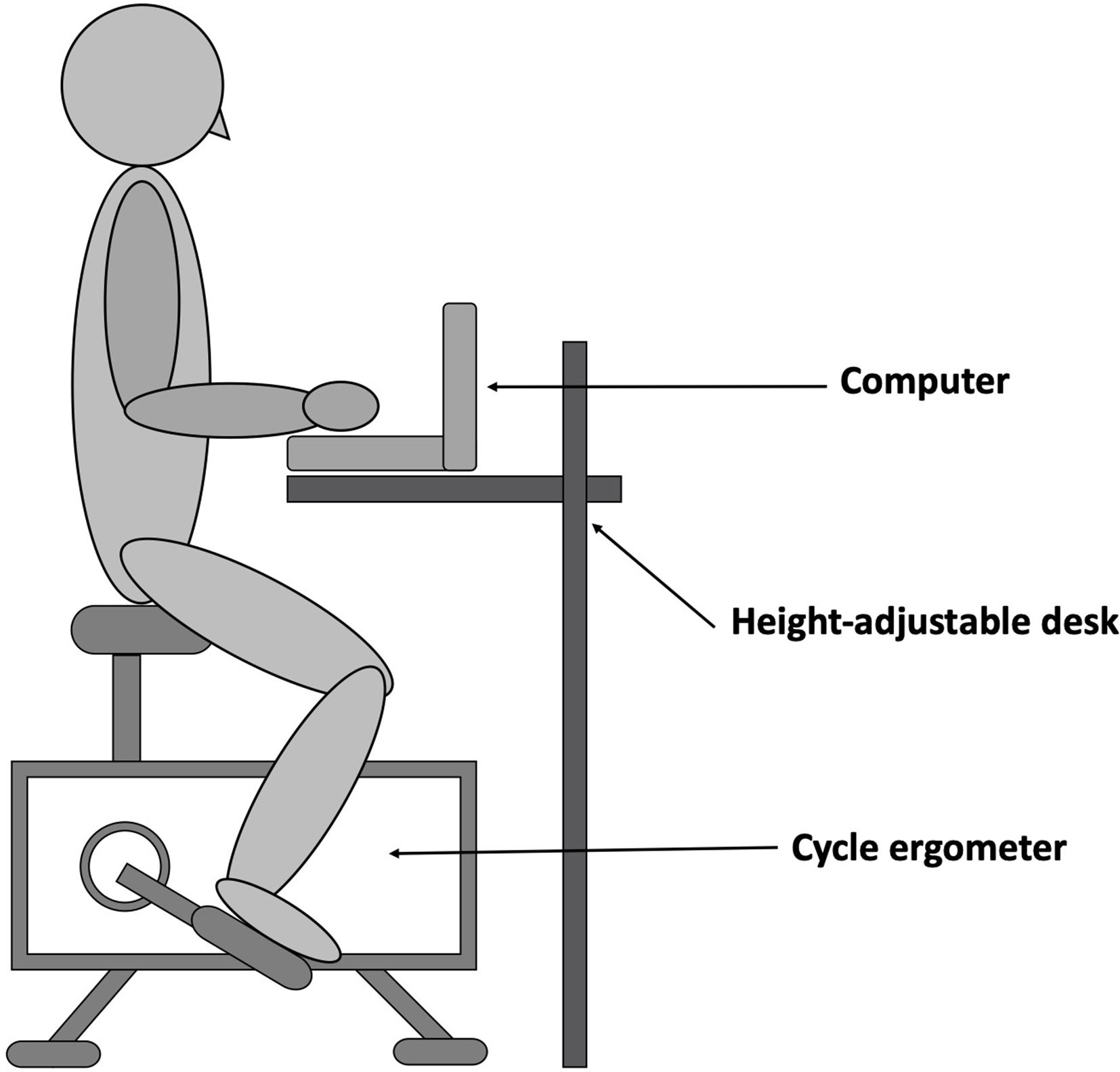
Illustration of performing the standardized computer typing task while biking on a cycle ergometer.
Sessions 2 and 3 (Bike and Type)
The second and third sessions involved identical experimental procedures to another, but at different cycling intensities (25% or 40% HRR; Commissaris et al., 2014) and were assigned in random order for each participant. Upon arrival, resting heart rate was measured by having the participant lay down in a supine position for 5 min. Using the maximal heart rate obtained in the first session and resting heart rate, the target heart rate (25% or 40% HRR) was calculated via the Karvonen formula. These heart rates were used as they have shown feasibility for computer work in the past (Commissaris et al., 2014).
For the Bike-and-Type task, the participant was instructed to cycle at their desired pedaling speed and reproduce a pre-determined text using the Mavis Beacon Teaches Typing software, used in previous mobile workstation studies (Fedorowich & Côté, 2018; Fedorowich et al., 2015; Yoon et al., 2019). The heart rate was continuously monitored by the researcher, and the resistance of the cycle ergometer was manually changed to keep the participant’s heart rate within the target heart rate zone (i.e., within the calculated target heart rate ±5 bpm) throughout the task. There were six 10-min bouts of Bike-and-Type, in which the target heart rate zone was maintained. At 9:30 min, the electromyography (EMG) data were collected for 30 s. At 10:00 min, the participant stopped cycling and typing, and the measures of typing performance, and other muscular characteristics were recorded. These results were presented in our previous manuscript (Yoon et al., 2019). The average duration of the interruption between bouts were 90 s. Then starting with the cycling to desired HR, the 10 min Bike-and-Type bout was repeated until six bouts were completed. This entire procedure was repeated during the third session at the different intensity/HRR with at least 48 hr and at most 10 days between each of the three sessions.
Data Collection
Bipolar Ag/AgCl surface electrodes (Ambu, Denmark) were placed over eight muscle sites based on SENIAM guidelines (Hermens et al., 1999). The EMG data were recorded at a sampling rate of 1000 Hz via the TeleMyo data acquisition system (TeleMyo, Noraxon, USA, 10–500 Hz operating bandwidth). The skin was shaved, abraded with alcohol, and the electrodes were placed parallel to muscle fibers. A reference electrode was placed over the medial head of the right clavicle, and the cables were attached to the electrodes and secured with medical tape. The electrode placement locations and maximum/reference isometric voluntary contraction (MVC/RVC) actions are described in Table 1. Two trials of MVC/RVCs were performed for each muscle, and the participant crossed their arms during RVCs of Lumbar Erector Spinae. Each MVC/RVC was held for 3 s, and there was 1 min of rest in between trials. These contractions were performed prior to the Bike-and-Type task.
Electrode Locations and MVC/RVC Actions for Each Muscle
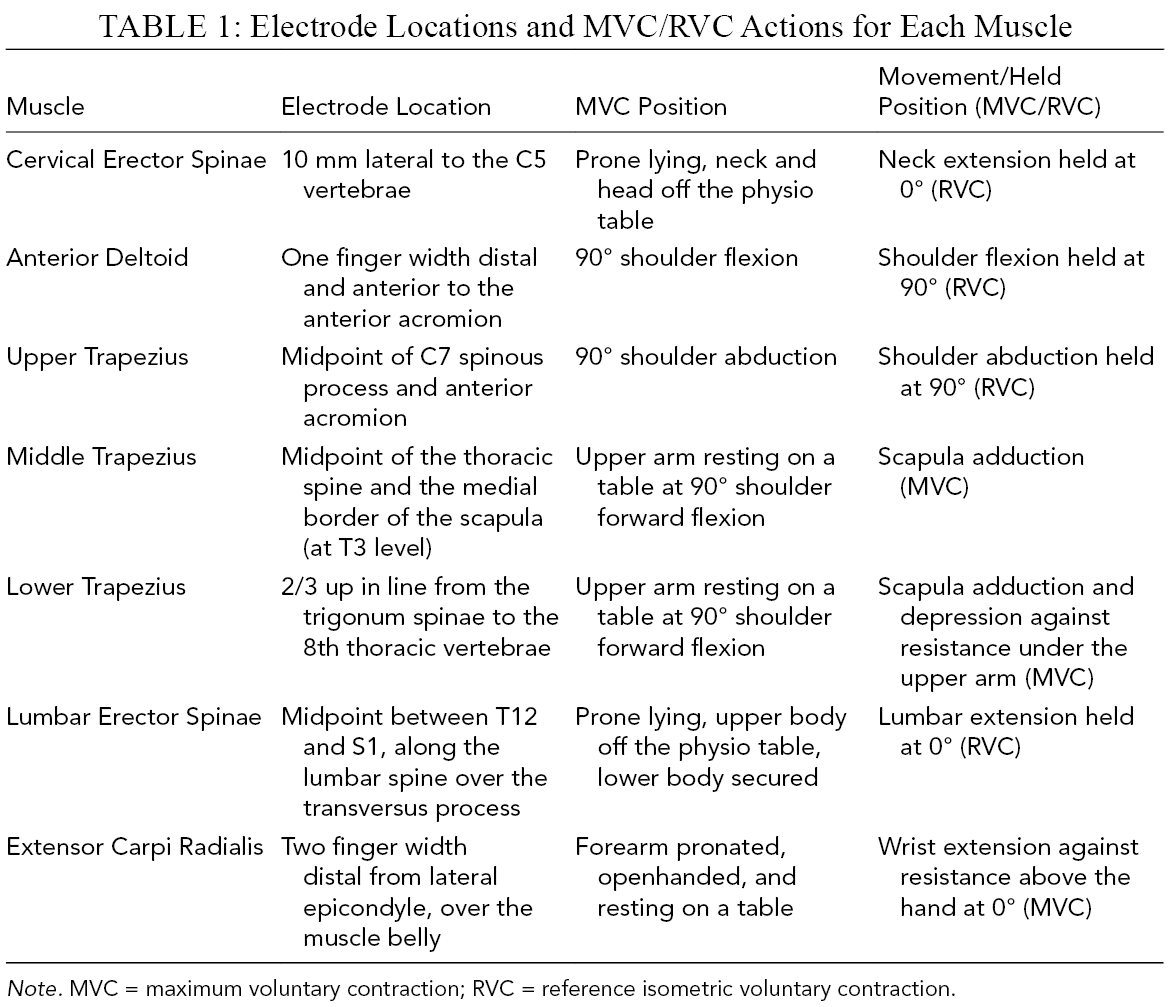
Note. MVC = maximum voluntary contraction; RVC = reference isometric voluntary contraction.
Data Processing and Analysis
Custom programs in Matlab (The MathWorks, Inc., Natick, MA, USA) were used for data analysis. Heartbeats were removed via a subtraction technique from contaminated channels (Bartolo et al., 1996; Marker & Maluf, 2014), described in detail by Minn and Côté (2018). All EMG data were band-pass filtered (Butterworth 2nd order, 10–450 Hz), full-wave rectified, and normalized to MVC/RVC values (expressed as %MVC/RVC). Root mean square (RMS) values were calculated over thirty 1-s nonoverlapping windows for each bout, and the average of 30 RMS values were used as the representative mean amplitude value of each muscle and bout. The coefficient of variation (CV; activation variability) was calculated by dividing the standard deviation for the 30 RMS values with the average RMS value for each muscle during each bout.
Functional connectivity of pairs of all the neck/shoulder muscles recorded from Cervical Erector Spinae, Upper, Middle, and Lower Trapezius, and Anterior Deltoid was calculated as the normalized mutual information (NMI; Johansen et al., 2013; Madeleine et al., 2011, 2016). NMI was calculated between pairs of filtered EMG series (i.e., band-pass filtered data) over 30 s lengths. NMI is a statistical method of quantifying the amount of shared activation between two muscles, accounting for both linear and nonlinear characteristics and of the relationships between both muscles’ EMG time series (Jeong et al., 2001). NMI is between 0, indicative of no connectivity, and 1, indicative of complete functional connectivity within a muscle pair (Johansen et al., 2013; Madeleine et al., 2011). More information on how NMI was calculated (Jeong et al., 2001; Madeleine et al., 2011) can be found in Supplemental Material 1. A limitation of the version of this method used in the current study is that it only involves normalization of the signal ranges and does not necessarily involve smoothing of the EMG signals. Thus, sources of EMG error that are usually corrected during smoothing may affect individual EMG signals and NMI calculations.
Statistical Analysis
Independent t-tests were conducted to test for sex effects (male, female) on height and mass. The dependent variables of EMG RMS, CV, and NMI were tested for main and interaction effects of the independent variables of Intensity (25%, 40% HRR), sex (male, female), and time (10, 20, 30, 40, 50, 60 min) via generalized estimating equations (GEEs; Link Function = Identity; Structure of Covariance Matrix = Exchangeable) in SPSS (v23, IBM Corporation). First, to test if time-course changes of the muscle activity metrics differed across sexes and pedaling intensities, we looked at the three-way interaction term of intensity × time × sex. Second, to test if pedaling intensity-dependent muscle activity metrics differed across the sexes, we examined the intensity × sex interaction term. Lastly, to test if the time-course changes differed between the sexes, we looked at the time × sex interaction term. Interaction effects were explored by post-hoc pair-wise comparisons (Wald X2) with sequential Bonferroni adjustments (two-tailed). The statistical significance was set at p < .05.
Results
Group Characteristics
Males were taller and heavier than females (Table 2).
Height and Mass of Male and Female Groups and p Values for Sex Differences
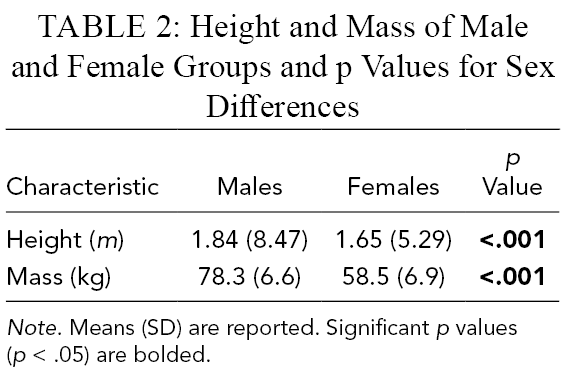
Note. Means (SD) are reported. Significant p values (p < .05) are bolded.
Muscle Activation Amplitude (Figure 2)
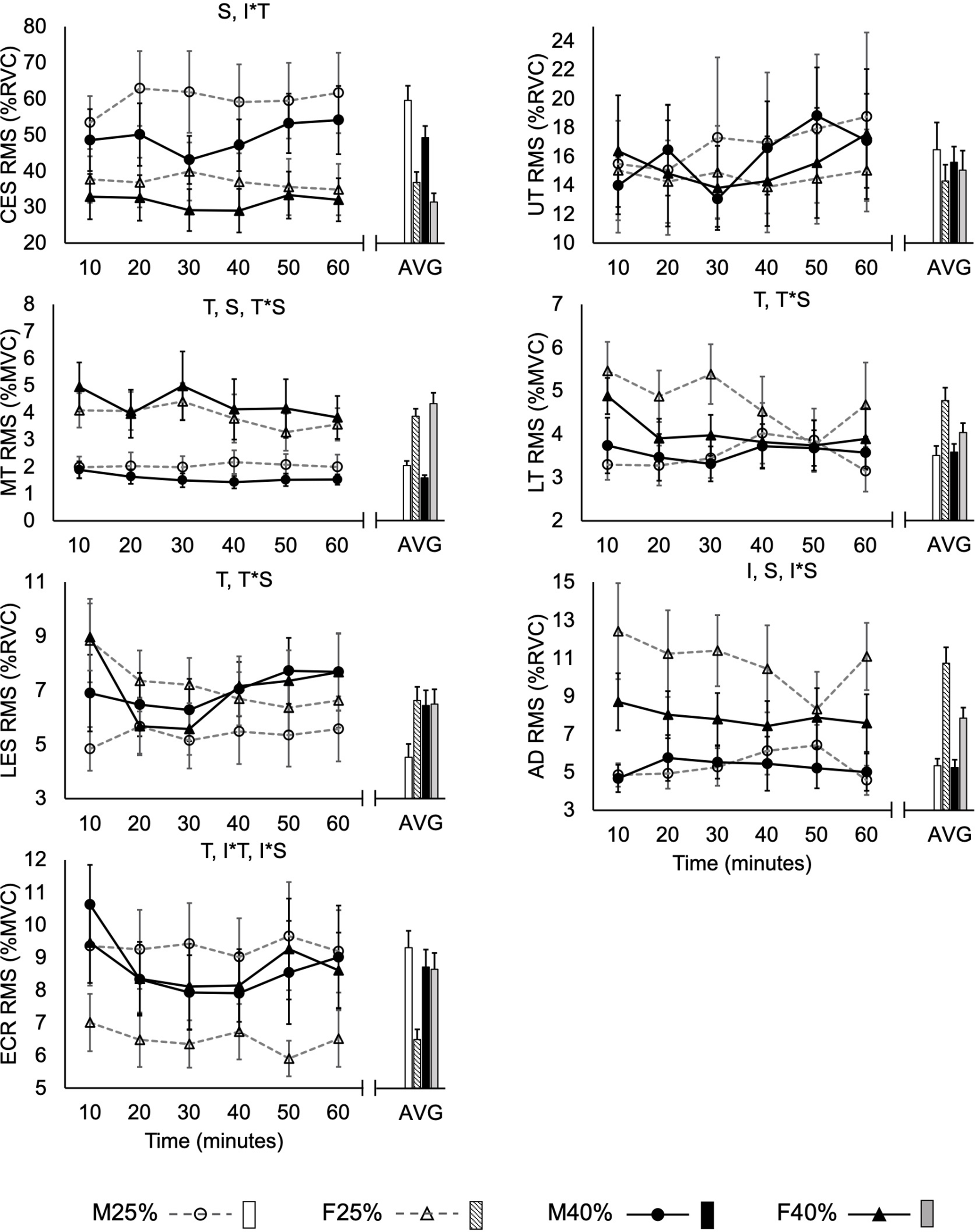
Muscle activation amplitude (RMS) normalized to maximal (MVC) or sub-maximal reference (RVC) voluntary contractions recorded from male (
Group average values for muscle activation, activation variability, and normalized mutual information are presented in Supplemental Materials 2–5, respectively. Further, Supplemental Materials 5 presents the p values of all main and interaction effects for all measured variables.
For all seven muscles, there were no significant three-way interaction effects (p > .05), indicating that the time-course changes were not different across sexes and pedaling intensities.
There were significant intensity × sex interactions in two of the seven muscles: anterior deltoid (X2 = 4.52, p = .034) and extensor carpi radialis (X2 = 4.26, p = .039). During the 40% HRR session (in comparison with 25% HRR), females showed lower anterior deltoid and higher extensor carpi radialis activations. Compared with the males, females had higher muscle activity in the anterior deltoid muscle and lower muscle activity in the extensor carpi radialis during the 25% HRR session. No differences between the sexes were observed during the 40% HRR.
There were significant time × sex interactions in three of the seven muscles: middle (X2 = 39.66, p < .001) and lower (X2 = 13.75, p = .017) trapezius, and lumbar erector spinae (X2 = 20.45, p = .001). Middle and lower trapezius activations decreased with time in females. Compared with males, females had higher activation of middle trapezius at all time points and of lower trapezius at 10 and 30 min. As for lumbar erector spinae activation, it decreased in females (activation in 10 > 20, 30 min) while it increased in males (30 < 40, 50 min). Lumbar erector spinae activation was higher in females compared with males at 10 min.
Finally, there were significant intensity × time interaction effects in two of the seven muscles: cervical erector spinae (X2 = 13.15, p = .022) and extensor carpi radialis (X2 = 11.30, p = .046). Cervical erector spinae muscle activation was lower at 30 min during the 40% HRR session compared with 25% HRR. Extensor carpi radialis muscle activation was greater during 40% HRR compared with 25% HRR at 10 min, and there was a decrease (10 > 20, 30, 40 min) only during the 40% HRR session. Main effects of sex, intensity, and time are indicated in Figure 2.
Muscle Activation Variability (Figure 3)
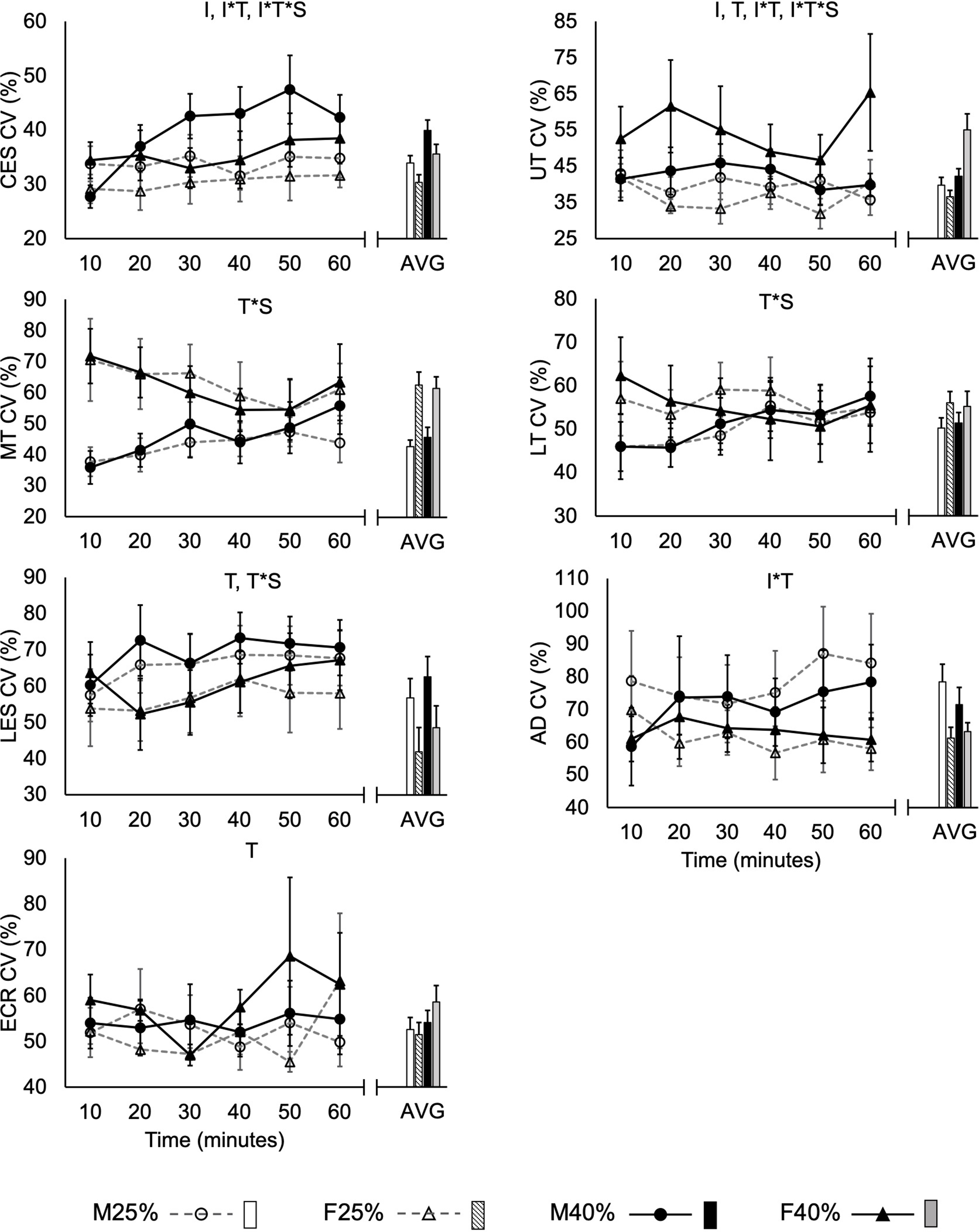
Muscle activation amplitude’s variability (CV) recorded from male (
There were significant intensity × time × sex interaction effects in two of the seven muscles: cervical erector spinae (X2 = 21.18, p < .001) and upper trapezius (X2 = 13.56, p = .019). Cervical erector spinae activation variability of males during the 40% HRR session increased (10 < 30, 40, 60 mins), whereas upper trapezius activation variability of females during 25% HRR session decreased (10 > 50 min).
There were no significant intensity × sex interaction effects (p > .05) in all seven muscles, indicative of no difference in intensity dependent activation variability across sexes.
There were, however, significant time × sex interaction effects in three of the seven muscles: middle (X2 = 44.39, p < .001) and lower (X2 = 15.98, p = .0069) trapezius, and lumbar erector spinae (X2 = 24.39, p < .001). Whereas activation variability of middle trapezius generally decreased with time in females (10, 20 > 40, 50 min), it increased in males (10 < 30, 50, 60 min). Lower trapezius activation variability increased in males (10, 20, 30 < 60 min), but no significant change was seen in females. Finally, lumbar erector spinae activation increased from the 20 to the 50 min in females, whereas it increased at 10 to 30, 40, 50, 60 min in males.
There were significant intensity × time interaction effects in three of the seven muscles: cervical erector spinae (X2 = 13.35, p = .020), upper trapezius (X2 = 17.95, p < .001), and anterior deltoid (X2 = 22.29, p < .001) muscle activation variability. Cervical erector spinae activation variability generally increased during the 40% HRR session, and at 50 and 60 min, 40% HRR session showed higher variability compared with 25% HRR. Upper trapezius activation variability was higher during the 20 min, whereas anterior deltoid activation variability was lower at 10 min during the 40% HRR session compared with 25% HRR. The main effects on CV are indicated in Figure 3.
Normalized Mutual Information (Figure 4)
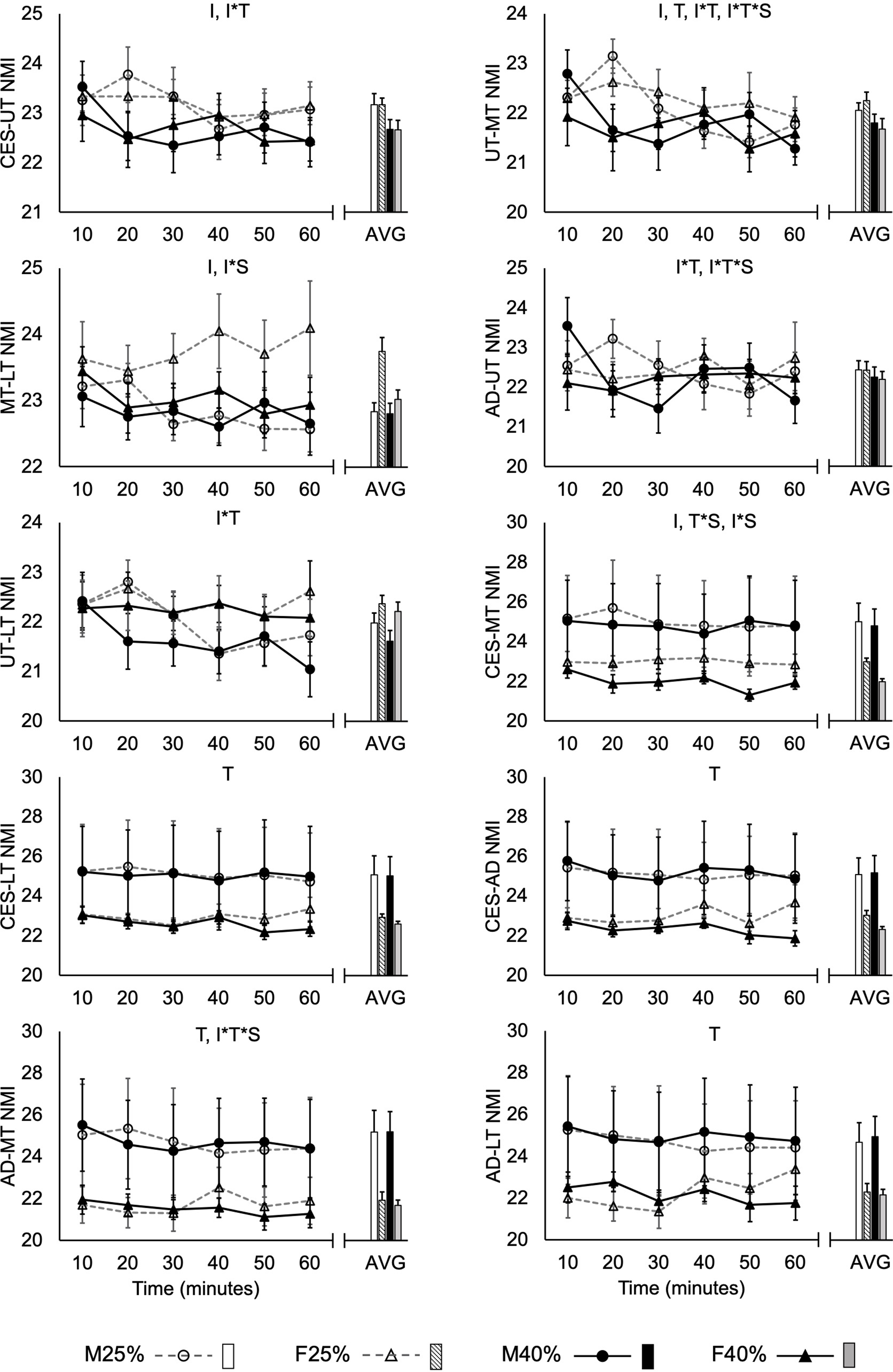
Normalized mutual information (NMI) within electromyographical time series of pairs of muscles recorded from male (
There were significant intensity × time × sex interactions on three of the ten NMI variables: anterior deltoid-middle trapezius (X2 = 12.14, p = .033), upper-middle trapezius (X2 = 12.39, p = .030), and anterior deltoid-upper trapezius (X2 = 12.25, p = .032). Male’s anterior deltoid-middle trapezius NMI during the 40% HRR session decreased from the 10 to the 60 min. Female’s upper-middle trapezius NMI was lower at 60 min during the 40% HRR session compared with 25%. Lastly, although anterior deltoid-upper trapezius NMI showed a significant three-way interaction effect, pairwise comparisons did not reach significance.
There were significant intensity × sex effects in NMI of two of the ten NMI variables: middle-lower trapezius (X2 = 4.46, p = .035) and cervical erector spinae-middle trapezius (X2 = 6.80, p = .0091). Only the female participants were affected by the pedaling intensity. NMI of middle-lower trapezius and cervical erector spinae-middle trapezius pairs in females were lower during the 40% HRR compared with the 25% HRR session, which was not seen in males. In addition, females had higher middle-lower trapezius NMI compared with males during the 25% HRR session.
There were significant time × sex interactions in just one of the ten NMI variables. Cervical erector spinae-middle trapezius NMI generally decreased with time in females (10 > 50, 60; 40 > 50 min) but not in males (X2 = 19.10, p = .0018).
There were significant intensity × time interaction effects in four of the ten NMI variables: cervical erector spinae-upper trapezius (X2 = 14.81, p = .011), upper-middle trapezius (X2 = 19.24, p = .0017), upper-lower trapezius (X2 = 16.57, p = .0054), and anterior deltoid-upper trapezius (X2 = 16.12, p = .0065). Cervical erector spinae-upper trapezius NMI was lower at 40% HRR session compared with 25% HRR during 20, 30, and 60 min. Upper-middle trapezius NMI decreased differently between 25% HRR (10 > 60 min) and 40% HRR (20 > 40, 60 min) sessions. Moreover, upper-middle trapezius NMI was lower at 20 min during 40% HRR compared with 25% HRR session. Lastly, upper-lower trapezius NMI significantly decreased (20 > 40 min) during 25% HRR session and was lower at 20 and 60 min during 40% HRR session compared with 25% HRR. Anterior deltoid-upper trapezius NMI showed significant intensity × time interaction effect, but pairwise comparison did not show a significant result. Main effects on NMI are identified in Figure 4.
Discussion
This is the first study to investigate the sex-specific neuromuscular response to cycling computer workstation. Our main findings were that (1) there were sex-specific time-based responses to different cycling intensities in the neck/shoulder muscles, (2) pedaling intensity only affected female’s neck/shoulder/forearm muscles, (3) the time-based muscle activation responses in the upper/lower back muscles differed between the sexes and suggest that 30min usage of cycling workstation is associated with healthy muscular patterns (i.e., unchanged/decreased muscle activation amplitude).
Sex-Specific Time-Based Responses to Different Pedaling Intensity
In line with our hypothesis, there were different time-course changes in muscle activity across sexes and pedaling intensities, but only in the neck/shoulder muscles. Intensity × time × sex interactions showed that cervical erector spinae activation variability increased while NMI of the anterior deltoid-middle trapezius pair decreased during the 40% HRR session in males. This may be related to our previous findings of more consistent performance through time at the 40% HRR pedaling intensity in females (Yoon et al., 2019). Increased activation variability is a characteristic of muscle fatigue development and may represent a mechanism of finding new motor patterns to substitute fatigued muscles and prolong task performance (Côté, 2014). Moreover, it is suggested that low mutual information may be a beneficial strategy in preventing the spread of fatigue symptoms across more muscles (Fedorowich et al., 2013), whereas shared connectivity increases with fatigue and in individuals reporting post exercise delayed onset muscle soreness (Madeleine et al., 2011). Hence, our observation in males may be explained by the fatigue developing in the cervical erector spinae muscle, which led to increasing its activation variability and decreasing its neck/shoulder functional connectivity. This could reflect a strategy to prevent the spread of fatigue symptoms to the cervical erector spinae muscle. Moreover, as 25% HRR intensity did not show any significant changes in males, these results suggest that a minimum threshold intensity level, higher than 25% HRR, may be necessary to reach this effect that is observed only in males.
Females, on the other hand, had a decrease in activation variability of upper trapezius during the 25% HRR session. Low variability has been shown to be associated to high fatigability especially in females (Fedorowich et al., 2013) and elevated risk for MSDs (Madeleine et al., 2011). This may be important for female computer workers since neck/shoulder MSDs are generally more prevalent in females than males and upper trapezius is an especially vulnerable muscle in females (Côté, 2012). However, comparisons between cycling and traditional computer workstations are needed within the same experimental paradigms in order to validate whether any cycling workstation can indeed provide a beneficial effect to the upper trapezius. Nonetheless, our results showed that there are time-based responses during 40% HRR pedaling in males and during 25% HRR in females, that together suggest more beneficial effects at the higher intensity in both males and females, although through changes in different features of muscle activation.
Pedaling Intensity Only Affected Females
Intensity × sex interaction results showed that pedaling intensity, as an independent variable, only affected females and not males. Female’s anterior deltoid activation, and NMI of middle-lower trapezius and cervical erector spinae-middle trapezius were lower in the 40% HRR session compared with the 25% HRR, whereas males had no significant difference between the intensities. High and increased muscle activity during computer work are suggested to be risk factors of MSD development (Cooper & Straker, 1998; Kleine et al., 1999), which could suggest that the 40% HRR is better than 25% HRR in terms of MSD development risks. Similar to the aforementioned positive effect of lower functional connectivity, it is possible that the anterior deltoid activation was able to be lower during the 40% HRR in females due to the lower NMI preventing spread of fatigue symptoms to the anterior deltoid muscle. This intensity-specific response may be related to the blood supply to these muscles, as we have previously shown greater upper trapezius and wrist extensor blood flow during the 40% HRR session compared with 25% HRR (Yoon et al., 2019). However, no sex differences in blood flow were found in that study (Yoon et al., 2019). As such, other cardiovascular factors such as female’s greater vasodilation (Parker et al., 2007) and lower muscle deoxygenation compared with males (Smith & Billaut, 2012), independent of strength and performance decline, could be at play. Moreover, a relationship between oxygenation and central motor output has been theorized in the past (Amann et al., 2006). Therefore, further investigation is warranted to explore the sex-specific relationships between neuromuscular and cardiovascular factors during computer work while pedaling at different intensities.
Sex-Specific Responses to Cycling Workstation
In the present study, time × sex interaction effects revealed that females (compared with males) had higher middle and lower trapezius, and lumbar erector spinae activation amplitudes during the beginning bouts of Bike-and-Type. Higher activity in those muscles is usually reflective of higher risk for upper and lower back pain. Similarly, higher risk of work-related upper and lower back pain in female weavers compared with males have been reported (Nag et al., 2010). Interestingly, these sex differences in lower trapezius and lumbar erector spinae activation levels disappeared with time, which may be due to the significant decrease in lower trapezius and lumbar erector spinae activations in females along with male’s significant increase in lumbar erector spinae activation. Thus, our results suggest that prolonged Bike-and-Type may lower these risk factors for upper and lower back pains in females, although this hypothesis could only be verified by longitudinal, prospective studies.
Middle trapezius activation level, however, was still significantly higher at every time bouts in females, but this difference between the sexes decreased over time which decreased from 2.6% MVC (minute-10 bout) to 1.9% MVC (minute-60 bout) difference between males and females. If the cycling workstation use was even more prolonged, similar to the length of a real occupational work, this sex differences in middle trapezius activation levels may have been even more minimized. Nevertheless, the middle trapezius helps stabilize the scapular and upper back regions, and has been shown to work in concert with the upper trapezius, more so in females compared with males (Johansen et al., 2013). Given the vulnerability of the upper Trapezius in females, these results may be important in preventing/managing computer-related upper/lower back MSD development in females.
Contrary to findings from Nag et al. (2010), it has also been reported that males suffer from lower back injuries more than females (Hooftman et al., 2009). Accordingly, we found that males had a significant increase in lumbar erector spinae muscle activation in the later bouts of Bike-and-Type (30 < 40, 50 min), while that of females decreased in the earlier bouts (10 > 20, 30 min). Hence, there seems to be a fatigue threshold with the cycling workstation where the healthy muscle activation response lasts up to 30 min. Previously, it has been shown that incorporating breaks between bouts of static posture can reduce subjective discomfort and fatigue of people working with traditional, seated computer workstations (Galinsky et al., 2007, Galinsky et al., 2000; Mclean et al., 2001). For future practical use, our results may be used to help identify work-to-rest periods during computer work with the cycling workstation. Based on our results, it is suggested that bouts of 30-min work followed by a rest period may be the way to optimize the use of a cycling workstation.
Limitations
Although the cycling workstation showed significant motor control response that can be viewed as injury-preventative, these results need to be compared with other modalities of computer work, particularly in the traditional sitting workstation, to fully investigate its practical benefits. Moreover, our computer task was not as complex or prolonged compared with a real working environment. For example, a real office work may involve computer typing and utilizing the mouse concurrently, in addition to accomplishing a more cognitively challenging task compared with copy and paste typing. Moreover, we used a session randomization approach, with the outcome that 66.7% of males, and 60% of females conducted their 25% HRR session in their session 2. This slight group difference may have affected our results, although, we believe, to a negligible amount. Finally, future studies with larger sample sizes could collect and analyze kinematics to determine the relationships between EMG changes, and other changes such as in kinematics and performance variables. Non-neutral posture is a known risk factor for work-related MSD (Mayer et al., 2012), and it is possible that subtle changes in kinematic characteristics such as trunk posture during the task may also moderate the observed effect on muscle activity. Further investigations are warranted to compare the different types of workstations in a more realistic working environment.
Conclusion
There are sex-specific risks to MSDs, and mobile workstations have been suggested to induce healthier muscular patterns. However, despite the increasing popularity of mobile workstations in the workplace, the impact of exercise intensity and its impact on males and females had previously not been investigated. Both sexes were impacted by the pedaling intensity, and our sex-specific temporal effects may be important to consider when implementing a cycling workstation in the workplace in order to prevent/manage muscle fatigue and MSDs. Studies of other, more prolonged mobile workstation tasks, and comparisons between other modalities of workstations are needed to determine the full extent of the benefits of mobile workstations towards musculoskeletal health.
Key Points
Muscle activity patterns of the upper body were dependent on sex and pedaling intensity during computer typing while cycling. The effect of different pedaling intensity wasmainly observed in females.
There were time-based changes that differed between the sexes. The neuromuscular fatigue symptoms seem to arise not until after 30 min of cycling workstation usage.
Our results should be considered when providing guidelines on time and intensity limits of cycling workstation dependent on the worker’s sex to prevent/manage MSD-related muscle activation patterns.
Supplemental Material
Online supplementary file 1 - Supplemental material for The Effect of Cycling While Typing on Patterns of Upper Body Muscle Activation
Supplemental material, Online supplementary file 1, for The Effect of Cycling While Typing on Patterns of Upper Body Muscle Activation by SangHoon Yoon, Thierry Lefrançois-Daignault and Julie N. Côté in Human Factors: The Journal of Human Factors and Ergonomics Society
Supplemental Material
Online supplementary file 2 - Supplemental material for The Effect of Cycling While Typing on Patterns of Upper Body Muscle Activation
Supplemental material, Online supplementary file 2, for The Effect of Cycling While Typing on Patterns of Upper Body Muscle Activation by SangHoon Yoon, Thierry Lefrançois-Daignault and Julie N. Côté in Human Factors: The Journal of Human Factors and Ergonomics Society
Footnotes
Acknowledgment
This work was supported by the Natural Sciences and Engineering Research Council of Canada (grant number RGPIN: 2015–05111).
Supplemental Material
The online supplemental material is available with the manuscript on the HF website.
Author Biographies
SangHoon Yoon is a MSc student in the Department of Kinesiology and Physical Education at McGill University in Montreal, Quebec, Canada. He received his BSc in Kinesiology (Honours) from McGill University in 2019.
Thierry Lefrançois-Daignault is a medical student at Université de Sherbrooke in Sherbrooke, Quebec, Canada. He received his BSc in Kinesiology (Honours) from McGill University in 2017.
Julie N. Côté is a professor and chair of the Department of Kinesiology and Physical Education at McGill University in Montreal, Quebec, Canada, and a regular member scientist of the Center for Interdisciplinary Research in Rehabilitation of Greater Montreal. She received her PhD in biomedical engineering from the University of Montreal in 2003.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.