
Abstract
Objective
Situation awareness (SA) refers to people’s perception and understanding of their dynamic environment. In primary care, reduced SA among physicians increases errors in clinical decision-making and, correspondingly, patients’ risk of experiencing adverse outcomes. Our objective was to understand the extent to which electronic health records (EHRs) support primary care physicians (PCPs)’ SA during clinical decision-making.
Method
We conducted a metanarrative review of papers in selected academic databases, including CINAHL and MEDLINE. Eligible studies included original peer-reviewed research published between January 2012 and August 2020 on PCP–EHR interactions. We iteratively queried, screened, and summarized literature focused on EHRs supporting PCPs’ clinical decision-making and care management for adults. Then, we mapped findings to an established SA framework to classify external factors (individual, task, and system) affecting PCPs’ levels of SA (1–Perception, 2–Comprehension, and 3–Projection) and identified SA barriers.
Results
From 1504 articles identified, we included and synthesized 19 studies. Study designs were largely noninterventional. Studies described EHR workflow misalignments, usability issues, and communication challenges. EHR information, including lab results and care plans, was characterized as incomplete, untimely, or irrelevant. Unmet information needs made it difficult for PCPs to obtain even basic SA, Level 1 SA. Prevalent barriers to PCPs developing SA with EHRs were errant mental models, attentional tunneling, and data overload.
Conclusion
Based on our review, EHRs do not support the development of higher levels of SA among PCPs. Review findings suggest SA-oriented design processes for health information technology could improve PCPs’ SA, satisfaction, and decision-making.
Background
Despite interventions such as patient-centered medical homes and electronic health records (EHRs), improvements in the quality and safety of primary care have not been consistently recognized (Beasley et al., 2020). As defined by the Institute of Medicine, primary care is “the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community” (Fiscella & McDaniel, 2018; Institute of Medicine, 1996). Primary care ranges from disease prevention to end-stage disease and palliative care; it encompasses acute care, chronic disease management, and all organ systems, age ranges, and genders (Institute of Medicine, 1996). Increasingly, primary care physicians (PCPs) are addressing multiple patient issues in one visit, averaging less than 20 min (Fiscella & McDaniel, 2018; Temte et al., 2020). Before, during, and after visits, there is a critical need for care coordination among the primary care team, including physicians, nurses, medical assistants, and clerks. Additionally, this coordination must extend to specialists, hospitals, and long-term care facilities (Beasley et al., 2020; Savoy et al., 2019). Without comprehensive, accessible, timely, and accurate patient information, PCPs cannot make decisions related to prevention, diagnosis, or treatment, which are needed to deliver high-quality care to patients (Beasley et al., 2011; Savoy et al., 2021).
EHRs often refer to a digital version of a patient’s paper chart and the associated health information systems (Office of the National Coordinator for Health Information Technology, 2019). EHRs can improve primary care decision-making and delivery by enhancing access to detailed patient information, ensuring more reliable communication between providers and care teams, and facilitating clinical decision support. Over 10 years after the Health Information Technology for Economic and Clinical Health (HITECH) Act aimed to improve the quality, safety, and efficiency of health care by promoting health information technology adoption, persistent issues of poor usability have limited EHRs’ expected benefits (Beasley et al., 2011; Howe et al., 2018; Roman et al., 2017; Sinsky et al., 2014). Usability is the extent to which a product or service can be used to achieve goals with effectiveness, efficiency, and satisfaction (International Organization for Standardization, 2018). In primary care practices, where EHR adoption has progressed rapidly since HITECH’s passage, negative unintended consequences are evident (Beasley et al., 2011; Colicchio et al., 2019; Eikey et al., 2019; Institute of Medicine, 2012; Zheng et al., 2016).
EHR user interfaces do not fully support the dynamics of primary care workflows, such as facilitating management of multiple problems per encounter, efficient EHR interactions, teamwork, and longitudinal care (Berg, 1999; Carter, 2015; Karsh et al., 2010; Rittenhouse et al., 2020; Sinsky et al., 2014; Zulman et al., 2016). Clinical information in EHRs is organized primarily for billing and other administrative management (Savoy et al., 2021). Reviewing patient history may involve navigating through multiple sections of the EHR (Roman et al., 2017) to find only partial answers, both increasing review time and lowering the likelihood of finding an answer (Aakre et al., 2019; Daei et al., 2020; Dwairy et al., 2011; González-González et al., 2007; Gorman, 1995; Gorman & Helfand, 1995). This increases PCPs’ cognitive workload and decreases their situation awareness (SA), defined as “the perception of the elements in the environment, the comprehension of their meaning, and the projection of their status in the near future” (Beasley et al., 2011; Endsley, 1988). A lack or loss of SA related to the perception of clinical findings, comprehension of patient condition, and projection of possible outcomes and treatments negatively impacts decision-making (Singh et al., 2006).
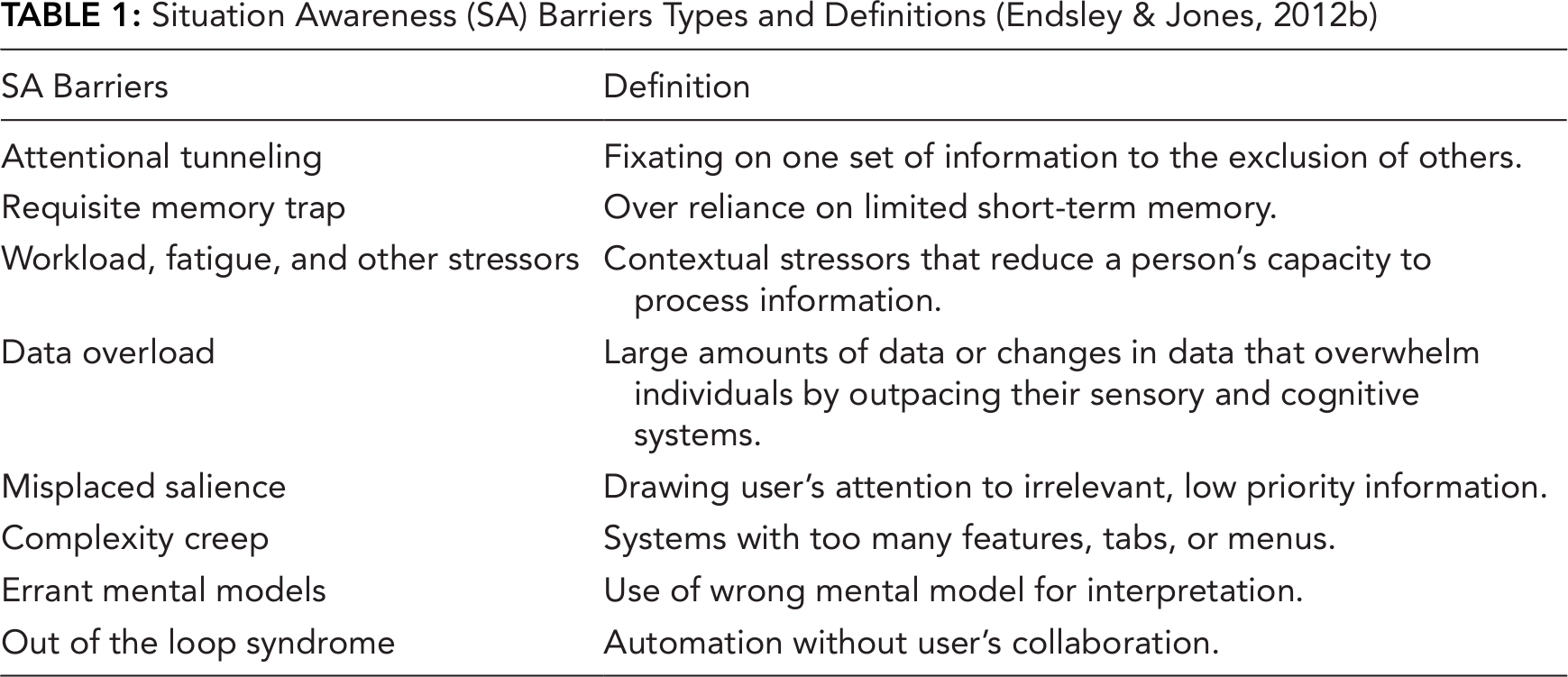
From aviation to health care, including anesthesiology, surgery, acute nursing, and emergency medicine, the SA framework has been used to understand both decision-making and errors (Gaba et al., 1995; Hazlehurst et al., 2007; Nibbelink & Brewer, 2018; Risser et al., 1999; Sitterding et al., 2012; Wauben et al., 2011; Wright et al., 2004). Using the SA framework, individual (e.g., goals and objectives, abilities, training, experience), task (e.g., stress and workload, complexity), and system (e.g., EHR capability and interface design) factors have been identified and analyzed to determine their impact on developing and maintaining SA (Endsley & Jones, 2012c). Previous analyses of clinical scenarios in primary care have demonstrated that decreased awareness impeded activities ranging from clinical problem identification to treatment planning (Beasley et al., 2011; Murphy et al., 2019; Powell et al., 2020; Singh et al., 2012). While EHRs are expected to provide information that PCPs need to support SA, usability issues have hindered PCP–EHR interactions, and these usability issues have the potential to foster SA barriers (i.e., often labeled “SA demons”; Table 1) that can increase medical errors (Beasley et al., 2011; Singh et al., 2012). There is little evidence demonstrating relationships among these PCP–EHR interactions and the development or maintenance of SA.
Situation Awareness (SA) Barriers Types and Definitions (Endsley & Jones, 2012b)
We aimed to understand how EHRs support PCPs’ SA by providing information needed to make clinical decisions and manage care for adult patients. Our long-term goal was to outline corresponding gaps in SA support that could be targeted by interventions.
Methods
To understand how EHRs support PCPs’ SA, we performed a systematic review and metanarrative analysis (Greenhalgh et al., 2005; Wong et al., 2013) using the SA framework. In contrast to meta-analyses, the metanarrative analysis enabled the inclusion of heterogenous (e.g., quantitative, qualitative, and mixed methods) studies to provide a comprehensive description of the current state of PCPs’ SA supported by EHRs. The metanarrative approach also permitted an open-ended and iterative approach to planning, searching, and synthesis of literature mapped to the SA framework (Greenhalgh et al., 2005; Stanton et al., 2017). SA concepts (e.g., information presentation and cognition) guided the systematic searching, screening, extraction and synthesis of the existing research (Figure A1).
Scoping and Searching
We used the SA framework to define the review’s scope, considering social dynamics of primary care and PCPs’ EHR interactions. We focused on common clinical decisions and tasks related to care management of adult patients that are often not supported by clinical decision support tools. For example, deciding whether to start palliative care, predicting quality of life and recovery time, and tracking progress toward patients’ stated goals are tasks for which clinical decision support tools do not exist. We systematically reviewed academic literature published between January 2012 and August 2020. By the end of 2011, initial findings related to HITECH’s implementation were published (Blumenthal, 2011). Thus, we chose 2012 as the starting year for our review. We included English-language manuscripts and standalone abstracts. Primary sources were the databases indexed by the metasearch product Primo (Ex Libris Group, 2020), including CINAHL, MEDLINE, PsycINFO, Web of Science, EBSCO, and ProQuest Central. Searches were simultaneous across these databases, and exact duplicates within a search were removed automatically.
A primary keyword search included situation awareness and primary care. To expand the search, two authors (AS, HP) built a compound query using related terms from the U.S. National Library of Medicine’s Medical Subject Headings. We tested and changed our search and screening processes iteratively. After estimating the relevance of results for each query, final queries included these terms: electronic health record, electronic medical record, patient record, electronic record, visuali*, interface, design, prototype, concept, dashboard, data display, requirements, information needs, information processing, primary care, healthcare, health care, situation* awareness, user-computer interface, presentation, salien*, usability, morae, and HCI.
Screening and Extraction
Search results were exported into reference management software (Center for History and New Media at George Mason University, 2013; Clarivate Analytics, 2016–2019). Four reviewers determined eligibility independently by working unblinded on separate subsets (205–217 articles per subset). Weekly meetings were held to review screening decisions. We included articles if their titles referred to primary or ambulatory care, or if the titles listed EHR tasks that may be performed in primary care (e.g., orders). We excluded articles based on abstracts. Types excluded were duplicate reporting (e.g., conference papers edited into journal papers), secondary work (e.g., position and review articles), and methods-oriented work (i.e., defining or reviewing protocols or metrics). Themes excluded were clinical decision support systems, migration from paper records, information needs from secondary uses of EHRs (i.e., not at the point of care), reminders used strictly as memory aids, decision support aids used strictly for prescribing, incidental (not central) findings about information needs, and usability evaluations of software interfaces that did not include information needs. The remaining papers were discussed in a consensus meeting with five reviewers (including AS). Then, two reviewers (AS, HP) reviewed the full-text of the included papers and extracted five elements: study focus, organization type, participants, analysis method, and results. In a series of consensus meetings, we excluded papers due to not reporting user attitudes (e.g., a software proof of concept), reporting only the needs of patients, or reporting needs in specialties other than primary care (Table A1).
To understand how EHRs support PCPs’ SA, review findings were mapped (Figure 1) to SA framework concepts (Endsley, 1995; Singh et al., 2012). Based on this framework, three types of factors can affect primary care SA. Individual factors include PCPs’ goals and objectives for clinical processes. Task factors include clinical tasks within a workflow to complete those processes. System factors include PCPs’ experiences using EHRs when completing those tasks.
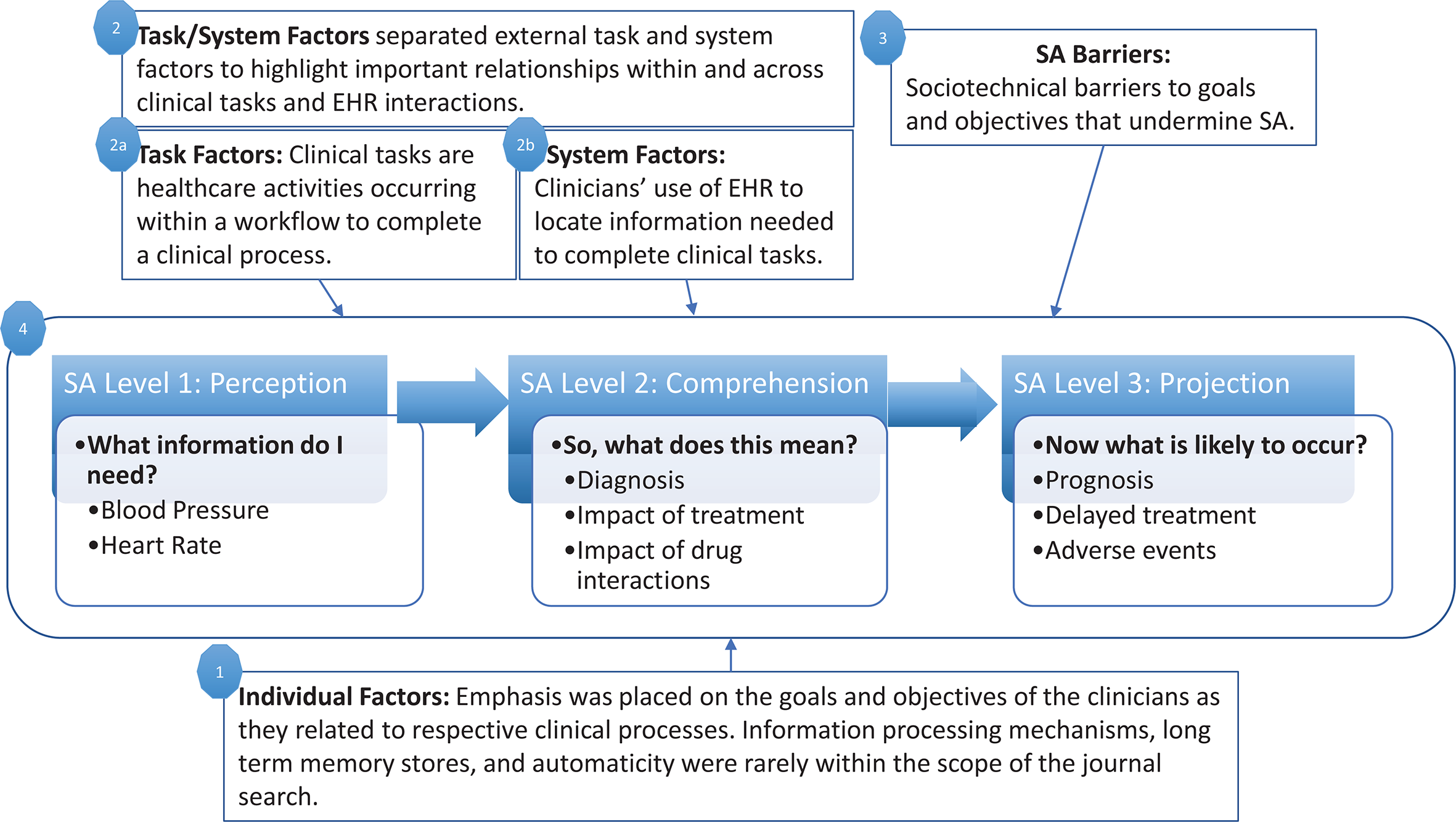
Adaptation of SA framework (Singh et al., 2012; Wright et al., 2004) that guided mapping of findings. SA = situation awareness.
Results
Search Findings
Our prepared and ad hoc searches identified 1504 unique papers (Figure 2). After applying our criteria iteratively to titles, abstracts, and full texts, 118 papers underwent review. In the majority of the studies that directly addressed SA, PCPs were not identified as primary stakeholders or users.
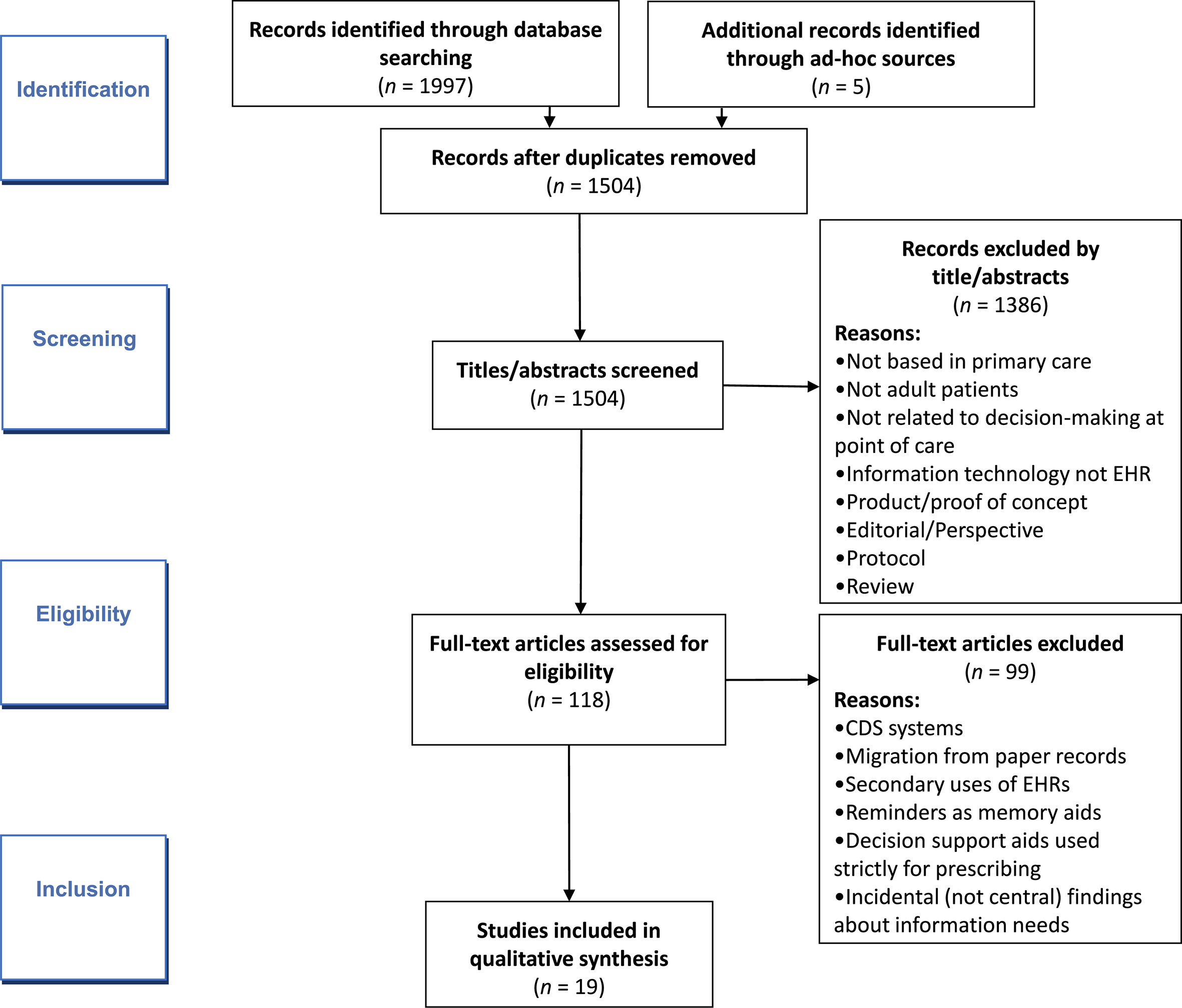
Document flow. * Criteria listed in methods section.
Overview of Studies
The resultant literature sample consisted of 19 papers published between 2012 and 2020 (Appendix 2). Twelve of the papers were published in medical informatics journals (Clarivate Analytics, 2021). Although different health care organization types were represented (educational, government, and community health care organizations), most of this diversity was between studies, not within them. Four studies were conducted across multiple health care networks (Flanagan et al., 2013; Harle et al., 2019; Pet et al., 2019; Robelia et al., 2017). Seventeen studies were descriptive or interpretive; only two (11%) were interventional (Belden et al., 2017; Del Fiol et al., 2016). Fourteen studies (74%) used interview- or focus group-based qualitative and exploratory methods, three involved surveys (Menon et al., 2016; Robelia et al., 2017; Singh et al., 2013), and two involved controlled evaluation (Belden et al., 2017; Clarke et al., 2014). Of 16 non-survey studies, 13 involved fewer than 30 participants.
Mapping to SA Framework
Figure 3 illustrates the synthesized review findings mapped to the components of the SA framework. Specific individual (goals of clinical processes), task (information requirements), and system (EHR interactions) factors that affect SA are listed. Major SA barriers identified are also represented.
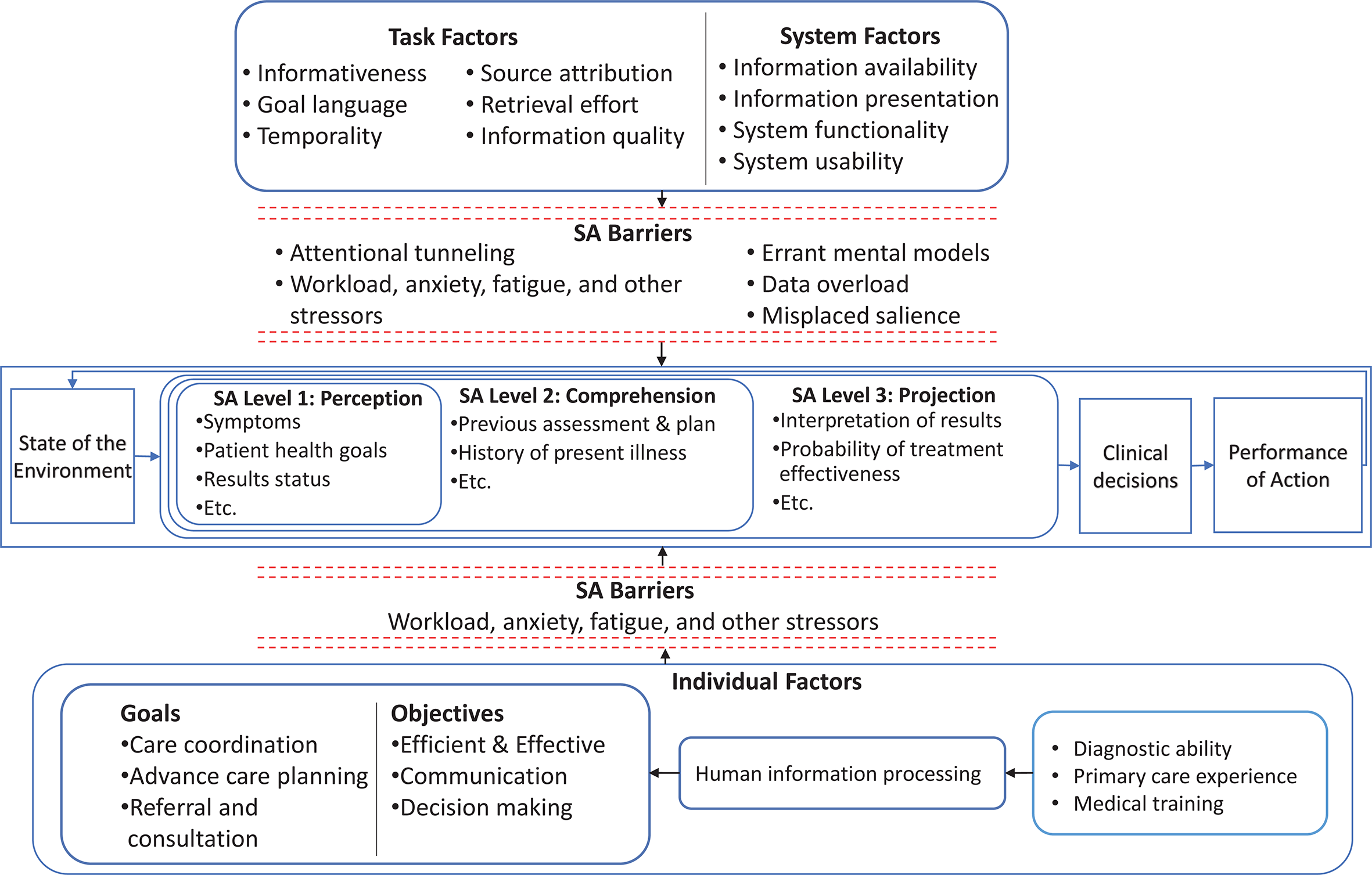
Summary of mapping to SA framework. This figure illustrates the synthesis of literature findings mapped to the components of the SA framework. SA barriers related to individual, task, and system factors are depicted with dashed-line barricades near the respective factors. SA = situation awareness.
In the following sections, we discuss PCPs’ information needs published in our literature sample and associated with levels of SA. Then, we discuss the individual, task, and system factors that affect SA and expound on the EHR’s impact on SA. Lastly, we discuss barriers to SA.
Information Needed From EHRs to Support Levels of SA for PCPs
Most studies focused on information needed to acquire the basic level of SA, SA Level 1 (Perception), and involved methods for gathering information from EHRs for review. Individual PCPs’ information needs included new symptoms, previous care plans (Singh et al., 2012; Wright et al., 2004), and changes in social determinants of health (Friedman et al., 2014; Koopman et al., 2015; Weir et al., 2015). Clinical teams’ information needs were driven by care transitions. Advanced levels of SA—Level 2 (Comprehension) and Level 3 (Projection)—were identified in 11 studies (Clarke et al., 2014; Friedman et al., 2014; Harle et al., 2019; Koopman et al., 2015; Menon et al., 2016; Pet et al., 2019; Robelia et al., 2017; Rogers et al., 2012; Rotenstein et al., 2016; Savoy et al., 2019; Weir et al., 2015). Achieving these advanced levels of SA is often based on the synthesis and interpretation of information gathered from the EHR and is important for clinical decision-making and care management. For example, PCPs needed previous assessment and plan documents (Clarke et al., 2014; Koopman et al., 2015) to better comprehend patients’ medical conditions and aid care coordination (SA Level 2). For SA Level 3, genomic labs (Pet et al., 2019) were the main reference of information considered for patient health projection or forecasting. Table 2 displays information needs specified across the studies and links them to the three SA Levels.
Information Needed From EHRs to Support PCPs and Their Teams’ Clinical Decision-Making, Organized by SA Level
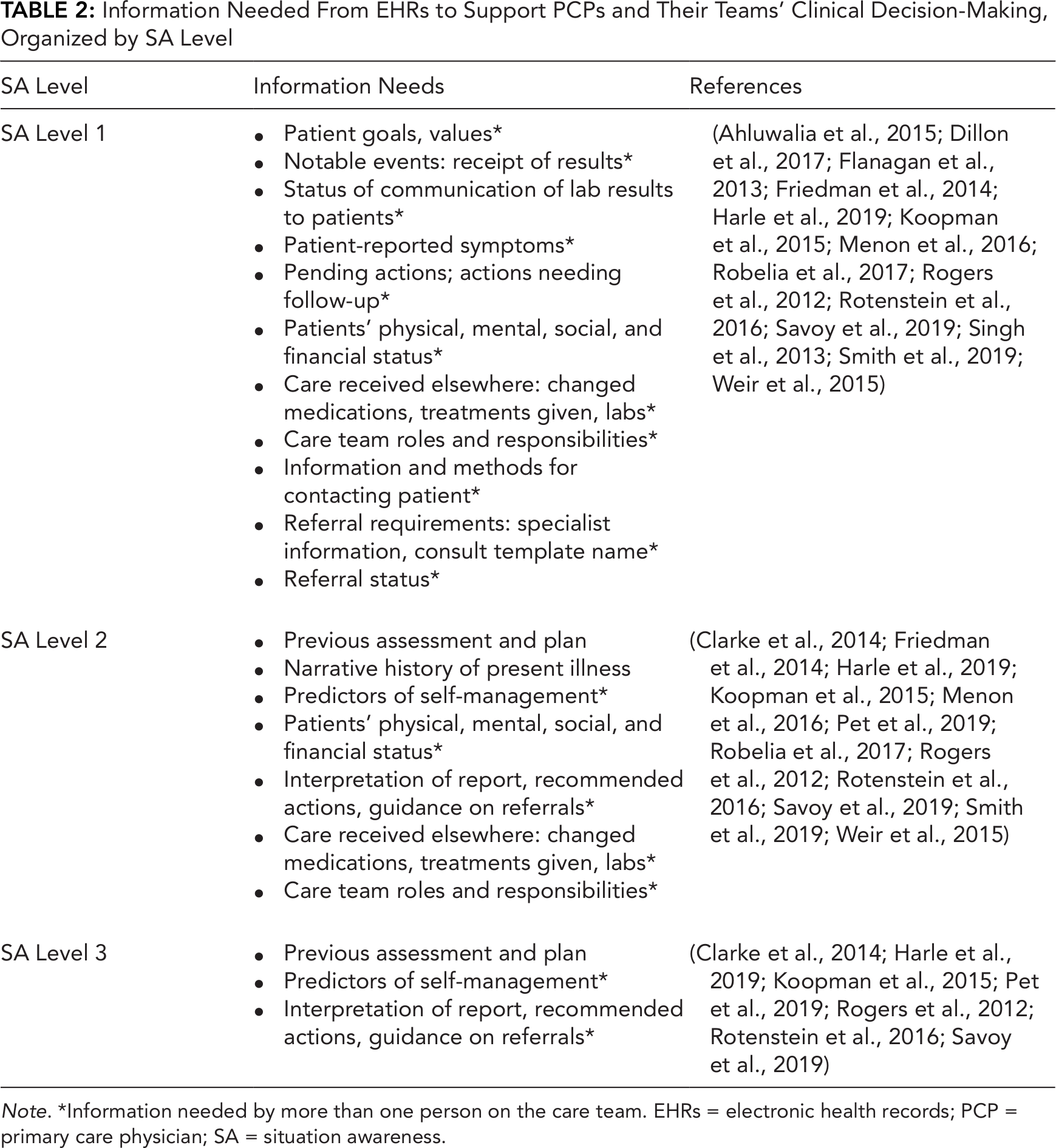
Note. *Information needed by more than one person on the care team. EHRs = electronic health records; PCP = primary care physician; SA = situation awareness.
PCP–EHR Interactions: Classification of Individual, Task, and System Factors That Affect SA
SA individual factors: Ineffective EHR-integrated clinical processes
Common goals for clinical processes included efficient communication and effective decision-making. These were classified as individual factors in SA because they shape the determination of important information. PCPs attempted to use the EHR to communicate and collaborate, relying on notes and alerts/notifications for information transfer, which would increase SA. However, findings across studies consistently indicated that EHRs were not effective tools for communication or collaborations (Ahluwalia et al., 2015; Flanagan et al., 2013; Koopman et al., 2015; Robelia et al., 2017; Rotenstein et al., 2016; Smith et al., 2019). Similarly, EHRs did not adequately support individual or team decision-making (Clarke et al., 2014; Harle et al., 2019; Koopman et al., 2015; Pet et al., 2019; Robelia et al., 2017; Weir et al., 2015). Contents of progress notes related to administrative reporting and metrics rather than information needed for clinical tasks and decision-making (Koopman et al., 2015). Insufficient information timeliness, quality, and access inhibited SA. Unmet information needs preceding a clinical decision were associated with medical errors (Singh et al., 2013). In an attempt to mitigate these medical errors, physicians across institutions established workarounds—actions addressing real or perceived limitations in technology (Cresswell et al., 2012)—in their clinical processes. Four papers described workarounds to EHRs, addressing SA Levels 1 and 2 (Flanagan et al., 2013; Friedman et al., 2014; Menon et al., 2016; Smith et al., 2019). EHR workarounds aimed to aid memory and increase awareness and efficiency (Flanagan et al., 2013; Smith et al., 2019). Decreased SA may have explained negative outcomes in care coordination (Clarke et al., 2014; Koopman et al., 2015), advance care planning (Ahluwalia et al., 2015; Dillon et al., 2017), and referrals (Harle et al., 2019; Savoy et al., 2019). For example, not knowing whether a specialty-care referral led to a consultation (Harle et al., 2019; Savoy et al., 2019) inhibited decision-making.
SA task factors: Inconsistent quality of EHR information
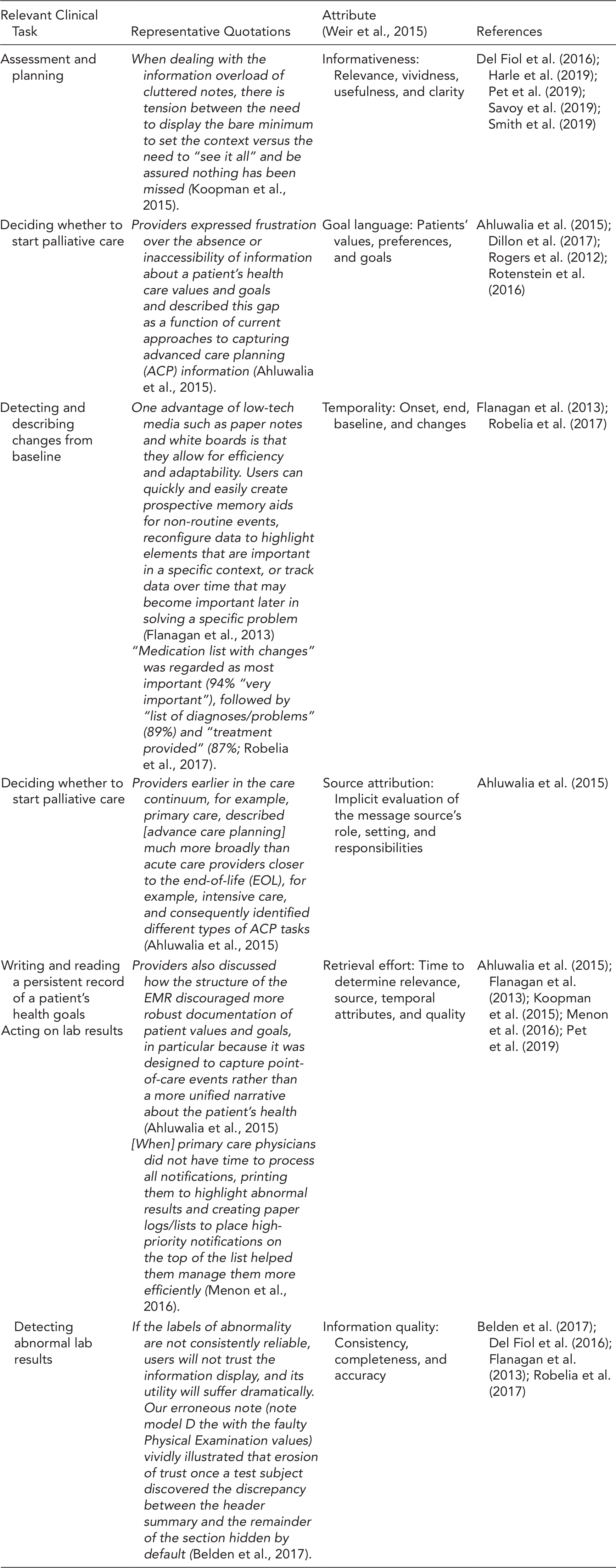
EHR information had attributes that positively or negatively affected PCPs’ SA and associated clinical tasks, decisions, or outcomes. With every clinical decision and task, PCPs regularly decided which information to pursue and use. Weir et al. (2015) identified six attributes of patient information—informativeness, goal language, temporality, source attribution, retrieval effort, and information quality—supporting a patient-centered medical home model of care (Table A4). We linked these attributes to clinical tasks done with the EHR across the studies. To achieve Level 1 SA, retrieval effort—time to determine the usefulness of information—was influential. This effort appeared to increase with case complexity, time since last visit, and EHR unavailability (Koopman et al., 2015; Singh et al., 2013). With this increase, it was harder for PCPs to gather and review recent notes and lab results. For Level 2 SA, temporality and information quality were vital for PCPs to identify a baseline status of interest and identify notable deviations or trends from that baseline (Belden et al., 2017; Del Fiol et al., 2016). This was particularly important for medication reconciliation (Robelia et al., 2017). For Level 3 SA, poor relevance, language, and quality of information caused issues with advanced care planning, which involved projection of outcomes and mapping of care concordant with accepted practices and with the patients’ preferences (Ahluwalia et al., 2015; Dillon et al., 2017).
SA system factors: Poor EHR usability
Although EHRs demonstrate increased usefulness over paper records, literature described poor EHR usability, identified negative experiences, or limited interventions. As a result, PCPs’ stress and workload increased, which decreases SA (Belden et al., 2017; Del Fiol et al., 2016; Flanagan et al., 2013; Friedman et al., 2014; Rotenstein et al., 2016).
PCPs’ experiences using EHRs included redundant interaction and information overload. Redundant interaction was described as repeated actions using one or more interfaces to complete a single task, including documenting information in multiple systems (Friedman et al., 2014). Related outcomes included increased time needed to review of patient records and clinical references (Del Fiol et al., 2016; Robelia et al., 2017), slower ordering of medication tapers (Friedman et al., 2014), and duplicated documentation (Friedman et al., 2014; Menon et al., 2016). Information overload was related to an inability to manipulate filters or sort EHR information. Tools to limit information overload via filtering, sorting, or querying remained unused (Singh et al., 2013). Outcomes associated with information overload included (1) increased time and effort for retrieval (Belden et al., 2017; Clarke et al., 2014; Koopman et al., 2015; Weir et al., 2015) and (2) increased difficulty in prioritizing information (Menon et al., 2016; Singh et al., 2013; Smith et al., 2019).
SA Barriers Present in PCP–EHR Interactions
Table 3 describes the link between social and technical (i.e., sociotechnical) and SA barriers. Social barriers to communication were related to ambiguities of physician expectations and responsibilities (Ahluwalia et al., 2015; Dillon et al., 2017; Smith et al., 2019). This ambiguity was amplified by the absence of messaging capabilities in EHRs, demonstrating errant mental models among EHR designers and care teams (Ahluwalia et al., 2015). Technical barriers to communication related to computing infrastructure and human–computer interfaces included EHR downtime (Flanagan et al., 2013), lack of interoperability among vendors limiting access to clinical information (Friedman et al., 2014), and inadequate support for managing notifications (Del Fiol et al., 2016; Menon et al., 2016; Singh et al., 2013; Smith et al., 2019). These were often associated with attentional tunneling, misplaced salience, and data overload, which decrease Level 1 SA. One illustration described the organization and presentation of progress notes (Belden et al., 2017; Clarke et al., 2014; Koopman et al., 2015), which facilitated billing and reimbursement more than building patient narratives (Ahluwalia et al., 2015; Clarke et al., 2014; Weir et al., 2015). Based on the literature sample, errant mental model, requisite memory trap, attention tunneling, and data overload were the most evident SA barriers.
Associations Among Sociotechnical Barriers and SA Barriers in Primary Care Medicine
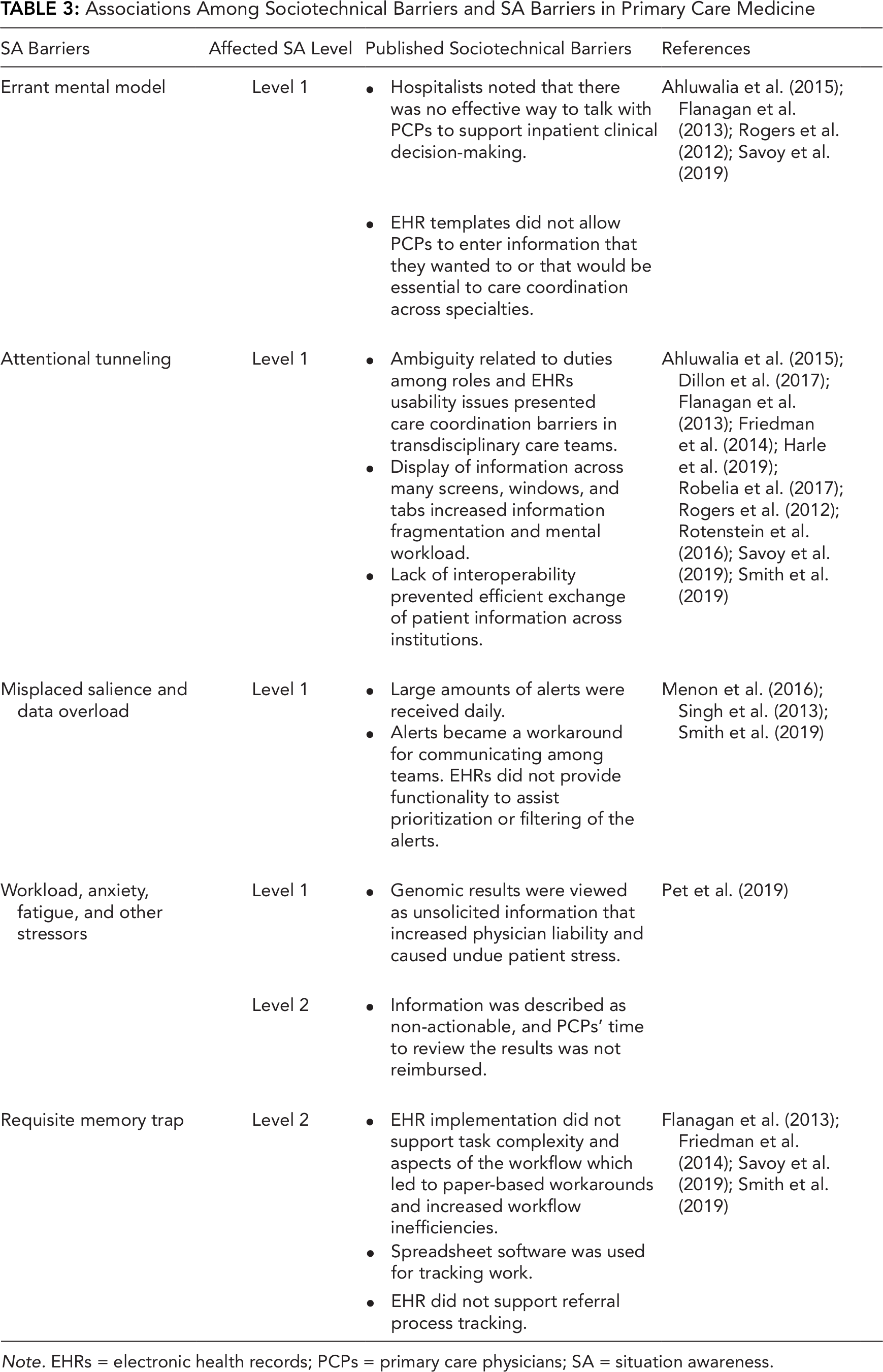
Note. EHRs = electronic health records; PCPs = primary care physicians; SA = situation awareness.
Discussion
The SA framework enabled us to analyze published findings using a systems approach that considered the combined effect of PCPs’ goals for clinical processes, information attributes required to complete clinical tasks, and usability requirements for physician–EHR interactions on PCPs’ SA. Based on our results, we discuss implications for SA in primary care and considerations for future research below.
Implications of SA in Primary Care
Finding patient events, lab values, and clinical status required redundant efforts and high mental workloads for PCPs and their teams. If perception of this information is hindering Level 1 SA, then higher levels of SA are not supported. With respect to the SA framework, existing research largely focuses on Level 1 SA. Our study suggests that there is a gap between PCP-pursued needs and EHR information and visualizations. EHRs are not capturing or presenting information in a manner that allow PCPs to efficiently use it in the context of their clinical workflow. More recently, technological workarounds and interventions are not integrated into the EHR and require PCPs to use additional user interfaces (e.g., Metke-Jimenez et al., 2019). Furthermore, there is a lack of focus on team SA, which is important given the widely adopted patient-centered medical home model in primary care. Without higher levels of SA, PCPs and their teams are prone to delayed action, inaction, or inappropriate action.
Requisite memory trap, attention tunneling, and data overload were the most common barriers examined. When EHRs are unable to support higher levels of SA and contain widespread SA barriers, PCPs are forced to create workarounds due to requisite memory traps, make decisions with limited information due to attention tunneling, or experience high levels of mental workload due to data overload. To build and maintain SA, researchers and designers need to ensure accurate mental models for PCPs, which guides their information interpretation. These models would inform aggregation of disparate elements of information to support comprehension and projections of patient conditions or treatment. Although PCPs’ expertise and workarounds resolve some sociotechnical barriers, there is tension between PCPs’ determination to care for patients and EHR issues. This makes health care delivery susceptible to medical errors, patients susceptible to safety risks, and providers susceptible to burnout (National Academy of Medicine, 2019). Clinical decision-making is forced to occur at the intersection of competing goals and priorities, high levels of uncertainty, and EHRs that do not support SA adequately.
From this review, major barriers for obtaining high levels of SA stemmed from errant mental models. These barriers persist when technology-centered designs are implemented rather than user-centered designs. When mental models are discussed, it is about the users of systems applying the wrong mental model for data perception. However, we propose another perspective of errant mental model, where EHR developers apply the wrong mental model. Major EHR vendors have challenges implementing a user-centered design process, and one of those challenges is their inability to conduct contextually rich studies of clinical workflow (Ratwani et al., 2015; Zheng et al., 2020). Additionally, communication breakdowns among interdisciplinary groups or research and practice contribute to errant mental models among EHR developers and the lack of successful user interfaces (Hettinger et al., 2021). These breakdowns invoked by ineffective deliverables have created difficulties in translating user requirements into implemented software features (Saleem et al., 2016).
Human Factors Approach to Improve EHRs’ Support of SA
Implementing a human factors approach for the (re)design of EHR user interfaces can improve PCP-EHR interactions. A recent review by Carayon and Hoonakker (2019) concluded that this approach positively affects not only the usability of systems but also the quality-of-care processes and outcomes. Based on our findings, the SA-oriented design process has the potential to improve EHRs’ ability to support higher levels of SA for PCPs. This particular human factors approach is a user-centered design process that consists of three main components: SA requirements analysis, SA design principles, and SA measurement and validation (Endsley & Jones, 2012a).
SA requirements analysis can be used to mitigate the knowledge gaps and ambiguity demonstrated across workflows in our literature sample. This type and similar analyses have been used to define the information needed for PCPs and supporting roles in healthcare teams for specific workflows or tasks (Militello et al., 2020; Savoy et al., 2019). For example, Savoy et al. (2019) described information needs for referring PCPs during the referral process. Their specification of distinct goals, tasks, and decision points throughout workflows identified information needs and how they shifted across decisions. Ostropolets et al. (2020) identified clinicians’ unmet information needs that arose from gaps in medical evidence to inform requirements for the design of future clinical decision support systems.
With these requirements, SA design principles (Endsley & Jones, 2012a) developed to combat the SA barriers identified by our metanarrative analysis can be applied to future EHR (re)designs. These SA design principles include general and specific guidelines to support higher levels of SA. For example, SA Design Principles 1 and 2 posit organizing EHR information based on PCPs’ goals (SA Design Principle 1) and directly presenting SA Level 2 information (SA Design Principle 2) to minimize demands on PCPs’ working memory. Emerging literature demonstrated the application of these and other human factors principles in the design of user interfaces for clinicians (Fischer et al., 2020; Harle et al., 2019; Savoy et al., 2018). For example, Fischer et al. (2020) used human factors design principles to create a visualization supporting decision-making about chronic diseases, increasing PCPs’ satisfaction.
Furthermore, SA measurement and validation provide feedback for iterative design and continuous improvement. Associated methods (e.g., SAGAT, SART, simulations, interviews, observations, rating scales) can be used before and after implementation of designs. Methods can also be adapted for remote and pragmatic evaluations to reduce potential PCP participation burden and provide evidence of impact on outcomes (Sauer et al., 2019; Woodward et al., 2020). For example, Woodward et al. (2020) used field observation and stakeholder input to inform the design of a neurosurgery referral system, which was put into practice; a pre-post implementation evaluation indicated the new system improved referral outcomes.
Limitations
This review has some limitations. Our primary keyword search was limited to academic publications published in English and indexed by commonly used databases, including MEDLINE and PsycINFO. In addition, we limited the review to PCP workflows and EHR interactions. Thus, we did not include articles with alternative methods of addressing SA, cognitive workload, or information needs. However, the combination of our search strategies helped to identify key literature with implications for SA in primary care. With a metanarrative approach, we could not define or calculate a standard effect. Additionally, our ability to assess the quality of each study was limited. As with other reviews, we denote the possibility of selective reporting and publication bias among individual papers.
Conclusion
Based on our review, current EHRs are unable to support the development of high levels of SA among PCPs. The SA framework advances our thinking about PCPs’ interaction with EHRs by considering the impact of social and technical factors on developing and maintaining SA needed to provide quality care. In various workflows, there are key barriers hindering PCPs’ development of Level 1 SA, upon which higher levels of SA depend. What information and how information is presented to PCPs through EHRs greatly influences SA and clinical decision-making. New research and implementation methods should be investigated to incorporate SA principles into health information technology design and evaluation to increase PCPs’ level of SA.
Key Points
With the SA framework, this metanarrative study advanced our understanding of PCPs’ interaction with EHRs and found that EHRs do not support the development of higher levels (Levels 2–3) of SA among PCPs.
Requisite memory traps, errant mental models, attention tunneling, and data overload were the most prevalent SA barriers present during PCP–EHR interactions.
Findings suggest that PCP decision-making is forced to occur at the intersection of competing goals and priorities, high levels of uncertainty, and EHRs that do not support SA adequately, which has negative implications for PCP mental workload and patient safety.
Based on our results, incorporation of SA-oriented design principles into future EHR and relevant health information technology design, development, and evaluation is recommended to increase PCPs’ level of SA.
Footnotes
Appendix 1. Review Steps
Appendix 2. Studies Included in Literature Sample
Clinical Tasks and Attributes of Related Information Needed to Support Point-of-Care Decisions in Primary Care
| Relevant Clinical Task | Representative Quotations | Attribute |
References |
|---|---|---|---|
| Assessment and planning | When dealing with the information overload of cluttered notes, there is tension between the need to display the bare minimum to set the context versus the need to “see it all” and be assured nothing has been missed (Koopman et al., 2015). | Informativeness: Relevance, vividness, usefulness, and clarity | Del Fiol et al. (2016); Harle et al. (2019); Pet et al. (2019); Savoy et al. (2019); Smith et al. (2019) |
| Deciding whether to start palliative care | Providers expressed frustration over the absence or inaccessibility of information about a patient’s health care values and goals and described this gap as a function of current approaches to capturing advanced care planning (ACP) information (Ahluwalia et al., 2015). | Goal language: Patients’ values, preferences, and goals | Ahluwalia et al. (2015); Dillon et al. (2017); Rogers et al. (2012); Rotenstein et al. (2016) |
| Detecting and describing changes from baseline | One advantage of low-tech media such as paper notes and white boards is that they allow for efficiency and adaptability. Users can quickly and easily create prospective memory aids for non-routine events, reconfigure data to highlight elements that are important in a specific context, or track data over time that may become important later in solving a specific problem (Flanagan et al., 2013) “Medication list with changes” was regarded as most important (94% “very important”), followed by “list of diagnoses/problems” (89%) and “treatment provided” (87%; Robelia et al., 2017). |
Temporality: Onset, end, baseline, and changes | Flanagan et al. (2013); Robelia et al. (2017) |
| Deciding whether to start palliative care | Providers earlier in the care continuum, for example, primary care, described [advance care planning] much more broadly than acute care providers closer to the end-of-life (EOL), for example, intensive care, and consequently identified different types of ACP tasks (Ahluwalia et al., 2015) | Source attribution: Implicit evaluation of the message source’s role, setting, and responsibilities | Ahluwalia et al. (2015) |
| Writing and reading a persistent record of a patient’s health goals Acting on lab results |
Providers also discussed how the structure of the EMR discouraged more robust documentation of patient values and goals, in particular because it was designed to capture point-of-care events rather than a more unified narrative about the patient’s health (Ahluwalia et al., 2015) [When] primary care physicians did not have time to process all notifications, printing them to highlight abnormal results and creating paper logs/lists to place high-priority notifications on the top of the list helped them manage them more efficiently (Menon et al., 2016). |
Retrieval effort: Time to determine relevance, source, temporal attributes, and quality | Ahluwalia et al. (2015); Flanagan et al. (2013); Koopman et al. (2015); Menon et al. (2016); Pet et al. (2019) |
| Detecting abnormal lab results | If the labels of abnormality are not consistently reliable, users will not trust the information display, and its utility will suffer dramatically. Our erroneous note (note model D the with the faulty Physical Examination values) vividly illustrated that erosion of trust once a test subject discovered the discrepancy between the header summary and the remainder of the section hidden by default (Belden et al., 2017). | Information quality: Consistency, completeness, and accuracy | Belden et al. (2017); Del Fiol et al. (2016); Flanagan et al. (2013); Robelia et al. (2017) |
Acknowledgments
Special thanks to our research team and student assistants, Zeba Kokan and Anna Mathew. This work was funded by the Human Factors Engineering Directorate in the Office of Health Informatics, U.S. Department of Veterans Affairs (VA), who helped define this work’s original scope. April Savoy and Himalaya Patel are supported in part by VA Health Services Research and Development (HSR&D) Center for Health Information and Communication (CIN 13–416). April Savoy is also supported in part by the following grants KL2TR002530 (A Carroll, PI), and UL1TR002529 (A. Shekhar, PI) from the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Sciences Award. Daniel Murphy, Ashley Meyer, and Hardeep Singh are supported in part by the Houston VA HSR&D Center for Innovations in Quality, Effectiveness and Safety (CIN 13–413). Additionally, Ashley Meyer is supported by a VA HSR&D Career Development Award (CDA 17–167).
Author Biographies
April Savoy is an assistant professor at Indiana University-Purdue University Indianapolis in the Purdue School of Engineering and Technology. She is a faculty investigator at the Regenstrief Institute and at the Center for Health Information and Communication at Richard L. Roudebush VA Medical Center in Indiana, where she also directs the Human Computer Interaction and Simulation Lab. She received her PhD in industrial engineering in 2008 from Purdue University.
Himalaya Patel is a researcher at the VA Health Services Research and Development Center for Health Information and Communication at Richard L. Roudebush VA Medical Center in Indianapolis, Indiana, where he manages the Human-Computer Interaction and Simulation Lab. He received his PhD in informatics in 2015 from Indiana University.
Daniel Murphy is the medical director and an assistant professor at Baylor College of Medicine in the Department of Medicine. He is an investigator at the Center for Innovations in Quality, Effectiveness and Safety at Michael E. DeBakey VA Medical Center. Dr. Murphy received his MD from the University of Miami School of Medicine in 2004. He received his MBA in 2006 from the University of Miami School of Business.
Ashley N. D. Meyer is an assistant professor at Baylor College of Medicine. She is a cognitive psychologist at the Center for Innovations in Quality, Effectiveness and Safety at Michael E. DeBakey VA Medical Center. Dr. Meyer co-directs the VA Patient Safety Center of Inquiry - Diagnosis Improvement Safety Center in Houston, Texas. She received her PhD in cognitive psychology/neuroscience in 2011 from Rice University.
Jennifer Herout is a program manager in the VA’s Office of Connected Care (OCC), where she oversees field testing prior to release of OCC tools. She received her PhD in industrial and systems engineering in 2008 from the University of Wisconsin.
Hardeep Singh is a professor at Baylor College of Medicine in the Department of Medicine. He is the chief of health policy, quality, and informatics program at the Center for Innovations in Quality, Effectiveness and Safety based at the Michael E. DeBakey VA Medical Center and Baylor. Dr. Singh received his MD in 1994 from All India Institute of Medical Sciences. He received his MPH in 2004 from Medical College of Wisconsin.