
Abstract
Objective
The strategies adopted by personal care attendants (PCAs) to deliver quality care when faced with challenges potentially impacting clinical outcomes were assessed using phenomenological methods.
Background
In Australia, recent outcry of unsatisfactory standards of care in residential facilities has instigated a national public inquiry. This study investigated how PCAs adapted to challenges in stressful and ambiguous everyday work scenarios to deliver quality care.
Method
A phenomenological approach was used to obtain insights into PCAs’ experiences, perceptions, opinions, and decision processes for enacting care. Ten PCAs working in rural-based residential aged care were interviewed using a novel scenario construction task with thematic and co-occurrence network mapping applied to derive insights.
Results
Seven themes were identified, revealing that participants formed close relationships with residents, influencing care provision but blurring personal boundaries. Key contextual factors in scenarios highlighted inadequate staffing and procedures, inadequate training, challenging residents, time poverty, and low support. Individually directed adaptive strategies were used to alleviate dissonance and maintain emotional resilience, including dynamic risk assessment involving rule breaking.
Conclusion
The findings suggest that in negotiating care delivery, PCAs strive to optimize rule-based compliance with safety, efficiency, and individualized attention to provide “good enough” care with fluidity. Implications for policy and practice are considered.
Application
Findings have implications for workforce development in the context of ever-increasing industry pressures. Findings identified challenging scenarios and role complexity, with decision-making occurring as a fluid and ongoing process across a flexible boundary of risk assessment influencing interactions between PCAs, registered nurses, and clients.
Keywords
Aged care is a growing context of healthcare. Personal care attendants (PCAs) in residential aged care routinely experience challenges related to safety culture, teamworking, communication, and tensions arising from compliance with policies and procedures, which impact care. This study examines how quality of care is maintained in residential aged care settings where interprofessional teamwork is tested by the industry’s ever-increasing demand for high-quality care.
In developed economies, more people achieve advanced ages relatively disease free, whereas others experience increased disability, chronicity, and frailty (Radford et al., 2015), requiring long-term residential care (Hugo, 2007; Winkler et al., 2006). High demand for residential aged care services has a corresponding demand for high-quality care, delivered in a regulated system and provided by skilled aged care workers.
The Australian aged care industry is government regulated with facilities accredited against standards of practice for quality of care, user rights, and accountability (Commonwealth of Australia, 2019). Facilities are government subsidized and may operate as for profit (34%), not for profit (charitable or religious based: 58%), or government owned (7%; Mavromaras et al., 2017), influencing workforce culture and ethos of care (Colón-Emeric et al., 2010).
Typical residents have higher levels of clinical acuity and frailty arising from complex medical needs including comorbid chronic conditions (Jeon et al., 2019), complicated by more than half of residents experiencing dementia and associated behaviors (Australian Productivity Commission, 2011). Residents are increasingly of multicultural backgrounds (Xiao et al., 2020), with predictions that by 2026, about one-quarter of aged care residents will be culturally and linguistically diverse (Gibson et al., 2001).
PCAs form an integral part of the aged care system, providing 80%–90% of direct care (Anderson et al., 2005) through delegation from the supervising registered nurse (RN). PCAs either follow their job descriptions by complying with rules or are encouraged to adopt a scope of practice approach focused on achieving quality resident outcomes (Corazzini et al., 2010). Due to their limited clinical knowledge, PCAs rely on their life experience by developing mental models of good care. Anderson et al. (2005) found PCAs’ practice is guided by the “golden rule” (p. 1011)—to treat others (residents) as they would like to be treated themselves, and through “mother wit” (p. 1011)—the wisdom accumulated through caring for their own children as a primary source of caregiving. These limited perceptions of quality care hinder learning and capability to detect and respond to significant health outcomes including pain, depression, infection, and challenging behaviors. Discordance between rules and applying caring wisdom to achieve quality outcomes for the resident also leads to PCA rule breaking to achieve individualized care (Kontos et al., 2011).
PCAs derive self-worth and satisfaction through personalized resident relationships, increasing motivation to care despite organizational structures that devalue their work (Pfefferle & Weinberg, 2008). The meaningfulness of doing “good work” buffers the inevitable stress and dissatisfaction that the physical and emotional demands of low status care work impose (Gao et al., 2015).
In Australia, PCAs undertake vocational tertiary education over 6 months, including 120 hr of practical placement to gain certification for aged care (Baldwin et al., 2014; King, Wei, et al., 2013). PCAs provide the majority of fundamental care, and although most PCA time involves interacting with residents, the role is loosely coupled with RNs who act as supervisors (Gao et al., 2014; Tuckett, 2007). This can create situations where PCAs feel low control (King, Mavromaras, et al., 2013) and a division of labor rendering RNs as “gate keepers” of information, influencing an “institutional division of disclosure” (Tuckett, 2007, p. 11). This is one reason why PCAs may disagree with decisions of care, but disagreements may also stem from managing two sets of relationships—one with the employer through the RN, and another with the client, illustrating competing logics of care: managerialism versus personalized care (King, 2012). Dealing directly with difficult scenarios (e.g., residents’ challenging behaviors) may intensify these feelings (Phillips et al., 2008), leading PCAs to feel their care quality is inadequate.
Delivery of care occurs across work units, demanding coordination to optimize performance (Runciman & Walton, 2007). The system has responded by increasing bureaucratization and governmentality (Sumner & Townsend-Rocchiccioli, 2003). While rules are effective for training and managing routine, predictable situations, the aged care workplace is growing increasingly complex (Fennell & Adams, 2011), and PCAs must acquire skill in applying procedures and adapting to novel events. In healthcare, this concept has been described as flexible boundaries (O’Keeffe et al., 2015) where quality care is delivered through risk assessment involving adaptation of safety rules (Figure 1). Engaging with safety rules to balance known risks with uncertainty may instill feelings of greater decision-making autonomy and job satisfaction while achieving clinical outcomes and quality care. As PCA work involves making practical decisions about safety, the application of a flexible boundary to manage resident welfare is likely to address perceived imbalances in the system to optimize decisions and deal with challenges (O’Keeffe et al., 2015; Petriwskyj et al., 2015). The paucity of human factors research on PCAs requires investigation with a methodology that yields concrete and first-hand examples of using strategies to break institutional rules that adapt/respond to risk.
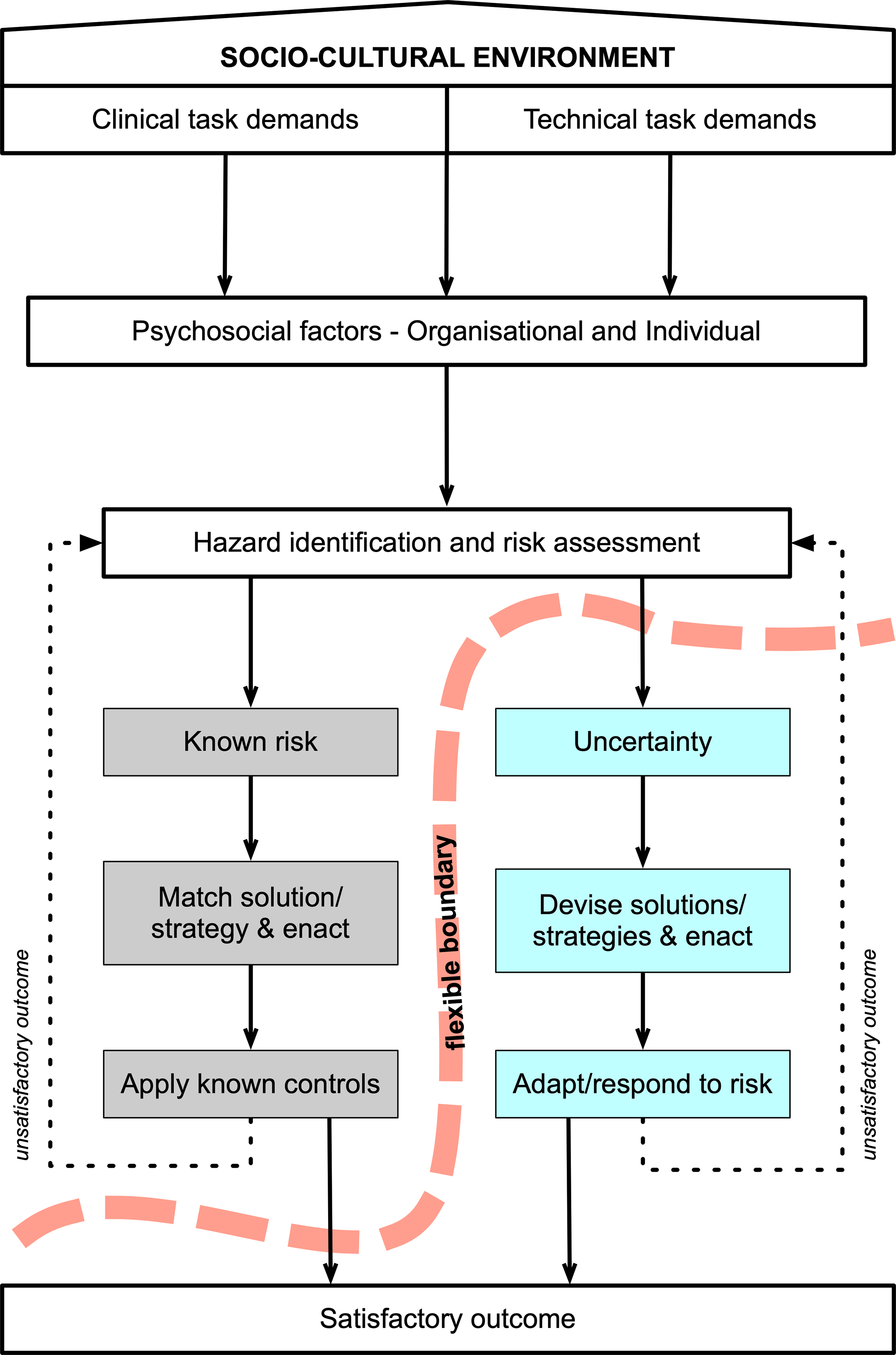
Theoretical notion of the flexible boundary of risk assessment (adapted from O’Keeffe et al., 2015).
The Phenomenological Approach and Scenario Invention Task Technique
A phenomenological approach (Creswell, 2013) was chosen for this study. The goal of phenomenology is to describe the meaning of the lived experience of a phenomenon and, therefore, is in contrast with other qualitative methods such as grounded theory (goal to develop an explanatory theory of social processes) or discourse analysis (goal to understand how language is used to create and enact identities and activities; Starks et al., 2007). As an interpretive approach, phenomenology allows us to investigate the “structures of consciousness as experienced from the first-person point of view” (Smith, 2006), and to “see the inherent logic of human experience and to articulate that logic or sense faithfully [and] without distortion” (Dukes, 1984). This allows the capture of collective real-life experiences across different individuals (Hammarberg et al., 2016), and helps form an accurate understanding of the essence (Moustakas, 1994) that is, what PCAs share as common experiences when trying to maintain quality care in challenging residential aged care scenarios. Uncovering these experiences is expected to also uncover the strategies used to enact care and adapt/respond to risk. To this end, using phenomenology allowed us to obtain rich, substantive insights into the decision processes, perceptions, and opinions of PCAs as a social unit (Cane et al., 2010; Curry et al., 2009; Ferroff et al., 2012), using interviewing as the key technique.
Grounded in human factors principles, the Scenario Invention Task Technique (SITT) enables an understanding about how people engage with work and involves participants creatively generating challenging work-specific stories (Naweed, 2015). Participants invent challenging scenarios that encourage transitions from analytical and creative thinking through to systems thinking processes (Checkland, 1980) that is, holistic perceptions and consideration of changes over time, when answering questions. The SITT has been applied to safety-critical work in rail (Filtness & Naweed, 2017; Naweed & Rainbird, 2015; Naweed, 2013; Roth et al., 2020), aviation (Naweed & Kingshott, 2019; Naweed & Kourousis, 2020), and tourism (Pabel et al., 2020; Reynolds et al., 2021), and has also been used to explore teamwork (Naweed, 2020).
In this study, participants created challenging scenarios based on their experiences, and then shared strategies they would apply to overcome these challenges to deliver quality care with a satisfactory outcome (Figure 1). This method enabled access to first-hand accounts of experiences, unpacking the phenomenon of adapting to risk. Investigating how PCAs understand, experience, but also maintain quality care despite challenges is paramount for identifying how care quality may be achieved. This research inquiry aimed to identify and explore the implications of strategies adopted by PCAs when responding to challenges to delivering quality care.
Methods
Sample
PCAs were recruited using convenience sampling based on experiences and willingness to participate. Inclusion criteria were (1) current employment as PCA, (2) minimum experience of one year, and (3) employed in residential aged care. Recruitment occurred via a specifically created Facebook page shared within social media outlets to maximize exposure. Consistent with recommendations for phenomenological studies (e.g., Creswell, 2013; Dukes, 1984; Riemen, 1986), 10 participants was the target sample size. Compared with other qualitative methods, a moderate sample size does not limit phenomenological research and in this case, fell within the “4–12 people” range supported by Creswell (2020). The SITT has also been applied successfully with this range (e.g., Naweed & Kingshott, 2019).
Participants
Seven females and three males (N = 10) participated in the study, all working in rural/regional residential aged care facilities in New South Wales, Australia. Despite being a convenience sample, most (n = 7) possessed over 10 years’ experience (Mexp = 11.7; SD = 5.27).
Procedure
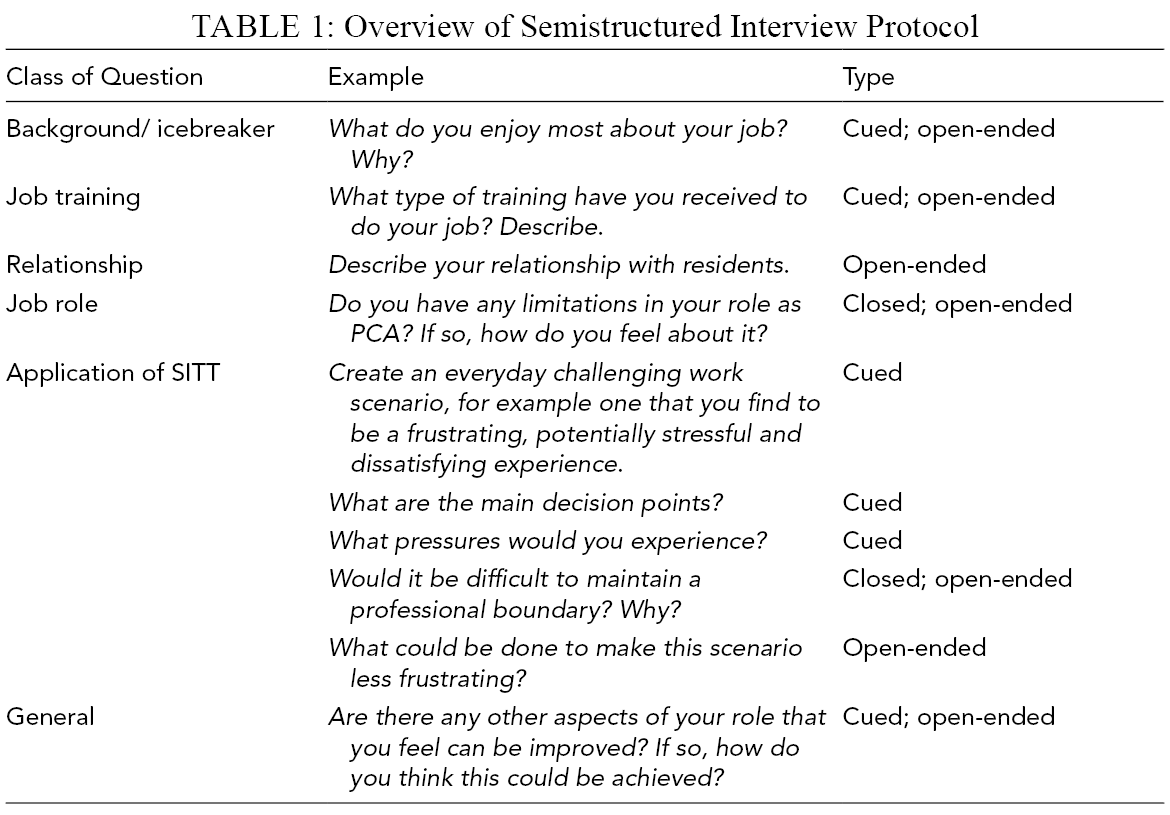
All interviews were performed face to face and ranged from 60 to 90 min. Three types of questions were asked to structure responses (Table 1). All data were collected in New South Wales, Australia.
Overview of Semistructured Interview Protocol
“Stand by” scenarios developed through piloting were applied if participants had difficulty performing the exercise (Table 2).
Narrative Descriptions of the Two Preprepared Hypothetical Scenarios Based on Their Potential as Everyday Encounters
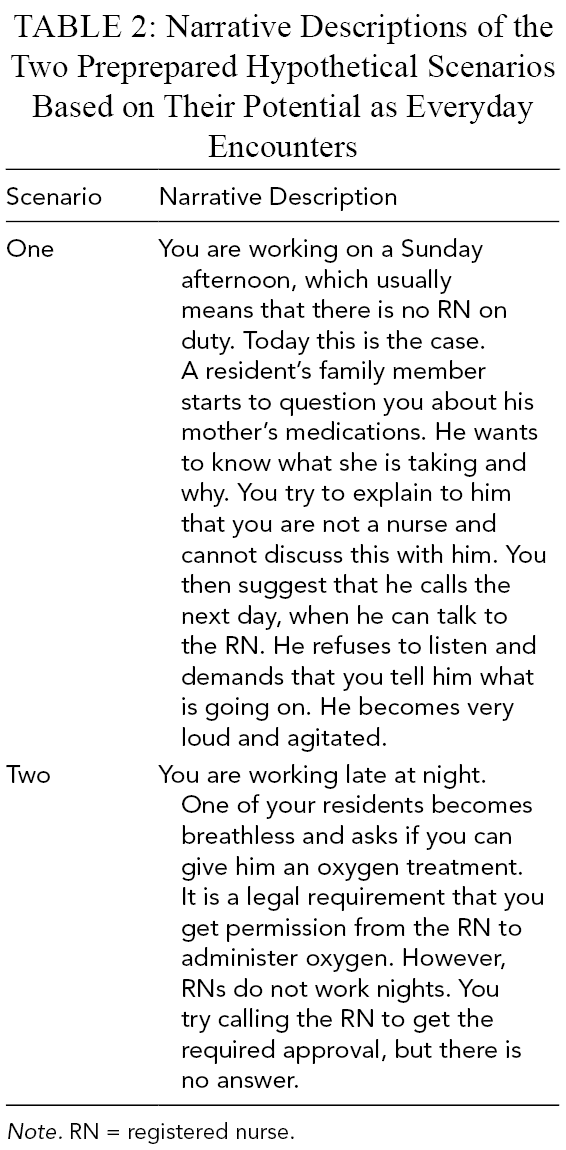
Note. RN = registered nurse.
Research Team
The research team comprised three investigators, one male and two females. Two were senior university researchers with human factors expertise, and one had worked previously in healthcare. The third member was undertaking an undergraduate psychology program and was also a qualified PCA. In line with the phenomenological approach (Creswell (2013, 2020), all three researchers discussed their assumptions and biases on the research topic. Analysis and writing were carried out predominantly by the senior researcher with no PCA or healthcare experience.
Ethical Considerations
Ethical concerns of competency and vulnerability were addressed by ensuring that participants could provide informed consent. The PCA-qualified research member ensured that participants did not feel coerced. Pseudonyms were created to preserve confidentiality and anonymity. This research complied with the American Psychological Association Code of Ethics and was approved by the Human Research in Ethics Committee at Central Queensland University (Approval no. H15/09-215). Informed consent was obtained from each participant.
Data Analysis
Two data types were analyzed in this study: (1) scenario-specific data from applying the SITT; and (2) general interview data, elicited to support greater understanding of the PCA role. Both were analyzed using the procedures of phenomenology described by Creswell (2013, 2020). Consistent with its focus on eliciting an idiographic interpretation of an experience (rather than an objective record), data gathering led to a focused analysis of textual descriptions (i.e., “what happened”) and structural descriptions (i.e., “in what context it happened”). This developed an understanding of the common experiences across scenarios by reflecting on the essential themes and the essence of the experience. The phenomenon was described by assembling and reducing the information to significant quotes and combining them into themes. Specifically, analysis was undertaken over five steps:
Each transcript was read to obtain the general meaning and listed every expression relevant to the experience;
Invariant constituents of data were found by reducing and eliminating overlapping significant statements and meaning units were made. In this step, scenario-specific data were categorized in terms of trends, patterns, and frequencies to promote links between textual and structural descriptions. This included extraction of scenario context and strategies used to maintain quality care.
Meaning units were clustered and developed into themes. These were verified for their essential or imaginative nature by checking if the phenomenon was the same if a certain theme was changed or deleted.
Themes were then arranged into a composite textual description focusing on “what” was experienced and the structural qualities of the experience were integrated into a universal structural description considering the context of each experience.
Finally, a composite description of the essence of the experience was developed, representing the group overall. The process resulted in a set of seven themes and 36 meaning units.
Analysis in all stages was undertaken with the assistance of CMapTools (ver. 6.01.01), aiding visualization of scenario data (Cañas et al., 2003).
Trustworthiness and Rigor
Rigor and trustworthiness were assured with credibility, applicability, and consistency as key criteria (Hammarberg et al., 2016). The protocol was piloted with three PCAs, during which time stand-by scenarios were created. The SITT facilitated data triangulation, allowing the research question to be answered, supported by verbatim quotes with pseudonyms protecting identity. The sampling strategy was adopted to obtain maximum insight and promote applicability. Scenario construction built rapport and trust, and the process itself facilitated member checks allowing scenario verification “in situ.” Data were collected and analyzed reflexively; involvement of a qualified PCA member ensured dependability, and the team remained critically aware of their role as research instruments, having to set aside their own views and experiences (Creswell, 2013).
Results and Discussion
Nine scenarios were generated—a standby scenario (Scenario 1 in Table 2) was used to stage discussion for one participant. Table 3 provides exemplars from the narrative descriptions of three scenarios obtained from participants.
Exemplars of Participant Scenarios
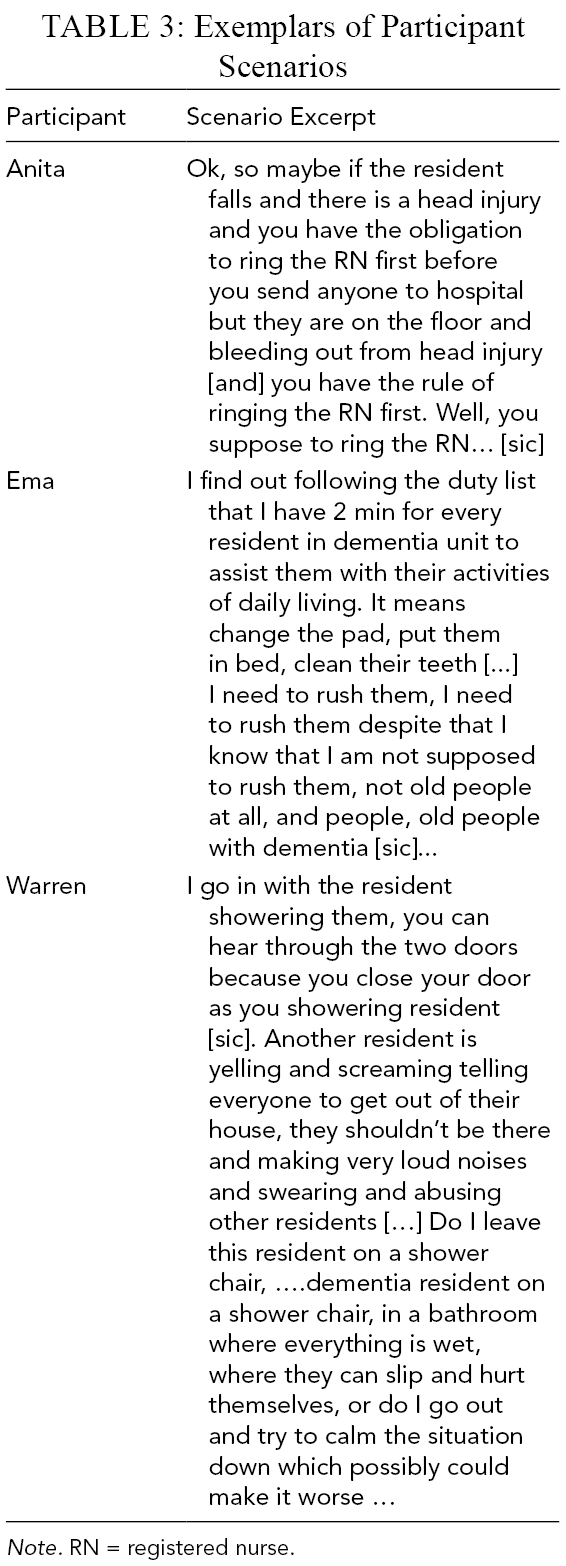
Note. RN = registered nurse.
Meaning units were constructed into a set of themes, structural and textural descriptions, and an essence. The themes and meaning units are presented in Table 4. The structure of the experience can be understood as “what happened” surrounding the central experience of adapting to risk when delivering quality care. The following seven themes emerged: like one of the family, “tender loving care” (TLC), against the clock, navigating (in)flexible boundaries, there’s no “I” in “team,” self-directed strategies for enacting quality care, and context matters. The following sections report the results using excerpts from data in tables.
Emerging Themes and Corresponding Meaning Units
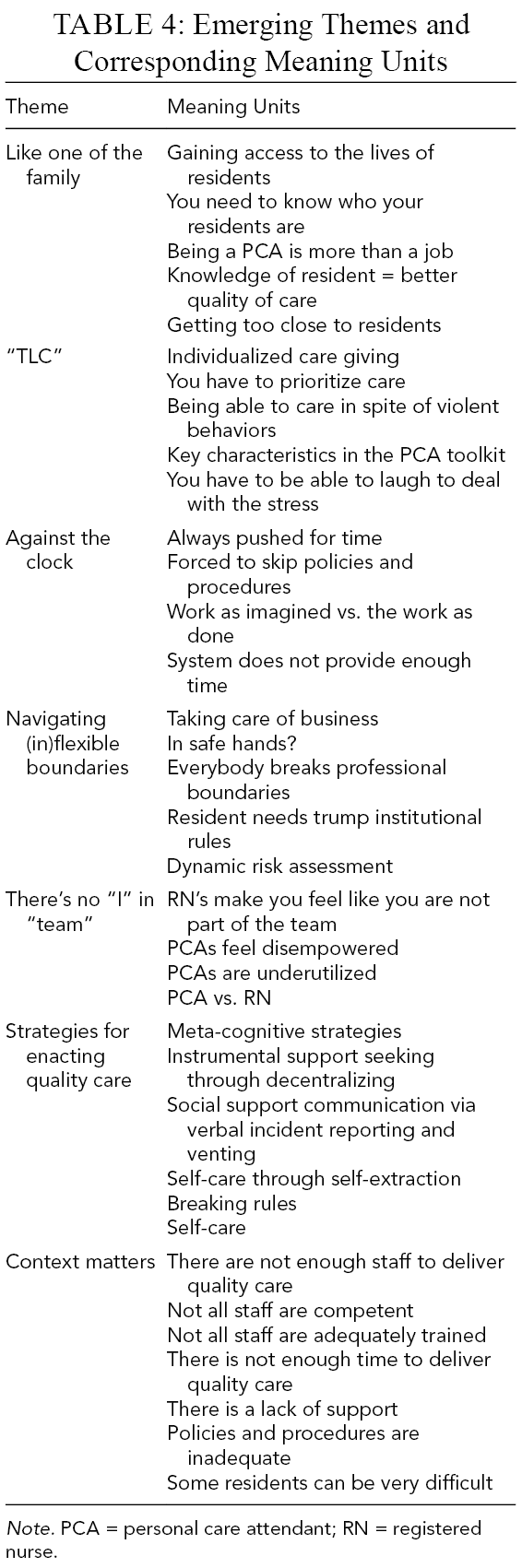
Note. PCA = personal care attendant; RN = registered nurse.
Like One of the Family
Table 5 presents excerpts from the theme “Like one of the family.” Relationship building with residents was considered the most important aspect of care and gaining access to residents’ lives was enjoyable and rewarding (Table 5, #1–2). To develop relationships, PCAs felt they needed to know their residents, describing some as like family (Table 5, #3–5). One participant countered this view, suggesting that whilst developing relationships with residents was important, treating them as family was risky (Table 5, #6). Most indicated that quality of care correlated positively with knowledge of the resident, in terms of friendship and personality (Table 5, #7–8). Some felt that at times, their relationships were too close (Table 5, #9–10).
Excerpts From the Emergent Theme “Like One of the Family”
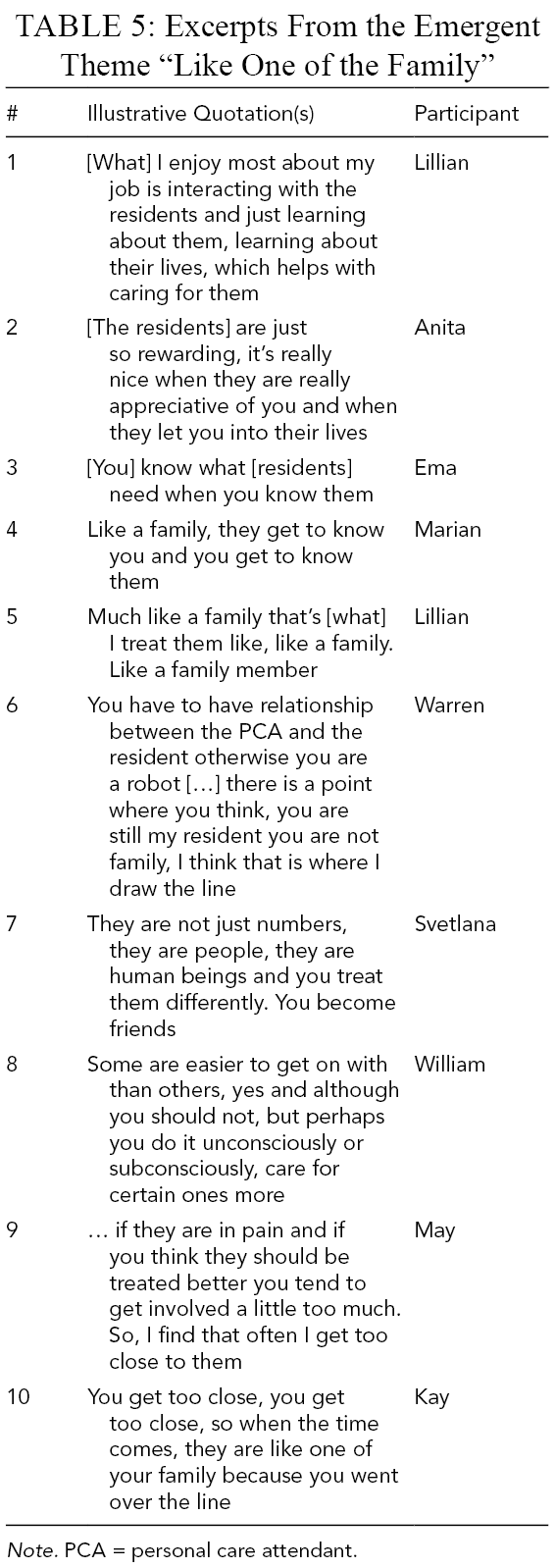
Note. PCA = personal care attendant.
“TLC”
Table 6 presents excerpts from the theme “TLC” (“tender, loving care,” a slang term to convey compassionate, caring, protective attention or treatment). Providing individualized care and advocating for residents were overriding objectives and achieving these fostered a sense of fulfillment (Table 6, #1–3) despite difficult and stressful resident behavior (Table 6, #4–5). Qualities considered important by PCAs included empathy, love, compassion, patience (Table 6, #6–8), and a sense of humor (Table 6, #9), reflecting their desire to provide quality care, despite the challenges.
Supportive Excerpts From the Emergent Theme “TLC”
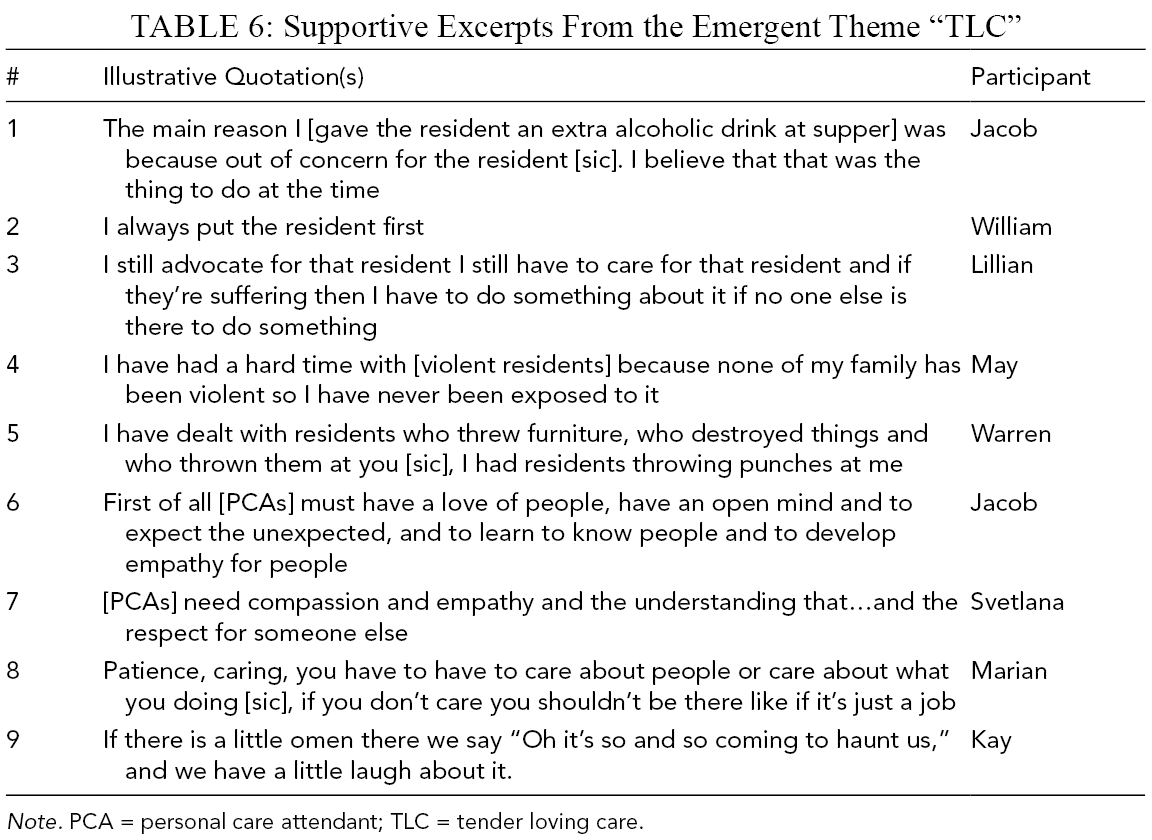
Note. PCA = personal care attendant; TLC = tender loving care.
Against the Clock
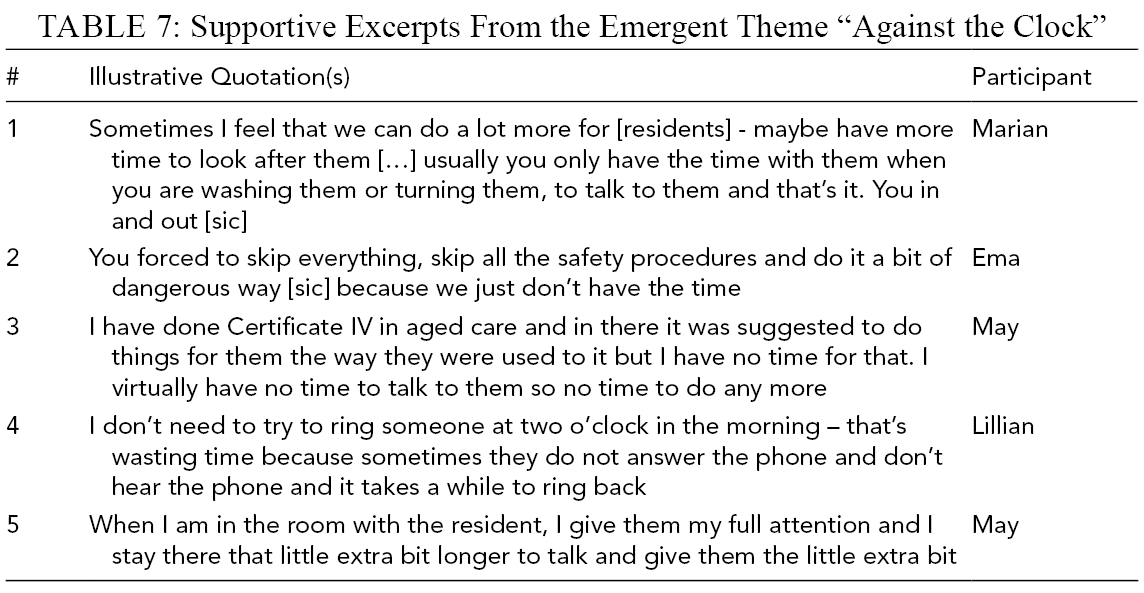
Table 7 presents excerpts from the theme “Against the clock.” Time poverty was considered a key barrier to implementing quality care (Table 7, #1), competing with safety rules (Table 7, #2), and not necessarily matching theory learned during certification training (Table 7, #3). Time poverty was exacerbated by entrenched organizational policies and procedures, for example, contacting an “on-call” RN for permission to follow a time-critical course of action could mean further delay (Table 7, #4). Provision of quality care was also described through awareness of a time budget (Table 7, #5).
Supportive Excerpts From the Emergent Theme “Against the Clock”
Navigating (In)flexible Boundaries
Table 8 presents excerpts from the theme “Navigating (in)flexible boundaries.” All felt boundaries and limitations were necessary and an inescapable part of their work (Table 8, #1–2). Nonetheless, all conveyed frustration at their inability to decide and act to benefit the resident, including doubts about what decisions they could make (Table 8, #3). All participants indicated that they routinely transgressed professional boundaries, did not comply with rules, or stretched the scope of their role. Participants who promoted the importance of such boundaries still placed residents’ needs above institutional rules if they felt it equated with achieving quality care (Table 8, #4–7). Going beyond the role in scenarios was justified with reference to social norms and through reconciliation of conflicts and dilemmas of doing things right (i.e., following rules) versus doing the right thing (i.e., ensuring the best interests of the residents; Table 8, #8–10).
Supportive Excerpts From the Emergent Theme “Navigating (In)flexible Boundaries”
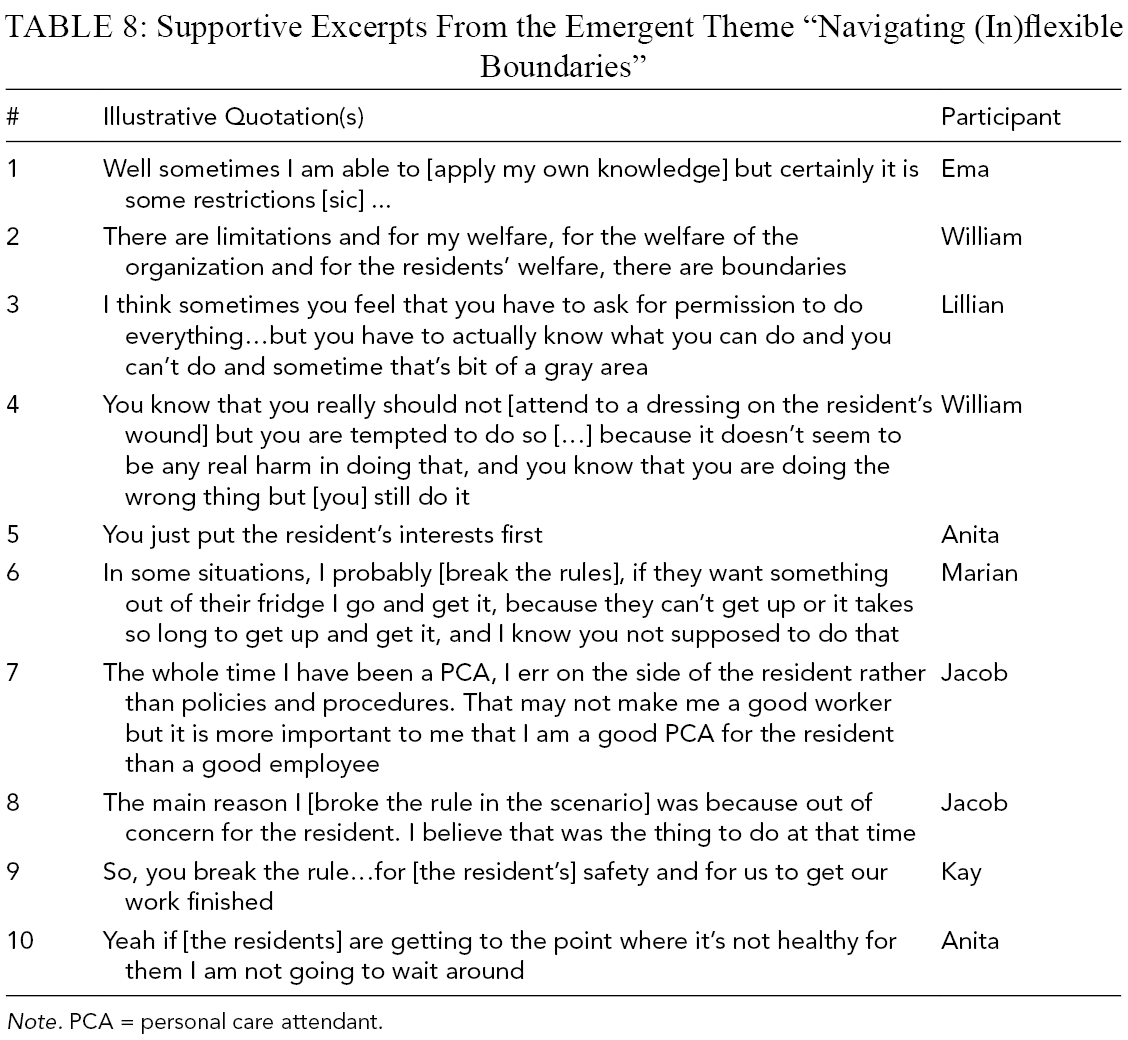
Note. PCA = personal care attendant.
There’s No “I” in “Team”
Table 9 presents excerpts from the theme “There's no ‘I’ in ‘team’.” All participants believed their knowledge of residents was superior to the RN due to the time spent with residents. Participants felt frustrated that their own expertise, views, and ideas were not respected (Table 9, #1–3). This was emphasized in scenarios like palliative care (Table 9, #4). Participants also expressed a desire for greater control and decision-making capacity, especially in emergency or stressful situations. In some cases, this desire was altruistic in that they were helping the RN or sharing workload (Table 9, #5–6).
Supportive Excerpts From the Emergent Theme “There’s No ‘I’ in ‘Team’”
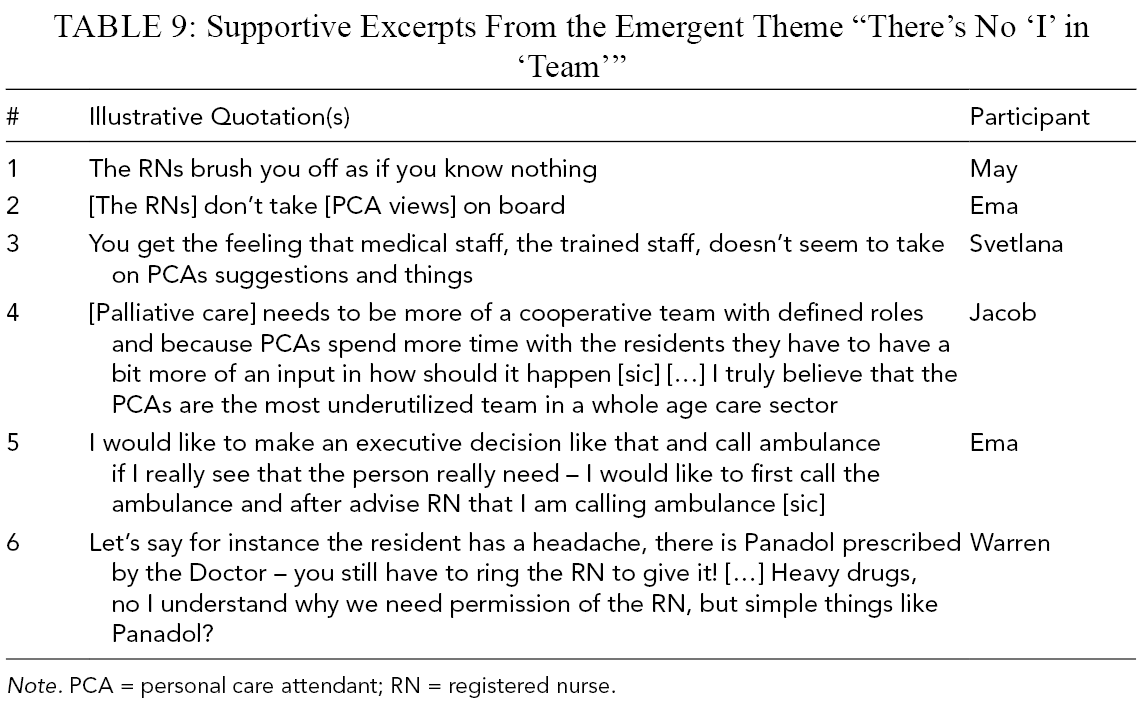
Note. PCA = personal care attendant; RN = registered nurse.
Strategies for Enacting Quality Care
The theme “Strategies for enacting quality care” was identified directly from scenarios and featured strategies describing how participants delivered care in challenging scenarios. Five strategy types were identified. Meta-cognitive strategies included compartmentalization techniques (e.g., “I build a wall”; “switching off”), self-reflection (e.g., “I think to myself ‘why am I here?’”), reframing (“I rationalize aspects of the job”), and perseverance (“I stay calm and get on with my job”). Decentralization exemplified an instrumental support-seeking strategy (e.g., “I ask for extra staff”; “I went to the manager”). Social support communication strategies also involved team coordination through incident reporting (“I talk to the RN”; “I talk to the manager”), and venting (e.g., “blowing steam”; “bitching with others”). Self-extraction strategies represented ways of separating the self from the task, physically and cognitively, and included escape (e.g., “time out and walk away”; “back off”), and work–life separation (e.g., “leave work at work”; “go home and read in Russian”). Lastly, rule-breaking strategies comprised dynamic risk assessment (“for her safety”; “I am not waiting”) and prioritization (“I err on the side of the resident”; “you just put the resident first”; Table 8, #5–10 for further substantive quotes). Compartmentalization techniques were most prevalent, featuring in more than half of scenarios. Distancing from the situation (mentally and/or physically), and terms such as switching off were prevalent responses. Lastly, even though all of these strategies were initiated by the PCA, many sought to maintain care quality by boosting self-care.
Context Matters
The final theme “Context matters” captured the structural descriptions of the scenarios in which the “strategies for enacting quality care” occurred. Table 10 maps contexts against strategies (i.e., textual descriptions), showing the frequencies across scenarios. Inadequate (institutional) procedures were most prevalent followed by staffing numbers, time poverty, and difficult residents. The context of scenarios shaped performance, with the two acting reciprocally. For example, PCAs dealing with difficult residents were more likely to feel frustrated when systemic factors were inadequate, such as limited resources like staffing or time, or having vague procedures.
Structural (Left) and Textual (Right) Descriptions of All Scenarios by Order of Frequency (Arranged Left-to-Right From Most to Least Frequent for Each)
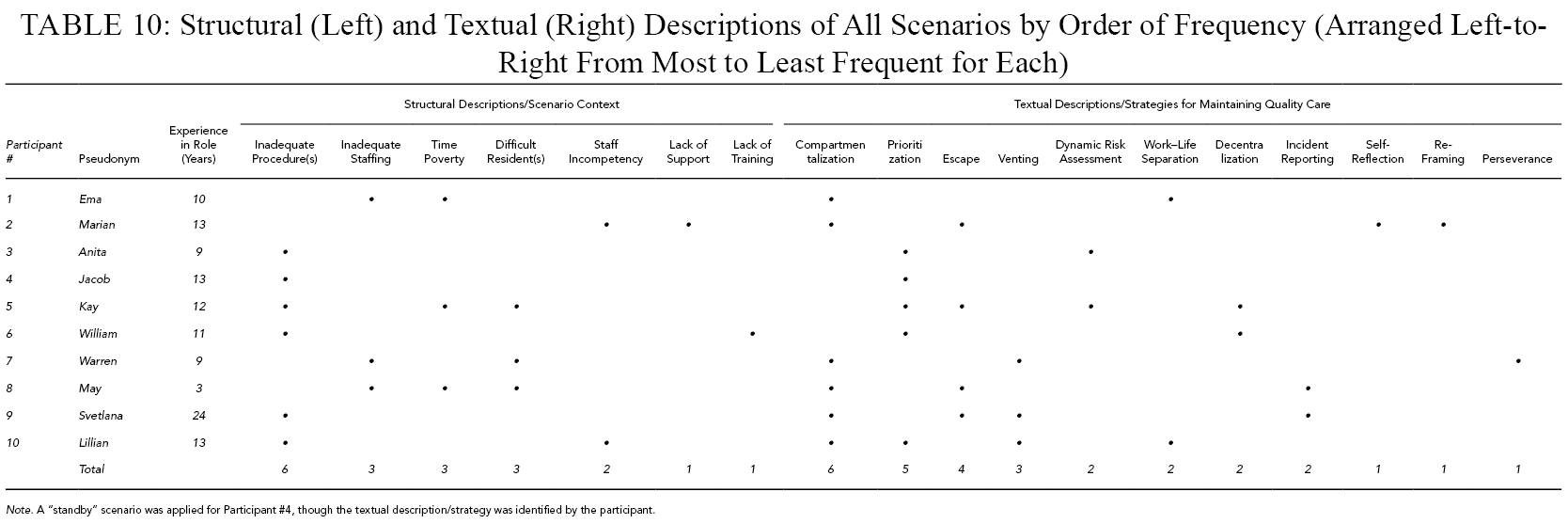
Note. A “standby” scenario was applied for Participant #4, though the textual description/strategy was identified by the participant.
Figure 2 arranges findings specific to the theme “Context matters” and previous themes into a co-occurrence matrix, visualizing the cross linkages and prevalence of each, reflecting intensity of relationship. The most prevalent factor, inadequate procedures, co-occurred most frequently with priority rule breaking, highlighting the adoption of adaptive strategies. Inadequate procedures co-occurred with most identified strategy types though to a lesser extent with meta-cognitive strategies. As the most prevalent type, meta-cognitive strategies based on compartmentalization techniques featured most with inadequate staffing, then with time poverty, and difficult resident(s). Compartmentalization techniques frequently co-occurred with venting, escape, work–life separation and incident reporting, each reflecting specific strategies to reduce dissonance. Escape co-occurred frequently with inadequate procedures, time poverty, and difficult resident(s), indicating a response to inadequate support systems and ambiguity.
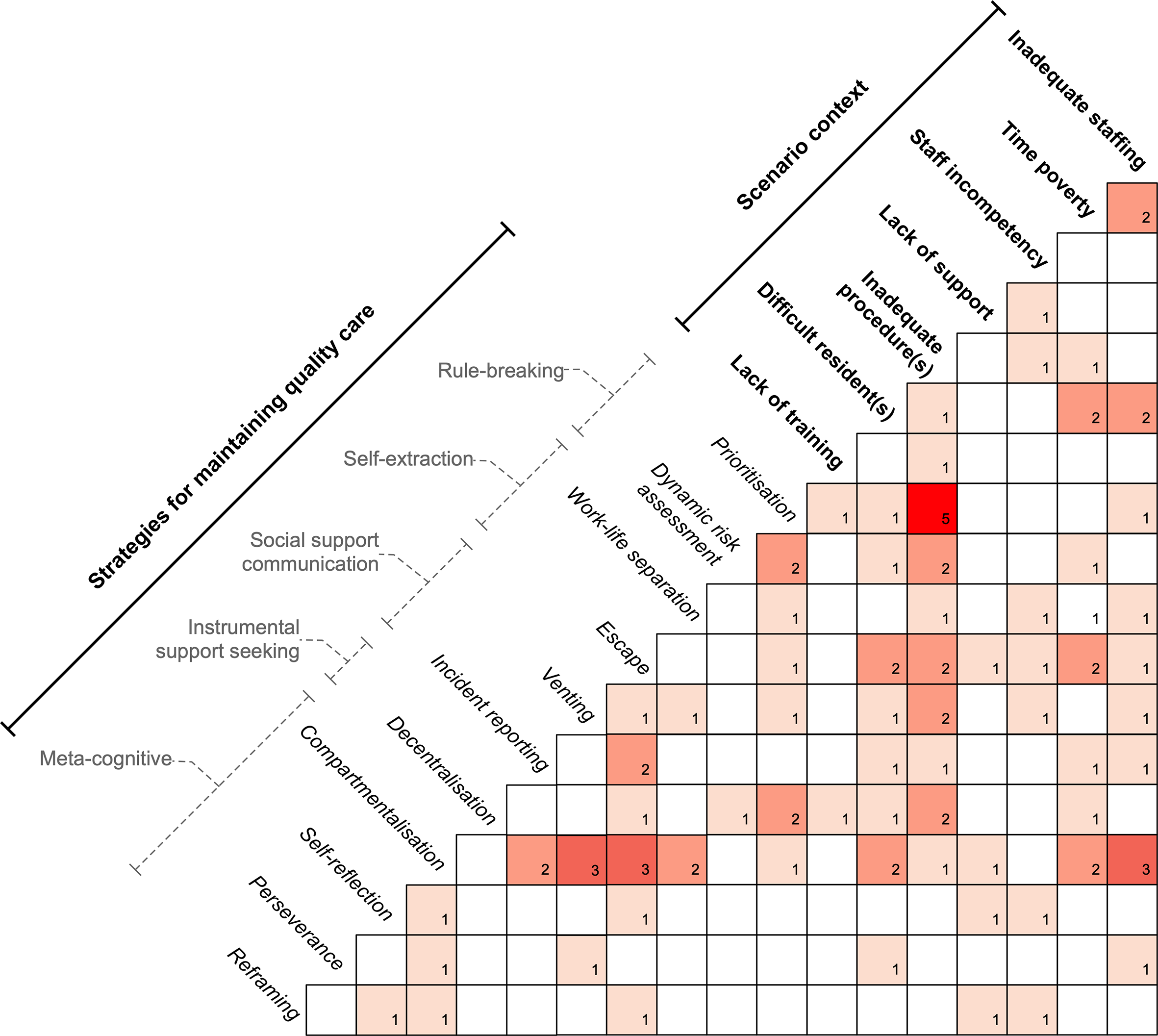
Pairwise co-occurrence matrix network for scenario context and strategies for maintaining quality care. Numbers correspond with frequency of co-occurrence with darker shading showing greater co-occurrence.
All the strategies (textual descriptions) appeared individually directed to improve emotional resilience and featured elements of self-care. For example, social communication strategies happened after the event in the scenario timeline, suggesting they served a cathartic function. Instrumental support seeking through decentralization did not occur frequently, perhaps reflecting contexts undermining its effectiveness (e.g., inadequate staffing, lack of support).
Essence: Versatility in Delivering Quality Care and Engaging with Risk
The findings revealed that PCAs made assessments of resident welfare with fluidity. The essence of experiences common to the phenomenon of adapting to risk in delivering quality care was versatility. Building close relationships with residents as reflected in “Like one of the family” and “TLC” was important for PCA identity, reflecting versatility in communication skills (i.e., through the creation of effective/productive relationships). Though participants were aware of the risks in exceeding professional boundaries, they felt that such relationships were inseparable from quality care and justified transgression. Accessing the lives of residents, connecting with them as family, and maintaining rapport despite violent behavior demonstrated versatility in practicing care. Versatility was also reflected in “Against the clock” and “Navigating (in)flexible boundaries” where scenarios demonstrated capacity to adapt to significant constraints governing resident care (e.g., time, institutional rules) to produce more satisfactory outcomes. Flexibility through drawing on resilience and self-efficacy strategies enabled PCAs to deal with feelings of invalidation and ineffective team coordination as reflected in “There’s no ‘I’ in ‘team’.” Finally, “Strategies for enacting quality care” and “Context matters” both depicted concrete examples of PCA versatility in responding to challenging scenarios aiming to maintain quality care. Given the number of co-occurring challenges, many strategies displayed resourcefulness in the capacity to manage the situation and continue to deliver quality care.
General Discussion
Findings support the notion that PCAs are active participants in maintaining quality care in a complex and dynamic system. PCAs respond to challenging situations by adapting their interactions to achieve required performance. Although rules and boundaries were considered essential, rule breaking was justified as an occupational norm benefiting the resident. Rule breaking was partly enabled by an inability to make ad-hoc decisions about care, particularly in emergency situations. Inadequate decision-making autonomy and job control has been recognized as a mechanism for frustration and low job satisfaction (Booth et al., 2005; Bowers & Becker, 1992; Gao et al., 2014). Delegating PCAs with greater decision-making autonomy along with appropriate training has also been shown to improve personal and professional sense of worth (Phillips et al., 2008).
Although rules governing PCA work implied rigidity, participants assessed risk impacting resident welfare and became more autonomous and responsive to the evolving nature of risk. This practice supports the flexible boundaries model (O’Keeffe et al., 2015), suggesting that for PCAs, decision-making is a fluid and ongoing process occurring across a flexible boundary of risk assessment, acceptance, and action. The ubiquity of rule breaking highlights the existence of more suitable context-specific options rather than one best response to a generic scenario. Bypassing procedures was encouraged by time poverty and lack of staffing and support, meaning that PCAs mostly dealt alone with difficult resident behaviors. Although these findings support previous research on PCAs (e.g., Tuckett et al., 2009), PCAs lacked the autonomy of RNs for decision-making, hence adopting strategies to engender versatility and “get the job done” despite barriers.
A variety of adaptive strategies were identified demonstrating PCA versatility in performing their role. Decentralization (i.e., distributing the process; calling in assistance) was common, though difficult to apply where facilities were understaffed. Compartmentalizing by creating physical and emotional distance from the situation (i.e., through walking away) was also used. Beyond self-preservation, walking away from a situation was a tactical negotiation for dealing with difficult residents, whereas separating work from home was considered an essential PCA skill. Some strategies, however, highlighted maladaptive approaches. Venting can strain relationships over time and since compartmentalization is often a defensive, self-protective process (Thomas et al., 2013), it is likely to increase aggression (MacNair, 2012).
Few PCA strategies were organizationally led; rather, most contextual descriptions were active impediments to creating a positive context for care or formally promoting PCA autonomy. In negotiating care, the scenarios showed that participants strove to optimize rule-based compliance with safety, efficiency, and individualized attention to provide “good enough” care. Workplace rules serve three primary functions: as organizational control, as a means of coordinating and supporting workers, and to codify organizational knowledge (Weichbrodt, 2015). Participants adapted organizational rules by assessing their applicability, first by judging the level of risk (considering safety, standards of care and dignity for the client), and second, by considering the level of rule usefulness to achieving goals, and finally the possible consequences. Assessments were then integrated into decisions for coordinating work (e.g., by prioritizing tasks to assist other PCAs and optimize competing needs) and identifying the scope for acting flexibly. Workarounds are a reality of care work when workers feel “controlled” by the system and are unable to achieve competing work demands, particularly the provision of good care in the face of time pressure and resource constraints (Debono et al., 2013).
Most PCA adaptive strategies affecting care quality and job satisfaction indicated perceived deficiencies in the PCA–RN dynamic, including the ability to make timely decisions, elicit greater respect, and having skills and expertise recognized. Some contextual descriptions (e.g., inadequate procedures) and strategies (e.g., rule breaking, meta-cognitive) characterized the PCA as a “cognitive system,” defined as an agent that maintains order in the face of disruptive influences and controls what it does (Woods & Hollnagel, 2006). Further, the PCA and RN may be considered a “joint cognitive system” (Woods & Hollnagel, 2006), where control is practically stretched between both parties, even if this is not reflected in procedures. This interplay was observed in scenarios where PCAs lacked control, but also by judgments that further disruption was not necessary, for example, calling the RN overnight could subsequently destabilize the system (e.g., upset and/or sleep deprive the RN, elevating risk).
Although further research is required to elaborate the nuanced and subjective views elicited through this study, findings from the scenarios reflect adoption of strategies for maintaining system performance. Flexing rules/procedures has implications not only for quality of work/care but also for developing better informed and adaptable risk assessment processes that create more efficiency in PCA work and the broader system.
Implications for Policy and Practice
Our findings carry implications for practice, indicating an opportunity to improve job design through fostering greater interdependence in the roles of PCA and RN (Toles & Anderson, 2011). Supporting the study of Anderson et al. (2005), our findings note that PCAs are observant and possess the fundamental information to inform quality care but lack the deeper knowledge allowing these cues to be linked to clinical implications. This gap could be narrowed through promoting information sharing and problem-solving in the form of case studies that contextualize cues and build the clinical understanding of PCAs with the RN acting as facilitator of care rather than chain of command (Anderson et al., 2005). Other strategies include use of structured communication tools to guide spontaneous information sharing and problem-solving (O’Keeffe et al., 2016). Altering job design has implications for policy and adds weight to the calls for attention to staffing ratios and skill mix that facilitate greater RN involvement in PCA on-the-job skill development.
Strengths, Limitations, and Future Directions
Participants were employed by different aged care facilities located in rural settings, which may operate differently than those in urban areas. Additionally, this study utilized highly experienced PCAs to elicit substantive expertise. Although the sample size did not limit the phenomenological approach used in this study, care must be taken when generalizing its findings. In conjunction with phenomenology, SITT application provided rich and concrete examples of adaptation to risk, which may not be apparent through observation or conventional interviewing.
Given study limitations, future research should include aged care facilities in urban locations and less experienced PCAs to more overtly examine specific dimensions of skill development and work satisfaction. Although RNs currently make decisions about resident welfare in safety-related and/or emergency situations, their number within aged care facilities is critically limited (Aged and Community Services Australia, 2015). Given the similarities in PCA and RN work, the application of “joint-cognitive system” theory in this dynamic warrants further investigation to determine where PCA capability may be enhanced with formal autonomy.
Conclusions
The aged care workplace is growing increasingly complex, and this study illustrates how care is enacted by PCAs in the face of constraining factors that produce challenging scenarios. PCAs draw upon a repertoire of individually directed adaptive strategies to manage constraints, highlighting an absence of organization-led initiatives. Rule breaking is a reality of enacting care, largely to optimize safety, compliance, and efficiency, lending evidence of PCA adoption of risk-based decision-making models. Though the rules in aged care facilities suggest rigidity, responses to competing demands reveal PCAs’ work is a dynamic and adaptive skill-based response necessary to perform effectively in complex and safety-critical situations. The role highlights that assessments of resident welfare are actually made with fluidity and autonomously despite organizational restrictions and lack of formal support. In addition to the satisfaction derived from building relationships, these adaptive strategies may explain how the PCA role continues to function despite current system demands and marginalization of expertise.
Key Points
Inadequate staffing and procedures, inadequate training, challenging residents, time poverty, and low support are all key challenges in the delivery of quality aged care from the perspective of personal care attendants (PCAs).
PCAs use a variety of individually directed adaptive strategies to alleviate dissonance and maintain emotional resilience.
PCAs tend to undertake fluid dynamic risk assessment to break institutional rules when encountering conflicts and dilemmas.
In the absence of formalized institutional support or PCA autonomy, PCAs enact a variety of work strategies and boost self-care, demonstrating versatility in delivery of aged care.
Use of a phenomenological approach with novel scenario generation techniques can elicit rich and concrete descriptions of challenging everyday work scenarios underpinning lived experience.
Footnotes
Acknowledgments
The authors are grateful to the Personal Care Attendants who participated in this study.
Author Biographies
Anjum Naweed is an associate professor at Central Queensland University with over 15 years of experience in human factors and cognition across a range of settings. He is a Certified Professional Ergonomist at the Human Factors & Ergonomics Society of Australia, an Associate Member of the Chartered Institute of Ergonomics and Human Factors, and a current Scientific Editor of the journal Applied Ergonomics. His interests focus on trying to understand and enhance the way that people perform in complex, often highly safety-critical environments.
Jana Stahlut obtained her honors degree in psychological science from Central Queensland University (2016) and completed a postgraduate diploma in Mental Health Counselling (2019). She has over 15 years’ experience in the aged healthcare sector.
Valerie O’Keeffe is Senior Research Fellow Human Factors at Flinders University, and a Fellow and Certified Professional Ergonomist of the Human Factors and Ergonomics Society of Australia. Valerie’s research interests focus on worker performance in healthcare settings and the influence of job quality and design on worker health and safety and client care.