
Abstract
Objective
The aim of the study was to estimate the risk of injury when repositioning patients of different weight with commonly used repositioning aids.
Background
Repositioning dependent patients in bed is the most common type of patient handling activity and is associated with high rates of musculoskeletal disorders in healthcare workers. Several studies have evaluated repositioning aids, but typically for a single patient weight and often without estimating risk of injury based on biomechanical analysis.
Method
Ten nurses performed four repositioning activities on three participants (50, 77, 141 kg) using three repositioning aids (pair of friction-reducing sheets [FRS], turn and position glide sheet, air-assisted transfer device) and a draw sheet. Motion capture, hand forces, and ground reaction forces were recorded. Spine loading was estimated using a dynamic biomechanical model.
Results
Hand forces and spine compression exceeded recommended limits for most patient weights and repositioning tasks with the draw sheet. FRS and glide sheet reduced these loads but still exceeded recommended limits for all but the 50-kg patient. Only the air-assisted transfer device reduced forces to accepted levels for all patient weights. Physical stresses were relatively low when turning patients.
Conclusion
Most repositioning aids are insufficient to properly mitigate risk of musculoskeletal injury in healthcare workers. Only the air-assisted transfer device was sufficient to adequately mitigate the risk of injury when moving patients of average or above-average weight.
Application
To safely move dependent patients, a robust solution requires mechanical lifts and may utilize air-assisted transfer devices for patient transfers.
Keywords
Introduction
Rates of musculoskeletal injuries among healthcare workers are higher than for almost all other occupations (Bureau of Labor Statistics, 2016) and most of these injuries are attributed to manual handling of patients (Davis & Kotowski, 2015; Holtermann et al., 2013; Smedley et al., 2003). Manually lifting patients exposes workers to forces that are known to cause risk of back injury, and training in manual lifting techniques does not reduce this risk (Kraus et al., 2002; Lavender et al., 2007; Martimo et al., 2008; Warming et al., 2008). By applying the NIOSH lift equation to postures adopted during manual patient handling, Waters et al. (2007) determined at most 35 lbs (156 N) could be lifted safely. Therefore, when lifting or mobilizing patients, mechanical lifts are recommended as the standard of care to protect healthcare workers from injury.
Of all the patient handling activities that healthcare workers perform, repositioning supine patients is most frequent (Poole Wilson et al., 2015; Vasiliadou et al., 1995). Recent data from the global risk consulting company AON suggest that nearly twice as many healthcare workers are injured when repositioning patients as compared to transferring patients between beds or chairs (AON, 2018). These repositioning activities include repositioning patients up in bed (boosting), laterally repositioning, and turning. Such activities tend to require more horizontal pushing and pulling than purely lifting against gravity. Repositioning patients can also involve rapid jerking motions as caregivers pull and lift to overcome the starting friction of the patient against the bed. The NIOSH lifting equation does not apply to these pushing, pulling, and rapid force exertions. Therefore, when repositioning supine patients, it is unclear under what circumstances patients can be safely repositioned manually, or whether aids like friction-reducing sheets (FRS) or lift equipment are needed. Understanding when assistive devices are needed is important so facilities can have the proper equipment available to allow caregivers easy access to the tools they need to reposition their patient safely.
Several studies have estimated spine loading on healthcare workers when performing the activities required to reposition patients in bed (Daynard et al., 2001; Schibye et al., 2003; Skotte et al., 2002; Skotte & Fallentin, 2008). These studies all consider boosting, lateral repositioning, and turning. The researchers found that lateral repositioning and boosting often exceeded the 3400 N action limit for acceptable compression forces on the spine (Waters et al., 1993). However, the studies did not systematically evaluate assistive devices or interventions designed to reduce the risk of injury during patient handling.
Other researchers have evaluated the use of assistive devices for at least one patient repositioning activity (i.e., boosting, lateral repositioning, and turning) or for laterally transferring a patient between surfaces. In several different experiments, at least one FRS was compared to a traditional cotton draw sheet for one or two activities (Baptiste et al., 2006; Bartnik & Rice, 2013; Bohannon, 1999; Fragala & Fragala, 2014; Fray et al., 2016; Larson, 2015; Lloyd & Baptiste, 2006; McGill & Kavcic, 2005; Theou et al., 2011; Weiner et al., 2017). Dependent variables included hand force, estimated spine loads, electromyography of the arm and shoulder, coefficient of friction measurements, and subjective ratings. There is general agreement among the studies that physical demands are lower when using an assistive device such as an FRS to reposition a patient as compared to using a draw sheet. However, in most studies differences among assistive devices tended not to be significant. Two studies have evaluated the turn assist feature common in many air surfaces available on hospital beds. Turn assist reduced hand force and spine loads when turning and laterally repositioning a 63-kg patient and a 123-kg patient (Wiggermann, 2016) and when turning an 82-kg patient (Budarick et al., 2019).
Previous studies of patient repositioning had a great variety in the types of patients and caregivers included. Several studies of patient repositioning have included different patient weights but only some of those have reported results by patient weight or considered patient weight as a factor in the analysis (Fray et al., 2016; Skotte & Fallentin, 2008; Zhuang et al., 1999). When considering the caregiver, past studies included as many as 77 caregivers in an unbalanced experimental design and 12 caregivers in a full factorial design (Fragala & Fragala, 2014). Several researchers included individuals without healthcare experience (Larson, 2015; McGill & Kavcic, 2005; Silvia et al., 2002). Other studies used only members of the research team to reposition patients or mannequins (Bartnik & Rice, 2013; Bohannon, 1999; Fray et al., 2016; Lloyd & Baptiste, 2006).
Although the existing body of literature is useful for understanding how well specific assistive devices work for certain repositioning activities, it is still unclear when a patient of a given weight can be safely repositioned manually, with a small repositioning aid, or whether lift equipment is needed. Most of these previous studies did not perform a biomechanical assessment of the load on the spine to estimate risk of injury. Moreover, these studies provide only a patchwork of limited comparisons of repositioning aids with disparate methods and dependent variables. Ergonomists and caregivers need to understand the relative risk of injury for all repositioning activities across multiple patient weights and with all current types of repositioning aids. Given the widespread use of repositioning aids, this lack of information is concerning.
The objective of this study was to compare the physical stress on caregivers across all repositioning activities, for multiple patient weights, and for each common type of repositioning aid. The results from these combinations of test conditions will allow caregivers to understand when repositioning aids are effective and when manual handling of the patient presents an elevated risk of injury.
Methods
This laboratory study evaluated healthcare workers as they repositioned individuals of differing body weight in hospital beds. The activities investigated were repositioning up in bed (boosting), lateral repositioning, lateral transfer between beds, and turning. During these tasks, hand forces, ground reaction forces, and postural data were collected to be used for biomechanical modeling.
Participants
Ten female “caregiver participants” were recruited from Southeast Indiana and Southwest Ohio, who had at least 1 year of experience in a role where they repositioned patients at least once per shift. Their mean (standard deviation) height and weight were 169.8 cm (7.6 cm) and 80.4 kg (16.6 kg), respectively. The caregiver participants wore their own form-fitting clothes that consisted of knit or spandex workout pants, T-shirts or tank tops, and athletic shoes. Three healthy “patient participants” were recruited to act as completely immobile patients. The patient participants were a 50-kg female, a 77-kg female, and a 141-kg male. These individuals participated in all experimental sessions except for the 77-kg female who was replaced with an 82-kg female for two sessions because of scheduling conflicts. This research was approved by Advarra IRB (Cincinnati, OH) and each participant provided written informed consent (Protocol #201706185).
Products
Three types of repositioning aids were evaluated across the different patient repositioning activities. Two Liko HandySheets (Hillrom, Batesville, IN, USA) were used to represent the category of the FRS. These sheets were intended to represent a particularly low-friction type of FRS and were placed under the patient as a pair as per manufacturer recommendations to maximize their effectiveness. The AirPal (AirPal, LimePort, PA, USA) was included to represent the air-assisted repositioning device (AARD). This device is connected to a blower which inflates the AARD under the patient. Small perforations on the underside of the device creates a flow of air which reduces the friction between the AARD and the bed. The Sage Turn and Position (TAP) glide sheet (Stryker, Kalamazoo, MI, USA) was chosen to represent the category of TAP systems which are used by caregivers to reposition patients, typically to offload parts of the body at risk of pressure injuries. Whereas the FRS and AARDs are generally not designed to be left under the patients and must be installed and removed before and after use, manufacturers claim that TAP systems can be left under the patient without increased risk to pressure injury. The standard cotton draw sheet which is still most commonly used to move patients was included as the baseline condition for all activities.
All trials were performed on the same Centrella Max hospital bed (Hillrom). Turning trials were performed with and without the turn assist on Centrella Max. For the lateral transfer, the patient participant was transferred from a Centrella bed with a foam mattress to the Centrella Max, so it would be representative of a transfer from either a bed or a stretcher with a foam mattress.
Data Collection
During the trials, hand forces of the caregiver participant were measured using force gages configured as described in a previous study (Wiggermann, 2016). Ground reaction forces were measured using a force plate (AMTI, Watertown, MA, USA). Data from an eight-camera optical motion capture system (Motion Analysis, Santa Rosa, CA, USA) were recorded at 60 Hz.
Procedure
Experimental sessions began by placing 38 motion capture markers in a modified Helen Hayes configuration on the caregiver participant (Clark et al., 2016). After the experiment was explained to the caregiver participant, she practiced with any repositioning aids that were different from what was typically used on her job. Caregiver participants performed all tasks from the patient’s left side of the bed.
The caregiver participant was instructed to begin the trial with both feet on the force plate and the bed was moved per caregiver instructions to achieve a realistic relative position between the caregiver and the patient. For the boosting trials, the caregiver was permitted to step off the force plate with her right foot as she shifted her weight to move the patient up in bed. If the caregiver participant stepped off the force plate, a visual inspection of the biomechanical model output was performed to verify that the relative maximum of spine load occurred before the caregiver stepped off the force plate, which was true for all affected trials. Other than these instructions, the caregiver participant was encouraged to perform the repositioning task as she would on the job. The movement adopted by the caregivers was generally most similar to the “parallel stepping” method described by Fray and Holgate (2018), but some torso rotation was also observable in most trials.
Because boosting and lateral transfers are commonly performed by a pair of caregivers, the same member of the research team (NW) assisted the caregiver participant from the opposite side of the bed. Turning and lateral repositioning trials were performed by the caregiver participant alone. Before each trial, the caregiver adjusted the bed to her preferred height and provided direction to the assistant, if present. Caregivers were instructed to adjust the bed to their preferred height without considering the height of the assistant. For the transfer trials, the caregiver also prescribed the height of the bed from which the patient was being transferred, typically so that it was a few centimeters higher than the destination bed.
Patient position was standardized across the four repositioning activities. For the boosting trials, the patient participant was centered along the width of the bed and the head was positioned at the lowest of two tape marks on the mattress that were 8 and 38 cm below the head-end edge of the mattress. When boosting the patient, the caregiver and the assistant pulled up the patient so that the head moved from the lower tape mark to approximately the higher tape mark, for a travel of approximately 30 cm. For lateral repositioning, the patient participant began with the right shoulder approximately 5 cm from the right edge of the bed and the caregiver pulled the patient until the left shoulder was approximately 5 cm from the left edge of the bed. This activity simulated the repositioning that might often be achieved before a caregiver turns a patient so that the patient has room to be rotated. For the lateral transfer trials, the side rails of both beds were lowered and the beds were pushed together side by side to minimize the gap between the mattresses. The patient participant began with the left shoulder approximately 10 cm from the edge of the origin bed and was moved until approximately centered in the destination bed. Before each turning trial, the caregiver directed the patient to assume the position that the caregiver would typically position a patient before turning in the clinical setting. Data for the turning trial were then recorded as the caregiver turned the patient toward the caregiver using a draw sheet. When turn assist was used, the caregiver engaged turn assist on each product either until the actuation was complete or until she was satisfied with the patient position. Each repositioning activity is illustrated in Figure 1.
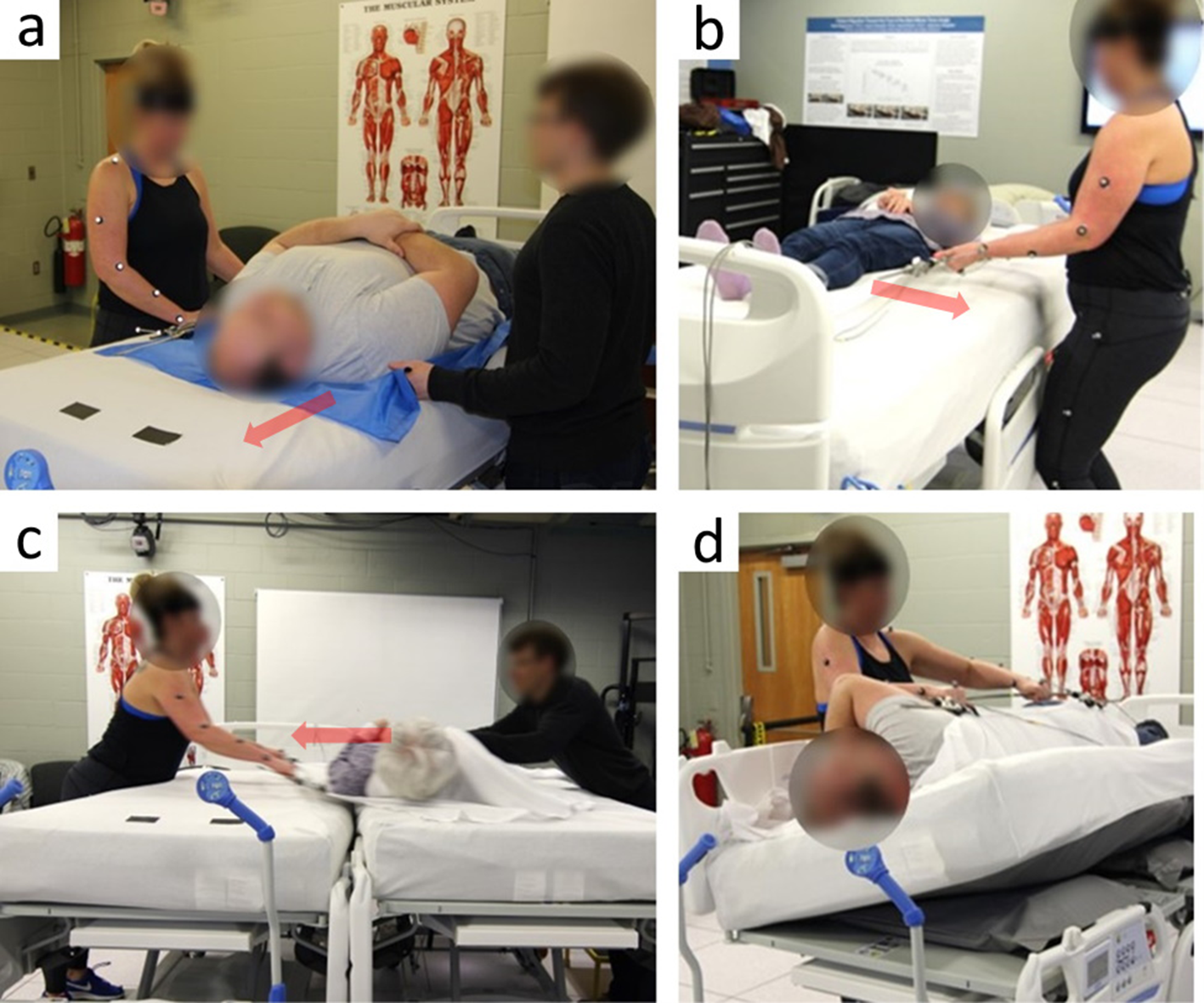
Repositioning activities: (a) boosting, (b) lateral repositioning, (c) lateral transfer, (d) turning with the turn assist condition. Red arrows indicate the direction of movement.
This experiment tested every feasible combination of repositioning activity, repositioning aid, and patient weight. The TAP sheet was not tested for lateral transfers because it was not designed for this purpose, and the 141-kg patient participant was omitted from some trials to limit the risk of injury to the caregiver participant. Each condition was replicated twice for a total of 66 trials per participant (Tables 1 and 2 for all conditions). Trials were randomized within patient participant. Caregivers were encouraged to rest as often as needed but rested a minimum of 60 s between trials and often longer if a change of equipment was required. For all caregiver participants, the entire experimental session lasted between 6 and 8 hr including lunch and other rest breaks.
Estimated Peak Spine Compression at the L5/S1 by Repositioning Activity, Repositioning Aid, and Patient Weight
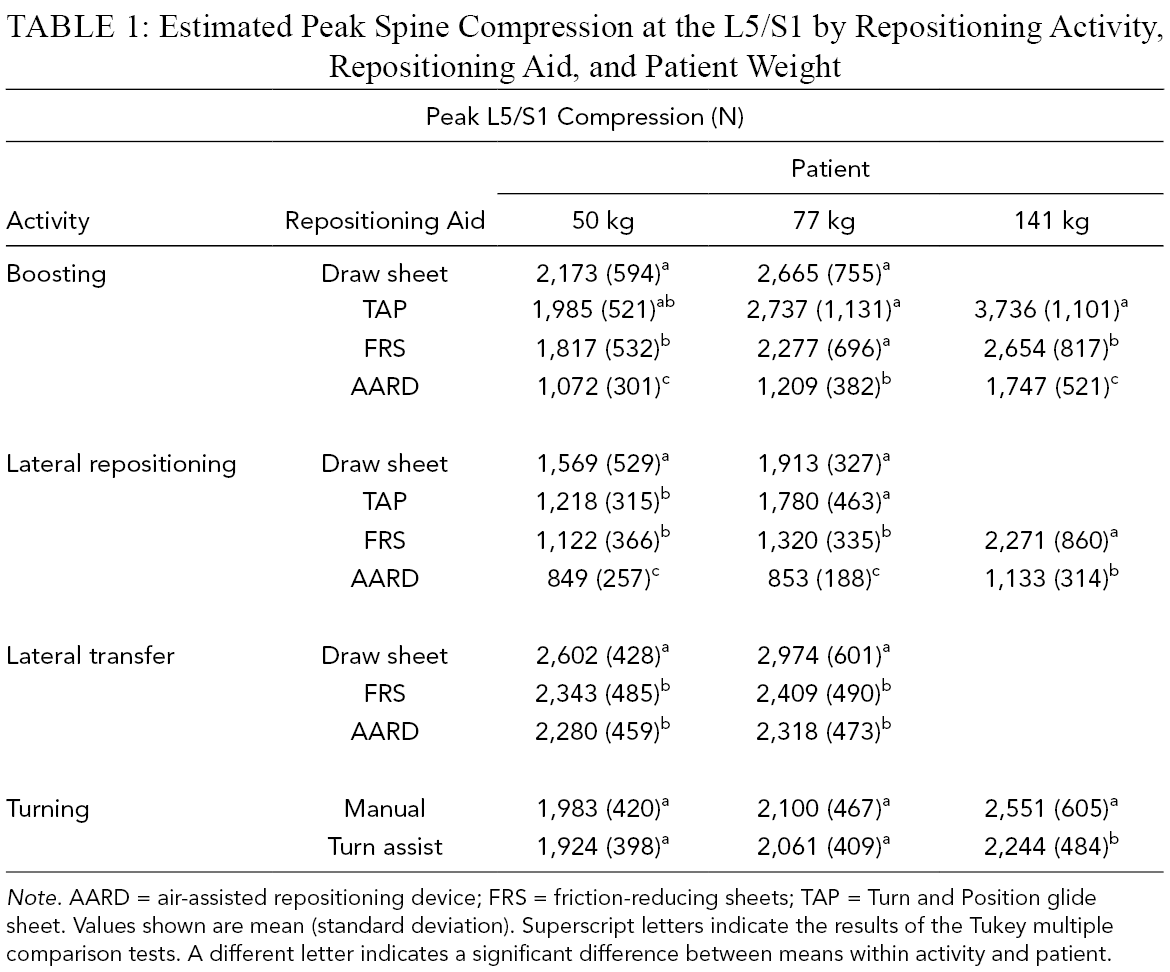
Note. AARD = air-assisted repositioning device; FRS = friction-reducing sheets; TAP = Turn and Position glide sheet. Values shown are mean (standard deviation). Superscript letters indicate the results of the Tukey multiple comparison tests. A different letter indicates a significant difference between means within activity and patient.
Peak Hand Force by Repositioning Activity, Repositioning Aid, and Patient Weight
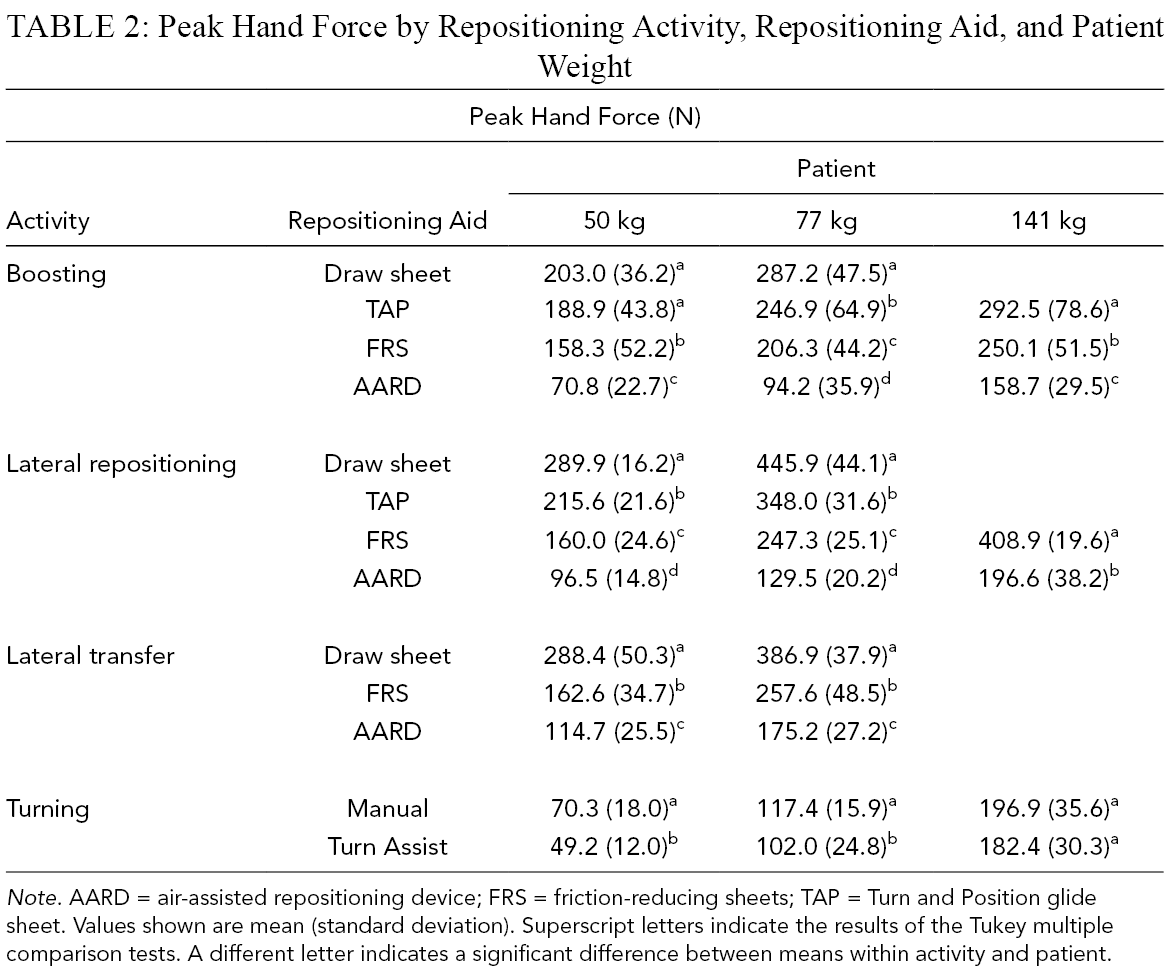
Note. AARD = air-assisted repositioning device; FRS = friction-reducing sheets; TAP = Turn and Position glide sheet. Values shown are mean (standard deviation). Superscript letters indicate the results of the Tukey multiple comparison tests. A different letter indicates a significant difference between means within activity and patient.
Biomechanical Model
Spine forces at the L5/S1 and muscle forces as a percentage of maximum voluntary effort (%MVE) were estimated using the AnyBody Modeling System (AnyBody Technology, Aalborg, Denmark). Anybody is a validated (Bassani et al., 2017) whole-body dynamic model that scales a custom human model for each participant, estimates kinematic movements, and performs inverse dynamics analysis (Figure 2) to estimate muscle forces and joint loads (Damsgaard et al., 2006). Motion capture marker coordinates, ground reaction force, and hand forces were all inputs to the model.
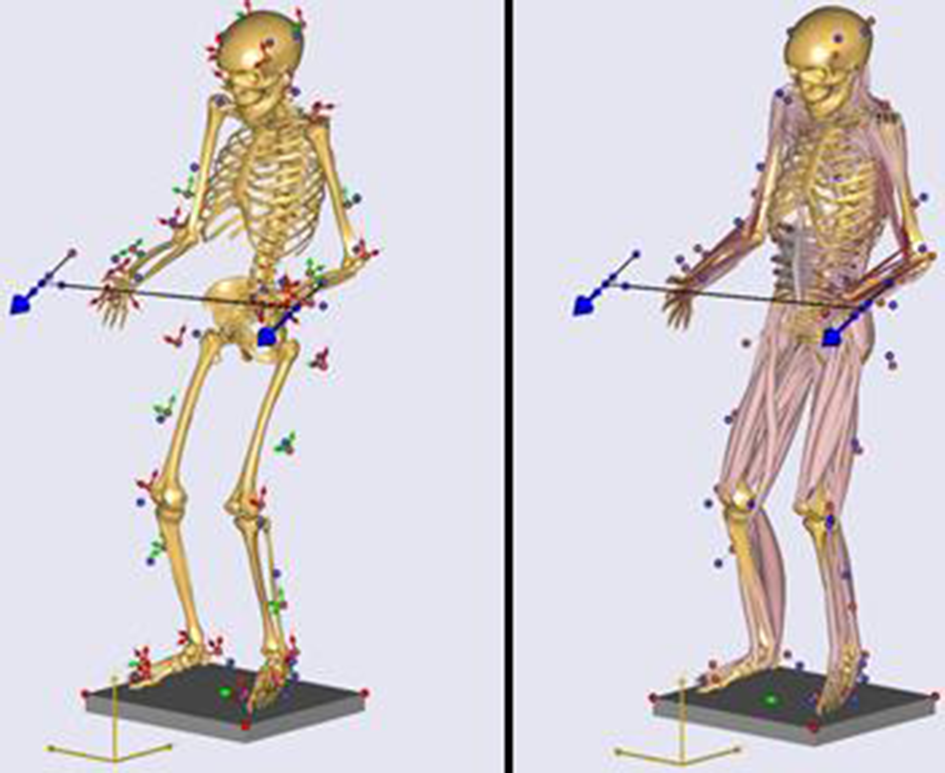
Graphical representation of the kinematic (left) and inverse dynamic (right) steps of modeling.
Relative to accepted injury thresholds, spine compression forces were consistently larger than shear forces, and shear forces were generally below 500 N. Therefore, the analysis of spine loading was limited to spine compression. Similarly, %MVE was greatest for the elbow flexors, so analysis focused on the left brachialis.
Statistical Analysis
For each repositioning activity, a repeated measures analyses of variance (ANOVA) was performed to test for the effects of repositioning aid and patient weight. Caregiver participant was included as a random factor. Within repositioning activity, post hoc comparisons of repositioning aid and patient weight were performed using Tukey–Kramer tests. An ANOVA and Tukey–Kramer test was also used to compare activities. All analyses were performed using Minitab software (v.16, Minitab Inc., Pennsylvania, USA), with significance criteria set as α < .05.
Results
Peak Compression at L5/S1
Both repositioning aid and patient weight significantly affected peak compression at the L5/S1 (Table 1). Across all activities, the draw sheet trended toward the greatest compression, followed by the TAP, FRS, and AARD with the lowest compression. Higher patient weight was also associated with greater spine compression across all activities. All activities significantly differed from one another, with the greatest spine compression for lateral transfers, followed by boosting, turning, and lateral repositioning.
Post hoc comparisons of peak spine compression among repositioning aids are shown in Table 1. Peak compression for the AARD was significantly less than those for the draw sheet and TAP across all activities and patient weights tested. For the remaining comparisons across devices, statistical significance varied by activity and patient weight. For turning, peak spine compression for turn assist was significantly less than manual turning for the 141-kg patient only. Means of peak compression forces exceeded 3,400 N only when boosting the large patient with TAP. Additionally, individual trials exceeded 3,400 N for boosting the 77-kg patient with the draw sheet, TAP, and FRS; and boosting and laterally repositioning the 141-kg patient with the FRS; and transferring the 50- and 77-kg patients with the draw sheet.
Peak Hand Force
Similar to spine compression, both repositioning aid and patient weight significantly affected hand force, and these factors also trended the same as for spinal compression with draw sheet, TAP, FRS, and AARD in order of greatest to least force. A comparison of spine compression and hand force for the boosting task is illustrated in Figure 3. For most activities and patient weights, all repositioning aids were significantly different from one another. For turning, hand forces were significantly lower with turn assist for the 50- and 77-kg patients (Table 2). All activities significantly differed from one another, with the greatest hand forces occurring for lateral repositioning, followed by lateral transfers, boosting, and turning.
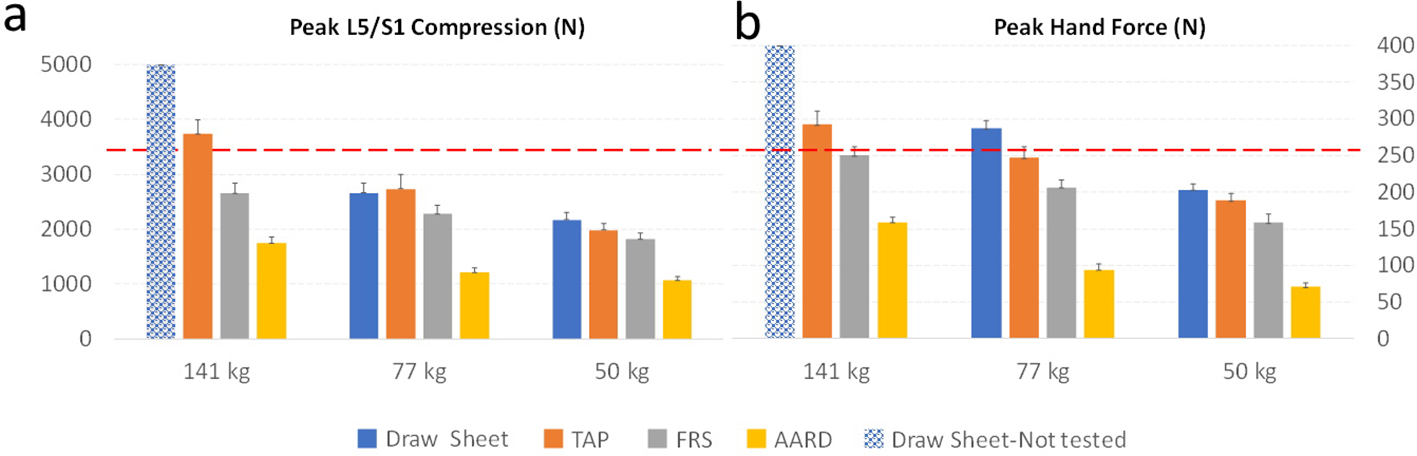
Mean of peak spinal compression (a) and peak hand force (b) for the boosting activity. Dotted line indicates the 3,400 N NIOSH limit (a) and 255 N psychophysical limit (b). Error bars depict standard error.
Estimated Muscle Exertion
Muscle forces as %MVE were greatest for the elbow flexors. The %MVE for the left brachialis during the boosting task is shown in Figure 4. The %MVE trended very closely with peak hand force.
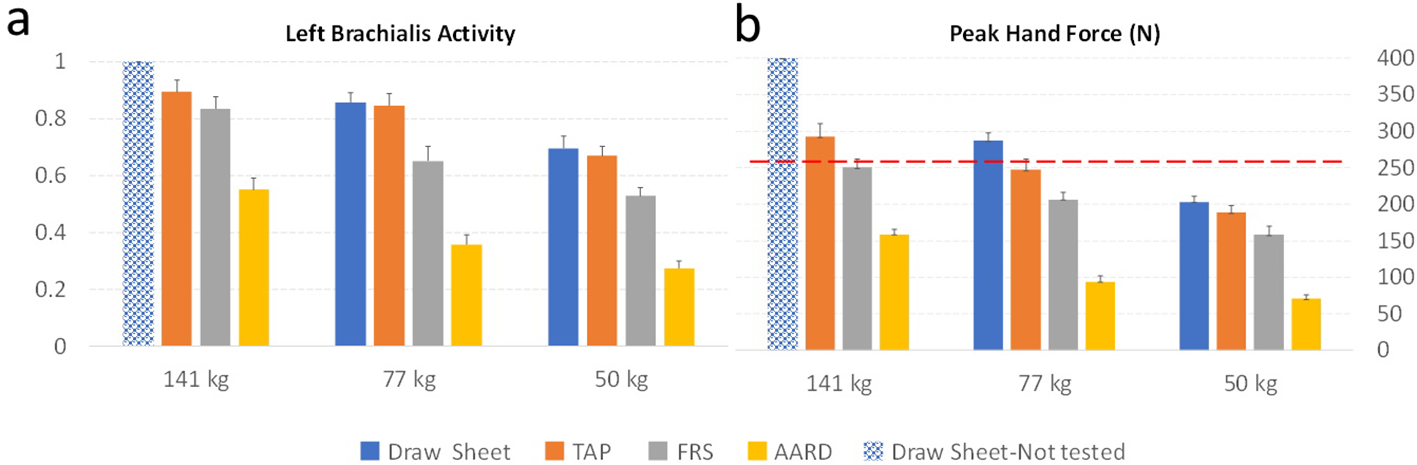
Mean of left brachialis activity as a proportion of maximal strength (a) and peak hand force (b) for the boosting activity. Dotted line indicates the 255 N psychophysical limit. Error bars depict standard error.
Interaction of Repositioning Aids and Patient Weight
A significant interaction between repositioning aid and patient weight was found for peak spine compression and hand force for all activities except turning. The general trend of these interactions was that increased patient weight corresponded to a greater increase in spine compression and hand force for the draw sheet and TAP than for the FRS and AARD.
Discussion
This study compared biomechanical stresses on the body for different patient repositioning activities, repositioning aids, and patient weights. Spinal compression, hand forces, and estimated muscle exertion all increased with patient weight. Physical stresses were greatest for the draw sheet followed by the TAP and FRS, and were lowest for the AARD. The draw sheet, TAP, and FRS exceeded recommended pull forces for many test conditions, suggesting that AARD or lift equipment is needed to address the risk of injury when repositioning patients.
For spine loading, only boosting the 141-kg patient with TAP exceeded the NIOSH-recommended 3,400 N limit (Waters et al., 1993). Although boosting and transferring the 141-kg patient with a draw sheet were not tested, these conditions would also likely exceed 3,400 N based on the trends in the results.
Based on Snook and Ciriello (1991), peak hand forces acceptable to 75% and 90% of the female population are 255 and 216 N, respectively, when pulling 2.1 m at waist height every 30 min. These peak hand force limits were exceeded for many patient weights, repositioning activities, and repositioning aids. The AARD was the only repositioning aid to reduce peak hand forces below the psychophysical guidelines for all patient weights and repositioning activities tested.
Relative to recommended limits, peak hand forces were consistently higher than spine compression. There were no test conditions for which spine compression was greater than peak hand forces when compared as a proportion of the recommended guidelines. For the boosting activity as an example, Figure 3 compares spine compression relative to the NIOSH’s 3,400 N limit and peak hand forces relative to the Snook guidelines. Although these guidelines were developed using different methods, this comparison shows how peak hand forces appear to be the primary limitation to safely repositioning the patient. The horizontal nature of the hand forces applied by the caregiver participants when repositioning likely explains the low spine compression values relative to hand forces. Accordingly, for the repositioning activities included in this study, repositioning aids should be selected based on force exposures at the hands.
Figure 5 illustrates the peak hand forces measured in the current study as compared to the psychophysical requirements. The comparisons in this figure are based on assumptions of posture and frequency used to select psychophysical limits from Snook and Ciriello (1991). The estimates of accommodation based on patient weight also assume a linear relationship between the weights tested in the current study, and should be interpreted with caution. Although the exact thresholds in this figure are sensitive to these assumptions, they generally illustrate that with the exception of the AARD, most repositioning aids fail to properly mitigate physical stresses on caregivers across patient weights and repositioning activities.
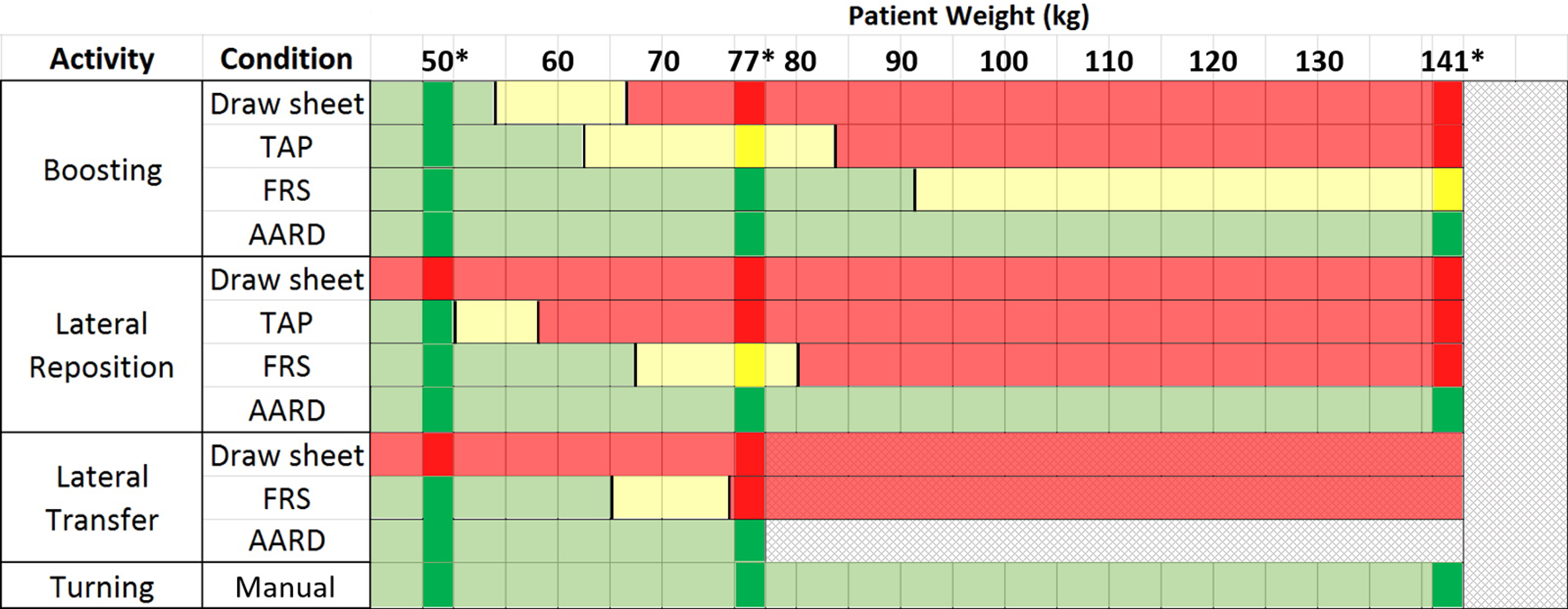
Guidelines for selecting repositioning aids based on patient weight. Hand forces measured in the current study are compared to psychophysical guidelines by Snook and Ciriello (1991). Green shading indicates hand forces less than pull forces acceptable to 90% of females. Red indicates forces greater than pull forces acceptable to 75% of females. Yellow accommodates 75% but not 90%. *Actual patient weights tested in the study; all other ranges are estimates. The black vertical lines between colors represent an interpolation of the hand forces between test conditions that corresponds to the psychophysical threshold.
The work methods used by Snook and Ciriello (1991) to determine psychophysical limits differ from the physical exertions of the caregiver participants in the current study. The hand forces in the current study were primarily horizontal, but some vertical force component was applied to overcome the starting friction when moving the patient. Nevertheless, the psychophysical guidelines provide the best comparison for estimating risk of injury to healthcare workers.
Although these psychophysical limits are not a direct estimate of biomechanical load, musculoskeletal disorders have been shown to increase when physical demands exceeded forces acceptable to 75% of the working population (Herrin et al., 1986). In the current study, estimated muscle forces as %MVE revealed that particularly the elbow flexors were near maximal effort when hand forces exceeded psychophysical guidelines. When the human body cannot accomplish a task due to either movement or strength limitations, a compensation pattern manifests to fulfill the task. Compensation strategies frequently employ the use of momentum, abnormal muscle recruitment, and adjacent joint movement. This often increases the risk of injury, especially in the shoulder complex, which is primarily stabilized by muscle alone (Paine & Voight, 2013). Muscles recruited to assist in compensatory strategies are typically not designed for such tasks, creating strains. Momentum stretches muscles and tendons beyond their safe range, and adjacent joints often become hypermobile creating inflammation and tissue damage. These findings are particularly relevant considering that rates of shoulder injuries are second only to back injuries in caregivers (Davis & Kotowski, 2015).
Spine compression values from the current study were similar to those of the research group of Skotte and Fallentin (2008) that also used a dynamic biomechanical model with an optimization algorithm for estimating muscle recruitment. Spinal compression from the current study of 2,665 and 2,100 N when boosting and turning a 77-kg patient with a draw sheet was very similar to the respective estimates of 2,616 and 2,044 N by Skotte and Fallentin (2008). However, the current study estimated 1,913 N when laterally repositioning the 77-kg patient with a draw sheet which is much less than the 3,167 N from Skotte and Fallentin (2008). It is possible these studies had methodological differences such as the height of the bed or distance of repositioning which were not described by Skotte and Fallentin (2008). The spinal compression estimates in the current study appear to be lower than an electromyography-assisted model. For the only comparable task evaluated by Marras et al. (1999), boosting a 50-kg patient with a draw sheet resulted in 3,861 N when averaging caregivers working on both sides of the bed compared to 2,173 N in the current study for the 50-kg patient.
Of the literature that reported hand forces when repositioning patients, Bartnik and Rice (2013) evaluated hand forces in a manner most similar to the current study. When boosting 29 individuals with a mean mass of 66 kg, a single caregiver produced a mean hand force of 222 N using a draw sheet (Bartnik & Rice, 2013) which is similar to the 203 and 287 N for the 50- and 77-kg patients from the current study. Similar to the current study, Lloyd and Baptiste (2006) measured hand force for a single investigator performing a lateral transfer of a mannequin and found the greatest forces for a draw sheet, followed by models of FRS, and the least force for two AARDs.
Repositioning aids appeared to reduce physical stress commensurate with their friction reduction, which is logical because the forces required to reposition patients were primarily horizontal. The AARD resulted in the lowest friction because of the cushion of air it generates between the AARD and the bedsheet. The pair of low-friction sheets for the FRS product had resulted in considerably lower friction than the single TAP sheet. Friction is also a function of normal force, which increases with patient weight and explains why physical stresses were greater when moving heavier patients.
This was the first study to provide a broad comparison of different repositioning aids for various patient weights across several repositioning activities. However, the study necessarily included only the most representative repositioning aids and three patient weights. This study only considered spine compression loads, estimated muscle activity, and hand loads. For the activities studied, hand forces appear to be the greatest indicator of risk of injury. Although pull forces are associated with injury, this causal relationship is not as well established as for lifting and back injury. The hand forces associated with repositioning patients may partially explain the high incidence of shoulder and neck injury in healthcare workers, but a lack of strong shoulder biomechanical models that explain the mechanism for injury limits the ability to develop tolerance thresholds for shoulder injury.
The system for measuring hand force was specially designed to minimize the effect on posture, but a 7-cm spacing between the sensors and the attachment to the sheet likely had a small effect. All trials studied the caregiver while performing care on the patient’s left side of the bed and it is reasonable to expect there could be small differences in posture or force generation when caregivers stand on the opposite side of the bed. The current study aimed to evaluate repositioning activities as they are commonly performed, but researchers have shown that alternative methods such as pulling from the head of the bed can reduce pull forces (Fray & Holgate, 2018).
These findings provide a general indication of which interventions might be suitable for which patient weights, but practitioners should exercise caution if using these results to establish policy. Two patients of the same weight may require different forces to reposition based on body habitus or amount of deformable soft body tissue. The recommendations in Figure 5 draw on guidelines that considered worker populations that might be younger, thinner, and healthier than the population of caregivers in many healthcare facilities. Furthermore, these repositioning activities might require more dynamic forces than Snook and Ciriello (1991) and may occur in a more stressful work environment which could increase muscle coactivation (Marras et al., 2000). Based on these considerations, the comparisons to psychophysical thresholds and the results in Figure 5 may not be sufficiently conservative to protect all healthcare workers.
This study did not evaluate the physical stresses required to place the repositioning aids under the patients, but the relatively low forces associated with turning the patient suggest that placing repositioning aids can be installed safely. These results are consistent with previous studies of patient turning (Budarick et al., 2019; Wiggermann, 2016). Alternatively, using an electromyography-assisted model Nagavarapu et al. (2017) identified spine compression forces that exceeded 3,400 N when applying slings under certain parameters. However, these risks were mitigated when the bed was elevated to knuckle height of the caregiver or higher. Consistent with previous studies (Budarick et al., 2019; Wiggermann, 2016), turn assist tended to reduce the physical stresses on caregivers and may be particularly appropriate for turning heavier patients or reducing cumulative load on caregivers. Turn assist has also been suggested for use in lateral repositioning to reduce pull force (Wiggermann, 2016). Integrated features such as turn assist serve as an example of interventions that are compatible with caregiver workflow and may be sustainably adopted because they require few extra steps.
The results of the current study clearly indicate that of the systems studied, the AARD is the only repositioning aid that is effective at mitigating risk of injury for most patient weights and repositioning activities. Because its thickness can contribute to the risk of pressure injuries if left under a patient, the AARD must be placed under the patient before repositioning and removed after each use. The AARD also requires the connection of an external blower which must be retrieved and disinfected by healthcare workers. The inclusion of the AARD for the boosting and lateral repositioning activities demonstrates differences in forces across products, but in practice the AARD is unlikely to be used for boosting and lateral repositioning because of the difficulty of placing and removing the product from under the patient. In fact, to turn the patient to place the AARD, a lateral reposition might first be required to make space for the turn. These extra steps and the additional cumulative workload should be considered when identifying suitable applications for the AARD.
In practice, a repositioning sheet together with a mechanical overhead lift can provide the most robust option for repositioning activities with the least impact to caregiver workflow. The repositioning sheet can be used to boost, laterally reposition, transfer, and turn the patient; and because its fabric is thin enough and breathable it can be left under the patient without significant impact to risk of pressure injury (Nelson et al., 2014). By not having to place the sheet under the patient, much greater compliance to safe patient handling protocols can be achieved. Furthermore, the mechanical lifting equipment can be used for other safe patient handling practices that include seated transfers from bed, toileting, and gait training. For these reasons, the use of lift equipment has been recommended by professional groups such as the American Nurses Association (2013) and the Facility Guidelines Institute (Cohen et al., 2010), as well as the National Institute for Occupational Safety and Health (2013).
Conclusion
When manually repositioning patients with a draw sheet, spine compression and hand forces exceeded recommended limits for many patient weights and repositioning activities. Repositioning aids reduced physical stresses, but the TAP and FRS did not adequately mitigate the risk of injury across all patient weights. Spine forces and hand forces did not exceed recommended limits when using the AARD for the patient weights tested. However, placing and removing the AARD from under the patient may increase the cumulative workload on caregivers. Patient weight should be considered when determining which repositioning aids to use. These findings reinforce recommendations for using mechanical lift equipment, which should be considered as a robust alternative to repositioning aids that can safely accommodate all patients regardless of weight.
Key Points
FRS and “TAP” sheets reduce physical stresses on healthcare workers when repositioning patients, but these devices are insufficient to properly mitigate risk of musculoskeletal injury for most patient weights.
For the repositioning activities tested, psychophysically developed guidelines for pull force were exceeded more often than the recommended limits for spine loading.
To safely move dependent patients, a robust solution requires mechanical lifts and may utilize air-assisted transfer devices.
Footnotes
Author Biographies
Neal Wiggermann is a specialist research scientist in Human Factors and Ergonomics at Hill-Rom. He received his PhD in industrial and operations engineering from the University of Michigan in 2011.
Jie Zhou is an advanced research scientist at Hill-Rom. He received his PhD in ergonomics and biomechanics from the University of California, Davis, in 2018.
Nancy McGann is a system manager of Ergonomics and Safe Patient Handling at SCL Health. She received a BS in Physical Therapy from Boston University in 1989.