
Abstract
Objective
The aim of this study was to determine and verify the optimal location of the motion axis (MA) for the seat of a dynamic office chair.
Background
A dynamic seat that supports pelvic motion may improve physical well-being and decrease the risk of sitting-associated disorders. However, office work requires an undisturbed view on the work task, which means a stable position of the upper trunk and head. Current dynamic office chairs do not fulfill this need. Consequently, a dynamic seat was adapted to the physiological kinematics of the human spine.
Method
Three-dimensional motion tracking in free sitting helped determine the physiological MA of the spine in the frontal plane. Three dynamic seats with physiological, lower, and higher MA were compared in stable upper body posture (thorax inclination) and seat support of pelvic motion (dynamic fitting accuracy). Spinal kinematics during sitting and walking were compared.
Results
The physiological MA was at the level of the 11th thoracic vertebra, causing minimal thorax inclination and high dynamic fitting accuracy. Spinal motion in active sitting and walking was similar.
Conclusion
The physiological MA of the seat allows considerable lateral flexion of the spine similar to walking with a stable upper body posture and a high seat support of pelvic motion.
Application
The physiological MA enables lateral flexion of the spine, similar to walking, without affecting stable upper body posture, thus allowing active sitting while focusing on work.
Keywords
Introduction
Up to 72% of the population in industrialized countries performs sedentary work (OECD, 2014). The average daily sedentary time of the general population is between 8 and 10 hours (Colley et al., 2011; Craig, Mindell, & Hirani, 2008; Matthews et al., 2008). Office workers in particular spend most of their working hours (around 75%) in sitting postures and only around 8% in non-static activities (Gorman et al., 2013). The risk of low back pain increases with prolonged sitting in unfavorable postures (Lis, Black, Korn, & Nordin, 2007; Pope, Goh, & Magnusson, 2002) and static sitting with continuous isometric muscular activity (van Dieën, de Looze, & Hermans, 2001; Vergara & Page, 2002).
Spinal research has shown that allowing and supporting spinal motion is better for the health of the spine than fixed postures, particularly for the intervertebral discs (Pope et al., 2002). To promote active sitting, designers began to make two types of dynamic office chairs. They made backless chairs unstable and equipped conventional office chairs with movable mechanics for seat and backrest. Backless chairs attempt to improve upright posture and active sitting. However, they increase spinal flexion and reduce postural sway, sway velocity, and muscle activity (Grooten, Conraddson, Äng, & Franzén, 2013). Other researchers showed that backless chairs do not improve sitting postures (Annetts et al., 2012; Ellegast et al., 2012; Gregory, Dunk, & Callaghan, 2006; O’Sullivan, McCarthy, White, O’Sullivan, & Dankaerts, 2012). They require strong continuous lumbar muscular activity to maintain an upright sitting posture, which may lead to discomfort or pain (Kingma & van Diëen, 2009; O’Sullivan, O’Sullivan, O’Keeffe, O’Sullivan, & Dankaerts, 2013; van Dieën et al., 2001; Vergara & Page, 2002). Relaxed sitting without the use of a backrest results in a decreased lumbar lordosis with increased cervical and thoracic muscular activity associated with low back pain (Caneiro et al., 2010; Womersley & May, 2006). An office chair should therefore have a backrest. The dynamics of chairs with backrests are commonly limited to backward tilt (sagittal plane) and rotation (horizontal plane) (Ellegast et al., 2012; Groenesteijn, Vink, de Looze, & Krause, 2009). Motion in the sagittal plane is a combined tilting of the backrest and seat in a predefined ratio (usually around 3:1). It facilitates relaxation of back muscles, relieves load on the spine, and increases trunk thigh angle (Bush & Hubbard, 2008; Harrison, Harrison, Croft, Harrison, & Troyanovich, 1999; Pope et al., 2002; van Dieën et al., 2001; Vergara & Page, 2002). However, backward tilt is associated with large upper body motion away from the office desk and a distracting change in the field of view (Bush & Hubbard, 2008; van Dieën et al., 2001). The rotation in horizontal plane is a combined motion of seat and backrest (1:1 ratio). Rotation can facilitate the work flow since the subject can use the backrest even when rotating the chair. There is however no evidence that tilting and rotating office chairs increase the activity of the seated subject (Ellegast et al., 2012; Jensen & Bendix, 1992; van Dieën et al., 2001).
Office work requires a stable position of thorax and head to leave the view of work undisturbed and facilitate use of keyboard and mouse (Bush & Hubbard, 2008; van Dieën et al., 2001). Thus, current dynamic office chairs, which facilitate backward tilting and rotation, might not promote active sitting as intended, presumably because they lead to large upper body motion with a distracting change in the field of view. Consequently, they impair the operators’ performance, which in turn restricts their ability to move.
To promote active sitting with a stable upper body posture, this study investigates an additional degree of freedom (DOF) for the seat of an office chair with backrest. The additional DOF extends existing seat dynamics to the frontal plane. The rhythmic movement sequences of walking (pelvic obliquity with lateral spine flexion) inspired the additional DOF, a chair mechanism with a pivoting seat in the frontal plane around a motion axis (MA) within the chair user’s body. This might maintain the thorax and head in a stable position to focus on work task while the dynamic seat allows lateral flexion of the spine.
However, the optimal location of the MA in terms of lateral flexion of the spine with a stable upper body posture is unknown. The aim of the present study was therefore to adapt the kinematics of the additional DOF to unconstrained lateral flexion of the spine by finding the physiological MA, followed by the implementation of these kinematic properties into the seat of a dynamic office chair. The study subsequently compared segmental kinematics between the chair with physiological MA and two chairs with a lower and higher MA. Since the additional DOF was inspired by the lateral spine flexion of walking, the spine motion of active sitting has also been compared to the motion when walking.
Method
This study was divided into two substudies (Figure 1). Study 1 investigated the location of the physiological MA, defined as the anterio-posterior axis around the lumbar spine rotates when pelvis and spine are not restricted by external factors. The location of the physiological MA subsequently saw implementation in the seat of a new office chair (chair C) and was compared to two seats with different MA in Study 2 (Figure 1). An additional comparison was made with data from literature about walking. Regional and institutional ethics committees approved the whole study.
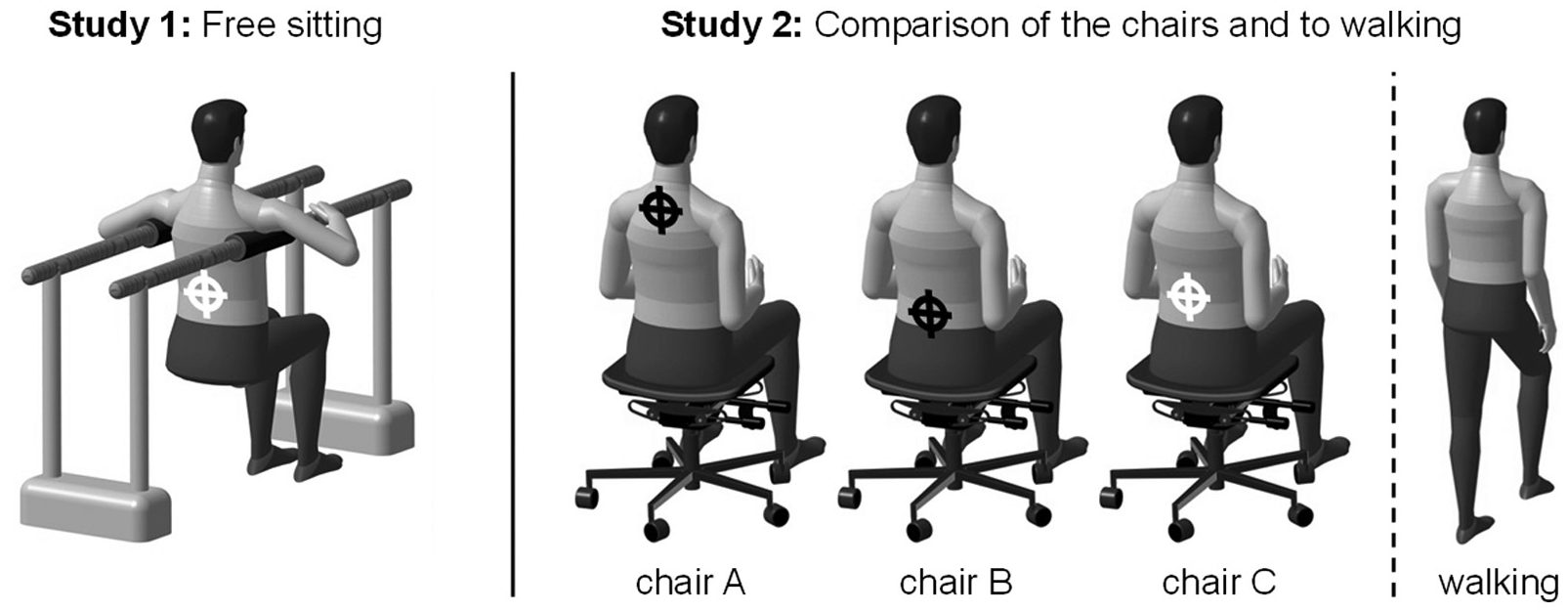
Structural overview of the conducted studies. In Study 1, pelvis and lumbar spine rotation around an anterio-posterior axis in free sitting were analyzed in order to find the physiological motion axis (bright circled cross), which was subsequently implemented in a new office chair (chair C) and compared to two chairs having the motion axis higher (chair A) or lower (chair B). Additional comparison of lateral spine flexion between active sitting on chair C and literature data of walking has been carried out.
Participants
Subjects without self-reported chronic complaints in the back and neck region over the past year or previous spine surgeries were recruited for both studies. Further inclusion criteria and participant characteristics appear in Table 1. Subjects were unfamiliar with the dynamic chairs. All participants gave their informed consent. As no differences in terms of participant characteristics (Table 1) between office workers and students were observed, the groups were pooled. For Study 2, eight new participants of both genders were recruited and five of Study 1 were lost due to illness and vacation. Subject characteristics did not differ between the two studies (based on Wilcoxon test).
Inclusion Criteria and Subject Characteristics of Study 1 and 2
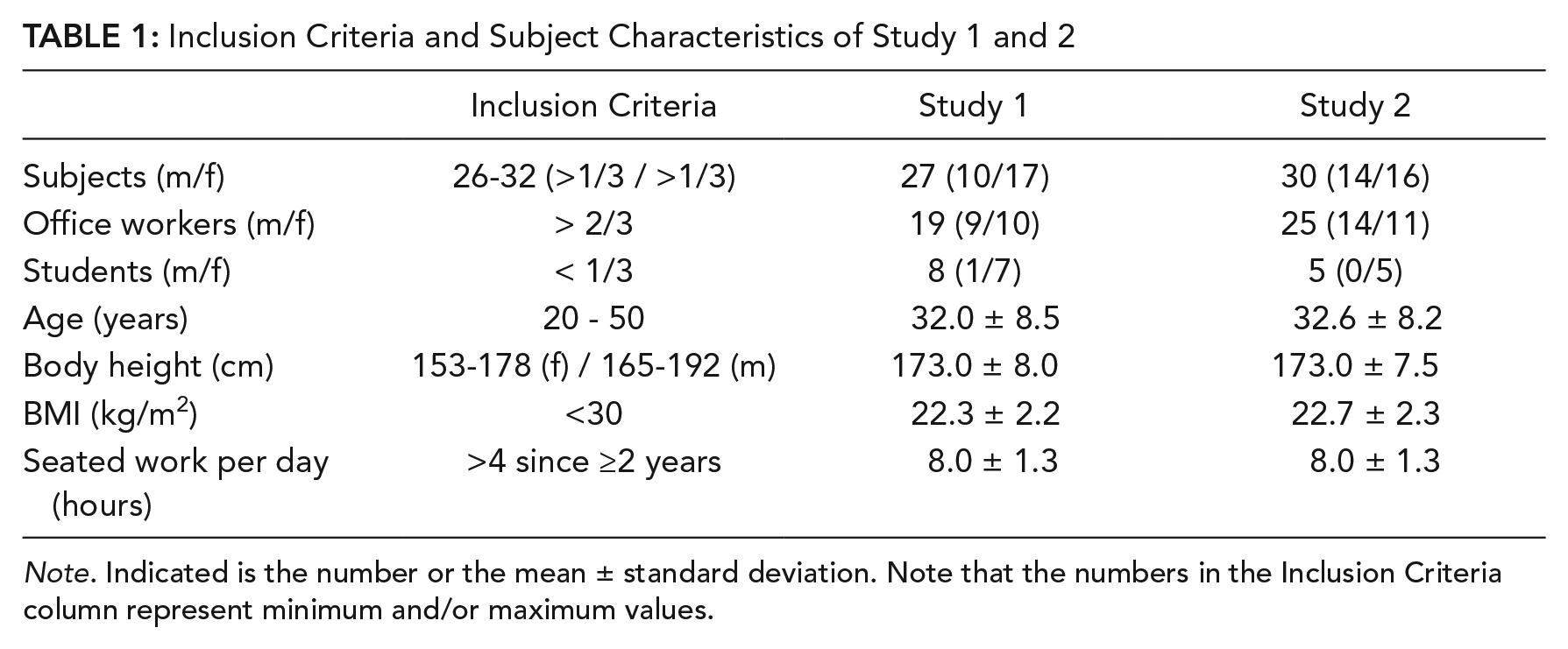
Note. Indicated is the number or the mean ± standard deviation. Note that the numbers in the Inclusion Criteria column represent minimum and/or maximum values.
Recording System
Ten infrared cameras of the Vicon MX system (Oxford Metrics Group, Oxford, GBR) with a recording frequency of 200 Hz and the Plug-in-Gait marker model (Davis, Õunpuu, Tyburski, & Gage, 1991; Kadaba, Ramakrishnan, & Wootten, 1990) with additional markers on the spine were used (Table 2). The Software Vicon Nexus 1.7.1 was used for subsequent three-dimensional marker reconstruction.
Definition of Marker Placement
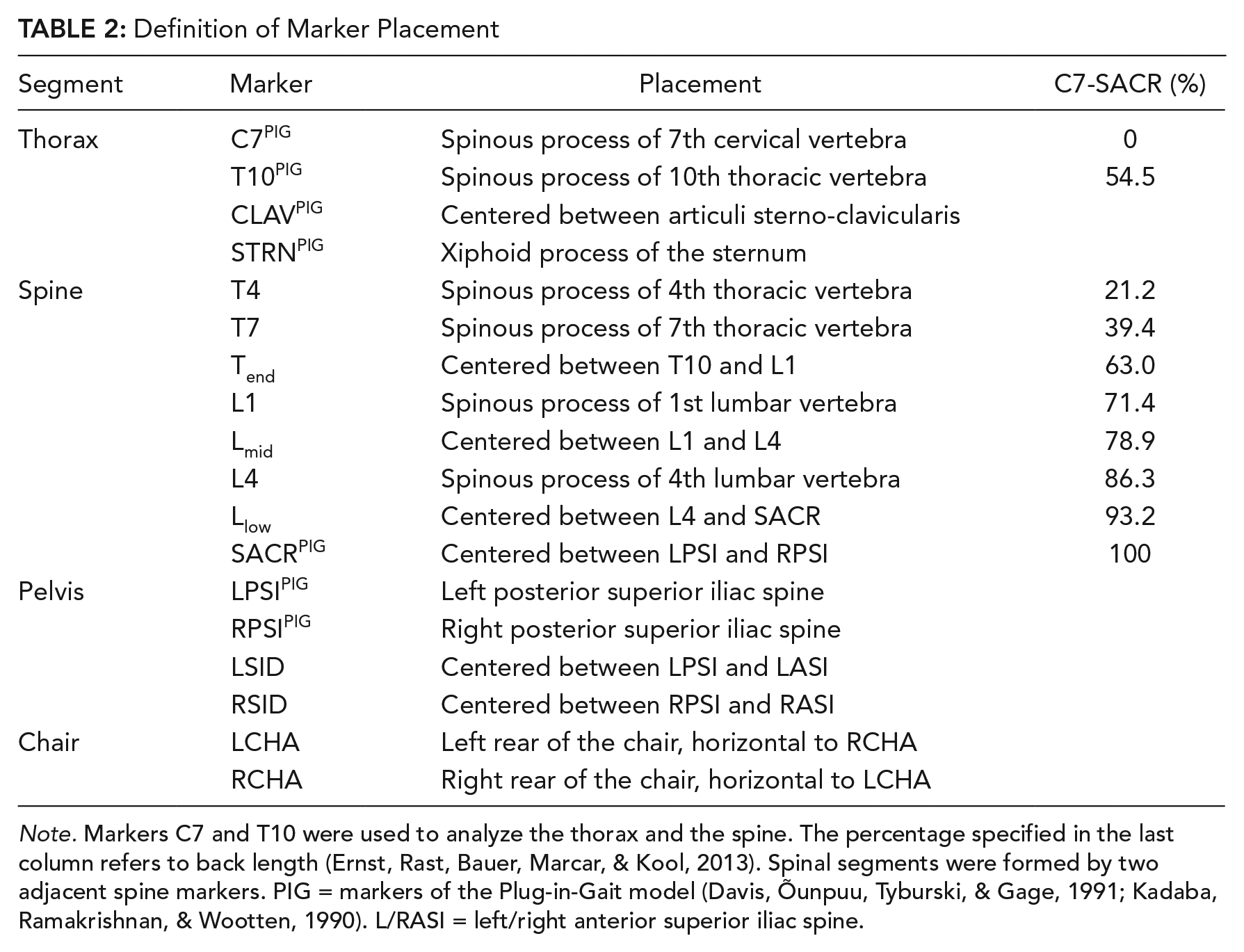
Note. Markers C7 and T10 were used to analyze the thorax and the spine. The percentage specified in the last column refers to back length (Ernst, Rast, Bauer, Marcar, & Kool, 2013). Spinal segments were formed by two adjacent spine markers. PIG = markers of the Plug-in-Gait model (Davis, Õunpuu, Tyburski, & Gage, 1991; Kadaba, Ramakrishnan, & Wootten, 1990). L/RASI = left/right anterior superior iliac spine.
Conditions and Tasks
Study 1
The location of the physiological MA was analyzed using a free sitting condition as shown in Figure 2. The parallel bars supported the body weight and minimized upper body motion according to the aim of the additional DOF. Since we assumed a different spinal motion pattern in relation to the range of motion (ROM) (Zwambag & Brown, 2015), every subject performed two different tasks to study their influence on the physiological MA: first a lateral rotation of the pelvis and the lumbar spine around an anterio-posterior axis in a spontaneously preferred ROM (spontaneous ROM task) with an acoustic rhythm of one beat per second to standardize the motion cycle duration and then a lateral rotation with maximum ROM (maximum ROM task) with a self-determined duration. Every recording consisted of six consecutive motion cycles (left-right motions).
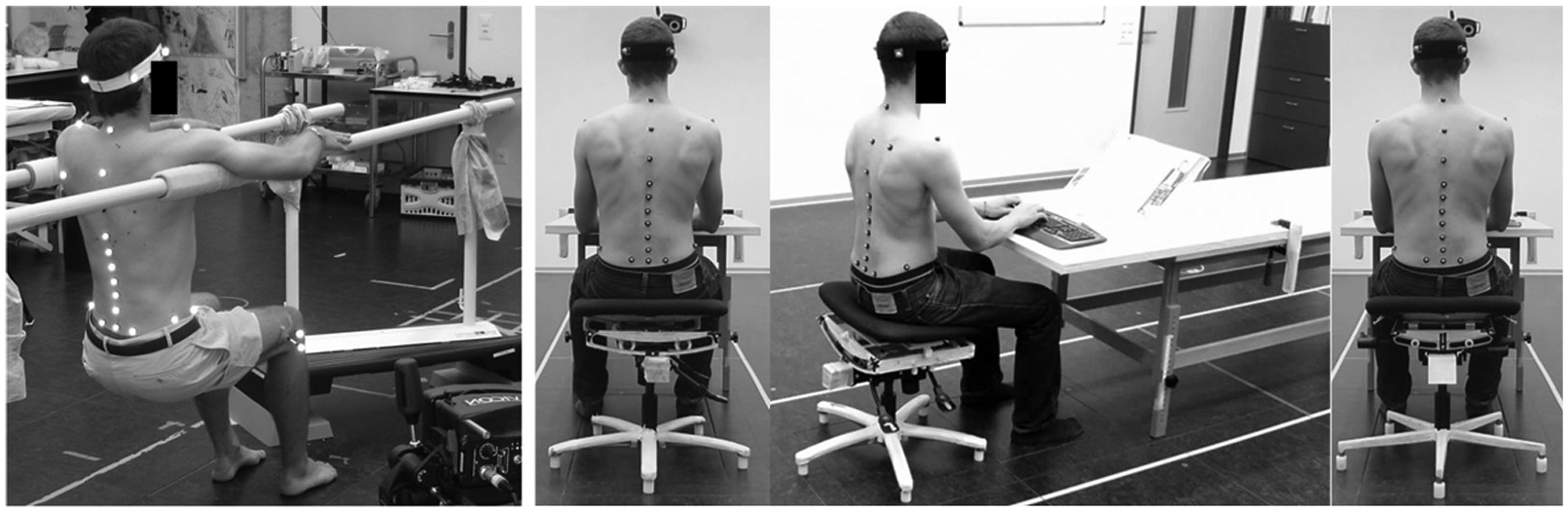
Subject in free sitting without any external force impacting pelvis and spine in Study 1 (left), and sitting on chair A, B, and C (from middle to right) in Study 2. In Study 2, subjects had no opportunity to see the slight differences in chair design during the measurement since the chairs were visually covered until the subject sat down. All chairs had the same seat and were only different in terms of the location of the motion axis.
Study 2
To study the influence of the MA location on the subjects’ motion behavior while working, three dynamic chairs were used (rotavis AG, Winterthur, CHE). All chairs were equipped with the additional DOF but different MA locations. The MA location was predefined either at the height of the clavicle (chair A, Schünke, Schulte, & Schumacher, 2007), umbilicus (chair B, Schünke et al., 2007), or at the MA level determined by Study 1 (chair C). The chairs were all constructed using the average anatomical landmark of the study population. The height of the clavicle was hypothesized to be the optimal MA location if the subjects move the seat in a small ROM with a relatively stiff spine in order to focus on the reading task. The level of the umbilicus was hypothesized to be the optimal location if the subjects move the seat in a large ROM with increased pelvic inclination due to the different loading condition compared to Study 1 (compressive vs. tensile load on the spine and pelvis). The chairs were compared by investigating the same ROM tasks as conducted in Study 1 since literature reports a different motion pattern of the spine in relation to loading condition and ROM (Bell et al., 2016; Lengsfeld, van Deursen, Rohlmann, van Deursen, & Griss, 2000; Zwambag & Brown, 2015). As office workers with low back pain might benefit from a particular spinal ROM training in sitting, the suitability of the chair could be analyzed by investigating the maximum ROM task. The construction of the additional DOF consists of four ball-bearings that can be moved in a guide rail below the seat. Accordingly, the investigated chairs differed in the shape of the guide rail but were equipped with identical seats (shape and cushion, Figure 2). The different loading conditions in this study compared to Study 1 made it necessary to increase the speed of the acoustic rhythm to two beats per second for the spontaneous ROM task. Every recording consisted of six consecutive motion cycles.
Outcome Measures
Study 1
The primary outcome measure of Study 1 was the location of the physiological MA to inform the development of a physiological DOF that was investigated in Study 2. Spontaneous and maximum ROM tasks were performed to investigate whether the location of the physiological MA depends on ROM, which would influence the construction of the dynamic office chair. Additionally, the relationship between the location of the physiological MA and anthropometric data was analyzed.
Study 2
The primary outcome measures of Study 2 were (a) thorax inclination, as measure of the upper body stability, and (b) dynamic fitting accuracy, as measure of the level of seat support of pelvic motion. We expected that thorax inclination would be the lowest on the chair with the physiological MA (chair C), meaning that subjects can rotate the pelvis and the lumbar spine around the anterio-posterior axis while holding the upper body in the most stable position. We also expected the dynamic fitting accuracy to be the highest for this chair, meaning that the angular difference between pelvis and seat inclination is the lowest.
Secondary outcome measures were (c) thorax translation to describe the upper body motion in relation to MA location, (d) lateral spine flexion as a measure for the actual spinal motion, and (e) segmental lateral spine flexion during the spontaneous ROM task to compare the seated kinematics with literature data of upright walking (Lee & Park, 2011; Syczewska, Öberg, & Karlsson, 1999). Because office workers try to maintain the thorax in a stable position (Bush & Hubbard, 2008; van Dieën et al., 2001), we expected no differences between different MA locations regarding thorax translation (as opposed to thorax inclination). Neither did we expect any differences regarding the actual lateral spine flexion. The comparison with walking data helped analyzing whether we had implemented the additional DOF adequately as planned.
Procedure
Study 1
The parallel bars were individually adjusted to the height of the anterior axillary fold, measured in upright sitting posture (defined by an angle of 90° in the ankle, knee, hip/pelvis, and a straight back). Anatomical landmarks were palpated according to the recommendation of Ernst, Rast, Bauer, Marcar, and Kool (2013) and documented to ensure identical marker placement in both studies. To become familiar with the lateral rotation of the pelvis and the lumbar spine around an anterio-posterior axis, subjects sat prior to the recordings on a prototype of the office chair equipped with the additional DOF for one minute (MA similar to chair A) while focusing on the acoustic rhythm. In order not to predefine the seat motion, the prototype was equipped with a supplementary tilt mechanism that provided an additional lateral inclination of the seat by ±15° without resistance. No further instructions were given. Recording in free sitting (without chair, Figure 2) consisted of three spontaneous and one maximum ROM task with short, self-chosen breaks in between.
Study 2
Participants adjusted the seat height of the chairs as in upright sitting in Study 1. Table height was adjusted 2 cm above the elbow height with the upper/lower arm in vertical/horizontal position. Prior to the measurement, subjects sat on the chair for one minute to become familiar with it. The chair order was randomized, and subjects were blinded to chair type. Three spontaneous ROM tasks and three maximum ROM tasks were recorded while subjects were reading a magazine (placed on the table in 45° to horizontal in a distance of 80 cm) and kept the ball of the thumb on the palm rest of a keyboard to simulate focused work with a fixed view (Figure 2). To eliminate interference between conditions, subjects walked on a treadmill for one minute at 3.6 km/h. The treadmill was set to 24% inclination to increase pelvic and spinal motion in the frontal plane (Lee & Park, 2011).
Data Analysis
Matlab 2012b (MathWorks Inc., Massachusetts, USA) was used for calculations and statistical analysis. The four cycles in the middle of each recording were evaluated. The y-direction of the coordinate system pointed along the viewing direction, the x-axis to the right, and the z-component in the cranial direction (Figure 3).
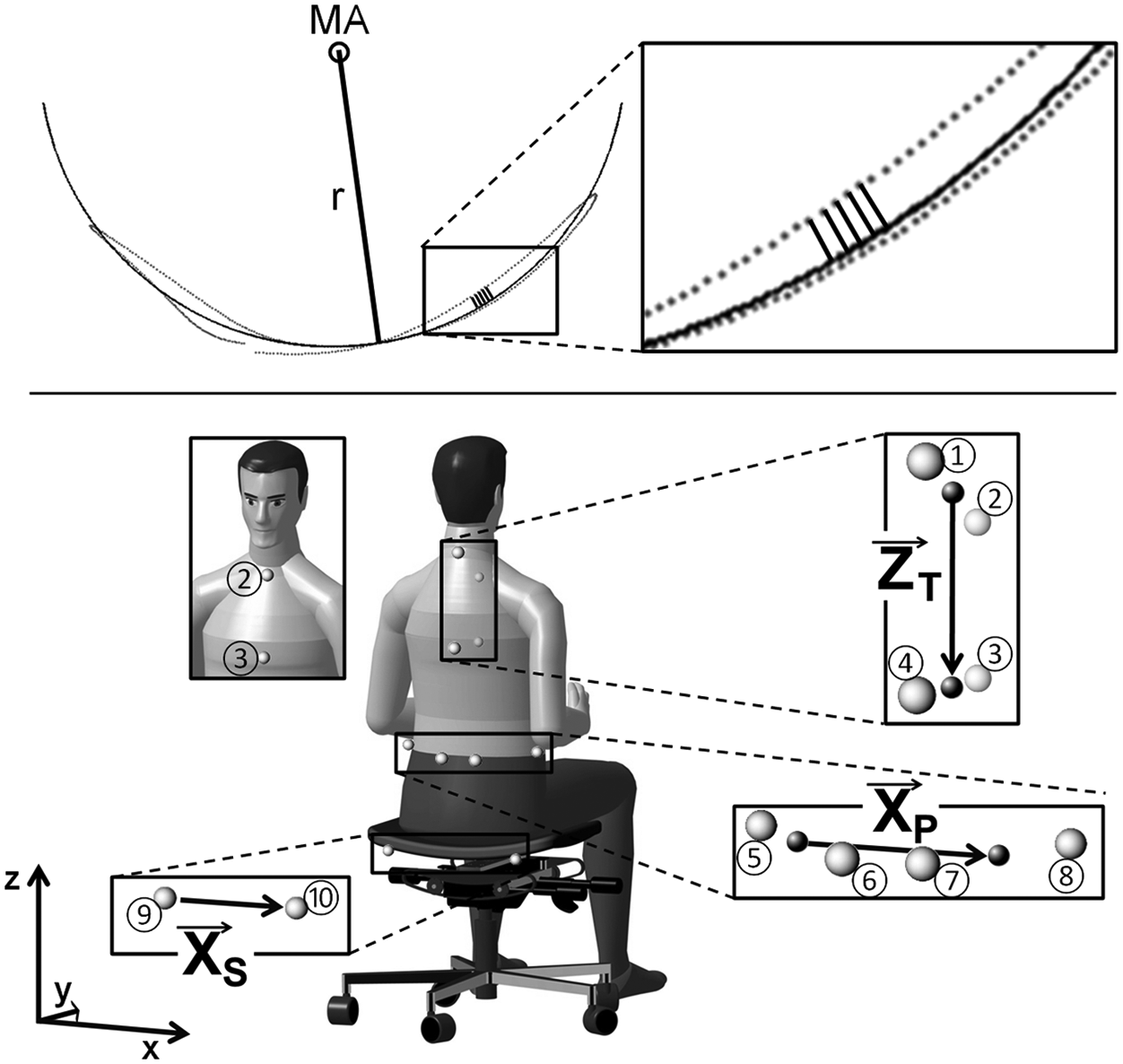
Primary outcome measure of (top) Study 1 and (bottom) Study 2. Top: Motion axis (MA) of selected marker in one motion cycle (to left and right, dotted line), approximated with circular least-square fitting (circular line) by minimizing the sum of all squared orthogonal deviations (black lines, shown for five consecutive time points) through adjusting circle size (radius r) and position (MA). Bottom: Directional vectors of thorax (ZT) to analyze thorax inclination as well as pelvis (XP) and seat (XS) to analyze dynamic fitting accuracy. ZT from midpoints of marker C7 (1) and CLAV (2) to STRN (3) and T10 (4); XP from midpoints of LSID (5) and LPSI (6) to RPSI (7) and RSID (8); XS from LCHA (9) to RCHA (10). For marker abbreviations, see Table 2.
Study 1
To determine physiological MA, motion trajectories in the frontal plane of the two most caudal spine markers were approximated using a least-square fitting (Pratt, 1987). The squared sum of the shortest distances between a fitted circle line and the recorded data points of a single left-right cycle were minimized by adjusting circle size and position (Figure 3). Motion trajectories were therefore centered (by subtracting the mean) to calculate the cross-product over each cycle. After time normalization, the coefficients of the characteristic polynomial were derived and Newton’s method implemented (starting at zero) to finally calculate the circle parameters. This approach required a lateral marker translation of at least 2 cm. Motion cycles below this threshold were not analyzed. MA of spontaneous and maximum ROM tasks were analyzed and compared.
Study 2
ROM for every cycle was calculated, halved, and averaged over all cycles per subject. Thorax inclination was analyzed using a directional vector pointing from midpoints of STRN and C7 to CLAV and T10 (Figure 3). Furthermore, the direction of thorax inclination relative to pelvis inclination was determined. The dynamic fitting accuracy was determined by calculating angular difference between directional vectors of the seat (pointing from LCHA to RCHA) and the pelvis (pointing from midpoints of LSID and LPSI to RSID and RPSI) (Figure 3).
The lateral translation of the thorax was analyzed by calculating ROM along x-axis of the midpoint of all thoracic markers. The lateral spine flexion was calculated from the difference between the directional vectors of the most cranial (C7 to T4) to the most caudal segment (Llow to SACR). To ensure a meaningful comparison between the upper body kinematics on chair C and walking, segmental lateral spine flexion was compared to literature on spinal motion in walking (Lee & Park, 2011; Syczewska et al., 1999). Spinal segments were therefore considered separately and divided into thoracic (from C7-T4 to Tend-L1) and lumbar spine (from Tend-L1 to Llow-SACR, see Table 2).
Statistical Analysis
Study 1
Spontaneous and maximum ROM tasks were compared using a nonparametric, two-sided Wilcoxon test. To describe the relationship between the location of the physiological MA and body height, Pearson correlation coefficient (CCPearson) was calculated. The level of significance was .01.
Study 2
Thorax inclination, dynamic fitting accuracy, thorax translation, and lateral spine flexion in different chair conditions were compared using Friedman ANOVA. If significant differences appeared, post hoc analysis using Wilcoxon test identified differences between individual conditions. The level of significance was .01.
Results
Study 1
In both tasks, all subjects initiated lateral rotation by movement of the pelvis and the spine and kept their thorax and head relatively stable. The physiological MA was determined in 9 (spontaneous ROM task) and 17 (maximum ROM task) subjects, respectively. Other subjects did not reach the predefined threshold for marker translation. No difference appeared in relation to ROM (n = 9). On average, the physiological MA was 20.3 ± 7.2 cm (mean ± standard deviation) above SACR marker (maximum ROM task), or at the level of T11 (Figure 4). Subsequently, chair C used in Study 2 was adjusted to the average physiological MA. A significant positive correlation to MA height appeared for body height (absolute: CCPearson = 0.70, relative: CCPearson = 0.68, p < .01) (Figure 4).
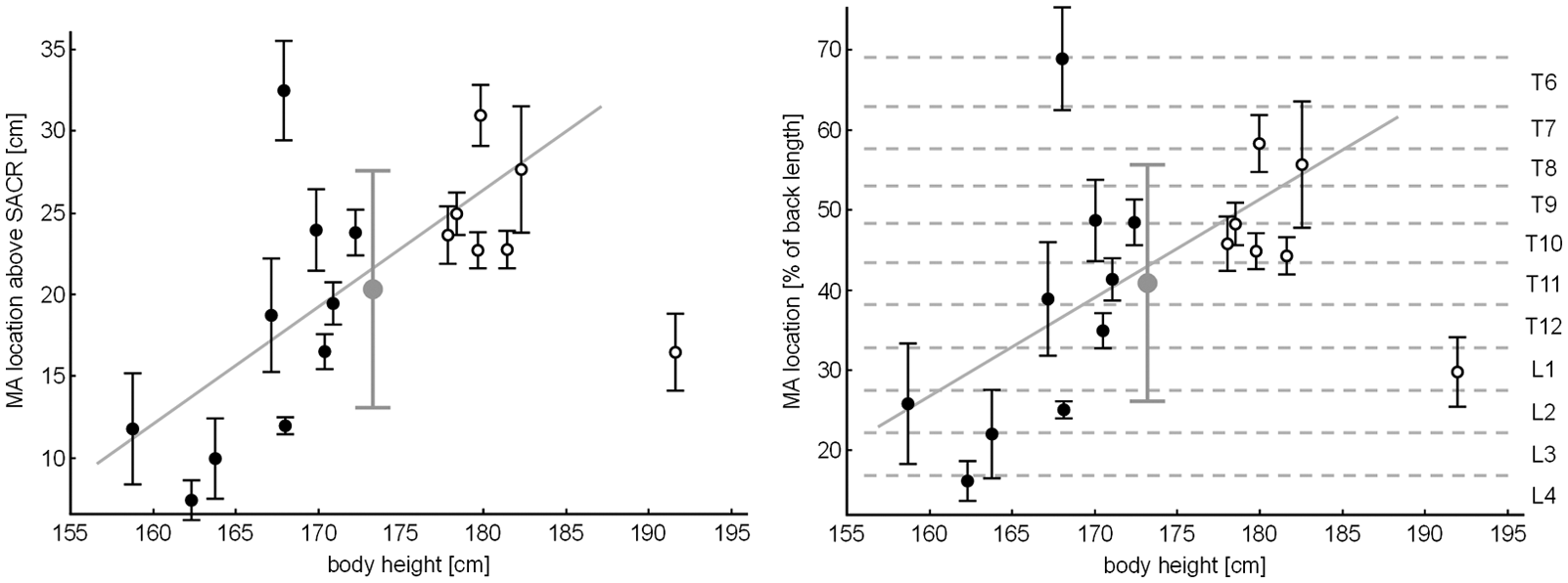
Motion axis (MA) location above SACR marker (left) and relative to back length (right) plotted against body height for women (solid circles) and men (circular lines) with intra-individual standard deviation (SD) and mean ± SD of all subjects (grey). The grey diagonal lines represent least-square fitting. Vertebral levels (sixth thoracic to fourth lumbar vertebra) are visually divided (dotted grey lines) and indicated on the right. The subject far right (body height > 190 cm) was an outlier (Cook’s distance = 1.4) and excluded to calculate correlation coefficient.
Study 2
Thorax inclination
In the spontaneous ROM task, the lowest thorax inclination was observed for chair C, followed by chair B and chair A (p < .01 to C, Figure 5). While 90% and 70% of the subjects inclined thorax and pelvis in opposite directions on chair B and C, 53% inclined thorax and pelvis in the same direction on chair A.
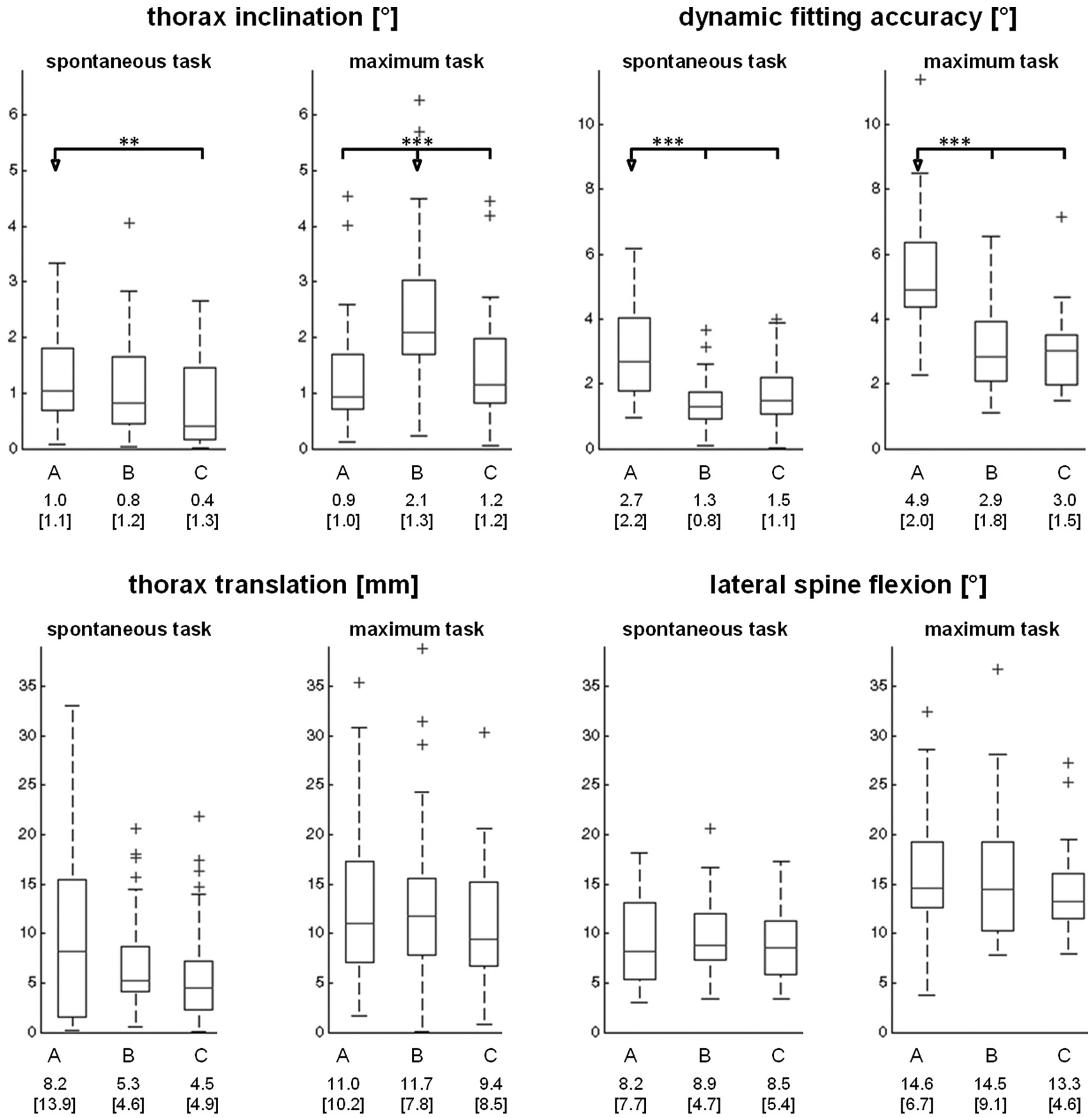
Outcome measures of Study 2: (a) thorax inclination, (b) dynamic fitting accuracy (expressed inversely as difference between pelvis and seat inclination), (c) thorax translation, and (d) lateral spine flexion for the motion in spontaneous and maximum ROM task on chair A, B, and C. Indicated and explicitly specified are the median and the inter-quartile-range (iqr = 25th to 75th percentile, indicated in brackets). The crosses mark the outliers (value more than 1.5 iqr higher than the 75th percentile). Statistical differences marked with asterisks (**p ≤ .01. ***p ≤ .001).
In the maximum ROM task, thorax inclination was significantly highest on chair B (p < .001). While 56% of the subjects inclined the thorax and pelvis in the same direction (chair A), 100% (B) and 83% (C) inclined it in the opposite direction.
Dynamic fitting accuracy
Dynamic fitting accuracy was significantly lowest for chair A (p < .001) in both tasks. No differences emerged between chair B and C (Figure 5).
Thorax translation
In both tasks, the range of thorax translation was statistically indistinguishable (Figure 5).
Lateral spine flexion
Subjects laterally flexed the spine in both tasks in the same range on all chairs (Figure 5).
Comparison between the chair with physiological MA and walking
Lateral flexion ROM of the upper thoracic spine was slightly lower than in walking (3.4° ± 2.3° vs. 4.4° ± 1.6°), and flexion ROM of the lumbar spine was greater (5.3° ± 2.0° vs. 2.8° ± 0.8°) (Lee & Park, 2011). However, the most stable segment during sitting and walking appeared both times at the same level (T7-T10, Table 3) (Syczewska et al., 1999).
Lateral Flexion of the Spine While Sitting on the Chair With Physiological Motion Axis (Chair C) Compared to Walking (Syczewska, Öberg, & Karlsson, 1999, n = 10)
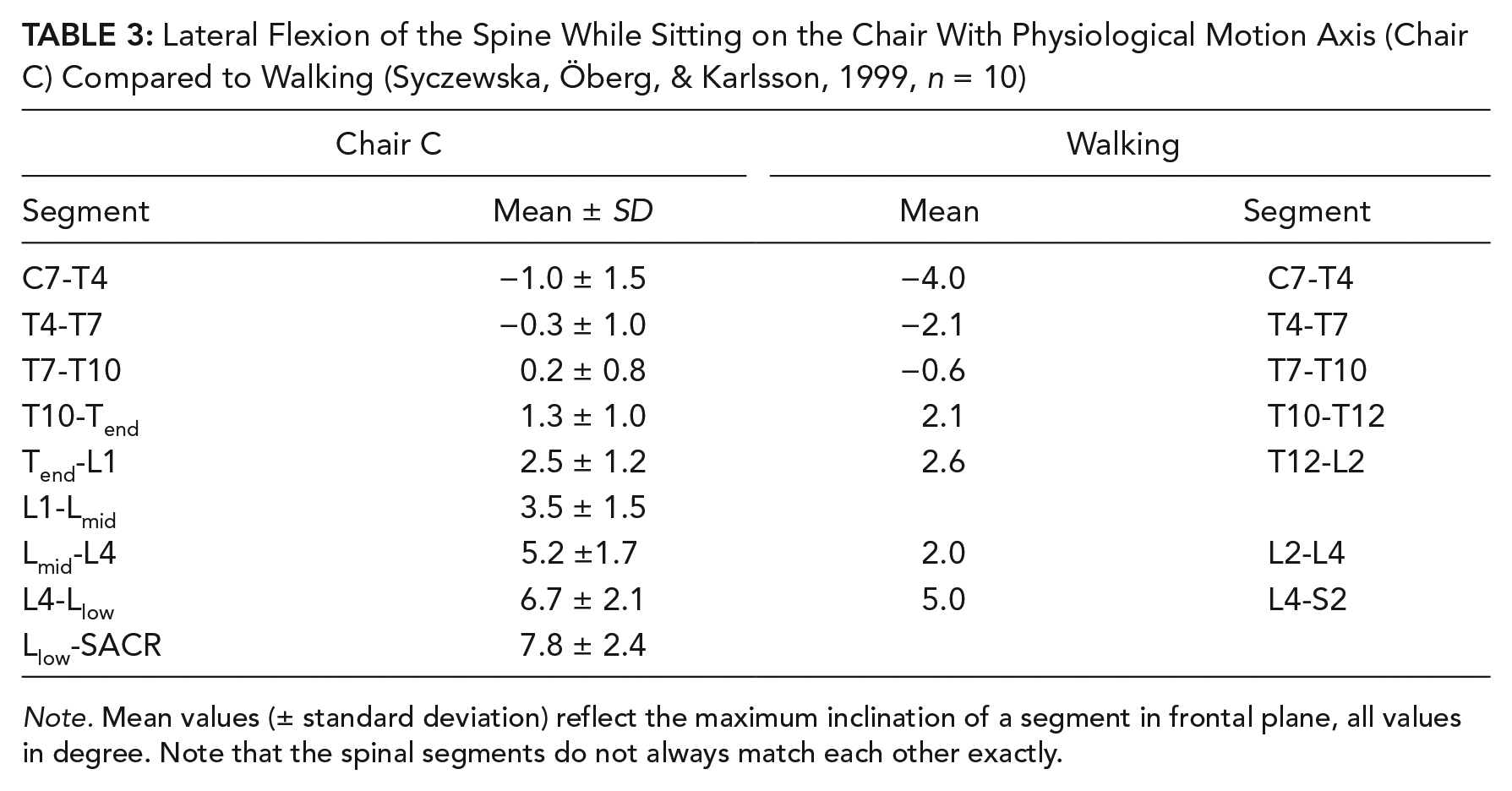
Note. Mean values (± standard deviation) reflect the maximum inclination of a segment in frontal plane, all values in degree. Note that the spinal segments do not always match each other exactly.
Discussion
In this study, we analyzed the physiological motion of the spine in the frontal plane to derive the boundary condition for an additional DOF of the seat of a dynamic office chair. Since office workers try to maintain a stable upper body location to preserve their work performance (Bush & Hubbard, 2008; van Dieën et al., 2001), the additional DOF supports pelvis motion and lateral spine flexion without affecting stable upper body posture. Although thorax motion was very small on all investigated chairs (≤1° and <1 cm in spontaneous ROM task), our results suggest that the chair with physiological MA allows the best active sitting without affecting stable upper body posture.
Study 1: Physiological MA
The physiological MA was located at the level of the 11th thoracic vertebra and did not depend on ROM and motion speed. Body height correlated with MA height, not only absolutely but also relatively, meaning that the taller the subject, the more cranial the MA. This observation is valid for subjects between 159 cm and 183 cm. Further studies should include office workers in a larger range of body heights to evaluate whether different locations of the MA should be recommended for different body heights.
Study 2
Chair comparison
The primary outcome of the chair comparison was the stable upper body posture and the level of seat support of pelvic motion. We considered these measures the most essential requirements for dynamic office chairs to maintain operator performance while active sitting in an office environment. Obviously, location of the MA matters. Dynamic fitting accuracy as measure for the level of seat support of pelvic motion was lowest for chair A with the highest MA location. The hypothesis for this chair was based on the assumption that subjects will spontaneously perform a limited ROM with a relatively stiff spine in order to focus on the reading task. However, this assumption did not apply. The seat of this chair inclined significantly less than the pelvis. In maximum ROM task, we observed that some subjects lifted the pelvis from the seat. This result puts the suitability of chair A for daily use in doubt. The pelvic support of the other two chairs was significantly greater. However, chairs B and C also had a small difference between pelvis and seat inclination. We assume that this difference results from the asymmetric compression of the seat cushion and gluteal tissue during lateral motion of the seat. Preliminary measurements on a pressure mat revealed shifting of body weight to the contralateral side in relation to seat motion.
Comparing these two chairs, upper body posture was significantly more stable on chair C than on chair B in maximum ROM task (p < .001) but not in spontaneous ROM task (p = .012). Although subjects had a stable upper body posture on both chairs in both tasks, the median angular motion of the thorax was almost twice as large on chair B than on chair C. Additional calculated effect sizes showed a medium (d = 0.6, spontaneous ROM task) to strong (d = 0.8, maximum ROM task) effect of chair type on thorax inclination (Cohen, 1992), indicating that MA location influences upper body stability. While the absolute difference of thorax inclination between chair B and C was of small magnitude, it might be relevant in the light of previous research on office chairs without frontal plane DOF (Ellegast et al., 2012). Compared to lateral thorax inclination seen during common computer tasks in the office (Groenesteijn et al., 2012), the differences between the chairs account for 13% to 30% of reported ROMs. Whether chair C is better in terms of operator performance compared to the other chairs needs to be addressed by future field research.
In Study 1, we found a significant influence of body height on the location of the physiological MA. However, no such relation appeared by analyzing individual subjects in the chair comparison. This means the chair with highest MA (A) was not preferable for taller subjects, and the chair with lowest MA (B) was not preferable for shorter subjects.
Comparison to walking
Lateral spine flexion was in the same range for active sitting and literature data of walking (Lee & Park, 2011; Syczewska et al., 1999). While the lumbar spine is more flexed in active sitting than in walking, the thoracic spine is more stable. However, this finding is in line with the aim of the additional DOF to increase mobility of the pelvis and the lumbar spine while not affecting stable upper body posture.
Critical Discussion and Future Research
This study is subject to some critical issues carefully taken into account. For the kinematic analysis, the Plug-in-Gait marker model was used. However, frontal pelvis markers were replaced with lateral markers to ensure their visibility while sitting at a desk. Because the pelvis is tilted backward in sitting compared to standing, the analysis routine of Vicon Nexus was unusable, and directional vectors were defined. With expected angular motion significantly less than 20°, this method corresponds very well to standard Euler angle calculation (Crawford, Yamaguchi, & Dickman, 1999).
To determine physiological MA, only the two most caudal markers of the spine were used. Extension of the evaluation to more cranially placed markers (L4 and Lmid) showed very similar results, indicating that the whole lower lumbar spine rotates around one MA. We assumed circular motion of the lumbar spine during lateral flexion. Checking this assumption revealed no systematic deviation of the recorded motion from the fitted circle. However, the assumption was not verifiable for 18 (spontaneous) and 10 (maximum ROM task) subjects that were excluded from MA determination in Study 1. The different motion seen for those subjects may be due to the fact that no detailed movement instructions were given in order to prevent unnatural motion. However, excluded subjects of MA determination were not different from the others in Study 2. Relative body height influenced the location of the physiological MA, with taller subjects having a more cranial MA. Future studies should investigate which factors might explain this relationship, such as agility of the spine or physical fitness of the subject. Furthermore, while this study used an average MA, future studies should investigate office chairs with personalized MA (adapted to body height).
Literature reports different spinal motion patterns in relation to varying load conditions and ROM (Bell et al., 2016; Lengsfeld et al., 2000; Zwambag & Brown, 2015). We therefore investigated two different ROM but were not able to observe a different motion pattern. This might be due to the fact that the individual vertebral body movements were not analyzed. In addition, low back pain patients are known to have a reduced range of lateral spine flexion (McGregor, McCarthy, Doré, & Hughes, 1997), and they might benefit from seated spinal ROM training. We investigated whether such training may be performed on the chair (maximum ROM task). Finally, the chair has demonstrated its suitability for active sitting with maximum ROM. To analyze the stable upper body location, we focused on thorax inclination and not translation. Preliminary tests indicated that there are no differences between the investigated chairs regarding thorax translation. In accordance with the literature (Bush & Hubbard, 2008; van Dieën et al., 2001), we assume that the subjects tried to keep the thorax in a stable position to focus on the reading task. Therefore, chair type would affect only thorax inclination but not translation, which has been confirmed by the study results. Unfortunately, comparisons to other studies investigating lateral spine flexion in sitting are limited because lateral flexion is usually initiated by an inclination of the thorax with fixed pelvis (Park & Yoo, 2011). For reasons described previously, we assume that a continuous angular motion of the thorax is not suitable for daily office routine. Finally, we had to remove the backrests of all chairs for motion analysis. Using a backrest might reduce upper body motion, but this is now a matter for future study. Although evidence appeared that the chair with physiological MA best fulfills requirements of dynamic office chairs, it will take a field study under real office conditions to investigate its suitability. Such a field study will indicate whether the backrest is used while moving the seat, whether the activity during daily office work would be increased, and whether the lateral motion affects work performance or not.
Conclusion
This study investigated an additional DOF of an office chair aimed to allow active sitting, a current recommendation from a human factors perspective, and adapted it to natural human kinematics. Based on our study results, we recommend placing the MA of the additional DOF at the level of the 11th thoracic vertebra of the chair users. A chair meeting this recommendation would enable considerable lateral flexion of the spine while maintaining a highly stable upper body posture. The spinal motion observed on this chair also matched spinal motion during walking. Further research shall evaluate whether the additional DOF decreases static sitting time while maintaining work performance and analyze short- and long-term effects of continuous lateral spine flexions on musculoskeletal health.
Key Points
The physiological axis of lateral flexion is the 11th thoracic vertebra.
The chair with that axis allows the best kind of active sitting.
Subjects’ spines showed considerable lateral flexion despite the stable upper body.
Spinal motion during active sitting is similar to walking.
Footnotes
Acknowledgements
One author of this study (S.O.) received funding from the Commission for Technology and Innovation, project LS-13718.1.
Roman Peter Kuster received his master’s degree in human movement sciences in 2013 from ETH Zurich, Institute of Human Movement Sciences and Sport. After working at the Institute of Physiotherapy at the ZHAW Zurich University of Applied Sciences, he transferred to the Biomechanical Engineering of the Institute of Mechanical Systems. His main interest is the combination of ergonomics and biomechanics at the workplace to prevent work-related health issues. He is currently doing a PhD at Karolinska Institutet to assess physical (in)-activity in desk based office work.
Christoph Markus Bauer studied physiotherapy at the Hoogeschool van Amsterdam, Netherlands. He moved to the Philips-University Marburg, Department of Medicine, where he received his master’s degree in 2012. He is the head of the Motion-Laboratory at the ZHAW Zurich University of Applied Sciences, Institute of Physiotherapy, and is currently doing a PhD at the Tampere University, Finland, in the field of movement analysis.
Sarah Oetiker received her master’s degree in human movement sciences in 2009 from ETH Zurich, Institute of Biomechanics. She worked at the ZHAW Zurich University of Applied Sciences, Institute of Physiotherapy from 2010 to 2014.
Jan Kool earned his PhD at Maastricht University, Netherlands, in the field of health sciences with the emphasis on quantitative research methodology. He is now working as research director at the Rehabilitation Center Valens, Switzerland.