
Abstract
Introduction
Over the past 20 years, the use of opioids for acute pain management has undergone a logarithmic increase. Despite our increased understanding of the opioid crisis in the U.S., orthopaedic surgeons frequently over-prescribe opioid pain medications in the postoperative period.1-3 In 2007, prescription opioid abuse cost insurers an estimated $72.5 billion dollars. 4
To minimize opioid use and associated detrimental side effects, opioid-sparing and opioid-free multimodal pathways have been developed in many orthopaedic subspecialties with promising results.5-7 Given the positive results noted in the literature, multimodal pain protocols are becoming increasingly utilized.8-14 Despite these overall positive results, financial implications of multiple drugs may be a burden and limit the widespread adoption of these protocols.
Cost, availability, and accessibility of medication for postoperative pain may impact a patient’s preferred treatment choice and their likelihood to obtain and maintain the use of that pain control regimen. The costs associated with an opioid-free multimodal, multi-drug post-operative pain regimen versus opioid/acetaminophen therapy have not been evaluated in the literature. Therefore, the aim of this study was to compare the cost of an opioid/acetaminophen therapy versus an opioid-free multidrug, multimodal postoperative pain management regimen after elective foot and ankle surgery to understand this cost difference and help guide the discussion between surgeon and patient when deciding postoperative pain management treatment options.
Methods
This study is a secondary analysis of data collected from 2 separate IRB-approved prospective studies that evaluated pain control after elective foot and ankle surgery from a single institution performed by 2 board certified fellowship trained orthopaedic foot and ankle surgeons.
The first study analyzed the use of opioid medication after hallux valgus surgery in 59 patients. The analysis included the average quantity and type of postoperative opioids used after hallux valgus surgery. 15 Patients were prescribed one of the following: Norco 5/325, Oxycodone 5 mg, Hydrocodone 5/325, or Percocet 5/325 in this study. This information was utilized to calculate the total cost of opioid pain medication consumed after hallux valgus surgery and the opioid/acetaminophen therapy group in our study came from this study cohort.
The second study assessed the pain of patients after elective foot and ankle surgery utilizing a novel opioid-free multimodal pain pathway. 16 The multimodal postoperative pain protocol included cyclobenzaprine (10 mg q8h for 2 weeks), ketorolac (10 mg q6h for 2 weeks), meloxicam (10 mg q8h for 2 weeks), pregabalin (75 mg q12h for 2 weeks), and acetaminophen (1 g q6h for 2 weeks). That study included 40 patients and the opioid-free group in our study came from this study cohort.
For each of these studies, the anesthetic method was determined for each patient by their anesthesiologist and was not specifically analyzed for its effect on the patient’s postoperative pain. Most commonly, patients had regional anesthesia and sedation for their anesthetic method, but this varied and these costs were not analyzed. Additionally, each of these studies assessed patient compliance with treatment, pain control on each regimen, patient’s satisfaction, and postoperative complications associated with treatment. The analysis also included returns to the operating room and/or visits to the emergency room or urgent care.
Utilizing information collected during these 2 studies, deidentified patient profiles were constructed using the patient’s insurance carrier to determine the cost of each patient’s postoperative regimen (opioid vs multimodal). Our objective was to evaluate the maximum cost a patient could have to pay out of pocket for either of these 2 drug regimens. To that end, our pharmacy colleagues loaded the patient’s insurance, our hospital pharmacy, and prescription(s) to run a claim that showed the cost of the medication to the patient. Due to multiple factors that could potentially affect the cost of the prescription such as: pharmacy chosen, deductibles, insurance carrier, and prior authorization, we made several key assumptions to attempt to equitably assess the maximum out of pocket costs to the patient for each of the regimens. First, we utilized the patient’s known insurance carrier so that we had the actual carrier the patient utilized. Secondly, we ran the cost for our hospital pharmacy to ensure data accuracy and integrity. Thirdly, we assumed that the patient hadn’t utilized any of their deductible. Therefore, we analyzed the highest cost the patient could have paid for the medication. Finally, we assumed that all medication(s) were both approved by the insurance carrier and paid for/picked up by the patient. The postoperative prescription costs, in U.S. dollars, of these 2 pain management groups were totaled, analyzed, and compared.
Data analysis started with a box and whisker plot to identify potential outliers. Through this method, 3 outliers were identified in both the opioid and opioid-free multimodal groups (6 total outliers) and were not included in the analysis. A paired t-test was used to compare the means of these 2 groups and to evaluate whether significant differences might exist between them.
Results
Prescriptions in the opioid group had an average cost of $8.92 (SD $5.74), and prescriptions in the opioid-free multimodal group had an average cost of $25.60 (SD $10.49), P < .001. The average difference in cost between the 2 regimens was $16.68 (Figure 1).
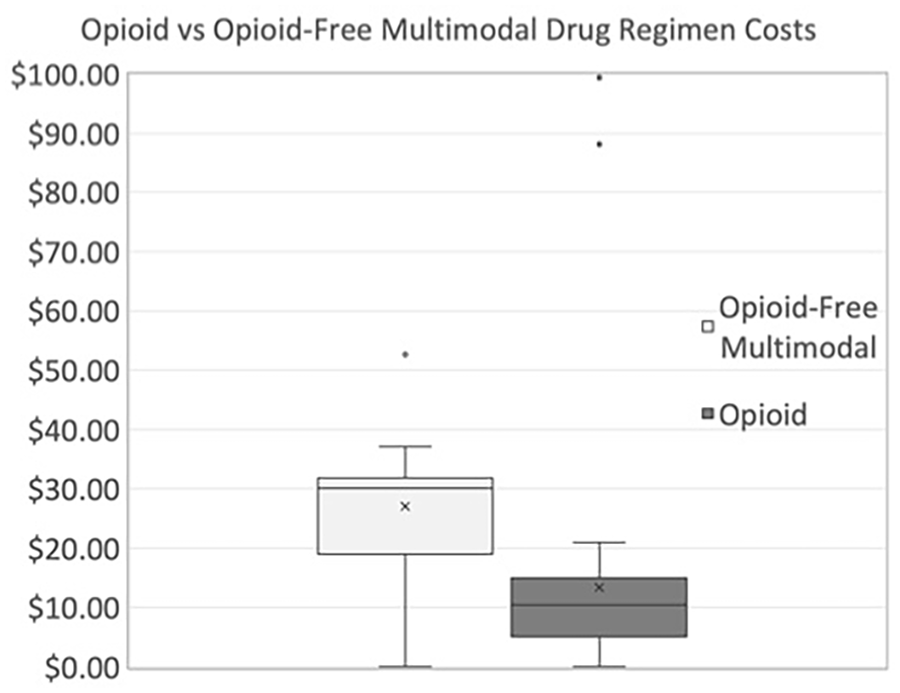
The postoperative pain treatment costs between the opioid/acetaminophen therapy and the opioid-free multimodal protocols for elective foot and ankle surgery.
For public health insurance, the opioid group average was $7.49 (SD $7.23) while the opioid-free multimodal group was $23.24 (SD $8.44), P < .001, with an average difference in cost between the 2 regimens of $15.75. For private health insurance, the opioid group average was $9.72 (SD $4.79) while the opioid-free multimodal group was $26.11 (SD $10.23), P < .001, with an average difference in cost between the 2 regimens of $16.39 (Table 1).
The Average Cost of Opioid-Free Multimodal Protocol and Opioid Monotherapy Stratified by Public Versus Private Health Insurance.
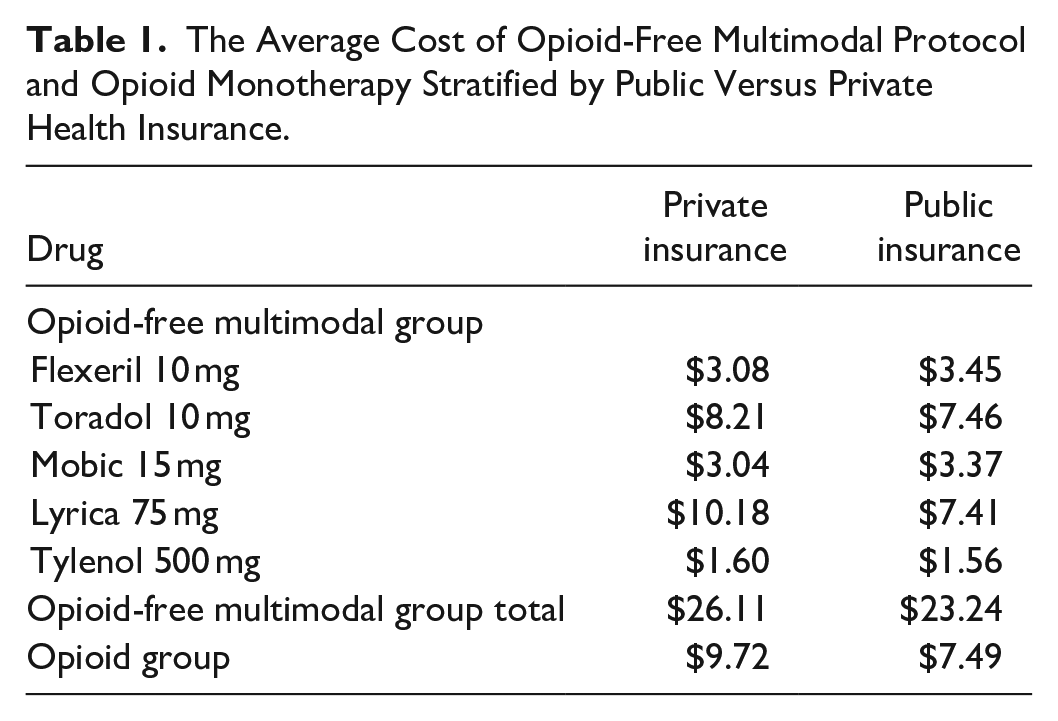
The average cost difference of the opioid-free multimodal regimen based on insurance (Private: $26.11, Public: $23.24) was $2.87 (P = .369).
Both treatments, in their individual studies, were demonstrated to be clinically effective for pain control. There were no returns to the operating room or visits to the emergency room or urgent care in the 90-day postoperative period for either treatment arm, and thus no additional non-prescription costs of care were added to either group.
Discussion
The objective of this study was to compare the cost of postoperative pain management treatment regimens after elective foot and ankle surgery between opioid/acetaminophen therapy and an opioid-free, multidrug, multimodal pathway. Our data demonstrated that patients whose postoperative pain was managed by the opioid-free multimodal pain pathway had statistically significantly higher prescription costs than treatment with opioid/acetaminophen therapy by around 17 dollars. However, we believe that this cost is likely not clinically significant for most patients given the overall cost of surgical intervention. This was the case for all health insurance types, with an insignificant difference in cost depending on insurance status (public vs private).
Previous studies have shown success in patient-reported outcomes after elective foot and ankle surgeries when treated postoperatively with either opioids or an opioid-free multimodal pain pathway.5-14,17 Other studies have defined the magnitude of the issue of the opioid crisis, which has continued to be detrimental both economically and to patients’ health.1-4,18-22 However, no previous study has analyzed the cost difference between these 2 pain treatment groups. Our study demonstrated that the opioid treatment group cost is lower than that of the opioid-free multimodal pain group. However, the cost difference was, on average, below $17, so this difference may or may not be clinically significant and will depend on the patient’s individual financial situation. As opioid-free postoperative pain management pathways continue to develop and prove to be effective, the relatively minimal average cost difference demonstrated in our study may be reassuring to surgeons and patients. Socioeconomic status along with the feasibility of patients accessing certain medications and their ability to comply with a multidrug regimen with potentially complex dosage instructions plays a role in treatment strategy. Therefore, knowledge of the price differences between the 2 methods of treatment gives the clinician an extra data point when making this medical decision.
In this study, there are some costs that we were unable to calculate that could affect the opioid/acetaminophen therapy group disproportionately to the multimodal treatment regimen. In the opioid/acetaminophen therapy group, there may be costs associated with opioid acute side effects that could require additional over the counter or prescription medications for example, constipation (polyethylene glycol) or nausea (ondansetron). Additionally, as of September 30, 2020, 10 states enacted laws or regulations that require certain medical professionals to prescribe or offer a prescription for naloxone along with opioids to some individuals under their care.23,24 In 2018, the mean out-of-pocket cost of naloxone was $35.13 for private insurance, $14.11 for Medicare, $2.85 for Medicaid, $72.67 for VA/Tricare, and $249.97 for the uninsured, which will raise the total cost for patients in the opioid treatment group if they live in a state that requires this additional medication. 25 There may also be additional significant long-term cost savings due to the avoidance of opioid dependence, diversion, or addition that also were not calculated due to being outside the scope of this study. We do know that prescription opioid abuse costs insurers an estimated $72.5 billion dollars annually. 4 Although assigning that dollar figure to individuals or patients in this study to represent the cost of opioid prescriptions may be relevant, it was also outside the scope of this study. Finally, there is a human cost to opioid addiction as well. Unfortunately, some patients become addicted to narcotics after orthopaedic surgery and ultimately lose their life to this addiction. This cost cannot be accounted for in a dollar figure, is real, and is outside the scope of this study.
There are limitations to this study. The 2 studies analyzed in this study were relatively small cohorts from the experiences of 2 fellowship trained orthopaedic foot and ankle surgeons. Prescribing patterns may be different among other surgeons. However, the opioid/acetaminophen prescriptions were prescribed based on standard guidelines which are relatively common in the orthopaedic community, so we believe there is generalizability in the population. 15 Additionally, regarding the opioid-free multimodal pain group, this is only one type of pathway, but it has been shown to be effective and thus was utilized in this analysis. 16 Other opioid-free pathways may have different associated costs and would need to be analyzed. However, with 5 total medications, this pathway is more inclusive than most in the literature and therefore we believe it represents a reasonable cost comparison group. We do know that, for the opioid/acetaminophen pathway, the patients filled the prescription because we counted the number of pills that they utilized. However, we didn’t count the number of pills taken for the opioid-free multimodal pathway, so we do not know if each patient filled all of the prescriptions given. However, if they did not, then the cost would be even lower than what we presented, which would demonstrate greater efficacy because their pain would have been controlled to their satisfaction without all of the prescribed medication. We ran our analysis based on our hospital’s pharmacy and the patient’s insurance to determine the cost as if they hadn’t met any deductible. So, our costs are the highest possible, especially compared to patients who had already met their deductible, live in a country with socialized medicine, or have worker’s compensation or another 3rd party that would completely cover the cost of the medication. Each insurance carrier often has a different pay structure with different pharmacies. So, the same patient could have different costs, even if they have the same insurance, by simply getting their medicine filled at a different pharmacy. This factor was outside the scope of this study and was not analyzed. Lastly, we weren’t able to analyze the cost of patients’ use of medication(s) not prescribed by our team. This could include over the counter medications for example, ibuprofen, acetaminophen, docusate, suppositories, diphenhydramine/pseudoephedrine or previous prescription medications that the patients may have saved at their home for example, hydrocodone, oxycodone, ondansetron, or cyclobenzaprine.
Conclusion
We found that patients whose postoperative pain was managed by the opioid-free multimodal pain pathway had a 17-dollar higher prescription cost than patients treated with opioid/acetaminophen therapy. However, we believe this price difference is likely not clinically significant for most patients and should not be a barrier to utilizing an opioid-free multimodal pain pathway because of the published benefits of limiting narcotic use for patients and society. We hope this information helps provide valuable information for the surgeon when making postoperative pain management decisions.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The opioid group in this study received approval from the Prisma Health Institutional Review Board (1852602). The opioid-free group in this study received approval from the Palmetto Health Institutional Review Board (Pro00075573).