
Abstract
Keywords
Introduction
Antimicrobial resistance (AMR) is becoming a global public health priority in view of its impact on morbidity, mortality, and healthcare costs.1 -4 In 2019, it was estimated that there were 1.27 million deaths globally attributable to bacterial resistance, with over 4.95 million deaths reported to be due to AMR. 1 As a result, AMR is increasingly seen as the next pandemic after COVID-19 unless sustained efforts are introduced across countries to improve appropriate antibiotic use. 5 These concerns have resulted in a number of national and international initiatives.6 -8 In 2015, the World Health Organization (WHO) released a Global Action Plan (GAP) to fight AMR. 1 The GAP subsequently became the prototype framework for the development of National Action Plans (NAP) in member countries.2 -6 However, different countries are at different stages of the development, implementation, and monitoring of NAPs including African countries.9,10
One of the key components of the GAP, and subsequently the NAPs, was the need to employ various strategies including Antimicrobial Stewardship Program (ASP) to optimize the use of antimicrobials. 1 ASPs are defined as organizational or system-wide healthcare strategies to promote the appropriate use of antimicrobials through the implementation of evidence-based interventions. 11 Effective implementation of ASPs, alongside institutional structures including functional drug and therapeutic committees (DTC) and infection prevention and control committees (IPC) that safeguard patient safety, in health settings helps improve patient outcomes, reduce AMR and healthcare-associated infections, and saves healthcare costs.12-14 However, there are concerns with available antimicrobial stewardship (AMS) champions as well as financial and human resources especially key personnel to effectively introduce ASPs into low- and middle-income countries (LMICs). 15 This is beginning to change with a number of ASPs successfully introduced in healthcare settings among a number of African and Asian countries in recent years.16 -20
The U.S. Centre for Disease Control and Prevention (CDC) developed the Core Elements of a Hospital ASP in 2014, which provides essential components and guidance for implementing robust ASPs in hospitals in the United States.21,22 More recently, the WHO in 2019 developed a practical toolkit for implementation and assessment of ASPs in healthcare facilities in LMICs. 15 The WHO ASP assessment tool, when applied on a periodic basis, documents current program infrastructures and activities and helps to identify the most critical elements that could support the effective implementation of the program. This is particularly important in sub-Saharan Africa (SSA) where the knowledge base of key hospital personnel concerning AMS and ASPs have been low alongside a lack of commitment and accountability for their implementation.23 -25 It is critical to address this due to the greatest burden of AMR in SSA. 1
These core elements of the WHO ASP toolkit are designed to guide healthcare facility management to address barriers toward the successful implementation of sustainable ASPs in LMICs. The major reported barriers to implementing ASP especially in LMIC include leadership/structural issues such as poor infrastructure, inadequate skilled human resource to champion ASP activities in hospitals, and a lack of adequate facilities/support to undertake diagnostic tests including culture and sensitivity testing to promote optimal antibiotic use. Other barriers of concern include poor attitude and low awareness of the concept of ASP among healthcare professionals (HCPs) as well as a lack of up-to-date information regarding AMR patterns within hospitals to improve future empiric prescribing.15,16,26 -32
The 7 core elements of ASP in the toolkit comprise of leadership commitment, accountability and responsibilities, AMS actions and interventions, education and training, monitoring and surveillance, and reporting and feedback. The effective implementation of ASPs in healthcare facilities starts with a well-conducted situational analysis. This will form the basis for the development of a stepwise sustainable AMS action plan that identifies what core elements of ASPs are in place, what are the short- and medium/long-term priorities to address, the human resource needs, and the overall barriers and facilitators of ASP implementation. 15
In 2017, Ghana developed its NAP to reduce AMR33-35 with ongoing monitoring. However, there are ongoing financial concerns to effectively implement agreed activities. 36 Encouragingly, through the help of UK-based institutions, AMS experts, and the Fleming Fund, some hospitals in Ghana have implemented ASPs, with this number increasing through continuous support.37 -39 However, currently, there is paucity of data regarding the extent of implementation of the core elements of ASPs in hospitals in Ghana to provide future guidance, especially among hospitals that have not currently undertaken any ASPs.
This study was therefore undertaken to help address this information gap by undertaking a survey to determine the extent of implementation of the core elements of ASPs among health facilities in Ghana. Alongside this, potential lessons could be gleaned from the assessment of the possible barriers for a sustainable implementation of ASPs in Ghana, a LMIC, to guide future ASP policies and programs to strengthen the country’s effort to fighting AMR.
Method and Material
Study Setting and Population
The current study was conducted in 2 of the 16 administrative regions in Ghana. The Regions, which were carefully chosen, included the Greater Accra Region, where the capital city of Ghana is located, and the Volta Region. Ghana’s population, according to the 2021 population and housing census report, currently stands at 30.8 million with Greater Accra Region being the second most populous region while Volta Region is the seventh. 40 The 2 regions share a boundary in the south-eastern part of the country with Greater Accra region being predominantly urban while Volta region is predominantly rural. Consequently, these 2 regions were purposively selected to represent the different dynamics in healthcare delivery among public Ghanaian hospitals with different populations. The public hospitals in both regions are predominantly utilized by the citizens in Ghana due to their acceptance of the national insurance scheme ensuring increased access to healthcare and are therefore more likely to be representative of the typical hospital setting in Ghana versus purely private hospitals. The 2 regions also include a range of hospitals from primary to tertiary hospitals, which is important for research into ASPs and their barriers.41,42
The study was conducted in 15 health facilities in these 2 regions who consented to participate and responded to the questionnaire. The 6 health facilities in the Greater Accra included Greater Accra Regional Hospital, Tema General Hospital, Ashaiman Polyclinic, Pantang Hospital, Shai-Osudoku District Hospital, and University of Ghana Medical Center. The 9 hospitals in the Volta Region included the Volta Regional Hospital (Hohoe), Keta Municipal Hospital, Battor Catholic Hospital, Ketu South Municipal Hospital, Peki District Hospital, Sacred Heart Catholic Hospital, and St. Anthony Hospital.
Study Design and Data Collection
A cross-sectional survey was conducted using a self-administered structured questionnaire to assess the implementation of the core elements of ASP among the 15 public hospitals in the Greater Accra and Volta Regions of Ghana.
The questionnaire was adapted from the WHO practical tool kit for ASPs in LMICs and CDC Core Elements of a Hospital Antibiotic Stewardship Program.15,20 The questionnaire was subsequently pre-tested among 4 experts working in the 2 regions to assess the questionnaire for the clarity and face validity. Suggestions made by these experts were subsequently incorporated into the final questionnaire.
The questionnaire was sub-divided into 10 sections. These included (i) general information on the facility such as bed capacity, level of care, staff strength, presence of a functional drug and therapeutic committee (DTC), and infection prevention committee (IPC), (ii) leadership commitment, (iii) AMS team accountability and responsibilities, (iv) pharmacy expertize, (v) AMS actions and interventions, (vi) education and training, (vii) monitoring and surveillance activities, (ix) reporting and feedback activities, and (x) challenges/barriers to implementation of AMS in the hospital. The responses provided for most of the questions assessing the extent of implementation of the core elements of ASP were “Yes,” “No,” and “Not sure” to facilitate analysis.
Sampling Method and Inclusion Criteria
All primary, secondary, and tertiary hospitals in the 2 selected regions were included in the survey. A web-based designed google questionnaire was distributed through the administrators of each hospital to be answered by a representative (including clinical coordinator, hospital chairman/secretary of the DTC, head of pharmacy department, and representative of the AMS team) of the hospital with in-depth knowledge of the operation of the AMS in their respective facilities.
Data Analysis
Data collected using the google online form were imported into Microsoft Excel and then into STATA version 14 for statistical analysis. Descriptive statistics and bivariate analysis, that is, Fisher exact test, were performed on the data.
Ethical Consideration
Informed consent were given by all respondents before access to the questions were granted. Detailed information about the survey was provided to the participants on the need for voluntary participation and withdrawal, and how potential risks have been addressed. Participating hospitals’ data privacy and confidentiality were also ensured by anonymizing all identifiers.
Ethical clearance was obtained from both the University of KwaZulu-Natal (BREC/00004236/2022) and the Ghana Health Service (GHS-ERC/01708/22).
Results
Characteristics of Participating Hospitals
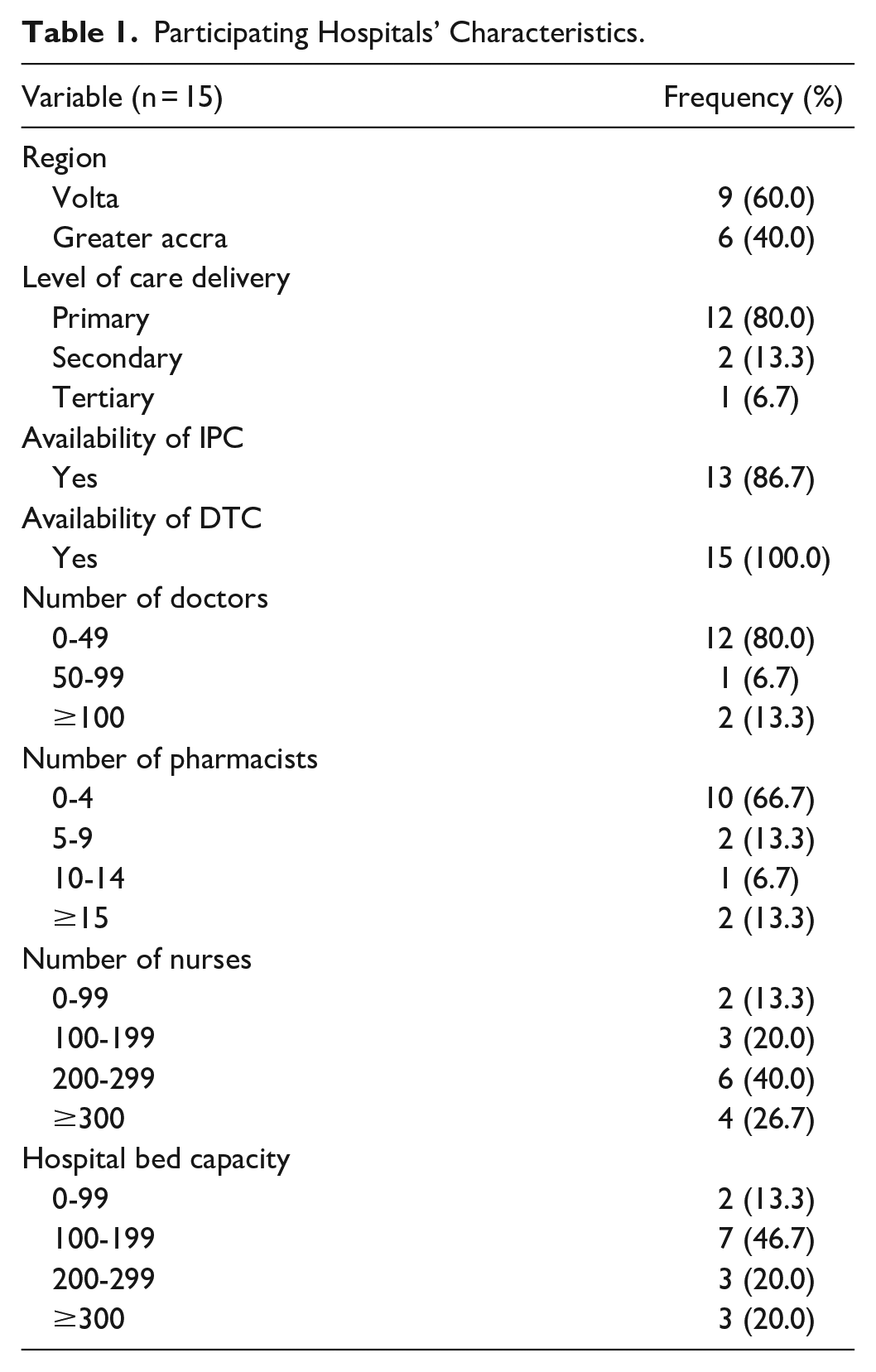
All 15 public health facilities in Greater Accra and Volta regions voluntarily participated in this study. Out of this total number, a majority (n = 9, 60.0%) were from the Volta region and were primary health care facilities (n = 12, 80.0%) followed by those providing secondary level of healthcare.
About half (n = 7, 46.7%) of the participating hospitals had bed capacities between 100 and 199 beds and most of them had less than 50 medical doctors (n = 12, 80.0%), less than 5 pharmacists (n = 10, 66.7%), and between 100 and 199 nurses. Most (n = 13, 86.7%) of the facilities had functional IPCs and all hospitals (n = 15, 100.0%) had functional DTCs (Table 1).
Participating Hospitals’ Characteristics.
The Core Element of Leadership Commitment to AMS Activities
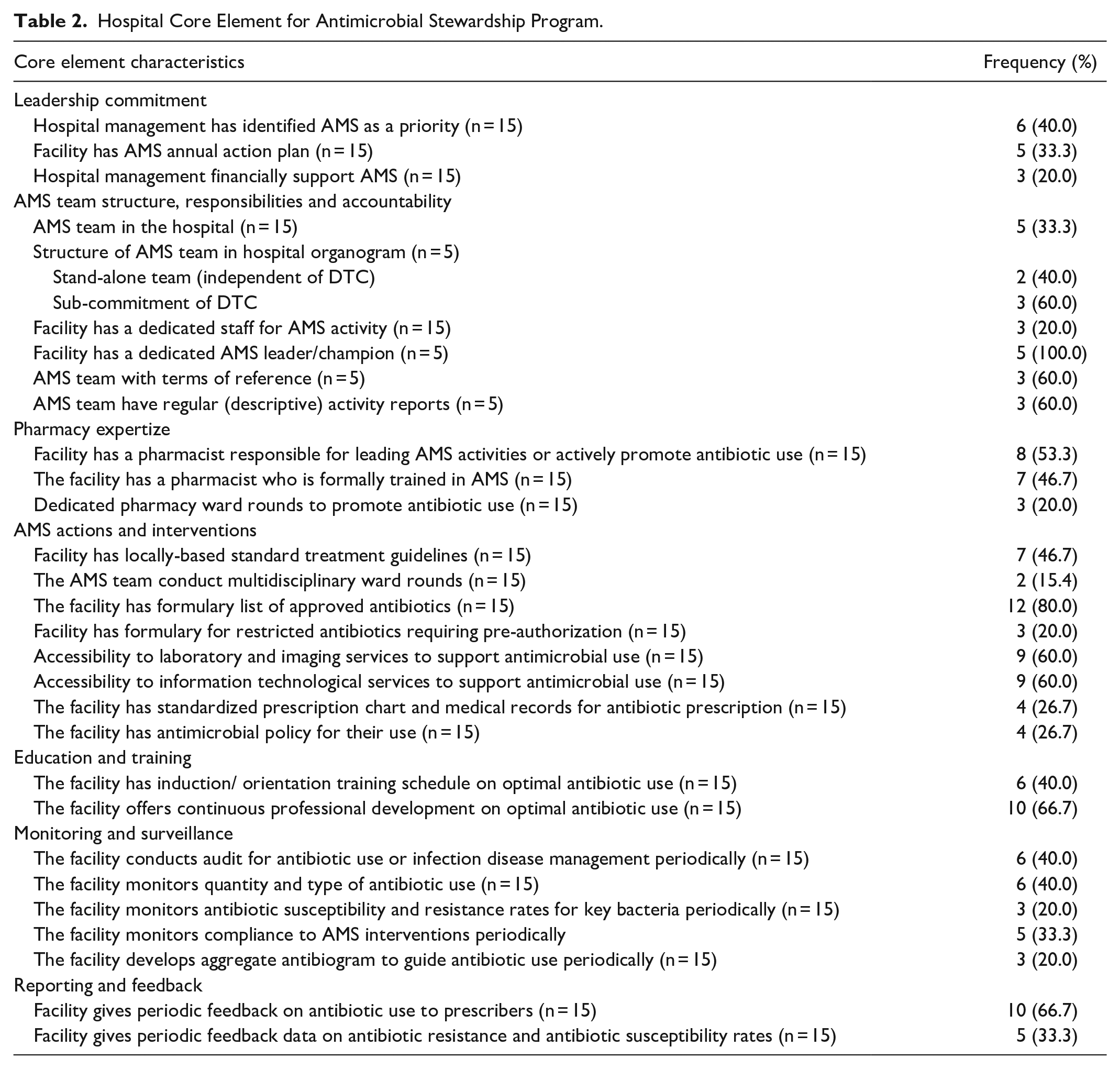
Less than half (n = 6, 40.0%) of the participating health facilities management had identified AMS as a priority in their key performance indicators for the year. One-third (n = 5, 33.3%) had AMS annual action plans with resources allocated for ASP activities and one-fifth (n = 3, 20.0%) of the surveyed facilities had a dedicated staff member who spearheaded AMS activities. A similar proportion (n = 3, 20.0%) had instigated dedicated budgeted financial support for AMS activities in the action plan (Table 2).
Hospital Core Element for Antimicrobial Stewardship Program.
The Core Element of AMS Team Structure, Responsibilities, and Accountability
One-third (n = 5, 33.3%) of the participating health facilities had an AMS team in place with a majority (n = 3, 60.0%) of them functioning as a sub-committee of the DTC. All of the facilities with AMS teams had dedicated leaders/champions responsible for leading the implementation of the ASP and majority (n = 3, 60.0%) had terms of reference for the day-to-day activities of AMS team members. The majority of the facilities with AMS team in place produced and disseminated regular activity reports to stakeholders to enhance sustainability and continued interest in AMS activities (Table 2).
The Core Element of Pharmacy Expertize on AMS
Just over half (n = 8, 53.3%) of the participating health facilities had a pharmacist (s) responsible for leading the implementation of AMS activities to promote the rational use of antibiotics. Less than half (n = 7, 46.7%) of these facilities had pharmacist who had been formally trained in AMS and one-fifth (n = 3, 20.0%) of these facility pharmacist (s) conducted pharmacy-only ward rounds to promote the rational use of antibiotics (Table 2).
The Core Element of the Extent of Implementation of AMS Actions and Interventions
About one-fourth (n = 4, 26.7%) of the participating health facilities reported that they had antimicrobial policies that guide their prescribing of antibiotics and similar proportion had standardized prescription charts and medical records for antibiotic prescriptions. Less than half (n = 7, 46.7%) of the facilities had locally-based standard treatment guidelines for the management of infectious diseases. Only 2 out of the 15 (15.4%) facilities had a team that conducted regular multidisciplinary wards. While most (n = 12, 80.0%) of the facilities had a formulary with a list of approved antibiotics, only 20.0% (n = 3) of them had a formulary with a list of restricted antibiotics, for example, antibiotics from the WHO Reserve list (43), that require pre-authorization by designated team or persons. Equal proportions (n = 9, 60.0%) of health facilities had laboratory and imaging services and information technology services that supported antimicrobial use (Table 2).
The Core Element of Education and Training on AMS
Concerning education and training of HCPs, less than half (n = 6, 40.0%) of the facilities had induction/orientation training schedule for their sensitization on AMR as well as how to optimize antibiotic prescribing, dispensing, and administration. However, most (n = 10, 66.7%) of the facilities offer a continuous in-service training on optimal antibiotic use for their staff HCPs (Table 2).
The Core Element of Monitoring and Surveillance of AMS Activates
Less than half (n = 6, 40.0%) of the facilities conduct regular audits of antibiotic use, and a similar proportion monitors the quantity and the types of antibiotic use. Only 20.0% (n = 3) of the facilities monitor antibiotic susceptibility and resistance rates for key bacteria periodically, and a similar proportion develops and regularly updates aggregated antibiograms for dissemination among HCPs in their facility. However, only one-third (n = 5, 33.3%) of surveyed facilities monitors compliance with specific interventions to promote the rational use of antibiotics (Table 2).
The Core Element of Reporting and Feedback of AMS Data to Staff
While one-third (n = 5, 33.3%) of the facilities gave periodic feedback data on AMR and susceptibility rates, two-thirds (n = 10, 66.6%) of them gave periodic feedback on antibiotic use to prescribers (Table 2).
The Association Between Pharmacist-led AMS Activities and Some ASP Core Elements
The core element indicator of having pharmacist(s) leading the implementation of AMS activities in their respective facilities was associated with having a pharmacist who has been formally trained in AMS (P = .001), the healthcare facility having an AMS action plan for the year (P = .026), facilities with AMS teams in place who are able to produce and disseminate regular activity reports to all key stakeholders (P = .007) and those with a formulary having a list of approved antibiotics for use (P = .026) (Table 3).
Fisher Exact Analysis of the Association Between Pharmacist-led AMS Activities and Some Core Elements.
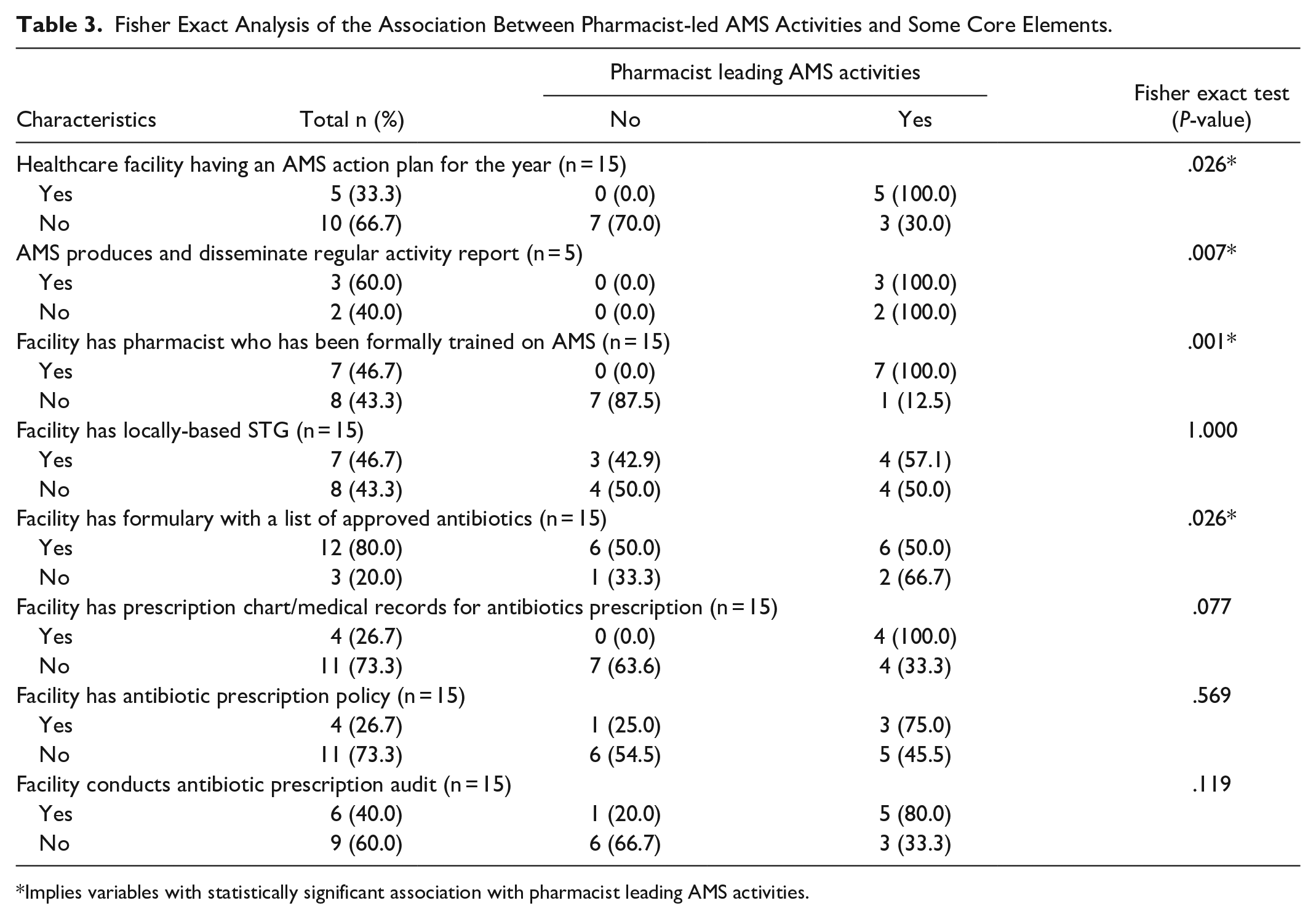
Implies variables with statistically significant association with pharmacist leading AMS activities.
Challenges and Barriers to Implementing AMS Activities
The most common barrier/challenge to implementing AMS activities reported by the facility representatives was the lack of human resources to spearhead AMS activities (73.3%), followed by staff time availability for attending to AMS activities (66.7%) and poor laboratory support (60.0%) (Figure 1).
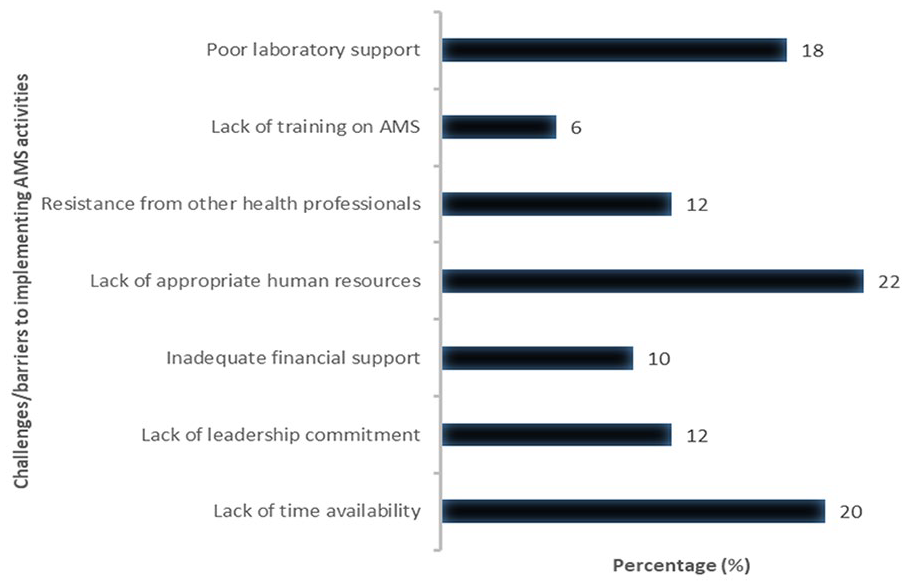
Barriers to implementing AMS activities.
Discussion
We believe this is the first comprehensive assessment of the core elements of ASP as way of identifying the level of its implementation in public hospitals in Ghana. We also believed it was necessary to evaluate the barriers and facilitators of ASPs among hospital in Ghana to guide policies and strategies toward achieving the Ghana NAP goals to fight the rising rate of AMR and its impact on the healthcare system.43 -46
With respect to the 7 core elements of implementing sustainable ASPs.15,21 leadership commitment emphasizes the necessity of a health facility having dedicated time, financial and human resources as well as prioritizing AMS activities to enhance appropriate antibiotic use. 47 Our study showed that most of the public hospital facilities surveyed had low management priority and dedicated financial support for AMS activities. Whilst this poor leadership support for ASPs has been reported in studies in other African countries and other LMICs.48,49 This needs to be addressed for a sustainable fight against AMR.
AMS accountability and responsibilities is demonstrated by facilities having an AMS team in place with clear terms of reference alongside the production and dissemination of regular activity reports. Without clear terms of reference describing the leadership structure and membership responsibilities of the AMS, there will be poor accountability toward the implementation of AMS activities. 15 Whilst all the surveyed facilities had a functional DTC and IPC, only one-third had AMS teams in place with a little over half of these having clear terms of reference and operating as a sub-committee. Whilst this is similar to the findings in Nigeria, 24 the poor accountability and reasonability toward AMS pose a serious threat to the effective implementation of ASPs in these hospitals in Ghana as well as the achievement of AMS targets in in the NAP. Encouragingly, some facilities responded that they were able to produce and disseminate regular AMS activity reports of their implementation to stakeholders.
Pharmacy and drug expertize as a core element of ASP recognizes the critical role that pharmacists play toward the effective implementation of AMS activities in hospitals.15,21,47 This suggests that pharmacists must be empowered through formal training and certificate programs in infectious disease management and AMS principles and strategies to enhance their contribution toward ASPs in hospitals. Several studies have shown that ASPs that are pharmacist-led have successful outcomes. Consequently, it is essential to identify empowered pharmacist to serve either as leaders or co-leaders to lead ASP implementation efforts in hospitals to improve future antibiotic use.19,49 -54 Our study showed that a little over half of the facilities had pharmacists leading AMS activities even though less than half of the pharmacists had received formal training on AMS. Their personal effort, through the conduct of a dedicated pharmacist-only ward rounds to optimize antibiotic use, was observed in only 20% (n = 3) of the public facilities surveyed, which is a concern that must be investigated and addressed. Pharmacist-led AMS activities was associated with pharmacist who have been formally trained on AMS, facilities with AMS action plans that have been endorsed and priority activities identified for ensuring appropriate antibiotic use, those who produce and disseminate regular AMS activity reports, and those that have formulary with approved list of antibiotics for use. This finding supports the evidence of the role of pharmacists toward successful implementation of hospital ASPs. However, their current role could be limited by lack of training in AMS, lack of management commitment, poor feedback, and accountability of AMS activities. 47
As mentioned, AMS interventions have proven to improve patient outcomes, reduce healthcare-associated infections reducing healthcare cost and minimizing the collateral damage from antimicrobial use.14,17,55 AMS interventions may be persuasive, restrictive or structural in their function. 56 Situational analyzes help with identifying potential gaps such as the prolonged prescribing of surgical antibiotic prophylaxis to prevent surgical site infections reported in many hospitals in Ghana which can be addressed with appropriate AMS interventions implementation such clinician education, audit of prescription with feedback to clinician and pre-authorization.16,57 Having standard treatment guidelines and standardized prescription chart and medical records that support effective antimicrobial audit for optimal choice and duration for empiric treatment of common infectious conditions.
Apart from the availability of an approved list of antibiotics that was available in most (n = 12, 80%) facilities, there was typically suboptimal implementation of AMS interventions among the surveyed public hospitals. This included the lack of availability of antimicrobial policies, standardized prescription charts and medical records, formularies containing restricted antibiotics such as pertinent antibiotics on the WHO Watch and Reserve lists, and multidisciplinary ward rounds to audit antibiotic prescriptions. 58 We believe these concerns could be attributed to a lack of formal training of most AMS team members on the principles and strategies of ASP implementation together with the low leadership commitment and accountability. This needs to be addressed going forward.
Education is a key component of every coordinated AMS effort to optimize hospital antimicrobial use due its direct impact on healthcare professionals’ knowledge, attitude, and practice.39,59-61 It is most effective when it is provided as part of other AMS interventions, including prospective feedback with feedback to clinicians, and when it is directed toward the actions most relevant to the type of HCP group, such as education on surgical antibiotic prophylaxis to the surgical team as part of the means to optimize antibiotic use among patients undergoing surgery.43,56 Education and training of HCPs to achieve AMS-related competencies may be delivered though several modes. These may include pre- and in-service training, face-to-face workshops, e-learning, blended learning with a mixture of technology and traditional face-to-face instruction, practical training at centers of excellence, and on-the-job training. 15
Less than half of the hospitals surveyed offered basic induction training to sensitize newly employed or recruited staff on AMR and optimal antibiotic prescribing, although approximately two-thirds provided continued education training and resources on AMS. The lack of structured in-service induction training on AMS among healthcare professionals in the surveyed public hospitals in Ghana has been observed in other healthcare settings in LMICs,62,63 although other hospitals elsewhere provide education for mostly doctors and pharmacists. 63
Monitoring and surveillance of AMS is another important core element that helps to identify opportunities for quality improvement in the utilization of antimicrobials in hospitals and to assess the impact of any AMS intervention. This element needs to be improved with as most of the surveyed facilities scored less than 50% for all parameters used for assessing it. In addition, only one-third of the surveyed hospitals monitor compliance to AMS interventions, while only 40% both conduct audit or point prevalence surveys of the quality indicators for appropriate antibiotic use.
Surveillance activities on antibiotic susceptibility and resistance rates for a range of key bacteria to enable regular update facility-wide antibiograms also needs to be improved on as barely one-fifth of the surveyed facilities were found to be doing this. The low tracking of antimicrobial use and susceptibility has been reported in some studies, including those in Ghana, principally due to the issue of the patient inability to pay out of pocket for such services and availability of microbiology plates for current antibiotics, while others have reported good surveillance activities.48,64,65 This observation poses serious challenge in the AMR fight as appropriate quality improvement measures and effective AMS interventions will be hampered due to poor and untimely monitoring and surveillance of antimicrobial use and their susceptibility practices.
Overall, ASPs must be designed to ensure regular updates to prescribers, pharmacists, and nurses as well as leadership on the process and outcome measures to stimulate and sustain stakeholders’ interest and continuous support for the programs. Feedbacks must include reports on the key audit findings regarding the appropriate use of antibiotic use with prescribers together with laboratory data on antibiotic susceptibility rates and facility aggregate antibiogram to help inform updates of clinical guidelines. These feedbacks can be communicated with specific action points to promote continuous quality improvement of the process and outcomes measures of the hospital ASP. 15
The finding of this survey showed low feedback on antibiotic susceptibility rates but high on antibiotic use. This may be due to a lack of access to microbiological laboratory infrastructure, poor availability of quality assured laboratories, and surveillance systems coupled with the high fee paying for microbiology services in most hospitals in Africa.66,67
Aside from the many barriers hampering the effective implementation of ASP in the 15 participating public hospitals in Ghana identified above, resistance to program implementation from other HCPs, lack of skilled human resources including infectious disease clinicians and pharmacists, clinical microbiologists, as well as a lack of available time for the performance of AMS-related duties competing with other traditional duties, were reported as other key barriers that needs to be addressed going forward. Some of these barriers have been observed in previous studies as factors that hamper successful implementation of ASPs in hospitals in Ghana and elsewhere.67 -69
We are aware of a number of limitation with our study. Firstly, our study was limited to public hospitals in Ghana for the reason specified earlier. Additionally, it was undertaken in 2 out of the 16 administrative regions in Ghana which may differ in terms of socio-economic and cultural characteristics. It is also worth noting our study did not segregate data based on the site and size of the facility during analysis to determine the statistical differences in the level of implementation of the 7 core elements of ASPs based on these features. Despite these limitations, we believe that the findings in this study will provide useful baseline information of the current level of AMS implementation among public hospitals in Ghana.
Conclusion
There is varied implementation of ASPs among public hospitals in Ghana. Almost all 7 core elements were sub-optimally available in most of the surveyed hospital. However, the most deficient ones that could threaten the effective implementation of AMS included lack of leadership commitment, pharmacy expertize, the level of AMS actions and interventions implemented, monitoring and surveillance of antibiotic use, and their bacteria resistance rates. Pharmacist-led ASPs were found to be associated with their formal training on AMS, leadership commitment, periodic dissemination of AMS activity reports, and formulary for restricted antibiotics development. Key barriers identified included lack of skilled human resources, lack of available time for AMS-related duties, and poor laboratory infrastructure. These needs to be addressed to enhance the routine implementation of ASPs in Ghanaian hospitals in order to achieve the agreed goals of the NAP.
Consequently, the results from this study should encourage further assessment of ASP across both private and public hospitals in Ghana to better understand the nationwide implementation and potential barriers to guide policies and operating procedures toward the fight against AMR.
Footnotes
Authors’ Contribution
Conceptualization: IAS, SC, VB; methodology, IAS, SC, VB; validation, IAS, SC, PY, VB; formal analysis, IS, BBG, VB; investigation, IAS, CS, PY, VB; resources, IAS; data curation, IAS, BBG; writing—original draft preparation, IAS, SC, PY, BBG, VB; writing—All authors; visualization, IAS, BBG, VB; supervision, IAS, SC, PY, VB; project administration, IAS, VB. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.