
Abstract
Keywords
Introduction
Patients admitted to the hospital with COVID-19 infection have been reported to be at high risk of developing coagulopathy,1-6 which is subsequently associated with poor prognosis.2,7 A high incidence of deep vein thrombosis (DVT) and pulmonary embolism (PE) has been reported among COVID patients with incidence rates ranging from 10% to 69%.1,4,6-19 This increased risk of thrombosis in patients with COVID-19 infection suggests they may benefit from higher dosage of anticoagulant to prevent VTE disease.16,19
Anticoagulant therapy for VTE prophylaxis has been associated with better prognosis in patients with severe COVID-19. 20 Other studies have shown reduced mortality among patients with COVID-19 treated with either prophylactic VTE doses or full anticoagulation.20,21 It has then been hypothesized that anticoagulation with heparin administered at doses higher than conventionally used for VTE prophylaxis may improve outcomes. 22 This led many clinical societies and leading institutes to develop guidelines regarding the optimal strategy for prophylaxis of VTE in COVID-19 patients. These guidelines have varied between recommending standard prophylaxis dose, intermediate prophylaxis dose and full therapeutic dose anticoagulation.23-25
Most of the guidelines cite several randomized controlled trials that have focused on the optimal dosing for VTE thromboprophylaxis in moderately or critically ill hospitalized patients with COVID-19.26-33 The trials mostly compared use of standard dose VTE prophylaxis against full dose anticoagulation. These trials have produced varied results. Only a few have compared intermediate dose prophylaxis with standard dose prophylaxis. In these studies, the safety profile for intermediate dose prophylaxis was acceptable.34-36
The optimal agent, timing, and intensity of regimens for preventing VTE in patients with COVID-19 is therefore still not clear. During the initial few months of this pandemic patients with COVID at our institution were treated primarily with standard dose DVT prophylaxis. As the pandemic matured, treatment guidelines were altered to recommend intermediate dose DVT prophylaxis. To better understand the differences in outcomes between patients treated with the standard DVT dose prophylactic versus those treated with intermediate dose DVT prophylaxis, we conducted a retrospective observational study to compare the incidence of symptomatic VTE disease in hospitalized patients treated with different VTE prophylaxis doses within our health system prior to and post the recommendation change.
Methods
Design
We performed a retrospective cohort study of hospitalized adult patients with confirmed COVID-19 infection to evaluate VTE occurrence rates stratified by pharmacologic VTE prophylaxis agents received. Approval was obtained from our local Institutional Review Board prior to initiation. For our retrospective cohorts, we divided the patients into 2 treatment groups based on the dose of DVT prophylaxis they received during their hospitalization that is, either the standard dose VTE prophylaxis or the intermediate dose VTE prophylaxis group. The standard dose DVT prophylaxis group included patients treated with unfractionated heparin 5000 units 2 or 3 times a day or enoxaparin 30 or 40 mg daily. The intermediate dose prophylaxis group included patients treated with unfractionated heparin 7500 units 3 times a day or enoxaparin 40 mg twice a day.
Data Collection
A multi-disciplinary therapeutics committee at Parkview Health System has provided continually updated treatment guidelines for COVID-19. These guidelines are distributed to the hospital medical staff and include recommendations for DVT prophylaxis dosing. Prescribing and dosing of VTE prophylaxis was performed based on the clinical judgment of the treating clinicians with the guidance of the treatment recommendations. The study period was from January of 2020 through September of 2021. Between January 2020 to April 2020 and subsequently after July 2021 hospital guidelines recommended standard dose prophylaxis for VTE prevention in patients with COVID-19 infection that is, either unfractionated heparin 5000 units subcutaneously 3 times a day or enoxaparin 30 to 40 mg subcutaneously daily. Between the period of May 2020 to June 2021, hospital guidelines recommended intermediate dose prophylaxis for patients with COVID-19 that is, unfractionated heparin 7500 units subcutaneously 3 times daily or enoxaparin 30 to 40 mg subcutaneously twice a day. Data was collected on all patients who met criteria and were admitted to 2 major Parkview Health System hospitals during the study period. Patients were identified using ICD-10 diagnostic codes for COVID-19 infection and then screened for eligibility. Exhaustive electronic health record (HER) chart review was then conducted for each subject included in the study, including review of discharge summaries, progress notes, diagnostic testing reports, medical treatment summaries, and procedure reports.
Inclusion and Exclusion Criteria
Patients were included in the study if they had a confirmed positive polymerase chain reaction test for SARS CoV-2 from an oral or nasopharyngeal swab and had received at least 3 doses of unfractionated heparin or 1 dose of low molecular weight heparin (enoxaparin) for venous thromboembolism (VTE) prophylaxis.
Patients were excluded from the study if they were younger than 18 years of age, pregnant, were on full dose anticoagulation at the time of admission (warfarin, intravenous heparin, LMWH or an oral direct anticoagulant), had a diagnosis of DVT or PE at the time of admission, or had active bleeding at the time of admission or presentation to the emergency department. Patients who received both standard dose prophylaxis and intermediate dose prophylaxis during the index hospitalization were also excluded.
Outcome Measures
Standardized outcome definitions were adopted and used for outcome adjudication. The primary outcomes were the occurrence of any venous thromboembolic event (deep vein thrombosis or pulmonary embolism). Primary VTE was defined as thrombosis of upper or lower extremity deep veins as reported on upper or lower extremity venous ultrasound, or pulmonary embolism (as evidenced by CTA chest showing evidence of pulmonary embolism or ventilation perfusion scan showing high probability of pulmonary embolism).
The secondary outcome measure was major or clinically relevant non major bleeding events. included:
No systematic screening protocol for VTE in patients with COVID-19 was in place during the study. Investigations were ordered at the discretion of the treating clinician.
Bleeding was assessed according to the International Society on Thrombosis and Hemostasis definitions of major bleeding and clinically relevant non-major bleeding. 37
Patient demographics and several laboratory values were analyzed and compared between cohorts. These results can be viewed in Table 1. We also analyzed initial unit patient was admitted to that is, medical floor verses ICU.
Baseline Patient Demographic Characteristics.
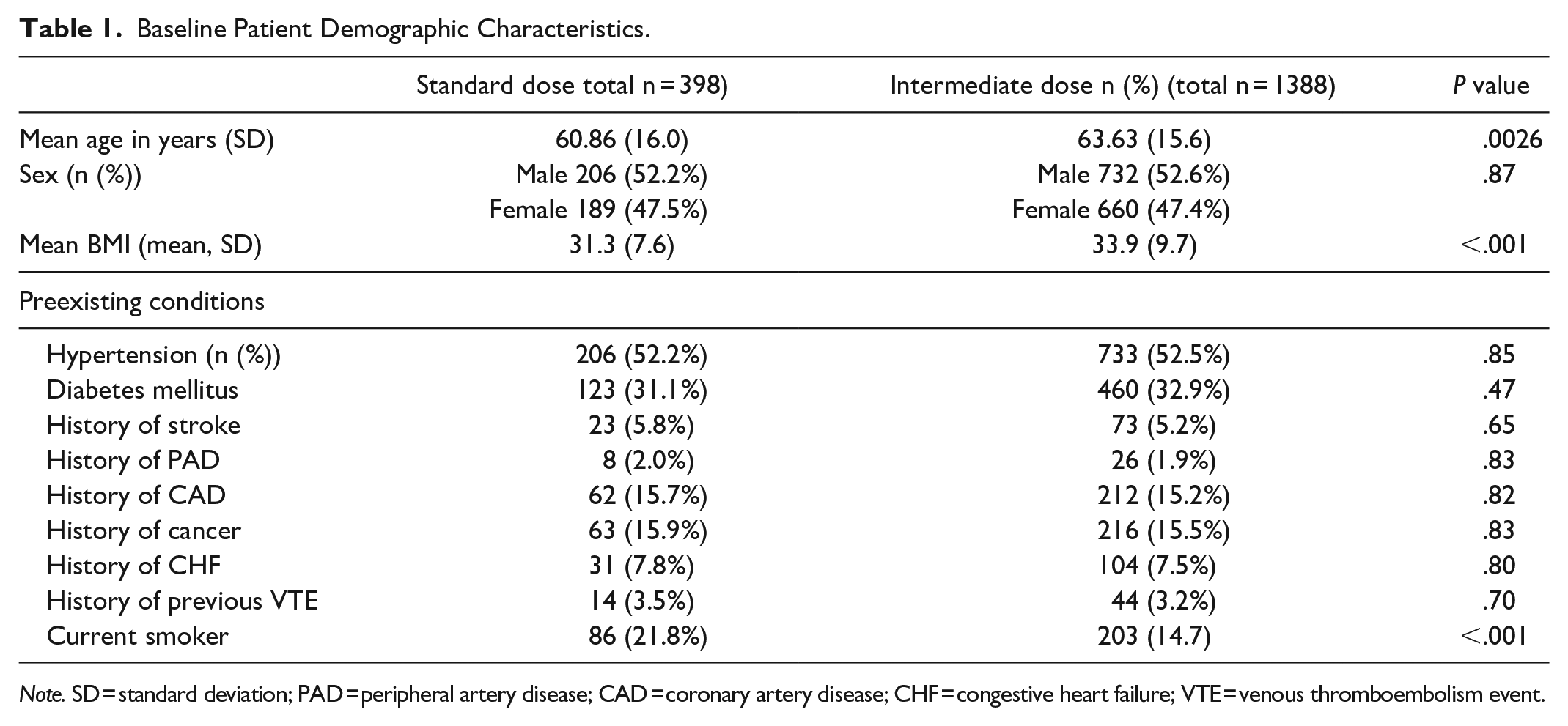
Note. SD = standard deviation; PAD = peripheral artery disease; CAD = coronary artery disease; CHF = congestive heart failure; VTE = venous thromboembolism event.
Statistical Analysis
Descriptive statistics, mean and standard deviation for quantitative variables, and counts and percentages for categorical data were calculated and stratified by dose of DVT prophylaxis received. Statistical methods for comparing the 2 groups were used. To test for statistical significance between the means of the 2 groups, we used the Welch’s t-test as the sample sizes were different in the 2 groups and assumption of homogeneity of variance was not met. Chi-square test of independence was used to determine whether there was an association between categorical variables. Data analysis was performed using statistical models in Python. A P-value of <.05 was considered significant for between group heterogeneity. Multiple logistic regression analysis was used to factor in differences between the 2 study groups with adjustments for potential confounding by age, body mass index (BMI) and history of smoking. BMI was calculated as the weight in kilograms divided by the height in meters squared (weight (kg)/height (m2)).
Results
Patient Characteristics
Figure 1 shows the disposition of the study population. A total of 2483 patient records were reviewed and from these 1786 (72%) adult patients met the inclusion criteria during the study period. One hundred ninety-three patients were excluded from the analysis due to missing data on type of COVID test used. Among the study sample, 398 (22%) patients were primarily treated with standard dose DVT prophylaxis, whereas 1388 (78%) patients were treated with intermediate dose DVT prophylaxis. Patients in the 2 treatment groups were not completely separated by time that is, at any one time during the study period, patients could be found in either treatment group.
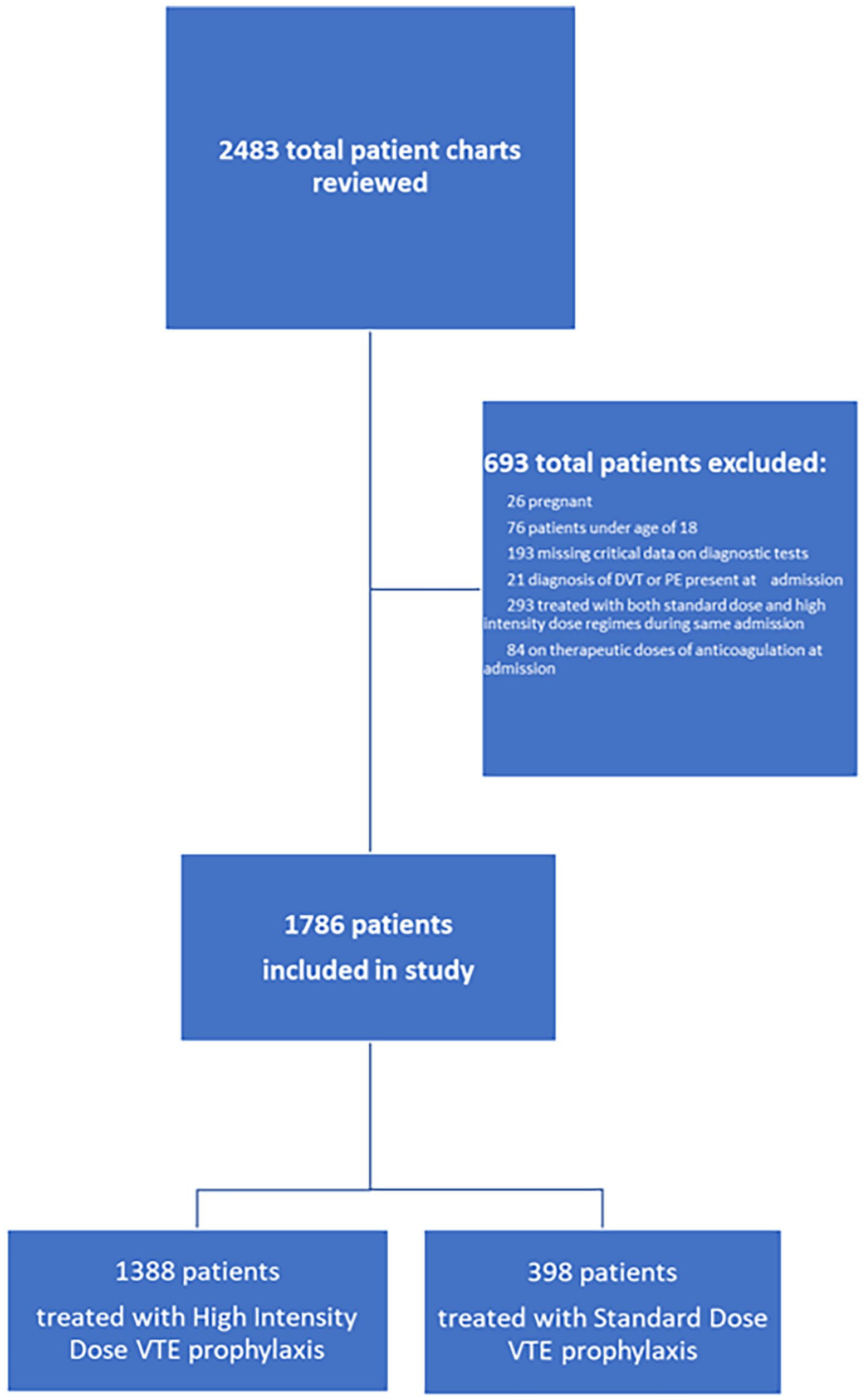
Patient flow diagram showing screening and enrollment of patients.
Table 1 outlines the main demographic characteristics of patients in both treatment groups. Patients treated with intermediate dose DVT prophylaxis were about 2.7 years older compared to those treated with standard dose prophylaxis. That is, 63.6 years (SD = 16.0) versus 60.9 years (SD = 15.6) P = < .001. The standard prophylaxis treatment group had more current smokers compared to the intermediate prophylaxis dose treatment group (21.8% vs 14.7%, P = < .001). The rest of the patient demographics were similar between the 2 treatment groups. See Table 1.
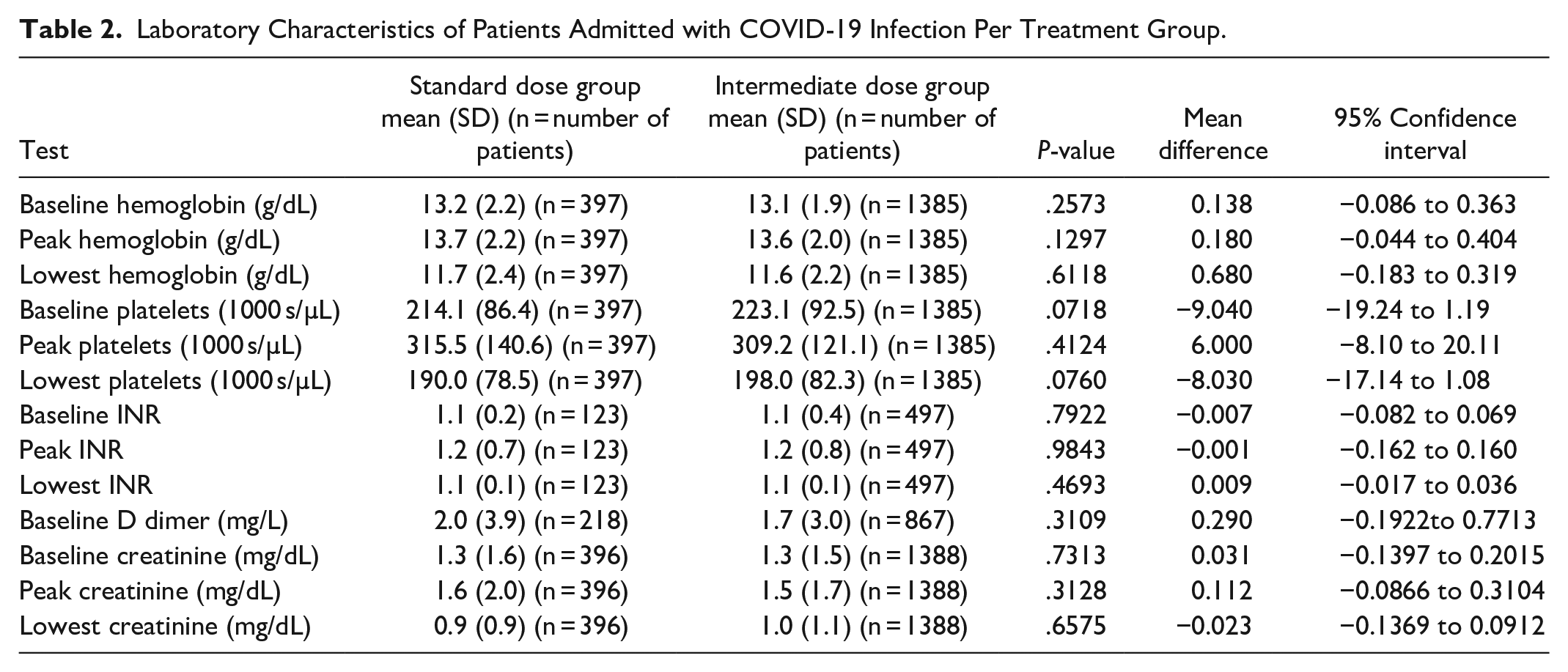
We also evaluated baseline laboratory characteristics. There was no statistically significant difference between the 2 treatment groups in terms of baseline and mean hemoglobin, baseline and peak creatinine level, baseline D-dimer level, or level of platelets. See Table 2.
Laboratory Characteristics of Patients Admitted with COVID-19 Infection Per Treatment Group.
The number of patients admitted directly to the ICU was similar between the 2 treatment groups. See Table 3.
Results for Number of Days Patients received VTE Prophylaxis and Proportion of Patients Initially Admitted to the ICU.

The mean number of days patients received VTE prophylaxis during the admission were similar between the 2 treatment groups, that is, 5.4 (SD) days versus 5.7 (SD) (Table 3).
Primary Outcome: Incident Venous Thromboembolic Event During Hospitalization
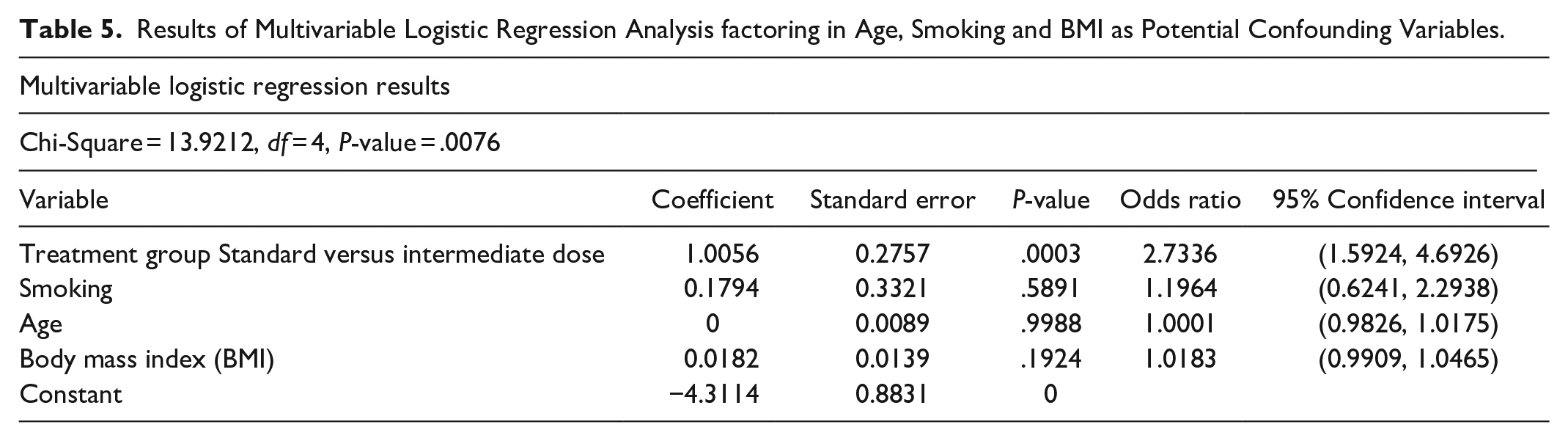
Overall, a total of 60 patients (3.4% of all subjects in the study) with COVID-19 infection were diagnosis who were diagnosed with an incident venous thromboembolic event during their hospitalization. There was a significantly higher incidence of VTE events noted in the standard dose prophylaxis treatment group when compared with the intermediate dose prophylaxis group (25/398 (6.3%) vs 35/1388 (2.5%) P < .001, [Odds Ratio 2.6197, 95% confidence interval = 1.5482-4.4327]. see Table 4). Multivariable-adjusted logistic regression, adjusting for age, obesity, and smoking, with the intermediate dose prophylaxis treatment group as the referent category revealed higher odds for incident VTE events in the standard dose prophylaxis group. The adjusted odds ratios were 2.7336 [95% confidence interval = 02131-0.6280] see Table 5. This Odds ratio means that patient treated with standard dose DVT prophylaxis had 2.7 greater odds for incident VTE during hospitalization than those treated with intermediate dose DVT prophylaxis.
Primary Outcomes of Total VTE events and Secondary Outcome of Bleeding Events in COVID-19 Patients.

Results of Multivariable Logistic Regression Analysis factoring in Age, Smoking and BMI as Potential Confounding Variables.
Secondary Outcomes: Bleeding Events
A total of 55 significant bleeding events were noted. There was no statistically significant difference in bleeding events between the 2 treatment groups (9 (2.3%) for standard dose prophylaxis group vs 46 (3.3%) for intermediate dose prophylaxis group P = .26). See Table 4.
Discussion
In this retrospective cohort study, we observed a higher incidence of VTEs in hospitalized patients with COVID-19 infection receiving standard dose DVT prophylaxis as compared to those patients receiving intermediate dose DVT prophylaxis. This difference persisted after multivariable-adjusted logistic regression analysis factoring in smoking, age and BMI. Heparin is known to have both antithrombotic and anti-inflammatory effect and it is possible that the intermediate dose prophylaxis regime may be more effective than the standard dose regime in preventing thrombotic events in our study population. Two studies completed before the onset of the COVID-19 pandemic had suggested that intermediate dose VTE regimes may be more effective in preventing VTE events in hospitalized patients.38,39 Previous studies evaluating the effect of VTE prophylaxis dosing in COVID 19 patients have produced conflicting results. The INSPIRATION trial evaluated the effect of intermediate dose VTE prophylaxis versus standard dose VTE prophylaxis similar to our study. 31 In the INSPIRATION trial, there was no statistically significant difference in the primary outcome of adjudicated venous or arterial thrombosis between the two treatment groups. The overall rate of DVT was about 3.5% which overlaps with the incidence rate we observed in our study.
In general, the total incidence rates of VTE events in our study of 3.3% (95% confidence interval: 1.8%-5.2%) were lower than have been reported in other studies that have reported DVT/PE rates as high as 32% (95% confidence interval: 25%-40%). 40 This is likely accounted for by the retrospective nature of our study. There was no routine screening for VTE events and only clinically manifested events would have been diagnosed in routine care of the patients. Most patients with either DVT or PE in studies showing high rates of VTE are asymptomatic that is, without additional symptomatology distinguishable from COVID-19 itself, and are diagnosed on routine screening.24-26,29,31
Baseline characteristics between the 2 treatment groups were in general similar other than statistically significant difference in age, BMI, and smoking. The population in the intermediate dose prophylaxis group was older by about 3 years (63 vs 60). Meta-regression analysis of previous studies has not shown an association between mean age and the prevalence of DVT/PE in patients with COVID-19. 40 Furthermore, if anything, age would be expected to increase the risk of VTE events rather than lower it. It is noteworthy that at our institute, a patient’s age was not used as a criterion for determining which dose of DVT prophylaxis was used during treatment.
Patients who received intermediate dose prophylaxis also tended to have a higher BMI (BMI 33.9 vs 31.3; P < .001). One possible explanation is that the treatment guidelines did recommend an intermediate dose prophylaxis for DVT prophylaxis in patients with a BMI of >40 kg/m2 during the period when our institution was once again recommending only standard dose prophylaxis for VTE prophylaxis.
Rates of current smoking were noted to be statistically significantly higher in the standard prophylaxis dose group. This could certainly have played a contributory role of increasing VTE risk in this treatment group. However even when the rate of active smoking was factored into multivariable logistic regression analysis, the incidence rate of VTE events remained statistically significantly between the 2 groups, suggesting that smoking was independently associated with the differences in incidence of VTE between the 2 groups.
The study populations were also very similar in terms of which unit of the hospital the patients initially admitted to, with about 15% of patients in both treatment groups requiring initial admission to the ICU. While this is not an accurate measure of severity of illness, it still suggests similarity in that regard between the 2 treatment groups. Previous studies have shown more benefit for higher than standard VTE doses of heparin or Low molecular weight heparin in non-critically ill patients and less benefit from intensifying anticoagulation in more severely ill patients.24,26 One suggestion for this phenomenon was that initiating therapeutic dose anticoagulation in patients with severe COVID-19 infection may not be enough to alter the consequences of an already severe disease process. 26
The rate of complications such as bleeding events or arterial events were not statistically significantly different between the 2 treatment groups. As would be expected there was a propensity for higher bleeding rates in the intermediate dose prophylaxis group.
Overall, this study looked at hospitalized patients with COVID-19 infection regardless of illness severity. While this can be seen as lacking discrimination for specific patient populations, it is also pragmatic as many hospital guidelines regarding VTE prophylaxis dosing are typically broadly applied regardless of level of care.
There are several limitations with our study. Firstly, the retrospective and observational nature of the study is an inherent weakness. There was no routine screening for VTE events and so asymptomatic DVTs or PEs could have been missed and hence affecting the overall rates of the primary outcomes. Secondly, we did not evaluate the severity of the illness in patients within the 2 treatment groups and it is conceivable that severity of illness could have contributed to outcomes. Our analysis showed similar rates of ICU admission between the 2 treatment groups suggesting the populations were similar. We also did not assess the effect of duration of prophylactic anticoagulation on VTE events.
Establishing the optimal regime for VTE prophylaxis in patients with COVID-19 infection is essential because of the reported higher prevalence of VTE events in this population. It is our hope that this study will add to the pool of knowledge regarding VTE prophylaxis in patients hospitalized with COVID-19 infection. We are cognizant of the fact that this pandemic has not been a static one, with ongoing evolution of the virus itself resulting in changes in virulence and severity of illness which may affect optimal VTE prophylactic dosing in this patient population.
Conclusion
In our study of patients hospitalized with COVID-19 infection, patients receiving intermediate dose prophylaxis experienced lower incident rates of VTE events compared to those receiving standard dose DVT prophylaxis without a statistically significant increase in the risk of bleeding events.
Footnotes
Acknowledgements
Emily Schroeder MD PhD.
John Falatko MD.
Disclaimers
The views expressed in the submitted article are the authors’ views and not an official position of the institution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.