
Abstract
Key Highlights
Almost all hospitalized cardiac patients admitted to tertiary care teaching hospitals encountered pDDIs.
The prevalence of clinically significant pDDIs was 5%, yet the majority of the pDDIs encountered (75%) (belonged to category C) warrants clinical monitoring.
Acute coronary syndrome, use of >10 drugs, and parenteral formulations were significantly associated with increased risk of pDDIs.
Introduction
The presence of multiple comorbidities in an individual inevitably presses for the recommendation/prescription of multiple drugs in outpatient and inpatient settings. This polypharmacy, defined as the regular use of 5 or more drugs, can eventually lead to numerous potential drug-drug interactions (pDDIs).1,2 pDDIs would mean those drug interactions known to occur due to concomitant administration of drugs irrespective of any adverse event following and may engender unexpected adverse drug reactions (ADRs), increased duration of hospital stay or readmissions, and in extreme cases, can also result in deaths.2,3 Therefore, these pDDIs, sooner or later, may precipitate drug toxicity and/or therapeutic failure, thereby creating a burden on both the health and economy of the patients.
ADRs, which are significantly contributed by DDIs (going as high as 30%), contribute about 0.6% to 5% to the incidence of hospitalization.4,5 The more concomitant drugs prescribed, the higher the risk of pDDIs in the patients. The risk of pDDIs can increase to 50% and 100% with 5 or 8 drugs, respectively. 6 In cases of cardiovascular disorders (CVDs), the average number of drugs per prescription ranges from 3 to 9; hence the prevalence of pDDIs in such scenarios is expectedly high, for example, 87.2% in Brazil, 21.3% in Nepal, 58.3% in Netherland, 27.3% in the USA and 56% in Bangladesh.3,7-14 This prevalence ranges from 30% to 99.6% in India.15-17 There might be other contributing factors, such as old age, the pharmacokinetic and pharmacodynamic nature of drugs prescribed, and the effect of cardiac disease on drug metabolism. 18 Another interesting facet to look out for is that CVDs, which include hypertension, cardiac failure, arrhythmias, coronary artery disease, and others, are frequently accompanied by other morbid conditions such as diabetes mellitus, thyroid disorder, and dyslipidemia. Consequently, polypharmacy results in higher chances of pDDIs and ADRs.
Various online databases are available that are commonly used for screening pDDIs, for example, Lexicomp interaction module, Micromedex drug interactions, Stockley’s drug interactions, Clinical Pharmacology Drug Interaction Report, and others. Many studies have compared their sensitivity to screen and detect pDDIs. Accordingly, Lexicomp Interactions, Micromedex, and Clinical Pharmacology Drug Interaction Report have been identified as reliable and sensitive tools for screening pDDIs.19-22
A compelling outcome from one of our umbrella studies on the drug prescription parameters guided us toward identifying a higher occurrence of pDDIs among inpatients of the cardiac department. 23 To further delineate and comprehend the prevalence and factors affecting pDDIs among cardiovascular drugs, this study was outlined to collect robust and meticulous data which could help limit ADRs associated with various drugs used in managing different cardiac diseases, thus promoting safer pharmacotherapy and ultimately improving therapeutic outcomes. The study findings will be helpful not only to physicians but also to other healthcare professionals like nursing staff, clinical pharmacists, and paramedics.
Methods
Study Design and Setting
The study was outlined as a retrospective observational study from April 1st, 2021, to December 31st, 2021, at the Department of Pharmacology in association with the medical records section, All India Institute of Medical Sciences (AIIMS) Raipur, Chhattisgarh, India. The Institutional Ethics Committee (IEC) of All India Institute of Medical Sciences Raipur, Chhattisgarh (www.aiimsraipur.edu.in) approved the study vide letter no. 1591/IEC-AIIMSRPR/2021 dated March 27th, 2021. The authors followed ethical principles for medical research as per the Declaration of Helsinki. The study involves retrospective data analysis, so informed consent is not required. This medical institute is an essential public tertiary care teaching hospital. In the last 2 years, the total number of outpatients were 530 050 and 267 230, while the total inpatients were 23 846 and 22 863, respectively.24,25 In our previous study, the maximum number of pDDIs were noted among drugs acting on the cardiovascular system; hence in the present study, we analyzed all the pDDIs based on the drug information available in the medical records of patients who were admitted in cardiology department in 2019. 23
Inclusion and Exclusion Criteria
The medical records of inpatients (defined as those admitted for at least 24 hours at the cardiology wards or cardiac intensive care units [CCUs]), which were complete and had at least 2 different drugs, were included for analysis. Incomplete records or records of patients admitted in the cardiology wards for <24 hours were excluded from the analysis. Data of individual patients were counted once in their order of admission, and in case the authors encountered data of multiple admission of the same patient, then they were excluded.
Data Collection
The data collection was performed in association with the medical records section, which included the patient’s socio-demographics, primary diagnosis, comorbidities, duration of hospital stay, and medication data. The dose and duration of the drugs prescribed were noted for every day individually from respective treatment charts. Each day had an individual treatment chart, and the total number of treatment charts was equal to the duration of stay in the hospital. The total number of drugs, drugs prescribed by generic name, and drugs from the National List of Essential Medicines 2015 (NLEM) were also noted. Screening for pDDIs was done with UpToDate Lexicomp drug interactions tools with institutional access. 26 Lexicomp is a sensitive and specific pDDIs screening tool that classifies them into class A (no known interaction, ie, no interaction exists between the specified agents), B (no action needed, ie, as the specified drugs may interact, but there is no clinical concern associated), C (monitor therapy, ie, documented that the benefits of an interaction outweigh the risk, appropriately monitor therapy in order to avoid potential adverse outcomes, dose reduction may be required of either one or both drugs), D (consider therapy modification, ie, the interaction is of clinical concern and patient status must be assessed whether benefits of concomitant use of drugs outweigh the risks and proper actions must be taken to realize the benefit and reduce the risks resulting from an interaction), and X (avoid combination: the risk of an interaction outweighs the benefits and are usually contraindicated/avoided).22,27 The pDDIs belonging to Category D or Category X were considered clinically significant.
Statistical Analysis
The data has been presented as descriptive statistics, that is, frequencies, percentages, mean, and standard deviation, as appropriate. Those prescriptions with category D and/or X pDDIs were considered for final assessment. The data has been presented as mean or percentage for continuous or categorical data. Multiple logistic regression was used to analyze the association between factors and the occurrence of clinically significant pDDIs, and a P-value < .05 was considered statistically significant.
The factors which might affect the clinically significant pDDIs were mainly based on previous literature and were divided into 2 categories, that is, patient-related factors (age, sex, diagnosis, comorbidities, duration of hospitalization) and drug-related factors (number of drugs per day, drugs used as fixed-dose combinations, drugs prescribed as parenteral formulation, and use of antibiotics). The use of fixed-dose combinations and parenteral preparation is widespread in cardiac settings; hence, the authors chose to analyze their association with clinically significant pDDIs. Furthermore, cardiac patients usually have other comorbidities, especially diabetes, hypertension, and dyslipidemia. Hence the authors also inspected the presence of a total number of morbidities and the triad of diabetes, hypertension, and dyslipidemia and whether they are risk factors for clinically significant pDDIs. Since acute coronary syndrome (ACS) was the most common condition leading to admission, the authors assessed its relation with clinically significant pDDIs.
Results
Three hundred sixty-two patients were admitted to the Department of Cardiology in 2019. Out of them, complete details of about 338 patients were available for evaluation and analysis, and the data is presented as per the records available. The mean age of these patients was 56.8 ± 9.9 years; the majority of them were male (n = 230, 68%) and commonly admitted for management of ACS (n = 279, 82.5%). The mean duration of hospital stay was 5.2 ± 2.7 days (range 2-24), during which they received 9.9 ± 2.6 drugs per day (range 2-20). These patients, on average, had more than 3 morbidities. The demographic and clinical characteristics of these patients have been presented in Table 1.
Demographic and Clinical Characteristics of Patients.
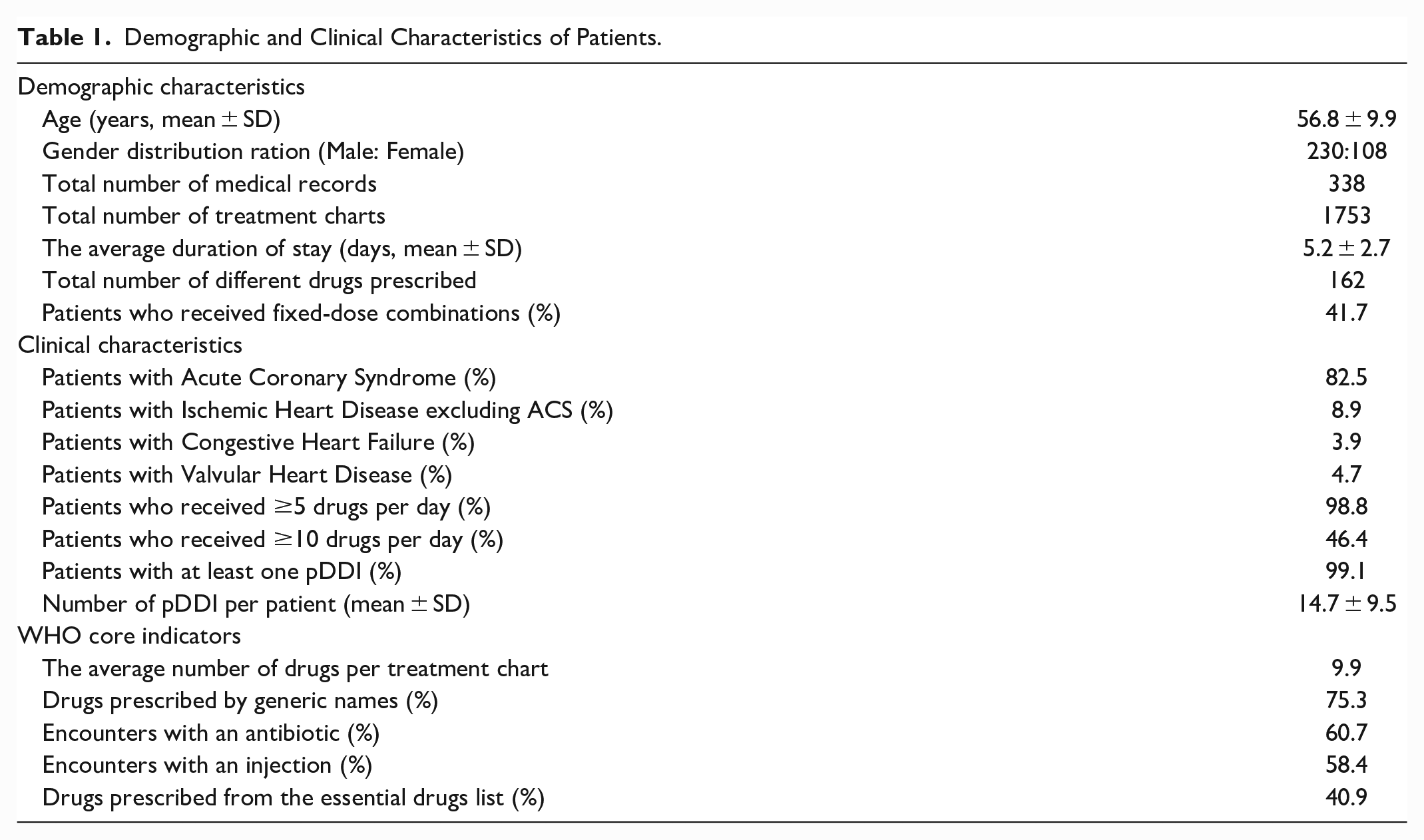
During our analysis, we found a total of 4966 pDDIs among 338 medical records, accounting for a mean of 14.7 ± 9.5 pDDIs (0-49) per patient, and 335 (99.1%) of them had ≥1 pDDI. Category C (75.3%) was the most common, followed by category B (19.6%). The pDDIs belonging to categories D, X, and A were 4.8%, 0.3%, and 0.08%, respectively.
The common category D pDDIs we observed were heparin + aspirin + clopidogrel (can increase risk of bleeding), glimepiride + metformin + teneligliptin (increased risk of hypoglycemia), and metformin + ranolazine (can lead to increased concentration of metformin). Similarly, the most frequent category X pDDIs encountered were ramipril + telmisartan (which can increase the risk of hypotension), cefuroxime + ranitidine, and cefuroxime + pantoprazole (in both of these combinations, there is a risk of reduced absorption of the antibiotic). Most category D and X interactions (91.9%) are pharmacodynamic. These pDDIs and their likely consequences have been detailed in Table 2. Interestingly, statins (atorvastatin or rosuvastatin) were found in numerous prescriptions, yet no pDDIs with them were found belonging to category D or X. Also, most of the patients were prescribed heparin or its analogs, but the use of oral anticoagulants was quite limited. A total of 177 (52.4%) patients had ≥1 category D and/or X pDDIs. Of these 177 patients, 129 (72.9%) had one, and 33 (18.6%) had only 2 clinically significant pDDIs.
Drugs involved in Category X and D pDDIs with their Mechanism and potential Results.
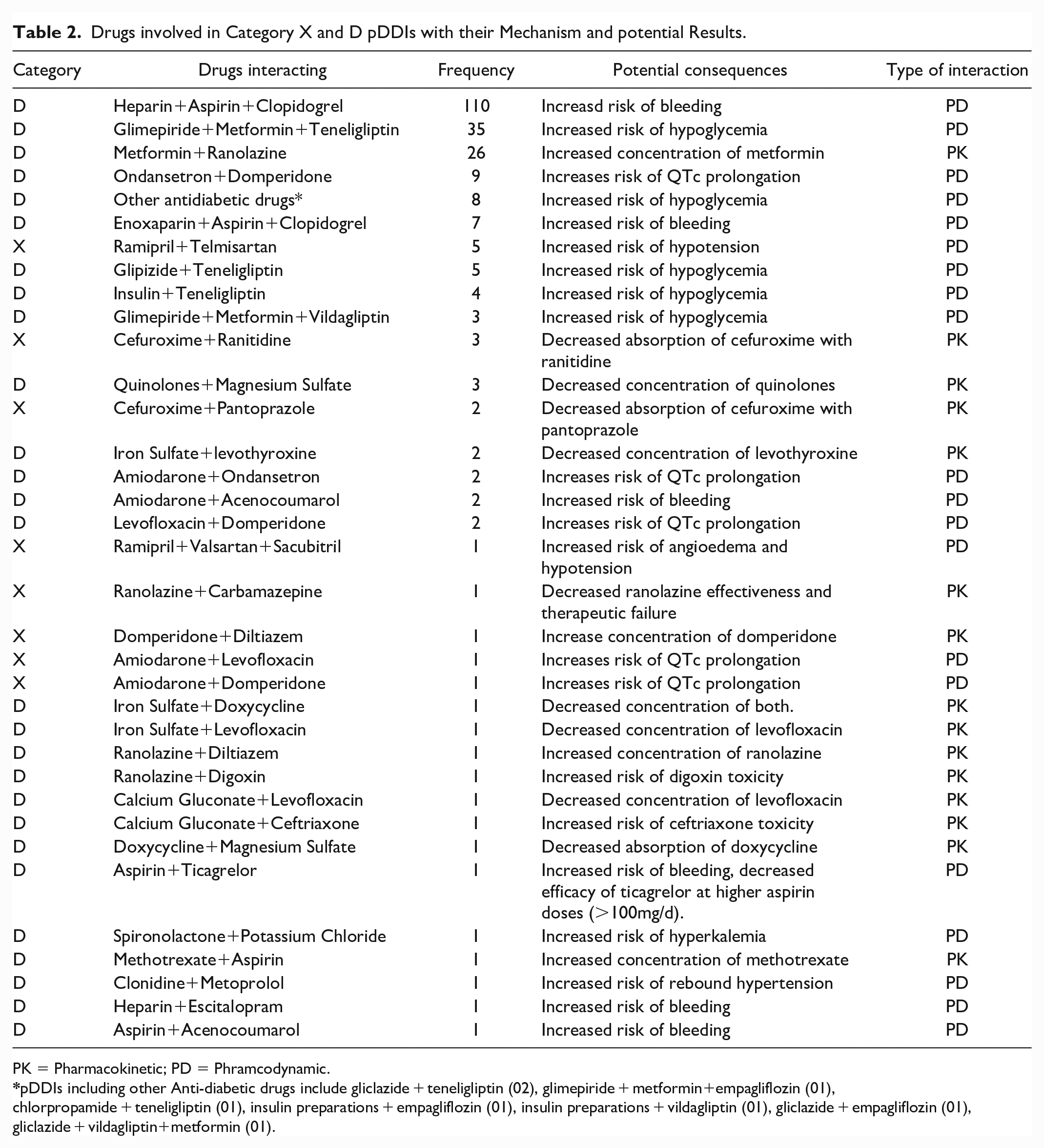
PK = Pharmacokinetic; PD = Phramcodynamic.
pDDIs including other Anti-diabetic drugs include gliclazide + teneligliptin (02), glimepiride + metformin+empagliflozin (01), chlorpropamide + teneligliptin (01), insulin preparations + empagliflozin (01), insulin preparations + vildagliptin (01), gliclazide + empagliflozin (01), gliclazide + vildagliptin+metformin (01).
In the analysis, the authors assessed the risk factors for category D and/or X pDDIs. The diagnosis of ACS (OR = 2.33; 95% CI: 1.1-5.12; P = .03), use of >10 drugs per day (OR = 2.46; 95% CI: 1.27-4.82; P = .008), and drugs prescribed as parenteral formulations (OR = 1.84; 95% CI: 1.57-2.21; P < .0001) had significantly higher prevalence of clinically significant pDDIs. The authors have considered > 10 drugs as a predictor of clinically significant pDDIs because the mean number of drugs per treatment chart was ~10.
Female sex (OR = 1.39), prescription of fixed-dose combinations (OR = 1.48), and presence of a triad of diabetes, hypertension, and dyslipidemia (OR = 1.78) were also associated with a higher risk of clinically significant pDDIs, which was statistically not significant. Age, comorbidities, duration of hospital stay, and usage of antibiotics were not associated with clinically significant pDDIs. The exact details are presented in Table 3.
Factors Affecting Category D and/or X pDDIs.
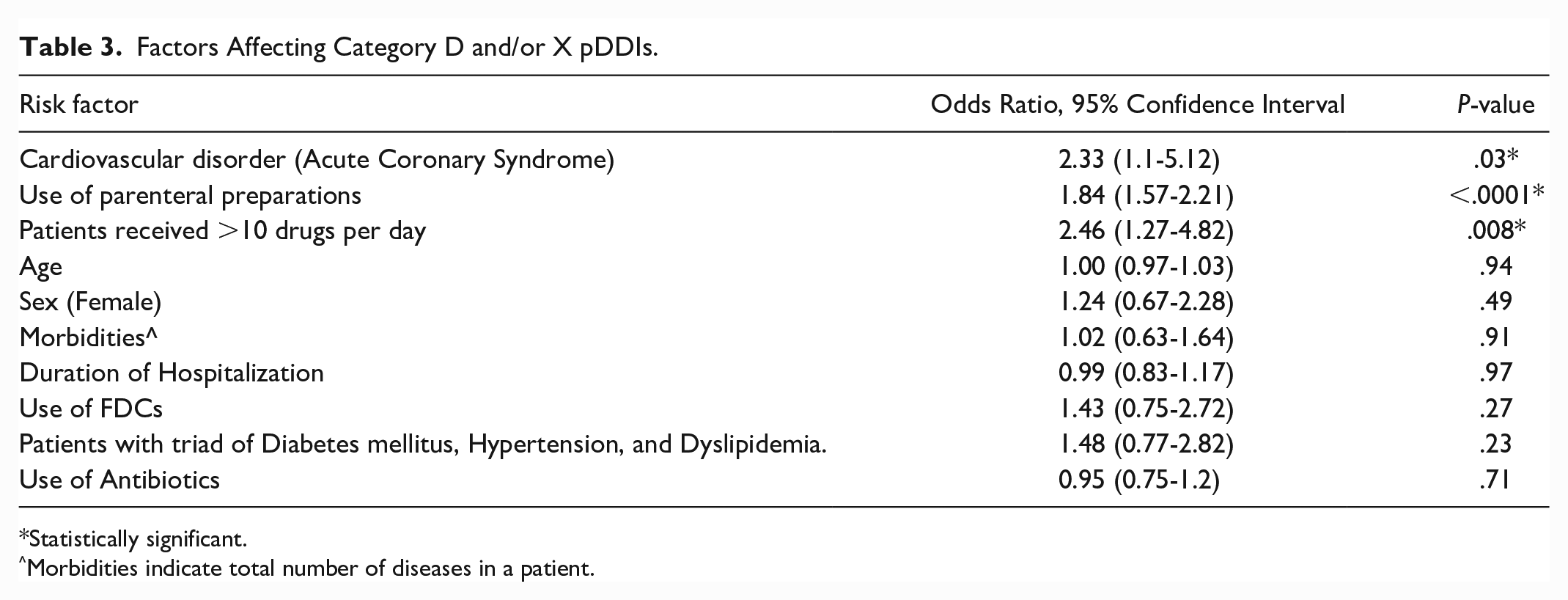
Statistically significant.
Morbidities indicate total number of diseases in a patient.
Discussion
In this retrospective analytical study, we evaluated the frequency and categories of pDDIs and the risk factors associated with their occurrence. The mean age of patients whose records we analyzed was 56.8 years, with the majority being male. Moreover, the most common diagnosis for which these patients were admitted was found to be ACS, with a mean duration of hospital stay being 5.2 days. These findings follow the usual epidemiological trends of CVDs.3,8,9,17 The proportion of patients with at least one pDDI in our study was 99.1%, which is relatively higher than a few published studies3,15 but similar to others.7,9,18 During the analysis, we also observed that, on average, 10 drugs were being prescribed per patient, which we found to be higher than reported in certain studies3,9,17 and similar to one study. 7 In our research, we reported that most of the pDDIs encountered belonged to category C (as per the rating scale mentioned in the methodology), which agrees with the previous studies where a similar rating scale was used.7,9,17 Furthermore, akin to former studies, in our study, the majority pDDIs were pharmacodynamic.3,8,9,15,17 Principally the demographic and basic characteristics were relatable to the previously published studies.
The authors observed that the risk of encountering pDDIs of category D and/or X was independent of age, comorbidities, concurrent use of antibiotics, and duration of hospital stay. In previous studies, identical findings have been reported, as age is unrelated to an increased risk of having clinically relevant pDDIs.7,9,17 In contrast, in a few studies, patients of the geriatric age group had a higher risk of pDDIs.3,10,18 The association of comorbidities with clinically significant pDDIs is equivocal, while few studies showed a positive correlation,11,17 and others did not report so.7,9 In our study, the simultaneous use of antibiotics was not found to be associated with the occurrence of category D and/or X interaction. Though in a previous study, infectious diseases were associated with an increased risk. 9
Another critical finding, we observed was that the duration of hospitalization was not associated with clinically significant pDDIs. The possible reason for this observation could be that the data in our study has been analyzed as a continuous variable. In contrast, in the previous studies, it was evaluated as a categorical variable.3,8,11,18
Female patients, those with a triad of DM, hypertension, and dyslipidemia, and those prescribed FDCs had a higher risk of clinically significant pDDIs, though not statistically significant. While with Alike to present study, sex was not a predictor for the occurrence of pDDIs,3,7,8,17,18 while in one study, females had more clinically relevant pDDIs, and in another study, males were more predisposed.9,10 The possible reason for these discrepancies could be the variable endpoints and the application of different scales for grading pDDIs.
The patients who received >10 drugs per day had a significantly higher risk of experiencing clinically significant pDDIs, comparable to previous studies.3,7-9,11,17,18 The patients with a primary diagnosis of ACS and using parenteral formulations had a considerable risk of encountering clinically significant pDDIs. The use of FDCs and parenteral formulations were new parameters that had not been assessed previously and were novel findings from our study. CVD patients are known to have multiple comorbidities, so drugs are routinely prescribed in combinations to reduce the pill burden and improve compliance with the therapy. 28 Despite such benefits of FDCs, their use escalates the risk of pDDIs. ACS is an emergency where the parenteral formulation is unavoidable, supporting our findings as both are significant predictors of clinically significant pDDIs.
In consensus with previous studies, we also observed that pDDIs encountered during analysis were common with anticoagulants and anti-platelets group of drugs.7,8,15,17 Both of these groups are prescribed routinely to patients with CVDs. Hence this observation was anticipated. 29 The other groups of drugs commonly involved were the hypoglycemic agents (oral and/or parenteral). In almost all of the patient records analyzed, we found that the combination of aspirin and clopidogrel (as an FDC) was prescribed frequently. Furthermore, if the patient required hypoglycemic agents, that was added as an FDC. Even though these FDCs offer an array of advantages to both the patient and the physician, there are a few crucial disadvantages associated with their use, such as difficulty in dose titration, therapeutic duplication, and increased risk of adverse reactions. 30
We also detected another recurrent pDDI between metformin and ranolazine. The interaction is likely to occur at a higher dose of metformin (>1700 mg/day) and ranolazine (1000 mg twice daily), and plausibly these drugs are co-prescribed due to the favorable effects offered by ranolazine to the patients of chronic stable angina and diabetes, in whom beta-blockers are to be avoided. 31 Also, ranolazine has the upper hand over beta-blockers in patients with asthma/chronic obstructive pulmonary disease, diabetes mellitus, bradycardia, AV block, hypotension, peripheral arterial disease, and vasospastic angina. 31 The pDDIs that were less frequent but with potential adverse outcomes were between angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs), resulting in hypotension. Furthermore, co-prescribing amiodarone with levofloxacin or/and domperidone increased the risk of QTc prolongation, which may be even more troublesome in CVD patients. The lack of clinically significant pDDIs among statins and co-administered drugs makes the former remarkably safe. Most pDDIs involving statins belonged to category B or C, which required monitoring only. Lesser use of oral anticoagulants can be attributed to their use in IHD (including ACS, which was the leading cause of admission [91% of patients]) has a limited role. At the same time, heparin and its analogs are recommended in such conditions. 32
Potential drug-drug interactions are the most common drug-related problems encountered in inpatients, and most pDDIs do not lead to an adverse clinical outcome.33,34 Even though the risk of adverse outcomes following pDDIs seems to be less, the seriousness of this outcome cannot be ignored. Electronic databases for screening pDDIs appear to be an attractive option to minimize such risk. The current databases may prove to help avert such unexpected pDDIs and rationalize pharmacotherapy. However, the downside of these screening tools is that they may show a vast number of interactions that could be clinically irrelevant as well. The key lies somewhere between fine-tuning the technology and the same supplementing clinical decision-making to improve patient care.
Our study was retrospective, and the authors did not follow up on these patients. Hence, the exact clinical outcome of these clinically significant pDDIs remains uncharted. For this purpose, a similar but prospective analysis would be an appropriate alternative to overcome these inconveniences and establish temporal relations between the occurrence of pDDI and adverse clinical outcomes. Moreover, since this was a record-based study (whereby only documented clinical status was available for analysis), it would be challenging for the authors to comment on the rationality of prescriptions. We would also like to bring focus onto another limitation that Lexicomp per se as software does not partake patient’s clinical condition and timing of drug administration into consideration, as a result of which specific drug interactions which might have been classified into category D or X may not have any adverse clinical outcome; instead, those drug combinations may end up proving beneficial to the patients.
Further, as it was a retrospective study, the findings can be a guide to reducing pDDIs in the future. As the institute followed NLEM-2015 in 2019, the included drugs in the list would likely appear as interacting drugs. Presently, routine use of Lexicomp for identifying interactions is being encouraged in the institute.
Conclusion
In the present study, the authors found a very high prevalence of pDDIs in patients with CVDs who were admitted to the tertiary-care teaching hospital in central India. Most of the pDDIs belonged to category C and required monitoring of therapy. The clinically significant pDDIs were associated with patients who had ACS, parenteral formulation, and received >10 drugs per day. The anti-platelets, anticoagulants, ACEIs, ARBs, and hypoglycemic agents were mainly involved in clinically significant pDDIs. Incorporating pDDIs screening tools and clinical pharmacologists in the multidisciplinary team will help prevent pDDIs, thus alleviating drug-related problems. More prospective studies on similar chains of thought are required to consolidate these findings.
Supplemental Material
sj-txt-1-hpx-10.1177_00185787231182569 – Supplemental material for Assessment of Potential Drug-drug Interactions (pDDIs) and Their Risk Factors Among Hospitalized Cardiac Patients in a Tertiary-care Center of Central India: A Retrospective Record-based Study
Supplemental material, sj-txt-1-hpx-10.1177_00185787231182569 for Assessment of Potential Drug-drug Interactions (pDDIs) and Their Risk Factors Among Hospitalized Cardiac Patients in a Tertiary-care Center of Central India: A Retrospective Record-based Study by Ajaya Kumar Sahoo, Alok Singh, Dhyuti Gupta, Suryaprakash Dhaneria and Prachi Arunima in Hospital Pharmacy
Footnotes
Acknowledgements
The authors thank Mr. Kalleshwara Iyyanahalli (In-charge Medical Records Department) for his support during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.