
Abstract
Background and Objectives:
Cardiovascular disease (CVD) is a major cause of premature mortality and morbidity in the UK and globally, driving health inequality and spiralling healthcare costs. Reducing CVD and its risk factors is a global policy priority. There is growing recognition that CVD risk trajectories are shaped in early life, with risk factors developing in children aged as early as 3–11 years, leading to later CVD events. Our objective with this study was to advance the evidence base on cardiovascular health promotion with children through primary schools.
Methods:
We conducted a systematic mapping and review of reviews to examine the factors associated with successful cardiovascular health promotion in primary schools and the intervention elements that impact knowledge and behaviour. Our work was informed by the needs of a community-based CVD-prevention initiative in London which sought to address the challenge of high CVD and childhood obesity rates locally.
Results:
Of 141 articles screened, only 15 focused on CVD health. Key findings revealed that curriculum-based approaches embedded in school routines and complemented by engaging children in a process of experiential learning can lead to statistically significant improvement in both knowledge and health behavioural change outcomes. The evidence shows that supporting children to attain positive CVD health-related behaviours is vital as they enter the foundational years of compulsory education.
Conclusion:
Schools, in particular primary schools, are crucial for early modelling and establishing the lifelong healthy habits that will positively impact children’s healthy behaviours and the wider population’s CVD health.
Keywords
Introduction
Cardiovascular disease (CVD) is a major cause of premature morbidity and mortality in the UK, particularly in areas of the country with greater deprivation and health inequality (Cheema et al., 2022; Nadarajah et al., 2023). CVD is also a global challenge and leading cause of death globally, accounting for 17.9 million deaths annually, accounting for 31% of all deaths worldwide (Højstrup et al., 2023; WHO, 2021). CVD places a substantial economic burden on healthcare systems and wider society through lost productivity and long-term care costs (Luengo-Fernandez et al., 2023).
Despite a 36% reduction in CVD mortality in the UK over the last two decades, it still contributes to a third of all deaths each year. Importantly, with rising levels of adult and childhood obesity and diabetes, along with worsening health and social inequality over the last decade, even those early gains are now threatened. Gains in life expectancy have begun to slow, with some areas now showing a clear reverse trend (Welsh et al., 2021). Recognising this challenge, the UK National Health Service (NHS), with successive Long Term Plans (NHS England, 2019, 2025), has identified CVD prevention as a major priority, while Public Health England has established ambitions about risk factor control to mitigate the growing CVD threat. These priorities are consistent with global frameworks such as the WHO Global Action Plan for the Prevention and Control of noncommunicable diseases and the UN Sustainable Development Goals, which emphasise the importance of early prevention (United Nations 2015; WHO, 2013). The influential review Health Equity in England (Marmot et al., 2020) listed better prevention and maintenance of wellbeing as key factors in attempts to build back fairer after the COVID-19 pandemic.
The focus population of this study – East London – is home to a diverse, multi-ethnic population with high levels of social deprivation. Significant health and social inequality manifests most dramatically in the life expectancy gap of over 10 years compared to West London. A large proportion of this health inequality is driven by CVD. East London records some of the highest levels of premature heart attacks in the region, with an estimated 10% of all heart attacks occurring before the age of 50 (local audit data, Barts Health). Addressing populations such as this, with the greatest need, is a key strategy towards reducing health inequity in England. The health needs of families in East London serve as a case study, illustrating a major international challenge and highlighting the need for scalable health-promotion models that can be adapted for diverse, high-risk communities.
Intervening early is needed given risk trajectories for CVD are established in childhood (Allen et al., 2020). UK public health interventions, such as the NHS Health Check, which do not target adults until around the age of 40 are often too late as adverse lifestyle patterns are already fixed, and early cardiovascular damage may already be present (Jacobs et al., 2022). A strong rationale therefore exists to shift preventive efforts into the primary school years and shape health behaviours before they become entrenched. Furthermore, primary schools offer a unique opportunity for increasing impact, as children can also act as ‘health ambassadors’, carrying messages about diet and exercise home to their families and thereby influencing the behaviour of the wider community (Sarkhani et al., 2021). Importantly, there is primary and secondary research on the impact of complex interventions to promote better health in schools (Dabravolskaj et al., 2020; Shackleton et al., 2016). However, less is known generally about targeting primary-school-age children with health promotion, rather than their older peers, and very little specifically is known about CVD interventions with primary school children. This study directly addressed this gap.
Study aims
Our aim in this study was to advance the evidence base on what is known about the optimal design and delivery of cardiovascular health promotion with children at primary school (ages ⩽ 11 years). Delivering school-based health education programmes is an established tool within public health. However, it remains uncertain how such education should be best delivered and by whom. There is increasing emphasis within the NHS on maintaining wellbeing, promoting prevention, and encouraging NHS Trusts to become anchor institutions for their local populations. A wealth of expertise in preventing the disease, both clinical and academic, resides within our hospitals and universities, yet it remains untapped for public health promotion. Whether health promotion in primary schools has a greater impact if delivered by experts in health remains to be understood.
This systematic mapping and review of reviews was conducted to directly inform real-world interventions such as the East London Cardiovascular Disease Prevention (ELoPE) programme, a community-based initiative in which healthcare professionals from a local NHS Trust deliver a standardised heart health education offering in primary schools. Using an in-depth systematic mapping, we established a robust evidence-based and conceptually informed framework for better understanding the components of effective school-based CVD health prevention, particularly through the ‘interdisciplinary lens’ of behaviour change theory and child-centred inquiry-based learning (Greenwood et al., 2020). Our work addressed the following research questions:
What is the nature and extent of the literature on school-based CVD and CVD-risk-related health-promotion programmes?
Are school-based CVD and CVD-risk-related health-promotion programmes delivered in primary schools effective in improving intended outcomes?
What are the key features of effective CVD and CVD-risk-related health-promotion programmes delivered in primary schools?
What are the gaps in the evidence base and priorities for new evidence synthesis and primary research?
The findings of systematic mapping and review of reviews shaped new thinking and conceptualisation in the delivery of the ELoPE programme to address the systemic issue of heart disease in later life.
Methods
Systematic mapping is a form of evidence synthesis that involves a methodical and structured process of categorising and analysing existing literature or evidence on a specific topic area to gain an overview of the key issues, trends, and debates in order to inform future research priorities, policy, and/or practice (Wolffe et al., 2020). In this study, we conducted a systematic mapping and review of reviews to identify and analyse the evidence on school-based CVD and CVD-risk-related health-promotion programmes. As indicated earlier, the impetus for our study was the ELoPE programme, a school-based intervention programme in England, hosted in The Barts Heart Centre (BHC) at Barts Health NHS Trust, the largest heart centre in the country serving the heart attack treatment needs of over 6 million people, and the first of its kind in the NHS. A core component of the ELoPE programme is to directly engage with children and schools, public health bodies, and local authorities to deliver robust heart health education by healthcare professionals, in order to improve health literacy, promote healthy behaviours early, and stem the epidemic of heart disease in later life. The intervention we developed was aimed at year groups 5 and 6 (9–11 years old) to align with the key stage 2 (KS2) and KS3 science programme in the National Curriculum in England on healthy living and bodies. This allowed meaningful coordinated engagement and an opportunity for children to better understand and make positive lifestyle choices, based on scientific and medical evidence about the heart and preventing heart disease. Early roll out of the programme in 2019 that engaged over 40 local primary schools showed evidence of promise that such an intervention was both feasible and acceptable. However, while the ELoPE programme was based on clinical knowledge of CVD, it was less focused on behaviour change. The rationale for the systematic mapping and review of reviews reported in this paper was to identify and analyse the evidence on school-based health-promotion studies to determine key factors and mechanisms of action to help refine a more effective behaviour-change intervention.
Search strategy
We conducted a comprehensive search focused on two key search terms: (1) school-based and (2) terms related to the intervention programme including cardiovascular, heart health, and nutrition. Synonyms for each of these terms were used to search titles, abstracts, and keywords, using both free-text terms and controlled vocabulary (e.g. MeSH terms such as ‘Cardiovascular Diseases’, ‘Health Promotion’, and ‘Schools’). We searched key bibliographic databases including Medline, CINAHL, and ERIC to identify existing review-level evidence on the programme characteristics and implementation of public health interventions delivered to primary school children in high-income country settings. The search strategy was developed in PubMed and translated for use across other databases. The database searches were not limited by date or study design. The approach was supplemented with hand searching of relevant sources (e.g. Cochrane Library, Google, and Google Scholar) and reference list checking of included systematic reviews.
Eligibility criteria
Papers were eligible for inclusion if they were systematic reviews synthesising evidence on the impact and/or implementation of school-based CVD or CVD-risk-related health-promotion interventions. ‘CVD-risk-related’ interventions were defined as those targeting modifiable behavioural and cardiometabolic risk factors established in childhood that are associated with CVD in adulthood, including diet, physical activity, and obesity. Reviews included in the systematic mapping focused on primary or secondary school settings in high-income countries; we excluded non-English, non-school-based, or non-systematic reviews. For the in-depth review of reviews, we included papers that were focused on interventions delivered in primary school settings only and either (1) included a quantitative meta-analysis of intervention effects or (2) explicitly examined programme design or delivery features relevant to the impact of interventions.
Ultimately, our aim was to describe and identify the key characteristics of successful public health programmes and interventions to inform the refinement of our intervention, including the logic model and theory of change.
Screening
Papers were screened initially by title and abstract and then on full report. To ensure a quality appraisal, at each stage of the review process, reviewers independently screened papers in pairs, only moving to screening by a single reviewer after a 90% agreement rate had been achieved.
Data extraction and critical appraisal
Informed by previous meta-reviews conducted by the EPPI-Centre (Sutcliffe et al., 2012), a tool was devised to extract information on the aims, intervention details and findings of included reviews. Reviewers extracted review authors findings as reported, in the form of numerical and narrative summary statements. Summary statements were captured for all outcomes and any sub-group analysis. Risk of bias of was assessed independently using the AMSTAR-2 tool (Shea et al., 2007). Data extraction and critical appraisal was conducted independently by two reviewers (KD and SP), who met to compare their work. Any discrepancies between the reviewers were resolved through discussion and consensus.
Systematic mapping
Prior to our narrative synthesis, a systematic mapping was undertaken to describe the breadth, focus, and characteristics of the existing systematic review literature on school-based CVD and CVD-risk-related health-promotion interventions. The mapping stage involved descriptively categorising reviews by intervention focus, school setting, outcomes measured, and type of synthesis conducted. The map developed through this process was used to identify a relevant subset of reviews for inclusion in the subsequent in-depth review of reviews.
Data synthesis
A narrative synthesis was prepared detailing the direction of effects across reviews. Although we considered statistical difference, effect size was our primary consideration when interpreting and synthesising results as studies not reaching statistical significance may have been insufficiently powered to detect a small but operationally significant effect. Results were presented at the level of the included systematic reviews, drawing on the outcomes and effect estimates as reported in each review. In addition, we reported the review authors’ analyses and conclusions regarding the programme components associated with successful intervention outcomes, as described in the included systematic reviews.
Evidence was then categorised as follows: (1) evidence of positive impact, when the direction of positive effect was statistically significant; (2) no evidence of difference, when it was not possible to detect statistically significant differences in the direction of effect between those receiving interventions and those in control or comparison groups for particular outcomes; (3) evidence of harm, when the direction of effect was negative, statistically or non-statistically; (4) inconsistent evidence, when there were conflicting findings among studies; and (5) insufficient evidence, findings were based on a single study or on two studies of poor quality. The final synthesis involved bringing together evidence across multiple reviews for each intervention form and outcome combinations.
Ethical approval
Ethical approval for this study was received from the University College London (UCL) Institute of Education research ethics committee (REC 1594).
Results
Search results
A total of 6,078 papers were screened on title and abstracts after duplicate removal. We obtained and re-screened full-text reports of 292 citations and excluded a further 118 reports at this stage. From this process, 141 systematic reviews were included in the map. We then applied a criteria-based framework to identify relevant reviews to answer our review of review questions, which reduced the pool of relevant systematic reviews to 12 items. Figure 1 outlines the review flow process.

Flow of studies through the systematic review.
Systematic map: overview of reviews
The systematic mapping of the nature and scope of systematic review literature on school-based CVD and CVD-risk-related health-promotion programmes which we developed provided valuable insights into the field. Between 1988 and 2024, there was a gradual increase in reviews published on school-based health promotion for CVD prevention, with the most significant growth occurring between 2012 and 2016, accounting for 42% (n = 59) of the reviews included in the initial map. The reviews predominantly focused on obesity, diet, and physical inactivity. Of the 141 reviews, 77 focused on obesity; 61 investigated nutrition and healthy eating; and 46 addressed physical inactivity and sedentary behaviour. Only 15 solely focused on delivering lessons on CVD prevention.
The majority of programmes and interventions described in the reviews targeted both primary and secondary school children (n = 86), while 31 reviews focused solely on primary schools and 24 secondary schools. Outcomes measured included changes in health behaviour, knowledge, and attitudes, often alongside anthropometric metrics like body mass index (BMI). In terms of methods, narrative reviews were the most common (n = 82), followed by meta-analyses (n = 55). A small number of reviews used qualitative, scoping, realist, or framework synthesis. Notably, 68% (n = 96) of the reviews included critical appraisal of their included studies, whereby they used validated tools to assess methodological rigour and make judgements on study validity, relevance, and applicability.
Review of reviews
Twelve reviews were identified from the systematic mapping to answer our questions about the impact of school-based CVD and CVD-risk-related health-promotion programmes delivered in primary schools and the key characteristics of successful programmes.
Key characteristics of included reviews
The geographical spread of the 12 reviews spanned all major continents, with the majority of their included studies coming from high-income countries. Although there was some slight variation in the age of children across reviews, the majority fell within the 5- to 11-year-old age range. The size of the evidence base varied considerably. This was largely due to the scope of the individual review aims. For example, where reviews did not apply study design filters or were broad on intervention types and outcomes, this increased the number of studies included. The majority of reviews synthesised evidence from randomised and non-randomised controlled trials to enable a synthesis of the impact of programme using statistical meta-analysis. Reviews also investigated which programme design and delivery features led to greater outcomes effects. This was often achieved by conducting a sub-group analysis or by narratively exploring trends in outcome data according to different types of programme components. The key characteristics of the included systematic reviews are provided in online Supplementary Table A.
Quality of the reviews
All the reviews were critically appraised using the AMSTAR 2 tool. When exploring the risk of bias within individual domains, our analysis revealed five domains consistently demonstrated a low risk of bias. Specifically, all reviews reported an explicit aim or research question alongside clear inclusion criteria; provided a rationale for the eligibility criteria of study designs; employed a comprehensive search strategy; described the included studies in detail; and disclosed conflicts of interest. However, an unclear or moderate risk of bias was identified in five domains where reporting was less consistent. For example, methods of duplicate study selection were reported in only five reviews, while duplicate data-extraction methods were outlined in four. Six reviews provided references when reporting their reasons for excluding studies, and four conducted a risk-of-bias assessment for included randomised trials. For non-randomised studies, this type of assessment was undertaken in only six reviews. In addition, six reviews failed to adequately reflect on the quality of the evidence base when interpreting their findings. High risk of bias was identified in just one domain, as the majority of reviews (n = 10) did not refer to an existing protocol. Of the 11 systematic reviews that used meta-analyses to assess intervention effects, all were carried out appropriately. Nine of these reviews assessed the potential impact of quality ratings to explore variation in their findings, while five further reviews explored sources of heterogeneity and publication bias. Table 1 provides an overview of the quality appraisal.
Quality appraisal of reviews.
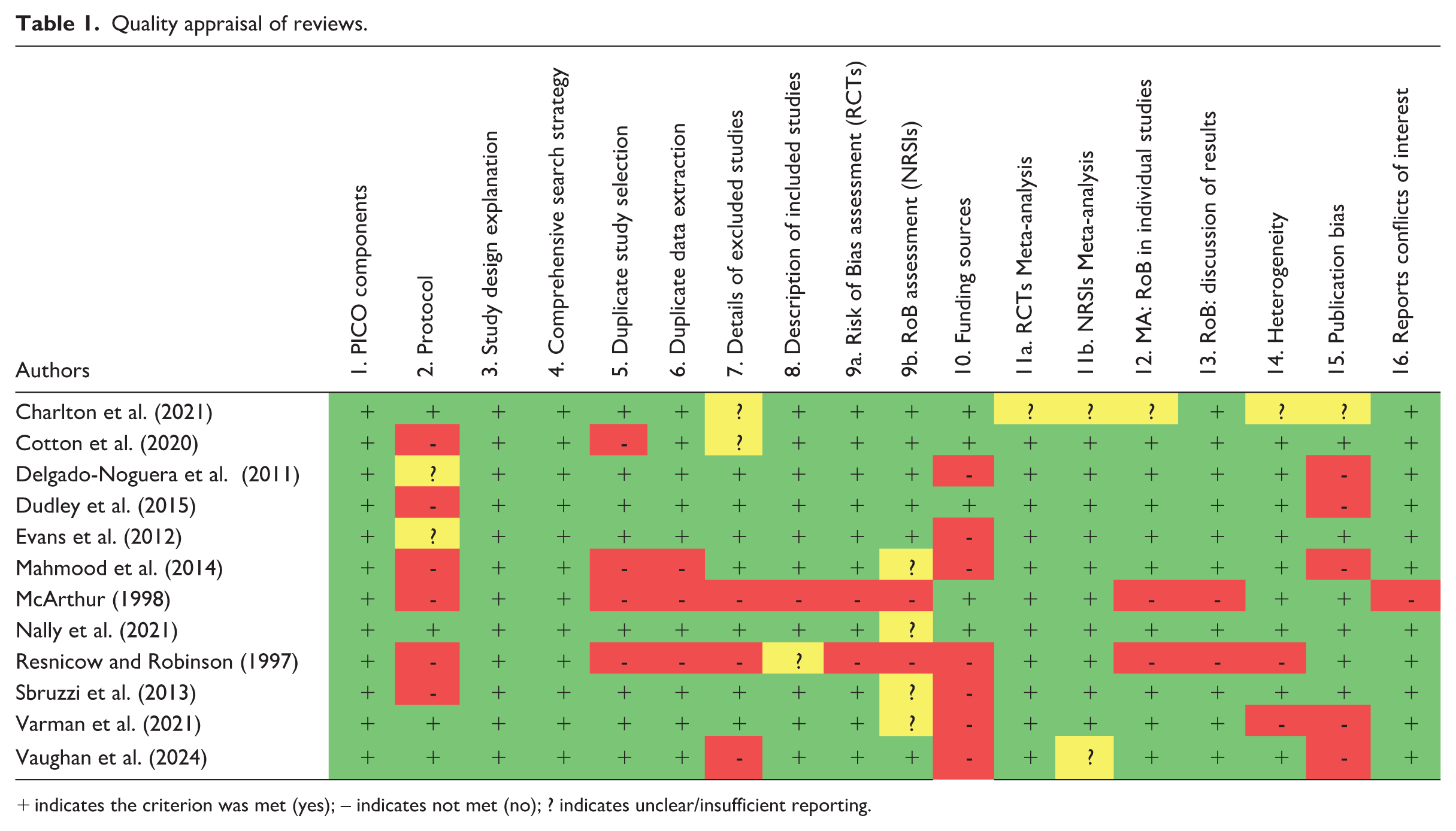
indicates the criterion was met (yes); – indicates not met (no); ? indicates unclear/insufficient reporting.
Evidence of impact
The findings showed promising evidence of impact of positive associations between CVD school-based health-promotion programmes and longer-term health behaviour and nutrition outcomes.
Cardiovascular programmes (n = 2)
Two reviews in the late 1990s found that school-based cardiovascular health-promotion programmes could positively impact primary school children’s CVD risk factors. McArthur’s (1998) meta-analysis showed a small but significant effect on healthy eating behaviours. The composite effect score of behaviours included the percentage of ‘heart health foods’ (not specified) and saturated fat in children’s food and their fruit and vegetable intake. In the review by Resnicow and Robinson (1997), the most significant positive effects were observed for reducing risk factors for CVD, through smoking-prevention initiatives, cognitive processing (e.g. improvements in knowledge, awareness, attitudes, and decision-making skills related to cardiovascular health), and physical activity and fitness (36%). In contrast, lower rates of change were noted between the intervention and comparison groups for blood pressure and adiposity measures.
Nutritional educational programmes (n = 7)
Seven reviews published between 2011 and 2024 examined the effects of nutrition-focused programmes on primary school children, focusing on changes in nutritional knowledge, cooking self-efficacy, and consumption. Three reviews (Cotton et al., 2020; Dudley et al., 2015; Varman et al., 2021) investigated the outcomes and effects of primary-school nutrition education programmes on enhancing children’s nutritional knowledge. The reviews highlighted the positive impact of enhanced curricula and experiential learning strategies, with a particular emphasis on the latter, which demonstrated a larger effect size on dietary knowledge. Dudley et al. (2015) synthesised studies measuring nutritional knowledge gains, revealing that both enhanced curricula and experiential learning significantly improve nutritional knowledge, primarily grounded in behavioural and social cognitive theories. Varman et al. (2021) corroborated these findings, noting substantial positive effects of experiential learning activities on children’s understanding of healthy eating. Cotton et al. (2020) expanded the scope by examining the combined effects of various teaching methods, including board games, and found that students exposed to nutrition education interventions scored higher on knowledge assessments than those without such interventions.
Six reviews measured changes in fruit and/or vegetable intake. Cotton et al. (2020) found an increase in intake when comparing children exposed to various learning approaches, ranging from the use of board games to the provision of fruits and vegetables in school canteen, to those in the control group. Dudley et al. (2015) found that experiential-learning approaches had the largest effect size, followed by cross-curricular approaches, curriculum-based approaches with contingent reinforcement (i.e. rewards for behaviour) approaches, and finally parental involvement. Evans et al. (2012) found that interventions focused on fruit and vegetables could improve fruit and vegetable daily intake by 0.25 portions without the inclusion of fruit juice, or by 0.32 portions if fruit juice is included. They found that improvements were largely based on increases in fruit, not vegetable, consumption
Delgado-Noguera et al. (2011) found that computer-based interventions could be successful in increasing fruit and vegetable intake. Conversely, they found no evidence of significant difference in the impact of free subsidised fruit and vegetables or multicomponent interventions on fruit and vegetable consumption. In their review, Varman et al. (2021) synthesised evidence on food-related behaviour change, with a specific emphasis on the effects of experiential learning activities on fruit and vegetable consumption. The meta-analysis revealed significant mean effect sizes in two out of five studies that involved parental participation, leading to increased healthy food intake. The remaining three studies showed medium effect sizes, with one successfully enhancing fruit and vegetable consumption through school gardening, taste-testing, and nutrition education, while the other two reduced unhealthy food consumption through various experiential activities. Similarly, Vaughan et al. (2024) conducted a meta-analysis of studies examining cooking interventions and their impact on children’s vegetable consumption, with a smaller positive effect.
Obesity-focused programmes (n = 3)
The outcomes and effects of obesity programmes targeting children under 12 years were documented in three reviews published between 2014 and 2021. A meta-analysis of two trials conducted by Mahmood et al. (2014) indicated that school-based obesity interventions were successful in reducing obesity prevalence among primary school children. Similarly, Sbruzzi et al. (2013) found evidence of positive effects of educational interventions in the treatment of obesity. On the basis of a meta-analysis of 26 randomised control trails, their findings suggest that education interventions could be associated with a significant reduction in waist circumference, BMI, and diastolic blood pressure. However, the impact of educational interventions in preventing childhood obesity in comparison to routine school curriculum or no intervention was yet to be demonstrated according to this study. Findings of Nally et al. (2021) (n = 37 Randomised Controlled Trials [RCTs] ) indicate that education interventions led to a small statistically significant reduction in BMI z-score but no meaningful decrease in BMI kg/m2. Inconclusive results were also reported for sedentary behaviour, energy intake, and fruit and vegetable intake.
Key features of successful programmes
Further analysis conducted by reviews provided aggregate data on the key features of successful programmes. The literature reviewed indicates that successful programmes are typically multi-component, combining nutrition education with experiential, hands-on learning approaches. Programmes that utilise various methods to engage students showed larger effect sizes than single-component interventions, particularly in improving fruit and vegetable consumption and BMI. Curriculum-based approaches, such as dedicated lessons on healthy eating integrated into existing subjects have demonstrated improvements in knowledge and health behaviours. In contrast, less successful programmes tended to rely on traditional, didactic teaching approaches with limited student engagement. However, it is difficult to isolate from the evidence whether taking a curriculum-based approach alone is the contributing factor to their impact.
Experiential learning, a feature in nutrition-focused programme only, showed statistically significant larger effect sizes when measuring the impact of nutritional knowledge on sugar, energy, and fruit and vegetable intake. Programmes combining nutrition education with hands-on learning were also more beneficial. Differences in programme providers and the extent to which this mediated their overall effect was not routinely investigated, with only one review finding modest effects impacts on children’s nutritional knowledge and behaviour. Although the majority of reviews described the length and frequency of programmes, assessment of programme intensity on outcomes was only explored in one review. This appears largely in part due to heterogeneity, with reviews including studies of programmes lasting 6 weeks to 6 years, as outlined in online Supplementary Table B. Overall, the evidence indicated that the delivery method and intensity of CVD prevention and health-promotion programmes may play a positive role in influencing health knowledge and behaviours, but how they achieve this goal is not yet well understood.
Discussion
Our systematic mapping and review of reviews provides novel insights into the impact of CVD-risk-related school-based health-promotion programmes for primary-school-age children, a critical but often neglected younger demographic for prevention health evaluations. It moves beyond simply asking if interventions were successful, to identify the key characteristics of programmes that improved CVD-risk-related outcomes such as behaviours and knowledge relevant to CVD prevention. Overall, the evidence indicates that school-based health-promotion programmes can successfully improve a wide range of CVD-risk-related metrics, from accumulation of knowledge to reduction in children’s BMI. Successful programmes were those that (1) included experiential learning activities, particularly those providing opportunities to taste and grow food; (2) adopted curriculum-based approaches; and (3) worked with a multi-component approach, potentially combining experiential learning and cross-curricula intervention.
Health-promotion programmes that adopted an experiential and child-centred approach tended to have a more lasting impact on children’s knowledge and behaviours. By encouraging students to take an active role in their learning, through hands-on activities such as taste-testing or school gardening, these programmes fostered greater engagement and personal investment. The evidence from our review shows that when children take the lead in their learning with guidance from teachers and health experts, they develop a deeper understanding of health concepts and are more likely to make longer-term behavioural changes. This approach positions children as active learners rather than passive recipients, which helps reinforce healthy habits. Adult scaffolding, through partnerships between educators and health professionals, has a critical role to play in this process, providing the necessary structure and support for students to make informed decisions while fostering autonomy in shaping their own health actions and behaviours.
While the included reviews demonstrate that school-based cardiovascular health-promotion programmes can have a positive impact, their findings often rely on small-scale experimental evaluations (measuring efficacy) that may not reflect the complexities of real-world implementation (effectiveness). Large-scale evaluations can help validate these findings, assess scalability, and explore systemic factors such as policy environments, resource allocation, and school capacity that influence the success and sustainability of interventions. The evidence-base points to a key limitation in existing research being the dearth of information on the optimal duration of programmes and interventions and the medium- to longer-term follow-up of their effects. Our synthesis showed while most reviews described the length of programmes, ranging from 6 weeks to 6 years, very few formally assessed the impact of this duration on outcomes. One review did find that obesity-focused interventions lasting at least 6 months were more likely to show a positive impact. However, none of the reviews provided evidence as to whether knowledge or behavioural changes were sustained as children transitioned to secondary school, underscoring a critical gap for future research.
A further limitation of the evidence base was that the small number of systematic reviews that focused explicitly on CVD prevention in primary school settings were published in the late 1990s. Although these reviews remain important sources synthesising evidence on CVD-specific school-based interventions for this age group, the age of the evidence means findings should be interpreted cautiously, particularly given changes in educational processes and contexts, intervention design, and changing public health priorities over time. Nevertheless, their inclusion was necessary to reflect the full extent of the available review-level evidence in this area.
The included reviews used robust methods to assess the impact of interventions and identify key characteristics of successful programme outcomes. Even when evidence shows that health behaviour change, for example, increased fruit and vegetable consumption after an experiential learning component, the underlying theory of change, or the mechanisms by which these interventions succeed, is often unclear. Thus, understanding how specific programme elements interact to drive change is critical, not only for replicating success but also for fine-tuning and tailoring interventions to new situations. Research into these causal processes could aid in the development of more targeted, effective interventions, allowing for greater scalability while maintaining impact. This would also help to shape broader CVD-prevention strategies, ensuring their relevance and long-term viability across a variety of educational settings.
Although school-based health-promotion programmes have the potential to improve children’s knowledge and behaviours, their success depends on school-level factors. Implementing programmes requires not only resources for materials, training, and curriculum integration but also ongoing support to sustain their impact over time (Herlitz et al., 2020; Meshkovska et al., 2022). To fully realise the benefits of health-promotion efforts, schools must evaluate their capacity to implement such programmes sustainably, potentially seeking external support or funding to bridge resource gaps. This approach can help ensure that all children benefit equitably, supporting long-term health behaviour change.
Implications for future work
The evidence from this review provides clear guidance for the design of the ELoPE programme. The evidence has highlighted how and why some school-based CVD health programme interventions work, not just whether they work. It has reinforced the importance of prioritising activities that actively engage with children, such as food tasting, cooking, and gardening, essentially activities embedded within the school curriculum to support and sustain health-related behaviours. It also underscores the importance of designing programmes that take into account scalability and sustainability, as well as structural factors such as school capacity and resources to ensure interventions move beyond small-scale implementation. To inform the iterative refinement of the ELoPE programme, our recommendation is to take a multi-component approach that integrates experiential activities with cross-curricular teaching and appropriate adult scaffolding to strengthen children’s knowledge of CVD, as well as health-related behaviours. Our study findings also highlight the importance of taking an integrated multidisciplinary approach that fosters deep collaboration between health and education experts in the co-delivery of a genuinely holistic school-based health-intervention programme.
It is crucial to acknowledge that the impact of school-based programmes is shaped by wider external factors, as children’s health behaviours are heavily influenced by their home and community environments. Indeed, the broader evidence base recognises that socioeconomic factors such as poverty and inequality are foundational drivers of CVD risk. While our review of reviews did not find data that systematically measured the impact of these interventions on the family unit or health equity, it revealed that the more successful programmes actively attempt to bridge the gap between school and home. For instance, reviews found that nutrition programmes incorporating direct parental involvement yielded significantly larger positive effects on children’s healthy eating behaviours. Mechanisms for this engagement included family-based support, home-based projects, and parent newsletters. Nevertheless, how these interventions overcome entrenched socioeconomic barriers and their differential impact across diverse family contexts remains poorly understood, making this a critical area for future research and evidence reviews.
A key recommendation from our findings is for policymakers to develop formal frameworks to facilitate closer collaboration between national education and health bodies, such as the Department for Education (DfE) and the NHS in England. The ELoPE programme we are continuing to develop provides one such local model. By establishing a partnership where local NHS expertise is delivered directly within schools and in partnership between clinicians, teachers, and educational professionals, the programme offers the potential for a scalable example of how governments can make a generational investment in tackling the roots of health inequality long before they manifest as adult disease.
Conclusion
School-based health-promotion interventions, particularly at primary school level, have the potential to reduce CVD risk in later life by supporting the adoption of healthy behaviours from an early age. Results from the meta-analysis provide evidence of the impact of multi-component approaches that integrate curriculum-based learning and experiential activities. However, the success of these programmes depends on investment in resources and tailoring interventions. Collaboration between educators, healthcare professionals, and policymakers is critical to support knowledge, funding, and implementation. By developing multidisciplinary partnerships and prioritising prevention from an early age, school-based interventions can play a pivotal role in tackling CVD and promoting health equity in the long term.
Supplemental Material
sj-docx-1-hej-10.1177_00178969261439552 – Supplemental material for Cardiovascular health promotion through primary schools: A systematic mapping and review of reviews
Supplemental material, sj-docx-1-hej-10.1177_00178969261439552 for Cardiovascular health promotion through primary schools: A systematic mapping and review of reviews by Lynn Ang, Kelly Dickson, Selam Petros, Charlotte Ives, Samantha Cliffe, Mohammed Khanji and Riyaz Patel in Health Education Journal
Footnotes
Acknowledgements
We acknowledge the support of all participants and participating schools for their invaluable contributions to the East London Cardiovascular Disease Prevention (ELoPE) programme. We also extend our gratitude to our respective institutions for enabling and supporting this research.
Authors’ Note
Mohammed Khanji is also affiliated with William Harvey Research Institute, Queen Mary University of London, London, UK.
Riyaz Patel is also affiliated with the Barts Heart Centre, Barts Health NHS Trust, London, UK.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UCL Health of the Public Small Grants Scheme. The funder had no role in the design, conduct, analysis, interpretation, or writing of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article as no new datasets were generated. Data extracted from the included reviews may be made available by the corresponding author upon reasonable request.
AI declaration
The authors declare that no assistive or generative artificial intelligence tools were used at any stage of the manuscript’s production.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.