
Abstract
Background:
This discussion paper addresses the health education implications of the enduring ‘monogamy-superiority’ myth – in the form of the assumption that monogamous relationships are inherently healthier, more stable or more fulfilling than consensually non-monogamous (CNM) arrangements.
Summary of Evidence:
Drawing on recent evidence, we highlight how relationships and sexual satisfaction do not differ significantly between relationship structures. Despite this, individuals in CNM relationships often encounter stigma, discrimination and structural barriers, which can negatively influence their well-being and deter open communication in healthcare and educational settings.
Implications:
For health educators and practitioners, these findings highlight the importance of inclusive, evidence-informed approaches that acknowledge relationship diversity as a legitimate and healthy variation of human intimacy. We outline key implications for practice, including challenging the personal and institutional biases that privilege monogamy; fostering safe environments that encourage open disclosure; integrating accurate information about consensual non-monogamy into health education and professional training; and advocating for structural changes that better accommodate diverse relationship configurations.
Conclusion:
Shifting the focus from relationship structure to the quality of communication, consent and mutual respect within relationships will allow health education to play a role in dismantling stigma and supporting more equitable and person-centred care. Embedding these perspectives into curricula, community programmes and clinical practice not only improves the experiences of people in CNM relationships but also strengthens health systems’ capacity to deliver responsive, culturally competent care.
Monogamy – the practice of having a single, exclusive romantic and sexual partner – has long been the dominant norm for intimate relationships in Western societies (Fairbrother et al., 2019; Scoats and Campbell, 2022). Popular culture and societal stereotypes often portray monogamous relationships as the gold standard for happiness, stability and even morality (Conley et al., 2013b). In contrast, people who engage in consensual forms of non-monogamy are frequently stigmatised, misunderstood or seen as deviating from what is ‘normal’ (Moors et al., 2013).
This entrenched privileging of monogamy, often referred to as the monogamy-superiority myth (Anderson et al., 2026), goes beyond related concepts such as mononormativity or monogamism, which describe the social dominance or structural privileging of monogamy. The monogamy-superiority myth instead refers to the belief that monogamous relationships are inherently happier, healthier or more moral than other relationship forms. These beliefs are reinforced by religious teachings, cultural narratives and legal structures that exclusively recognise dyadic partnerships (Anderson et al., 2025; Conley et al., 2013a). Health and mental health educators and professionals may unwittingly carry these same assumptions into their practice, either knowingly or not, affecting how they understand and counsel clients, students and patients about relationship issues (Vaughan et al., 2019; Woodbridge, 2022).
Recent research challenges these assumptions. Studies increasingly demonstrate that consensually non-monogamous (CNM) relationships, including open relationships, polyamory and swinging, can offer the same levels of emotional and sexual fulfilment as monogamous partnerships (Hamilton et al., 2021). Meta-analytic evidence shows no inherent advantage of monogamy in terms of relationship or sexual satisfaction (Anderson et al., 2026). Despite this, people in CNM relationships often face stigma, social disapproval and systemic barriers, from difficulty disclosing their relationship status to concerns about discrimination in healthcare, workplaces and legal systems (Anderson et al., 2025; Valadez et al., 2020).
This paper reviews the evidence debunking the monogamy-superiority myth, explores the stigma and structural challenges faced by CNM individuals and considers the implications for health education and healthcare practice. By translating current evidence into practical recommendations, this paper seeks to support educators and health professionals to deliver more inclusive, evidence-informed care and education that recognises relationship diversity as a healthy and legitimate variation of human intimacy.
Consensual non-monogamy: forms and prevalence
CNM is an umbrella term describing relationship structures in which all partners consent to or come to an agreement under which partners can pursue multiple sexual and/or romantic relationships simultaneously (Hamilton et al., 2021; Scoats and Campbell, 2022). Unlike infidelity, CNM relationships are defined by transparency and agreement – everyone involved knows about and agrees to the arrangement. CNM may reflect a relationship structure, a sexual practice within relationships or even a broader identity, orientation or preference that shapes how individuals approach dating and intimacy (Gupta et al., 2024). Importantly, an individual’s identification as CNM does not always align with their current relational configuration – for example, someone may identify as non-monogamous while being single or in a monogamous partnership which can generate confusion, uncertainty or relational tension. Such experiences – including erasure, ambiguity or misalignment between identity and relationship form – may contribute to a range of negative outcomes, including shame, self-doubt and reduced authenticity, echoing similar effects observed among Bi+ populations 1 whose identities are often invalidated or misrecognised (McCole and Anderson, 2025). Moreover, orientations towards non-monogamy can shift over time and context, reflecting the dynamic nature of relational desires and practices (Cardoso et al., 2021; Rubel and Burleigh, 2020). Consensually non-monogamous relationships exist in a variety of forms with distinct norms and expectations, which may overlap and be enacted differently across relationships (Cohen, 2016). Some common examples are shown in Table 1.
Some common forms of CNM relationships.
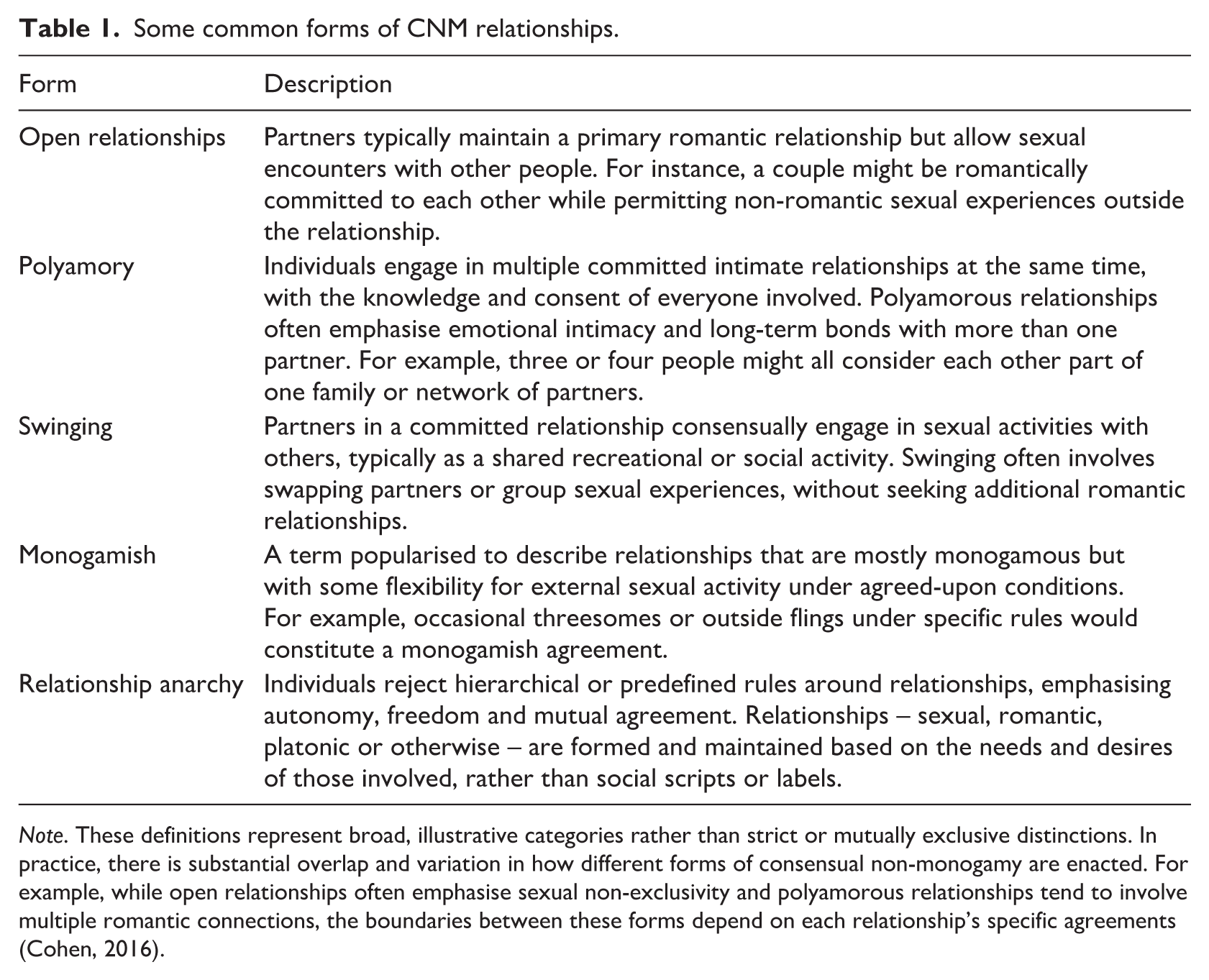
Note. These definitions represent broad, illustrative categories rather than strict or mutually exclusive distinctions. In practice, there is substantial overlap and variation in how different forms of consensual non-monogamy are enacted. For example, while open relationships often emphasise sexual non-exclusivity and polyamorous relationships tend to involve multiple romantic connections, the boundaries between these forms depend on each relationship’s specific agreements (Cohen, 2016).
Contrary to the belief that CNM is rare, research shows it is a significant minority practice. Frequently cited statistics reveals that about 5% of adults in the USA are currently in some form of a CNM relationship (Rubin et al., 2014; Scoats and Campbell, 2022). In addition, roughly one in five single people in the USA (around 20%) have engaged in or practised CNM at some point in their lives (Gupta et al., 2024). Around 12% report that a CNM relationship represents their ideal relationship configuration (Haupert et al., 2017). These figures may even underestimate prevalence, as stigma and fear of judgement likely lead to underreporting. Nonetheless, this suggests that millions of people have some experience with CNM relationship arrangements (Conley et al., 2013a).
Prevalence can also vary among community subgroups. Notably, CNM appears to be more common in some lesbian, gay, bisexual, trans and gender diverse, intersex, queer and asexual (LGBTIQA+) communities. For example, surveys have found that around one-third of gay men report being in open relationships (Levine et al., 2018: see Figure 1). This may reflect historical and cultural factors, such as more flexible norms regarding sexual exclusivity within these communities (Hosking, 2013, 2014). Of note, having a marginalised sexual or gender identities in addition to being CNM may result in overlapping forms of stigma which can increase vulnerability to psychological and physiological health risks (Rubin-McGregor et al., 2025).
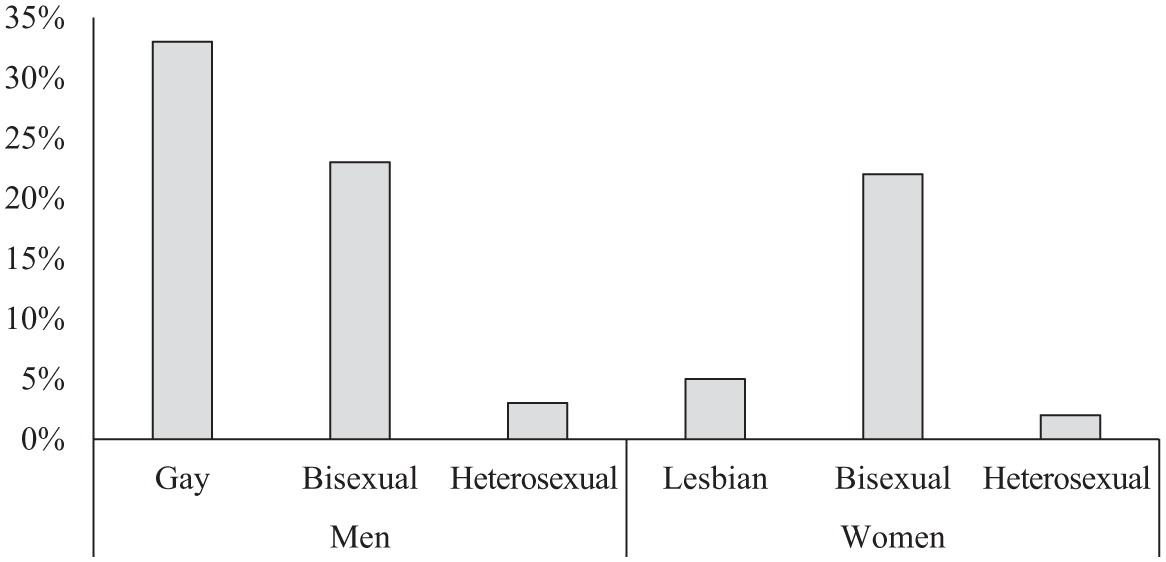
Rates of open relationships as a function of sexual identity from the US 2012 survey of sexual health and behaviour.
However, large-scale studies suggest that, beyond sexual orientation, there are no known significant demographic differences between individuals who practise CNM and those who do not (e.g. age, education, income, race, religion or political affiliation; Haupert et al., 2017). Across age, culture and identity, people practicing CNM represent a diverse population – ranging from young singles exploring dating, to married couples with occasional external partners, to polyamorous families raising children. Given this diversity and prevalence, CNM is an ongoing and increasingly relevant consideration for health educators and practitioners who aim to provide inclusive, evidence-informed care and education.
The ‘monogamy-superiority’ myth and public perceptions
Despite increasing visibility of diverse relationship models, public attitudes towards CNM remain largely negative. Mononormativity – the assumption that monogamy is the default and superior form of intimacy – continues to shape how CNM is perceived (Sandbakken et al., 2022). Monogamous relationships are frequently seen as more loving, trustworthy, committed and stable, while CNM arrangements are often dismissed as risky, unstable or purely sexual (e.g. Balzarini et al., 2019; Hinton et al., 2019; Murphy et al., 2021). Research consistently shows the strength of these biases. In experimental studies, participants rated individuals in monogamous relationships more positively across dimensions such as stability, morality and social acceptability, a pattern often described as the ‘monogamous halo effect’ (Balzarini et al., 2018; Conley et al., 2019). These perceptions are reinforced by deep-rooted social and cultural narratives.
Media representations further entrench these views. Popular films, television and literature frequently idealise monogamous romance while portraying CNM relationships as unstable, unethical or doomed. Positive representations are rare, which perpetuates the idea that anything outside one-to-one coupling is inherently problematic (Conley et al., 2013a; Moors et al., 2017). These stereotypes also contribute to the misconception that CNM is inherently unsafe – ignoring evidence that, when practised ethically and with good communication, CNM relationships can be just as emotionally fulfilling and health-conscious as monogamous ones (Conley et al., 2015; Füllgrabe and Smith, 2023; Gupta et al., 2024). Moreover, the evidence shows that people in CNM relationships are more likely to communicate about sexual health than their monogamous counterparts (Lehmiller, 2015).
It is important to note that legal and institutional structures also favour monogamy, contributing to the sense of its superiority. Marriage, child-rearing and family law in almost all countries legally recognise only two adults in a conjugal partnership. 2 Multi-partner relationships typically have no legal recognition – for instance, one cannot legally marry or register more than one partner, and typically only two co-parents can have recognised custody or parental rights for a child (Morrison et al., 2013). This means polyamorous families must often ‘work around’ laws (e.g. using contracts or co-parenting agreements) and sometimes lie about their arrangements to fit within legal parameters.
Health insurance policies, inheritance laws, hospital visitation rights and other benefits are also usually structured around monogamous dyads (Anderson et al., 2025). Consequently, people in CNM relationships may be forced to hide their status on official forms, or else forfeit rights (e.g. a third partner not being recognised as a next-of-kin in a medical emergency). These structural inequalities send a message that CNM relationships are inherently less legitimate. They also deter individuals from openly identifying as CNM, since ‘coming out’ can mean loss of legal protections or access to services (Klesse, 2006; McCrosky, 2015; Vaughan et al., 2019). Beyond public perceptions, CNM stigma also shapes sexual-health access and experiences. Recent research documents how CNM clients often face presumptions about risk, discomfort in disclosing relationship arrangements and structural misfit within sexual-health service design (Campbell et al., 2024; Scoats and Campbell, 2025). In short, monogamy’s privileged status in society – socially, legally and institutionally – underpins the myth of its inherent superiority.
For health educators, understanding this context is key. It is imperative to understand that clients or students may have been exposed to forms of direct or vicarious discrimination and marginalisation. 3 Moreover, many of them will have internalised some degree of monogamy-superiority thinking. Educators should recognise that CNM is often widely misunderstood and stigmatised (labelled as ‘cheating’, immoral or purely sexual; Barker and Langdridge, 2010; Hutzler et al., 2016). Debunking misconceptions is part of the task at hand: for example, clarifying that consensual non-monogamy is not the same as infidelity, and that it can be practised respectfully and ethically.
Relationship and sexual satisfaction: debunking the myth
The monogamy-superiority myth rests on the belief that monogamous relationships uniquely foster happiness, commitment and stability, while consensually non-monogamous relationships are assumed to be riskier and less fulfilling, despite a lack of empirical support. Some early studies comparing relationship configurations appeared to show greater satisfaction among monogamous couples, but these effects often disappeared when accounting for factors such as relationship length or the impact of stigma and social stressors on CNM participants (see Conley et al., 2013b: for a critical discussion). Over time, more robust studies have begun to show that CNM relationships can be just as emotionally and sexually fulfilling as monogamous ones (Conley et al., 2018; Parsons et al., 2012; Wood et al., 2018) and also found that individuals in CNM relationships were no less satisfied or committed than monogamous individuals.
We recently conducted a comprehensive meta-analysis of all available studies comparing relationship outcomes in monogamous and CNM relationships (Anderson et al., 2026). This study meta-analysed the data from 35 separate studies across multiple countries (n = 24,489). The findings decisively debunked the monogamy-superiority myth. The meta-analysis found no statistically significant differences between the groups (relationship satisfaction: Hedges’ g = −0.05, 95% CI [−0.20, 0.10], p = .496; sexual satisfaction: Hedges’ g = 0.06, 95% CI [−0.07, 0.18], p = .393). In plain language, both monogamous and CNM individuals are equally satisfied on average in their relationships and in their sex lives.
This research provides the strongest evidence to date that monogamy per se is not a predictor of greater happiness or fulfilment in relationships. The meta-analysis allowed us to conclude that relationships and sex are equally satisfactory for monogamous and CNM individuals. Importantly, this held true across various subgroups and circumstances. For instance, we performed subgroup analyses to test whether certain conditions might change the outcome. For example, we were interested in whether CNM might work well for some demographics but not others. However, the results were consistent across different samples (e.g. LGBTIQA+ vs heterosexual) and relationship types (e.g. open relationships vs polyamorous vs monogamish). Similarly, relationship satisfaction was equivalent between relationship types even when explored at the facet level: trust, commitment, intimacy and passion were approximately equal between those in CNM and monogamous relationships.
Notably, the meta-analysis also highlighted an intriguing point – specifically, that CNM relationships manage to be just as satisfying as monogamous ones, even in the face of significant stigma and societal challenges (Anderson et al., 2026). As indicated above, individuals in CNM relationships often contend with higher levels of discrimination and must navigate complex disclosure issues (Moors et al., 2013; Valadez et al., 2020) – factors which might be expected to harm their relationship or sexual satisfaction. From a minority stress perspective (Borgogna et al., 2024), these stressors can impose additional psychological burdens, yet CNM relationships are comparable in quality to monogamous ones in spite of these stressors (see also Füllgrabe and Smith, 2023). This resilience may reflect adaptive coping strategies, strong community connections and relational skills that help buffer stress. Despite this extra stress, individuals in CNM relationships reported equitable satisfaction to individuals in monogamous relationships, suggesting a strong degree of resilience and positive functioning within CNM relationships (Füllgrabe and Smith, 2023).
It may be that the benefits inherent to CNM relationships counterbalance the external stressors. For instance, CNM people often report experiencing greater diversity of emotional and sexual needs being met, since different partners can fulfil different needs (for instance, one partner might provide intellectual companionship, another adventurous sexual exploration, etc.; see Moors et al., 2017). They also frequently cite personal autonomy and freedom as advantages – the ability to explore connections without the constraint of exclusive monogamy can lead to a sense of empowerment and authenticity in how people experience the intimate and romantic aspects of their lives (Aguilar, 2013). Furthermore, individuals in successful CNM relationships may have better communication and negotiation skills, as their relationship style demands frank discussion of boundaries, jealousy and needs (Moors et al., 2017). These practices can foster deep trust and honesty. The assumption that non-monogamy equates to lack of commitment or low trust is not borne out when one actually studies people’s experiences (Lecuona et al., 2021).
In our previous work, we have argued that infidelity – a common cause of relationship dissatisfaction in monogamous relationship structures – is often substantially reduced or differently configured in CNM relationships (Anderson et al., 2025, 2026). In monogamous relationships, a single act of cheating can be devastating, often leading to violations of trust and even breakups. However, the direction of effects is not always straightforward – relationship strain can precede infidelity, and infidelity can then amplify or expose pre-existing problems. In many cases, it is the secrecy, betrayal of agreed rules or the public ‘discovery’ of the infidelity (rather than the extra-dyadic sex itself) that precipitates crisis. Indeed, infidelity is one of the most commonly cited reasons for divorce or relationship counselling among monogamous couples (Labrecque and Whisman, 2017). By contrast, CNM arrangements aim to make extra-dyadic desires more explicit, negotiated and consensual, with what might otherwise count as ‘infidelity’ being re-defined in advance and open to re-negotiation. This does not imply that there are no conflicts or trust issues in CNM relationships – jealousy can and does still occur, and infidelity can still take place when (i.e. agreements within the relationship can be broken; Hosking, 2013). But because the rules are co-constructed and revisited, ruptures are more often framed as boundary-violations within an agreed CNM structure, rather than as evidence that the relationship itself is invalid, fostering a relationship environment in which transparency and consent are prioritised over secrecy and prior assumptions.
From a health education perspective, these findings are crucial. Rather than simply challenging negative attitudes towards CNM, they highlight a specific risk for health educators and practitioners: namely, the tendency to misattribute relationship difficulties to the relationship structure itself rather than other factors. They call into question the common misconception – among both the public and many professionals – that monogamy is inherently linked to better relationship outcomes. Health practitioners often assume that a client’s relationship difficulties might arise because they are in a non-traditional arrangement and/or that encouraging monogamy will lead to more stability (Anderson et al., 2025; Valadez et al., 2020). The evidence reviewed here suggests that such assumptions reflect a form of structure-based bias rather than an evidence-informed assessment of relationship functioning. Instead, relationship satisfaction appears to be shaped far more by relational processes – such as communication, consent, negotiation and mutual respect – than by whether a relationship is monogamous or consensually non-monogamous. In practice, a monogamous couple rife with poor communication and mismatched expectations may be far less ‘healthy’ than a well-functioning polyamorous family who communicate clearly and meet each other’s needs. Thus, the focus for educators and counsellors should shift from valorising monogamy to helping people build skills for healthy relationships, period – whether monogamous or CNM.
Stigma, disclosure and mental health in CNM relationships
Despite the evidence that CNM relationships can be just as loving and fulfilling as monogamous ones, stigma towards CNM relationships and the people in them is prevalent (Moors et al., 2013). This stigma has tangible effects on the people involved, creating a cycle that can impact their mental health, their relationships and their willingness to be open about their lives. Researchers have begun examining how stigma surrounding CNM plays out in day-to-day experiences – particularly how it influences the decision to disclose or conceal one’s relationship orientation.
For many CNM individuals, deciding whether to ‘come out’ about their relationship style is a complex and ongoing negotiation. A recent qualitative study of 32 CNM adults in Australia explored how people navigate disclosure in various settings (family, friends, work, healthcare, etc.; Anderson et al., 2025). The findings highlighted several key themes. First, decisions around disclosure are rarely straightforward. Participants described carefully assessing each situation – a new job, a new friend, a healthcare appointment – and then adopting strategies of selective disclosure, sharing only with trusted people, or using intentionally vague language to avoid unwanted attention. Second, disclosures were often met with negative reactions. Participants reported responses ranging from awkwardness and subtle disapproval to outright rejection or harassment. Third, structural and institutional barriers compounded these challenges. Participants described fears of workplace discrimination or reputational harm, particularly in conservative or highly regulated professions. These fears are not unfounded – prior research documents that CNM individuals have experienced job termination, social ostracisation and even loss of child custody as a result of their relationships, reflecting the ongoing stigma and legal risks associated with non-traditional family structures (Moors, 2023; Sheff, 2017; Witherspoon and Theodore, 2021). Finally, healthcare emerged as a particularly fraught context (see also McCrosky, 2015). Unless health providers had received specific training or had prior experience of work with clients in CNM relationships, participants frequently encountered ignorance, judgement or awkwardness when disclosing their relationship status. Many felt that healthcare professionals lacked the knowledge or sensitivity needed to engage with CNM clients, an issue explored in more detail later. Converging evidence from sexual-health settings similarly shows that CNM clients anticipate stigma and tailor disclosure to perceived safety (Campbell et al., 2024; Scoats and Campbell, 2025).
Together, these themes paint a picture of a marginalised group that must navigate a mononormative world that is not built to accept or cater to them. In the Australian study described above (Anderson et al., 2025), every participant encountered actual or anticipated rejection due to disclosing CNM. This included hearing secondhand of others in their community losing jobs or being excluded by family, which reinforced their own fears (i.e. vicarious discrimination, see Saunders et al., 2025). The net effect is that many non-monogamous individuals are forced to conceal a core part of their identity. Research shows that anticipation of stigma leads to concealment – and indeed keeping a significant aspect of one’s life secret can create stress, anxiety and shame (Hinton et al., 2022).
The cumulative effect of this stigma is evident: CNM people often feel they must remain vigilant and carefully manage information about their lives. They may only discuss their true relationship situation in safe circles (close friends or online forums under pseudonyms). Some create almost a double life, in which their polycule (network of partners) is known and celebrated in private, but each individual publicly pretends to have either a single partner or none. From a health standpoint, this kind of concealment and fear can contribute to stress-related health issues and discourage people from seeking help or testing (e.g. being afraid to honestly discuss their sexual history with a doctor might hinder appropriate STI testing; Conley et al., 2012, 2015; see Borgogna et al., 2024, for a minority stress account). Indeed, in Anderson et al. (2025), some participants noted they had difficulty obtaining appropriate sexual healthcare because providers made incorrect assumptions or downplayed their needs – for example, one female participant said doctors told her she did not ‘need HIV testing because [she was] a woman’ (p. 1490) ignoring the fact that she might be involved in group sex or have partners of various genders.
In summary, the stigma surrounding CNM creates a challenging social environment that forces many to hide their relationships. This concealment is a rational response to real risks (discrimination, judgement), but it can negatively affect mental and even physical health (Borgogna et al., 2024; Mahar et al., 2024). The monogamy-superiority myth fuels this stigma, by framing CNM as inferior or problematic. Therefore, dispelling the myth and increasing public acceptance of relationship diversity is not just an academic exercise – it has practical importance for the well-being of a substantial minority population. We turn specifically to how these issues play out in healthcare and education settings, and what can be done to improve the situation.
Implications for healthcare and health education
The research evidence is clear: CNM relationships are a valid and healthy form of human intimacy, and those who practise CNM can have equally satisfying and loving relationships as anyone else (Anderson et al., 2026). Yet, many individuals in CNM relationships face stigma and knowledge gaps when interacting with others (Anderson et al., 2025; Valadez et al., 2020). For health professionals and educators worldwide, there is an important opportunity – and responsibility – to update perspectives and practices so as to be more inclusive of relationship diversity. This is especially pertinent in fields such as sexual health, mental health, counselling and family therapy, in which assumptions about ‘normal’ relationships abound. Here, we discuss key implications and make several recommendations for future forms of health education.
A key starting point is for providers to recognise and challenge personal biases (Thompson et al., 2020). Many health professionals and practitioners were trained in systems that implicitly view monogamous, heterosexual relationships as the healthiest or default model. These ingrained assumptions can lead to clinical misjudgements, such as attributing anxiety, relational conflict or sexual health risks solely to non-monogamy when such issues are common across relationship types. By engaging with the growing evidence base that debunks stereotypes about CNM, providers can approach their clients without prejudice or misplaced assumptions. This shift in mindset is fundamental to creating affirming and effective care.
Healthcare settings should be environments in which clients feel safe to disclose their relationship status. Research shows that many CNM individuals will avoid sharing this information unless they perceive clear signs of acceptance (Anderson et al., 2025; Valadez et al., 2020). Small but meaningful adjustments can foster this safety. Intake forms, for example, should avoid assuming monogamy and allow clients to self-describe their relationship status. In consultations, using neutral, inclusive questions about having partners (rather than a partner) signals openness. Finally, if clients do share information, responses grounded in curiosity and empathy can build trust (e.g. ‘are there ways in which your relationship structure affects your health needs that I should know about?’). Similarly, assumptions about risk and discussions about sexual health should be tailored to actual behaviours and needs, not stereotypes (McCrosky, 2015).
In sexual-health contexts, brief CNM-affirming guidance aligns with our broader recommendations: use behaviour-based rather than relationship structure-based sexual histories, adopt inclusive intake forms (e.g. make reference to ‘partners’ rather than ‘partner’) and normalise conversations about agreements and boundaries. Studies from Canada (Flicker, 2019) and the UK (Scoats and Campbell, 2025) emphasise the value of training clinicians to recognise consensually non-monogamous diversity and to approach clients without stigma. Building on these contributions and experiences, our analysis situates such recommendations within a broader health-education agenda and links them to empirical evidence that monogamy holds no inherent advantage in relationship or sexual satisfaction.
Another critical step is for providers to actively educate themselves and their colleagues about CNM. Lack of provider knowledge is a common barrier, even among well-meaning professionals working in education and health. Continuing professional development can help bridge this gap. For mental health professionals, a non-judgemental, client-centred approach is especially important (Flicker, 2019; Vaughan and Burnes, 2022). Therapy should focus on the client’s concerns without pathologising non-monogamy itself. Unfortunately, CNM clients often report experiences of therapists attributing unrelated difficulties – such as family conflict or trauma – to their relationship structure rather than other factors, which can be harmful and counterproductive (Schechinger and Moors, 2021). Instead, therapists should validate their clients’ chosen relationship style and provide support within that context. For example, if a polyamorous client is struggling with jealousy, effective therapy might involve building communication strategies and coping tools tailored to their specific relational dynamics, rather than recommending a shift to monogamy. Therapists should also be attuned to internalised stigma, helping clients explore feelings of guilt or shame that arise from dominant forms of societal messaging. In couples or polycule therapy, inclusive approaches that make space for multiple partners and voices can strengthen therapeutic outcomes (Schechinger et al., 2018; Schechinger and Moors, 2021).
For counselling and mental-health training, anti-oppressive and CNM-affirming competencies have been articulated in recent frameworks (Vaughan and Burnes, 2022), including approaches that de-pathologise relationship structure, adopt polycule-inclusive modalities and use supervision to counter mononormative bias. We agree with these approaches and believe our recommendations extend this work by advocating for the integration of CNM-affirming principles into pre-service health-education curricula and interprofessional training. Specifically, we emphasise the importance of formal training and supervision that equips practitioners to recognise mononormative bias, work competently with multi-partner relational dynamics and support clients in articulating and negotiating their agreements without pathologising relationship diversity (Moors et al., 2023; Schechinger and Moors, 2021).
Beyond clinical practice, there is a role for education and public health to reduce stigma and promote better understanding. Integrating discussions of relationship diversity into sex, sexuality and relationships education curricula, for instance, can help normalise CNM and equip individuals with the language and frameworks to engage in these relationships ethically (Lameiras-Fernández et al., 2021). Recognising that people form fulfilling relationships in both monogamous and CNM arrangements helps promote a more inclusive and informed public discourse. Such an approach is not about advocating for any particular lifestyle but about presenting accurate information and dismantling harmful myths – for example, that CNM relationships are inherently unstable or less committed. Professional education programmes, including nursing, medical and counselling curricula, should also incorporate content on CNM to ensure future providers are equipped when these topics arise in practice.
Finally, there is a need for structural and policy change to ensure equity and safety for people in CNM relationships. Beyond the individual clinical practice and service-level adjustments discussed earlier, this includes institutional and regulatory reforms that address how relationship diversity is recognised within healthcare and related systems. At an institutional level, this may involve reviewing policies that implicitly assume dyadic family structures, including hospital visit rules, consent and decision-making frameworks, and eligibility criteria for services. On a broader scale, healthcare professionals can lend their voices to policy and professional conversations about legal and administrative recognition of diverse relationship structures, particularly in areas such as healthcare decision-making, parental recognition and child custody. While such changes may be slow in coming about, coordinated institutional reform and professional advocacy have a critical role to play in shifting systems towards greater equity and safety for CNM individuals and families.
Conclusion
For too long, the idea that ‘monogamy is superior’ has gone unchallenged in both the popular imagination and professional practice. But as scientific research accumulates, it becomes evident that this is a myth, not a fact. Relationship satisfaction and sexual satisfaction are not determined by whether a relationship is monogamous or CNM. However, these dynamics are typically navigated through ongoing communication and explicit re-negotiation of boundaries, fostering a relationship environment in which transparency and consent are prioritised over secrecy and assumption (Anderson et al., 2026). Loving, healthy relationships come in many forms – from the devoted monogamous married couple to the polyamorous triad deeply committed to each other’s well-being. What matters most are qualities such as mutual respect, trust, communication and consent. Monogamy can foster those qualities, but so can CNM. Indeed, people in open or polyamorous relationships often demonstrate high levels of communication and trust, precisely because they navigate complexities that monogamous couples might not face (Moors et al., 2017; Wood et al., 2018). The success of these relationships, even in the face of societal disapproval, speaks volumes.
Breaking the monogamy-superiority myth is not just an academic exercise, however – it has practical implications for public health, mental health and educational outreach. By understanding that CNM is a valid way of living, health professionals can avoid misdiagnosing or pathologising what is simply a difference in relationship orientation. We have seen how damaging stigma can be: it can silence individuals, lead to subpar healthcare interactions and cause unnecessary psychological and social distress. However, there is also evidence we are also witnessing positive change – there is a growing body of evidence that is contributing to greater visibility and normalisation of CNM. There is a growing recognition that, just as we strive to be inclusive of various sexual orientations and gender identities, we should also be inclusive of different relationship orientations.
For health educators and providers worldwide, the charge is clear – there is an urgent need to update frameworks to include CNM as a legitimate and healthy variation of human relationships. This means educating ourselves, our students, and our patients and clients that monogamy is a choice, not a yardstick of relationship quality. It means providing care that is free of judgement and grounded in the actual needs of the individual or individuals in the relationship as they present to us. By so doing, we not only improve the healthcare experiences of CNM individuals – enabling them to discuss their lives openly and receive appropriate care – but we also contribute to dismantling the broader stigma, leading to better mental health and relationship outcomes.
Put simply, acknowledging the equality of relationship satisfaction across structures should lead us to the simple but powerful conclusion that love and happiness are not confined to one relationship model. As the evidence mounts, it is incumbent on us as health education to ensure that our narratives, curricula and practices reflect this truth, fostering a more inclusive understanding of relationships in the communities we live in, work for and serve.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Joel Anderson was supported by an Australian Research Council Discovery Award (DE230101636).
AI statement
The authors did not use generative AI in the preparation of this manuscript.