
Abstract
Background:
Comprehensive sexuality education (CSE) aims to equip youth to make informed decisions about their bodies and sexuality to lead healthier lives. The nature of sexual and reproductive health (SRH) education in Canada is determined locally by provincial and territorial governments, resulting in inconsistent coverage, delivery, and quality of curricula. This study assessed the strengths and gaps of Canadian SRH curricula using the United Nations’ International Technical Guidance on Sexuality Education and offers evidence-based policy recommendations.
Methods:
Provincial and territorial SRH curricula for Grades 6–12 for Canadian public schools were extracted from publicly available governmental websites and examined using the 94 learning objectives across 8 Key Concept Areas (KCA) and 27 Topics obtained from the UNESCO Guidance. Each curriculum was reviewed by two researchers and given a Comprehensiveness Score (CS). The number of Guidance learning objectives addressed within a Topic was calculated as the Topic score, and the sum of the Topic scores within a KCA was reported as the KCA score.
Results:
The mean CS across Canada was 57.94%, with the highest score being 81.91% (ON) and the lowest being 37.23% (NWT). KCA 5 (Skills for Health and Wellbeing) (65.93%) and KCA 2 (Values, Rights, Culture and Sexuality) (63.46%) had the highest coverage across Canada, while key gaps included KCA 8 (Sexual and Reproductive Health) (51.44)%. The lowest-scoring topics were Topic 8.2 (11.54%) and Topic 1.4 (21.79%), with learning objectives on long-term parenting and relationships, and HIV and AIDS stigma and care widely missing.
Conclusions:
SRH curricula across Canada vary in comprehensiveness. Increasing alignment and comprehensiveness of SRH curricula across the country, while allowing for context-specific additions in each province or territory, could improve the quality and consistency of SRH education. In addition, SRH curricula should be regularly evaluated and updated as needed, ensuring they reflect societal changes and are evidence-informed.
Keywords
Background
Comprehensive Sexuality Education (CSE) is defined as a curriculum-based approach that engages with the cognitive, emotional, physical, and social aspects of sexuality, emphasising age-appropriate, incremental learning, and gender equality (UNESCO, 2018). CSE has the potential to equip youth to explore their sexual identity, foster healthy behaviours, build healthy relationships and improve informed decision-making, ultimately leading to improved health outcomes (Action Canada for Sexual Health & Rights, 2020). Studies exploring the SRH education needs and priorities of Canadian youth have identified a desire for more inclusive SRH education, a shift away from a biological lens to including topics such as healthy relationships, safety and the social and emotional aspects of sex (Action Canada for Sexual Health & Rights, 2020; Laverty et al., 2021; Walters and Laverty, 2022). In addition, for SRH education to be effective, teachers and instructors need to be offered prolonged and consistent support in delivering material that resonates with the needs of their learners (Action Canada for Sexual Health & Rights, 2020).
Curriculum-based SRH education in Canadian public schools is not coordinated at the federal (national) level; instead, it is offered by individual provinces and territories (Statistics Canada, 2024). This flexibility allows curricula to be tailored to the needs of learners in different provinces. While certain Canadian (Action Canada for Sexual Health & Rights, 2020; Davis et al., 2023; Health Canada, 2003; SIECCAN, 2019) and international (UNESCO, 2018) conceptual frameworks and broad guidelines are available for CSE curriculum design and delivery, there is currently no central system to oversee the design, delivery, and update of curricula across Canada. Subsequently, there is also no unified system to report these results or evaluate programme delivery and impact (Action Canada for Sexual Health & Rights, 2020; Robinson et al., 2019, 2024; Walters and Laverty, 2022), and the extent to which guidelines and frameworks have been implemented remains largely unknown.
There is limited literature conducting a systematic evaluation of public school SRH curricula, particularly at the national level. Two notable examples include a report by Action Canada for Sexual Health & Rights (2020) and a study by Robinson et al. (2019), both of which report inconsistencies in SRH curricula across provinces and territories and identify the need to address essential (albeit controversial) topics such as gender identity, abortion, sexual orientation and pleasure. SRH is often embedded within the Health Education curriculum; therefore, some studies have evaluated Health Education curricula across Canada, with SRH education being a minor component within their broader analysis (Lu and McLean, 2011; Robinson et al., 2024). These studies similarly highlight inconsistencies in the content and delivery of SRH curricula across provinces and territories, noting that outdated materials often reinforce heteronormative narratives and fail to reflect the realities and needs of two-spirit, lesbian, gay, bisexual, transgender, queer, and other sexual and gender diverse (2SLGBTQ +) young people (Lu and McLean, 2011; Robinson et al., 2024).
This article derives from the first phase of a larger study by the Canadian Advisory of Women Immigrants, a non-profit organisation dedicated to responding to and meeting the SRH education needs of Canadian immigrant and refugee youth. The broader study aims to understand the needs and priorities of public school educators who utilise the current curricula to deliver SRH education for Grades 6–12 to young people from different racialised backgrounds in Canada. However, before examining the cultural responsiveness of curricula, it is necessary to gain an in-depth understanding of the topics currently included in SRH curricula and how they might vary across provinces and territories. This article assessed how comprehensive SRH curricula are in Canadian public schools for Grades 6–12 and provides evidence-based recommendations to guide the targeted improvement of SRH curricula.
The United Nations (UN) International Technical Guidance on Sexuality Education (UNESCO, 2018) provides a framework to enhance CSE design, delivery and evaluation, and identifies CSE learning objectives across eight Key Concept Areas (KCAs). The Guidance has been used internationally in a variety of ways: as a framework for document analysis of different CSE frameworks (Harel and Yamamoto, 2025; Mukanga et al., 2024); as a source of reference for the development of national CSE guidelines and education modules (Liu et al., 2023; Yakpir and Atuguba, 2022); and as a complement to existing guidelines to assess its relevance for use within specific contexts (Goldman, 2012, 2013, 2015). To date, Robinson et al. (2019) is the only study to present a systematic evaluation of the comprehensiveness of Canadian provincial and territorial SRH curricula for Grades K-6 using the Guidance. This study presents a similar evaluation for provincial and territorial curricula for Grades 6–12.
Methods
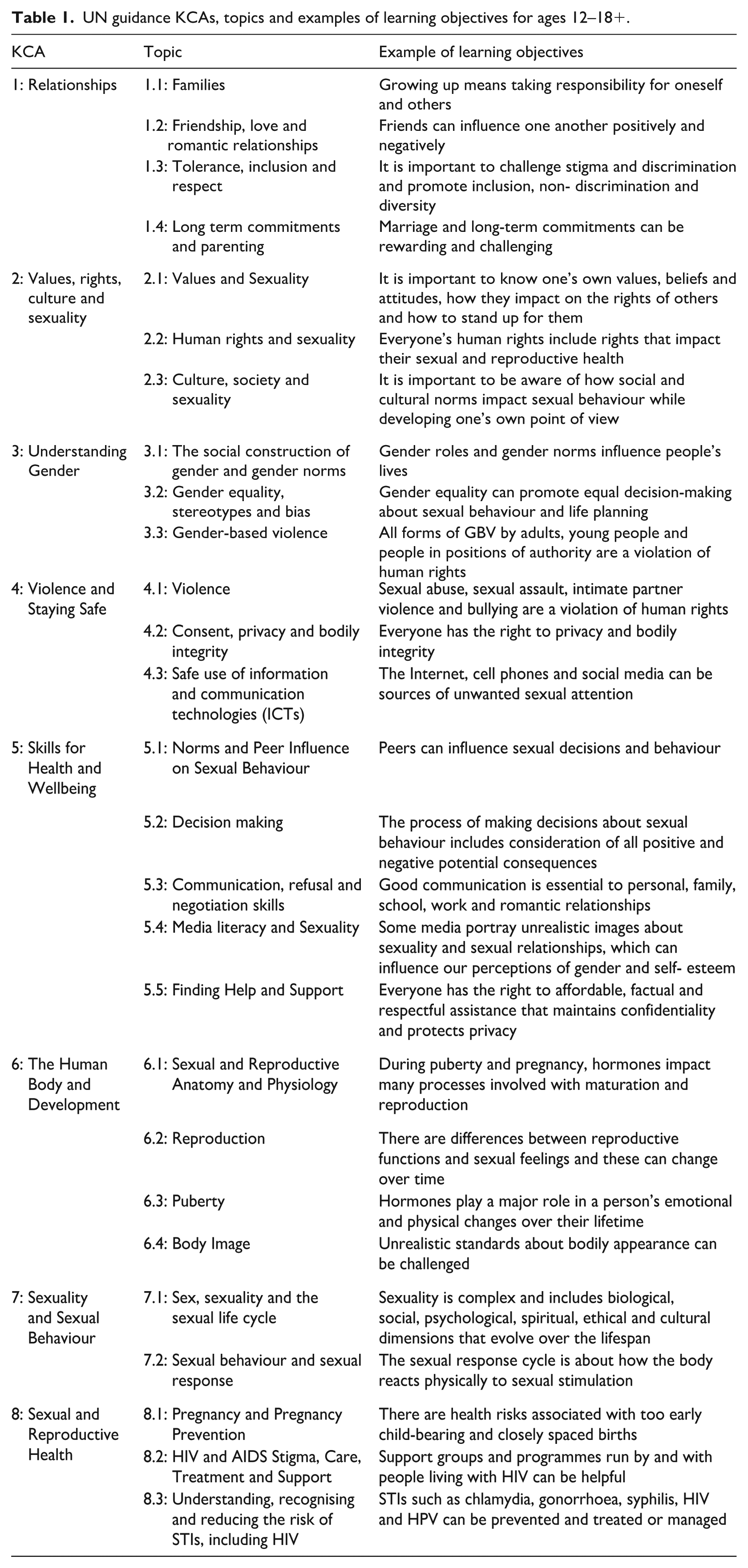
This study used document analysis to evaluate the comprehensiveness of SRH curricula across Canadian provinces/territories for Grades 6–12 using the UN Guidance as the evaluation framework (Atkinson and Coffey, 1997; Bowen, 2009). The Guidance provides a detailed framework for CSE that identifies eight broad KCAs and operationalises the KCAs into 27 Topics with learning objectives within each topic for age groups: 5–8, 9–12, 12–15 and 15–18+ years (UNESCO, 2018). As this study focused on Grades 6–12, the learning objectives for the latter two age categories were used, resulting in eight KCAs, 27 topics and 94 learning objectives (Table 1).
UN guidance KCAs, topics and examples of learning objectives for ages 12–18+.
The courses within which SRH education is delivered in Canadian public schools for Grades 6–12 were identified, and both mandatory SRH curricula and optional courses 1 were included in the study. SRH-specific learning objectives for each Grade 6–12 were then extracted from government websites between April 2023 and May 2024 and compiled into a spreadsheet, organised by province/territory (see supplemental online file). The learning objectives identified for each province or territory were assessed for alignment with the international Guidance. If a learning objective in the Guidance was identified in any grade between 6 and 12, it was assigned a score of 1; if not, it received a score of 0. Therefore, a score of 0 indicates that a student progressing through the public education system in Grades 6–12 in that province/territory would not have the opportunity to learn that specific objective. We refer to this total score as the Comprehensiveness Score (CS). The maximum score possible is 94, indicating that all of the Guidance learning objectives have been met for Grades 6–12. In addition, the number of Guidance learning objectives addressed within a Topic was calculated as the Topic score. The sum of the topic scores within a KCA was reported as the KCA score. All scores were described and converted to percentages for comparability across provinces/territories and across Canada to determine gaps and strengths of SRH curricula (Vetter, 2017).
Two researchers (RM, ZA) independently reviewed each curriculum, with discrepancies resolved by a third member of the team. The analysis utilised publicly available documents; therefore, no ethical approval was required.
Results
CS, KCA, and Topic scores for each province and territory are outlined in Table 2. The average CS across Canada was 57.94%, ranging from 37.23% (35/94; NWT) to 81.91% (77/94; ON). The most extensively covered KCAs included KCA 5 (average KCA score 65.93%), closely followed by KCA 2 (63.46%). These included learning objectives relating to peer influence, decision-making, communication skills, and media literacy. KCA 8 received the lowest average score (51.44%), while the lowest-scoring topics were Topic 8.2 (11.54%) and 1.4 (21.79%). At the time of the analysis, five provinces (ON, MB, BC, PEI, SK) had opt-out policies 2 for SRH education, while only AB had an opt-in policy 3 ; the remaining provinces/territories lacked any formal policy.
CS, KCA scores, and topic coverage for SRH education curricula across Canada.
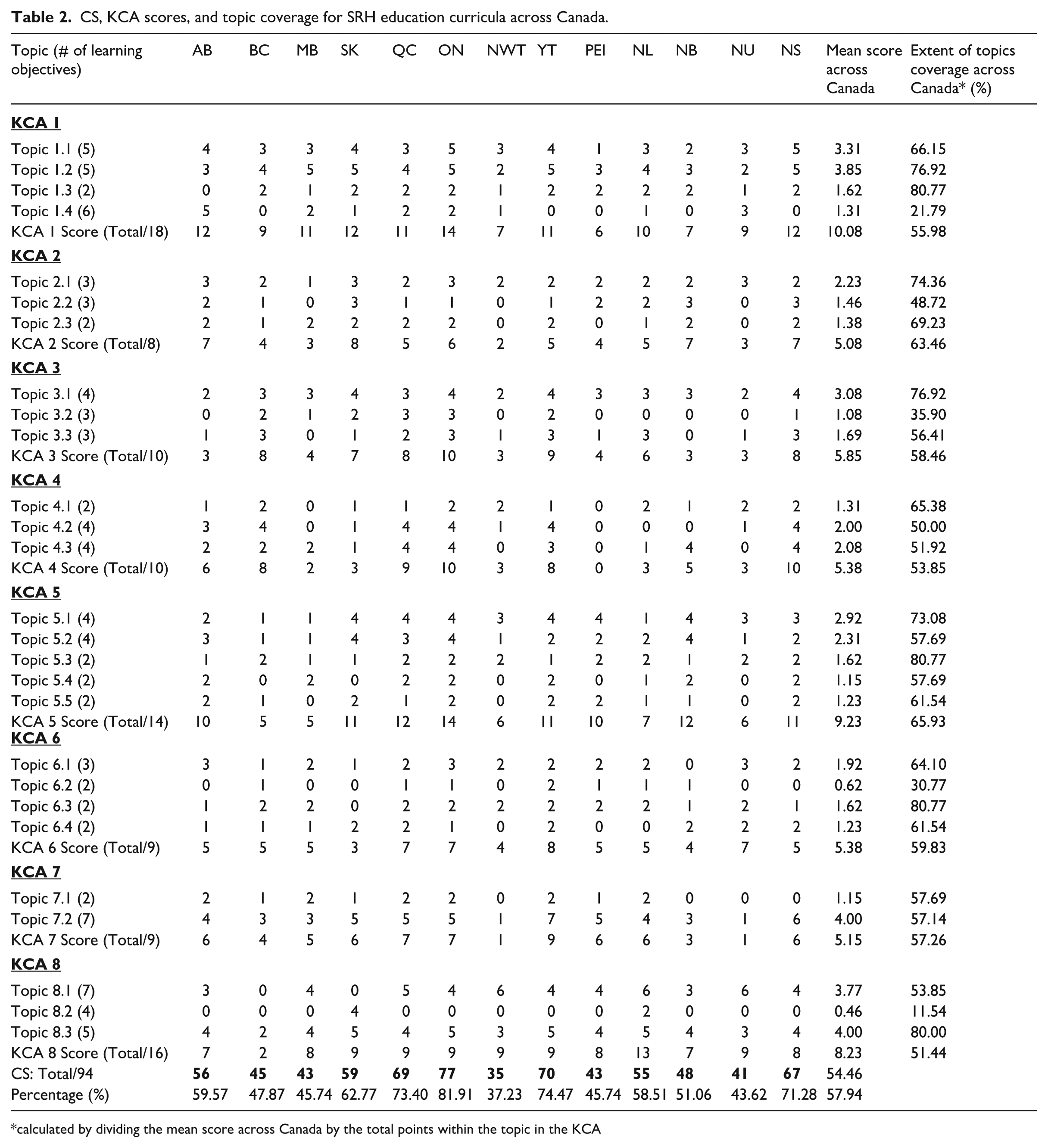
calculated by dividing the mean score across Canada by the total points within the topic in the KCA
British Columbia (BC)
Redesigned in 2019, SRH education in BC is embedded within the Physical and Health Education curriculum – a mandatory course until Grade 10. The CS was 47.87% (45/94). The two highest-scoring KCAs (80%) were KCA 3 and 4. The curriculum heavily covered sexual and gender identity, consent, gender-based violence, risk assessment and seeking help. KCA 8 had the lowest score (12.50%), addressing only two of the learning objectives in Topic 8.3 on STI prevention and safer sex communication. There was also no mention of contraceptives in the learning objectives.
Alberta (AB)
AB’s SRH curriculum is integrated into Physical Education and Wellness (Grades 4–6; updated in 2022), Health and Life Skills (Grades 7–9; updated in 2002), and Career and Life Management (taken once between Grades 10–12; updated in 2002). The CS was 59.57% (56/94). The highest KCA score was for KCA 2 (87.50%), with learning objectives emphasising values, attitudes and norms in sexual decision-making. The lowest-scoring KCA was KCA 3 (30%), with no objectives in Topic 3.2, and the three learning objectives included covered the effect of social influences on sexuality and gender, and the signs and consequences of various forms of violence.
Saskatchewan (SK)
SRH is delivered within the Health Education curriculum for Grades 1–9 (updated in 2009) and within Wellness for Grade 10 (updated in 2012). The CS was 62.77% (59/94). SK was the only province/territory in Canada with a perfect score in KCA 2, emphasising sexual rights, and the influence of social, cultural, and religious factors on sexual behaviour. It was the only province with a perfect score for Topic 8.2, while all other provinces/territories had a score of 0% except for NL (50%). The lowest KCA scores were in KCA 4 (30%) and 6 (33.33%); within these KCAs, the curriculum did not include learning objectives on consent, boundaries, reproductive physiology, and anatomy. SK was the only province across Canada to have 0 learning objectives for Topic 6.3, as puberty is taught once in elementary school and not discussed again.
Manitoba (MB)
In MB, SRH is delivered within the Physical Education and Health curriculum for Grades 5–10 (updated 2005), excluding Grade 6. The CS was 45.74% (43/94). The highest KCA scores were observed for KCA 1 (61.11%) and KCA 7 (55.56%), with an emphasis on influences on sexuality and gender roles, including friends and family, and the components of maintaining healthy relationships. In contrast, curricular gaps included KCA 5 (35.71%) and KCA 4 (20%). There were limited learning objectives on peer influence on sexual behaviour, communication skills and the concept of consent.
Ontario (ON)
ON’s SRH curriculum was last updated in 2019 and is mandatory for Grades 1–8 (Human Development and Sexual Health education) and optional to Grades 9–12 (Health and Physical Education). With the highest CS in Canada (81.91%; 77/94), ON was the only province to have three perfect KCA scores – 3, 4 and 5 – while other provinces/territories had either one (NS, YT, SK) or no perfect KCA scores. Learning objectives emphasised gender stereotypes and biases, consent, safe usage of social media, navigating peer norms, decision-making, and communicating sexual needs. The remaining KCA scores ranged from 75% to 80%, a score that was considerably higher than other provinces. The lowest KCA score belonged to KCA 8 (56.25%), which covered STI prevention but had 0 learning objectives on HIV and AIDS (Topic 8.2) and comprehensive pregnancy options like adoption or abortion (Topic 8.1).
Quebec (QC)
As of 2024, SRH education is delivered mandatorily for all elementary (Grades 1–6) and secondary grades (Grades 7–11) through two ways: through a Culture and Citizenship programme; and as Learning Content in Sexuality Education (Gouvernement du Québec, 2025a). The CS was 73.40% (69/94), the third highest in Canada, after ON and YT. The highest KCA scores belonged to KCA 4 (90%), 5 (85%) and 3 (80%), with learning objectives on consent, social and peer influences on sexual behaviour, and discrimination based on gender and sexuality extensively covered. KCA 8 had the lowest score (56.25%). Learning objectives on HIV and AIDS (Topic 8.2), how to access contraceptives (Topic 8.3), and practices that can threaten or support a healthy pregnancy (Topic 8.1) were missing from the curricula.
New Brunswick (NB)
Updated in 2017, NB’s SRH education is mandatory in Grades 6–10, and is embedded within Personal Wellness (Grades 6–8) and Physical Education and Health (Grades 9–10). The CS was 51.06% (48/94). The highest KCA score belonged to KCA 2 (87.50%), emphasising all learning objectives on human rights and sexuality (Topic 2.2). For each grade, the curriculum had an Anti-Discrimination section, which highlighted the impact of biases and stereotypes, as well as the importance of acceptance among peers. The curriculum also emphasised KCA 5 (85.71%) and included learning objectives on sexual decision-making (Topic 5.2), media influences on decision-making (Topic 5.1), and medical consent laws for minors (Topic 5.2). The lowest KCA score was in KCA 3 (30%), with learning objectives for Topics 3.2 and 3.3 entirely missing.
Prince Edward Island (PEI)
SRH education is delivered as a part of the Health Curriculum and is mandatory until Grade 9, with the most recent curriculum being piloted in 2020. This curriculum had a CS of 45.74% (43/94). The highest KCA score was for KCA 5 (71.43%), with learning objectives focused on how to act on personal values in the face of peer pressure (Topic 5.1), the skills necessary to do this (Topic 5.3), and identifying and accessing support for sexual health (Topic 5.5). PEI was the only province/territory across Canada to have a KCA score of 0. There were no learning objectives for KCA 4, entirely missing discussions about violence, consent, privacy and bodily integrity.
Newfoundland and Labrador (NL)
In NL, SRH education is mandatory and spans from Kindergarten to Grade 9. The curriculum dates to 1995, except for Grade 9, which was updated in 2008. NL had a CS of 58.51% (55/94). The highest KCA score was for KCA 8 (81.25%), which was also the highest KCA 8 score across Canada. It is one of two provinces (the other is SK) to have any learning objectives for HIV and AIDS (Topic 8.2). The lowest KCA score was for KCA 4 (30%), with no learning objectives on consent (Topic 4.2) and one learning objective on analysing media portrayals of relationships and sexuality (Topic 4.3). The word ‘consent’ does not appear in the curriculum at all.
Nova Scotia (NS)
SRH objectives in NS are included within the Health Education curriculum for Grades 1–9, with the last revision in 2022. The CS was 71.28% (67/94). NS was one of two provinces/territories, along with ON, to have a perfect score for KCA 4, including learning objectives on the recognition of healthy and unhealthy relationships, and the influence of factors on decision-making and providing consent. The lowest KCA score was KCA 8 (50%), with no learning objectives for Topic 8.2, health risks based on the timing of pregnancy, or the option of adoption.
Yukon (YT)
YT’s SRH curriculum was updated in 2024 by adapting BC’s SRH programme to the YT context, including Indigenous ways of knowing (Government of Yukon, 2023). The curriculum uses trauma-informed teaching approaches to SRH education from Kindergarten to Grade 12. The CS was 74.47% (70/94). It was the only province/territory across Canada to have a perfect KCA score for KCA 7, with learning objectives on the intersection between mental health, consent, and the different types of sexual activities. YT had the highest KCA 6 score (88.89%) across Canada and was the only province/territory to have a perfect score for Topic 6.2. The lowest KCA score was for KCA 8 (56.25%), wherein learning objectives on sexually transmitted infections were included (perfect score for Topic 8.3), but those on HIV and AIDS, health risks based on the timing of pregnancy, or the option of adoption (Topics 8.1–8.2) were missing.
The Northwest Territories (NWT)
At the time of this study, the NWT was currently undergoing a curriculum renewal process (2023–2028) in partnership with BC’s Ministry of Education, to adapt BC’s curriculum to the unique context and needs of the territory (Northwest Territories Department of Education, Culture and Employment, 2022). This evaluation did not include any of the curricula being piloted, as it was still under revision, and thus, the most recent 1995–1996 SRH curriculum for Grades 6–9 was assessed. It had the lowest CS across Canada (37.23%; 35/94). The KCA with the highest score was KCA 8 (56.25%), which included learning objectives on preventing and navigating unplanned pregnancy, STIs, and contraception, but none for Topic 8.2. The lowest KCA score was for KCA 7 (11.11%), which was the lowest KCA 7 score across Canada, tied with NU. Learning objectives on important concepts such as sexuality over the lifespan, pleasure, and the intersection between culture and sexuality were absent.
Nunavut (NU)
NU’s SRH curricula follow NWT’s Health Programme for Grades 3–9 with additional Inuit culture-based SRH modules for Grades 10–11. The Curriculum Development division also provides online resources for teachers to support the delivery of education, such as information pamphlets in English, Nunavik, and the four major regional dialects of Inuktitut, along with translation guides for SRH terms to increase accessibility (IRespectMyself, n.d.). The CS was 43.62% (41/94). The highest KCA score was for KCA 6 (77.78%), with learning objectives emphasising anatomy, puberty, body image, and self-esteem. The category with the lowest KCA score was KCA 7 (11.11%), which was also the lowest KCA 7 score across Canada, tied with NWT. No learning objectives mentioned sexual desire, pleasure, or the intersection between culture and sexual behaviours.
Discussion
Although national and international CSE guidelines exist, there is a scarcity of literature systematically evaluating SRH curricula across Canada using these standardised guidelines (Action Canada for Sexual Health & Rights, 2020; Robinson et al., 2019). This study was the first to assess the comprehensiveness of SRH curricula for Grades 6–12 in the Canadian public school system using the UN’s International Technical Guidance on Sexuality Education. As only provincial/territorial learning objectives for Grades 6–12 were assessed, it is important to note that any learning objectives in the Guidance that were unsatisfied could have been met in previous grades not included in the analysis.
This analysis revealed variability in SRH curricula comprehensiveness across Canada, with an overall CS ranging from 37.23% (NWT) to 81.91% (ON). The average CS was 57.94% across Canada, with 8 of 13 provinces/territories scoring between 40% and 62%. This variation in the CS across provinces may be interpreted as a result of curricula being mandated at the provincial/territorial level, as stated by section 93 of the Constitution Act of 1867, and may indicate a province or territory’s commitment to SRH education (The Constitution Acts 1867 to 1982, 1982). ON had the highest CS in Canada, with a curriculum that was developed after consultations with more than 70 health-related organisations and stakeholders in 2015 and included more comprehensive topics, such as safe use of technologies, LGBT+ identities, and healthy relationships (Jolly, 2015; Ontario, n.d.). ON’s high CS may be partly attributed to the province’s strong emphasis on collaboration and prioritisation of SRH education.
Outdated SRH curricula often do not adequately address the current SRH needs of young people (Robinson et al., 2024). At the time of this study, those of the NWT were currently undergoing major revisions (2023–2028) from their previous 1995–1996 form (Government of Northwest Territories Education, Culture and Employment, n.d.). Partnering with BC’s Ministry of Education, NWT was adapting BC’s curricula to their unique context. Therefore, if NWT’s curricula renewal efforts prioritise the current SRH needs of youth and make intentional efforts to improve the comprehensiveness, their CS (37.23%), currently the lowest in the country, may improve once these changes are implemented.
In addition to the large variation in CS across Canada, the KCA scores also varied between provinces/territories (Table 2). For example, BC’s coverage of KCA 8 was limited to 12.50%, compared to NL (81.25%). This KCA was the least covered across Canada, with an average of 50.96%. This is concerning, as a significant proportion of Canadian youth aged 15–24 are at high risk for STIs and unplanned pregnancies (Rotermann and McKay, 2020). KCA 7 had low coverage in NWT’s curricula (11.11%) compared to other provinces/territories. In contrast, NWT’s KCA score for KCA 8 was one of the highest (56.25%) across Canada. ON’s curricula, with scores on most KCAs above 75%, also scored 56.25% on this KCA.
These findings highlight the differing strengths and gaps in each province and territory’s SRH curricula. Based on our analysis, the provinces/territories most in alignment with the UN Technical Guidance were ON (81.91%), followed by YT (74.47%) and QC (73.40%). Robinson et al. (2019) also found ON’s SRH curricula to be one of the most aligned provinces/territories with the UN Guidance for Grades K-6, however, they found QC to have the least comprehensive SRH curricula across Canada. This discrepancy may be attributed to recent updates restructuring QC’s sexuality education beginning in the 2024–2025 school year, along with grade-specific differences in SRH education outcomes (Gouvernement du Québec, 2025a). In addition, Robinson et al. (2019) found that KCAs 1, 5, and 6 were the most covered in SRH curricula across Canada, while KCA 2 was the most underrepresented. In contrast, this study found KCAs 2, 5, and 6 to be the most covered, possibly suggesting that topics within KCA 2 are reserved for older grades. In both studies, some topics, such as Topic 1.4 (Long term commitments and parenting) and Topic 8.2 (HIV and AIDS stigma, care, treatment, and support), were largely missing across all grades.
It is important to note that this analysis only focused on provincial/territorial SRH curricula learning objectives, and there exist supplementary curriculum resources that complement these learning objectives (AB, BC, QC, YT, NU, NS, NWT, MB, NL, NB). These take the form of components used by the discretion of educators, and their existence adds to the variability of SRH education delivered across the country (Action Canada for Sexual Health & Rights, 2020). For example, while there was no mention of contraceptives in BC’s SRH learning objectives, lesson plans on the topic are available in an optional Supporting Student Health Guide for educators to use at their discretion (British Columbia Ministry of Education and Child Care, 2022). In QC, the Ministry of Education provides broad SRH objectives, but specific lesson plans are provided through school boards or education institutions (Gouvernement du Québec, 2025b). Because of this, lesson plans across Quebec may vary depending on the school board or staff, further adding to the variability of SRH curricula.
While content variability is inevitable in a regionally governed education system, a potential benefit of this system is the increased flexibility for SRH curricula to be adapted to the province/territories’ unique context. Young people from equity-deserving communities face additional barriers in accessing culturally responsive SRH education (Walters and Laverty, 2022). Sexual and reproductive health beliefs are deeply embedded within socio-cultural contexts, requiring culturally responsive CSE policies and practices (Szlachta and Champion, 2020; UNESCO, 2018). However, most SRH curricula reviewed adopted an approach that neglected the socio-cultural backgrounds and experiences of immigrant populations. Furthermore, resources were seldom provided to enable learners to navigate their unique socio-cultural circumstances. A notable exception was the NU SRH curricula that could be adapted to improve accessibility and relevance to Indigenous populations through resources like Tukisiviit- Do you Understand?, a language guide for SRH terms, anatomy, STIs, and risk behaviours (IRespectMyself, n.d.; Pauktuutit Inuit Women of Canada, 2012). The NWT also has an educator resource that outlines how to deliver culturally appropriate SRH education to Dene, Inuit and Metis populations (Northwest Territories Department of Education, Culture and Employment, 1998). NU and NWT were the exceptions, while most other provinces/territories had limited culturally responsive SRH education, leaving young people from these communities unprepared to deal with SRH-related issues and seek alternative sources of SRH education (Meherali et al., 2022; Rukh-E-Qamar et al., 2024).
Because SRH education is mandated by provincial/territorial governments, its focus and delivery are at the discretion of the political party in power and often influenced by the party’s ideology and priorities (Thomson, 1994), with recent debate about ON’s SRH education being a case in point (Bialystok et al., 2020; Bialystok and Wright, 2019). SRH education is a heavily debated and controversial topic, driven by cultural, religious, and social perspectives on sexual minorities and youth sexuality (Bialystok et al., 2020; Thomson, 1994). In 2015, ON’s SRH curricula were updated from the 1998 version to include a more comprehensive range of topics. However, these changes were met with public protests, angry newspaper articles, and a decline in public school enrolment (Bialystok and Wright, 2019). When the conservatives came into power in 2018, they repealed the new curriculum and reverted it to the regressive 1998 version, triggering uproar from the more liberal public, only to reinstate an updated 2019 curriculum fairly similar to the original 2015 version (Bialystok et al., 2020). Amid these political battles, the sexual education of youth is often compromised.
Several Canadian provinces (NB, SK, AB) have recently enacted conservative policy changes in SRH education, fuelling anti-2SLGBTQI+ discourse (McMackon, 2024). This is concerning as 2SLGBTQI+-inclusive learning objectives in KCA 3 are among the lowest KCA scores across these provinces. Both NB and AB curricula lack 2SLGBTQI+education, scoring the lowest (30%) compared to the national average of 58.46%. Policy 713 in NB (New Brunswick Department of Education and Early Childhood Development, 2025) and AB’s proposed Education Amendment Act 2024 (Government of Alberta, 2025) may further lower these KCA scores, as they seek to restrict students’ ability to express gender identity by requiring parental consent to change names or pronouns if under 16. These policy changes are likely to further alienate 2SLGBTQI+youth, rather than promote inclusion and respect. LGBTQ+ young people already face homophobic and transphobic harassment in school settings, often with little support and intervention from school structures (Taylor and Peter, 2011). There is some evidence that the lack of LGBTQ+ inclusive SRH education has driven LGBTQ+ youth to seek alternative sources of education, such as the Internet, resulting in lower confidence when engaging in sexual relationships and higher rates of STIs, violence, and risky sexual behaviours (Charest et al., 2016).
In addition, some provinces/territories have opt-in/out policies, providing parents with the choice to exempt their child from essential SRH education altogether. Parental decision-making may be rooted in misconceptions, including fear of children engaging in sexual activities, increased pregnancies and STIs, support for conservative political ideologies, and religious/cultural beliefs (Goldman, 2008). Contrary to parental belief, withholding essential SRH education from youth – many of whom become sexually active at a young age – increases their vulnerability to unintended pregnancy, STIs, and other risk-related sexual behaviour (Brough, 2008; Goldman, 2008; Grace, 2018). Ensuring universal access to broad-based inclusive SRH education is a foundational concern – without such access, any discussion of comprehensiveness becomes secondary.
It is important to recognise that SRH curricula comprehensiveness does not directly equate to SRH education delivery to youth, as there are access barriers (i.e. socio-cultural contexts, opt-in/out provisions), variations in educator delivery and preparedness (i.e. availability of supplementary materials), and optional SRH courses to be chosen by students. Political factors also play a significant role in the development, delivery, and priorities of SRH curricula, highlighting the complex, intersectional, and rapidly changing dynamic landscape of SRH education for youth. As many SRH curricula in Canada currently fall short of international standards and youth needs, the need for policy and curricular revisions is warranted.
Implications for future policy and practice
This study provides evidence to guide policymakers and curriculum planners in strengthening SRH education to better equip young people to lead healthier sexual lives. To enhance comprehensiveness and consistency across Canada, ministries of education may consider utilising existing national (Action Canada for Sexual Health & Rights, 2020; Davis et al., 2023; Health Canada, 2003; SIECCAN, 2019) and international (UNESCO, 2018) CSE guidelines to aid in curriculum planning and development. Consistent implementation could help reduce variability and political influence, while adaptation to regional and cultural contexts may ensure relevance and retain essential topics. Although CSE guidelines do not specify curriculum renewal intervals, policy makers are encouraged to establish processes for the ongoing evaluation and revision of SRH curricula in collaboration with stakeholders, ensuring curricula reflect societal changes and are evidence-informed (Robinson et al., 2024; SIECCAN, 2019).
Currently, SRH curricula are not consistently delivered across all grades, limiting exposure to needed information and comprehension (Robinson et al., 2024). Expanding SRH education throughout elementary and high school may enable progressive learning that aligns with developmental milestones. In addition, the development and implementation of high quality educator training resources may further address the needs of equity-deserving populations and ensure standardisation of SRH education delivery (Robinson et al., 2019). Collectively, these evidence-based recommendations aim to address gaps in comprehensiveness, promote regular curriculum renewal, expand education across all grades, and strengthen educator preparedness, ultimately fostering more equitable and effective SRH education in Canada.
Conclusion
SRH education comprehensiveness currently varies across Canadian provinces and territories, reflecting differing socio-cultural and political contexts. There is a need for improved alignment of SRH education across Canada, more regular evaluations and updates to SRH curricula, and a shift towards CSE-based approaches. Findings from this review can guide policymakers and curriculum developers in reforming SRH education to further equip young people with the means to make informed decisions and improve their sexual well-being and that of their partners. Future SRH curricula should be more closely tailored to the needs of equity-deserving groups and delivered in a culturally responsive way. Further studies are needed to evaluate the extent to which SRH curricula are culturally responsive and meet the needs of migrant and other equity-deserving youth to guide targeted improvements to SRH education for these populations.
Supplemental Material
sj-docx-1-hej-10.1177_00178969251376867 – Supplemental material for Does Canada have comprehensive sexual and reproductive health education? A national assessment of public school curricula
Supplemental material, sj-docx-1-hej-10.1177_00178969251376867 for Does Canada have comprehensive sexual and reproductive health education? A national assessment of public school curricula by Radha Maradiya, Ksenia Kholina, Zara Ahmed, Ana-Maria Dumitrache, Yuvika Dandiwal, Harini P. Aiyer, Marianna Kovtun and Hani Rukh-E-Qamar in Health Education Journal
Footnotes
Acknowledgements
We thank Pram Thennakoonwela, Rehma Khan, Jessica Dekker, and Aviva Sharma for their contributions to this study.
Data availability
This study analysed publicly available documents, references to which are included in this published article and its supplementary file.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.