
Abstract
Objectives:
This study aimed to assess satisfaction with family and patient education in relation to children with spina bifida, addressing gaps in the literature that often overlook family perspectives and interdisciplinary strategies.
Design:
Qualitative study.
Setting:
Paediatric healthcare setting.
Method:
Based on a literature review, semi-structured interviews were conducted with seven family members/relatives of children with spina bifida, six physiotherapists, and six physicians specialised in paediatrics. Interview data were analysed using inductive reflexive thematic analysis.
Results:
We identified four key themes from interviews with family members and relatives: (1) the need for ongoing guidance from healthcare professionals; (2) the importance of organisational and conceptual support; (3) the value of empathetic interactions with healthcare providers; and (4) the desire for informed autonomy in decision-making and care. In addition, expert interviews revealed four themes: (1) the collaborative optimisation of structured education; (2) advocacy for specialisation; (3) recognition of relatives’ proactive information-seeking efforts; and (4) the relevance of empowerment and resilience.
Conclusion:
This study highlights the need for ongoing guidance for the families of children with spina bifida. By developing and disseminating comprehensive educational resources, fostering cooperation between healthcare professionals and clinics, and providing emotional support, healthcare professionals can enhance the well-being of families. Cultivating resilience through informed participation and compassionate care is key to empowering families to manage the challenges associated with the condition effectively.
Keywords
Introduction
Approximately one in every thousand pregnancies in Europe, totalling over 5,000 pregnancies annually, is impacted by neural tube defects, including anencephaly, spina bifida and encephalocele (European Commission, 2022). The global incidence of spina bifida ranges from 0.3 to 4 cases per 1,000 births (Sozialversicherung, 2016). Depending on the severity of the disease, the symptoms can vary from mild, barely noticeable neurological deficits to paraplegia and severe multiple impairments (Mayatepek, 2023).
To provide those affected and their families with the best-possible support and prevent comorbidities and early morbidity, interdisciplinary and ongoing medical care is essential (Psihogios et al., 2015). Furthermore, close collaboration with patients and families, as well as the development of individual coping and self-management strategies is of considerable importance (Lindsay et al., 2014; Psihogios et al., 2015). An increase in self-efficacy coupled with the growing confidence of children affected to achieve set goals and work towards them also play a major role in dealing with the illness (Lindsay et al., 2014). Comprehensive and easily understandable patient and family education provided alongside therapeutic and medical interventions is essential for this purpose (Lindsay et al., 2014; McPherson et al., 2020). This form of education can ensure that the families of children with a chronic condition are adequately informed to make autonomous decisions on health matters (LeBovidge et al., 2017).
If families possess a high level of knowledge regarding treatment options and their consequences, and they make well-informed conscious decisions in favour of or against specific measures, the likelihood of achieving expected success is greater than in cases where care and treatment are determined by others (LeBovidge et al., 2017). Despite the recognised importance of information and education in the therapeutic and medical care of patients and their relatives, there has been insufficient investigation into patient education for children affected by spina bifida and the education of their relatives. The aim of this study was to comprehensively explore satisfaction with family and patient education for children with spina bifida, considering the perspectives of family members and relatives, physicians and physiotherapists.
Methods
Design
To acquire a comprehensive understanding from relatives and experts (specialists for paediatrics and physiotherapists specialising in paediatrics) regarding satisfaction with family and patient education in children with spina bifida under the age of 13 years, we conducted a literature review and semi-structured qualitative interviews using reflexive thematic analysis (Braun and Clarke, 2006). Inductive coding informed by a critical realist ontology and a constructivist epistemology was used to understand interviewees’ subjective experiences and perceptions. The comprehensive consolidated criteria for reporting qualitative research (COREQ) were used to structure the study report (Tong et al., 2007).
Ethical approval and informed consent
This study was conducted in line with the principles of the Declaration of Helsinki and the principles of biomedical ethics outlined by Beauchamp and Childress (2009). The study was approved by the Ethics Committee of the Danube Private University Krems (reference: DPU-EK/004). Relatives and family member, physiotherapists and clinicians received both oral and written information about the study, with opportunities to ask questions. They were given ample time to consider their participation and were assured they could decline to respond or withdraw from the study at any point without affecting the treatment of their child or their professional roles. Written informed consent was obtained from all participants prior to their participation.
Sample
Although the study was conducted at a single clinic, family members and relatives were recruited through multiple channels, including through clinic staff, postings on relevant websites and private social media pages of self-help/advocacy groups, as well as through snowball sampling. Eligibility criteria for study participation of relatives included (1) being the direct relatives of children with spina bifida (age < 13 years); (2) speaking fluent German; and (3) not having any diagnosed cognitive deficits. Relatives and family members were excluded if their children with spina bifida had been diagnosed with any other neurological or psychiatric condition.
Physicians and physiotherapists with paediatric expertise were purposively recruited from clinics, rehabilitation centres and independent physiotherapy practices across Austria which treat children with spina bifida. For inclusion in the study, they needed to be fluent in German and possess a minimum of 7 years of professional experience in paediatrics, with a regular (⩾30 hours/year) commitment to caring for children with spina bifida and their families. This experience threshold was set to ensure participants had sufficient clinical exposure and expertise to provide reflective, practice-based insights. Theoretical saturation (i.e. when no new insights emerged from the analysis) informed the decision when to halt data collection (Saunders et al., 2018).
For qualitative studies of this kind, the inclusion of 6–12 participants is recommended (Guest et al., 2006). Seven family members and relatives (including one couple), six physicians and six physiotherapists were approached, agreed and interviewed to ensure a diverse range of insights.
Data collection
Literature search
A comprehensive literature search was conducted using Medline/PubMed, the Physiotherapy Evidence Database (PEDro) and the Cochrane Library, covering all records up to January 2021, to establish a foundation of existing knowledge. The aim was to explore key concepts related to caregiver satisfaction and patient education in the context of spina bifida. The search spanned November 2020 to January 2021.
Studies were eligible for inclusion if they (1) focused on children and adolescents up to 18 years of age; (2) addressed patient, family or caregiver education or information; and (3) were available in German or English. The search strategy and search results for each database are detailed in online Supplemental File 1.
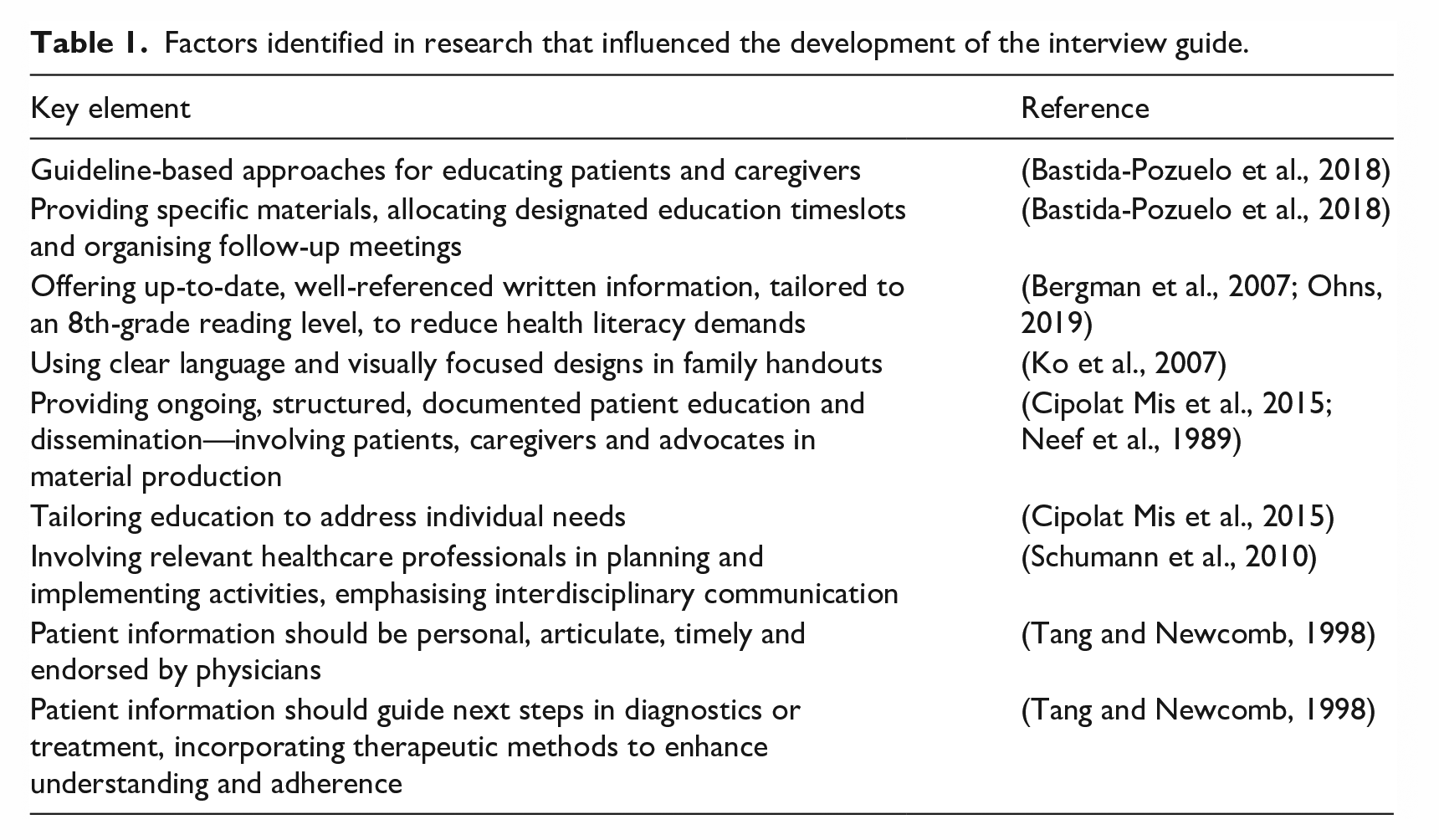
A total of 421 articles were initially identified. After removing duplicates, 378 records remained. Title and abstract screening led to the exclusion of 366 studies. The remaining 12 articles were assessed in full text, resulting in the exclusion of four that did not meet the inclusion criteria. Ultimately, eight studies were included in the final synthesis (Bastida-Pozuelo et al., 2018; Bergman et al., 2007; Cipolat Mis et al., 2015; Ko et al., 2007; Neef et al., 1989; Ohns, 2019; Schumann et al., 2010; Tang and Newcomb, 1998). See Figure 1 for a PRISMA flow diagram (Page et al., 2021). These studies informed the development of the interview guide (further information can be obtained from the corresponding author upon request), with key elements summarised in Table 1.
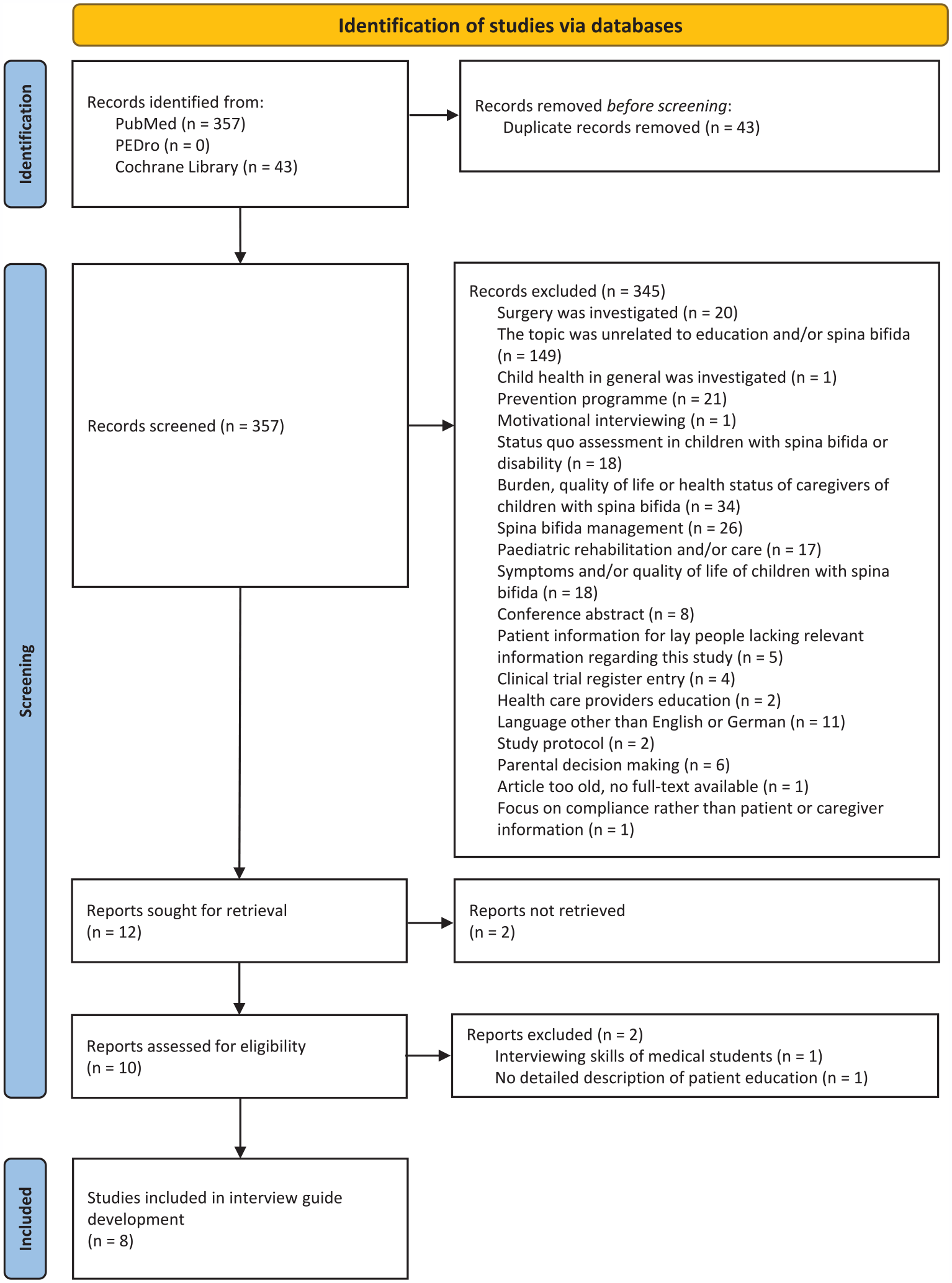
PRISMA 2020 flow diagram.
Factors identified in research that influenced the development of the interview guide.
Qualitative interviews
Between January and August 2021, semi-structured interviews were conducted with family members and relatives, physicians and physiotherapists. Participants chose in-person or telephone interviews at their convenience. A trained female physiotherapist-researcher (VW), supported by her academic supervisor (BS), conducted all the interviews.
Interview guides were piloted with additional interviewees, adjusted based on two interviews per group and primarily aimed to collect relatives’ experiences with spina bifida education and information. Several adjustments were made to enhance clarity, relevance and depth. Questions with technical language or medical jargon were rephrased for accessibility – for example, ‘Which other members of the multidisciplinary healthcare team are involved in delivering counselling, information or clinical care?’ was revised to ‘Which other professional groups were involved in providing counselling, information or care?’ Overly broad questions that risked surface-level responses were also reformulated to prompt more specific reflection on content, method, timing and delivery. For instance, ‘How should information about spina bifida be given to parents?’ was replaced with ‘Imagine you could design a way to send information on spina bifida to parents concerned: what would you tell them? How? Through which channels? At what point in terms of their child’s age?’ Additional prompts such as ‘Please elaborate on this’ and ‘Could you describe this a little further?’ were added to encourage richer responses.
Before the study began, the interviewer spent time establishing a relationship with the interviewees by asking about personal goals and reasons for conducting the research. Throughout, the use of open-ended questions facilitated a comprehensive exploration of participants’ experiences and knowledge. Field notes were taken, and audio recordings transcribed (Dresing and Pehl, 2018).
Data analysis
A reflexive thematic analysis informed by the work of Braun and Clarke (2006) was conducted by the three authors (VW, SM and BS) using f4analyse software (Marburg, Germany). To enhance reliability and validity, peer scrutiny and debriefing took place. Reflexive thematic analysis centres on engaging with and reflecting on data through a structured process comprising six phases of analysis (Braun and Clarke, 2006), aiming to identify consistent patterns of meaning. First, all transcripts were read and re-read to ensure deep familiarisation with the data. Initial codes were then generated inductively, identifying meaningful features across the dataset. These codes were organised into potential themes, which were subsequently reviewed for internal coherence and relevance to the research question. Themes were then refined, clearly defined and named to capture their central organising concepts. Finally, a written narrative was developed to illustrate each theme with data extracts, providing a coherent and interpretive account of participants’ experiences. Further details of the process of analysis are available from the corresponding author of the paper on request.
Findings
Seven relatives and family members (including one couple), six physiotherapists and six physicians (two paediatric urologists, one paediatric orthopaedic surgeon, one paediatric surgeon, one neurosurgeon and one neuropaediatrician) were interviewed. Participant characteristics are shown in Table 2. Interview duration ranged from 29 to 45 minutes.
Characteristics of the relatives, physiotherapists and physicians.
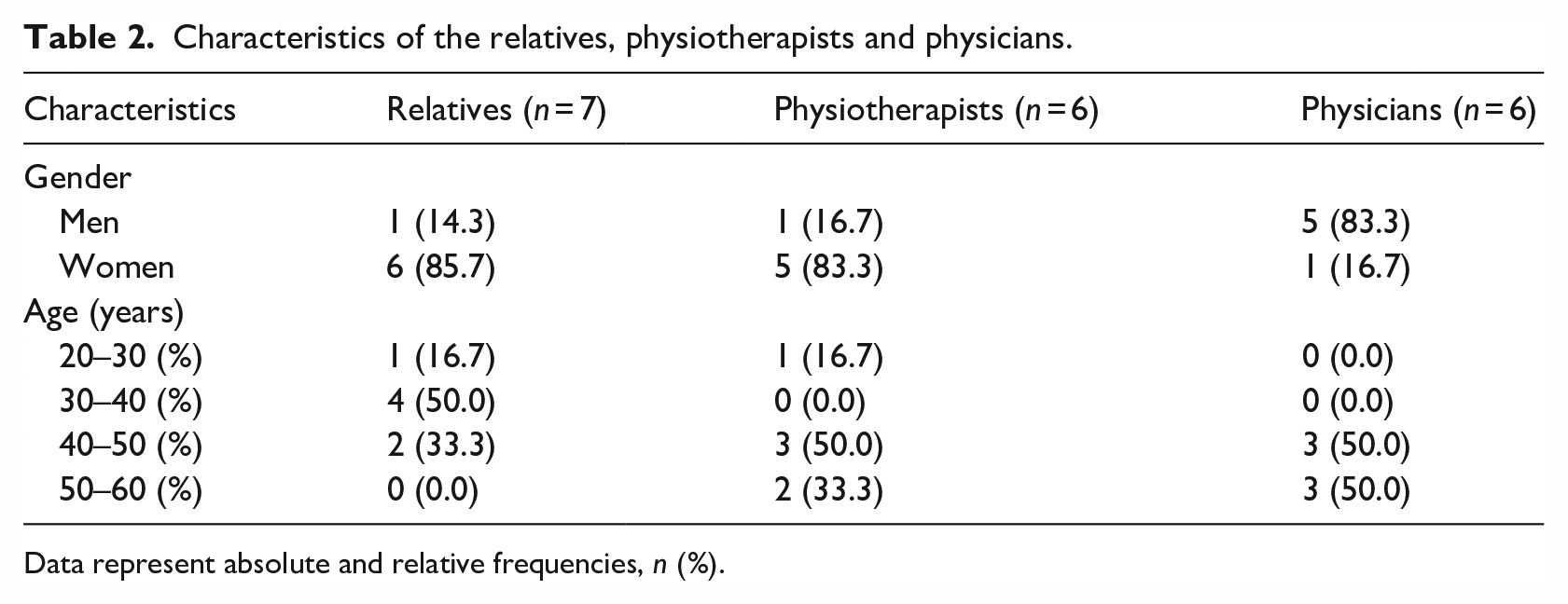
Data represent absolute and relative frequencies, n (%).
Analysed interview data from relatives led to the identification of four themes. No clear patterns related to gender or age were present in the data. Participants’ perspectives appeared to be shaped more by their experiences and roles than by demographic characteristics. Physiotherapists and physicians showed substantial convergence in codes and concepts. Four overarching themes were developed for both expert cohorts during theme development.
While perspectives varied between relatives and experts, overlapping patterns were identified in some aspects across both groups. A thematic map of the findings is presented in Figure 2. A fuller description of themes and quotes is provided in online Supplemental Files 2 and 3.
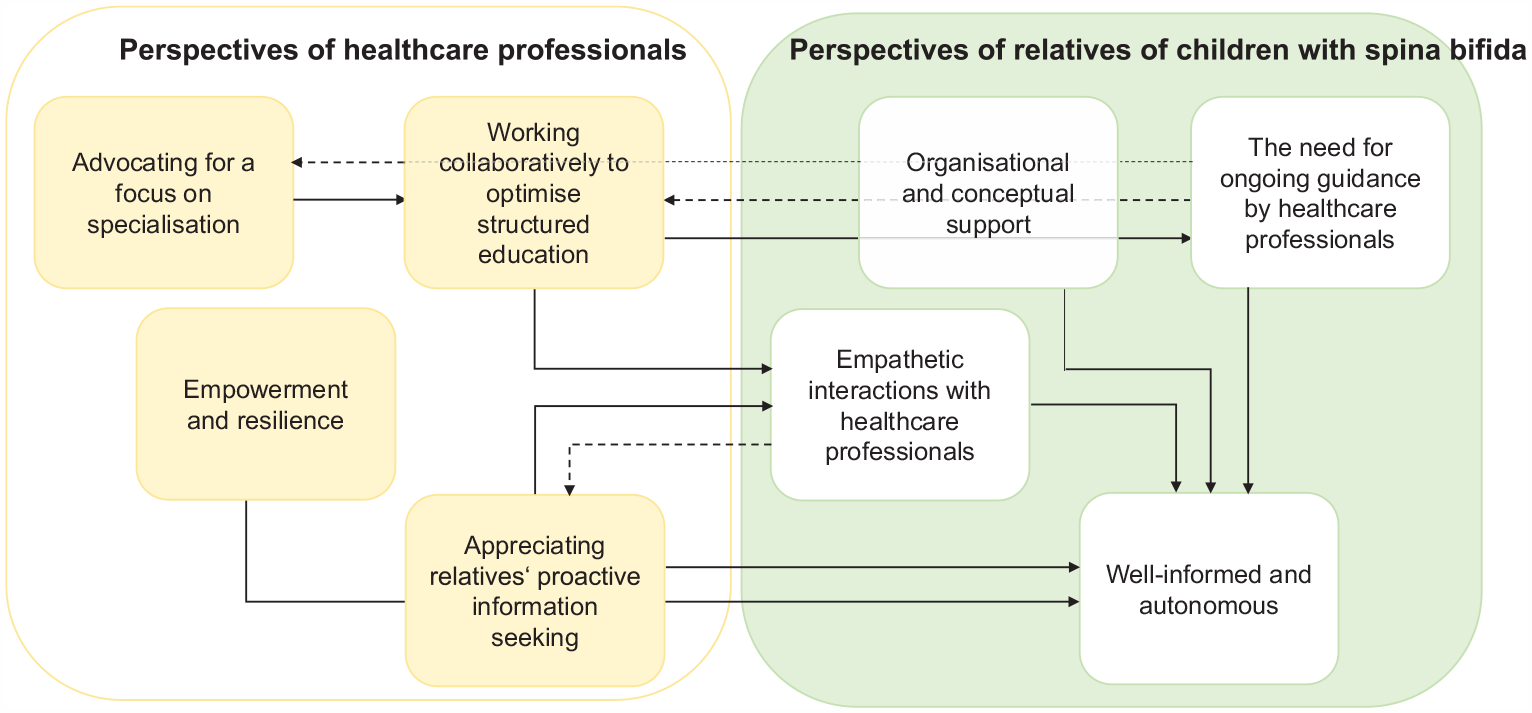
Thematic map.
Relatives’ perspectives
Theme 1: The need for ongoing guidance by healthcare professionals
Well-structured hospital stays, consistent close monitoring and education provided by healthcare professionals were seen as positive by relatives. However, relatives missed guaranteed ongoing health information and care at home, especially for children with specific needs. Support services for families affected by the condition were considered limited and not extending to siblings. Furthermore, integrating children with spina bifida into kindergarten and school was regarded as challenging without dedicated information about how best to achieve this goal.
Theme 2: Organisational and conceptual support
The lack of a systematic approach to providing information was evident in the experiences of families where there was a child living with spina bifida. Carers had frequently to take the initiative to find relevant services and information. YouTube channels were seen as a valuable source of visual information. However, there was a need for more comprehensive and detailed educational materials tailored for children with spina bifida. In terms of therapy, the desire was expressed for easily implementable recommendations that could be incorporated into daily life. Enhancing coordination and planning between professionals caring for children with spina bifida could ensure timely access to crucial medical and social services. Relatives expressed the desire for more open communication, networking between specialised centres and referral to other specialists when necessary. Having a consistent main contact person to provide support and structure for families was also seen as valuable. There was a clear desire for closer collaboration between medical professionals and families to enable both to find solutions together.
Theme 3: Empathetic interactions with healthcare professionals
While some initial consultations and explanations were challenging due to a perceived lack of empathy from professionals, relatives also had deeply supportive and empathetic interactions with paediatricians. They emphasised the importance of being taken seriously, listened to attentively and seen as valued participants in their child’s care by medical staff, and having patient education tailored to their situation. Empathy from healthcare professionals was a significant uplifted otions. Participants shared that counselling could be improved and highlighted the need for support that extended beyond medical expertise and focused on strengthening the family. Despite the challenges, relatives consistently perceived the quality of life (QoL) of the children as good. One participant noted their child’s positive progress and expressed the desire to include information about the potential for a good QoL in patient materials for relatives.
Theme 4: Well-informed and autonomous
Sharing experiences with other relatives provided a source of strength. The mutual exchange of information was seen as highly beneficial. One participant highlighted the transformative impact of connecting with other mothers. Apart from information exchange, self-help groups also offered the opportunity to provide support to new families facing similar challenges. Another participant voiced a positive experience, valuing other families that shared a lot of helpful information and provided them with the opportunity to get to know other parents facing similar situations. One participant reflected on the learning process, noting that parents often searched for information about the congenital condition independently, primarily online. Face-to-face meetings were frequently supplemented by digital communication and resources. Relatives indicated that when seeking information about procedures from medical doctors, they were frequently required to seek multiple opinions, and it brought great relief when several of them aligned with the same advice. Online Supplemental File 2 provides example quotes from interviews with relatives.
Experts’ perspectives
Theme 1: Working collaboratively to optimise structured education
Experts described various strategies and materials that could be used to educate families affected by spina bifida. Some clinics used a formal approach, assigning responsibilities to specific members of staff to educate parents on medical fundamentals and the congenital nature of the condition, particularly with respect to urology, future prospects and managing expectations. However, a marked discrepancy was highlighted. While education was often delivered in an ad hoc, individualised manner, the scheduling of key medical appointments followed a well-defined structure. Despite the absence of an agreed-upon unitary approach, a strong emphasis was given to interdisciplinary cooperation and professional exchange. In addition, the use of printed educational materials was highlighted, with some clinics undertaking steps to ensure adequate education for both relatives and affected children. Efforts were ongoing to improve educational materials and incorporate digital resources as part of broader educational offerings. To prevent overwhelming parents, especially on sensitive issues, it is crucial to allocate ample time for education to take place. As parents frequently attend medical appointments particularly with small children, education can occur concurrently, with a gradual transition of information provision to older children.
Theme 2: Advocating for a focus on specialisation
Professionals involved in healthcare training pointed out a lack of practical focus, which was particularly difficult for those new to the field. Experts highlighted the transition to adulthood as particularly challenging for the care of individuals affected by spina bifida. They suggested that this was partly because the effort required was high, while the outcomes are often limited. A key concern was the amount of time needed to gain expertise in spina bifida care, which could make it difficult to provide suitable adult healthcare. Experts agreed that specialised departments were needed to ensure lifelong care and educational support. They also stressed the importance of strong networks between clinics to improve care quality. However, some noted that setting up specialised centres could be difficult due to the low incidence of spina bifida, which also makes counselling centres uncommon.
Theme 3: Appreciating relatives’ proactive information seeking
Family and relatives’ proactive gathering of information was appreciated by the experts consulted and showed recognition of the initiative they had taken even if it could sometimes pose challenges for medical staff to respond to. The active involvement of relatives in engaging with a congenital condition and delivering therapy and care at home was seen as advantageous for the development of affected children. The close emotional and relational connections between relatives and affected children with spina bifida were considered especially significant, with respect to both affective bonds and the practical demands of ongoing care delivery. Self-help groups were seen as playing a vital role in providing crucial support for both affected children with spina bifida and their families and relatives, complementing the services offered by health and medical facilities.
Theme 4: Empowerment and resilience
In addition to managing care relating to spina bifida, experts observed that relatives often found themselves having to deal with social stress. Beyond medical appointments and various kinds of surgery and other interventions that could sometimes lead to complications, experts emphasised that the most significant challenges for those affected were the social aspects of living with spina bifida. Families and individuals affected by the condition welcomed being well-informed when making medical decisions, as well as the ability to lead an independent life. Despite the challenges and obstacles described, experts observed a good QoL among those affected. Experts noted an extraordinary level of resilience among children with spina bifida. They acknowledged that good-quality patient and family education could empower patients and families by providing them with the means to handle stress and uncertainty. Experts considered it remarkable how patients could endure serious challenges while maintaining a sense of positivity about life. The social and psychological struggles faced by children with spina bifida frequently outweigh the physical challenges they encounter. Online Supplemental File 3 provides some example quotes from the interviews with physiotherapists and physicians.
Discussion
In this study, we explored satisfaction with family and patient education for children with spina bifida, gathering insights from relatives, physicians and physiotherapists. Our findings reveal a lack of systematic information available to families, consistent with previous research highlighting deficiencies in educational programmes relevant to children with rare chronic conditions (Fisher, 2001; Menrath et al., 2019). There is a need for coordinated efforts across the education, social care and healthcare sectors to provide individualised support that addresses both medical and social needs (Gaintza et al., 2018).
Relatives stressed the importance of timely education, structured hospital stays and consistent medical monitoring, while noting challenges in ongoing home care with varying levels of support. They called for better communication, more coordinated networking between specialised centres and greater collaboration between medical staff and families, as reflected in current spina bifida care coordination guidelines (Speybroeck et al., 2020). Research suggests that education programmes, led by both professionals and parents, can enhance self-efficacy and improve management of the child’s condition and family well-being (Kieckhefer et al., 2014).
The relatives of children with spina bifida expressed the need for educational materials tailored specifically for their condition, highlighting the importance of thorough and conceptually robust support. Consistent with findings from a systematic review (Fisher, 2001), they stressed the importance of being taken seriously, listened to attentively and valued in delivering their child’s care, while receiving personalised medical information. Consistent advice from multiple medical professionals provided reassurance to parents seeking information, linking their desire for reliable information with a longing for normality and certainty despite negative experiences.
Our findings highlight how sharing experiences in self-help groups can be a valuable resource for families of children with spina bifida, fostering strength and resilience. This aligns with other studies showing that self-help groups and rare disease associations can offer psychological and emotional support, raise public awareness, promote social visibility and connect families with specialised care (Gaintza and Darretxe, 2023; Litzkendorf et al., 2020). In addition to offering efficient, cost-effective access to information, they have been shown to provide meaningful opportunities for mutual exchange and support (Litzkendorf et al., 2020). Similarly, research has demonstrated that self-management programmes led by lay counsellors – trained individuals without formal mental health credentials – can be as effective as those delivered by professionals (Barlow et al., 2002).
Peer support, whether structured or informal, in groups or one-on-one, has also proven valuable (Anderson et al., 2013; Hemming et al., 2025). However, a systematic review found no existing studies of peer support specifically for families of children with spina bifida (Levy et al., 2019), and notable gaps remain in the literature regarding self-management support for children, young adults and carers (Anderson et al., 2013). Confirming recent findings (Mardhiyah et al., 2022), we found that prioritising participation and independence often led to a satisfactory QoL for those with spina bifida, despite social stress and often serious medical interventions. Relatives voiced concerns about the lack of systematic information provided to them, relying on own initiative and platforms like YouTube. Existing literature highlights the need for high-quality educational content (Arpa and Aydin Ozturk, 2023), which is accessible and comprehensible even with language barriers (Çiftci et al., 2023; La Scala et al., 2022; Sax et al., 2019).
Experts highlighted the need for structured educational strategies to support families dealing with spina bifida, noting the lack of universal guidelines. While some clinics adopted interdisciplinary and organised approaches, there was agreement on the importance of specialised departments offering lifelong care and education. Effective collaboration between clinics, coordinated care and clear communication protocols was also stressed. A lack of practical focus in healthcare training was seen as particularly difficult for newcomers. Our findings reflect existing research on the challenges of spina bifida care, especially during the transition to adulthood, and reinforce the value of multidisciplinary support for adolescents (Reynolds et al., 2023) and gradual, tailored education for families (Beierwaltes et al., 2020a; Beierwaltes et al., 2020b; Wilson and Mukherjee, 2020).
Findings from this study highlight the need for healthcare systems to prioritise extending information and care beyond the hospital, ensuring that families receive consistent support. Gaps in family and patient education and service delivery can be addressed by fostering cooperation between healthcare professionals and clinics. Both relatives and experts highlighted the importance of empathy and active listening. Healthcare providers should aim to offer compassionate, holistic care that goes beyond medical treatment. Integrating emotional support and professional counselling into services can help strengthen family dynamics and promote long-term well-being.
We acknowledge that there may be barriers to bringing about the changes identified earlier. Such barriers include limited personnel resources and time, insufficient communication and collaboration between service providers and the fact that mental health and emotional support are often not prioritised as part of care. Other challenges may include disengaged or uninvolved relatives and family members, relatives’ negative prior experiences with healthcare professionals or the healthcare system, lack of training and experience among professionals, unclear interdisciplinary boundaries and high staff turnover – as highlighted in a recent mixed-methods study of mental health services for children and youth with neurodevelopmental disabilities and their families (Heslon et al., 2024). Additional barriers identified in two systematic reviews include difficulties and power imbalances in doctor–patient relationships (Joseph-Williams et al., 2014; Légaré et al., 2008). For example, overly rigid clinical processes, entrenched practice norms and limited time may make it difficult to integrate family education into care pathways that support shared decision-making (Boland et al., 2019). Such practice norms may reflect cultural expectations that healthcare professionals should provide specific recommendations or make decisions on behalf of patients and families. Moreover, implementing peer support can be challenging due to difficulties in recruiting suitable peer workers and the need to ensure their well-being through high-quality training and support. This is essential not only to protect against burnout but also to ensure the long-term sustainability of such work (Hemming et al., 2025).
The proactive role of family and relatives in seeking information and participating in care activities at home can be immensely beneficial for children with spina bifida. Experts acknowledged and valued this, noting that it can significantly contribute to the child’s development. Self-help groups and peer support networks offer crucial emotional and practical support, complementing medical services. Despite facing numerous challenges, families and individuals with spina bifida exhibit remarkable resilience and positivity, qualities that can be further strengthened through education and encouragement from healthcare professionals. Recognising and fostering this resilience is vital, suggesting that families need to be informed and actively involved in decision-making to promote independence and strengthen their capability to manage their child’s condition.
Limitations
This study has several limitations. First, the potential for recall bias and socially desirable responses is recognised, although steps were taken to mitigate these biases, including establishing rapport and trust, framing questions within specific timeframes and using prompts related to significant events to aid in accurate recall. Second, there was a gender imbalance, with 12 of the 19 participants being female (63.2), in line with international studies of willingness to participate in research (Otufowora et al., 2021). In contrast, five of the six physicians were male. Finally, while member checking did not occur, rigorous checks on the consistency of the data were conducted by multiple researchers. Despite these limitations, we believe our study offers valuable insights into family and patient education in spina bifida.
Conclusions
In this study, the relatives and family members of children with spina bifida appreciated structured hospital stays and consistent education from healthcare professionals but desired ongoing health information and support at home in relation to their children’s unique needs. They highlighted the importance of comprehensive educational materials and better coordination between medical staff and families. Relatives reported receiving varying levels of support and empathy from healthcare professionals and maintained a positive outlook on their children’s QoL, advocating for holistic support through the informed sharing of experiences. Experts recommended joint approaches to educate families, emphasising the use of printed materials and integrating education into successive medical appointments to avoid overwhelming them. They noted the challenges of transitioning children into adulthood and stressed the need for ongoing care and education support. Families saw informed participation in medical decision-making as very important both for themselves and for their children, especially when they entered young adulthood and sought the ability to live independently. Experts recognised that effective education could empower families and build resilience by equipping them with skills to manage stress and uncertainty. While our findings highlight some gaps in family and patient education for children with spina bifida, we acknowledge the limitations of this small-scale qualitative study and stress the importance of high-quality follow-up research to advance knowledge in this field.
Supplemental Material
sj-docx-1-hej-10.1177_00178969251364963 – Supplemental material for Family and patient education for children with spina bifida: A qualitative study
Supplemental material, sj-docx-1-hej-10.1177_00178969251364963 for Family and patient education for children with spina bifida: A qualitative study by Verena Wutzlhofer, Sarah Mildner and Barbara Seebacher in Health Education Journal
Footnotes
Acknowledgements
We thank the relatives, physicians and physiotherapists who participated in this study.
Data availability statement
Due to the sensitive nature of interview data, full transcripts from this study are not publicly available. However, interested researchers can request access to anonymised excerpts of these by contacting the corresponding author. Access will be contingent upon ethical approval and agreement to a data-use policy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.