
Abstract
Background:
Recovery Colleges offer an educational approach to personal recovery within mental health services. Fundamentally, course design and delivery incorporates co-production via collaboration between practitioner and peer trainers.
Objective:
What guidance, training and support have been provided for peer and practitioner trainers who participate in the design and delivery of Recovery College courses?
Method:
A scoping review was conducted using Ovid, Embase, PsychoInfo, PsycArticles, HMIC, Global Health, Cochrane, Social Policy and Practice databases. Data were summarised using descriptive analysis focusing on themes including individuals’ experience of co-production, training, guidance and support provided to co-produce courses within the Recovery College setting.
Results:
Of the initial 360 articles identified, 19 met the study inclusion criteria. Across the articles, co-production was recognised as beneficial for those involved. The identified themes were collaborative experience, training, guidance and support provided for trainers co-producing Recovery College education.
Conclusion:
This scoping review highlighted the limited training, guidance and support provided to those participating in co-production of Recovery College education.
Background
Recovery Colleges opened in England in 2009 to offer an educational approach to personal recovery in mental health. They have been recognised as a transformative method for change within mental health services (Shepherd et al., 2010). Co-production is considered to be one of the fundamental components established within Recovery Colleges, at all development and delivery stages of both the organisation of Recovery Colleges themselves and the courses they provide (Perkins et al., 2012). This scoping study explored how the peer-reviewed published literature on Recovery Colleges has accounted for the guidance, training and support provided for peer and practitioner Recovery College trainers.
Defining co-production
Co-production within mental health practices, policies and literature is portrayed as ‘doing with’ rather than ‘doing to’ or ‘doing for’ mental health service users (Slay and Stephens, 2013). It has been defined as a paradigm shift required within mental health services for culture change and the sharing of the role of leadership and decision-making process (Minghella and Linsky, 2018). Co-production aims to achieve positive change by connecting and empowering people by valuing and utilising their contributions (Department of Health, 2018). The development of co-production draws upon historical progress in the mental health service user movement and the recognition that services provide optimal care when those using them are closely involved in their development and delivery (National Survivor Use Network, 2024).
Co-production and Recovery Colleges
Recovery Colleges were set up to support mental health recovery through learning and education collaboratively developed by those with lived experience and individuals from a professional background. They are non-clinical spaces where the focus is on mental health promotion through education rather than clinical treatment. Recovery Colleges staff and volunteers are a combination of those with ‘professional expertise’ (practitioner trainers) and those with ‘lived experience’ (peer trainers), or sometimes both (Perkins et al., 2012). Students at Recovery Colleges can be service users, carers and staff who wish to explore mental health recovery principles and practices (Perkins et al., 2012). Across accounts of Recovery College establishment in 22 countries one of the emergent common themes was the importance of co-production (King and Meddings, 2019). When the characteristics of Recovery Colleges were compared across the United Kingdom, students stated the most prevalent feature was co-production, including subthemes of quality, experience and expertise and course planning as an aspect of the course strategy and approach (Anfossi, 2019). This indicates that co-production is not only a feature of the course delivery but is also present in design, quality assurance and the wider expectations of what Recovery Colleges do and how they function.
Mechanisms of co-production within Recovery Colleges
Co-production is characterised by equal, respectful and productive relationships between those seen making decisions and those affected by decisions (Rethink, 2015). This collaboration aims to shift the usual power dynamic found in mental health care and treatment and in educational settings, by utilising strengths, supporting participation and fostering engagement between services and service users. In theory, this ought to embed equality between those providing and using services, but without guidance, the process can be missing important stages or features, resulting in tokenism due to the lack of understanding of the complexity of co-production (Roper et al., 2018). The mechanisms of how Recovery College members move from doing to (coercion) to doing with (co-production) requires exploration (Slay and Stephens, 2013).
Slay and Stephens (2013) formulated a set of principles to maintain co-production standards, including suggestions for blurring role distinctions, recognising assets and sharing skills. These principles permit flexibility and the organic materialisation of a relationship within co-production rather than defining instructions for how it should be done. Their principles reflect that a single way of doing co-production loses authenticity as, like the ethos of mental health recovery, the aim is for a unique transformative experience with a foundation that recognised the sharing of experience and responsibility as the catalyst for change (Lewis et al., 2017). However, those new to Recovery Colleges and co-production will likely benefit from guidance regarding how to make it work for them, in their unique circumstances.
Given the proliferation of Recovery Colleges and the acknowledgement of co-production between people with lived and clinical experience in the design, delivery and participation in such settings, there is a need for a detailed understanding of how co-production is enacted within such settings. This scoping review explores the evidence of what and how Recovery College trainers have been guided or trained to co-produce.
Methodology
A scoping review was conducted to explore co-production within Recovery Colleges using a methodology framework to map and synthesise all available literature and a range of sources (Arksey and O’Malley, 2005) and checked against the PRISMA-ScR equator guidelines (Tricco et al., 2018).
Defining the research question and objective
The review engaged with one over-arching question:
What guidance, training and support have been provided for peer and practitioner trainers who participate in the design and delivery of Recovery College courses?
and one objective:
To identify examples of training, guidance and support available to inform the co-production process within Recovery Colleges.
Study selection
Our search focused on the experience of the peer and practitioner trainers rather than the students’ experience, as this paper aims to look at how to support the co-production process for trainers in adult Recovery Colleges.
Interpretation and synthesis
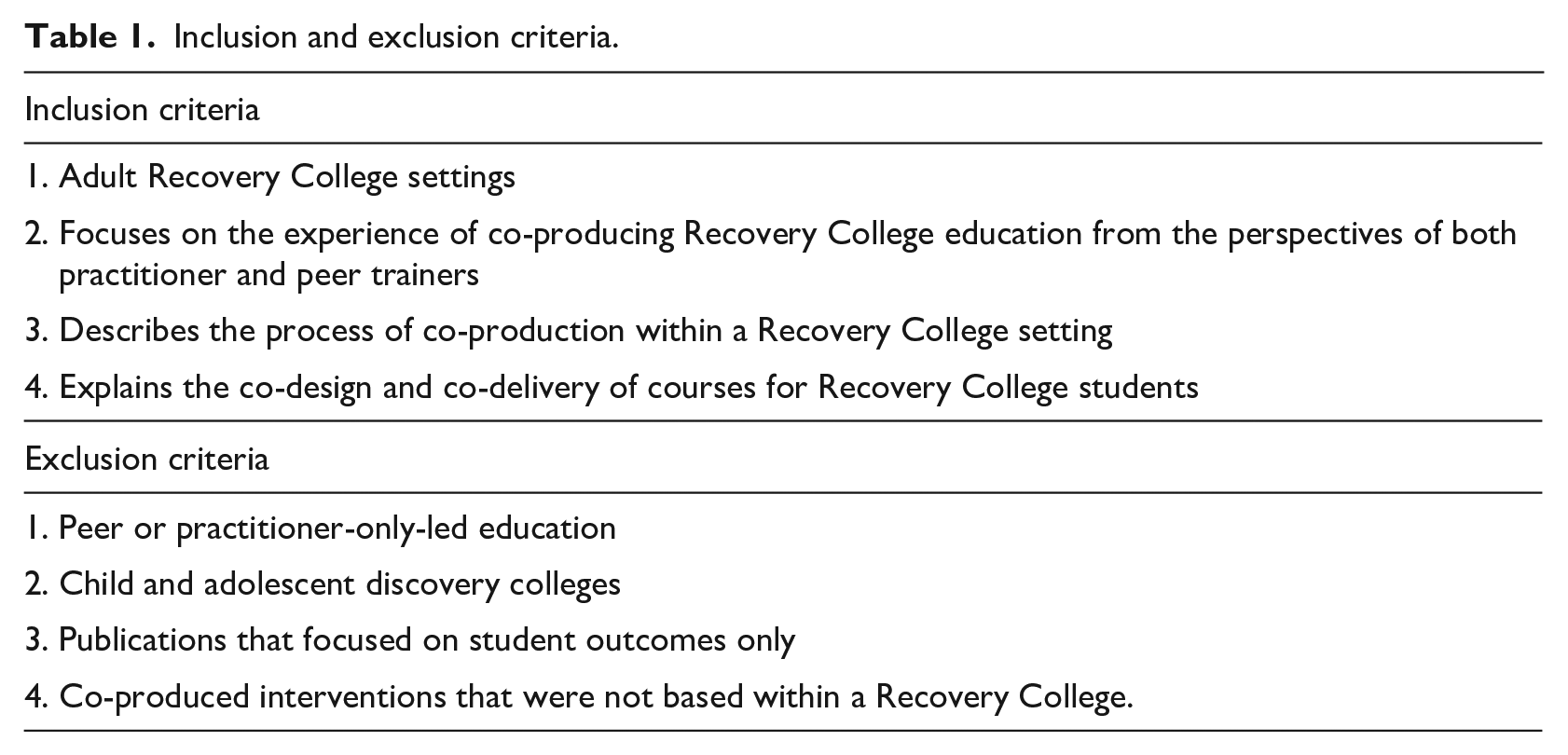
Eligibility was determined by inclusion and exclusion criteria (see Table 1), for example, the removal of articles that focused on student experience without discussing co-production, peer or practitioner-only training and psychoeducational or clinical intervention co-produced but not based in Recovery Colleges.
Inclusion and exclusion criteria.
Participants
Participants were comprised of Recovery College ‘peer trainers’ (recruited due to having experience in mental health recovery) and Recovery College ‘practitioner trainers’, who are clinicians with multi-professional mental health service background, including nurses, occupational therapists, social workers, psychiatrists and psychologists. Some of the articles also included participants who self-defined as carers for those using mental health services, and they also came under the title of peer trainers, given they are drawing on lived experience.
Concept
The papers include peer and practitioner trainers who had co-produced courses for Recovery College adult students. In the ethos of Recovery Colleges, courses are delivered to a student group that may include a combination of service users, carers, supporters such as volunteers, and mental health service providers, as co-learning is a component of recovery education.
Context
The courses were delivered in a Recovery College, mainly within statutory mental health services. Recovery Colleges differ in remit, size and target population since each has developed within a specific context and in its own way. The review only includes papers where the site was described as a Recovery College and focusing on adult mental health recovery courses and structures that fitted the criteria stated in the published guidance for Recovery Colleges (Perkins et al., 2012).
Search
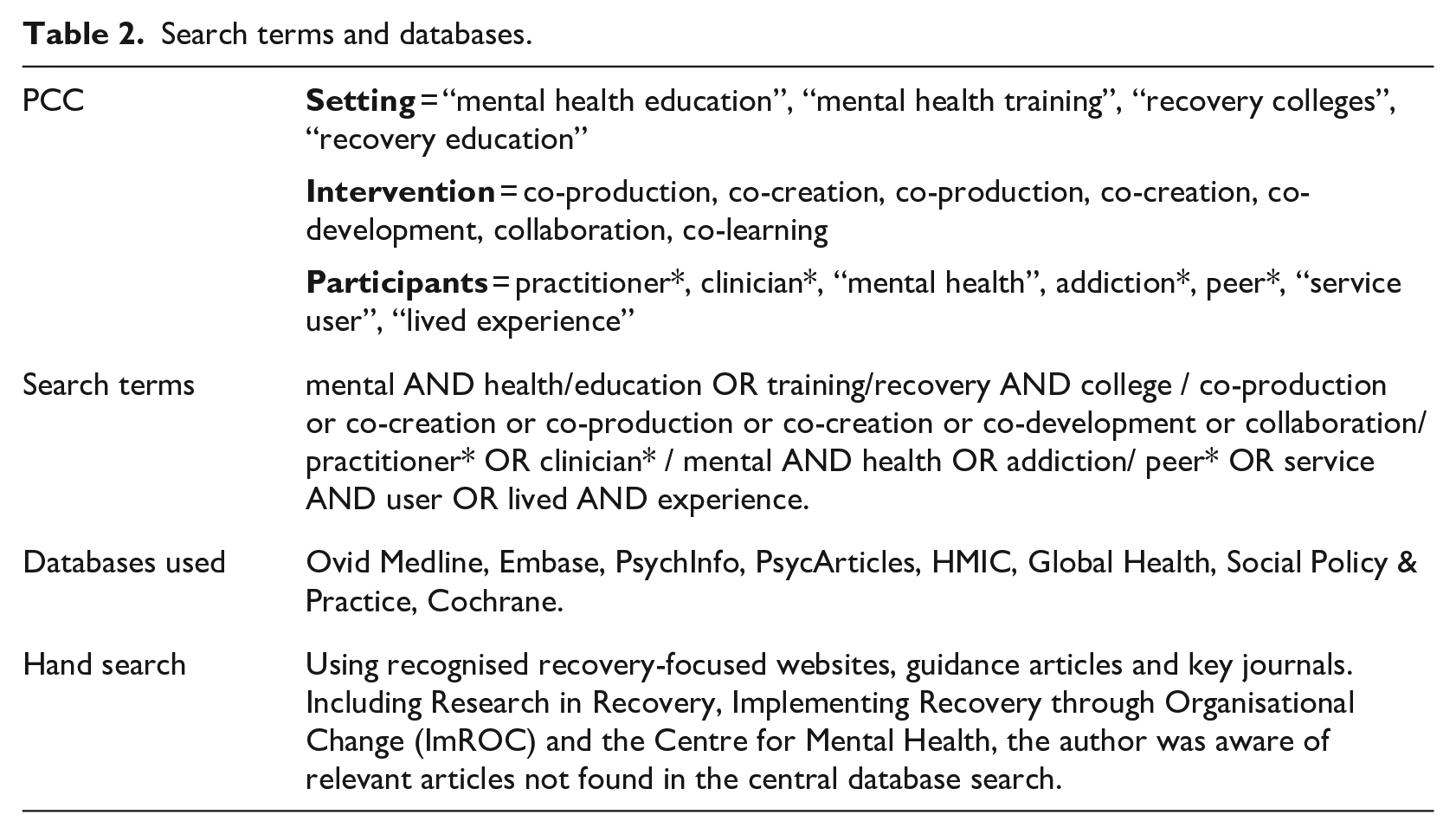
The search was conducted by the lead author between 2022 and 2024 and based on piloted searches and keyword phrases used in the principal publications centred on Recovery Colleges and co-production (see Table 2).
Search terms and databases.
Summarising and reporting
Articles were subjected to descriptive analysis focusing on themes including individuals’ experience of co-production, training, guidance and support provided to co-produce courses within the Recovery College setting. Recommendations were generated in line with the key findings and gaps identified in the literature.
Results
The search resulted in 360 articles between 2014 and 2023. Recovery Colleges launched in 2010; hence research has only been available since their inception. Following an abstract review against the inclusion and exclusion criteria, a total of 19 articles were identified as eligible for review (Figure 1).
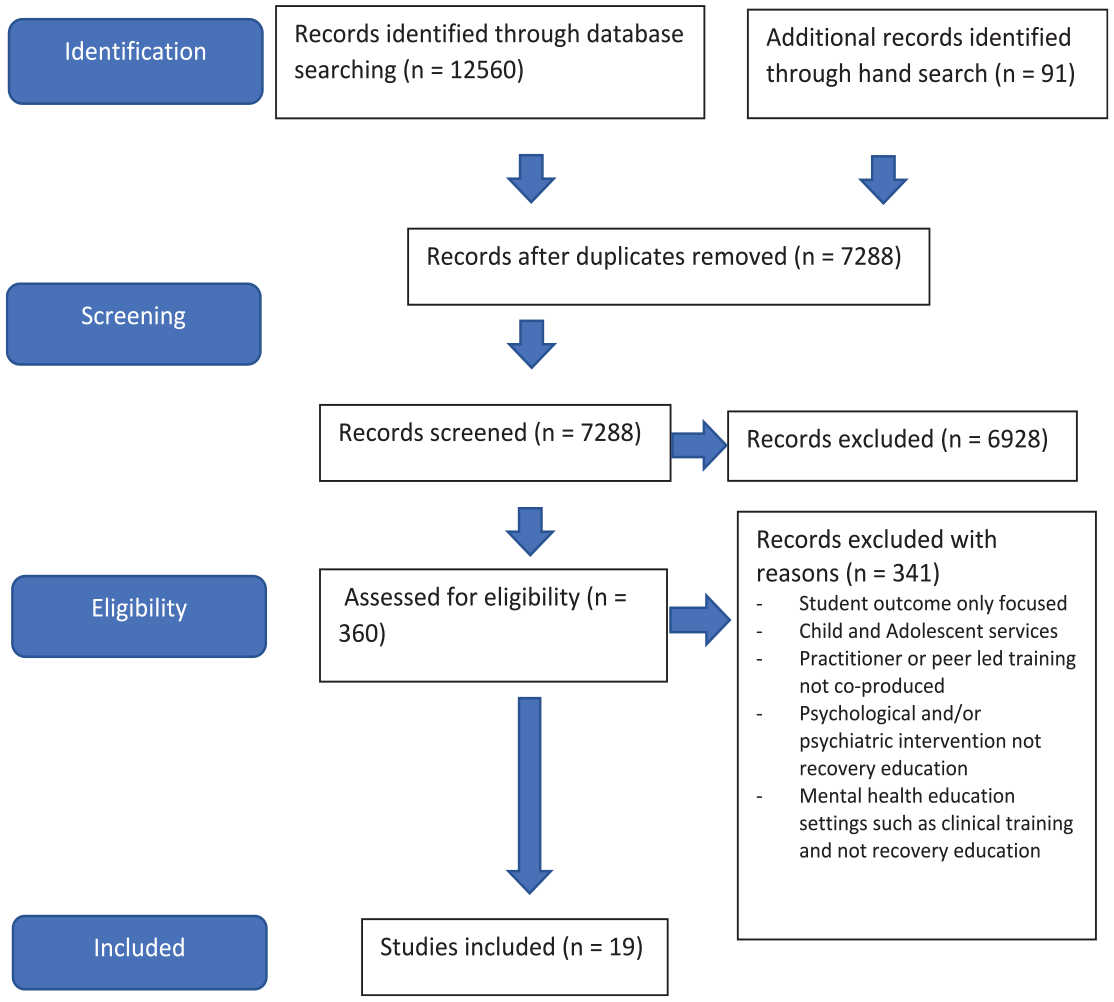
Preferred reporting items for systematic reviews and meta-analysis (PRISMA).
Characteristics of included articles
The search resulted in 19 articles which used the following research designs: mixed methods (n = 3) (Crowther et al., 2019; Doroud et al., 2024; Kay and Edgley, 2019), qualitative studies (n = 8) (Ali et al., 2022; Cameron et al., 2018; Dalgarno and Oates, 2018, 2019; Gill, 2014; Toney et al., 2019; West et al., 2022; Whish, 2021), case studies (n = 5) (Lewis et al., 2017; Meddings et al., 2014; Morgan et al., 2018; Perkins et al., 2012; Pledger, 2018), quantitative studies (n = 1) (Hayes et al., 2023), literature reviews (n = 1) (Bester et al., 2022) and a scoping review (n = 1) (Lin et al., 2023).
One study had a sample size (n = 1) but met the study eligibility criteria as it provided a transparent reflection on the peer trainer’s experience of co-production (Pledger, 2018). The largest sample size (n = 82) was present in a Recovery College pilot andincluded educators and staff, students, supporters and external stakeholder participants with some identifying (n = 23) as having more than one role (Doroud et al., 2024). Two articles used the same sample (n = 8), but did so to report on different data and findings, with one focusing on the meaning of co-production, while the other explored the process of collaborative working (Dalgarno and Oates, 2018, 2019).
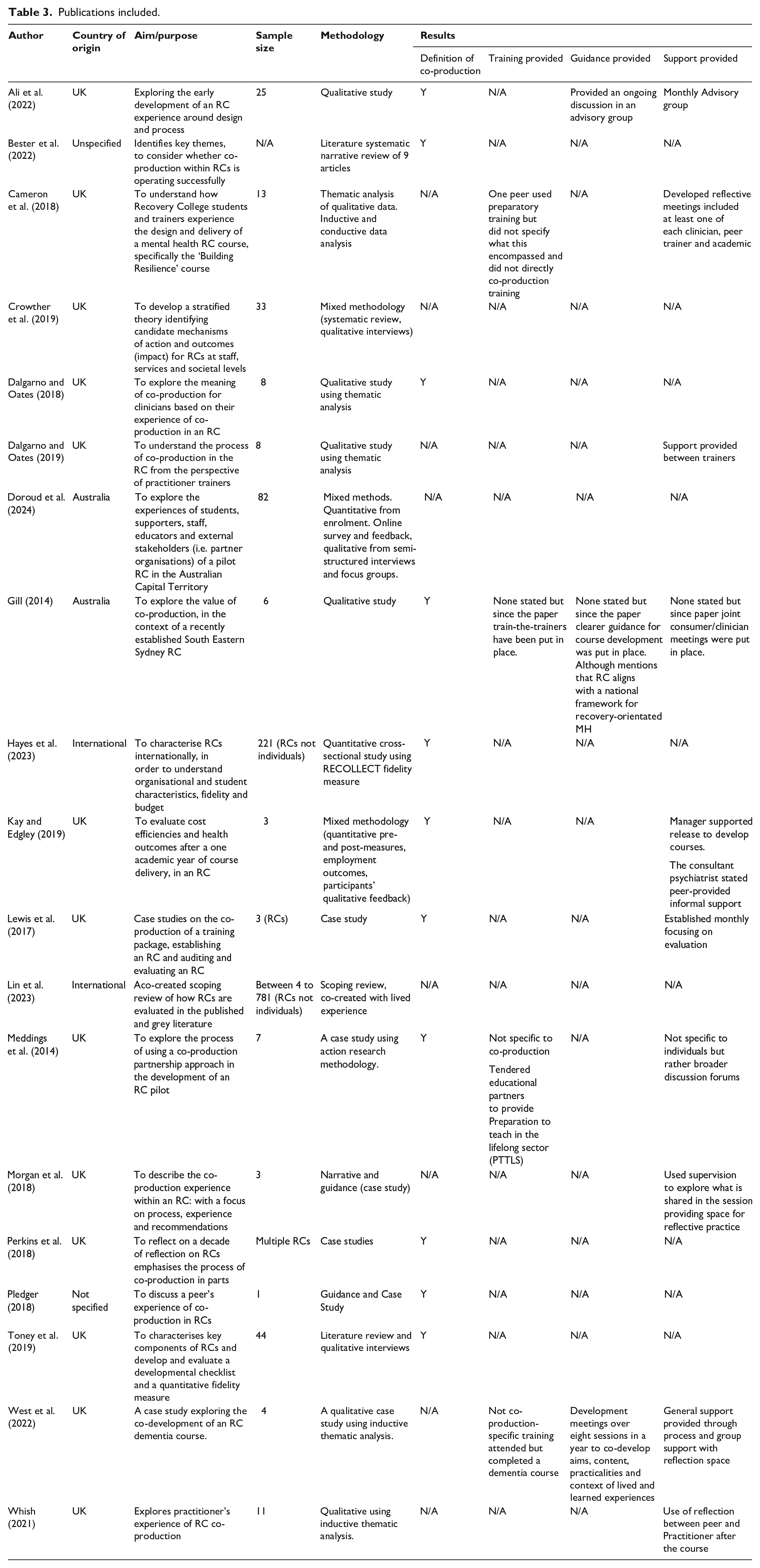
The majority of the articles were from the UK (n = 13) with others from Australia (n = 2). Two articles combined data from a variety of international Recovery Colleges with one including information from Africa, Asia, Oceania, Europe, North America and England (n = 1) and the other from Australia, the USA, Canada, Italy, Ireland and the UK (n = 1). Two articles had unspecified origins of data collection (n = 2). The details and findings from each paper are shown in Table 3.
Publications included.
Characteristics of co-production collaboration
A few articles focused only on the co-production experience of practitioner trainers (n = 3; 16%) (Dalgarno and Oates, 2018, 2019; Kay and Edgley, 2019), or of peer trainers (n = 2; 11%) (Meddings et al., 2014; Pledger, 2018). Other articles reported on a combination of participants’ co-production experience, for example, practitioner and peer trainers (n = 4; 21%) (Bester et al., 2022; Morgan et al., 2018; West et al., 2022; Whish, 2021), or peer trainers, practitioner trainers and students receiving the training that was co-produced (n = 7; 37%) (Ali et al., 2022; Cameron et al., 2018; Crowther et al., 2019; Doroud et al., 2024; Gill, 2014; Perkins et al., 2018; Toney et al., 2019). A cross-sectional study involving different Recovery Colleges, examined fidelity, characteristics and evaluation (n = 2; 11%) (Hayes et al., 2023; Lin et al., 2023), and another one was unspecific (n = 1; 5%) (Lewis et al., 2017).
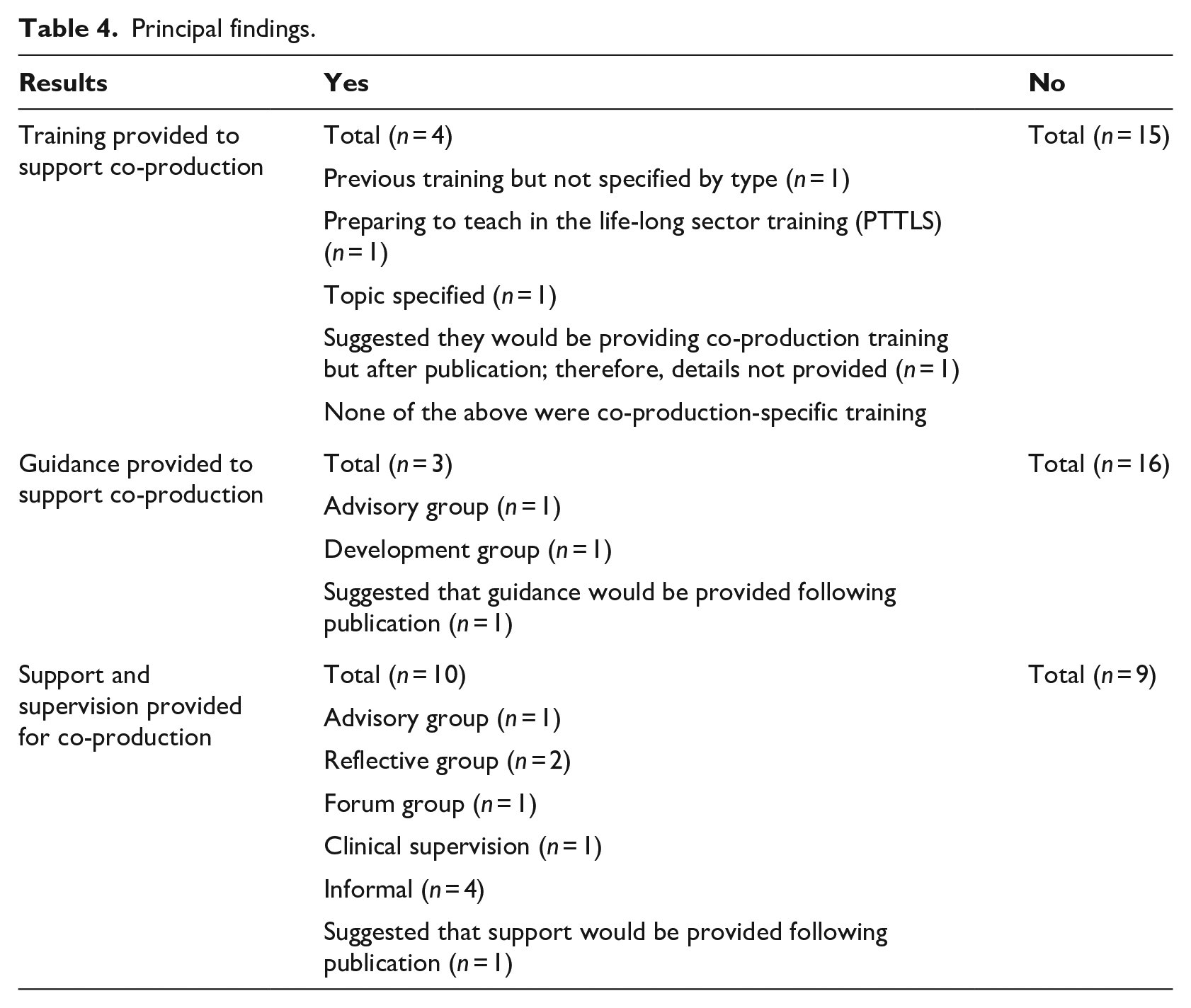
Data exploring co-production definitions, training, guidance and support is summarised by category in Table 4.
Principal findings.
Identifying examples of training, guidance and support available to inform the co-production process within Recovery Colleges
The articles were searched to find any practical examples of training, guidance and/or support provided for practitioner and/or peer trainers to enable them to co-design and co-deliver training within Recovery Colleges.
Co-production training
There was widespread recognition that practitioners and peers were unprepared for co-production work when commencing their Recovery College roles, with clinicians in particular voicing the need for both individual and mandatory workforce training on co-production (Bester et al., 2022; Doroud et al., 2024; Gill, 2014). It was said that ‘the co-production process is a key hallmark of a Recovery College, and experience suggests that all need to pay close attention to the training of those involved in the process and establishing mechanisms that foster and facilitate it’ (Perkins et al., 2018: 20). In recognition that training should be provided, potential topics include understanding co-production, recovery, and purposeful storytelling before developing courses (Gill, 2014). Another recommendation included commissioning facilitation skills training for practitioner and peer trainers but acknowledged that co-production might not be included in this training (Morgan et al., 2018).
While three articles reported examples of providing prior training about delivering courses, importantly, none of these provided specific training on co-production. The first example provided a ‘preparing to teach in the lifelong sector’ (PTTLS) for peers course, but due to pragmatic reasons, not all practitioner trainers received this training (Meddings et al., 2014). In a second example, the Recovery College offered trainers the opportunity to attend a dementia course running within their mental health trust, which benefitted their co-design plans (West et al., 2022). A third example described the use of preparatory training for peer trainers but did not specify what this encompassed; although this was not focused on co-production practice, it did assist participants to adopt active learning approaches (Cameron et al., 2018).
In short, although there was agreement on the need for co-production training in Recovery Colleges, we did not find any practical examples of providing this.
Guidance on co-production
Similarly, there appeared to be a lack of guidance on how to do co-production, with only one article referring to written operational guidance that supported a safe environment to operate in an educational rather than clinical way, though specific details about what this consisted of were not given (Morgan et al., 2018).
Three articles gave examples of providing guidance for co-production development via group meetings and discussions. In one example, an ongoing discussion came in the form of an advisory group to explore areas of course development (Ali et al., 2022). A second example used bi-monthly forum meetings for anyone interested in Recovery College development, partnership forums and task groups, offering help on the decision-making process in co-production (Meddings et al., 2014). The third example, concerned the development of a dementia course, where the group met over eight sessions a year to co-develop aims, content, practicalities and context of lived and learned experiences, recognising the need for a shared learning process, reflecting, communicating and exploring challenges (West et al., 2022). These groups appeared to be an informal space to reflect co-design and were supported by co-production as a group rather than a couple co-producing.
Support provided for co-production
Support for co-production came in numerous formats, such as in groups or individually, including supervision and discussions between practitioners and peers in the design and development groups.
Group support
Two articles provided insight into their focus on supporting each other by maintaining and reviewing co-productive practices. These included small group activities facilitated to explore their understanding and the process of co-production (Ali et al., 2022). Another group revisited the meaning of co-production for those involved, using the fundamental principles for guidance (Morgan et al., 2018). This ensured transparency and that the co-production ethos was maintained throughout via collaborative support.
Mutual support
In some instances, the development of co-production knowledge and skills was provided within the collaborative relationship, with informal support from the practitioners via the peer trainers who had experience with the course structure (Dalgarno and Oates, 2019). This was often done during the debrief after the course to explore feelings and share personal stories (Dalgarno and Oates, 2019). A consultant psychiatrist described this support form as follows: ‘the peer was very informative and helpful throughout my time’ (Kay and Edgley, 2019: 12). In another article, the practitioner offered support to the peer by contacting them after a course to ‘check in’ (Whish, 2021: 28). These articles highlighted how support can be informal and a part of the co-production relationship.
In summary, the need for support in relation to co-production was recognised (Perkins et al., 2018). For example, to assist a co-production clinician, the need for support was advocated (Gill, 2014). However, it is recognised that everyone involved in co-production may need advice, guidance and a reflective space, to explore their experiences (Doroud et al., 2024). Offering support to peers and practitioners is essential in course development and in exploring communication, relationship management and role definitions.
Some participants believed ‘authentic’ co-production required the additional resourcing of collaborative online tools, staffing and educator remuneration (Doroud et al., 2024: 7). Co-production was described as an ongoing process, and its development was not recommended as structured but evolving through reflection withina the co-production relationship (). Nevertheless if neglected and not given guidance, co-production is vulnerable to degradation (Lewis et al., 2017). Although it was not suggested that there should be a standardised approach to co-production, findings highlighted the need for guidance to ensure that co-production did not become tokenistic.
Discussion
While there was consensus on the importance of using co-production in the articles reviewed, few examples of specific training, guidance and support on how to do this were provided .
Lack of clarity around expectations of the practitioner and peer trainer roles
Across the articles, commonalities included sharing ideas, goals, values and visions to bring about change through educational provision. The ‘co-production journey’ appeared to benefit from being allowed to evolve rather than having a scripted, standardised formula, in line with the difference between a planning versus dynamic approach (Dalgarno and Oates, 2019). At the same time, there was confusion about expectations and roles in co-production relationships. Therefore, the use of principles such as an assets-based approach, building on capabilities, reciprocal relationships, and blurring boundaries in roles and facilitation, may provide a checklist for those undertaking co-production (Slay and Stephens, 2013). Encounters arise around co-production when there is no clarity to resolve power dynamics and guarantee joint decision-making. One example might include ‘who has the final say’ of what is included in the course implying only one of the trainers has the power to make the ultimate end decision. This suggests from the start there is a need for clear diplomacy on ‘who will do what’, project plan, goals, responsibilities and task allocation (Meddings et al., 2014). Otherwise, co-production may fail when a balance of responsibility and accountability comes down to who is of the higher position within the Recovery College rather than who may be best to lead on specific topics and areas.
Guidance, training and supporting those to co-produce recovery education
Co-production is a fundamental asset to Recovery Colleges, but it was evident across the articles that there was a deficiency in guidance, training and ongoing support. This contrasts with clinical and teaching practices that require policy guidance, training and supervision as prerequisites. Although fidelity guidelines have been provided to facilitate co-production as a standard within Recovery Colleges (Lin et al., 2023), these do not explore the nuances such as training, guidance and supervision described in this scoping review. Standardised guidance on co-production may provide a roadmap for those involved, by establishing a quality-assured standard of practice and enhancing capacity and confidence to engage, including through clearly defined roles and expectations for those involved (NHS England, 2023). In guidance exploring co-producing and co-designing within healthcare it was acknowledge that a ‘one size fits all’ approach may be problematic because it reduces space for flexibility and innovation, by not taking into account variations within each setting (Robert et al., 2022). This suggests the value of preparatory guidance as a foundation for those co-producing, with possible follow-up training which to allow an exploration of issues such as conflict resolution, power sharing and responsibilities, developing working agreements and giving feedback (Dalgarno and Oates, 2018).
The provision of guidance could potentially be followed by ongoing support in groups and individually, allowing for reflective co-production practice and shared learning (Morgan et al., 2018). Co-production involves managing the co-production relationship with finding mutual understanding but also acknowledging the diversity of knowledge, skills and experience. It cannot be assumed that co-production will come naturally or has been a part of previous clinical or personal experience. Rather, it implies a journey that may require advice and support to value individuals and overcome obstacles. In support of this, it may be beneficial to conduct further research on co-production to develop evidence-based guidance, training and supervisory advice that explores methods of co-production, role defining, collaborative decision-making and problem-solving in pursuit of effective practice.
Strengths and limitations
This scoping review included the perspectives of both practitioner and peer trainers involved with co-production and provides a diverse overview of narratives relevant to Recovery Colleges and courses at different stages of development.
There are limitations to this review however. First, it did not include a comprehensive search of grey literature, and it is possible that this would have identified examples of individual recovery colleges reporting examples of their training/guidance documents and reports. In addition, the authors are aware of projects that offer peer development provided by Implementing Recovery through Organisational Change (ImROC), which offers, courses to support the development of Recovery Colleges and peer roles. These courses have not yet been written up for publication. Second, increasingly Recovery Colleges are being set up in non-English speaking countries; however, our search was limited to identifying articles published in the English language. Third, it is acknowledged that the search has only included Recovery Colleges that have described their practice as co-production or co-creation and therefore may not include articles that have used alternative wording for co-production.
Conclusion
There is a consensus that co-production in Recovery Colleges is fundamental to the success of recovery education. However, for co-production to be successful, there needs to be ‘buy-in’ and clear practical recommendations around guidance, training and continuous support for those who wish to participate. Further research is needed to support the development of evidence-based guidance and training materials. This could explore gaps in learning and support mechanisms for co-production, providing content to design research-based guidance, which might inform the development of one or more co-production training packages. Guidance and training is also required for managers, supervisors and others working in the mental health services that host Recovery Colleges, in order to ensure productive and supportive practice.