
Abstract
Objective:
With growing international interest in youth mental health as well as the other health issues faced by young people, school health education draws the attention of scholars from both East and West. However, what stands for health education in the context of a ‘health and physical education’ (HPE) curriculum varies widely between locations internationally. This article considers how we might understand what counts as health education as part of HPE in different policy contexts.
Method:
Informed by Foucauldian concepts of discourse, knowledge/power, and truth, we used Fairclough’s textually oriented discourse analysis to conduct a critical discourse analysis of official HPE curriculum policy in three different nation states (Aotearoa New Zealand, China and Japan).
Findings:
In Aotearoa New Zealand, curriculum discourse reflects a socio-critical approach to health education within HPE. In China, physical fitness dominates discourse on health education in HPE. In Japan, health education in HPE is directly connected to notions of safety and disease.
Conclusion:
In each of these three countries’ HPE curricula, we can see how global policy discourses construct particular ‘truths’ about the place and purpose of health education in schools. It is important to understand why different perspectives exist, because these different ‘truths’ are not just variations in policy content, but also reflect each country’s approach to health education as a response to unique challenges and priorities, shaping how health is understood and practised.
Introduction
With the growing international interest in youth mental health and other health issues, school health education has drawn the attention of scholars from both East and West (Leahy et al., 2015; Meng et al., 2025; Rich et al., 2019). However, in this journal and other English-language publications, curriculum analysis has so far been dominated by attention to white, Western English-speaking contexts with limited consideration of health in the education policies of countries such as China and Japan. This is, of course, the result of a Western-dominance of educational policy analysis (Mundy et al., 2016), the English-language dominance of publications in the field of health education, and an over-reliance on Western journals and scholars.
In places such as China and Japan, health education occupies a difficult space, caught between its – often tentative – place within the school curriculum, and expectations that it will make a positive difference to young people’s health (e.g. McCuaig et al., 2022; Shu et al., 2024; Zhang et al., 2022). Because the survival of health education in many schools relies on a social and historical commitment to child and youth well-being (Fitzpatrick and Tinning, 2014; Sharma, 2012), health education is often, in turn, inextricably linked to health problems (Leahy et al., 2015). This tension both serves and disadvantages the provision of health education in schools. On the one hand, concerns for child and youth health make it difficult to erase health education curriculum even if it has low status; on the other hand, the utilitarian ends of addressing health problems means there is little potential for the design of a rich, critical, health curriculum such as that envisioned by Lupton and Leahy (2021; see also Fitzpatrick and Powell, 2019).
A number of scholars have argued that the aim of making young people healthy is in direct tension with aims of ‘educating about health’ (Fitzpatrick and Burrows, 2017; Gard and Leahy, 2009; Leahy et al., 2015; Quennerstedt et al., 2010). For example, Wright et al. (2018: 118) state that the primary goal of schools is to focus on educational outcomes; they suggest that ‘health education cannot be, nor should it be, expected to solve broader social health issues’. However, school health education still occupies an uneasy position in the curriculum and is frequently collapsed with health promotion (McCuaig et al., 2022). This is related to the ongoing and historical place of schools as sites of health intervention and monitoring (Burns and Proctor, 2023).
While health education – including health, hygiene, and the education of the body – has had an established place in schooling in many Western countries since the early or mid-20th century (Burns and Proctor, 2023), it has also overlapped in complex ways with physical education (Kirk, 2018). This overlap has been formalised over the past few decades with health and PE being explicitly combined in the national curricula of many countries, including Aotearoa New Zealand, 1 Australia, China, Japan, and the United Kingdom.
Scholars from both East and West have raised concerns that the policy joining of health and PE together facilitates the latter being defined by health outcomes (Culpan, 1996/97; Tinning, 2000; Xiong, 2020). Quennerstedt (2008: 269) has argued that ‘health is, rather, a concept with different meanings in different contexts’ and Sinkinson and Burrows (2011) have suggested that health education is underserved in its policy connection with PE, which tends to take priority. They argued that who teaches health education – in relation to PE – matters. While “HPE” (or PEH – physical education and health) has become an internationally accepted symbol, the relationship between “health education” and “PE” may have very different meanings and effects depending on the policy, social and political context within which it is used. The problem then, of what the “health” in HPE actually means, remains both contested and assumed. The ‘H’ in HPE seems to exist somewhere on a continuum between physical health aims and a much broader conceptualisation of health education as explicitly educative. It is worth considering therefore what stands for official curriculum policy on health education in various nation states and how these representations impact the possibilities for health as educational practice.
According to Ball (2012), educational policy is a complex articulation of values, presumptions, silences and politics (see also Liu, 2004) and is increasingly neoliberalised. Policy shapes what is considered legitimate knowledge and whose interests are prioritised or marginalised within it. Context not only shapes policy but also defines what is possible within, through, and as a consequence of policy (Ball, 2012). Penney (2016: 133) observes that ‘specific contexts matter in the sense that they create conditions of possibility for particular reform agendas to be pursued’.
In this article, we employ critical discourse analysis (CDA, Fairclough, 2003), to analyse official health education curriculum policy statements in three countries – Aotearoa New Zealand, China and Japan. We explore how the policy construction of health education discourses becomes reasonable in these different socio-cultural and geographical contexts and examine what stands for health education within HPE in school curricula. We begin with a brief background to the health education curriculum policies of the three countries and present an overview of our theoretical approach and methods. We then summarise our findings as they relate to each nation state and the wider socio-cultural context within which health education is situated. The overall aim of this inquiry is to understand the ways in which policy contexts shape the possibilities for what health education comes to mean in different places and to highlight how the ‘H’ in HPE can mean very different things.
Health education in Aotearoa New Zealand, China and Japan
New Zealand health and physical education curriculum policy
Health education is one of three different but related subjects (the other two are physical education and home economics) in the Aotearoa New Zealand health and physical education (NZHPE) learning area. Health education was first joined with PE in official curriculum policy in 1993. Regardless of whether this integration was an attempt to redefine PE in terms of health or merely a convenient categorisation of complementary subjects (Culpan, 1996/97), the NZHPE curriculum policy retains this designation in most up to date statement of provision, The New Zealand Curriculum (NZC, 2007). The NZC is a single policy that defines the learning principles and achievement aims and objectives of all learning areas (HPE, Mathematics, English, Science, Social Science, Technology, The Arts, and Languages) for all schools in Aotearoa New Zealand. Within it, the NZHPE section shows how learning experiences in HPE are made up of the intersection of key areas of learning, underlying concepts, and achievement objectives (organised by four strands). Health education is mainly concerned with the key areas of learning related to: body care and physical safety, mental health (including alcohol and drug education), food and nutrition, and sexuality education. Learning in PE relates to sports studies, physical activity, and outdoor education. The NZHPE curriculum also includes four underlying concepts: hauora, 2 attitudes and values, a socio-ecological perspective, and health promotion (Ministry of Education New Zeala (MOENZ), 2007). and the NZC document provides a separate description for each of health education and PE. Health education is explicitly focused on an educative approach to health and includes detailed learning statements related to understanding how personal, social and cultural factors intersect with health and well-being as well as the development of competencies and skills. Learning also relates to social and political health concerns with the aim of students’ developing skills to promote personal, interpersonal, and societal well-being. PE highlights how learning in through and about a wide range of movement. It also takes an expressly sociocultural and critical approach to the role of physical activity and sport in society (MOENZ, 2007).
China’s physical education and health curriculum policies
China’s physical education and health (CPEH) curriculum policies are distinct from other subjects and address the two different stages of compulsory education (years 1–9) and senior high school (years 10–12). Current CPEH policy documents are named Physical Education and Health Curriculum Standards for Compulsory Education (义务教育体育与健康课程标准, 2022) and Physical Education and Health Curriculum Standards for General Senior High Schools (普通高中体育与健康课程标准, 2020). Health education was formally brought into the national curriculum policy in the early years of the 21st century, when the curriculum area was renamed from ‘physical education’ to ‘physical education and health’. Unlike previous PE curriculum policies focused on sport skills and performance, CPEH emphasises health and physical fitness (Jin, 2013). This shift is attributed to 1987 State Council-approved National Student Physical Health Survey System, which highlighted a declining trend in Chinese students’ physical health. This led to a change in the CPEH curriculum policies direction towards promoting youth health and a ‘health first’ guiding philosophy. The structure of CPEH curriculum policies includes statements on the curriculum nature, rationale, objectives as well as academic achievement and implementation recommendations. Physical education and health education are not clearly separated from one another in the documents and key content includes physical fitness, motor skills, and specialised sports skills with an emphasis on improving students’ physical health (Ministry of Education of the People’s Republic of China (CMOE), 2020, 2022). Content also includes knowledge and skills relevant to nutrition and food safety, disease prevention, the relationship between exercise and the environment, and mental health (CMOE, 2020, 2022).
Japan’s health and physical education curriculum policies
Health and physical education in Japan (JHPE) is detailed in national curriculum policies, including the Curriculum Guideline for Primary School (小学校学習指導要領, CGPS, 2017a), the Curriculum Guideline for Junior High School (中学校学習指導要領, CGJH, 2017b), and the Curriculum Guideline for Senior High School (高等学校学習指導要領, CGSH, 2018). In the CGPS, ‘PE’ is recognised as a subject, and ‘health’ as an area of learning within PE. PE is described as a subject that maintains and promotes health, with the purpose of developing good habits for a healthy life (MEXT, 2017a). The CGJH and CGSH documents both make reference to ‘health and physical education’ as a subject, but describe health education and PE as two separate areas. In these latter documents, PE focuses on movement and sports with an emphasis on sports-related knowledge and skills. Key movement contexts are physical fitness, apparatus gymnastics, track and field, swimming, ball games, budo, dance, and theory (MEXT, 2017b, 2018). Health education topics include mental health, health and environment, injury prevention, healthy lifestyles and disease prevention (MEXT, 2017b, 2018). Health education and PE share a common aim to ‘enable students to maintain and promote their physical and mental health throughout their lives and to realise a rich sporting life’ (MEXT, 2017a: 17, 2017b: 24, 2018: 21).
Methodology
Policy discourse, by privileging certain positions while silencing others, constrains what can be thought, written or said and thereby acts as a disciplinary technique (Foucault, 1981). In this context, Fairclough (2003) suggests a focus on both a linguistic analysis of policy texts and the social construction of policy discourse, via a process he describes as textually-oriented discourse analyses. Textually oriented discourse analysis seeks to bridge the gap between socially inspired research that avoids textual analysis and language-focused research that overlooks social theory (Fairclough, 2003). That is, in CDA, textual analysis and discourse theory are seen as interconnected and intertwined.
For textually oriented discourse analysis, Fairclough (2003: 6) notes that specific software packages allow one to identify keywords in text and to ‘investigate distinctive patterns of co-occurrence or collocation between keywords and other words’. In this study, we used NVivo 14 to assist us to identify different discourses surrounding ‘health’ in the HPE curriculum policies in Aotearoa New Zealand, China, and Japan. We conducted a word frequency search in NVivo 14 and formed a word cloud 3 for those words that appeared in the same sentence as ‘health’. This was a way of exploring the relational differences in discourse by looking at the co-occurrence patterns of words in texts (Fairclough, 2003). We then undertook a wider analyses of these policy discourses within the social and political context of their official policy status in Aotearoa New Zealand, China, and Japan. We focused specifically on how the construction of health education discourses becomes reasonable within these different socio-cultural contexts and examined what health education might stand for in school policy.
Findings
New Zealand HPE (NZHPE) curriculum policy: personal health and learning
Figure 1 shows the word cloud generated to reflect the top 10 high-frequency words that appeared in a sentence at the same time as ‘health’ in the NZHPE curriculum policy. The word cloud indicates that the terms ‘development’, ‘physical’, ‘personal’, ‘communities’, ‘students’, ‘influence’, ‘needs’, ‘wellbeing’, ‘analyse’, ‘education’, ‘learning’, ‘promote’ (in descending order of frequency, see Appendix 1 for the words with frequencies and similar words included in the count) are situated around ‘health’. Further exploration in the policy text reveals that, in addition to ‘health and physical education’ as a specific name for this learning area, ‘personal’ is the word that appears most frequently in conjunction with ‘health’, as ‘personal health’.
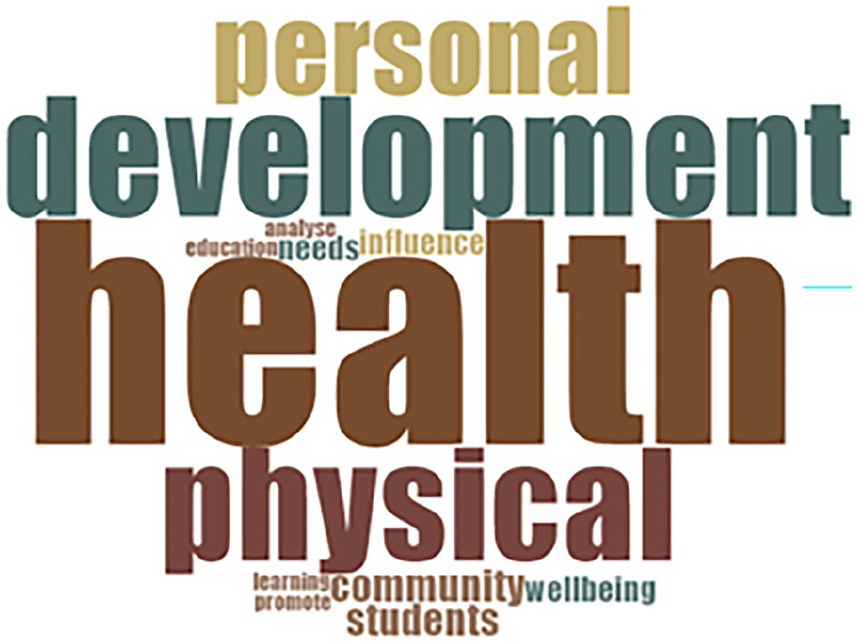
Top 10 high-frequency words for the NZHPE curriculum policy document.
‘Personal health’ is also part of the title of one of the four strands 4 of NZHPE: namely, personal health and physical development. The related achievement objectives corresponding to ‘personal health and physical development’ are then grouped as ‘personal growth and development’, ‘regular physical activity’, ‘safety management’, and ‘personal identity’ (MOENZ, 2007). In the description of the four achievement objectives, with the exception of regular physical activity, which emphasises the importance of physical activity on students’ personal lifestyle to enhance well-being (MOENZ, 2007), the other three objectives highlight responsibility for making ‘good’ decisions about one’s health while also placing personal health in the context of wider community health. For example, in personal growth and development, it is stated that students will ‘describe their stages of growth and their development needs and demonstrate increasing responsibility for self-care’ (level 2). 5 In safety management, the document requires students to ‘critically analyse dilemmas and contemporary ethical issues that influence their own health and safety and that of other people’ (level 8). In personal identity, students will ‘critically analyse the impacts that conceptions of personal, cultural, and national identity have on people’s wellbeing’ (level 8).
Importantly, ‘community’ and ‘health’ are also high-frequency co-occurring words in the document. The above examples all show the explicit socio-critical and learning orientation given to health within the NZHPE document (Dixon and Robertson, 2021; Fitzpatrick and Burrows, 2017). So, while personal health is a repeated notion, this is incomprehensible without contextualisation within communities and environments. It is interesting to examine how this relationship is expressed. As is also evident in the word cloud, the term ‘influence’ is the most frequently occurring verb that precedes or follows ‘health’ throughout the policy, for example, ‘factors that influence the health of individuals’(MOENZ, 2007: 23); ‘Identify how health care and physical activity practices are influenced by community’ (level 3); ‘Critically analyse dilemmas and contemporary ethical issues that influence their own health’ (level 8). Thus, the learning objectives in NZHPE highlight the interrelationships between individuals and the wider socio-cultural environment (Burrows and Wright, 2004). This is underscored using a specifically social-psychological approach – based on the work of Bronfenbrenner – that positions the individual as somewhat separate from society and culture and thus ‘influenced’ by external environments. However, the focus on ‘critically analysing’ also shows the explicitly educative focus of this policy, which emphasises an approach to health education that engages students with learning about wider social and political contexts and relations of power, rather than requiring behaviour change (Fitzpatrick and Tinning, 2014).
Positioning health within a socio-ecological perspective in the NZHPE curriculum policy was intentional (Burrows and Wright, 2004; Culpan, 1998; Sinkinson and Burrows, 2011). However, this framing also creates a tension between health as a social and political concern and health as personal responsibility. The document explicitly stresses that young people need to develop their knowledge, skills, attitudes, and values to ‘take critical action to promote personal, interpersonal, and societal wellbeing’ (MOENZ, 2007: 23). This requires young people to understand the socio-cultural, historical, and economic factors affecting health issues (Tasker, 1996/97). While learning in health education does focus on students’ own decisions, these are interconnected with society and the emphasis remains on learning about decisions, rather than on the behaviour or performance of particular decisions. There is thus a tension between the ‘personal’ – a key feature of neoliberal-dominated education contexts (Ball, 2012; Powell and Pluim, 2020) and the explicit socio-critical approach to learning. Health education, as productive of ‘good’ citizens who take responsibility for their health status and are able to make ‘good’ decisions (Burrows and Wright, 2004; Sinkinson and Burrows, 2011), sits alongside an emphasis on individual judgement, influences and actions for ‘good’ health. It does not, however, require students to demonstrate or enact these judgements, influences and actions in practice, and so learning remains the focus over health outcomes.
Chinese PEH (CPEH) curriculum policies – the relationship between health and physical fitness
Figure 2 shows the word cloud generated to reflect the top 10 high-frequency words that appeared in a sentence at the same time as ‘health’ in the CPEH curriculum policy documents. In the centre of the word cloud is the character for ‘health’ (健康). The word cloud indicates that the terms ‘students’, ‘sports’, ‘physical fitness’, ‘physical activity’, ‘level’, ‘curriculum’, ‘learning’, ‘standards’, ‘physique’, ‘skills’, ‘knowledge’ (in descending order of frequency, see Appendix 1 for the words with frequencies and original Chinese words included in the count) are situated around ‘health’. Further exploration in the policy text reveals that, in addition to ‘physical education and health’ as a specific name for this subject, ‘physique’ (体质) is the word that appears most frequently in conjunction with ‘health’, as ‘physical health’ (体质健康).
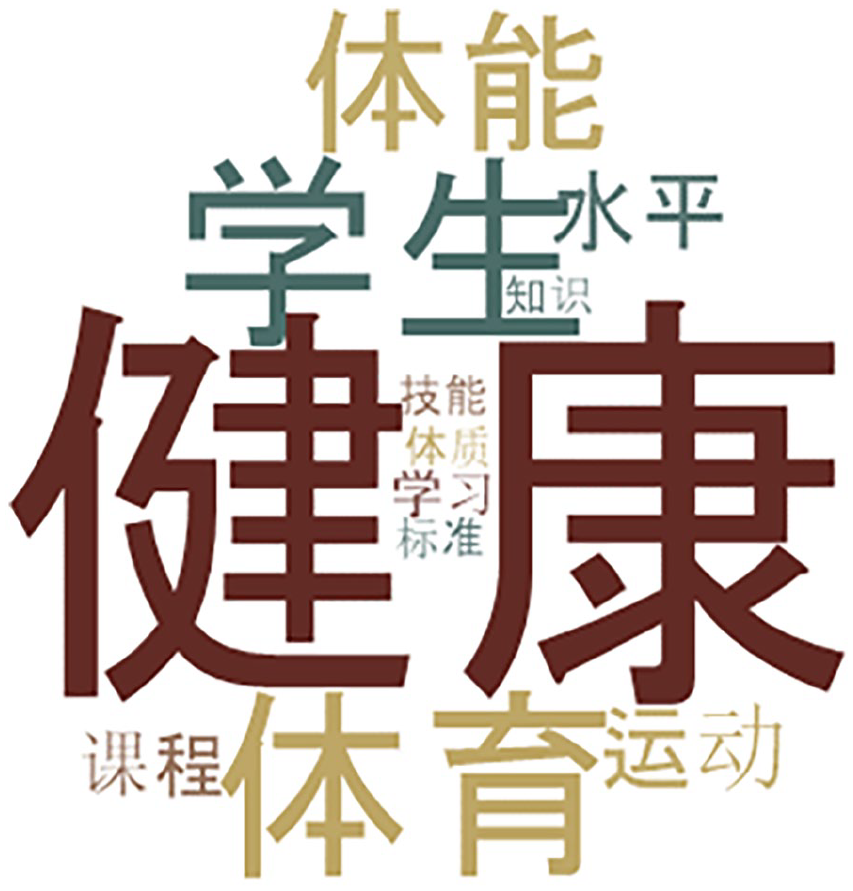
Top 10 high-frequency words for the CPEH curriculum policy documents.
The term most closely related to ‘physical health’ (or ‘health’) is ‘physical fitness’ (体能). In the word cloud, ‘physical fitness’ is the third highest-frequency word related to ‘health’ (after ‘student’ and ‘sports’). Physical fitness is a compulsory curriculum content of CPEH in both compulsory education and senior high school, where students are required to practise fitness exercises and pass fitness tests. This is recognised as a means of promoting students’ health (CMOE, 2020, 2022). The compulsory education policy requires each CPEH lesson to include about 10 minutes of physical fitness practice, with the aim of addressing national concerns about Chinese students’ physical fitness levels and health (Ji, 2022). Importantly, the two policy documents referred to earlier also contain several references such as ‘actively participating in a variety of physical fitness practices to meet the National Student Physical Health Standard (NSPHS)’; ‘developing appropriate physical fitness plans based on the results of the NSPHS’; and ‘describing the importance of physical fitness to health’ (CMOE, 2020, 2022). The NSPHS refer to a national policy document enacted in 2014 as ‘a comprehensive assessment of students’ physical health level in terms of body shape, physical function and physical quality. . . [which together constitute] the individual assessment standard of students’ health’ (CMOE, 2014: 1). In practice, this means that young people’s health is tested primarily through the 50-metre run, high jump, and other fitness tests (strength, speed, endurance, flexibility etc.). Thus, health in the CPEH curriculum policies attaches significant value to, not only the notion of physical fitness, but its actual performance (Shao, 2023).
The terms ‘mental health’ and ‘social resilience’ appear 15 times and 4 times, respectively, in the CPEH curriculum policies (CMOE, 2020, 2022). Both are, however, positioned in the documents as the ‘products’ of pursuing physical health and given lower status. For example, the CPEH curriculum policies are organised around a standards-based approach to learning and assessment. The content and assessment of physical health are thus described in detail and explicitly assessed (as shown above). Narratives about mental health and social resilience are, however, presented in a more generalised way, such as ‘understanding and experiencing the positive impact of physical activity on mental health’ (CMOE, 2022: 7); ‘knowing the contents and features of mental health, and applying methods of improving mental health’ (CMOE, 2020: 17); and ‘enhancing social resilience’ (CMOE, 2020: 26). As Xiong (2020) argues, physical health is more likely to be recognised in CPEH curricula as the ‘health’ standard and the health requirement of health education. Mental health and social resilience are related outcomes but the curriculum intentions for these are much less clear. Health education within CPEH curriculum policy then is specifically conceptualised as the performance of physical health as constructed and measured by indicators of physical fitness.
Japanese HPE (JHPE) curriculum policy – the relationship between health and safety
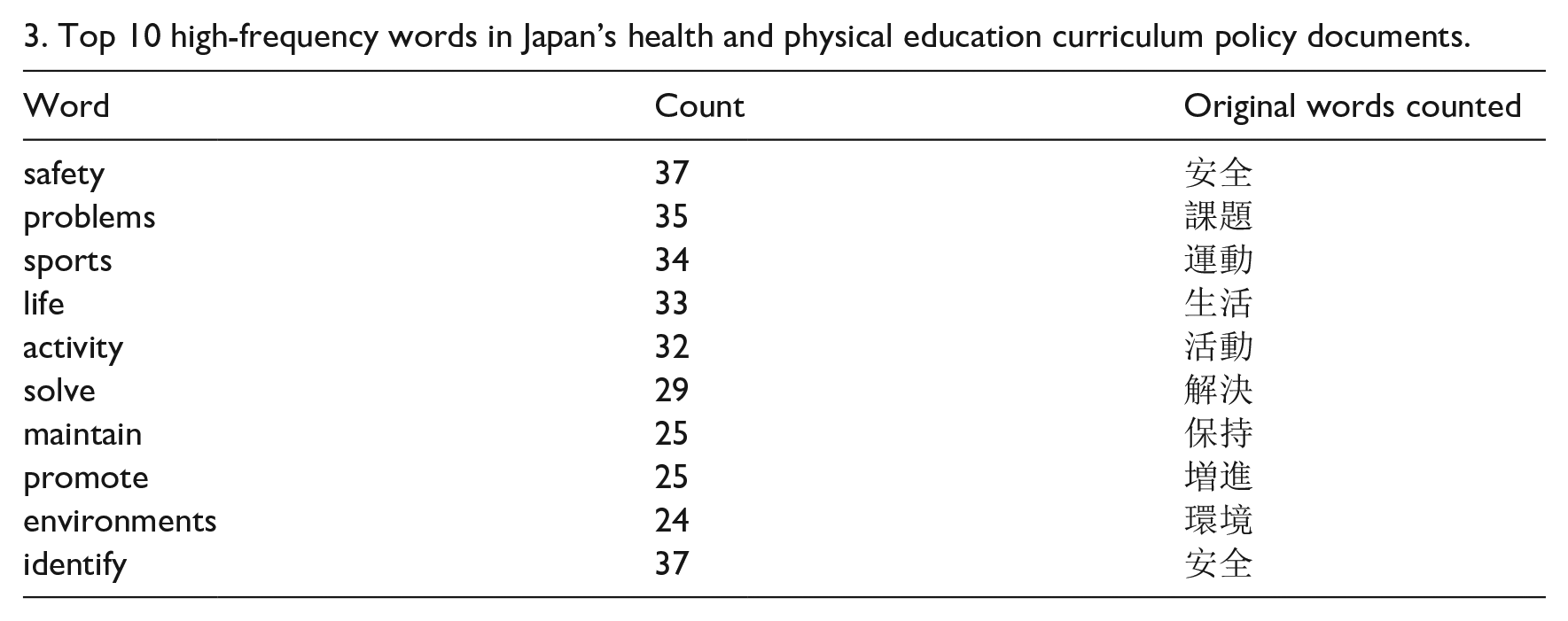
Figure 3 shows the word cloud generated to reflect the top 10 high-frequency words that appeared in a sentence at the same time as ‘health’ for the JHPE curriculum policy documents. In the centre is the character for ‘health’ (健康). The terms ‘safety’, ‘problems’, ‘sports”, “life”, “activity”, “solve”, “maintain”, “promote”, “environments”, “identify” (in descending order of frequency, see Appendix 1 for the words with frequencies and original Japanese words included in the count) are situated around “health”. Further exploration within the policy text reveals that “maintain”, and “promote” are the verbs most frequently linked to “health” and the terms “safety”, and “problem” are the nouns most frequently linked to “health”.
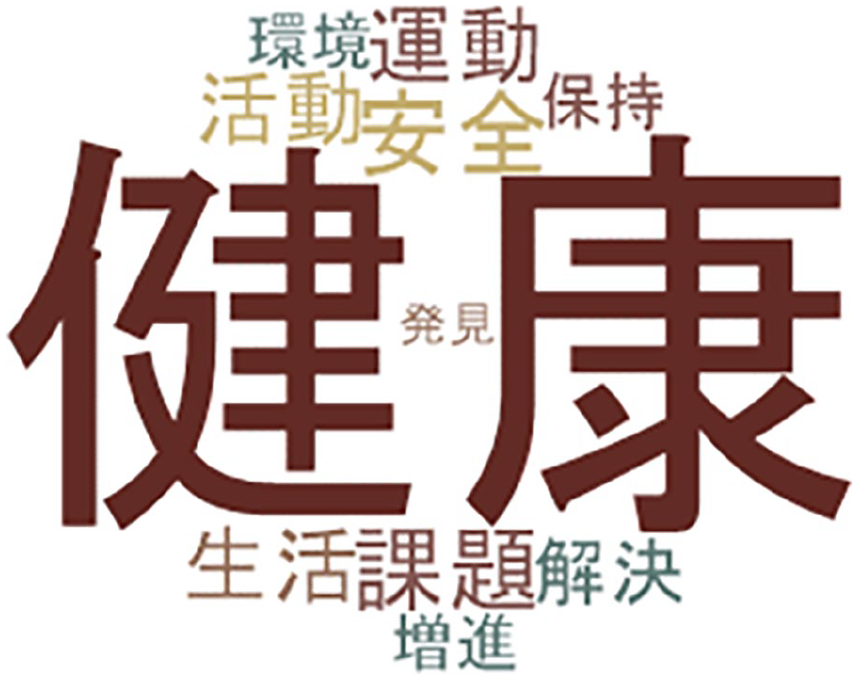
Top 10 high-frequency words for the JHPE curriculum policy documents.
The presence of the two verbs ‘maintain’ and ‘promote’ health aligns directly with the general objective of JHPE curriculum policies: namely, ‘to develop the competencies that enable students to maintain and promote their physical and mental health throughout their lives and to realise a rich sporting life’ (MEXT, 2017a: 17, 2017b: 24, 2018: 21). The related competencies are divided into three points in the policies, namely ‘acquiring knowledge and skills for health and safety’, ‘identifying and solving health problems’, and ‘developing attitudes towards life that aim to maintain and promote health’ (MEXT, 2017a, 2017b, 2018). The nouns ‘safety’ and ‘problem’, which frequently co-occur with health are key in this respect.
‘Health and safety’ (健康・安全) appears 32 times in the JHPE curriculum policy texts, including as ‘ensuring health and safety’, ‘valuing health and safety’, ‘understanding health and safety’ (MEXT, 2017a, 2017b, 2018). The notation ‘・’ in Japanese, known as a nakaguro, is used to separate multiple words to indicate a unified concept (Japan Translation Federation, 2019). That is, the JHPE curriculum policies emphasise the understanding of ‘health and safety’ as a whole concept. In the documents, ‘health and safety’ are directly connected to students’ personal lives (MEXT, 2017a, 2017b, 2018). ‘Health and safety’ content includes repeated mention (12 times) of the ‘prevention of injuries’, including swimming accident injuries, traffic accident injuries, natural disaster injuries, labour injuries, and criminal injuries 6 (MEXT, 2017a, 2017b, 2018); The ‘prevention of diseases’ is mentioned 16 times, including modern infectious diseases, lifestyle-related diseases, diseases caused by smoking, alcohol consumption, and drug abuse, as well as mental illnesses (MEXT 2017a, 2017b, 2018).
‘Problem’ is the noun that most often appears in conjunction with ‘health’, as in ‘health problems’. Further exploration in the policy texts reveals that ‘health problems’ and ‘disease prevention’ are closely linked. For example, in the policy for primary school, health education learning contents include the prevention of disease, the aim to identify problems related to the causes of illness, methods of prevention, and the impacts on health of factors such as smoking, alcohol consumption, and drug abuse (MEXT, 2017a). In the policy for junior high school, teachers are encouraged to guide students to acquire a deeper understanding of healthy living and disease prevention by designing activities aimed at identifying and solving problems (MEXT, 2017b). Importantly, the policy for senior high school states that students should be guided to understand the health issues and health interventions that have evolved in response to changes in the country’s disease and social structure, as well as modern infectious and lifestyle-related diseases and their prevention (MEXT, 2018).
The focus on disease prevention in the JHPE curriculum policies is unsurprising. A rapidly declining birth rate and an ageing population have brought about significant changes in demographic structure, leading to an explicit focus on the burden of disease in Japanese society (Hirata et al., 2023; Nomura et al., 2017). This concern appears specifically in the policy for senior high school, which encourages schools to consider and address the health concerns caused by declining birth rates, population ageing, and changes in the incidence and prevalence of particular diseases (MEXT, 2018). Therefore, the concept of health in the JHPE curriculum policies is expressly concerned with the medical aspects of disease avoidance and health maintenance. The focus is on learning about these issues in the hope that such learning will lead to a long-term reduction in the social and economic burden associated with disease and healthcare costs. In some ways, this policy seeks to shift responsibility for the nation’s biomedical health onto members of the younger generation by encouraging them to identify and solve health problems.
Conclusion
Our analyses of the official HPE curriculum policies of Aotearoa New Zealand, China, and Japan reveal different discourses surrounding health and health education in each country, shaped by their unique historical, cultural, and political contexts. These differences are, however, connected to wider global policy discourses related to the body, fitness and health. Together, our findings underscore the value of CDA in highlighting the implicit assumptions and values embedded in health education policy discourses. While the core objective of promoting health and well-being is common, the concept of health and the purpose of health education are different in each of these policies according to the ‘truth regimes’ of each (Foucault, 2000). Discourse is not merely the use of language but a complex network encompassing knowledge and power. In the context of health education policies, the policy texts of different countries are forms of discourse that construct concepts and practices of health through specific relations of knowledge and power.
In Aotearoa New Zealand, curriculum discourse reflects a socio-critical approach to health education within HPE and does so explicitly by focusing on learning about health and well-being at the personal, interpersonal, and societal levels. It also, however, has inherent tensions between the socio-critical stance taken and an individualistic and personal-responsibility approach to health. In China, health is governed by concerns about youth fitness levels and determined by fitness testing, with mental health considered important but viewed as a result of physical activity and fitness. Physical health is thus a dominant discourse in HPE in China and one that displaces learning and insists on the performance of fitness itself. In Japan, health in HPE is connected to notions of safety and disease, driven by concerns about an ageing population, low birth rates, and the burden of disease, with youth health seen as the answer to future economic woes. This approach is expressly focused on addressing physical health concerns and disease but the pathway to achieving these goals is positioned as the lifelong duty of young people.
In each of these curricula we can see how global policy discourses construct particular ‘truths’ about the place and purpose of health education in schools. These include the health of nations as the express responsibility of schooling and position the behaviours and practices of schooling and young people as sites of hope for future economic and physical prosperity. In the process of globalisation, discourses with ‘truth’ formulae do not replace each other, but coexist in different societies and cultures. It is important to understand why different ‘truths’ exist, because ultimately it impacts how
‘we are judged, condemned, classified, determined in our undertakings, destined to a certain mode of living or dying, as a function of the true discourses which are the bearers of the specific effects of power’. (Foucault, 1980: 94)
In this sense, health education policies in different countries are not just about conveying health-related ‘knowledge’ but are also about shaping and maintaining social order and power relations. The different truths explored in this paper are not merely variations in policy content, but also reflect each country’s approach to health education as a response to unique challenges and priorities, shaping how health is understood and practised. In policy analysis, the ‘H’ in HPE within different policy contexts cannot therefore be taken for granted in terms of either its meaning or related practices.
Footnotes
Appendix 1
3. Top 10 high-frequency words in Japan’s health and physical education curriculum policy documents.
| Word | Count | Original words counted |
|---|---|---|
| safety | 37 | 安全 |
| problems | 35 | 課題 |
| sports | 34 | 運動 |
| life | 33 | 生活 |
| activity | 32 | 活動 |
| solve | 29 | 解決 |
| maintain | 25 | 保持 |
| promote | 25 | 増進 |
| environments | 24 | 環境 |
| identify | 37 | 安全 |
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.