
Abstract
Objective:
Health and self-care education to 5- to 11-year olds is key to disease prevention and health promotion. This study aimed to evaluate how self-care education is delivered to primary school-aged children in England.
Design:
Non-participant ethnographic observation.
Setting:
A sample of primary schools, extracurricular clubs and religious schools in England.
Methods:
In-class observations were undertaken in primary school settings and textual narrative synthesis was used for analysis.
Results:
A total of 11 teaching sessions were observed. Self-care topics were covered in subject areas including science, physical education and personal, social and health education lessons. Healthy eating and nutrition, physical exercise, mental health and hygiene were key areas covered. While the sessions emphasised the importance of healthy behaviours, the link between healthy behaviours and health promotion was not always apparent. Methods of delivery varied considerably across educational settings.
Conclusion:
Strategic policy adjustments are recommended to establish a standardised curriculum for the delivery of self-care education, thereby fostering equitable opportunity for learning. Further emphasis on self-care in the context of disease prevention, health promotion and management of minor ailments is needed.
Introduction
The World Health Organization (WHO) defines self-care as ‘the ability of individuals, families and communities to promote and maintain their own health, prevent disease, and to cope with illness – with or without the support of a health or care worker’ (WHO, 2022). The seven pillars of self-care include knowledge and health literacy, self-awareness of physical and mental conditions, physical activity, healthy eating, risk avoidance, hygiene, and rational use of products and services (WHO, 2016).
Knowledge and awareness regarding responsible self-care can improve people’s ability to look after their well-being and to know where and when to seek advice and professional support. Knowing about self-care better prepares individuals to deal with ill health, reduces the burden on National Health Service (NHS) services and improves health outcomes, as well as reduces ‘sick’ days and absence from school (Fielding, 2015).
Giving people the knowledge and confidence to self-care and see a healthcare professional when needed promotes better health control and prevents long-term illness (Rafferty et al., 2017). If individuals manage minor illnesses on their own this can reduce visits to doctors. This economic allocation of resources enhances patient outcomes and personal responsibility for healthcare (Banks, 2010). The best and most efficient approach to reach a huge segment of the population, including children, school employees, and the public, is through schools (Pérez-Rodrigo and Aranceta, 2001).
Schools have a pivotal role to play as settings for programmes and interventions to improve child health. Nutrition programmes implemented within schools have shown promise in enhancing nutritional outcomes, particularly increased fruit and vegetable consumption (Porter et al., 2018). These initiatives, many of them inspired by the WHO Health Promoting Schools (HPS) approach, include nutrition education, food environment modifications and eHealth interventions (O’Brien et al., 2021). The Alberta Project Promoting active Living and healthy Eating (APPLE) Schools in Canada found that in schools which included educational interventions about diet, activity levels and body weight, students ate more fruit and vegetables, consumed fewer calories, were more physically active, and were less likely to be obese (Fung et al., 2012).
Recognising that the interaction between health and education is bidirectional is crucial. Healthier children tend to excel academically. For example, adequate sleep and proper nutrition enhance cognitive and learning abilities in children (Davies et al., 2018). Children in good health tend to exhibit a stronger work ethic in school. They demonstrate improved focus, increased participation in school activities, and better attendance, all of which enhance academic performance. Importantly, this relationship is influenced by learning engagement rather than by variations in intelligence (Viner et al., 2020).
Children’s mental health and resilience are closely tied to school attendance and participation (Clarke et al., 2021). Schools are key to helping children acquire social skills, engage in physical activity and address mental health challenges. Promoting resilience among students is essential for their mental well-being and academic success (Nally et al., 2021). Education itself is a lifelong determinant of health. A whole-school approach is vital to ensure that interventions are implemented effectively in schools (Ponsford et al., 2022). Children’s educational experiences shape their health behaviours and long-term outcomes. Ensuring every child receives a good quality education during their early school years is critical for their future health and well-being (Shea et al., 2017).
Empowering children with the ability to practise self-care and manage minor ailments such as coughs, colds and simple wounds or rashes can instil a sense of health consciousness, shaping them as future members of society (Prinsloo, 2016). During the primary school years (5–11 years), children experience increased self-awareness, growing independence and the emergence of self-regulatory behaviours, making this period crucial for fostering skills to promote self-management (Jones et al., 2022). Members of this age group begin to grasp cause-and-effect relationships, a critical development necessary for understanding the importance and consequences of health behaviours. This period is therefore ideal for imparting knowledge about self-care and health awareness (Pamungkas and Chamroonsawasdi, 2019).
Successful self-care requires the development of three key components: self-care maintenance, monitoring and management, alongside growing healthcare autonomy. In addition to basic self-care maintenance skills, it is important to build on these components as children mature (Beacham and Deatrick, 2013).
Studies have shown that absenteeism, whether due to illness or other reasons, is associated with lower academic achievement at all levels of education (Aucejo and Romano, 2016). Students who are frequently absent often struggle to catch up with their classmates, leading to decreased academic performance (Claymore, 2019). Increasing the focus on basic subjects such as reading, writing, and arithmetic could be helpful in enabling children to catch up (Lessof et al., 2018). In addition, equipping students and parents with self-care skills can empower them to manage minor health issues without the need for school absence (Garcia and Weiss, 2018).
It has been suggested that children who are not engaged in structured activities during the summer holidays are more likely to exhibit sedentary behaviour, which can adversely affect their physical and mental health (Larose et al., 2023). However, it is important to note that participation in sports or recreational activities also plays a significant role in promoting physical activity during this time, even if these activities are not formally organised on educational lines. While structured educational activities can provide important learning opportunities, any active engagement – whether educational or recreational – can be beneficial for children’s health and well-being.
Ponsford et al. (2022) have stressed the importance of school-based health promotion, highlighting key factors such as supportive environments, integrated health education, and active student participation. However, there is a gap in understanding how self-care, particularly in managing minor ailments and promoting health autonomy, is addressed among primary school-aged children. Through direct observation in classroom settings, this study aimed to teaching and learning about self-care in primary school-aged children in education settings, looking at what is taught to children in the lessons, and how.
Aim
To explore how self-care education is delivered to primary school-aged children in England across various educational settings, including mainstream schools, extracurricular clubs, and religious schools.
Research question
How is self-care education delivered to primary school-aged children in England, and what variations exist in content, engagement, and alignment with the national curriculum in different educational settings?
Methods
This study utilised a non-participant ethnographic observation technique rooted in the traditions of interpretivism ethnography (Hammersley and Atkinson, 2019). This approach allowed for an in-depth examination of the natural classroom environment, capturing real-time interactions between teachers and students without affecting the educational dynamics. The non-participatory role of the researcher ensured minimal disruption to the learning environment and facilitated the collection of authentic, unfiltered data on how self-care education is delivered. This method was especially well suited to exploring varied educational settings, as it enabled the researcher to observe contextual factors influencing teaching and learning about self-care.
Participants
Eleven in-class observational studies on a self-care-related topic were undertaken to gather data on what was taught. The sample was limited to schools in the West Midlands area of England which expressed interest. A range of different educational settings were included in the study: namely two primary schools, one after-school club, and one religious school. These settings were chosen to explore how different environments might contribute to the delivery of self-care education.
Schools were identified through purposive sampling to target educational settings actively delivering self-care education. The study was advertised through professional networks and local educational forums, inviting interested schools and other educational settings to participate. Participating schools and settings were not formally linked to the first author’s university but were approached due to their known involvement in health education initiatives. After-school and religious settings were selected to provide complementary insights into how extracurricular and faith-based education supplement in-class health education. The final sample represented a range of socioeconomic backgrounds, including both urban and suburban schools, to ensure diversity in the observed practices.
Classes were selected based on the content being delivered and focused on teaching sessions covering health education topics such as healthy eating, physical activity, mental health, and hygiene. Teachers identified lessons aligned with these topics, ensuring that the observations reflected a broad spectrum of self-care education being taught to primary age students in different settings. The observed classes were independent of each other and each provided a single-point snapshot of the curriculum delivered during one session.
Instrumentation
Observation sessions were coordinated with the primary schools’ senior management teams, which informed parents and guardians about the data collection process and distributed information sheets outlining the study. Parents provided consent for their children’s participation, and children were informed in an age-appropriate and reassuring manner that they could decline to participate or step away at any time without any consequences. Efforts were made to ensure children felt comfortable and at ease during the observations. All communications with participants and guardians were undertaken by the schools and after school clubs. No opt outs were requested.
Procedure
The senior management team at each school identified specific lessons on self-care and health education, and the researcher (SO) was invited to attend. Teachers were provided with consent forms, information sheets, and the opportunity to ask any questions.
Data were collected, including demographic information about the participating students (such as age, gender, and year group), the content of the lessons, the nature of children’s interactions with each other and the teacher, class engagement and indications of their prior knowledge. The researcher also recorded general information about the setting, teacher–student interactions, resources, teacher role and student actions. Interactions within this context refer to the verbal and non-verbal exchanges between students and teachers, including questions, responses and discussion. In contrast, class engagement pertains to the overall involvement of students in the lesson, including pupils’ attentiveness, participation in activities, and enthusiasm. The observer adopted a non-participatory role, and participant comments were not recorded verbatim.
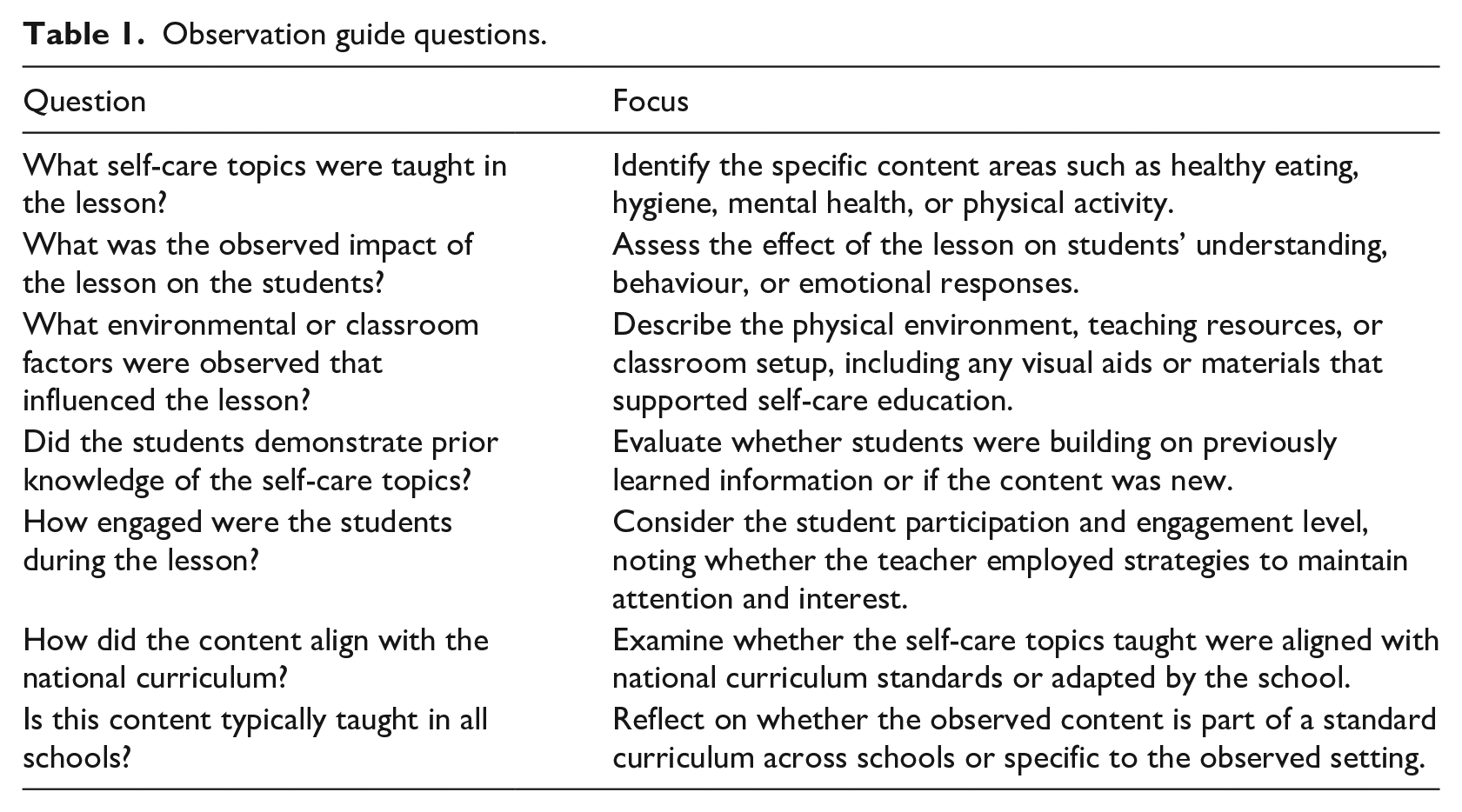
Throughout the study, the focus was on key aspects of the classroom dynamics, including children’s prior knowledge of healthy behaviours, their engagement with the teaching material, and their emotional reactions to health topics (Table 1). For example, during one observation, a Year 3 class (8–9 years old) discussing healthy eating demonstrated prior knowledge of food groups and actively participated in conversations about what constitutes a balanced diet. In another instance, a Year 6 class (10–11 years old) engaged in a mindfulness session showed notable changes in emotional state, with students reporting increased calmness and focus after breathing exercises. These examples illustrate the varied responses and knowledge levels observed in different age groups and settings.
Observation guide questions.
Following the observations made in each setting, a detailed description of the interaction between teachers and children was prepared, along with reflections on the observed environment. No identifiable information was collected.
Data analysis
Textual narrative synthesis was employed to analyse the data from the observational studies (Lucas et al., 2007). This method involved grouping the findings from each observation into categories, allowing for structured summaries that allowed the extracted data to be contextualised. Unlike thematic analysis, which organises data via codes and themes highlighting shared features and commonalities, narrative synthesis as undertaken here focused on the context and characteristics of each mini observational study.
Findings
A total of 11 in-class observations were conducted. The year groups focused on ranged from reception class (4–5 years old) to year 6 (10–11 years old). Activities observed included teaching sessions on mental health, healthy eating, physical activity, hygiene, and self-care.
Healthy eating
The Year 3 (7–8 years old) PSHE lesson on healthy eating involved 29 students who engaged in discussion about food, showing their prior knowledge of healthy eating options. The school’s meal provision closely aligned with suggestions in the Eat Well plate, which provides visual guidance on a balanced diet with proper proportions of food groups (fruits, vegetables, carbohydrates, proteins, and dairy). Conversations about healthy choices continued during lunchtime, where students discussed the food they had brought with them in their lunch boxes (see Table 2).
Summary of direct observation sessions and outcomes.
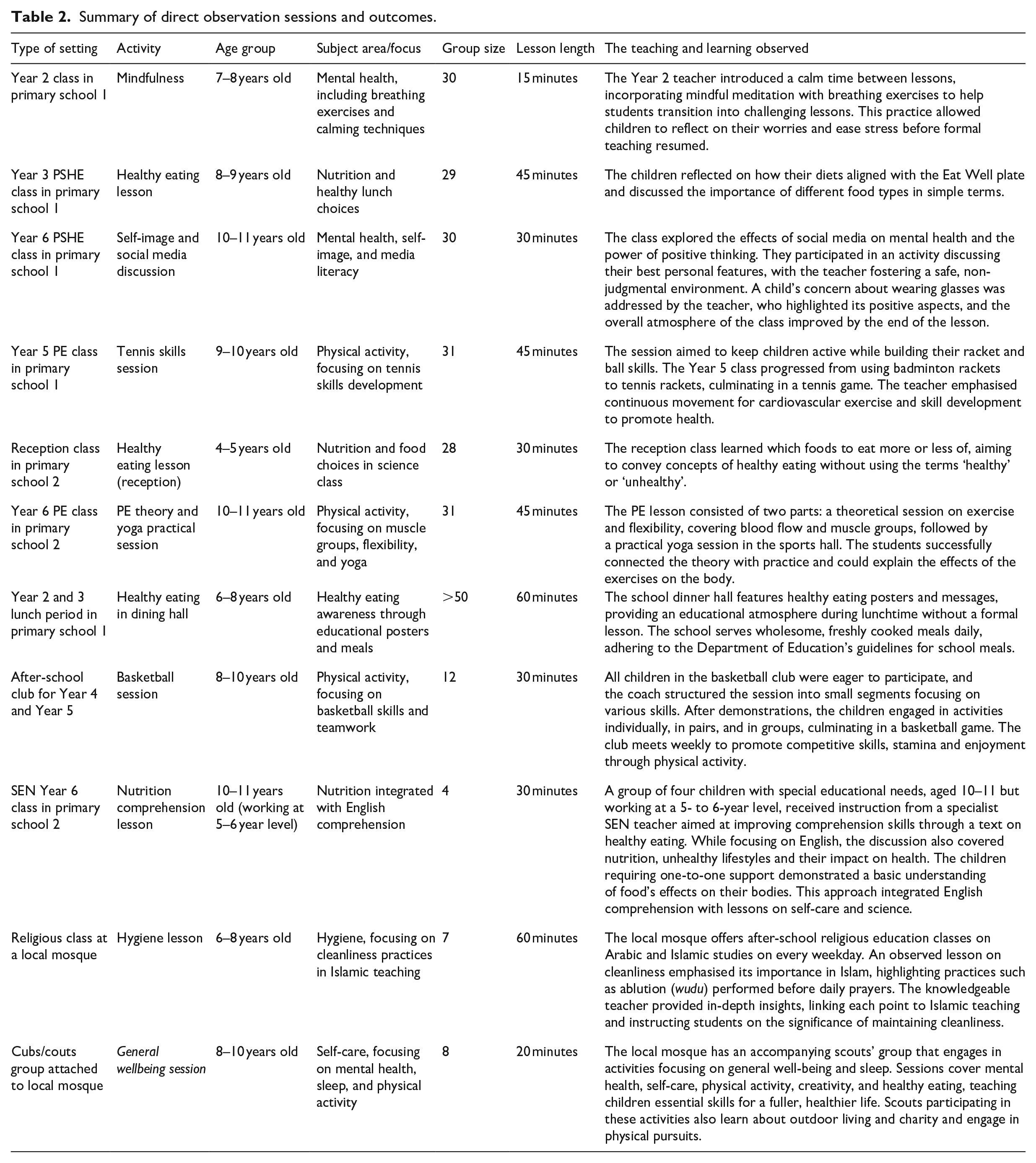
The reception class (4–5 years old) learned about healthy eating in their science lesson, with age-appropriate discussions. Some children shared insights learned at home, such as being encouraged by their mothers to choose more fruit over chocolate.
The school prioritised healthy eating in its dining hall, offering fresh meals that were cooked from scratch. Reception to Year 2 (4–7 years old) students received free school meals, and staff were trained to accommodate any special dietary requirements. Educational posters and nut-free options were prominently displayed. Guidance on packed lunches was available on the school website and regularly emailed to parents.
In the special education needs class observed, four children aged 10–11 years worked with a nutrition-focused text to improve both their comprehension of the English language and their understanding of healthy eating. The teacher provided individual support, incorporating activities that addressed both comprehension skills and nutritional knowledge, thereby enhancing their overall learning experience.
Physical education
The importance of physical education was strongly emphasised in the school observed, which offered lunchtime and after-school clubs for ball activities.
A Year 5 (9–10 years old) physical exercise (PE) lesson with a focus on tennis skills was observed (Table 2). Some children had prior experience of racket skills, while others were using a racket for the first time. Throughout the observation, students were engaged, running, working in pairs, and developing their skills individually, with a noticeable improvement in both skills and confidence. The continuous movement engaged in indicated substantial physical activity, and many students appeared out of breath.
In a Year 6 (10–11 years old) PE class in the same school, students demonstrated a basic knowledge of human body parts and applied principles of science and anatomy to their physical education. The students also practised care in their stretch activities to avoid overstretching particular muscles or muscle groups, as instructed by their teacher.
Mental health
A Year 2 (6–7 years old) mindfulness class in primary school 1, included 30 children, focusing on breathing and ‘time out’ to enhance mental health (Table 2). Following the lesson, the students reported feeling more relaxed and prepared for what followed, expressing comfort and self-acceptance. The activity provided an opportunity for students to voice concerns about any matter that might be worrisome to them, and their calmer demeanour reflected increased composure and focus. Although not part of the official curriculum, the school supported the teacher by scheduling this activity for the class’s well-being.
In a Year 5 (10–11 years old) PSHE lesson in primary school 1, 29 students discussed self-image and social media influences. All students initially shared negative comments about themselves. To counter this, the teacher encouraged them to pair up and identify positive attributes in one another, which helped build confidence and foster a sense of positivity. The teacher emphasised the value of personality and kindness over appearance, reinforcing the importance of positive self-image and self-respect for overall health and well-being.
Religious setting
Seven students were observed in a religious education class that took place inside a local mosque. This learning environment differed from that commonly found in schools, as children sat on the floor and wrote in their books while the teacher dictated. The walls were bare, adorned only with calligraphy frames. The teacher frequently paused to demonstrate specific actions related to cleanliness rituals such as handwashing, face, arms and feet washing, and the children followed the instructions attentively. Emphasising cleanliness, the teacher linked health, the environment and faith, highlighting the need to be clean before attending class.
In addition, the madrasah had a scouts’ group. An observed activity for cubs (8–10 years old) focused on general well-being and sleep. Older scouts offered sessions on mental well-being, self-care, and healthy habits such as getting sufficient sleep, physical activity, and creativity. Children participating in the scouts group also learned outdoor skills, the importance of engaging in charitable activities, and enjoying PE.
Discussion
This study highlights significant variations in the self-care education provided to primary school-aged children in an area of England. Although the National Curriculum in England provides a description of key topics to be included, it does not provide detailed guidelines on how each subject should be taught (Leite et al., 2020).
The healthy eating sessions observed in this study suggest that students progressively deepen their understanding of nutrition as they advance through their education. Resources such as the Eat Well plate illustrate the different food groups and their nutritional benefits (Harland et al., 2012). While the curriculum requires learning about nutrition, including the roles of macronutrients, there was a noticeable lack of emphasis in the educational settings observed on the consequences of unhealthy eating habits. Previous research has pointed out the ambiguity of school-based health education, resulting in inconsistent content delivery by teachers (Oates, 2011).
Evidence of progression could be observed in this study, with younger student classes being presented with only basic information about nutrition, while older students engaged with more complex concepts. Importantly, schools have the flexibility to decide how they will teach the curriculum and decide on age-appropriate content, allowing for the use of a spiral approach where topics are revisited and deepened over time (Tirol, 2022).
The Healthy School Meals campaign across the UK, led by the celebrity chef Jamie Oliver, sought to improve the quality of school food and combat childhood obesity (Naik, 2008). Evidence reveals a positive correlation between nutritious diets and improved behaviour and academic outcomes (Bellisle, 2004). With projections in the UK indicating that one third of children may be obese or overweight by the end of primary school (Ijaz et al., 2021), it is crucial to recognise that unhealthy dietary patterns established early can persist into later life (Anderson and Butcher, 2006). Through the careful use of reinforcement, schools can promote healthy eating in both classroom settings and during lunchtime, fostering positive dietary habits among students (Manolev et al., 2019). Curriculum flexibility also allows for interdisciplinary teaching, exemplified in the Special Educational Needs class observed where nutrition education was integrated with a focus on comprehension skills.
The COVID-19 pandemic in England heightened the focus on mental health awareness, with many primary school children lacking critical developmental skills due to lockdown during the pandemic (El-Osta et al., 2021). To support students in the transition back to in-person learning, some teachers have ntroduced mindfulness sessions, which, while not part of the National Curriculum, support learning and encourage students to voice their concerns (Sapthiang et al., 2019). Observations in this study indicated that these sessions had a positive impact on students, helping them develop vital self-care skills.
In addition, the Year 6 teacher in primary school 1 addressed the mental health impact of social media by facilitating discussion about self-image and confidence as part of a PSHE lesson. Engaging in conversations such as this can help mitigate the negative self-perceptions that often come with social media use (Mumber et al., 2022).
Finally, observations within a religious education setting underscored the importance of cleanliness and self-care in Islam (Özdemir and Frank, 2000). Similar principles are evident in Judaism and other religions, where rituals such as handwashing are emphasised (Klein, 2021). In contrast to the primary school settings focused on, teaching in religious environments of the kind focused on here tends to be heavily structured, reflecting the choices parents make to provide their children with a religious education.
Implications for school health policy, practice, and equity
This study highlights the crucial role schools play in delivering self-care education to young children, revealing significant variations across different educational settings. The lack of a standardised curriculum led to interesting variations in approach and health knowledge, influenced by whether the setting fostered learning through a curricular, an extracurricular or a religious education approach.
Developing a national policy framework for a self-care curriculum could ensure equitable access to high-quality health education for all children, regardless of socioeconomic status or geographical location. Such an approach could aim to equip all students with self-care skills, such as healthy eating, mental health awareness, physical activity and hygiene.
Integrating self-care education as a core component of the national curriculum, rather than as an addition to it could have an important role to play in the delivery comprehensive health education across a range of learning environments, including extracurricular clubs and religious schools. Achieving this, however, requires public consent and collaboration between schools, public health agencies, and others to create teaching and learning activities tailored to the needs of diverse student populations and address disparities between advantaged and disadvantaged groups (Osman et al., 2024).
Limitations
This study is the first ethnographic exploration of self-care education among primary school-aged children. Its strengths include the researcher’s non-participatory role, which sought to reduce bias and allowed for natural interaction between teachers and students. However, some serious limitations must be considered. The small sample size – only 4 educational settings and 11 sessions – means that the study’s findings cannot be considered representative in any way, making the research exploratory rather than definitive.
In addition, informal self-care education settings, such as assemblies and parental meetings, were not included, potentially overlooking important influences on children’s self-care and health-related knowledge. While evidence of the use of spiral curriculum approach was noted, the observed lessons lacked explicit links across year groups.
Future research should involve a broader and more diverse sample to capture the full range of educational practices in a wider range of educational settings.
Conclusion
This study aimed to evaluate how self-care education is delivered to primary school-aged children in England. The findings revealed considerable variation in teaching methods and content across different educational settings, with topics such as healthy eating, mental health, and hygiene commonly included. While the study highlights the potential of early self-care education, it also identifies gaps in standardisation and alignment with health promotion goals. These insights contribute to understanding current practices but are limited to the observed settings, warranting further research in a range of different contexts.
Footnotes
Acknowledgements
The authors thank the key personnel who facilitated access to the educational settings observed.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The University of Birmingham’s Ethical Review Committee approved ethical permission for this study (approval number ERN_21-1091).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.