
Abstract
Objective:
Schools and the education system are powerful tools for cultivating healthy lifestyles. This research focuses on characterising the factors contributing to the development of health-promoting schools in Israel, and understanding how schools can offer a framework for improving students’ health. Fullan’s triple change model with its focus on three phases in the change process in schools – the initiation phase, the implementation phase and the institutionalisation phase – served as a framework for analysis.
Design and setting:
This qualitative-constructivist study involved the analysis of data collected from 26 elementary school principals in Israel, 15 of whom belonged to the health promotion school network (HPSN) and 11 who did not. In addition, 10 health promotion leaders from within the schools were interviewed.
Methods:
Data collection took place by means of semi-structured interviews. in which the questions asked referred to the three phases identified in Fullan’s process of change model. We analysed the data using thematic content analysis.
Results:
Each identified theme was associated with one of the phases proposed in Fullan’s model of change. The initiation phase included collaboration with key stakeholders, principals’ personal commitment, and dissemination of ideas through personal connections. The implementation phase included gaining access to appropriate tools and materials, action to deal with barriers to change, and the creation of a holistic health promotion environment. The institutionalisation phase included the development of administrative strategies such as adherence to routines, the inclusion of regular events in the school calendar, and the allocation of time frames for the activities undertaken.
Conclusion:
Fullan’s model proved useful in analysing efforts to develop health-promoting schools. The model signalled the importance of using a structured approach throughout the institutionalisation phase in a manner attuned to the unique nature of the school. Alongside identifying key factors that support assimilation, it is crucial to assess their integration into the school culture. The school principal’s role is critical throughout all the phases of the development process.
Introduction
Childhood is an opportune moment for the development of healthy habits (Story et al., 2009). In the light of this, and in view of the fact that obesity among children is on the rise internationally (World Health Organization [WHO], 2020) and in Israel (Regev et al., 2019), it is important to implement health promotion in schools. In many countries, health promotion programmes in schools are based on the WHO’s (1986, 2020) concept of the health-promoting school (HPS). HPSs aim to improve students’ knowledge, attitudes, skills and behaviours in relation to health (Kann et al., 2007).
WHO has identified several barriers to the implementation of the HPS programmes, including lack of policy and guidelines for implementation as well as the absence of a lobby working for the cause. In addition, lack of coordination between government departments and key stakeholders hinders uptake and assimilation, as do cultural barriers and lack of evaluation (WHO, 2020).
Factors that help an HPS programme to succeed include providing training for staff, appointing a leader for the programme and receiving administrative support (Velardo and Drummond, 2019). School principals testify that parental involvement helps drive change, and therefore the wider community should be involved in the process (WHO, 2020).
In a review of articles to establish a scientific foundation for the HPS approach, eight components were identified as central to success: preparation for the development in the school, policy and institutional anchoring, professional development for staff, sound leadership and management practices, good organisational support, student involvement and participation, partnership building and networking and planning and action for sustainability (Samdal and Rowling, 2011).
According to Fullan et al.’s (1980) triple change process model, there are three phases characteristic of change processes in schools: The initiation phase, in which a new plan is launched; the implementation phase, in which the change is introduced into practice; and the institutionalisation phase, in which the change becomes an integral part of the organisation (Fullan et al., 1980; Oplatka, 2015). There are several factors that facilitate the initiation phase: the number of innovations and their quality; accessibility to information, as well as the dissemination of innovation through personal contacts (conferences, meetings and workshops); and training for the team that will lead the change (Fullan et al., 1980). Importantly, in a study in Australia that included interviews with staff members, teachers testified that personal support from school principals in the implementation of a new programme led to an improvement in the atmosphere in the school and an improvement in results (Mohammadi et al., 2010). Furthermore, while some school principals may feel uneasy about assuming their role in change leadership, they recognised its necessity when overseeing to turn a school into an HPS (WHO, 1986, 2020) programme (Adams et al., 2023). In the initiation phase, support from the district, the national or local ministry of education and external agents such as organisational consultants can also influence the process (Fullan et al., 1980).
This is consistent with the conclusion of the WHO (2020) that the lack of policies, guidelines and coordination between governments and key stakeholders (schools, health institutions, academic bodies, leaders in the community etc.) pose barriers to implementation. In interviews conducted with staff members in primary schools in Australia, participants described the importance of receiving administrative support and resources (Velardo and Drummond, 2019). Findings from a survey in the USA reinforce this claim and suggest that over 70% of the schools that implement health promotion programmes did so because they were supported in doing so by the state or a school district (Eaton et al., 2007). In Israel, it has been found that the involvement of key stakeholders such as supervisors from the Ministry of Education, school principals, academic advisors and community leaders can help to integrate a focus on health behaviour into life in school (Hayek et al., 2019).
Another critical factor in the initiation phase is the attitude of the local community and whether it takes the form of pressure, support or opposition (Fullan et al., 1980). Important also are the views of guardians and parents (WHO, 2020). In Israel, especially in many higher income status communities, parents are deeply involved in schools and have views to express about new programmes and change (Oplatka, 2015).
In the implementation phase, it therefore is important to calibrate the change to the unique character of the school and the community it serves. Fullan et al. (1980) have identified a number of factors related to the characteristics of change in schools. They include its depth, the extent of implementation by teachers and their ability to understand it. In a study in Australia, both staff and students suggested that it was important to ‘tailor’ an HPS to each school so as to align with its principal characteristics (Mohammadi et al., 2010).
In the institutionalisation phase of work, the goal was to change an enduring feature of the school. Changes are best assimilated over time when the learning that takes place in the school deepens and there are administrative arrangements to support it, which include work frameworks, resources, assessment and a clear development process (Oplatka, 2015). In interviews in primary schools in Australia, it was found that providing staff training and appointing a programme leader facilitated the ongoing implementation of the health promotion programme (Velardo and Drummond, 2019). In addition to providing a positive experience for the teachers, when implementing health promotion programmes, attention must be given to the quality of students’ experiences and their relationship with teachers (Samdal et al., 1998). A study in 96 schools in the USA found that working with the entire school community is important in facilitating the institutionalisation of programmes to promote health (Osganian et al., 2003).
Health promotion programmes in school based informed by the HPS framework have been implemented in many countries (WHO, 1986, 2018). In Israel, the Ministry of Education has developed health promoting programmes in schools informed by the principles in the Ottawa Charter for Health Promotion (Ministry of Health and Ministry of Education, 2022). Some schools belong to the health-promoting schools network (HPSN). Other schools do not, but nevertheless carry out health promotion activities. A school that is interested in gaining recognition as an HPS and which joins the network must develop a long-term programme, appoint a health leader, develop an annual plan and conduct staff training (Tesler et al., 2014).
According to Hayek et al. (2019), several factors support the success of health promotion programmes in schools, among them the publication of official standards by the Ministry of Education that can set out what needs to be achieved. In addition, training programmes for school principals and senior teachers can enhance awareness, and lead to successful implementation. Health promotion works best when it is an integral part of the ongoing curriculum in subjects such as physical education, social sciences and biology. To strengthen commitment, students should be involved in planning, and schools should seek the involvement of parents in programme design (Hayek et al., 2019).
Against this background, this study sought to contribute to the current understanding of how schools can offer a framework for improving students’ health. Its aim was to characterise the factors contributing to the development and institutionalisation of HPS in Israel as perceived by school principals and health promotion leaders. Fullan’s triple change model as detailed above serves serve as the framework for analysis.
Methods
Our work took the form of a qualitative study with data being collected by means of semi-structured interviews with school leaders (Elo et al., 2014), with a focus on the phases identified in Fullan’s change model. After a pilot interview had been undertaken, minor changes were made to the data collection instrument. Questions asked included the following: “Describe the process of developing the health promotion programme (when did you start, what was the trigger for it; How did you become exposed to the idea of health promotion in schools?); What difficulties did you encounter when you decided to start the programme, and How was the programme adapted to the needs of the school? Further examples of the questions asked are available via the following link: https://docs.google.com/document/d/1qG5Umcoi0NgBD_KesW2DY-MGGEwVIstNXqZmkmOGALQ/edit?usp=sharing
Participants
In Israel, elementary education (grades 1–6, ages 6–12 years old) takes place in four main sectors: Jewish secular, Jewish religious, Jewish ultra-Orthodox and Arab (Knesset, 2022). Three of these sectors were included in this study but we excluded the ultra-religious sector due to its reluctance to participate in research. To ensure a reasonably representative sample, multi-stage cluster random sampling took place to create three initial clusters.
Two sub-clusters were then sampled from within each sector, distinguishing between schools that were affiliated with the HPSN and those that were not. Locating suitable participants in both clusters was undertaken using lists of elementary schools and health promotion network affiliations sourced from Ministry of Education and Ministry of Health websites. Random sampling of units, defined as schools led by a principal or a principal and health leader, was then carried out for each sub-cluster.
The schools not affiliated with the HPSN underwent further classification after interviews, based on school principals’ reports, using a 3-point scale reflecting their engagement (or otherwise) with health-related activities adapted from Tesler et al.’s (2014) work. Scale values ranged from 1 for no activities to 3 for full engagement but not part of the HPSN (Table 1).
Classification of the schools by level of engagement in health-related activities.
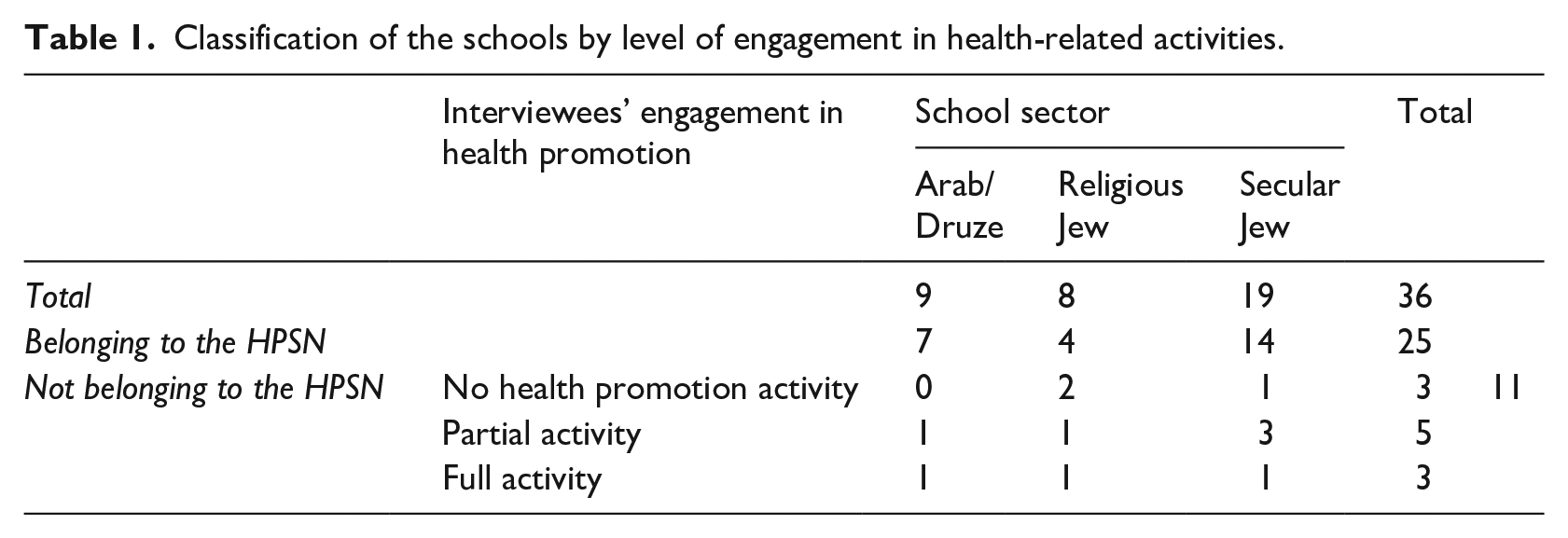
Of the 120 randomly selected schools, 26 agreed to participate, resulting in a response rate of 20%. A majority of school principals (69%) were women, while 31% were men, representing all seven geographical districts in Israel. In addition, interviews were conducted with 10 health promotion leaders in schools, all women, from schools belonging to the HPSN and whose principals participated in the study (Table 1). Since the interviews were conducted on the Zoom platform, informed consent and assurances of confidentiality were documented and the recordings were saved.
Data saturation was reached after conducting 32 interviews, with no new themes emerging. In line with best practice in qualitative research (Shkedi, 2003), four more interviews were then conducted, bringing the total number of interviewees to 36 in total (26 school principals and 10 health leaders).
Interviews
Using the semi-structured interview protocol, 36 interviews were conducted on Zoom lasting about 40 minutes each, between 2022 and April 2023. The mean length of the school principals’ interviews was 30 minutes, and the mean length of the health leaders’ interviews was 23 minutes (online supplemental Appendix 1). I kept (Shkedi, 2003).
The interviewer (A.Z.Y.) had prior experience conducting interviews and had been trained in qualitative research. They were aware that every interview is the product of an interaction between the interviewer, the interviewee and the research field (Shkedi, 2003). During the interview, the interviewer was careful to maintain a balance between personal involvement and a neutral stance to avoid introducing bias.
Ethical approval
The study received ethics approval from the Ethics Committee of the University of Haifa and the Ethics Committee of the Ministry of Education. The details of interviewees were kept confidential. Since the interviews were conducted using Zoom, we made sure that privacy was maintained and only audio recordings were saved.
Qualitative analysis
Thematic content analysis was used to analyse the data. Each interview was analysed separately and then the data were brought together to identify seven independent themes. Each theme was allocated to one of the phases in Fullan’s model. Each of these themes is presented below together with pertinent quotes and accompanying explanations.
Throughout the analysis process, dialogue and critical reflection took place between the two authors. Dialogue between the two researchers took place throughout the analysis to resolve any ambiguities or differences of opinion.
Results
The resultant data took the form of 36 transcribed interviews from school principals and health leaders who collectively came from 26 elementary schools.
Seventy percent of the interviewees were members of the HPSN. Of the remaining 30%, 8% said their school did not conduct any health promotion activities, 14% said it conducted just a few activities and another 8% said it carried out a wide range of health promotion activities.
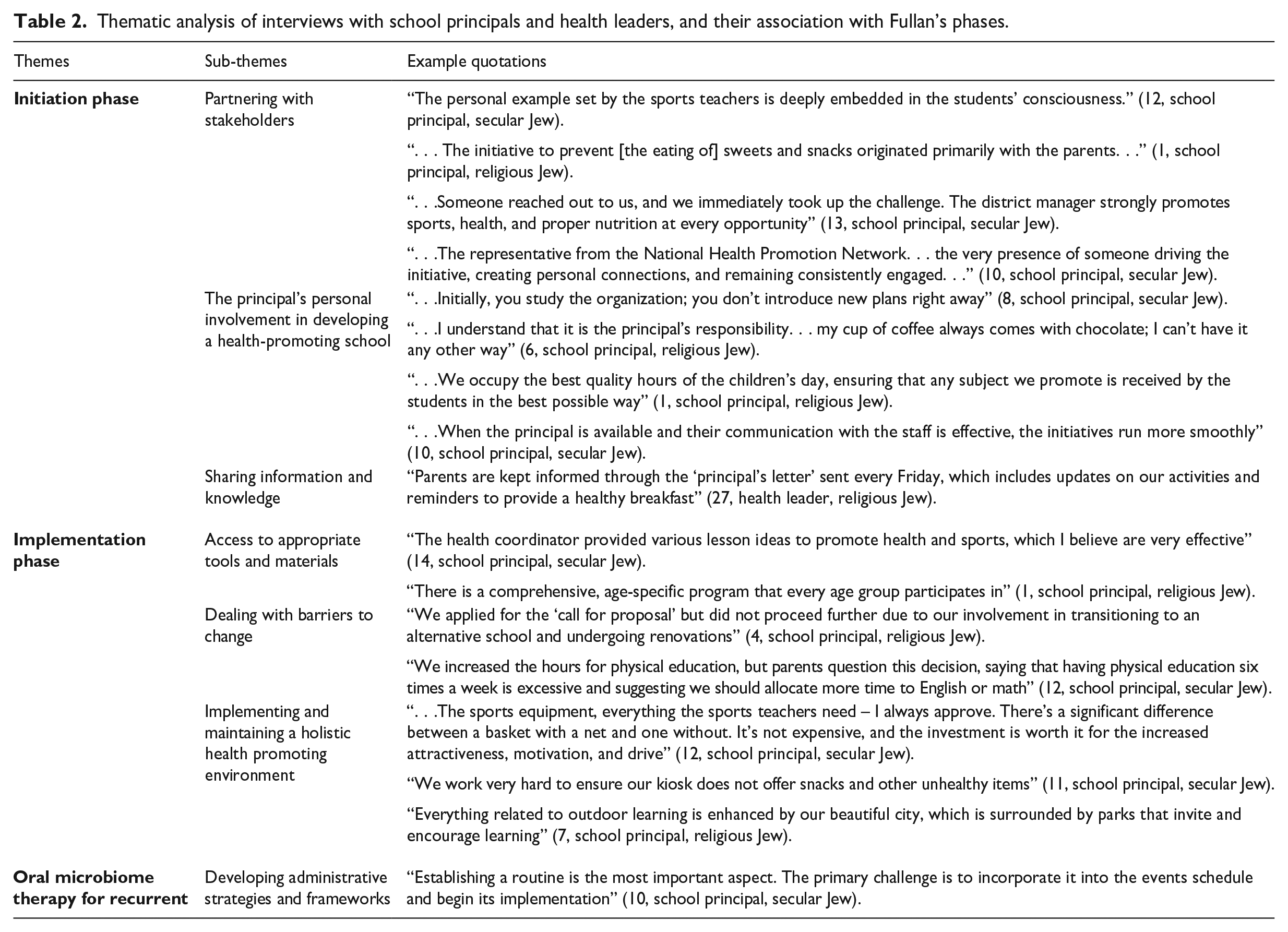
Thematic analysis of interviews with school principals and health leaders, and their association with Fullan’s phases.
Initiation phase
Three themes that were identified as associated with the initiation phase. They were partnering with stakeholders, the importance of the school principal’s personal involvement in developing an HPS, and distributing information and knowledge.
Partnering with stakeholders
Interviewees emphasised the important role of different stakeholders and their active involvement in moving the process forward to facilitate the initial phase. This enabled a shared dialogue and collective brainstorming to develop and customise a suitable approach for the school. Significant stakeholders included partners within the school community such as parents and teachers.
. . . they [the teachers] . . . eat their healthy sandwich with the children, they talk about it . . . (13, school principal, secular Jew) I know that if the coach tells them that, it’s holy of holies. (13, school principal, secular Jew) I presented the programme to the parents. Many nurses, doctors and engineers volunteered and were ready to do their part. (11, school principal, secular Jew)
Stakeholders also made reference to administrative and regulatory bodies associated with the work of the school, such as the Ministry of Education.
. . . Here, each school is given standard hours for physical education . . . and this . . . allows me to add more . . . (1, school principal, religious Jew)
Links between the HPSN, other schools and local sports associations were also seen as important.
[Our work] encourages activities, competitions, partnerships between school communities and other schools. (32, school health leader, secular Jew) I am in contact with the “Parachute House” [a rehabilitation centre for discharged soldiers] in the city . . . we had an activity day there . . . (1, school principal, religious Jew)
The school principal’s personal involvement in developing an HPS
Interviewees stressed the role of the school principal in initiating health promotion efforts within the school. The principal’s personal beliefs about health as well as their views about the influence of the school on student health habits were key factors affecting implementation.
It’s important to bring health into the school environment . . . and share accurate information about life. Education starts at home, but it takes root within the school. (2, school principal, religious Jew) . . . Yes, I know we can be very significant in this matter . . . (5, school principal, religious Jew)
The school principal’s seniority and experience and their status within the school community, as well as the frequency of their involvement in personally overseeing health promotion initiatives, were highlighted as factors influencing success.
. . . In schools where principals have [only] a few years of experience, or need time to establish their position or deal with urgent challenges that require higher priority . . . there [can be] difficulties . . . (10, school principal, secular Jew) . . . [with] a principal who is not there, it will not happen’. (4, principal, religious Jew)
Sharing information and knowledge
Interviewees drew attention to the importance of the school principal leading the way within the school community. Their role encompassed discussion about the need to promote health from a young age. It also included the identification of practical ways to encourage the uptake of healthy practices, both within the school environment and at home.
Having a health promotion leader to lead the process of change through personal involvement was also considered significant.
. . . The ability to appoint a person in charge who is eager and has the ability to speak, to create programmes [is very important]’. (10, principal, secular Jew)
Participants noted that using newsletters and social media could assist with knowledge sharing in the community.
. . . it is written into the school’s regulations . . . parents are aware . . . it’s something that is in the school’s DNA . . . (3, school principal, religious Jew)
Engagement with the whole school community including parents was seen as very important.
Implementation phase
In this phase, and assuming that the significance of an HPS approach has also been communicated to stakeholders, it is crucial to equip teachers with the necessary tools to translate ideas into tangible practices. Three themes that were identified as associated with this phase were as follows: access to appropriate tools and materials, dealing with barriers to change and implementing and maintaining a holistic health-promoting environment.
Access to appropriate tools and materials
Interviewees expressed how being exposed to practical ideas and existing programmes served as inspiration to design content tailored to the school.
Teachers . . . and principals also want to see a programme. They won’t copy . . . but you will see an example of how it works. (8, school principal, secular Jew)
They emphasised that each school should have its own unique programme.
If you find something, a need in the school that connects to it . . . [with] any programme you want to introduce, you can be a little flexible and adapt it to things that come up within the school and integrate it . . . (8, school principal, secular Jew)
In addition, participants stressed the need for a structured plan to ensure the ongoing implementation of health promotion throughout the school, covering all relevant fields of knowledge and practice.
Our whole educational belief at school is based on this. We . . . define our uniqueness [through] – ‘sports and health . . .’ (13, school principal, secular Jew)
Dealing with barriers to change
Ongoing processes of change within the school can pose a barrier to the successful implementation of health promotion. Another significant obstacle could be parental objection to the type of food students are allowed to bring to school or the allocation of specific time for sports and health promotion compared to what they perceive as more important subjects like mathematics.
Some parents are difficult to communicate with, and persist in sending cakes and sweets to the school, despite efforts to encourage healthier options. (17, school principal, secular Jew)
According to school principals, the more effectively the school administration can deal with these barriers, the greater the likelihood of successfully implementing HPS work.
Implementing and maintaining a holistic health-promoting environment
An optimal environment for health promotion entails having adequate and well-maintained sports facilities. It also involves allocating resources appropriately. In addition, the school environment should facilitate access to nutritious food. This means ensuring that pupils and teachers bring with them not only a healthy breakfast from home but also the availability of wholesome options in the cafeteria and microwave ovens for students to heat up the meals they have brought from home.
. . . a healthy breakfast throughout the year. I know that they are already accustomed to having a sandwich, vegetable, and fruit for breakfast. (14, school principal, secular Jew)
As part of an overall environment to encourage healthy lifestyle development, students and teachers should work together on health committees, in project development, and in other ways. School principals who were successful in gaining access to open spaces surrounding the school such as nearby parks, and incorporating outdoor learning, were especially successful in implementing health promotion initiatives.
Our proximity to the park . . . literally within walking distance . . . we encourage lessons in nature . . . (1, school principal, religious Jew)
Institutionalisation phase
In this phase of work, it is important to establish mechanisms to maintain change over time. One theme was associated with this phase.
Developing administrative strategies and frameworks
School principals emphasised the importance of institutionalising health promotion within the school. Establishing routines, such as regular meetings of the school management team and with teachers to develop topics and materials related to health, is central in this respect. Scheduling health promotion events as part of the regular school calendar helps ensure health promotion remains high on the agenda. Allocating regular time slots and incorporating health-related lessons into students’ weekly schedules covering topics such as physical activity and nutrition are key ways of ensuring health promotion inclusion.
I put in four hours of physical education during the week . . . another hour of play time . . . that’s five hours . . . every day they engage in such physical activities. (10, school principal, secular Jew)
Discussion
Analysis of the interviews identified seven main themes. A closer look at the themes enabled us to associate each of them with one of the phases in Fullan’s model (Oplatka, 2015). Three of the themes corresponded to the initiation phase, three of them corresponded to the implementation phase, and one theme corresponded to the institutionalisation phase.
During the initiation phase, the active involvement of a variety of stakeholders in health promotion is crucial, echoing Fullan’s emphasis on the need for support to change agents (Oplatka, 2015). Parental involvement, proactive support by the Ministry of Education and the local authority, teacher partnerships and support from health promotion networks were also highlighted as important in enabling the success of a healthy school. The appointment of a dedicated health leader with appropriate compensation for the role was also seen keys for success. It is important for teachers to set a positive example for students. This includes actively choosing nutritious meals to eat alongside students and engaging in conversations about sports and physical activity. It is important for teachers and coaches to express interest in students’ physical activity and provide encouragement to maintain a healthy diet.
Parents are also important in driving the process. They can do this by showing an understanding of the value of health promotion, volunteering to give talks and supporting activities in the field of health. The significance of partnering with the Ministry of Education and the local authority lies in their capacity to support and foster engagement in health promotion initiatives. These organisations can prioritise health promotion by allocating budgets for physical education time and related activities. In addition, they may arrange for schools to participate in district-wide activities, with participation being strongly encouraged.
Members of the HPSN highlighted the various ways in which the network had supported them, especially in the initial stages of work. This included the provision of tools for HPS planning, ideas for practical activities, conferences and meetings and facilitating exposure to initiatives in other schools. The network was also seen as fostering convivial relationships and providing a contact person who could disseminate relevant materials.
In addition, school principals’ motivation, perception of health promotion and availability highlighted as influential factors in this phase of work. Principals emphasised the importance of a thorough understanding the organisation before implementing any changes. Therefore, the tenure of the principals and the level of trust bestowed upon them by the community are significant factors. Principals stressed that when a school principal adopts a health-conscious lifestyle, it can influence the entire school environment. Conversely, when school principals are not actively involved in health promotion, they may have difficulty encouraging the uptake of healthy habits by students.
Finally, by engaging with the local environment and establishing connections with community sports centres, schools can enhance and expand sports activities, thereby increasing participation.
Fullan et al. (1980) emphasised that the second phase of change (implementation) requires linking the change to the unique character of each school and developing a plan to integrate change into the school’s everyday practice. In this study, school principals and health leaders independently mentioned the importance of adapting the programme to the school taking advantage of opportunities within the school and its surroundings. In a study in France, efforts to implement a health-promoting environment in elementary schools did not proceed as planned because of a mismatch between the conceptual framework for the work and the opportunities available in the individual schools themselves (Darlington et al., 2018). Ultimately, a single programme cannot be introduced in the same manner in every context. There is a need to tailor programmes and interventions to each school and its context. In this study, interviewees noted that implementation and assimilation of new initiatives are more effective when a wide range of teachers actively participate and health promotion is integrated across multiple fields of knowledge.
According to Fullan et al. (1980), many change processes in school never reach the stage of institutionalisation. Changes are assimilated only when the learning that takes place in the school deepens, when there are administrative plans in place and when there is a clear development process to facilitate institutionalisation. One of the models can be used to implementing HPS programmes is the RE-AIM model, developed by Glasgow et al. (1999). According to this model, intervention effectiveness is dependent on five factors, the final factor being maintenance – to ensure the programme’s continuity. Maintenance has two distinct aspects: the sustained operation of the programme and the continuity of the desired change it aims to bring about. Interviewees in this study especially noted that the existence of regular, consistent and recurring health promotion activities and the integration of health promotion work into a range of different fields of knowledge contributed to the sustained operation of programmes.
A review by Herlitz et al. (2020) suggested that the sustainability of health interventions in schools (and ultimately their institutionalisation) is dependent on schools developing and retaining senior leaders and staff who are knowledgeable, skilled and motivated to continue delivering health promotion in changing circumstances. Belonging to a network of schools can help in this respect by providing opportunities for interaction communication and support in peer meetings and in other ways.
Strengths and limitations
Taken together, findings from this study shed light on the key elements of successful health promotion programmes in elementary schools, as aligning with Fullan’s model. They provide valuable insights for directing resources and planning, implementing and institutionalising health promotion in elementary schools. However, it is important to acknowledge the limitations of this study. Throughout the study, interviewer bias may have influenced responses, and the perspectives of school principals and school health leaders who declined participation were not captured. In addition, there is a growing body of research suggesting that school culture has an important role to play in influencing the outcomes of any process of change (Hinde, 2004). Shared relationships between members of the school community matter when it comes to implementing of blocking change. Future research on the implementation and integration of HPS approaches should seek to elicit the perspectives of a variety of different school community members in order to develop a more comprehensive understanding. In future research, it may also be desirable to utilise quantitative methods in partnership with the approaches used in this study to add value to our understanding of the process of implementing HPS programmes.
Conclusion
In this study, the qualitative accounts provided by school principals and health leaders were largely aligned with the stages identified in Fullan’s model which views educational change as an ongoing process rather than a one-time event. Knowledge of these stages may assist in the planning, implementation and institutionalisation of future forms of health promotion in elementary schools. Findings indicate that the enthusiasm and commitment of school principals is central to success in developing HPS work, alongside community and stakeholder engagement. Providing teachers with access to high-quality resources and materials, implementing a structured curriculum with adequate time for health-related activities and ensuring the school’s adeptness to overcoming challenges are important next steps. Sustaining health promotion necessitates creating an environment which is conducive to healthy behaviours, physical activity and good nutrition. Ongoing mechanisms are needed, however, to monitor, evaluate and support health promotion efforts.
Supplemental Material
sj-docx-1-hej-10.1177_00178969241279284 – Supplemental material for Factors contributing to the development of health-promoting schools, applying Fullan’s triple change model – A qualitative study
Supplemental material, sj-docx-1-hej-10.1177_00178969241279284 for Factors contributing to the development of health-promoting schools, applying Fullan’s triple change model – A qualitative study by Ayala Zak Yehuda and Orna Baron-Epel in Health Education Journal
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.