
Abstract
Background:
Sexual and reproductive health education is central to both international and national public health policy and priority action areas. However, menstruation education remains peripheral in both policy and school curricula. This article aims to investigate the extent and depth of menstruation education in Australia available outside of mainstream education channels.
Methods:
We conducted an inductive content analysis of publicly available Australian sexual and reproductive health educational resources targeting young menstruators and parents, which at least mentioned menstruation. Resources were accessed via a desktop search (using Google) to ensure that they were accessible to the public and were provided by not-for-profit or government organisations.
Results:
We identified a total of 31 resources from 10 organisations and subjected them to conventional content analysis. Our inductive coding process focused on the extent and depth of menstruation content. The main content areas included a discussion of pads and tampons, menarche, period pains, when to see a doctor and pre-menstrual syndrome. Three key themes were identified across the resources: holism, normalisation and managing menstruation.
Conclusions:
We develop recommendations for organisations developing or improving their menstruation resources and offer future direction for sexual and reproductive health policy and education in Australia that is inclusive of menstruation. The recommendations relate to the three themes identified during the analysis and include concepts such as recognising the biological changes that come with menstruation, variation of menstruation experiences, normality and assumptions about menstruation and menstrual hygiene management.
Introduction
Sexual and reproductive health education is central to international public health agendas that seek to reduce risks of sexually transmitted infections and unplanned pregnancies and prepare adolescents for adulthood (Walsh-Buhi, 2018; Williams and Davidson, 2004). Broad in scope, sexual and reproductive health encompasses puberty, pregnancy, sexuality and menstrual health, with the understanding that being sexually and reproductively healthy and educated constitutes a human right (Starrs et al., 2018; Winkler and Roaf, 2014), and is central to health and survival, sustainable and economic development, and the overall well-being of humanity (Winkler and Roaf, 2014).
In this article, we present an analysis of freely available menstrual education in Australia. We acknowledge that many people who have ovaries, a uterus or vagina do not identify as female and that many people who identify as male have ovaries, a uterus and vagina. We intentionally use the gender-neutral term menstruators to focus on the biological function of body parts rather than the gendered constructions of bodies, as we acknowledge that gendered constructions do not account for the experiences of many transgender or non-binary people or those with intersex variations. While our analytical attention is directed towards the extent and depth of menstruation content of freely available resources, we believe beginning with an inclusive definition is paramount to ensure we do not exclude the experiences of people who identify as non-binary and/or trans and people with intersex variations.
Menstruation 1 is a natural monthly occurrence of vaginal bleeding for most menstruators who have reached puberty and is vital to a functioning reproductive system (Chandra-Mouli and Patel, 2017). Even though menstruation is a normal and healthy biological function, we argue that there is little consideration of this dimension of reproductive and sexual health across international bodies, policy and literature. For example, the World Health Organisation (WHO, 2021), while defining sexual and reproductive health as separate concepts, makes no explicit mention of menstruation or menarche. By comparison, the Guttmacher-Lancet Commission (Starrs et al., 2018) presents a single definition of sexual and reproductive health, which acknowledges as a component of reproductive health, alongside entitlement to private, dignified and hygienic management of menstruation (Starrs et al., 2018). Beyond this, there is no further elaboration of menstruation; an absence that has been noted by several scholars (Phillips-Howard et al., 2018).
In Australia, national and local sexual and reproductive health priorities have demonstrated a similar lack of commitment to menstrual health. At a national level, a recent National Women’s Health Strategy identified maternal, sexual and reproductive health as one of five priority health issues. Despite the inclusion of family planning, sexually transmitted infections, reproductive health, maternal health and breastfeeding as key issues, there was no mention of menstruation (Department of Health and Aged Care, 2019). This is also evident at state level where despite ‘aiming to empower women’, Queensland’s current Sexual Health Strategy (Queensland Health, 2016) omits any mention of menstruation or menstrual health.
Recent reviews of Australian sexual and reproductive health education have similarly reflected an absence of menstruation content (Collier-Harris and Goldman, 2017; Williams and Davidson, 2004). In addition, a review of Australia’s school curricula on sexual and reproductive health targeting young people aged 6–16 (school years 1–10) found little evidence of puberty-specific content and limited mention of menstruation (Collier-Harris and Goldman, 2017). Taken together, these reviews and recent policy documents reflect Australia’s narrow sexual and reproductive health focus. This suggests that mainstream educator’s roles in delivering puberty and/or menstruation education lacks specific curriculum guidelines. As a result, the content of this education varies between education settings and educators raising questions about the quality and quantity of menstruation education young menstruators receive in mainstream education settings.
We view these gaps and omissions as problematic considering empirical links between insufficient menstrual knowledge, awareness and hygiene, cultural taboos, school absenteeism, poor mental health, social stigma and fear and anxiety surrounding menstruation (Miiro et al., 2018; Reingold et al., 1989; Sommer et al., 2016; Sommer and Sahin, 2013). However, they are arguably reflective of a broader socio-cultural context in which menstruation is taboo and highly stigmatised (Thomson et al., 2019). The stigma attached to menstruation is pervasive and has wide-ranging effects, impacting a menstruator’s confidence and capacity to seek information, healthcare, or support throughout the menstrual cycle and/or to manage menstruation with dignity, comfort and safety (Wilson et al., 2018). Furthermore, insufficient knowledge and education of menstruation limits the capacity to identify symptoms requiring further investigation, exacerbates complications experienced during menstruation and limits menstruation health literacy more broadly (Armour et al., 2021; Miiro et al., 2018). These gaps therefore contribute to the inequalities experienced by menstruators.
In terms of menstruation educational materials, scholars have argued that such materials overwhelmingly construct menstruation as an illness and problematic biological function that requires careful ‘management’ with signs and symptoms to be hidden through the use of specific products and medication (DeMaria et al., 2020). There is little if any positive framing; menarche brings with it undesirable changes which the menstruator must learn to cope with (Diorio and Munro, 2000). The majority of such materials are produced by menstrual product companies (Erchull et al., 2002), with the goal of preparing ‘girls to be consumers’ and publishers likely to cover topics that ‘further their economic interests’ (p. 470). In their landmark analysis of menstrual education and advertising published between 1932 and 1997, Erchull et al. (2002) identified an emphasis on secrecy and concealment (with language such as ‘keep fresh as a daisy’: p. 471) and overwhelming attention to the negative aspects of menstruation, such as ‘cramps, moodiness, and accidents’ (p. 469). The authors also found minimal attempts to include reference to the subjective experiences of menstruating and poor evidence of full or accurate descriptions of the physiological aspects of menstruation.
Such constructions see menstrual product positioned as the solution to stigma, facilitating the absorption of all fluid and odours (to ensure minimal ‘leakage’), so as to be invisible through clothing, concealing menstruation and small and unobtrusive enough to carry discretely to the bathroom (Kissling, 1996). This framing situates menstruation within a discourse of capitalism, in which menstruation is a problem to be fixed through consumption, devoid of any socio-cultural context and failing to recognise menstruation as a complex socio-cultural and economic issue (Bobel, 2019).
With this context in mind, we aimed to provide an analysis of menstruation education available to menstruators and their parents outside of mainstream education channels and where commercial interests are less likely to be foregrounded. Our analysis addresses the following two-part question–what is the extent and depth of menstruation content in current sexual and reproductive health education for menstruators and/or parents of menstruators in Australia?
Methods
The data for this analysis were publicly available menstruation resources (e.g. initiatives, materials and programmes) and/or sexual and reproductive health resources developed and funded by both Australian non-governmental and governmental organisations. Academic and curriculum resources were excluded due to the potential for varied education delivered by teachers and educators, driven by the limitations of menstruation content in curricula at the time of analysis. In addition, resources from commercially or financially interested organisations were excluded so as to limit any risk of bias or conflict of interest due to commercial benefits for/of educational material. Resources behind paywalls were also excluded. Guided by discussion of the ethical use of online data (Roberts, 2015), the use of publicly accessible data for this content analysis does not warrant formal ethical clearance The first author conducted searches using Google (Australia) in 2018, to ensure that the resources selected were publicly (and freely) available. Searches were conducted using the terms: ‘sexual health education Australia’, ‘reproductive health education Australia’, ‘puberty education Australia’, ‘menstrual hygiene management education Australia’ and ‘menstruation education Australia’. 2
To be eligible for inclusion, resources needed to be printable (e.g. as web pages or brochures), at least mention menstruation, have been developed since 2010 3 and target Australian menstruators/or parents. Non-printable resources such as videos or audio files were excluded due to the additional analytic layers present, such as animations and tone of voice which were not able to be sufficiently compared with printable resources during analysis. Searches were limited to results displayed on the first three pages (as data had reached saturation), and a three-click rule was implemented. This was to limit the number of clicks required to reach resource and to simulate real-life search. Each Google search identified 27 websites (i.e. 3 pages each listing 9 websites) making a total of 135 websites to assess for eligibility. From these, 117 were excluded, most commonly due to not being educational resources, and 8 being duplicates. The second author conducted a second check of the original 135 websites in 2021 to ensure the final data set met the study’s inclusion criteria. The final data set included 10 organisations with between 1 and 13 educational resources, resulting in a total of 31 posters, diaries and webpages. Target audiences included parents, teenagers and First Nations Australians as well as culturally and linguistically diverse menstruators.
A content analysis was conducted as it is a flexible tool particularly appropriate when existing theory or literature is limited (Hsieh and Shannon, 2005), as was the case in this study. Content analyses allow themes to be inductively identified from the data, keywords and concepts, which together form a coding scheme which is then sorted into themes, forming meaningful clusters of data (Hsieh and Shannon, 2005). We followed this process by first familiarising ourselves with the resources. Using Microsoft Word, the first author began by coding all keywords and ‘topics’ within the resources, insofar as they related to menstruation. For example, period pains and toxic shock syndrome were ‘topics’ that the resources covered and hence became codes. Once the first author had inductively coded all content, the list of content areas was then checked with the third author to ensure no repetition or potential missing data. The first author then coded each resource according to this refined list of content areas, to address the first part of the question about the extent of content coverage across the resources.
The second part of the analysis was addressed by a deeper examination of the content of the resources (depth of the resources). This involved coding using the following questions as a guide: how is menstruation described; what assumptions about menstruation are evident; which aspects of menstruation are focused on and which aspects are absent? In addition, the coding involved attention to the language use, colour and imagery used in the resources.
Throughout the study, the authors held regular data meetings to discuss the resources, particularly as these related to the themes and coding process, resulting in the refinement of the coding process and informing the development of three key themes: namely holism, normalisation and managing menstruation.
Results
Ten organisations, each with at least 1 resource, were included in the analysis, resulting in 31 resources. For clarity and brevity, the results are presented by organisation and presented in summary in Table 1.
Menstruation-relevant content areas of resources ordered, by organisation. a
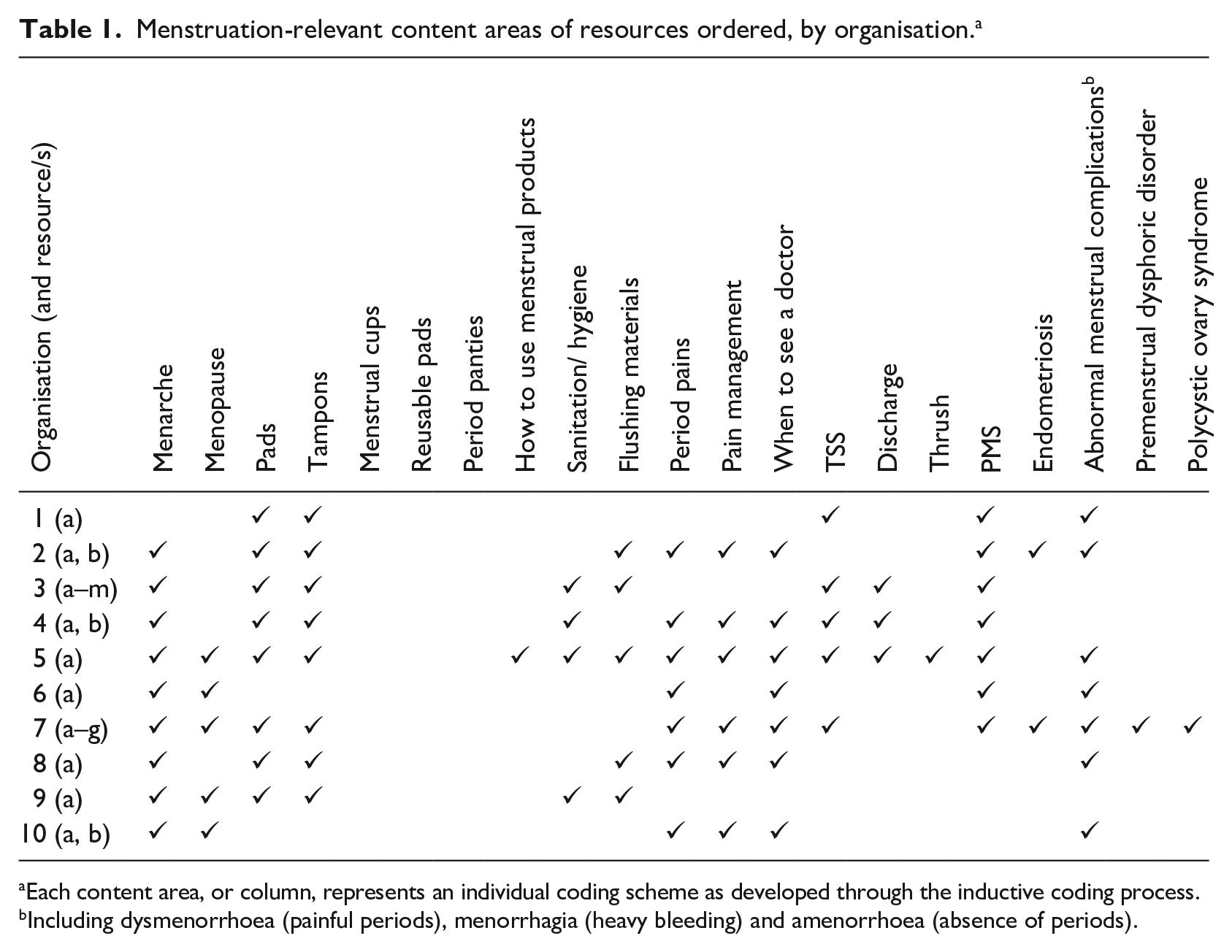
Each content area, or column, represents an individual coding scheme as developed through the inductive coding process.
Including dysmenorrhoea (painful periods), menorrhagia (heavy bleeding) and amenorrhoea (absence of periods).
To address the first part of our research question (extent of menstruation content), we identified a total of 21 content areas across the 31 resources. However, we were interested in the coverage of content by organisation in order to discern patterns and the placement of certain content areas across the data set. Our analysis identified clear patterns in relation to the most and least common content areas. Menarche, pre-menstrual syndrome, period pains, when to see a doctor and pads and tampons were covered by all but two of the organisations. Comparatively, endometriosis, polycystic ovary syndrome, premenstrual dysphoric disorder and how to use menstrual products were only mentioned by three organisations.
We also found examples of high and low levels of content coverage: Organisations 5 and 7 had high levels of content coverage, attending to many aspects of menstruation and puberty. However, Organisation 1 had low levels of content coverage, limited to pads and tampons, toxic shock syndrome, pre-menstrual syndrome and other complications. Beyond these distinct examples of low and high coverage, there was considerable variation in the extent of content coverage across the remaining seven organisations.
In attending to the positioning of menstruation through language use, colour and imagery, we identified three key themes that reflected the depth of content across the data set: (1) holism acknowledging of the holistic nature of menstruation; (2) normalisation normalising the concept of menstruation and (3) managing menstruation through education about menstrual products and infrastructure.
Holism
Holism concerned the extent to which menstruation was presented as inclusive of more than ‘just’ biological changes. All the organisations acknowledged the biological changes and processes related to the menstrual cycle, but most did not go beyond this biological framing. For those that did, menstruation was framed most notably by referencing the associated psychosocial changes, possible experiences of pain and methods for pain management. Psychosocial changes focused on a range of feelings that might be experienced alongside menarche and menstruation including shyness, stress, feelings of isolation, cravings and confusing thoughts. Although 6 of the 10 organisations discussed pain during menstruation, few discussed the nature or type of pain (such as cramps and stomach pain). Recommendations on how to manage the natural symptoms of menstruation were typically medicalised and included visiting a doctor or taking pain medications. We noted a more holistic construction of menstruation was evident where non-medical solutions such as mild exercise, heat packs, herbal remedies and stretching were encouraged. However, overall holistic framings of menstruation were lacking, with little acknowledgement of changes during menstruation beyond the biological level.
Normalisation
Seven of the 10 organisations acknowledged the variety of ages of menarche, lengths of menstrual cycles and menstruation periods. This information was important in serving to normalise differences between and within menstruators. However, few organisations acknowledged that having a menstrual cycle outside of what was considered the ‘average’ length was ‘normal’ or ‘okay’.
Normalisation was also achieved through the visual presentation of resources, with resources targeting different audiences. We noted that resources directed at younger people used bright colours and images, cartoons and had gentle and personable language (e.g. ‘sometimes you may bleed for as little as two days, or sometimes for as many as eight. This range is totally normal’. 5a: p. 10). Humour was also used with members of this demographic, for example depicting the beginning of a menstrual period with a cartoon of a woman opening a door, saying: ‘Vagina! Auntie Flo is staying for a few days!’ (5a: p. 11).
Resources directed at parents on the other hand tended to use minimal colours and relied on text and direct language over visual depictions (e.g. ‘. . . Most of the blood and tissue comes out in the first couple of days . . . The amount of bleeding varies’. 8a: p. 1). Resources targeting First Nations Australians tended to use bright colours and culturally distinct cartoons, with gentler, clearer and more sensitive language (e.g. ‘Monthly bleeding is not something to be scared of because it is perfectly normal’ 3m).
Normalisation was also approached in other ways, for example ‘girls can do everything they normally do, such as run, swim and dance’ (5a: p. 13) and ‘menstruators should not be afraid of their bleeding’ (3m). Statements describing bleeding as a natural experience that does not interfere with daily activities or routines served to position menstruating as a normal and healthy process.
Managing menstruation
The final theme pertained to aspects of managing menstruation and tended to focus on product options and infrastructure. Discussions of pads and tampons as the primary product options were evident, with the choice typically presented as an either/or scenario: for example ‘should I choose pads or tampons?’ (5a). Of the 10 organisations, 7 focused exclusively on pads and tampons. The remaining three organisations included a broader range of products, two of which mentioned period pants, menstrual cups and reusable pads. In terms of the viability of these products, menstrual cups were presented as an alternative to tampons and pads and reusable pads were presented as alternatives to disposable pads. Across all resources, there was little guidance on the benefits of each option, or how best to choose.
Information such as visual instruction or written information on how to use products was limited, potentially assuming that readers would know how to use menstrual products, for example ‘sanitary pads or tampons are used to absorb your period’ (1a: p. 1), or directing them elsewhere for this information, for example ‘. . . pads and tampons can be bought at the pharmacy or supermarket and come with instructions’ (4a). As an exception, one resource provided a textual description of how to insert a tampon.
Only one resource showed examples of the packaging of pads and tampons allowing the reader to know what to look for when purchasing. This was notable given several other organisations only showed images of unpackaged and unwrapped pads and tampons, assuming knowledge of how to identify these products by their packaging on the shelves.
Education on infrastructure was largely absent with a few exceptions, such as a poster advising to dispose of pads and tampons in a bin, not by flushing down the toilet and advice for parents to help their children find a toilet at school with a sanitary disposal bin. In addition, while advice to use sanitary bins is helpful when bins are available, there was no information on how to dispose of menstrual products in the absence of such infrastructure. Reference to sanitation and hygiene was also largely neglected with only 3 of the 10 organisations’ resources mentioning sanitation and/or hygiene, for example, ‘wash your hands before and after inserting a tampon’ (5a: p. 12).
Discussion
The aim of this analysis was to assess the extent and depth of menstruation content within and across 10 organisation’s publicly available educational resources targeting menstruators or parents. Regarding the extent of content coverage, most resources mentioned pads and tampons as the main product options, describing menarche, period pains, when to see a doctor and pre-menstrual syndrome. However, mentions of reusable menstrual products were less common and the topics of premenstrual dysphoric disorder, polycystic ovary syndrome and how to use menstrual products were often neglected.
We identified three themes relevant to the extent and depth of Australian menstruation resources: holism, normalisation and managing menstruation. Holism considered the extent that menstruation education extends beyond biological changes and encompasses psychosocial changes, embodied experiences of pain (such as cramps and discomfort) and both medical and non-medical pain management. We found few of the resources went beyond a biological framing. Simplified or commodified menstrual education is said to ignore structural aspects such as oppression, gender dynamics and the value of local knowledge (Curry et al., 2022). It is therefore essential that organisations adopt a holistic lens to educate and enhance the health literacy of menstruators and parents effectively and comprehensively.
Normalising, the second theme, considered the extent to which differences between and within menstruators regarding bleeding and cycles were acknowledged. Key elements of this theme also included the fact that difference is normal and expected, along with normalising the fact that menstruators will bleed, that bleeding is normal and that it is normal to talk about bleeding. Only a few organisations fully reflected this level of normalising menstruation, which is central to normalising the diversity of menstruation experiences (Przybylo and Fahs, 2020). Furthermore, dismantling menstrual taboos through normalisation is essential to reduce negative social norms and work towards achieving gender equality (Wilson et al., 2018).
The third theme, managing menstruation, considered the extent to which product options went beyond the binary of pads and tampons. We found evidence of major assumption-making regarding prior knowledge around product use, with few resources providing descriptions or images depicting packaging and information on how to use, empty, change or dispose of products. The assumption of sufficient product knowledge for readers has the potential to limit the educational capacity of these resources and/or result in product misuse or non-use.
Our analysis of menstruation education content aligns with previous work with respect to the framing of menstruation as an illness and problematic function. We consider these findings to be influenced by the social and gender inequalities and silences that surround menstruation education. While the menstruation education available (at the time of this analysis) to menstruators and parents outside of mainstream education channels included in this analysis does serve to challenge the findings of previous scholars, we note that there is still much to be done to address silences about menstruation and the structural factors that perpetuate gender inequalities for menstruators in Australia. This is evident in the apparent limitations to the holistic framing of menstruation and discussions of managing menstruation. In what follows, we make recommendations to inform the future development of menstruation education and research.
Implications for practice and/or policy
To address the social and gender inequalities surrounding poor menstruation education and stigma, we argue that future educational resources should be guided by the themes developed in this paper.
Holism involves recognising that the onset of menstruation brings not just biological changes but also psychosocial and emotional changes. Possible experiences of pain during menstruation and non-medical methods for pain management should also be attended to.
Normalising menstruation can be achieved by acknowledging the variety of ages of menarche, lengths of cycles between and within menstruators and acknowledging that some variation is normal, but excessive variation should not be ignored. Menstruators should also be reassured not to be afraid of menstruation, that menstruation is natural and it should not interfere with daily activities – and if it does to seek support. Education and broader awareness of menstruation should also seek to normalise the concept of menstruation itself to reduce any stigma and societal silences that hinder open and safe communication.
Managing menstruation should be encouraged by limiting assumptions about product knowledge, aiming to inform about all types and aspects of menstrual product use, including cost, environmental and infrastructural considerations, images of packaging and information on the frequency of changing. Furthermore, descriptions of how to use products should be detailed and comprehensive.
Future research should evaluate the impact of menstruation education on menstrual health literacy and well-being. While this analysis has dealt with the extent and depth of publicly available resources, an impact evaluation could involve an exploration of how the method of delivery of these resources (online vs face-to-face) could influence their effectiveness and engagement with the content itself.
Avenues for future practice could include advocacy by researchers and health professionals to include menstruation within Australian sexual and reproductive health policy – a notable gap in the Australian context. Researchers should also advocate for discussion about the environmental and financial impacts of different menstrual products.
Limitations
The research sample in the study was limited by its exclusion of resources from financially or commercially interested organisations, do as to reduce any risk of bias or conflicts of interest. The sample was also limited by the number of search pages included in the attempt to replicate a real-life search, which may have excluded eligible resources from this analysis. Furthermore, despite the original dataset from 2018 being checked in 2021 to ensure that the resources were still available for inclusion, we acknowledge the limitations of the age of the data particularly with respect to discussion of, and changes in, menstruation education in recent years.
Conclusion
In summary, this paper argues for the importance of shaping educational resources that attend to all aspects of menstruation. We advocate for both local and international sexual and reproductive health practitioners, policymakers and researchers to acknowledge menstruation as an important element of health and well-being, and more broadly, social and gender equality, in national policy, professional practice and school curricula. Engaging with menstruation from a holistic perspective – which normalises menstruation and the diverse ways of managing bleeding – will enable further progress to be achieved.
Footnotes
Acknowledgements
BB and BW conceptualised and designed the study, conducted the analysis (led by BB) and prepared the original manuscript. CM contributed to the final version of the manuscript preparing it for submission. We thank Nikki Whitmore for her insights on the use of inclusive and non-gendered language in menstruation resources.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.