
Abstract
Objectives:
Among Aboriginal children, the year between birth and 1 year of age has the highest mortality rate compared with any other age. Prompt administration of cardiopulmonary resuscitation (CPR) leads to better outcomes and a lower likelihood of ongoing sequalae. Current education on infant CPR is not provided to parents except in certain circumstances in a neonatal intensive care unit. Currently, there are no identified CPR education courses specifically available for Aboriginal or Torres Strait Islander people, meaning that current infant CPR education courses are not culturally responsive.
Design:
Partnering with an Aboriginal community from the Bindjareb region of the Western Australian Noongar nation, the researchers used a co-design approach and an Aboriginal Participatory Action Research (APAR) design to explore how to deliver culturally safe and responsive infant CPR community education. This resulted in the development of the Koolangka Infant Life Saving Education Framework (KILSEF), which can be used to guide future planning and delivery of culturally safe and responsive community level infant CPR education.
Results:
The study findings identified that members of the Aboriginal community were very interested in receiving infant CPR education, but the barriers identified from mainstream CPR course delivery need to be removed for the community to benefit from culturally responsive ways of learning. Culturally responsive community CPR education should be provided in culturally safe places and the focus of learning should be on the practical applications of CPR and less on the academic pre-reading and written requirements. Explanations should be provided in lay terms and patience is required to communicate ideas in ways that facilitate understanding, and the course may need to be delivered over several days to accommodate community participant availability.
Conclusion:
Addressing Aboriginal community concerns and barriers allowed for the implementation of culturally responsive infant resuscitation education which was highly valued by community members and led to increased community confidence and participation in CPR education.
Introduction
Prompt administration of cardiopulmonary resuscitation (CPR) is crucial to survival in emergencies where an individual has stopped breathing or has had a cardiac arrest (Department of Health, 2018). Currently, infant resuscitation is not habitually offered as part of antenatal or postnatal education for expectant parents in Australia and is often only offered to selected parents of high-risk newborns as part of their discharge planning from neonatal intensive care units (Barry, 2015).
Several studies have aimed to determine how best to teach parents infant cardiopulmonary resuscitation, (Barry, 2015; Barry et al., 2019; Bergamo et al., 2016; Guo and Hampton, 2021; Hollenberg et al., 2019; Knight et al., 2013; Orkin et al., 2012; Pierick et al., 2012; Stephens, 2019), however, as authors we were not able to identify any research that investigated Aboriginal and Torres Strait Islander 1 people’s perspectives on infant resuscitation education. Given the rural and remote location of many Aboriginal Australian communities, timely emergency services access may be not be available dependant on seasonal conditions and/or travel distances. Therefore, first responders are more likely to be parents or members of the community, and first aid courses rarely cover the challenges of performing CPR in remote locations or where emergency services are unavailable (Case et al., 2018; Orkin et al., 2012). It has also been noted that infants (0-12 months) are the most likely group under the age of 18 who would require resuscitation in the general population (Naim et al., 2021).
Among Aboriginal Australian children, the year between birth and 1 year of age has the highest mortality from any cause compared with any other age during childhood and adolescence, with over 80% of deaths in the under-5 age group occurring between the ages of 0 and 1 (Australian Bureau of Statistics, 2019; Shipstone et al., 2019). Although specific numbers vary it has been reported that Aboriginal Australian infants under the age of 1 are between 1.5 and 3.5 times more likely to die of sudden unexpected death in infancy when compared with their non-Indigenous counterparts, (Shipstone et al., 2019, 2020; Zarnowiecki et al., 2018). Given that parents are usually the first to find their child unresponsive, they should have the skills to deliver swift CPR to improve outcomes for the infant (Weinmeister et al., 2018). There is currently no specific infant CPR education designed to meet the distinctive needs of Aboriginal Australian people. This study aimed to answer the following research question:
Research Question 1 (RQ1). What are Aboriginal parents’ and extended family members’ perceptions and understandings of infant cardiopulmonary resuscitation?
Methodology
Design
Using an Aboriginal Participatory Action Research (APAR) co-design approach, this study used an interpretive descriptive design to elicit Aboriginal community participants’ perspectives and understandings of infant CPR education. APAR has demonstrated that health promoting interventions designed by the community are more readily accepted into that community because ownership is maintained (Dudgeon et al., 2020). In the application of APAR, the researchers and community Elders and leaders work together to form a partnership in which they collaboratively formulate the research protocol, develop the research questions, collect the agreed data, distribute the findings back to the community for review and discussion, and adhere to the data sovereignty procedures to disseminate the findings (Dudgeon et al., 2020; Springer and Skolarus, 2019). This type of research process ensured that the researchers remain transparent in their objectives, and community participants are supported to identify their own health agendas, develop research skills, and become decision-makers for their community health education activities (Springer and Skolarus, 2019).
Community setting and participation
In this study, the authors worked collaboratively with the Bindjareb Noongar Aboriginal community through the Winjan Aboriginal Corporation (Winjan) community organisation, to gain a detailed understanding of perceptions and perspectives on infant resuscitation. One of the authors (C.N.) has close ties with Winjan through previous research collaborations, so trust and relationship building was already well established.
As a community organisation, Winjan serves the Bindjareb people of Mandurah, a town in the southwest of Western Australia. The Aboriginal population of Mandurah is 1718 (840 men and 875 women) with a median age of 20, and the average number of people per household is 3.3 equating to approximately 520 households (Australian Bureau of Statistics, 2016).
Winjan Elders and leaders were well versed in the objectives of the study because of the co-design and collaboration on the study protocol and data governance protocol. This resulted in local Elders facilitating the recruitment of the community participants. A total of 16 community participants (14 women and two men) were recruited for the study.
Governance
To ensure the ethical conduct of the research a number of advisory committees were consulted (National Health and Medical Research Council, 2018). An Aboriginal Health Professional Advisory Committee comprising Aboriginal Health Workers from two regional Aboriginal Community Controlled Health Services advised on the study. The research teams also worked with the Elder Aboriginal Advisory Group at Murdoch University Ngangk Yira Institute of Change to ensure cultural safety using the APAR framework. This advisory group approved the data management plan which was developed with Winjan Elders and leaders so as to meet CARE and FAIR principles for handling, managing, and/or analysing Indigenous data (Carroll et al., 2021, Lowitja Institute, 2023, Russo Carroll et al., 2020, Walter et al., 2020, National Health and Medical Research Council, 2018). The study was granted ethical approval by Murdoch University (2021/128) and the Western Australian Aboriginal Health Ethics Committee (WAAHEC) (HREC1071).
Data collection
Yarning circles were used to collect the data. Yarning has been shown to be an appropriate method of data collection in Aboriginal research since it allows for detailed qualitative data collection in a culturally responsive way and encourages the sharing of experiences, thoughts and ideas (Walker et al., 2014).
Bessarab and Ng’andu (2010) first described yarning as having four phases: collaborative yarning, social yarning, research topic yarning and therapeutic yarning. While a series of semi-structured questions were used to guide the yarning (see online supplemental material file 1), the Elder community participants supported the conversations to move through the four phases: social yarning to introduce the community participants to the researchers; collaborative yarning to answer any questions relating to the research and its processes; research yarning to converse about the topics introduced by the semi-structured questions; and therapeutic yarning which occurred due to the sensitive nature of the topic and the difficult feelings it brought up in some community participants (Bessarab and Ng’andu, 2010). Two yarning circles were held, and each was attended by between 10 and 16 community participants with numbers fluctuating as people came and went as needed. The yarning circles were audio recorded with community participants’ consent.
It was evident in the first yarning circle that although community members were aware of infant resuscitation as a topic there was little knowledge about the process or the learning objectives of current CPR courses. It was decided at this yarning circle that a standard CPR course would be provided for community members to attend and experience. A second yarning circle was then held 1 week after the CPR course had been delivered to discuss the experience and how it could be improved to be more culturally responsive for community members.
Data analysis
The data were analysed using thematic analysis (Clarke and Braun, 2017). An inductive approach allowed the data to determine the final themes. NVivo data assisted with the five-step analysis process presented in Table 1.
Grouping together of codes and themes.
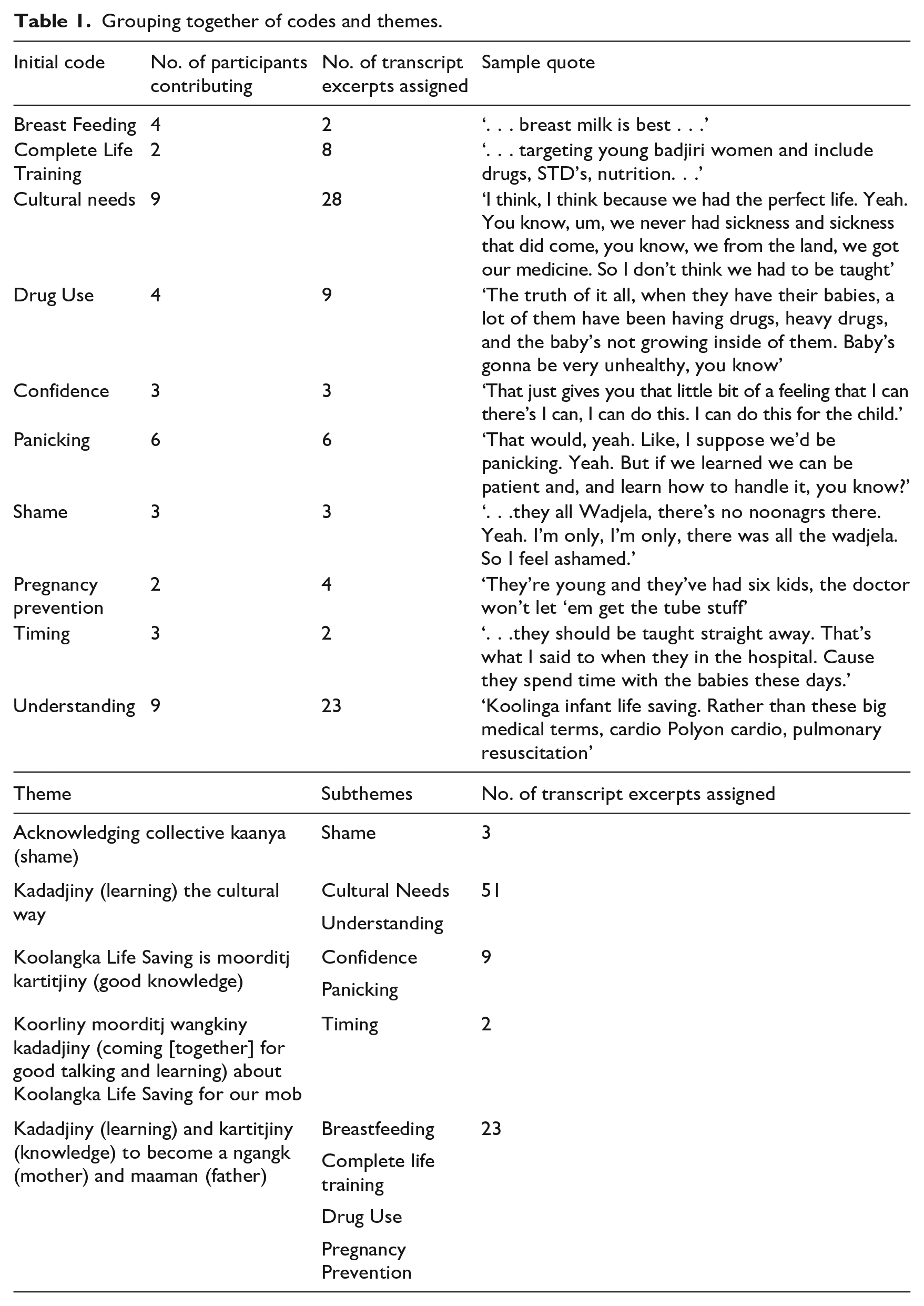
First, familiarisation with the data took place after the audio recordings had been transcribed. A second step involved coding the feelings or ideas expressed in the transcribed texts. Following an initial coding, the research team began to combine codes and identify patterns between them so as to generate draft themes. The draft themes were then reviewed, defined and given names as advised by community Elders and leaders. Using Noongar language in the themes helped demonstrate ownership, stewardship and custodianship of the data (Kennedy et al., 2022).
Findings
The findings are presented according to five overarching themes. The themes are evidenced by community participant verbatim comments. Altogether, the analysis resulted in five themes with 16 subthemes (see Table 2).
Principal themes.
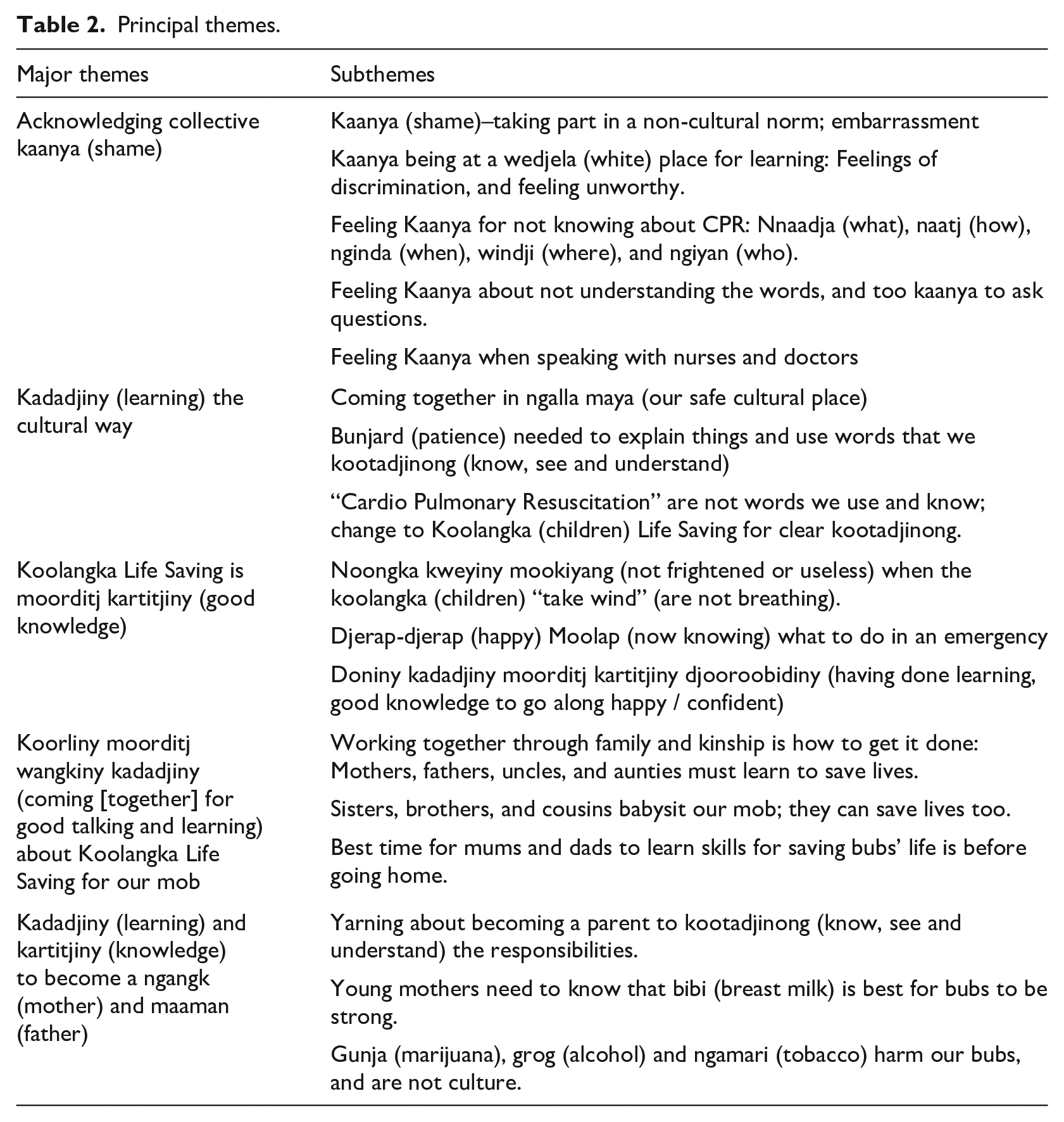
The five themes included acknowledged collective kaanya (shame); kaadadjiny (learning) the cultural way; Koolangka Life Saving as moorditj kartijiny (good knowledge); koorliny moorditj wangkiny kaadadjiny (coming [together] for good talking and learning) about Koolangka Life saving for our mob; and kaadadjiny (learning) and karitjiny (knowledge) to become a ngangk (mother) and maaman (father).
Acknowledging collective kaanya (shame)
All community participants in the first yarning circle voiced an experience of kaanya when having to take part in a class that involved predominantly white participants and that was not culturally responsive to their needs. Community participants reported how they felt isolated and unwelcome in these circumstances, and this impacted their ability to learn and take part.
Participants experienced kaanya and embarrassment for not understanding medical jargon, and kaanya for being in a wadjela (white) place of learning where they felt discriminated against, and unworthy. Community participants who had been involved in mainstream CPR courses with wadjela previously described how this had made them feel:
They are all wadjela, there’s no Noongars there. I’m the only one there with all the wadjela. So I feel ashamed. And like you can’t get into it. You feel shame but if it’s all Noongars and in the place you’ll get into it. You won’t feel that shame.
Another community participant noted that too often in such settings information was not provided in a way that was readily acceptable to the community:
They won’t say they don’t know the big words. And none of us was well educated. I know my spelling and that really good. But when it comes to big words . . . we don’t understand.
Some community participants felt that using nursing students from local universities might be a way to provide classes in Aboriginal community-controlled centres together with patient instructors. This would allow multiple instructors to provide the education needed allowing more one-on-one time to ensure community members understood the material:
Older nurses at the hospital judge us . . . nursing students (from the university close by) could teach the classes as they are less judgemental.
Another community participant noted that nursing students tended to cause less shame because they were still learning themselves.
. . . [We] don’t want to be shamed that we don’t know (about CPR), so student nurses would be good as they are sharing what they have just learned.
Kaadadjiny (learning) and kartitjiny (knowledge) to become a ngangk (mother) and maaman (father)
This theme was demonstrated by discussion relating to the need to yarn about becoming a parent in order for the younger generation to kootadjinong (know, see and understand) the responsibilities of parenthood, and how this has changed from what it would have been the case in the past. Traditionally, information about parenting would have been passed down from each generation to the next. But after colonisation and experience of the Stolen Generations
2
this no longer occurred:
That started with our stolen generation. We were taken; put in missions. We didn’t know how to look after our family because of that. And that’s the effect. Now it’s a ripple effect of what’s happened.
There was also a need for young mothers to know that bibi (breast milk) is best for babies to be strong and healthy. Women Elders in the group felt that the younger generation did not understand the importance of breast milk for their babies, opting to bottle feed them instead. Other Elders in the group noted the need to talk about the effects of drug use as part of prenatal education as gunja (marijuana), grog (alcohol) and ngamari (tobacco) ‘harm the bubs’ (infants) and are not part of traditional culture.
It was felt that educating young boodjaree (pregnant) women was the key to improving the health of their newborns and infants, and culturally responsive education surrounding prenatal, pregnancy and postpartum health would be beneficial for families and the community especially when discussing premature and small babies:
It’s different now these days . . . (discussing premature and small babies) . . . [You need to] find something that puts weight on these babies, breast Milk. You like to see that . . . breast milk is best–‘tittie milk’. These (referring to young mothers) they don’t do it. They give bottle. They don’t wanna breast feed because they could have the plans; ‘I’m going out’.
Another community participant discussed how many parents held the belief that the authorities might take their newborns away after birth because of drug use in pregnancy:
The truth of it all, when they have their babies, a lot of them have been having drugs, heavy drugs, and the baby’s not growing inside of them. Baby’s gonna be very unhealthy, you know. It’s the worst things. Now that’s making women have it (baby) early. They’re having their drugs. They’re (babies) not gonna be having breast milk either. Then they panic when they see doctors standing around and saying, ‘cause you’ve been on drugs’. They (doctors) know what they’re talking about. So they (young mothers) already got an anticipation and an understanding that the baby might be taken away.
Another community member felt the best way to demonstrate the risks of drug use in pregnancy was to show video footage of what might happen as a consequence of use:
I think maybe one good way of educating them (young mothers), is there’s gotta be some footage of . . . expecting mothers and something that did go wrong. The pain that she went through because of that and some footage along those lines.
Koolangka Life Saving is moorditj kartitjiny (good knowledge)
Following a discussion of what was required for infant resuscitation and the type of scenarios this kind of education could be useful for, community participants felt that this was valuable and important knowledge to have. Several Elders and community participants indicated that they were djerap-djerap (happy) moolap (now knowing) what to do in an emergency as well as doniny kaadadjiny moorditj kartitjiny djooroobidiny (having done learning, good knowledge to go along happy/confident).
Community participants described how this knowledge could increase individual confidence in an emergency situation, how it would be beneficial to the community, and how it assisted them – noongka kweyiny mookiyang (not being frightened or feeling useless) when koolangka (children) ‘take wind’ (are not breathing). Knowing what to do in an emergency situation meant they could take control of the situation and not feel so helpless. Community participants who attended the arranged CPR course stated that they felt more confident afterwards and now knew what to do in an emergency:
This will help the community. The community will be able to cope with these little babies that are out in the homes. So, you are gonna feel a bit more comfortable. If some things gonna go wrong, you can cope with this. You can cope in that first few minutes before the ambulance gets there. You’ve got the tools. You’ve got the knowledge at least, that you’ve helped that little person.
One community participant noted that knowing what to do in an emergency situation would help ease the panic associated with such events:
I suppose we’d be panicking. But if we learned we can be calm and learn how to handle it, you know? If we’re on the phone to somebody, I’d be shouting, screaming, crying, that’s me. But if I learned this, then I could do it, you know, just say, it’s all right. It’s gonna be okay, to whoever else is there. It’ll be good for us to have this, first so we’re not panicking and shouting out. We’re not screaming out crying. It’s okay–we’re just calm.
Koorliny moorditj wangkiny kaadadjiny (coming together for good talking and learning) about Koolangka Life Saving for our mob
Discussion surrounding women’s and men’s business and generational change took place under this theme as well as the importance of coming together as a community to learn and share the education received together. Community participants said that working together through family and kinship was how to get things done: mothers, fathers, uncles and aunties must learn to save lives particularly given the cultural importance of the family and the shared care of infants and children. Education needed to be provided to extended family members, as raising an infant is a community endeavour culturally and many family members are involved in an infant’s life:
That should be another thing. Men should be encouraged to attend a CPR course because a lot of times, the women could be at work and the men are at home with the kids when something goes wrong. So I think that the CPR should be for everyone.
Another community member said,
And of course, probably from a family perspective, that’s exactly what we would be wanting to encourage because it’s not just you or you or you who’s the caregiver, the caring in Aboriginal families is the responsibility of everybody, you know? So, a child has six mums, seven mums . . . Aboriginal people want their close relatives.
Kaadadjiny (learning) the cultural way
The impact of colonisation on Aboriginal ways of being, knowing and doing meant that culturally responsive education needed to take place in community spaces where community members felt safe. Coming together in ngalla maya (our safe place) to hold classes specifically for Noongar people was suggested as one way to change the feelings of shame about attending class, and to support the learning that took place in that class.
Beyond cultural safety, community participants felt that having the bunjard (patience) to explain things and use words that they kootadjinong (know, see and understand) was the most effective way of providing education. Having more time, and educators try different ways to explain concepts, would provide the best experience and help participants better understand the course material:
But if you find in the home place (safe cultural space), like I went in a community centre, they [community members] feel more comfortable going there to do it and you probably don’t get shame. When there’s not many Noongars there, you don’t know if you’ll do it that day. Because once I went to a first aid (course) and I’m like, nah, shame. I just felt uncomfortable. Cause I didn’t know anyone.
A community participant who had attended a previous CPR course described the shame they experienced due to the inconsistencies with culture and their learning style:
The course should be taught by someone patient, who doesn’t mind going over it again. When I done the first aid course, they only explain once and then you get tested on that and you’re so confused. It may take much longer. It may not be just six hour[s]. It may [need to be] be longer because of the patience and explaining things over and over, and making sure that there’s that understanding. So ideally it would be better if it was delivered in the community, like here at a community hall where this is . . .
Discussion
The study’s findings confirmed that while learning CPR way was viewed as valuable by members of the community, multiple barriers stood in the way of community members receiving this information and education. Community participants felt that a specific course just for Aboriginal people, held in a safe place such as community-controlled centre, would enable more community members to attend and be fully immersed in the course without experiencing shame.
Aboriginal Australian infants are noted to be at higher risk for pre-term birth and post birth complications than the general population, leading to higher risk of having a sudden and unexpected collapse due to a number of aetiologies leading to death (Askew et al., 2020; Commonwealth of Australia, 2020; Ford et al., 2018). Many issues require to be addressed in order to close the health disparity gap (Bertilone and McEvoy, 2015; Shipstone et al., 2019). Central to success, however, is providing parents with prenatal education which stresses the importance of breastfeeding and the avoidance of drug use during pregnancy, as well as infant resuscitation education.
To be successful, such education might use videos and pictograms to illustrate key points and demonstrate ideas. In addition, educators need to be patient and use plain language when explaining ideas. Utilising stories or describing situations that community members have experienced will help them to understand and develop relevant skills more easily. This is in keeping with how traditionally Aboriginal communities have learned and how Elders have shared cultural knowledge and practices with younger generations. Using colloquial phrases such as ‘the baby took their wind’ in this study helped communities members understand emergency situations more easily. This is important as first responders who do not know how to perform CPR are often instructed step-by-step over the phone (Weinmeister et al., 2018). Given that parents are the most likely first responder for children in the under 12-month age group, and the importance of immediate CPR for recovery without sequalae (Chia and Lian, 2014; Department of Health, 2018), the use of appropriate language could help save lives. All the community members in this study felt they would be better suited to assist in an emergency if they had prior understanding of what to do.
During the course of this work, several problems were identified with standard CPR education. Current CPR classes are not only expensive but are not provided at suitable times for parents and family members and do not take into account Aboriginal understandings of time (Boroditsky and Gaby, 2010; Janca and Bullen, 2003). They typically also have several requirements such as the need for pre-reading, student identification numbers, and computer access that seriously limit the ability of community members to participate. Community participants in this study expressed feelings of shame and judgement when trying to take these classes but felt that utilising nursing students from the local university to conduct classes might allow for free classes at more suitable times, and at a slower pace. Working with nursing students could enable community members to feel more confident to ask questions and get involved because the students themselves had only recently acquired the skills themselves. This type of education provided in a culturally responsive way could lead to increased confidence, knowledge and skills in community members’ CPR abilities.
The findings from the research have used to develop the Koolangka Infant Life Saving Education Framework (KILSEF) which can be used as the basis for the planning, facilitation and delivery of culturally responsive infant resuscitation education for Aboriginal families and communities in this setting. The KILSEF has four main components which include attention to location, content, cultural learning, and the removal of barriers. Further information about these components can be found in Figure 1.
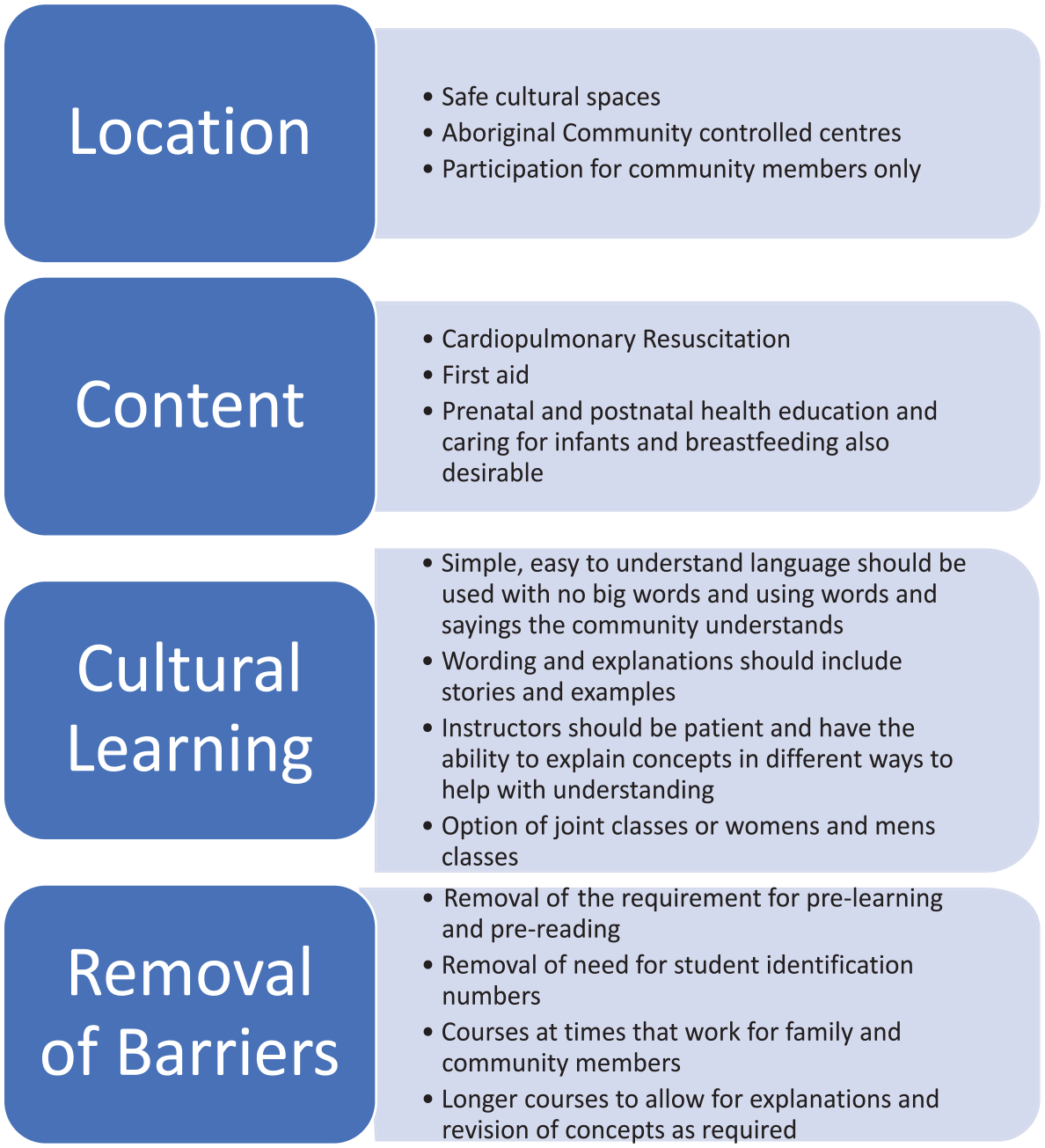
KILSEF components.
Limitations
This study was conducted with one Aboriginal language group community in southwest Western Australia. While its findings and the guiding concepts of the KILSEF cannot be generalised beyond this context, the culturally responsive approach the study adopted will hopefully provide inspiration to others working in different settings.
Conclusion
Providing infant resuscitation education in a culturally responsive way was highly valued by community participants in this study. Participants’ confidence, knowledge and skills to administer CPR were improved by attending the course. The Koolangka Infant Life Saving Education Framework provides the groundwork for implementing a culturally responsive resuscitation education classes for Aboriginal families and communities which is considered beneficial by the community it aims to serve.
Supplemental Material
sj-docx-1-hej-10.1177_00178969241247763 – Supplemental material for Koolangka Infant Life Saving: Culturally responsive infant CPR education for Aboriginal Australian parents
Supplemental material, sj-docx-1-hej-10.1177_00178969241247763 for Koolangka Infant Life Saving: Culturally responsive infant CPR education for Aboriginal Australian parents by Nakita Stephens, Caroline Nilson, Roz Walker and Rhonda Marriott in Health Education Journal
Footnotes
Acknowledgements
We thank the Bindjareb Noongar Community members for working alongside us and sharing their experiences and involvement in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.