
Abstract
Objectives:
Pain education has been shown to reduce pain and disability in people with persistent pain by increasing their understanding of ‘how pain works’. There are many resources that people can engage with to help them learn about pain. The primary aim of this study was to investigate the resources with which people with persistent pain engage, to learn about pain. Secondary aims included investigating the helpfulness of those resources, whether people assess the quality of the resources with which they engage and whether the resources sought differed according to whether or not they had a diagnosis for their pain.
Design:
Cross-sectional descriptive study.
Setting:
Online and paper-based surveys.
Methods:
People with persistent pain were recruited through advertising on social media and through local university health clinics. Participants completed a survey providing details about their pain condition, the resources with which they engaged to learn about pain, how useful they found these resources and whether they assessed the quality of the resources used.
Results:
Data were collected from 127 online surveys (80% female; age [±SD] was 41 [±16] years). Healthcare professionals were the most common resource with which participants engaged (85.0%), followed by the Internet (68.5%) and scientific articles (52.8%). Books and scientific articles had the highest helpfulness rating; healthcare professionals and pamphlets had the lowest. Most respondents (85.3%) reported assessing the quality of the resources they engaged with.
Conclusion:
Despite being the most common resource participants engaged with, healthcare professionals were awarded some of the lowest helpfulness ratings. Care needs to be taken to ensure that people with persistent pain are directed towards learning resources that can provide helpful, relevant and evidence-based information.
Introduction
Persistent pain – or pain enduring longer than 3–6 months – has a large impact on individuals and more broadly on society. In 2019, persistent pain affected 20.4% of US adults (Merskey and Bogduk, 1994; Zelaya et al., 2020). People with persistent pain frequently encounter difficulties with education, employment, social activities and activities of daily living (Dueñas et al., 2016; Hadi et al., 2019; Roehrs et al., 2013). In 2010, persistent pain costs the USA US$560 to US$635 billion due to decreased employment productivity and quality of life (Institute of Medicine Committee on Advancing Pain Research, Care, and Education, 2011).
Pain education can benefit people with persistent pain by reducing pain-related worry, improving pain-related self-efficacy, reducing pain and disability (Butler and Moseley, 2013; Lee et al., 2016). Contemporary understandings of pain regards pain as a biopsychosocial issue. That is, one’s pain experience can be influenced by psychological, social and tissue-based contributions (Louw et al., 2019). Pain education can address the common misconception that pain is an accurate indicator of tissue damage (Nijs et al., 2011). Numerous studies have demonstrated the benefits of pain education among different pain populations, including persistent widespread pain (Meeus et al., 2010), persistent neck pain (Van Oosterwijck et al., 2011) and persistent low back pain (Moseley, 2002, 2003, 2004, 2005; Ryan et al., 2010; Vos et al., 2020). A recent network meta-analysis concluded that of all psychological treatments, pain education offered the most sustainable benefits (Ho et al., 2022).
There are many ways that people with persistent pain can learn about pain, including through books, podcasts and healthcare professionals, as well as online resources such as blogs and websites. Those seeking online information tend to be well educated (Hesse et al., 2005; Mannion et al., 2013; Shinchuk et al., 2010) and demonstrate fear avoidant behaviour (Mannion et al., 2013) and high levels of perceived disability (Ferreira et al., 2010; Henderson et al., 2013; Mannion et al., 2013). Currently, little is known about the resources people with persistent pain use to learn about pain, and how helpful they find those resources.
Given the benefits of pain education for people with persistent pain, it is important to understand which resources people with pain are most likely to engage with, so that we can ensure that these resources are providing people with accessible, evidence-based information. This will help us better understand whether there is a need for health professionals to educate and provide consumers with higher quality resources, or whether we need to consider improving commonly utilised resources so as to provide consumers with better quality information.
Therefore, the primary aim of this study was to investigate the resources with which people with persistent pain (⩾6 months) engage, to learn about pain. Secondary aims were to investigate (1) how helpful people consider those resources to be, (2) whether these people assess the quality of the resources used and (3) whether the resources with which people engaged varied according to whether or not they had received a specific diagnosis for their pain.
Methods
Research design
This was a cross-sectional descriptive study. People with persistent pain were asked to complete either a paper-based or online survey providing details about the resources with which they engage to learn about pain. The research proposal was lodged and locked on Open Science Framework (https://osf.io/4t7nz) before data collection for transparency, integrity and reproducibility, as recommended in the pain field (Lee et al., 2018). The study adhered to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist for observational studies (Von Elm et al., 2007) and the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) reporting guidelines for online surveys (Eysenbach, 2004). The University of South Australia Human Research Ethics Committee approved the research (ID 204043). The funders played no role in the design, conduct or reporting of this study.
Participants
Convenience sampling was used for recruitment. We aimed to recruit a minimum of 100 people worldwide with persistent pain, and capture a diverse and wide representation of pain conditions. Online surveys were advertised on social media, and flyers containing a QR code that linked to the online survey were displayed in local university health clinics. Paper surveys were also available at local university health clinics. When attending the health clinic, people could complete the survey or post their responses via replied-paid envelopes. People were eligible to participate if they were 18 years or older, currently had pain for 6 months or more, and could read and write in English. People were excluded if they had had surgery in the past 6 months, were pregnant, had given birth in the previous year or had cancer-related pain. Participants were made aware that their participation in the survey was voluntary and that they could withdraw at any stage without consequence. Voluntary progression through the survey was taken as participant informed consent. Unique site visitors and survey view rates were not recorded.
Survey design
The survey was open between November 2021 and May 2022. Data were collected and managed using REDCap electronic data capture tools hosted at the University of South Australia (Harris et al., 2009, 2019). Participation in the survey was anonymous. Survey questions were initially developed within the research team and small modifications were made after piloting by two people with persistent pain. The content of the online and paper surveys was identical, except for a question asking the country of residence on the online survey. Both surveys included multiple-choice and open-ended free text questions (copies of the online and paper surveys can be obtained from the corresponding author on request).
The survey was divided into four sections. There were one to nine question items per page, over a total of five pages. Section 1 required participants to address questions confirming their eligibility to be involved in the study. In sections 2 and 3, participants were asked questions regarding their demographics, for example, age, sex, gender, education level, financial status, main activity/occupation and type of residential location (e.g. rural, city); how supported they felt by family, friends or community; and information that related to their pain (e.g. diagnosis related to their pain or the location of pain if they did not have a specific diagnosis, duration of pain and pain intensity). Section 4 asked participants to report on the resources they used to learn about pain, how useful they found these resources and whether they assessed the quality of the resources with which they engage. If participants reported assessing the quality of the resources with which they engaged, a follow-up question prompted them to describe how they did this. If they did not assess the quality, participants were asked why they did not do so. If participants engaged with Internet resources, they could provide details about the types of websites they used. Participants were then asked to indicate the helpfulness of each resource with which they engaged by providing a score on a five-point Likert-type scale (1 = very helpful, 2 = somewhat helpful, 3 = neutral, 4 = somewhat unhelpful, 5 = very unhelpful/harmful). Not all questions had a non-response option. For the online survey, all eligibility screening questions, basic demographic questions (i.e. country, age, gender) and our primary research question (the resources people access to learn about pain) were all mandatory (i.e. they were required to complete these questions before they could proceed any further). Respondents were able to change their answers while completing the survey (but not following completion) and there was no summary page at the end of the survey.
Data cleaning and statistical analysis
Data from the REDCap survey platform and the paper-based responses were downloaded into an Excel spreadsheet (manual data entry of paper responses was performed by T.X.). Data cleaning was performed in Excel whereby invalid responses (i.e. responses where participants did not follow the instructions) or surveys with incomplete responses for questions regarding the primary research aim were excluded. Survey responses were also excluded if participants did not meet the eligibility criteria.
The cleaned data were then transferred to IBM SPSS statistics, version 27.0 (IBM Corp, Armonk, NY) for analysis. Descriptive statistics – means and standard deviations or percentages – were used to report participant demographics and pain-related information. To address the primary research aim, all resources were listed with the percentage of participants who reported engaging with each resource provided. To address the secondary research aims, the mean and standard deviation of the helpfulness rating for each resource, the percentage of participants who assessed the quality of the resources they used and the strategies participants used to assess the quality of resources were calculated and reported. Resource usage of people with a diagnosis for their pain and people without a diagnosis for their pain were reported separately. Data from the free text responses were synthesised and categorised. Free text responses that were not related to the research aims were removed.
Results
Survey sample
Three hundred one participants responded to the survey, including 298 online and 3 paper-based responses. After data cleaning, 127 valid online responses were included for data analysis. The survey completion rate was 65.4%. The detailed data cleaning process is shown in Figure 1.
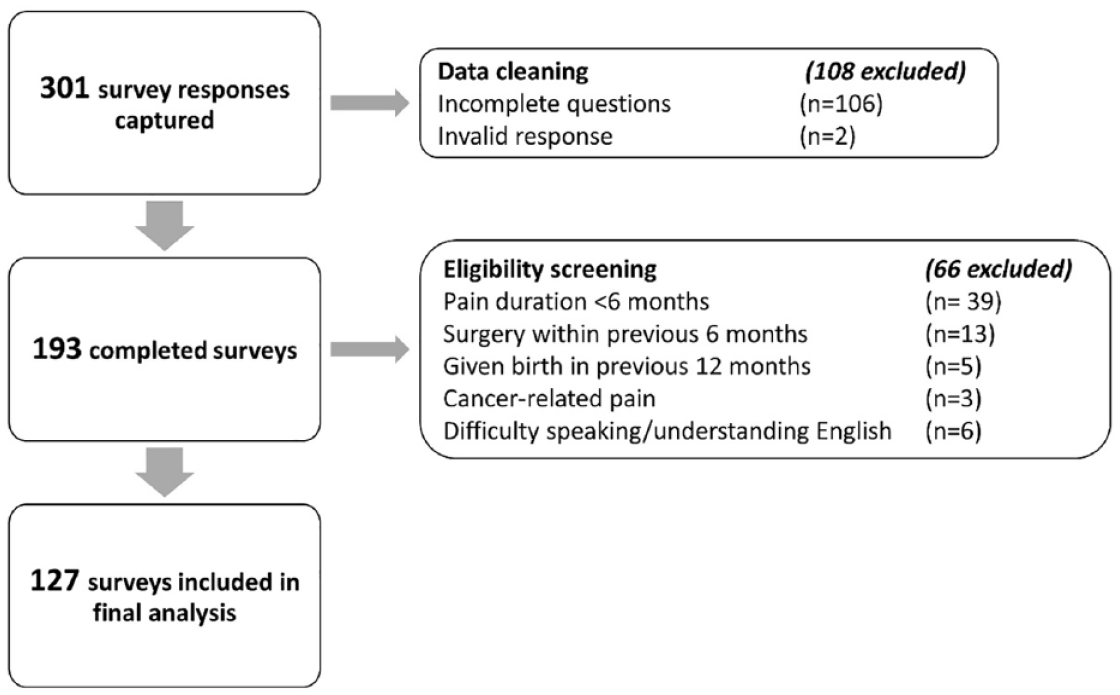
Flowchart of the data cleaning process.
Demographics
Among 127 eligible participants, the mean (±SD) age was 41 (±16) years, and 80.3% identified as being a woman. Table 1 provides the full demographic data of participants. Participants came from 22 different countries, with the majority coming from Australia (n = 59, 46.5%), the UK (n = 23, 18.1%) and the USA (n = 12, 9.4%). Additional demographic- and condition-related details can be found in the Online Supplemental Material associated with this paper.
Demographic characteristics of participants.

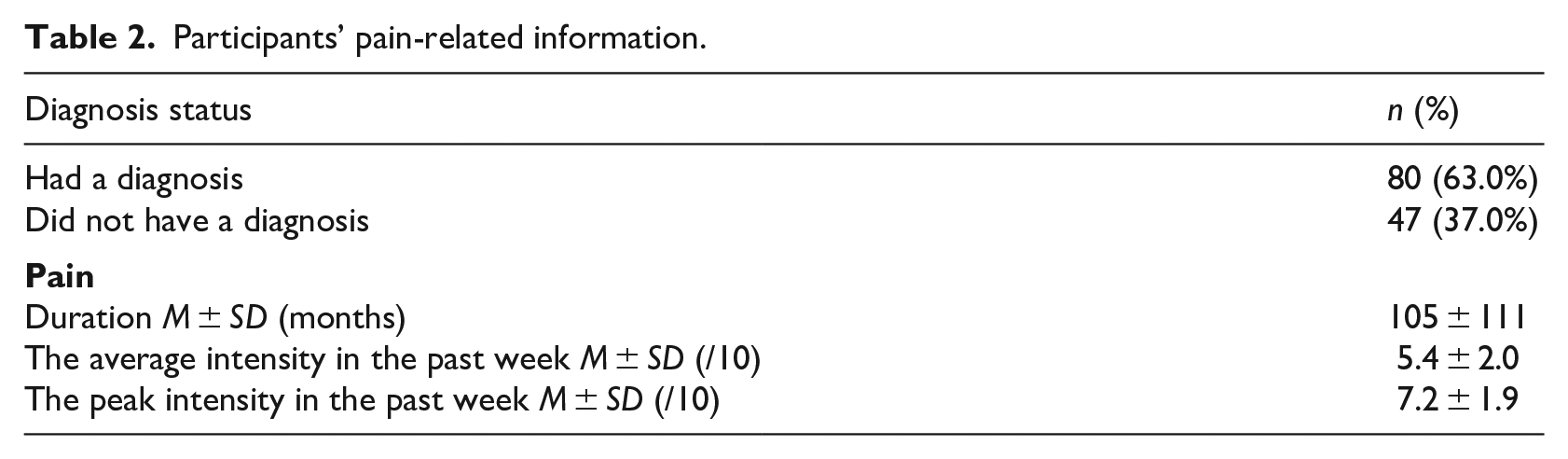
Eighty (63.0%) participants reported at least one diagnosis, with 49 different diagnoses reported. The most common diagnoses were fibromyalgia (n = 17), osteoarthritis (n = 9) and sciatica (n = 7). A detailed list of the participants’ diagnoses can be found in Supplemental Material. Most participants experienced widespread pain (n = 40), followed by limb(s) pain (n = 25), spinal pain (n = 24), pelvic pain (n = 12), head pain (n = 7), chest pain (n = 3), abdominal pain (n = 2) and facial pain (n = 1). Eleven participants’ pain location was non-specific. Table 2 outlines participant pain-specific information.
Participants’ pain-related information.
Pain-specific resource-seeking behaviour
One hundred fourteen (89.8%) participants engaged with more than one resource to help them learn about pain. Healthcare professionals were the most common resource accessed (n = 108, 85.0%), followed by the Internet (n = 87, 68.5%) and scientific articles (n = 67, 52.8%). Of those who reported engaging with the Internet, the most common websites were commercial (n = 18), followed by governmental (n = 16), organisational (n = 13) and educational (n = 5). Forty-seven participants reported accessing Internet-based resources that were classified as ‘non-specific’, which means these resources could not be identified as any of the four categories above (i.e. commercial, governmental, organisational and/or educational).
The most helpful resources were books and scientific articles, each receiving helpfulness scores of 1.68 ± 0.91 and 1.82 ± 0.92, respectively (with 1 being ‘very helpful’ to 5 being ‘very unhelpful/harmful’). The least helpful resources were magazines and pamphlets, each receiving helpfulness scores of 2.67 ± 1.21 and 2.60 ± 1.51, respectively. Healthcare professionals received one of the lowest helpfulness scores among all reported resources (2.39 ± 1.17).
Table 3 lists the pain-specific learning resources participants reported engaging with and the perceived helpfulness of each resource, and is reported according to diagnosis status (i.e. those with and without a diagnosis for their pain).
Pain-specific learning resource use and their perceived helpfulness.
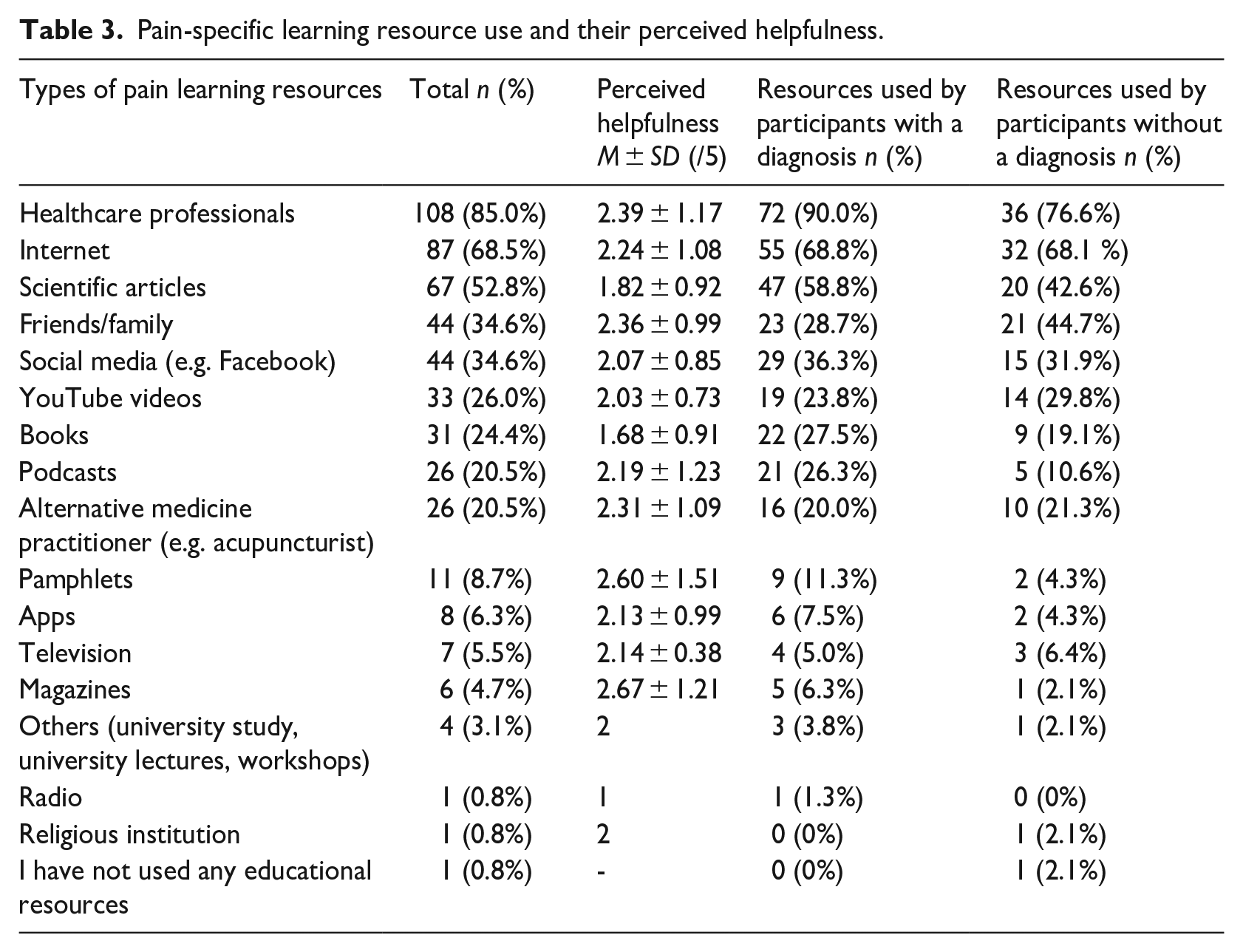
Overall, helpfulness scores ranged from 1.68 (books) to 2.67 (magazines) for all resources (difference of 0.99 out of 5; 19.8%). On a Likert-type scale, this represents a helpfulness difference between ‘neutral’ and ‘somewhat helpful’, and ‘somewhat helpful’ and ‘very helpful’.
Assessing the quality of resources
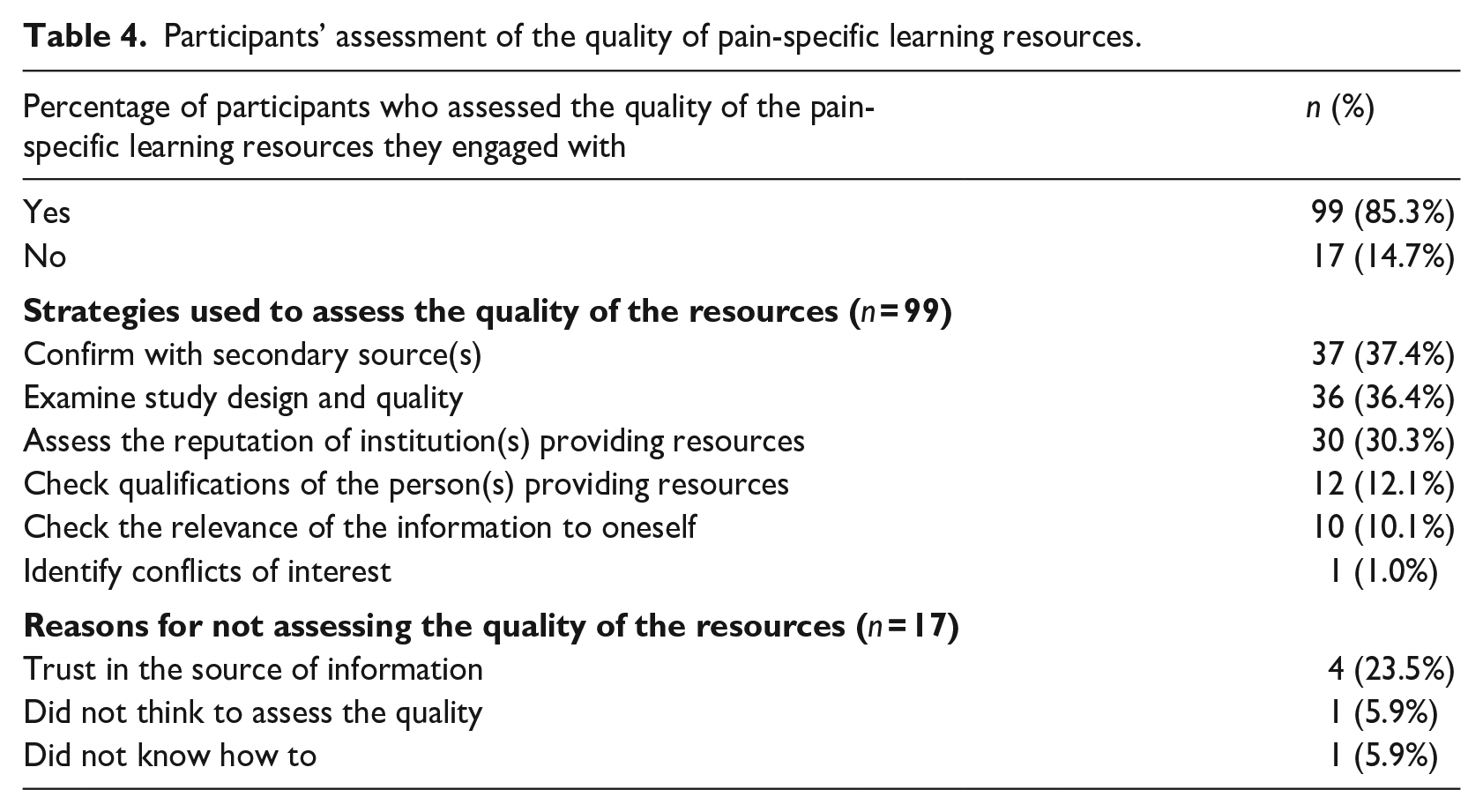
One hundred sixteen (91.3%) participants responded to the question that asked participants whether they assessed the quality of the pain learning resources they engaged with. Of those, 99 participants (85%) responded ‘yes’, indicating that they did assess the quality of the resources they used. Table 4 provides further details about participants’ assessment of the quality of pain learning resources.
Participants’ assessment of the quality of pain-specific learning resources.
Discussion
The primary aim of this study was to investigate the resources with which people with persistent pain (⩾6 months) engaged to learn about pain. Secondary aims were to investigate (1) how helpful people considered those resources to be, (2) whether these people assessed the quality of the resources they used, and (3) whether the resources with which people engaged varied according to whether or not they had a specific diagnosis for their pain. The results demonstrate that healthcare professionals were the most common resource participants engaged with, followed by the Internet and scientific articles, and most resources were reported to have a degree of helpfulness. Among the commonly used resources (>20% of participants), books had the highest helpfulness rating, followed by scientific articles. Despite being the most common resource reported, healthcare professionals had one of the lowest helpfulness ratings.
Our findings suggest that the most common resource with which people with persistent pain engage (i.e. health professionals) was reported as being one of the least helpful resources. Similar to previous work, we found that people with persistent pain identified healthcare professionals as a common source of information for their pain (Briggs et al., 2010). Despite this, people reported healthcare professionals to be only ‘somewhat helpful’ to ‘neutral’, possibly because their healthcare provider did not provide timely help, lacked knowledge of their condition (Thompson et al., 2018), were unable to provide up-to-date evidence-based care (such as pain science education) into their practice (Chambers, 2018) or their rating reflected their overall perceived quality of care.
Regardless, this highlights the need for healthcare professionals to be equipped with the knowledge and resources to provide timely pain education to their patients. In Australia, this is aligned with workforce training targets developed in partnership with people living with persistent pain (Slater et al., 2022), as well as the National Strategic Action Plan for Pain Management which highlighted ‘education and training of health professionals’ as a key priority (Australian Government Department of Health and Aged Care, 2017). Other research has also highlighted the need for healthcare professionals to be better informed on pain-related education and care (Moore et al., 2022). Interventions to equip healthcare professionals with contemporary pain science knowledge are underway. For example, the Pain Revolution initiative provides advanced skills to regional healthcare professionals to enable them to educate their colleagues and general community about contemporary pain science and education concepts (Pain Revolution, 2023). The initiative focuses on three core pain learning concepts which are valued by people with pain: understanding that pain does not necessarily link to tissue injury, the effects of experiences and emotion on pain, and the potential for people to modulate their overprotective pain system (Leake et al., 2021). A community-wide approach to pain education has been proposed as another avenue to promote broader pain-related knowledge mobilisation (Moseley, 2019).
The second most common learning resource with which people engaged was the Internet; however, this was rated as somewhat helpful to neutral. This low rating may be due to the unregulated nature of some websites. Recent research has shown that online information often lacks accuracy, comprehensiveness and credibility (Moore et al., 2021), with inaccurate and unclear recommendations, and the endorsement of treatments that are inappropriate. Despite this, social media and YouTube videos, both of which are Internet-based resources, were reported to be used by 34% and 26% of respondents, respectively, and rated relatively high in helpfulness (both 2/5, where 1 reflects the highest helpfulness rating). Social media provides a platform for connecting and exchanging thoughts and experiences with others in a similar situation (Goudman et al., 2022), and this type of engagement has been found to increase general well-being, a user’s sense of control and belonging (Barak et al., 2008). Furthermore, YouTube videos often provide pain education in plain language with vivid animation, enhancing the overall experience of users, and may increase their perceived helpfulness (Heathcote et al., 2019; Machado et al., 2016). Given the disparity of helpfulness ratings between the Internet, social media and YouTube, Internet-based information may need to increase strategies of engagement (such as animations or interactivity) to improve the perceived helpfulness.
Other resources that people rated as helpful were books and scientific articles. Books may be rated as helpful due to them being authored by experts in the field. Similarly, the ‘professional’ and ‘expert’ nature of scientific articles might influence participants to rate them as being more helpful. That books and scientific articles are often written by authors with impressive credentials may have led to these resources being viewed as more credible, and therefore more helpful (Thon and Jucks, 2017).
Participants with a diagnosis for their pain often engaged with healthcare professionals, scientific articles and podcasts to learn about pain. In contrast, participants without a diagnosis for their pain tended to obtain information from friends and/or family. This could be expected because when people engage with their healthcare professionals, there is an opportunity to discuss not only their condition or diagnosis but also pain more broadly. On the other hand, those without a diagnosis may be less likely to receive information from healthcare professionals because they might be seen as still ‘searching for a cause’, and therefore in the absence of any diagnosis-specific information, are more likely to confide in their family and friends. Despite this, friends/family were rated as ‘low’ in helpfulness. Importantly, not all participants with a diagnosis learned about pain from their healthcare professionals, which could mean some healthcare professionals may not incorporate pain-specific education into their model of care. These findings raise the point that information-seeking behaviour is unlikely to be a unitary phenomenon but is likely guided by several interacting psychosocial (e.g. social supports/relationships, education, mental health status) and medical factors (e.g. diagnosis, clinician, co-morbidities). Such an interplay of complex factors is difficult to capture within an online survey, and more comprehensive data on ‘lived experience’ (captured by interviews, for example) might provide more nuanced insights into information-seeking behaviours in people with pain.
Eighty-five percent of participants reported that they assessed the quality and trustworthiness of the resources with which they engaged. The most common strategy (37.4%) was to confirm the information they received with a secondary source, followed by examining the study design and quality, or assessing the general reputation of the institution providing the information. These findings are similar to those reported in a recent systematic review investigating how consumers evaluate the quality of online health information (Sun et al., 2019). The review reported that most participants assess the quality of the information by confirming with another source or assessing the reputations of the institution(s) providing the information (Sun et al., 2019). It might be helpful for healthcare professionals to provide patients with access to multiple resources that provide consistent messaging.
Limitations and strengths
There are limitations to the study findings. First, this work involved data collection from a small sample (n = 127) that overrepresented women (n = 102, 80.3%). This is greater than the proportion of those with persistent pain (about 62% of whom are women) (Johannes et al., 2010; Mogil, 2012). Second, because data were captured using an online survey, it is unlikely to represent all people with persistent pain, especially those who do not (or are unable to) engage with the Internet. Third, students (n = 41, 32.3%) and people with a higher education (n = 82, 64.5%) constituted a high proportion of participants and therefore the sample may be overrepresented by people with higher levels of health literacy. Fourth, unique site visitors were not recorded, and therefore, we cannot exclude the possibility that some participants completed the survey more than once. However, there were no incentives for people to complete the survey, so the likelihood of this remains low. Finally, approximately 85% of participants were from Western countries, which reduces the generalisability to non-Western countries. Future research is needed to tackle these limitations.
This study also had strengths. The study had substantial reach, covering 22 countries and 49 painful conditions. While we recognise that some countries and painful conditions had low representation (i.e. 11/22 countries and 34/49 painful conditions had n = 1) and is unlikely to be representative of that country or painful condition, we were still able to achieve good geographical spread in the sample. The research protocol was also pre-registered on Open Science Framework prior to data collection, a practice recommended in pain research to increase rigour and transparency (Lee et al., 2018).
Future directions
Future research should explore how to improve the helpfulness of resources that people engage with to learn about pain. This may include further studies to clarify why healthcare professionals are reported to be unhelpful in providing pain education, and then exploring strategies to assist such professionals to improve their pain education in clinical and community settings. Due to the small sample size and limited generalisability of the results, future studies should also target a larger sample that with greater diversity in culture, ethnicity, gender and pain conditions, to further explore pain learning resource-seeking behaviour. It would also be worthwhile investigating the resource-seeking behaviour of those with lower education levels, and people who are less likely to engage with the Internet.
Conclusion
The findings from this study revealed that the most common resources with which people with persistent pain engage to learn about pain were healthcare professionals, the Internet and scientific articles. Overall, most resources were reported to have a degree of helpfulness. Importantly, some of the most common resources that people engaged with also rated low in helpfulness. This suggests that these resources may need to be further developed to ensure they provide patients with evidence-based, relevant and helpful information about pain, in an accessible, engaging and easily understood manner. To improve the helpfulness of resources, it is critical to ensure that the insights from consumers are incorporated when planning the content and delivery of these resources.
Supplemental Material
sj-docx-1-hej-10.1177_00178969241241214 – Supplemental material for What resources do people with persistent pain use to help them better understand their pain? A cross-sectional survey
Supplemental material, sj-docx-1-hej-10.1177_00178969241241214 for What resources do people with persistent pain use to help them better understand their pain? A cross-sectional survey by Tenglong Xie, K Jane Chalmers, G Lorimer Moseley and Sarah B Wallwork in Health Education Journal
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.L.M. has received support from Reality Health, Connect Health UK, Institutes of Health California, AIA Australia, Workers’ Compensation Boards and professional sporting organisations in Australia, Europe and South and North America. Professional and scientific bodies have reimbursed him for travel costs related to the presentation of research on pain and pain education at scientific conferences/symposia. He has received speaker fees for lectures on pain, pain education and rehabilitation. He receives royalties for books on pain and pain education. S.B.W. has received speaker fees for lectures on pain and rehabilitation. T.X. and K.J.C have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: S.B.W., K.J.C. and G.L.M. are supported by an Australian National Health and Medical Research Council (NHMRC) Leadership Investigator Grant awarded to G.L.M. (ID: 1178444).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.