
Abstract
Objective:
Most countries teach limited information about sex and reproductive health education, often concentrating on how not to get pregnant. In this study, we examine what 16- to 18-year-olds in England have learnt and their views about reproductive health education.
Design:
This is a mixed-methods study. An anonymous, online survey was conducted on Qualtrics software using multiple-choice and open-ended questions. Schools were recruited via the Biotutors forum, and they distributed the survey to students aged 16–18 years.
Setting:
Data collection took place across England.
Methods:
A total of 931 students completed the survey, of whom 636 were girls, 250 were boys, 31 as other genders, and 14 did not disclose their gender. Quantitative data were analysed descriptively, and associations were explored using Chi-square tests. Qualitative data were analysed thematically.
Results:
Over half (65%) of the students rated the sex education they had received as adequate or below. Over half (74%) reported that they do not, or only sometimes, talk to their parents/guardians about these topics. Half (49%) did not know when a woman is most fertile. Students showed a better knowledge of female fertility than male fertility. There was no relationship between how much teaching respondents said they had received and their knowledge of reproductive health topics. From the free text question ‘How do you think we can improve sex and fertility education in schools?’, five themes were identified: inclusivity for all students; comprehensive with relevant topic variety; logistical improvements needed to teaching; the need for honest, transparent and non-judgemental teaching; and sex positivity.
Conclusion:
Schools should teach a wider range of issues relevant to sexual and reproductive health. Data from this study have assisted the creation of a teachers’ education resource which is being developed in partnership with the International Reproductive Health Education Collaboration (IRHEC).
Introduction
Sexuality education has been defined by the World Health Organization as involving the provision of ‘accurate, age-appropriate information about sexuality and their sexual and reproductive health, which is critical for their health and survival’ (World Health Organization, 2023). The importance of good-quality sexuality education is now well-established (Elia and Tokunaga, 2015; European Expert Group on Sexuality Education, 2016; Pound et al., 2017; UNESCO, 2009). It has been shown to improve the health and well-being of young people early in their lives and as they progress into adulthood (Goldfarb and Lieberman, 2021). Good-quality sexuality education is an important contributor to health and well-being (UNESCO, 2023). In recent years, students report sexuality education has been found to be lacking in quality in many countries, including England (Maslowski et al., 2022), the UK more generally (Pound et al., 2016; Maslowski et al., 2023), the Netherlands (Cense et al., 2020) and Norway (Helbekkmo et al., 2021), where the focus is often on preventing the negative consequences of sexual behaviour, without acknowledging issues such as infertility, sexual pleasure or sexual diversity (Helbekkmo et al., 2021).
The International Reproductive Health Education Collaboration (IRHEC) (formerly the International Fertility Education Initiative) has been working on the development of inclusive, comprehensive sex and reproductive health education resources for teachers and the public for some time (Harper et al., 2021). The IRHEC uses the term ‘sex and reproductive health education’ instead of ‘sexuality education’ or ‘fertility education’, to ensure the inclusion of reproductive health topics, not just topics relating to sex and sexuality (which include sexual relationships and intimacy, gender orientation etc.), and those relating to having children. In addition to the sexuality education that many schools provide, in the IRHEC’s view, sex and reproductive health education should include a focus on the menstrual cycle, fertility, how to avoid a pregnancy, how to become a parent, contraception, sexually transmitted infections (STIs), preconception health, endometriosis, polycystic ovarian syndrome (PCOS), miscarriage, pregnancy, fertility, infertility and the menopause.
However, cultural, linguistic, political and logistic challenges exist in many countries in relation to the provision of sex and reproductive health education. There remains resistance from some parents who believe that this kind of education is likely to increase sexual activity or leads to an earlier sexual debut. In addition, culture-specific challenges exist.
In England, since 2020, the Department for Education has required schools to teach relationships education in primary schools and relationships and sex education (RSE) in secondary schools (Department for Education, 2019). The current curriculum includes reference to the specific need to teach ‘the facts about reproductive health, including fertility, and the potential impact of lifestyle on fertility for men and women and menopause’. Analysis of the existing curriculum in England (Maslowski et al., 2022) and the curricula in each of the four nations of the UK (Maslowski et al., 2023) has shown that the majority of topics that should be included in reproductive health education, such as fertility, endometriosis and menopause, are not being taught.
We used an online survey to evaluate the knowledge and attitudes of secondary school students (aged 16 -18 years) in England relating to their school sex and reproductive health education and attitudes to family building. A primary analysis of the first 221 responses to 4 questions included in the survey has already been published (Maslowski et al., 2022). The data regarding students’ attitudes to having children are reported elsewhere (Biswakarma et al., 2024) and in this paper we have examined the survey questions relating to their knowledge and views to sex and reproductive health education.
Methods
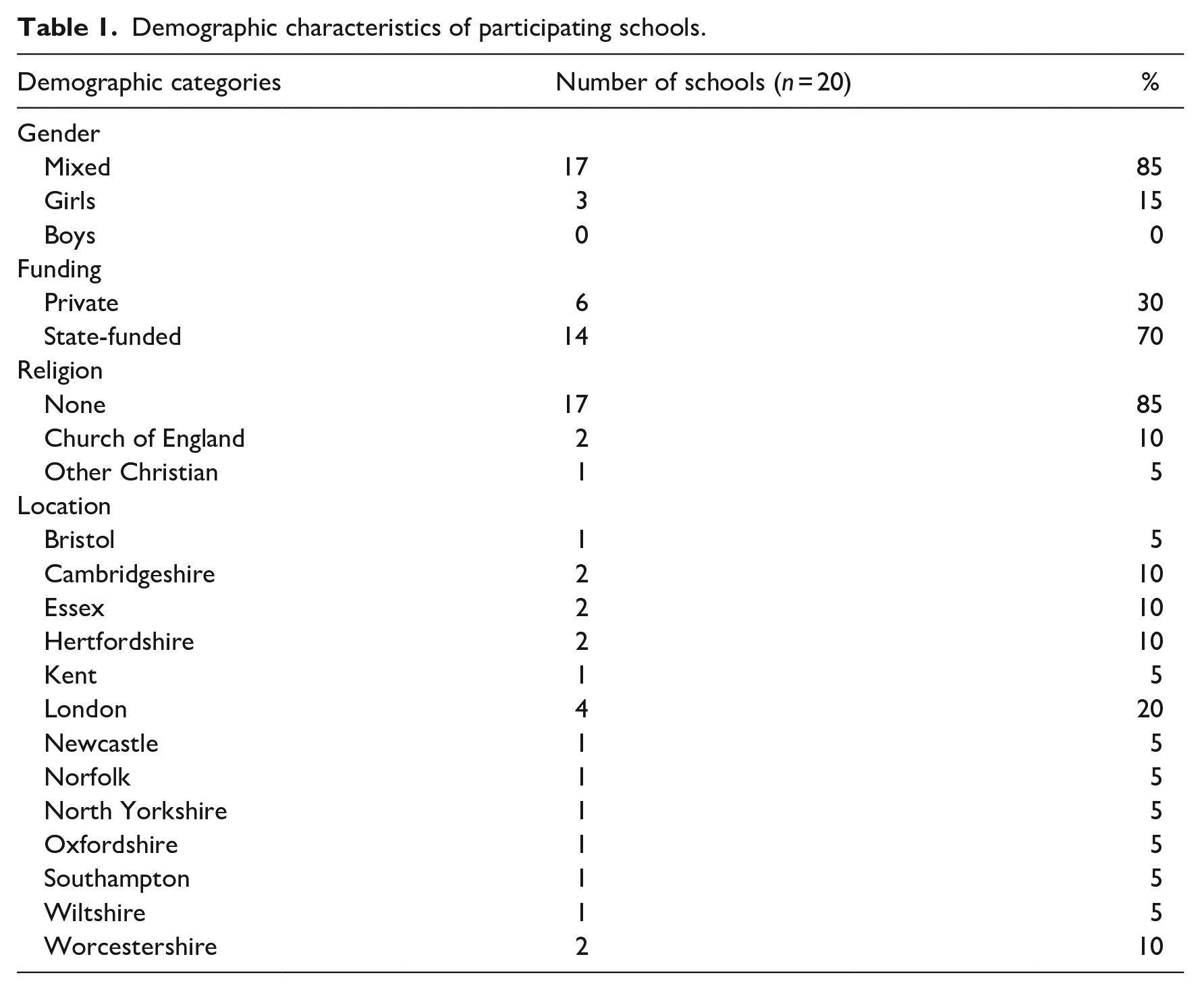
The data on the questions relating to attitudes to having children have been reported elsewhere (Biswakarma et al., 2024). In this paper, only those survey questions relating to the respondents’ demographics, knowledge and views to sex and reproductive health education were analysed. Data were collected from students in 20 secondary schools across England approached through an open invitation to teachers to participate posted on the Biotutors forum. Teachers were responsible for distributing the survey to year 12 and 13 students (aged 16–18 years). Table 1 details participating schools’ principal characteristics.
Demographic characteristics of participating schools.
A 47-item online survey was developed using Qualtrics software. The survey included a mixture of multiple-choice and open-ended questions asking about sex, reproductive health, fertility and reproduction. The questions were created following a review of the RSE curriculum for secondary schools in England and the equivalent curricula elsewhere in the UK (Department for Education, 2019; Maslowski et al., 2022, 2023) and from questions asked in a previous enquiry (Harper and Botero-Meneses, 2022).
The survey began by providing background information about the study, data protection information and how to make any complaint. It then asked students for their consent. Those who consented were then asked a series of demographic questions. These were followed by questions about their views about sex and reproductive health education both in and outside school; their experiences discussing sex and reproductive health with their parents/guardians; their understanding of basic fertility concepts and any plans they had for having a family in the future. Some teachers gave students time in lessons to complete the survey, while others gave the students the web link to do so in their own time.
Data analysis
Data were analysed descriptively, and associations were explored using Chi-square tests (IBM SPSS Statistics Version 27.0.1.0). Due to low respondent numbers, the gender identities of transmale, transfemale, non-binary and other respondents were combined into an ‘other’ category in the analyses. Students who chose ‘prefer not to say’ when asked about their gender were excluded from gender-based analyses.
The one qualitative question ‘How do you think we can improve sex and fertility education in schools?’ was answered by 507 students and results were analysed using thematic analysis (Braun and Clarke, 2021). Phase 1 involved reading the responses of participants to familiarise ourselves with their character and identify similar words and patterns throughout the responses. Phase 2 involved re-reading the responses while highlighting repeated patterns of response to form initial codes. In phase 3, the data were re-read, and meaningful elements of text were identified and assigned codes, allowing more data to be categorised using these codes. Phase 4 involved reading the data again to make sure the text had been thoroughly analysed; the initial codes were yet refined further so that the material could be organised thematically. Phase 5 involved a process of describing and comparing themes in order to more clearly define and name them. Phase 6 entailed writing up the findings.
The survey was validated in part through its use of existing, validated questions and in part by a pilot in which individual interviews were undertaken with five students, conducted over Zoom. Feedback from these interviewees confirmed the intelligibility and relevance of the survey questions and resulted in only minor rewordings.
Thematic analysis is particularly appropriate for the analysis of qualitative data when the aim is to identify recurrent themes and tentatively explore the relationship between variables (Alhojailan, 2012). Nowell et al. (2017) among others stress the importance of being explicit about how qualitative data analysis is undertaken if study findings are to be trustworthy. Adhering to the six-phase approach advocated by Braun and Clarke (2021) therefore helped ensure reliability and validity.
The study was approved by the UCL Research Ethics Committee (ID Number: 9831/006) in 2021.
Results
From a total of 1,267 students who began the survey, 1,243 provided their consent to participate, but 202 did not submit, so a total of 931 responses are included in this analysis.
Demographics
All the schools were located in England. The principal characteristics of the schools are shown in Table 1. The majority of schools (85.0%, 17/20) were mixed-sex, 3 (15.0%) were girls-only schools and 70.0% (14/20) were state-funded.
The demographic characteristics of study participants are shown in Table 2. The majority of students (68.3%, 636/931) were female, 250 (26.9%) were male, 31 (3.3%) identified as either transmale, transfemale, non-binary or other and 14 students (1.5%) chose not to identify their gender.
Demographic details of participating students, according to gender.
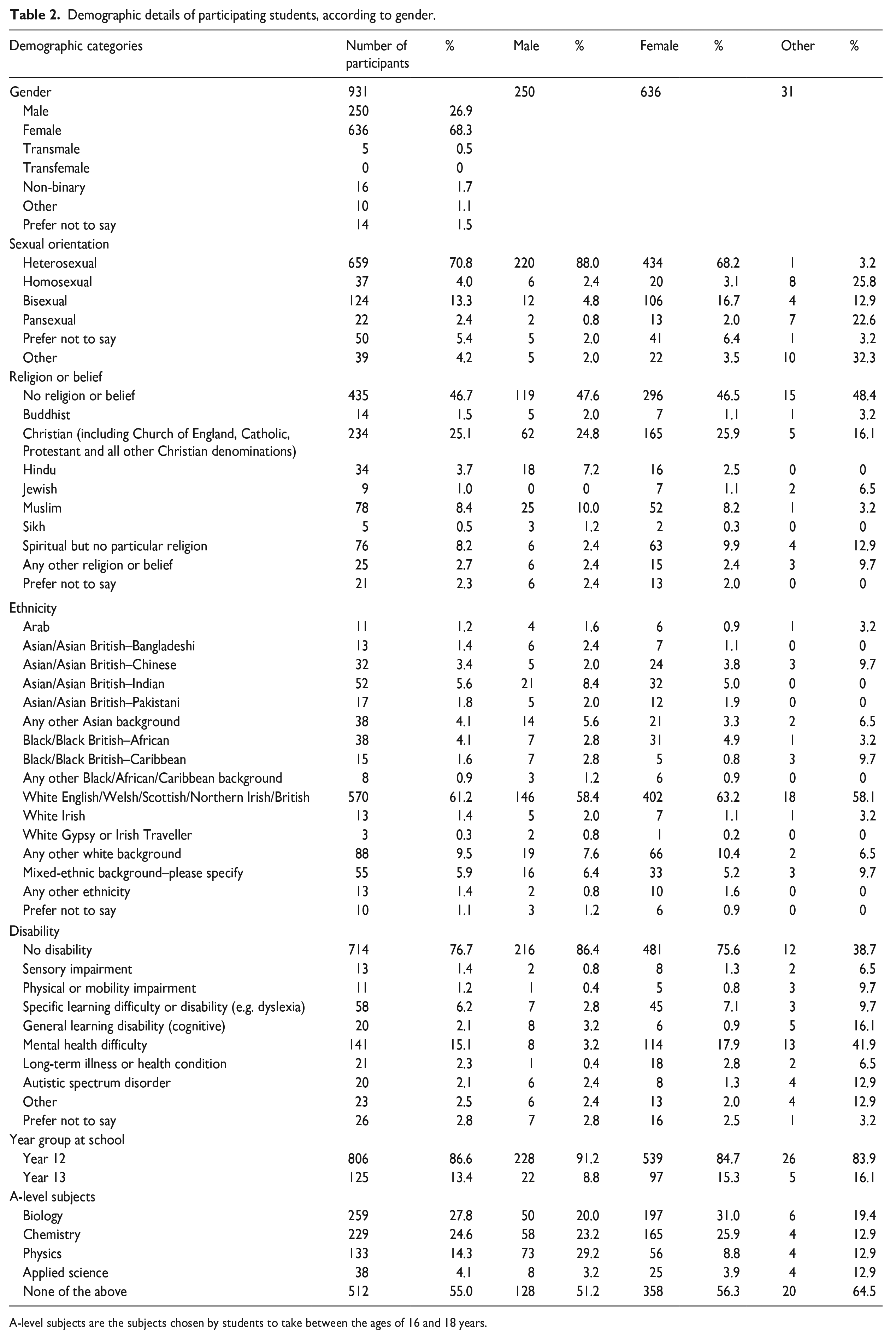
A-level subjects are the subjects chosen by students to take between the ages of 16 and 18 years.
Most students (70.8%, 659/931) identified as heterosexual, and 46.7% (435/931) had no religion or belief. The most common ethnicity was White English/Welsh/Scottish/Northern Irish/British (61.2%, 570/931) and most students did not identify as having a disability (76.7%, 714/931).
Sources of sex and reproductive health education
Students were asked whether they had received any sex education at school and to rate the quality of the education they had received from very poor to very good. The majority of students (69.7%, 649/931) reported having ‘yes, a little’ sex education at school (Figure 1), and only 34.7% (323/931) reported that their sex education had been good or very good (Figure 2).
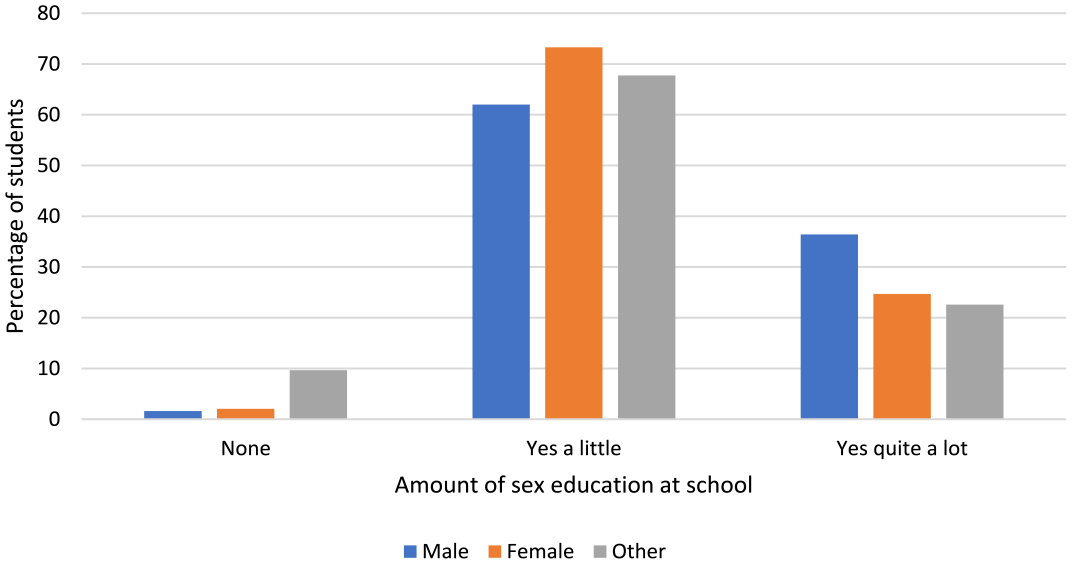
Exposure to sex education at school, as reported by students.
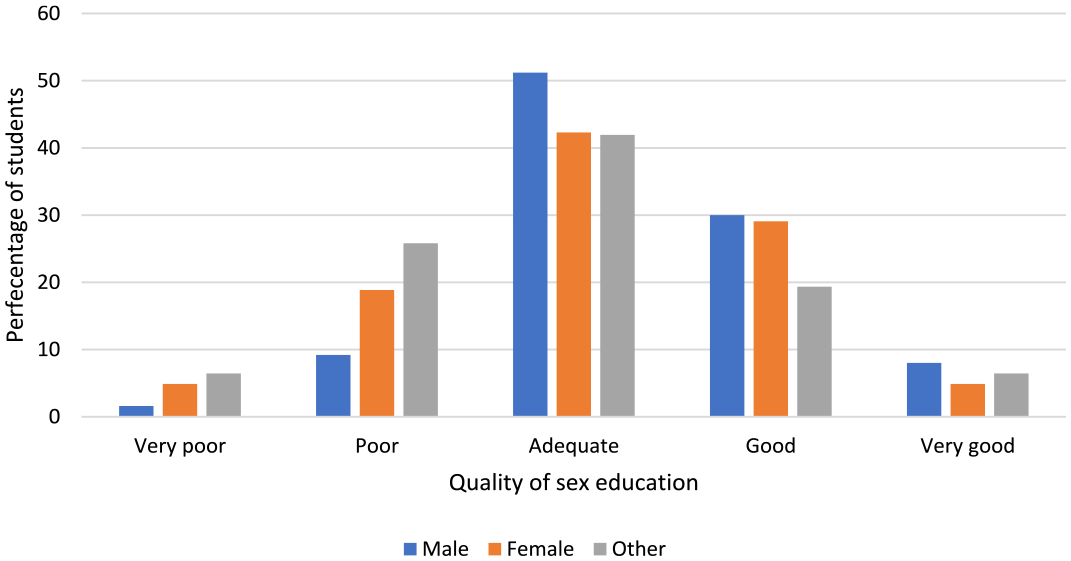
Student-reported quality of school sex education received.
Students were asked to choose from a list of 25 topics those that they had been taught at school and those which they had learnt outside school. They were also asked to identify where they had learnt about the topics they had learnt outside school. Topics such as STIs, contraception, puberty and the menstrual cycle had been learnt about in school by the majority of students, while topics such as abortion, miscarriage, menopause, endometriosis and PCOS were more likely to be learnt about outside school (Figures 3 to 5). In terms of the topics learnt outside school, the most common sources were the Internet (70.8%, 659/931) and social media (61.4%, 572/931) (Figure 6).
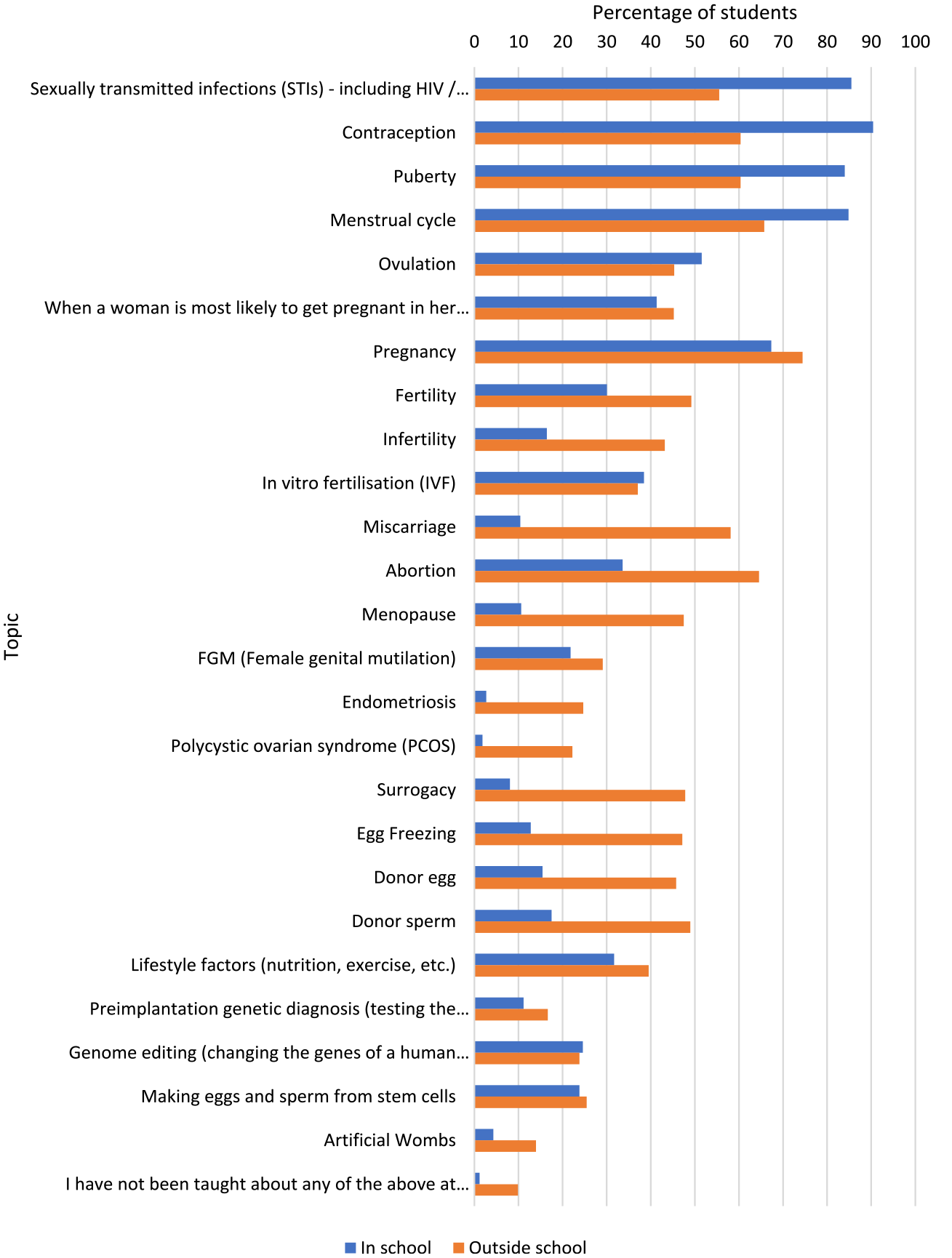
Topics that students reported learning in and outside school, presented as a percentage of students.
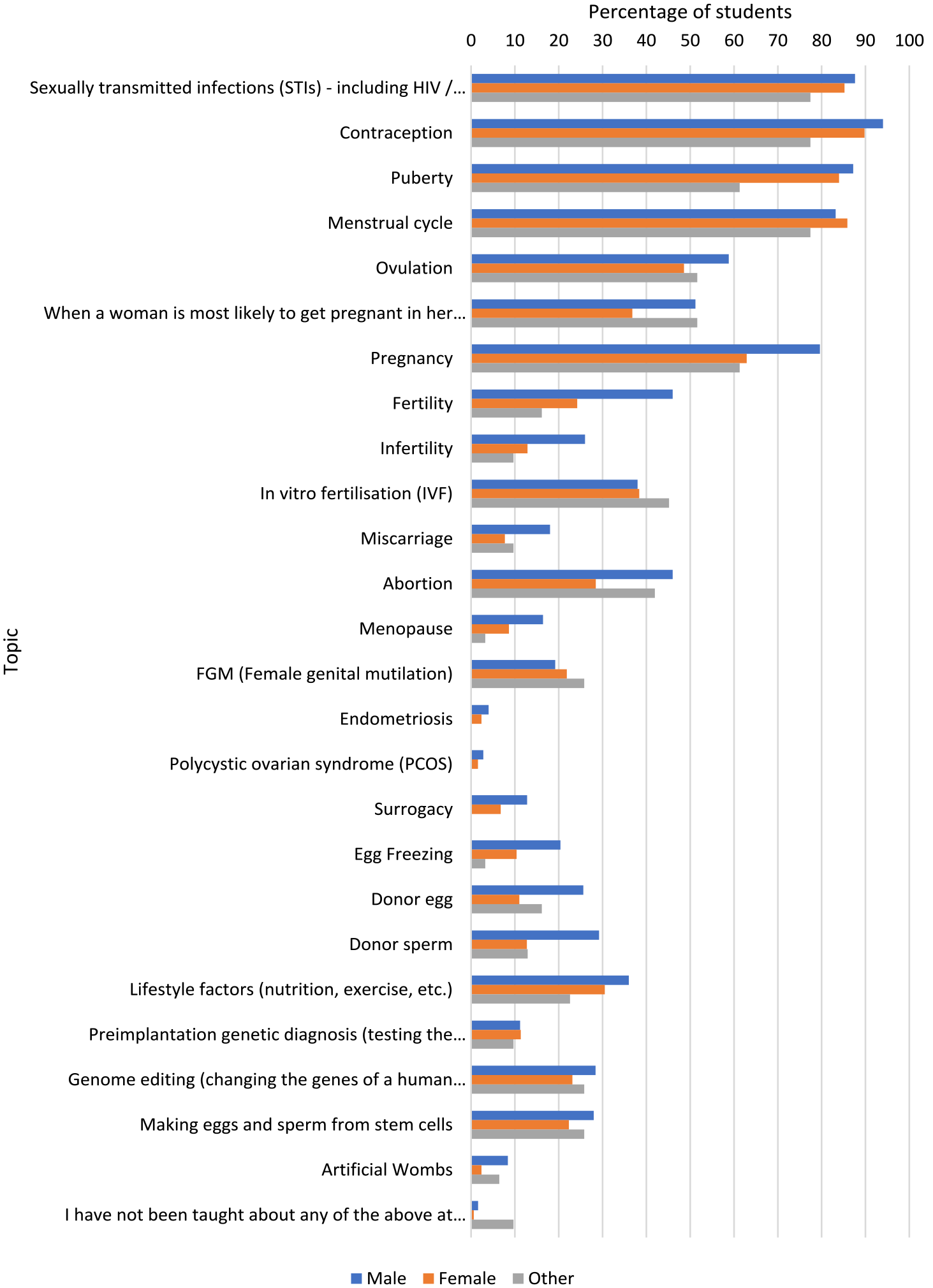
Topics students reported learning in school, by gender.
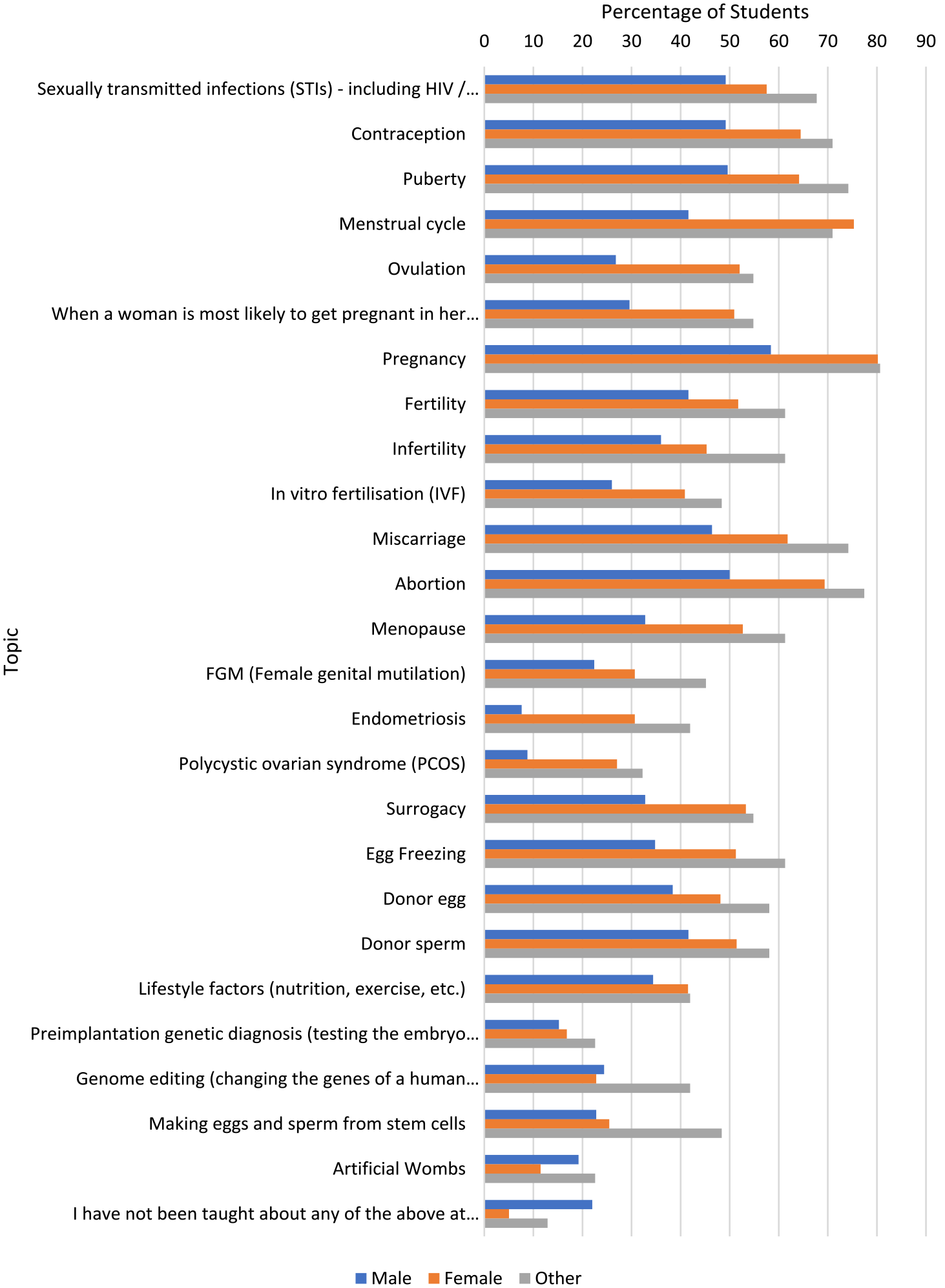
Topics students report learning outside school, by gender.
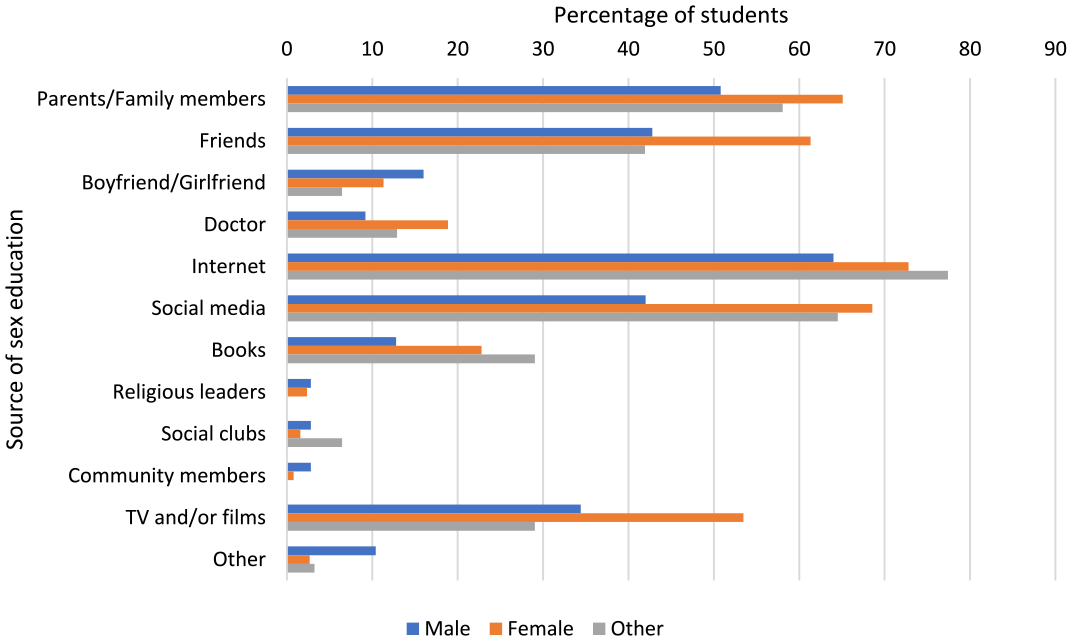
Where students reported learning about topics not learnt in school, presented as a percentage of students, by gender.
The survey also asked students whether their parents/guardians talk with them about sex, fertility and/or having children. Only 21.64% of students (199/931) answered ‘yes’, while 31.8% (296/931) answered ‘no’ and 42.2% (393/931) answered ‘sometimes’. The distribution of responses by gender is shown in Figure 7.
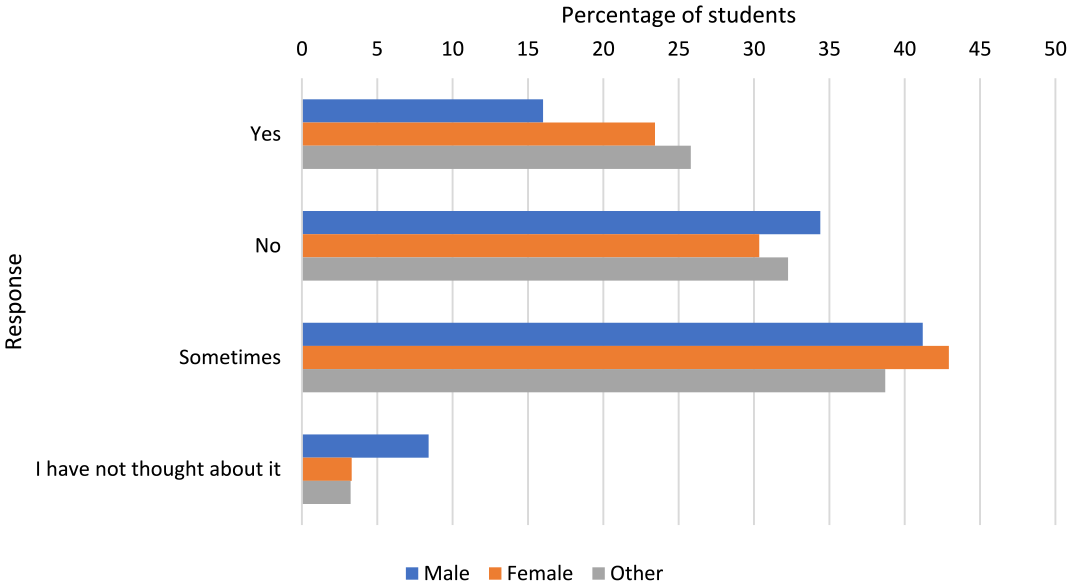
Responses to whether parents/guardians talked to the students about sex, fertility or having children, presented as a percentage of students, by gender.
If students answered ‘no’ to the above question, they were asked why they did not talk to their parents/guardians about sex, fertility or having children and whether they wanted to speak to them about these topics (Figures 8 and 9).
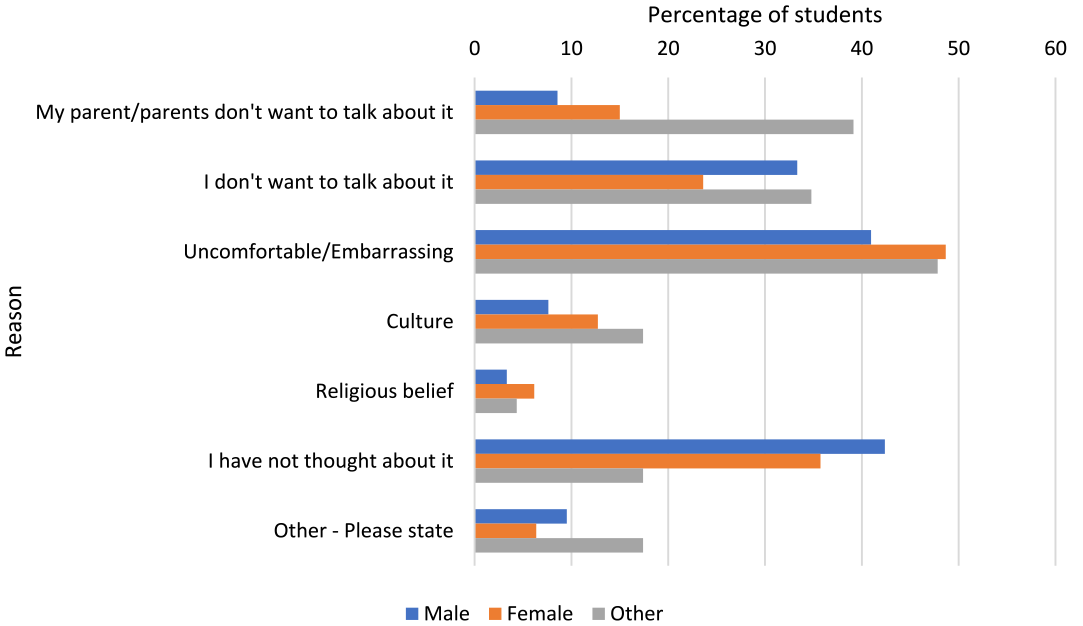
Reasons students do not talk to their parents/guardians about sex, fertility or having children. Presented as a percentage of students, by gender.
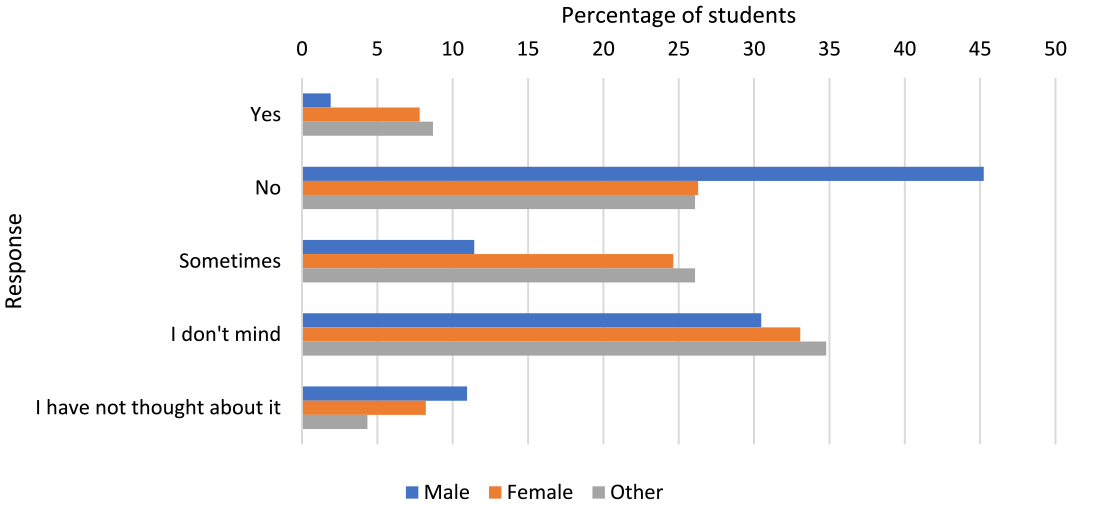
Students’ responses to being asked whether they want to speak to their parent/guardian about sex, fertility and/or having children.
Knowledge of reproductive health topics
Approximately half of the students (51.3%, 478/931) correctly answered that a woman is more fertile around the middle of her menstrual cycle. The majority of students (80.8%, 752/931 and 94.6%, 881/931) correctly answered that men and women, respectively, are most fertile between the ages of 18 and 35 years. When asked about the oldest age they thought a woman could have children naturally, the most popular answer was 45 (23.0%, 214/931), followed by 50 (20.8%, 194/931). Ten students (1.1%) answered that a woman can have children naturally at age 80+. When asked the corresponding question for men, the most popular answer was 80+ (35.6%, 331/931), followed by 70 (12.2%, 114/931).
Students were asked what happens to the quality and number of eggs as a woman ages. Notably, 73.4% (683/931) answered that egg quality deteriorates, and 79.1% (736/931) said that the number of eggs decreases.
When asked about what happens to the quality and number of a man’s sperm as he ages, 54.8% (510/931) answered that the sperm quality deteriorates and 57.8% (538/931) answered that sperm number decreases. Notably, 21.4% (199/931) answered that the sperm number says the same and 19.1% (178/931) did not know what happens to a man’s sperm count as he ages.
Students were asked whether they knew how different groups of people can have children and whether they think parental lifestyle is important for the health of the child. The majority of students reported understanding how single men (79.1%, 736/931), single women (89.8%, 836/931), same-sex female couples (84.0%, 782/931) and same-sex male couples (78.8%, 734/931) can have children. The majority of students (73.1%, 681/931) answered that a healthy lifestyle is important for both parents, in relation to the health of the child.
Chi-square tests were undertaken to determine whether there was a relationship between the amount of sex education students reported having had at school (two classes: ‘quite a lot’, 261 students; and ‘none’ or ‘a little’, a total of 670 students) and their fertility knowledge. There was no association between the amount of sex education received and the frequency of correct responses to any of the questions about fertility knowledge. For example, the cross-tab for the amount of sex education versus time in her cycle when a woman is most fertile (two classes: correct = ‘around the middle of her cycle’; incorrect = all other responses, i.e. ‘anytime in her cycle’, ‘end of her cycle’, ‘I am not sure’ and ‘start of her cycle’) gave a Chi-square result of 0.085 (p = .771).
Qualitative findings
Students were asked how they thought that sex and fertility education in schools could be improved. Five outliers wrote that sex education was fine as it is or could not be improved. The rest felt it could be improved. A thematic analysis of the responses provided enabled five themes to be identified: inclusivity of all students; comprehensive for all students, with relevant topic variety; logistical improvements needed to teaching; the need for honest, transparent and non-judgemental teaching; and sex positivity.
Inclusivity of all students
Students expressed displeasure at the heteronormative nature of current sex and fertility education. They asked that sex education be more inclusive of LGBTQ+ students. They also pointed out that people with disabilities and chronic health conditions may have specific needs when it comes to sex and reproductive health education.
Students recognised the need for a more inclusive approach so that all students are learning things that are relevant to their own lives, circumstances and sexual and reproductive health needs. The vast majority of students who responded requested that all topics be taught to people of all genders and that RSE classes should not be provided separately based on gender.
‘Be more open to all the possibilities and situations rather than the heteronormative situation or the completely healthy body and mind situation’. – Female, bisexual ‘Improve diversity of teaching e.g. more about lgbtq relationships’. – Female, heterosexual ‘. . . And more education about how people in a homosexual relationship can have children. How lessons about sexual health are right now, i can see how someone who is homosexual may feel lost or like there is no opportunity for them to have kids due to the lack of information about it in a lesson, there is too much about heterosexual relationships and not enough about homosexual relationships, even regarding std’s as well’. – Female, heterosexual
Comprehensive, with relevant topic variety
Students were critical of the narrow set of topics taught in RSE and felt that more need to be included. They also felt that the topics that were taught needed to be taught in more detail and in a way that made them relevant to real life rather than just biology. Topics that were frequently suggested for addition to the curriculum included consent, fertility and infertility, endometriosis, PCOS, miscarriage, abortion, masturbation, menopause, menstruation, pregnancy, sexual assault and how to access sexual and reproductive health services.
‘Learn more about issues such as infertility and surrogacy and miscarriage–all we’ve done in school is go over and over having safe sex and talked about periods which whilst is important is barely scratching the surface of things people need to know about. If miscarriage and infertility were better taught, then that could reduce the guilt and embarrassment people who struggle with it would feel’ – Female, heterosexual ‘Make the education a bit more “real world” in the sense that [currently] it can be difficult to apply current knowledge to what is needed in life’. – Male, heterosexual ‘Teach about discharge, erectile dysfunction, masturbation (especially female which gets completely disregarded) and remove the idea of “you don’t need to know that” — we do. Do not use the tea analogy
1
when teaching consent, explain that any unenthusiastic response is a “no” and teach non boys to ask for consent too’. – Female, sexuality unspecified
Logistical improvements to teaching
Students recommended more teaching time be dedicated to reproductive health topics, with an age-appropriate progression of teaching and learning, starting younger and progressing all the way through formal education. They also recommended recruiting specialist speakers and encouraging more open discussion in class. Some students also suggested asking the class what they want to be taught and tailoring information accordingly.
‘More of it- we normally only have around 6-10 sessions per academic year in the senior school and often they don’t teach us enough through that or teach us things that are obvious to us at a later age’. – Male, heterosexual ‘More lessons, less stigma about it, particularly from teachers who may be uncomfortable about it’. – Male, heterosexual ‘just have way more of it in lessons so that it feels normal. PSHE days make it seem weird and occasional. if people have to learn it in class and be tested on it then they’ll actually think about it and remember it’. – Female, bisexual
Honest, transparent and non-judgemental teaching
Transparent and honest teaching and discussion were important to students. Many requested that the taboo around reproductive health topics be removed and that students be empowered to discuss sexual and reproductive health without fear of judgement or stigma. Students wanted the teaching environment to be open and honest, to allow students to ask questions of teachers who are comfortable and knowledgeable about these topics. They also asked that they it be acknowledged that students are mature individuals who need a comprehensive understanding of this information.
‘down the stigma around periods to do with period products, conditions such as endometriosis as we receive no education on those’. – Female, heterosexual ‘Have judgment-free lectures’. – Male, heterosexual ‘Don’t sugar coat it – say it how it is, and be accepting when children have questions or let them ask anonymously since I found it so embarrassing asking in front of a class. Do a Google form or something’. – Female, heterosexual ‘Yes more frequent and detailed information. I do not know so much and I have to look to sources that I can’t trust and are not verified to find out. I want to be told. I also don’t want schools to underestimate the maturity of students as we are being increasingly exposed to this information (correct or not) at a younger age’. – Female, bisexual
Sex positivity
Students said that they are often taught in a way that seems intended to scare them away from having sex. They also felt that they were often only taught the negative consequences of sexual activity and that the importance of sexual well-being was neglected. They requested that female sexual pleasure and the positive aspects of sex be more fully discussed, rather than just a focus on male pleasure.
‘I think female sexual health is quite easily brushed over and needs to be taught in more depth. I think it is also important to be taught sexual pleasure- particularly female sexual pleasure because the orgasm gap is real and part of it is to do with social stigma so I believe it is important to break it. We should also be taught conceiving methods outside the heteronormative range as well as more details about fertility and infertility. I also have never met someone who was taught anything about menopause in school except the fact that it exists- which also contributes towards social stigma. I don’t believe genders or sexes should be separated when learning about sex’. – Female, sexuality unspecified ‘More of an emphasis on sexual enjoyment and pleasure, it would be beneficial to give students a surface level understanding of this topic to avoid much of the awkwardness that comes with first-time sexual experiences. Although I understand the fun of exploring yourself, a lot of men could do with some general knowledge on how to pleasure someone who has a vagina’. – Male, pansexual
Discussion
The aim of this study was to better understand secondary school students’ knowledge and views about reproductive health education. Most students reported having received some sex and reproductive health education at school, but only a minority of students felt that this education had been ‘good’ or ‘very good’. How can we improve this?
Topics relating to sex education, such as contraception, STIs, puberty and the menstrual cycle, were more likely to have been learnt about in school, while a number of other topics relating more to reproductive health, including miscarriage, fertility and infertility, abortion, endometriosis, PCOS and menopause, were more likely to have been learnt about outside school. It is worrying that so few teenagers learn about two disorders that affect so many women: endometriosis (Ellis et al., 2022) and PCOS (Deswal et al., 2020), 2.7% and 1.8%, respectively. Perhaps even more significantly, only just over 10% of respondents reported having learnt about menopause and miscarriage. Almost every woman will go through menopause, and one in four pregnancies end in miscarriage. Menopause surveys have shown that women under 40 (Munn et al., 2022) and over 40 (Aljumah et al., 2022; Harper et al., 2022; Tariq et al., 2023) have very little knowledge of menopause, which negatively affects their experience. These topics should now be taught in schools (Department for Education, 2019). It is interesting that over 20% of students have learnt about ‘sexy science’ topics such as genome editing and making eggs and sperm from stem cells, which are techniques of the future and not strictly relevant to current reproductive health. Sex and reproductive health education would be improved if all the topics listed in Figures 3 to 5 were taught using evidence-based information (Breuner et al., 2016).
The Internet and social media were viewed by students as popular sources of sex and reproductive health information outside school, with variation seen between students of different genders in terms of where they found information outside school. The Internet and social media provide widely available sources of information but the quality of the information being presented has not been evaluated for accuracy, especially with regard to sex education (Fowler et al., 2022). In focus groups we carried out with young people, participants were unsure if online influencers were giving them correct information (Hamilton and Harper, 2023). Sex and reproductive health education might be enhanced by better use of social media to engage young people, especially as some issues are not relevant to them at the current time, such as pregnancy and menopause.
While most students knew the age at which adults are most fertile, our results showed significant misunderstanding of other reproductive health topics such as the maximum age at which women are able to conceive a child naturally and what happens to sperm as men age. Most students showed an understanding of how different groups of people can have children (e.g. same-sex couples and single people) and what happens to a woman’s eggs as she ages. These findings are consistent with the wider literature examining fertility knowledge among secondary school students (Ekelin et al., 2012), as well as among university students (Hashiloni-Dolev et al., 2011; Lucas et al., 2015; Mogilevkina et al., 2016) and young adults (Bunting et al., 2013). Other studies have found that there is an overestimation of the efficacy of assisted reproductive technologies (Hashiloni-Dolev et al., 2011; Lucas et al., 2015). A lack of understanding of basic reproductive health concepts has the potential to lead to people not fulfilling their family goals later in life (Harper et al., 2017; Harper and Botero-Meneses, 2022). These findings therefore emphasise the importance of topics being taught accurately by experienced teachers to enable students subsequently to make informed reproductive health choices.
Respondents in this study had many insightful suggestions as to how sex and reproductive health education could be improved. LGBTQ+ youth are not well-served by the current heteronormative approach to sex education. Students identified this situation needs to be changed, which is in line with wider literature (see, e.g. Cense et al., 2020). A 2022 study interviewed LGBTQ+ university students aged 18–21 years in Northern England about their experiences of sex education and where they gained their knowledge, if not from school sex education (Sill, 2022). Participants reported that the sex education they received in school was neither inclusive nor relevant to their needs. They acquired most of their ‘sex education’ from pornography, online blogs or the Internet (Sill, 2022). It has also been shown that education curricula that are LGBTQ+ inclusive reduce homophobia and homophobic bullying among student populations (Goldfarb and Lieberman, 2021).
Participants also felt that sex and reproductive health education should start at an earlier age and continue for longer in an age-appropriate way. An analysis of the UK curricula relating to sex and reproductive health revealed that the curriculum offered in Scotland is both comprehensive and age-appropriate (Maslowski et al., 2023). The challenge, now, is to find out whether this curriculum is actually being delivered in the intended manner, and how students experience it. It is possible that the Scottish system could be adapted and rolled out across countries to improve the sex and reproductive health education system. Before this, however, we need to determine whether the programme really is being taught effectively and whether students think it is suitable.
Students in the study also wanted sex and reproductive health education to be taught in a sex-positive manner that cultivated honest, non-judgemental discussion about relevant issues. They acknowledged the stigma and taboo that often surrounds sexual and reproductive health and recognised the importance of normalising these conversations. Young people want the education they receive to be realistic, age-appropriate and sex-positive (Coleman and Testa, 2007; Forrest et al., 2004; Hirst, 2013). Hirst (2013) argues that in order for sex education to be useful, positive messages should be central to its teaching. Participants in this study also suggested that sex and reproductive health education could be improved if teachers are well-trained, knowledgeable and confident when talking about sex and reproduction. This is in line with wider research which recognises that sex and reproductive health education should be taught as a special subject and that it is most successful when students feel safe to actively participate (Pound et al., 2016).
Overall, our findings contribute to on-going debate about what might be included within sex and relationships education and how topics might best be taught. There are arguments as to how the relationship between reproductive health education and sexuality education can be conceptualised but in terms of the practicalities of how reproductive health might best be taught in school, it seems appropriate to see reproductive health education as a broader category than fertility education but as a topic that sits within sexuality education/sex education/RSE/sex and relationships education – all terms that have been used to describe these topics.
Limitations
Participants in this study were students, mainly female, attending schools in England, and aged 16–18 years. It would have been interesting to see if students elsewhere in the UK where the approach to teaching may vary share similar views. The somewhat adventitious nature of our sampling strategy (through selected teachers and schools responding to an open call) means that our findings do not give a representative view of all year 12 and 13 secondary school students in England.
Conclusion
In a mixed-methods study that elicited responses to an anonymous, online survey using multiple choice and open-ended questions, we enquired into what 16–18-year-olds in England had learnt, and their views, about sex and reproductive health education. Over half of the students responding to the survey rated their sex education as adequate or worse. Well over half reported that they either do not, or only sometimes, talk to their parents/guardians about these topics. Half did not know when a woman was most fertile. Students showed a better knowledge of female fertility than male fertility. There was no relationship between how much school sex education respondents said they had had and their knowledge of key reproductive health topics.
Students felt strongly that current sex and fertility education was overly heteronormative in character and needed to be more inclusive. They were also critical of the narrow set of topics that were taught to them and many recommended that more teaching time be dedicated to teaching reproductive health. Finally, many students commented that they are often taught in a way that seems intended to scare them from having sex; they also felt that the importance of sexual well-being is neglected. They also wanted female sexual pleasure to be more fully discussed, rather than the present situation where the focus is on male pleasure.
We conclude that schools should be teaching more about reproductive health. The same survey has now been conducted in Belgium, Japan and Greece with slight variations and it will be interesting to compare the data across these countries. This type of research is needed in all countries that wish to bring in or improve the quality of their school reproductive health education. The data collected so far have been used in developing an educational resource under the auspices of IRHEC that will be freely available from that organisation’s website in early 2024.
Footnotes
Acknowledgements
Many thanks to Jacky Boivin, Adam Balen and Mara Simopoulou for reviewing the survey questions. We would like to thank all the schoolteachers for encouraging their students to participate in the study and the students who did so. Many thanks to students who took part in the cognitive interview sessions. The schools that participated in the research were: Bramptom Manor Academy, Clifton College, Herne Bay High School, Hills Road Sixth Form College, Hitchin Girls School, Kensington Aldridge Academy, Joyce Franklin Academy, King Edward VII Academy, London Academy of Excellence, Longsands Academy, Malvern St James Girls School, Marlborough College, Newcastle Royal Grammar School, Richard Taunton Sixth Form College, Rossett School, Royal Masonic Girls School, Saffron Walden County High School and Wheatley Park School.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joyce Harper is the founder of Reproductive Health at Work and gives paid talks about reproductive health. She was also a scientific advisor to Flo, Adora Health and Haleon at the time of this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this project was funded by the Institute for Women’s Health additional fee element, UCL London.
Data availability
The data underlying this article are available on reasonable request to the corresponding author. A copy of the survey used in the study is also available from the corresponding author.