
Abstract
Objective:
Policy development is the biggest gap for health-promoting sports clubs. The present study aims to identify Irish sports club’s involvement in health promotion (HP) policy development.
Design:
Mixed methods concurrent survey design, with quantitative data providing insights into priorities, activities and documentation and qualitative data documenting stakeholders’ perceived needs.
Setting:
Two hundred and thirty-nine sports clubs in Ireland.
Method:
The survey measured perceptions of HP, the importance of promoting 10 health topics (e.g. suicide prevention, healthy eating, addictive behaviours) and corresponding actions relevant to HP in club policy documents and future needs. Quantitative data were analysed using multivariate statistics. The policy cycle was used to conduct a deductive analysis of qualitative data on sports clubs’ perceived needs.
Results:
A high importance score (>70%) was found for the 10 health topics. Sports clubs reported their greatest investment was in physical activity promotion, and the lowest investment was in supporting the participation of disabled people. Up to two thirds of sports clubs had no HP policy. Irish sports clubs’ perceptions of HP showed higher but similar patterns of response relative to sports clubs in other countries.
Conclusion:
Findings suggest that sports clubs consider HP to be an important part of their remit, but up to 66% have no policy in this regard. The policy cycle analysis helped identify the key tools needed to promote sports clubs’ HP policy development. Practical implications include fostering the inclusion of HP in sports clubs’ development plans by establishing templates and receiving support from sports federations.
Introduction
Beyond the contribution of sports participation to levels of physical activity (PA) (Kokko et al., 2019), sports clubs can also enhance the sports experience and health and wellbeing of their members, as well as contribute to sustainable development through health promotion (HP) (Eime et al., 2013). The European Commission White Paper on Sport (European Commission, 2007) has suggested that the HP aspects of sports participation are often undervalued and need to be further developed.
This article focuses on sports clubs that have been defined as having in common ‘the provision of opportunities for competition and sports practice, while some can also be considered social organisations, promoting social welfare and health’ (Donaldson and Finch, 2012: 4). The precise mechanisms through which sports clubs can play a role in fostering positive health behaviours and the health status of their members have been less well studied, however, especially regarding how sports clubs define their priorities and practices in relation to HP, as well as the needs and wishes of their members (Donaldson et al., 2021).
Policies are central to HP development (Golden et al., 2015), be they in the form of formal written policies, unwritten statements, written standards and guidelines, formal procedures, and informal policies (or lack thereof) that may directly or indirectly affect community or population health (Pogrmilovic et al., 2019). HP policies can be considered a first step to developing and supporting HP practice in sports settings (Finch and Donaldson, 2010). Yet, research has shown that coaches’ and managers’ understandings of the value of sports clubs’ policies in relation to HP are often very weak (Lane et al., 2017).
An Australian study demonstrated that only 3% of the 640 included sports clubs had a written policy addressing five key health behaviours (Dobbinson et al., 2006). A previous study of 16 Gaelic Athletic Association clubs in Ireland documented low policy index scores for HP by means of evaluation of eight items on sports clubs’ HP policies based on the Health Promoting Sports Clubs index (Lane et al., 2017). Nevertheless, a pre- and post-evaluation of an HP intervention called the Healthy Club Project helped to increase these scores (Lane et al., 2021), suggesting action can be undertaken to foster organisational changes.
In a study comparing 10 grassroots football clubs in France, officials explained that written documents defining sports clubs HP policy were non-existent and that informal meetings and discussions were largely used to support the approach to HP taken by sports clubs (Van Hoye et al., 2016). Moreover, previous work in Finland revealed that managers’ guidance with respect to HP focused primarily on performance achievement, rather than on non-performance goals (Kokko et al., 2011). The main barriers to HP policy development in sports clubs have been identified as the need for support from health agencies, sample policies to follow, and more information on policy regulation (Johnson et al., 2020; Meganck et al., 2016).
Against this background, the aim of this study was to investigate how sports clubs in Ireland address HP as part of their work. The study assessed HP-related needs, policies and actions in a sample of sports clubs.
Methods
Design
A mixed-methods concurrent survey design was used (Creswell and Clark, 2007), with quantitative data providing insights into priorities, activities and documentation, while qualitative data shed light on stakeholders’ perceived needs. The use of a single questionnaire allowed club officials and members from a broad variety of sports clubs to provide their views in response to the questions asked.
Procedure and participants
In Ireland, 26 Local Sport Partnerships (LSPs) work at a sub-national sport level to promote PA to the community. Each was invited to distribute an email about the project to sports clubs in their area. The email detailed the study’s research aims and provided a consent form and link to an online survey on Qualtrics. The contact person approached was usually a manager (an executive or board member) but could also be a coach or volunteer. An initial email was sent out on 23 May 2022 to the LSPs, and a reminder email was sent in the middle of June. Data were collected between 23 May and 10 August 2022.
Measurement
The study was approved by the Education and Health Sciences Research Ethics Committee of the University of Limerick (reference: 2021_11_05 EHS). The average time taken for questionnaire completion was 20 minutes. Informed consent was sought and obtained on the first page of the online survey. The questionnaire had four different sections: (1) demographic data, (2) HP policy development indicators, (3) HP perceptions and (4) perceived needs to develop HP policies.
Demographics
This first section of the questionnaire elicited information about the respondent and their sports club (gender, age, experience of sports clubs, primary role in the club, number of members and volunteers in the club, club foundation date, club facilities).
HP policy development indicators
This second section of the questionnaire was in two parts: an informal part (importance of health topics as priorities for the club and daily actions taken to provide for these) and a formal part (presence of a health topic in different written documents) relevant to the policy.
In the informal part, questions on important areas for development (‘priorities’) and the ongoing implementation of the club’s actions (‘actions’) in respect of 10 health topics were assessed using a 0 to 100 scale (see Table 1 for details) informed by previous research on health topics (Kokko et al., 2011). In the formal part, participants answered ‘Yes’ or ‘No’ to questions asking whether each of these 10 topics was referred to in the sports club’s written materials (defined for the purpose of this study as a development plan, information for staff, information for participants, signage, or a website).
Priorities and actions of sports clubs in terms of health topics.
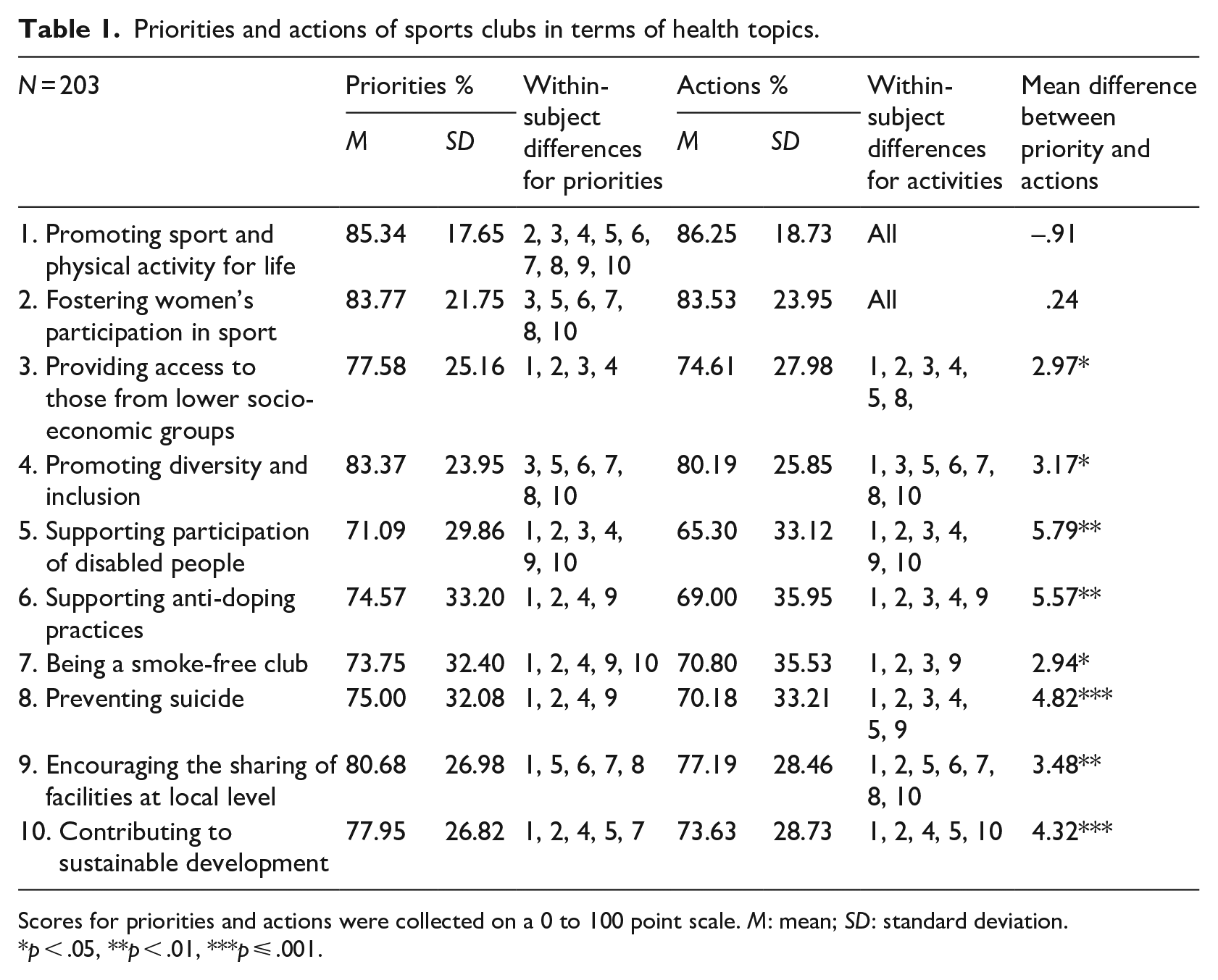
Scores for priorities and actions were collected on a 0 to 100 point scale. M: mean; SD: standard deviation.
p < .05, **p < .01, ***p ⩽ .001.
The 10 health topics chosen were based on those identified in an Irish national policy analysis (Van Hoye et al., 2023), as being supported by national and local policies (e.g. sport, health, youth, and so on). To compare formal and informal policies, two scores were calculated. To know how many health topics were included in formal policies and to identify the strength of the overall HP approach adopted, a health topic score was calculated on a 10-point scale by summing the number of health topics where participants answered ‘Yes’ to having a policy focusing on that health topic. To identify the range of formal policies covering a single health topic, a second score (0–5) was calculated based on the ‘Yes/No’ responses to whether clubs had policies corresponding to each of the five types of policy document previously mentioned.
HP perceptions
This section of the questionnaire evaluated participants’ perceptions of the HP activities undertaken by their club. The macro-level (club-level) scale of the e-PROSCeSS questionnaire was selected, as other scales largely focused on managers’ and coaches’ activities. The scale used was based on the health-promoting sports club model (Van Hoye et al., 2020). It focused on four health determinants: organisational (11 items; Cronbach’s α = .75; e.g. “My sports club has written regulations in regard to health behaviours in general or on specific health topics [e.g. alcohol or drug abuse, healthy eating, and so on]”); social (11 items; Cronbach’s α = .88; e.g. “My sports club promotes integration through sport); environmental (10 items; Cronbach’s α = .71; e.g. “My sports club has clean infrastructures [e.g. locker rooms, practice fields, other spaces]”) and economic (four items; Cronbach’s α = .82; e.g. “My sports club has staff with designated responsibilities to address the health of members”). Respondents responded to each item using a six-point Likert-type scale ranging from ‘Totally disagree’ to ‘Totally agree’. A version of this scale has been previously validated in France with a similar population (Johnson et al., 2022).
Needs regarding the development of HP policy
The questionnaire concluded with an open-ended section structured around the policy cycle (Young and Quinn, 2002). This aimed to elicit information from sports clubs about their perceived needs for the development and implementation of HP policies. The policy cycle is a theoretical model showing the different stages policy development goes through, from agenda setting to evaluation (see Figure 1). Reference to the policy cycle was important as support needs may vary depending on what stage of policy formulation the club has reached (Johnson et al., 2020). It offers a useful way of framing questions to establish what type of support and linkage to which organisation(s) outside of the club may be supportive. One example of a question asked was ‘What does you sports club need to put health promotion on the agenda?’.
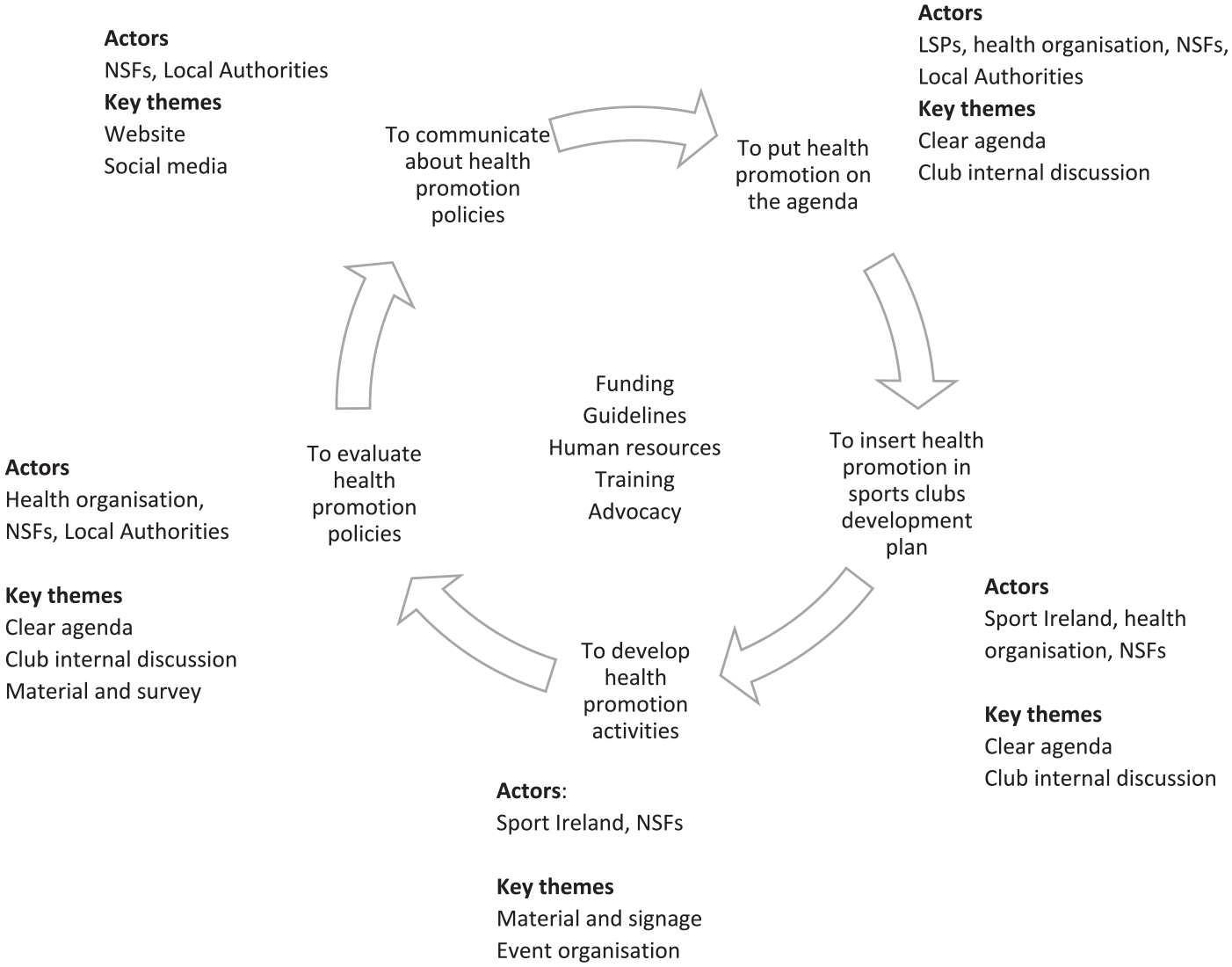
Actors and themes mentioned as support for health promotion in sports clubs, organised with the policy cycle.
Data analysis
Descriptive statistics (means, standard deviations, cross-tabulations) were calculated using SPSS 23. T-Tests were conducted to assess the difference between priorities and actions for each health topic. Two univariate analyses of variance (ANOVAs), with one within-subject factor, were carried out to examine the prevalence of health topics priorities and of health topics actions, respectively. Multivariate analyses of variance (MANOVAs) were used to test gender (male or female), type of sport (individual, collective or multi-sport) and type of respondent (manager, coach, others) for their potential influence on sports clubs’ scores for HP priorities, actions implemented and perceptions.
Requirements of normality (with skewness ranging from −1.50 to 2.04 and kurtosis ranging from −1.20 to 8.22), linearity, homogeneity of variance, homoscedasticity and independence were met. Little’s Missing Completely at Random test (p = .002) showed that data were not missing at random (from 0% to 13% of missing data for the first questionnaires and 45% for the e-PROSCeSS scale), and therefore, data replacement was not undertaken.
Inductive thematic analysis was used to analyse participants’ responses to open-ended questions concerning their sports clubs’ needs in relation to the development of HP policies, for each step of the policy cycle. The policy cycle was used to focus in turn on agenda setting (identification of issues requiring sports clubs’ executive action); policy formulation (to define and formulate policy on them), implementation (to put policy actions in place) and evaluation (to assess the success and effectiveness of the policy) and communication (to disseminate information about the policy and related actions).
The first author coded each unit of meaning deductively using content analysis (Braun and Clarke, 2023) for each of the step of the policy cycle. Each quotation was inputted into an Excel sheet, and categories were created for each step of the policy cycle. The whole team checked the classification and naming of the categories. A recurrence analysis was undertaken on the data collected, including in Figure 1 with only those barriers, which at least three different clubs mentioned in respect of the same theme.
Attention was also given to identifying stakeholders who could be supportive during the different stages of the policy cycle in order to explore how cross-sectoral collaboration could take place to support sports clubs in their work.
Findings
Participants
Three hundred and seven participants clicked a link to the survey. The final sample consisted of 239 participants (77%; 116 women, 121 men, 2 other), who provided answers to more than half of the questions. Their mean age was 33.07 years (SD = 9.47). Almost half of the sample had had more than 15 years’ experience as a club manager (44%), and a further 35% had had more than 5 years experience in their club. Their main activity in the club was manager (66%), coach (20%) or ‘other’ (mostly sports participant) (14%). The types of sports practised were team sports (47%), individual sports (46%) and multi-sports (practising in different sports disciplines, 7%).
Health topics priorities and actions
Respondents’ scores on how much each health topic was a priority for the club ranged from 71% to 85%, with the promotion of PA (85%) being the most prioritized area and supporting participation of disabled people (71%) being the least prioritised one. The ANOVA with one within-subjects factor with all topic scores revealed a significant main effect F(9, 1,773) = 11.35, p < .001, η² = .06, illustrating a significant difference between health topics. Post hoc tests revealed differences between most of the variables (see Table 1).
Respondents’ scores on how much each health topic corresponded to an action in their club ranged from 65% to 86%, with the promotion of PA (86%) being the most highly rated, whereas supporting the participation of disabled people (65%) was the lowest rated. The ANOVA with one within-subjects factor (each topic score) revealed a significant main effect F(9, 1,775) = 21.25, p < .001, η² = .10. Post hoc tests revealed differences between most of the variables.
To compare sports club’s priorities and actions on each health topic separately, paired t tests were calculated on average scores. Results revealed significantly higher scores for priorities than actions for each single health topic, except for two: PA promotion and women in sport participation (see Table 1).
Reference to health topics in sports clubs’ written material
Less than 6% of the clubs reported having all types of written materials (i.e. a development plan, documents for staff and for participants, signage and a website) (see Table 2) on a single health topic, the highest percentage being on promoting PA and the lowest on contributing to sustainable development.
Percentage of sports clubs having existing documents on health topics.
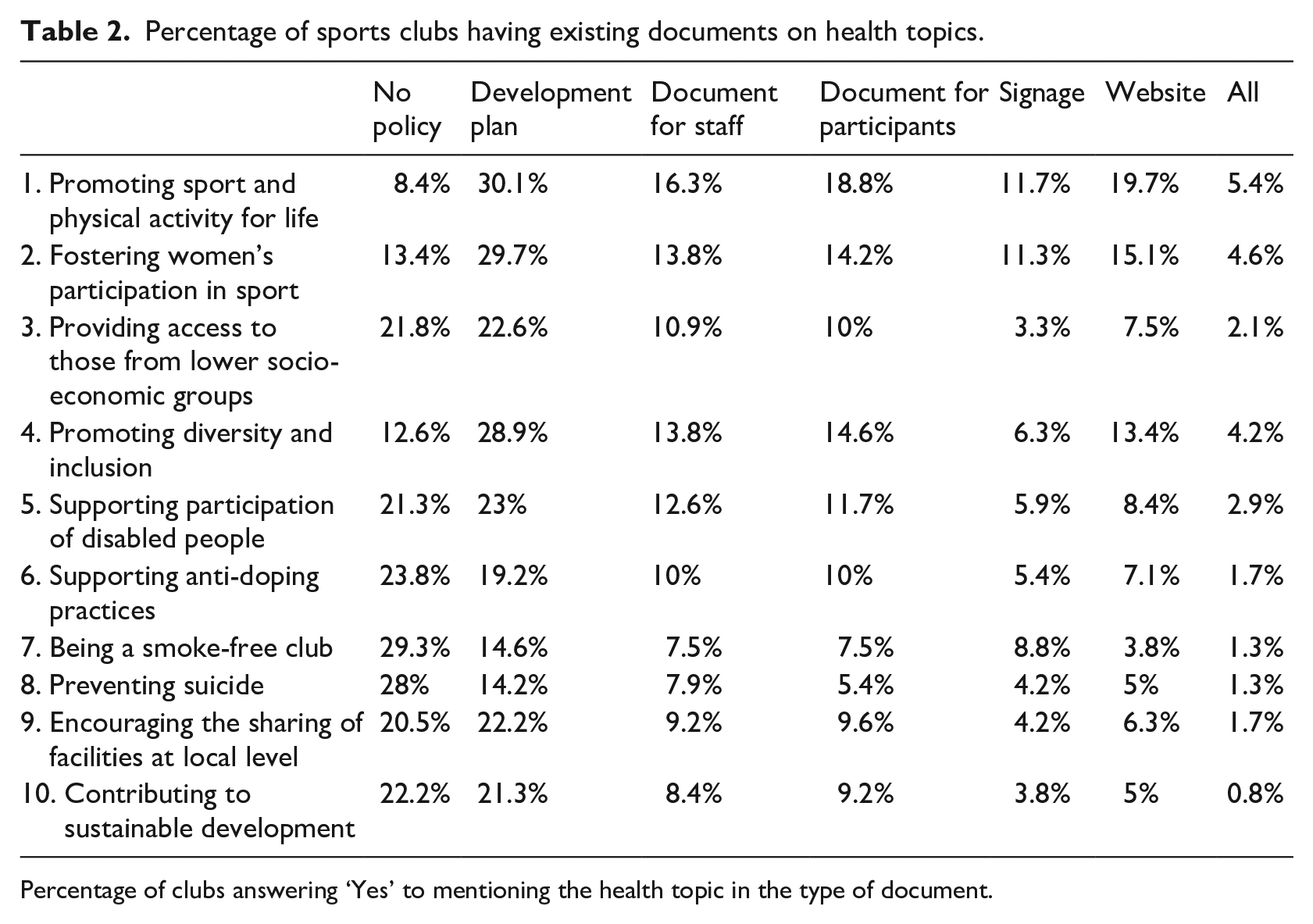
Percentage of clubs answering ‘Yes’ to mentioning the health topic in the type of document.
Only 11% of the sports clubs covered all health topics in their development plan, 10% in information for staff, 5% in information for sport participants, 5% on club signage and 2% on the club’s website. On the 10 health topics that could be covered by a club, the mean number of topics covered by a single club in their development plan was 5.56 (SD = 2.98), 4.40 (SD = 2.92) in the information provided for staff, 4.43 (SD = 2.75) in the information provided for participants, 3.69 (SD = 2.72) in the club signage and 3.89 (SD = 2.41) on the club website. The percentage of clubs not having a policy on any health topic ranged from 8% to 29%. The health topic that received the highest score was being a smoke-free club, which, on the other hand, was the topic least often included in the sports clubs’ policies. The health topic that received the lowest score was promoting PA, which was the health topic most often considered in the sports clubs’ policy. This highlights the important gap between commitment and implementation at the club level.
Development plans mentioning at least one health topic were present for 14% to 30% of sports clubs depending on the health topic. The most targeted health topic was promoting PA, and the lowest was preventing suicide. The percentage of clubs distributing documents to staff and participants ranged from 7.5% to 16% and 7.5% to 19%, respectively. In both categories, the highest-rated health topic was promoting PA, and the lowest-rated topic was preventing suicide. HP Signage had been placed by 4% to 12% of the clubs. The most targeted health topic was promoting PA, and the least was contributing to sustainable development. Having a section on health topics on the club’s website ranged from 4% to 20%, where the most mentioned health topic was promoting PA, and the lowest being a smoke-free club.
Health-promoting sports clubs’ perceptions based on the e-PROSCeSS scale
The HPSC macro scale showed higher scores for social determinants than for environmental, organisational and economic ones. The frequency of a ‘Do not know’ response to items was low (between 0.4% and 3.3%) and was replaced by missing variables (no answer) following a descriptive analysis, as in previous research (Johnson et al., 2022). The ANOVA with one within-subject factor (each topic score) revealed no significant main effect F (3,390) = 100.73, p < .001, η² = .44. Post hoc tests revealed significant differences between all the variables. Scores in Ireland were significantly higher than those in France (see Supplemental Online Appendix 1) for all types of health determinants but showed a similar overall pattern of results.
Confounders
Respondent gender and type of sport showed no significant differences for the different informal and formal policies studied, as well as the type of determinants in the e-PROSCeSS scale. Comparing average scores on each type of determinants of health, only the respondent’s role in the club (either being a manager or coach or ‘other’) affected HP perceptions, Wilk’s λ (8, 250) = 2.67, p < .01, η² = 08. Univariate ANOVA revealed significant differences between the type of respondent, ‘others’ and managers or coaches. The category ‘others’ had significantly lower scores than coaches or managers for the social and environmental determinants.
Qualitative analysis of needs to implement HP
A total of 337 contributions from 105 participants were analysed. Qualitative responses to sports club’s needs at different stages of the policy cycle showed that five themes were cited more than three times for each of the stages: funding, guidelines, human resources, training and advocacy.
Among the different contributions mentioning funding, two main themes were present: grant aid (e.g. ‘a small grant for publishing materials’) and financial inputs (e.g. ‘money’ or ‘funding’). Guidelines were requested in terms of more information (e.g. ‘informed opinion on how to prevent this’ or ‘more knowledge’) or advice (e.g. ‘guidelines we could follow’, ‘list of criteria to follow’). Human resources took the form of the need for more volunteers (e.g. ‘more volunteers’ or ‘more involvement from everyone’) or appointing a specific person to look after HP (e.g. ‘appoint health officer’ or ‘having health promotion volunteers’). Training was mostly cited in the form of the need for workshops at the club (e.g. ‘Holding workshops which are facilitated by people trained in HP to educate club volunteers on how to incorporate these principles into our club agenda’ or ‘free guidance seminars’) or feedback on club activities or raising awareness of club committees (e.g. ‘to provide guidance in the form of online/in person meetings with updated information that will help to understand what we may be missing’ or ‘training for Officers of a club and show them the benefits of it’). Advocacy was considered a necessary step to develop an internal commitment to HP (e.g. ‘If committee members had a better understanding of HP . . . ’ or ‘A well-chosen diverse sub-committee given the remit to be forward thinking’) and to provide evidence on the benefits of HP in sports clubs (e.g. ‘Concise Health Benefits’ or ‘Showing the benefits of promoting general health and increased participation and membership’).
To put HP on the agenda, help was requested from four types of organisations: local sports partnerships, health organisations, national sports federations and local authorities. Except for the opportunity to benefit from the expertise in HP of health organisations (e.g. ‘Expert advice’ or ‘Strong support from health organisations’), the type of support was not specified. Defining a clear agenda for the club (e.g. ‘having health in the centre of agenda’ or ‘Health and Safety are on the Agenda for all Club meetings’) and having internal discussions (e.g. ‘regular meets and club discussions’ or ‘more talks with members as a group setting’) were the two other actions requested by sports clubs in order to put HP on the agenda.
To support the incorporation of HP into a sports club’s development plan, Sport Ireland (i.e. the Irish sports agency), health organisations and national sports federations were the three most requested stakeholders. Sport Ireland was expected to provide guidelines, encouragement and education campaigns, while the two other bodies were asked to provide support in terms of guidance and advice. A clear agenda (e.g. ‘Have them as items for agenda similar to child protection’) and club internal discussion (e.g. ‘Club committee to work together to make goals for the plan’) were also mentioned in this stage.
To develop HP activities, Sport Ireland and national sports federations were asked for support both in terms of guidelines and education campaigns. Themes included the provision of support material (e.g. ‘signage at club once plan is implemented’ or ‘written documents to volunteers’) and support in organising events (e.g. ‘regular guest speakers addressing groups’ or ‘regular activities, encouraging more members to participate’).
To evaluate HP policies, the assistance of HP organisations, national sports federations and local authorities was requested. Two main actions were identified: support in the implementation of a monitoring systems (i.e. a system that can help club to self-evaluate or an evaluation undertaken by the state), and the provision of evaluation templates or surveys. Three themes were also mentioned by more than three people: having a clear agenda (e.g. ‘Set goals/standards’ or ‘Strategic Plan’), using club internal meetings (e.g. ‘Show the club committee that ongoing evaluation would lead to improved outcomes’ or ‘Evaluate HP in talks with participants’) and the provision of evaluation materials or surveys (e.g. ‘provided with a survey template’).
Finally, to communicate HP actions, support was sought from local media, local authorities and national sports federations. Two themes were evident at this stage, the quality of the website and its maintenance (e.g. ‘better website’ or ‘New website currently under development’) and an enhanced social media presence (e.g. ‘Additional information on social media’ or ‘well maintained and moderated social media outlets’).
Discussion
The high scores (>70%) given to the different health topics in this study indicate that sports clubs consider HP to be an important part of their remit. This is encouraging in comparison to previous Flemish results, which showed that 30% of sports club managers did not consider HP a priority (Meganck et al., 2014). Sports clubs’ greatest investment was in PA promotion, which is the health topic closest to their core business (i.e. their sports offer) (Kokko et al., 2019). This finding is similar to that reported in previous French (Van Hoye et al., 2018) and Finnish (Kokko et al., 2011) research. Support for disabled people to participate also received low scores both in terms of priority and daily activities and is consistent with a previous literature review that showed that sports clubs mostly fail to provide activities for members of this population or only do so in the form of short-term programmes or events (Geidne and Jerlinder, 2016).
Participating clubs also scored higher for ‘priorities’ than ‘activities’ for most health topics, illustrating a strong commitment, but fewer activities undertaken, similar to findings in previous studies (Van Hoye et al., 2018). Regarding policy support for implementation, the findings are noteworthy, as PA has been the topic most promoted by national governments across Europe in the last few years (Gelius et al., 2021; Van Hoye et al., 2019) and is included in monitoring systems (Gelius et al., 2021). In addition, being a smoke-free club was of low priority, despite national public health policies to reduce smoking, both in Ireland and elsewhere in Europe. This may perhaps be explained by the fact that smoking policies rarely see sports clubs as their main target, and sports clubs do not have the person power to enforce the policy (Lane et al., 2021). Support for anti-doping practice might be expected to be considered very important for sports clubs as it concerns performance and respect for sports regulations and is therefore linked to the core business of the clubs. However, this was not the case in the present work. Similar findings have been found in respect of substance use prevention (Van Hoye et al., 2018).
Depending on the health topic concerned, up to one third of the sports clubs in this study reported including HP in their development plan, which stands in contrast to findings from a qualitative study in France in which sports clubs reported not having any HP policies at all (Van Hoye et al., 2016). Our findings are however similar to those in a previous Irish study (Lane et al., 2021) and in an Australian study of 640 sports clubs (Dobbinson et al., 2006), where the number of clubs that reported having a policy on a health topic ranged from 9% to 45%. A study of the Gaelic Athletics Association Healthy Club project revealed that clubs involved in the programme developed initiatives on four health topics on average: PA, diversity and inclusion, healthy eating and mental fitness. Anti-bullying education and substance use education were the least invested in areas of work (Lane et al., 2021). These results are better than those previously found in a study of 640 Australian sports clubs, where only 3% of clubs had a policy on five different health topics: being a smoke-free club, sun protection, healthy catering, the responsible serving of alcohol and injury prevention (Dobbinson et al., 2006).
Of the 10 health topics addressed in the questionnaire administered in this study, the mean number of topics covered in development plans was five, with a further four being mentioned in other documentation. The Australian study cited earlier (Dobbinson et al., 2006) identified the challenge of having a policy targeting multiple behaviours. These results are important if we want sports clubs to consider HP as a means of fostering participants’ health, as recommended by public health researchers. Engaging with multiple behaviours as part of an intervention can have a synergistic effect, increasing the impact of the intervention (Lippke et al., 2012; Lippke and Ziegelmann, 2008). Moreover, multi-level strategies call for the need to strengthen the development of health-promoting sports clubs using a settings-based approach (Dooris, 2006).
With respect to HP, Irish sports clubs’ perceptions followed a similar pattern to that observed in several other European countries, including Finland (Kokko et al., 2009), Belgium (Meganck et al., 2014) and France (Johnson et al., 2022), with social and environmental determinants of health receiving higher scores than organisational and economic ones, and with scores in Ireland being much higher than those in France. There is a need therefore to work on organisational and economic factors relevant to HP in sports clubs, and a good starting point for this is through policy documents and processes within the club (Johnson et al., 2022).
The results of this study suggest that Irish sports clubs’ needs in regard to development and implementation of HP policies are close to those identified in Australian and Belgian research concerning HP in sports club settings (Casey et al., 2012; Meganck et al., 2016). Five themes recurrent across the policy cycle category were the need for funding, human resources, guidelines, training and advocacy, which identified elsewhere as key priorities given the voluntary nature of sports clubs and their work (Casey et al., 2012).
Strengths and limitations
This study has several strengths, including the diversity of participating sports clubs, as well as a specific focus on HP policies in sports clubs, both quantitatively and qualitatively. Nevertheless, several limitations should be noted. First, the sample was a convenience sample and is not representative of Irish sports clubs since the survey was sent out through LSPs and not to sports clubs directly. Second, data were self-reported and may reflect biases such as overestimates of HP perceptions and actions by sports clubs’ representatives. No observations of HP action or sports clubs document analysis were undertaken to cross-check the results. Future work could usefully focus on a smaller number of clubs, investigating both self-reports and written documentation, complemented by field observation at the clubs, to better understand policy framing, as well as to provide insight into policy implementation.
Conclusions
Study findings show that Irish sports clubs prioritise HP to some extent and are undertaking relevant actions, even if the highest priorities tend to focus on PA promotion, rather than engagement with other health issues such as smoking or suicide prevention. Importantly, not every sports club had a development plan and/or other policy documents making reference to health topics, meaning there is considerable room for improvement in terms of HP. Future research is needed to understand why sports clubs invest more in some health topics rather than others, as well as how sports clubs in Ireland develop and implement their HP policies.
Supplemental Material
sj-docx-1-hej-10.1177_00178969231221956 – Supplemental material for Health promotion policies, perceptions, actions and needs in sports clubs in Ireland
Supplemental material, sj-docx-1-hej-10.1177_00178969231221956 for Health promotion policies, perceptions, actions and needs in sports clubs in Ireland by Aurelie Van Hoye, Benny Cullen, Aoife Lane, Kevin Volf, Liam Kelly, Enrique Garcia Bengoechea, Anne Vuillemin and Catherine Woods in Health Education Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this project received funding from the European Union’s Horizon 2020 Research and Innovation Programme under a Marie Skłodowska–Curie grant agreement (reference: 101028401).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.