
Abstract
Objective:
Over the past three decades, cultural competence has been widely promoted in the health disciplines, including in health education and promotion, as a tool to address health disparities and promote health equity among diverse populations. Cultural intelligence (CQ), or the individual’s capability to adjust to cultural situations based on multiple factors including cognitive, metacognitive, motivational and behavioural characteristics, can be another useful tool when addressing the needs of diverse groups. The goal of this study was to assess the level of CQ among health education specialists and its relationship with cultural competence skills (CCS) among members of this group.
Design:
Five hundred and forty randomly selected health education specialists in the USA completed an online survey. The survey included questions to assess CQ, CCS and demographic information. Descriptive statistics and analysis of variance were used to analyse the data.
Results:
Results from the study showed that there was a significant variation in CQ among health education specialists based on race/ethnicity, education, the percentage of cultural/racial/ethnic diverse people they serve, and participation in professional development training. There was also a positive correlation between CQ and CCS, and between each of the CQ capabilities and CCS. Finally, both CQ metacognitive and cognitive capabilities were significant predictors of the overall CCS score.
Conclusion:
Findings from this study showed that CQ is associated with CCS among health education specialists. The results of the study suggest that health education specialists should consider CQ a useful tool with which to increase CCS.
Keywords
Introduction
Over the past three decades, cultural competence has been widely promoted in the health disciplines, including health education and promotion, as a tool with which to address health disparities and promote health equity among diverse populations (Luquis et al., 2006; Luquis and Perez, 2003, 2005, 2006, 2008, 2014, 2021; Orlandi et al., 1992; Tervalon and Murray-García, 1998). Cultural competence has been defined as ‘a developmental process defined as a set of values, principles, behaviours, attitudes, and policies that enable health professionals to work effectively across racial, ethnic, and linguistically diverse groups’ (Joint Committee on Health Education and Promotion Terminology, 2012: 11). The National Center for Cultural Competence (NCCC) (n.d.) describes cultural competence as a ‘set of values and principles, and demonstrated behaviours, attitudes, policies, and structures that enable them [organisations] to work effectively cross-culturally’. Similarly, cultural competence has been defined by the US Department of Health and Human Services as ‘a set of congruent behaviours, attitudes, and policies that come together in a system, agency, or among professionals that enables effective work in cross-cultural situations’ (as cited by Luquis, 2021: 834).
The NCCC (n.d.) further sees ‘cultural competence is a developmental process that evolves over an extended period’ with individuals being ‘at various levels of awareness, knowledge, and skills along the cultural competence continuum’. For some time, cultural competence has been an integral part of the competencies and sub-competencies of health education specialists in the USA (National Commission for Health Education Credentialing (NCHEC), 2019) and the broad competencies of public health professionals working with diverse populations (Council on Education for Public Health (CEPH), 2016). As health education specialists seek to develop further their cultural competence along the continuum, Luquis (2021) has proposed that health education specialists may find it helpful to use cultural intelligence (CQ), or the capacity to function effectively in culturally diverse situations (Cultural Intelligence Center (CIC), 2021), as a useful tool when addressing the needs of diverse populations.
While the concept of CQ shares some similarities with cultural competence, it draws from intelligence research, including emotional and social intelligence, and stresses an understanding of diverse cultures, problem-solving and adaptations in various cultural settings (Earley and Peterson, 2004; Livermore, 2011). Earley (2002) defined CQ as the individual’s capability to adjust to cultural situations based on multiple factors including their cognitive, motivational and behavioural characteristics. CQ reveals the individual’s ability to gather, understand and take actions to function effectively in multicultural situations and across cultural settings (Ang et al., 2007; Earley and Peterson, 2004; Solomon and Steyn, 2017). Based on Sternberg’s (1986) theoretical framework of different ‘loci’ of intelligence, Earley and Ang argued that intelligence goes beyond cognitive abilities to include motivational and behavioural capabilities, leading to their development of the concept of CQ. Ang and Van Dyne have further developed the multidimensional aspects of CQ which they see as characterised by four different factors: cognitive CQ (or CQ knowledge), metacognitive CQ (or CQ strategy), motivational CQ (or CQ drive) and behavioural CQ (or CQ action) (Ang et al., 2007; CIC, 2021; Earley, 2002; Earley and Peterson, 2004; Livermore, 2011; Rockstuhla and Van Dyne, 2018; Solomon and Steyn, 2017).
CQ knowledge refers to an understanding of culture, cultural values, cultural differences and the cultural self, as well as how culture shapes the individual’s behaviour (Earley, 2002; Earley and Peterson, 2004; Edwards, 2017; Livermore, 2011). Individuals with high CQ knowledge understand the differences and similarities between cultural groups (Ang et al., 2007). CQ strategy represents an individual’s awareness and ability to plan when confronting cross-cultural situations (Earley, 2002; Livermore, 2011). An individual who possesses high metacognitive CQ is aware of, and questions, cultural assumptions when interacting with other individuals (Ang et al., 2007). This could be the result of either formal education or personal experience based on their own background or professional training. Constructs of CQ knowledge and strategy go beyond a basic understanding of health-related beliefs, practices, cultural values, and the incidence and prevalence of chronic diseases among racial and ethnic groups as is often discussed via the concept of knowledge as part of cultural competence (Luquis, 2021). Health education specialists with an understanding of cultural systems, interpersonal and cultural values, and cultural differences between diverse groups can be more effective cross-culturally (Luquis, 2021). Health education specialists who can anticipate cultural dynamics and plan appropriately tend to be more effective when interacting with members of diverse communities.
CQ drive describes the individual’s motivation to use their cultural knowledge to engage and direct their attention to learning to function in cross-cultural situations (Ang et al., 2007; Earley, 2002; Livermore, 2011). Unlike cultural competence, CQ drive relies on ‘intrinsic motivation’ (i.e. natural interest and enjoyment of cultural experiences), ‘extrinsic motivation’ (i.e. the benefits from such interaction) and self-confidence (i.e. self-efficacy to engage in interaction) (Konanahalli et al., 2014; Livermore, 2011). It has been suggested that health education specialists who have the confidence and drive to function in culturally diverse settings will be more successful in navigating these experiences (Luquis, 2021). Finally, CQ action (behavioural) implies the flexibility to behave and act appropriately within a particular cultural setting and/or cross-cultural situation (Earley, 2002; Earley and Peterson, 2004; Livermore, 2011). Those with behavioural CQ show appropriate behaviours informed by their broad range of verbal and non-verbal communication skills (Ang et al., 2007). Moreover, behavioural CQ has been further defined as ‘an individual’s capability to enact a wide repertoire of verbal and nonverbal actions when interacting with people from different cultures’ (Van Dyne et al., 2012: 304). While culturally competent individuals may conduct themselves according to their understanding of the values and beliefs of different cultural groups, individuals with behavioural CQ will carefully assess whether the situation requires changes in their behaviour by drawing on their CQ knowledge and strategy. Health education specialists who can recognise and adapt their actions in encounters with culturally diverse groups are more likely to effectively navigate these situations in a culturally appropriate manner. CQ actions (behavioural) connect to the other CQ elements of knowledge, strategies and drive (Luquis, 2021).
Although CQ may be a new concept for many health education specialists in the USA (i.e. health educators or health promoters), other disciplines and professions (i.e. health care, business, education) have learned and applied CQ in their respective fields. For example, CQ has been associated with professional competencies, culturally appropriate care and leadership skills in nursing (Göl and Erkin, 2019; Rahimaghaee and Mozdbar, 2017; Richard-Eaglin, 2021). Similarly, Solomon and Steyn (2017) have found that CQ helps improve employees’ performance, involvement, satisfaction and adaptation when working cross-culturally; Edwards (2017) has advocated the use of CQ to enhance the clinical practice of social work practitioners to improve their work with culturally diverse populations. Richard-Eaglin (2021) has stated that professionals with high CQ demonstrate flexibility in adjusting their views, behaviours and skills in cross-cultural interactions. Thus, in principle, we might expect that health education specialists with a high level of CQ should be more competent when engaging with diverse cultural groups and working in cross-cultural settings. Using a CQ approach, health education specialists can develop more personalised cross-cultural interactions, based on a psychological model of cultural adaptation that engages with knowledge, learning, motivation and behaviour (Luquis, 2021). Finally, action to develop CQ allows health educators to practice cultural competence skills (CCS) in different settings while acquiring the confidence to work with diverse populations.
As health education specialists work with diverse populations within the USA and elsewhere, they may find it helpful to utilise the CQ framework in their work (Luquis, 2021). Having high levels of CQ may be beneficial when assessing diverse populations’ needs and developing and evaluating health promotion programmes as part of the health education specialists’ professional role. Despite the benefits of incorporating CQ into health education, no previous study has assessed the level of CQ and its relationship to professional characteristics and skills among health education specialists; hence, there exists a gap in the health education and health promotion literature. The goal of this study, therefore, was to assess the level of CQ among health education specialists and its relationship to expected CCS among members of this group. The study aimed to answer the following questions: (a) what is the overall level of CQ among health education specialists; (b) what is the level of each of the CQ components (knowledge, strategies, drive and actions) among health education specialists; (c) what demographic characteristics contribute to CQ and CCS levels among this group; and (d) what is the relationship between overall CQ, each CQ component and CCS among members of this group? The findings of this study should help to identify the level of CQ and factors associated with it among health education specialists. Findings from this study may also highlight the need for health education specialists to include CQ concepts as tools to learn to increase professional competence when engaging with diverse cultural groups and working in cross-cultural settings.
Methods
Sample
The authors purchased and received permission to use the list of current National Commission for Health Education Credentialing Inc. (NCHEC)-certified health education specialists in the USA. The NCHEC certifies health education specialists (i.e. health educators and health promoters), promotes professional development and strengthens professional preparation and practice. The list contained approximately 12,000 names and email addresses for active members. Four thousand participants were initially randomly selected from the list to participate in the study. Each participant received an initial invitation email and two reminders 3 and 6 weeks after the initial invitation. Due to an initial low response rate (less than 10%) after two reminders, we decided to randomly select an additional 4,000 participants from those not initially selected. Like the initial group, members of this group received an initial invitation and two subsequent reminders. Each participant was given the chance to enter a random draw for 10 Amazon gift cards of $25 as an incentive for their participation. A separate link was included at the end of the survey for those who chose to participate in the draw to keep their contact information separate from their survey responses. Participants in both of the above groups received a link to access the survey which also contained the informed consent form and contact information for the PI and Co-PI. Implied consent was obtained as part of this study by completion of the survey, and participants were asked to keep a copy of the consent statement for their records.
Procedure
Instrument
A survey instrument was developed by the authors. It included 12 questions to assess participants’ demographic characteristics and whether they had received cultural/diversity training as part of professional development. The survey also included the Expanded Cultural Intelligence Scale (39 items) to assess levels of CQ (CIC, 2018). The scale includes 9 items to measure motivational CQ, 12 items to measure cognitive CQ (i.e. cultural general and context-specific knowledge), 9 items to measure metacognition CQ and 9 items to measure behavioural CQ. The overall scale has been validated and determined to be reliable to measure each CQ capability score and the overall CQ score (Van Dyne et al., 2012).
Data collection
Participants completed the survey using the Qualtrics platform. Once they had begun the survey, participants could skip any question they did not want to answer. Completion of the survey took between 15 and 20 minutes. The study protocol was approved by the Pennsylvania State University and Fresno State Institutional Review Boards.
Following a series of demographic questions, participants were asked to select the answer that best described their capabilities relative to those of their peers on a 7-point Likert-type scale (1 = strongly disagree; 7 = strongly agree) in response to statements related to their level of CQ in each of the capabilities. A high score represented a high CQ capability and high capability in each of the subscales. Participants responded to statements such as: ‘I thrive on experiencing cultural differences that are new to me’, ‘I can describe different views of beauty and aesthetics across different cultures’, ‘I adjust my understanding of a culture while I interact with people from that culture’ and ‘I change my use of pause and silence to suit different cultural situations’. Reliability analysis using the study data showed high reliability for the full CQ scale (Cronbach’s alpha = .952) and respective subscales, motivational CQ (Cronbach’s alpha = .852), cognitive CQ (Cronbach’s alpha = .917), metacognitive CQ (Cronbach’s alpha = .898) and behavioural CQ (Cronbach’s alpha = .929).
Participants were also asked to respond to a 15-item scale to assess their cultural and linguistic competence-related skills (CCS). The 15 items were developed based on published literature and the NCHEC (2019) and CEPH (2016) expected cultural and linguistic competence-related skills for health education specialists (Luquis and Perez, 2021). The 15 items represent health education specialists’ competencies, including whether participants can conduct a culturally related needs assessment; plan, implement and evaluate culturally appropriate health education intervention; and develop culturally and linguistically appropriate content to implement with diverse populations. Each participant was asked to select the answer that best described their level of competence as part of their job using a 5-point Likert-type scale (1 = strongly disagree; 5 = strongly agree). Statements included items such as: ‘I can design culturally appropriate public health, health education, and/or health promotion interventions’, ‘I can develop culturally and linguistically appropriate strategies and materials’, ‘I can understand and respect values, attitudes, and beliefs among diverse ethnic/racial and cultural groups’ and ‘I can recognize and adapt to cultural differences in the public health context’. Reliability analysis using the current data showed high reliability for this scale (Cronbach’s alpha = .953). A factor analysis, using data from the current study, with a varimax rotation on the 15 items showed that two factors accounted for 67% of the variance. The result was derived using a factor loading of .5 or greater as a criterion to identify the different factors. The two factors included the capacity to assess needs, develop, implement and evaluate culturally and linguistically appropriate health education programmes, content and strategies for diverse populations (9 items), and the capacity to understand, recognise and adapt to diverse cultures, and to identify resources and factors impacting diverse populations (6 items) (the result of this analysis is available upon request from the corresponding author of this paper).
Data analysis
Descriptive statistics including measures of central tendency were used to describe the results of the study. Analysis of variance (ANOVA) was conducted to determine the differences in CQ and CCS levels based on participants’ race/ethnicity (i.e. White, Black, Hispanic) and their degree of education (i.e. bachelor’s, master’s, professional). ANOVA was also used to compare the variance in CQ and CCS levels among those participants who worked with different percentages of diverse people (i.e. 0–25, 26–50, etc.) and those who had attended training in diversity (i.e. Yes, No). Pearson correlation coefficient and multiple regression analysis were used to determine the relationship between CQ and CCS. All the analyses were conducted using SPSS software version 28. A significant value of p < .05 was used to determine the significance of the results.
Findings
Of the 8,000 individuals invited to participate in the study, 673 completed the survey and 540 completed all the questions. Results from the descriptive analysis revealed that the majority of the respondents had at least one degree in health education (100%), were women (89%), were aged between 20 and 49 (77%), identified as White-non-Hispanic (66%), had a master’s degree (60%), worked full-time (87%), had been working in health education less than 15 years (73%) and had participated in cultural/diversity training (83%). Over one-third (36%) of the participants lived in the South of the USA, followed by the West (27%) and Midwest (21%). Over one quarter of participants worked in public health departments/government offices (28%), followed by academia/higher education (24%), community organisations (16%) and healthcare settings (15%). When asked to estimate the percentage of diverse people they work with, less than one-third (29%) indicated that 26%–50% of the people are from diverse backgrounds (see Table 1).
Demographics and other characteristics of participants (N = 542).
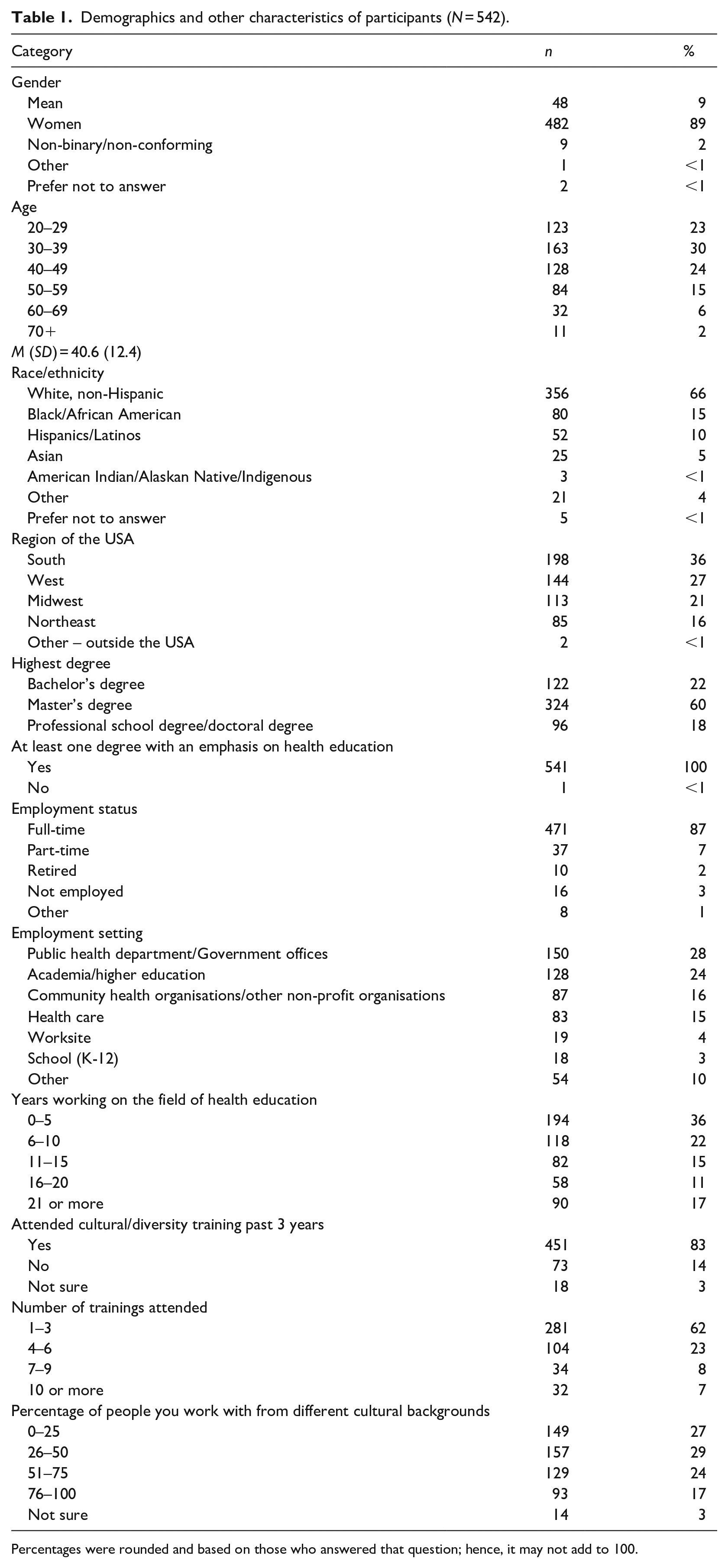
Percentages were rounded and based on those who answered that question; hence, it may not add to 100.
For scores on the CQ scale and each dimension, the average of the sub-dimensions was used to create average scores for the four factors and the full scale. Similarly, the average score was calculated for the CCS scale. Results showed that the mean scores of CQ motivational and CQ metacognitive were higher than the other CQ capabilities and the overall mean score of CQ. The mean score of CCS showed that on average participants felt confident in performing each of the skills (see Table 2).
Descriptive statistics for cultural intelligence, its dimensions and cultural competence skills.

ANOVA was conducted to determine the differences in CQ and CCS levels based on participants’ race/ethnicity (i.e. White, Black, Hispanic) and their degree of education (i.e. bachelor’s, master’s, professional). ANOVA was also used to compare the differences in CQ and CCS levels between participants working with different percentages of diverse people (i.e. 0–25, 26–50, etc.) and those who had attended training in diversity (i.e. Yes, No). This revealed a significant difference in CQ between health education specialists by race/ethnicity, F (3, 528) = 27.00, p < .001, education, F (2, 534) = 4.22, p = .015, and the percentage of people respondents served or worked with (i.e. students, clients, community members) who came from diverse backgrounds, F (4, 532) = 14.63, p < .001. There was no significant difference in CQ based on whether they had participated in cultural/diversity training. Due to the small size of some of the race/ethnicity categories, race/ethnicity was combined into four categories: White, non-Hispanic, Black/African American, Hispanic/Latino and others. A post hoc Bonferroni analysis showed that White, non-Hispanic individuals had a lower mean CQ overall score compared to the Black/African American, Hispanic/Latino and other racial/ethnic groups. Participants with higher levels of education and a higher percentage of diverse clients had a higher CQ total mean score (see Table 3). A post hoc Bonferroni analysis showed that those individuals with a bachelor’s degree had a lower mean CQ overall score compared to those with a master’s degree or professional qualification. A post hoc Bonferroni analysis also showed that those participants who worked with a higher percentage (i.e. over 76%) of diverse clients had a higher mean CQ overall score compared to those with less than 75% of diverse clients. Similarly, the ANOVA showed significant differences in CCS between health education specialists based on race/ethnicity, F (3, 531) = 7.79, p < .001, education, F (2, 537) = 4.79, p = .009, the percentage of people from diverse backgrounds served, F (4, 532) = 7.84, p < .001, and whether they participated in a cultural/diversity training, F (2, 534) = 3.24, p = .040. A post hoc Bonferroni analysis showed that White, non-Hispanic participants had a lower mean CCS score compared to Black/African American, Hispanic/Latino and other racial/ethnic groups. A post hoc Bonferroni analysis also showed that those with a higher degree (e.g. PhD or professional doctorate) had a higher mean CCS score than those with bachelor’s or master’s degrees. A post hoc Bonferroni analysis showed that those who worked with a higher percentage of diverse clients (i.e. over 50%) had a higher mean CCS score compared to those who worked with less than 50% of diverse clients. Finally, those who had participated in cultural/diversity training had higher mean CCS scores than those who had not participated in this type of training (see Table 3).
Cultural intelligence and cultural competency skills mean score, by participants’ characteristics.
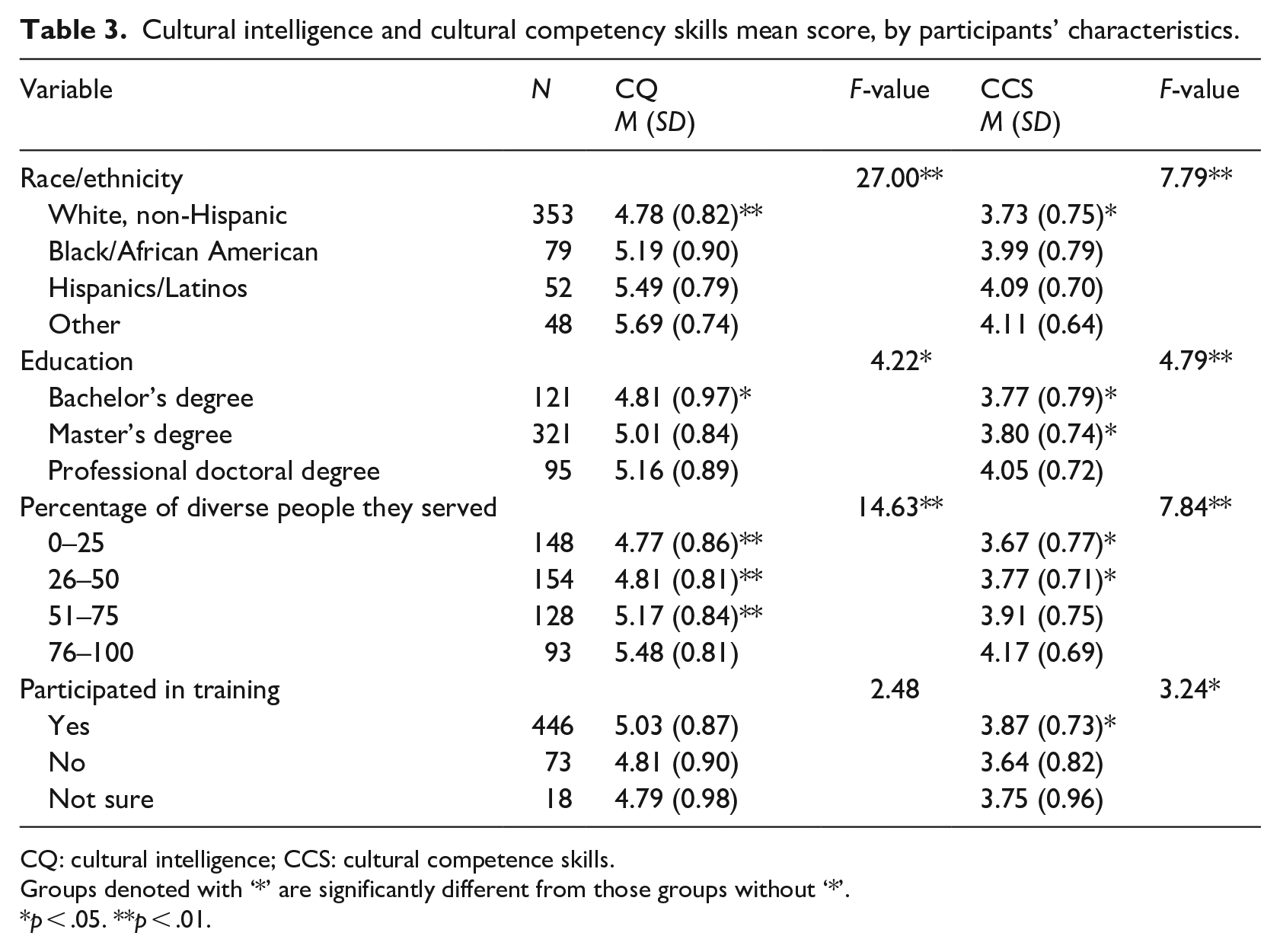
CQ: cultural intelligence; CCS: cultural competence skills.
Groups denoted with ‘*’ are significantly different from those groups without ‘*’.
p < .05. **p < .01.
Results from the correlation analysis showed a significant positive relationship between CQ and CCS (r = .632, p < .01). This relationship was also significantly positive for cognitive (r = .581, p < .01), metacognitive (r = .561, p < .01) and behavioural (r = .497, p < .01) CQs. While the relationship between CCS and motivational CQ was also significant, it was low (r = .340, p < .01) (see Table 4). To determine the effect of each of the CQ dimensions (i.e. independent variables – motivational, cognitive, metacognitive and behavioural) in predicting CCS among health education specialists and to determine the best predictors of CCS (i.e. dependent variable), a multiple regression analysis was conducted. The overall regression was statistically significant, R2 = .421, F (4, 530) = 96.28, p < .001. Results analysis showed that both cognitive CQ (β = .362, p < .001) and metacognitive CQ (β = .297, p < .001) were significant predictors of the CCS among health education specialists (i.e. health educators and health promoters) (see Table 5).
Correlation between cultural intelligence, its dimensions, and cultural competence skills and the mean scores of the variables.
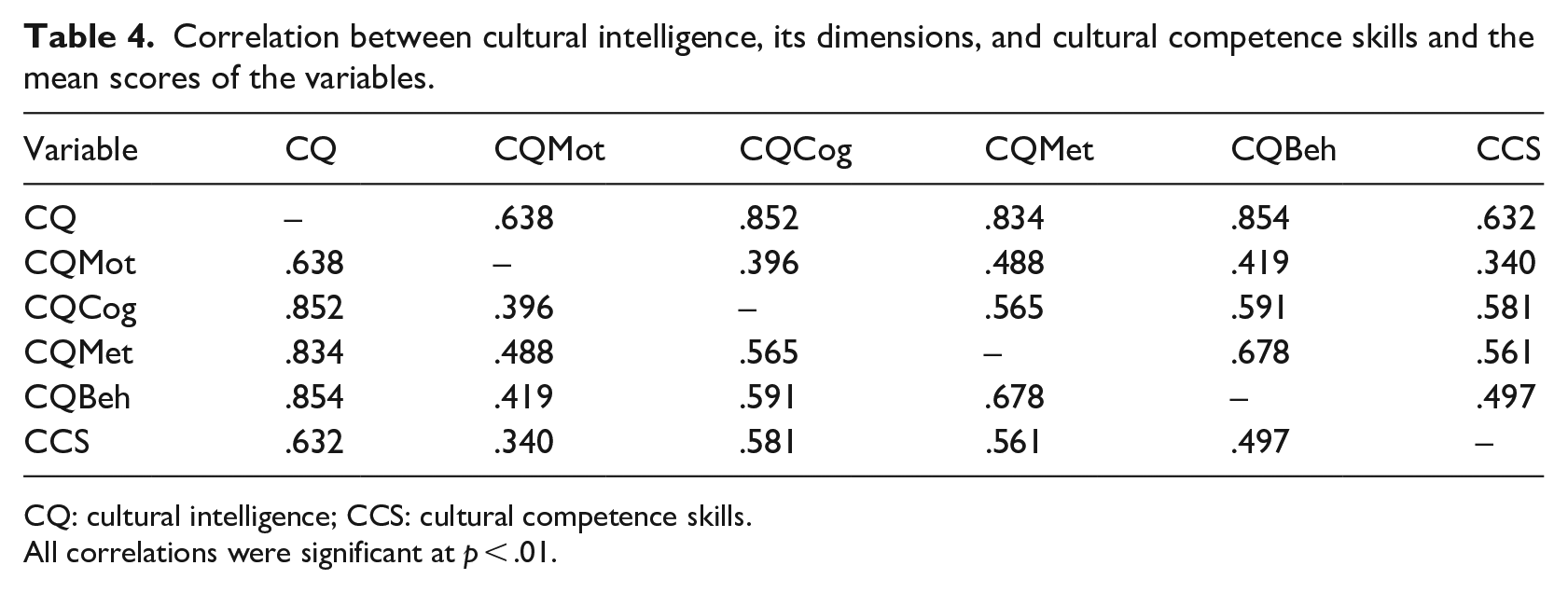
CQ: cultural intelligence; CCS: cultural competence skills.
All correlations were significant at p < .01.
Simultaneous regression model for cultural intelligence on health education specialists’ cultural competence skills.
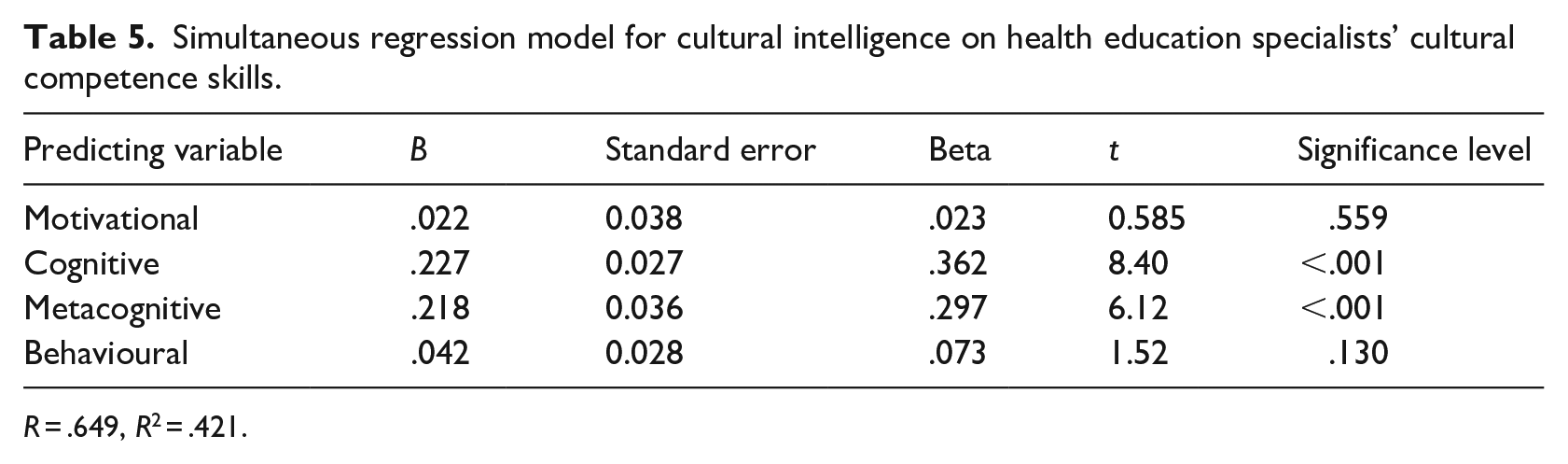
R = .649, R2 = .421.
Discussion
This study is one of the first attempts to assess CQ and its association with CCS among health education specialists in the USA. Findings from the study suggest that health education specialists had a higher-than-average CQ score (i.e. 3.5) on the 1- to 7-point scale and that there was a strong relationship between CQ and CCS among health education specialists who participated in this study. This finding aligns with those in Rahimaghaee and Mozdbar’s (2017) study, which found a relationship between CQ and nurses’ professional competency. However, in contrast to our study, their work engaged with professional competency as a whole and not cultural competency skills specifically.
The results show that CQ cognitive and metacognitive capabilities were significant predictors of CCS. Thus, individuals who increase their CQ cognitive and metacognitive capabilities may also increase their CCS. This finding was somewhat similar to a previous study in which the authors found that the metacognition dimension of CQ was the most powerful predictor of professional competency (Rahimaghaee and Mozdbar, 2017).
Findings from this study suggest that a relationship exists between CQ and CCS. Future research should examine their effects on the quality of the health education programmes provided to diverse populations. Moreover, the findings revealed that both cognitive and metacognitive dimensions are important predictors of CC skills; hence, health education specialists should continue to develop their understanding of cultural systems, values and differences, alongside the capacity to anticipate cultural dynamics and respond accordingly so as to increase their CCS when working with diverse groups.
Findings from this study also suggest that levels of CQ and CCS vary among individuals from different racial/ethnic backgrounds. Future research should further explore the effect of race and/or ethnicity on levels of CQ and CCS. In addition, because higher education and working with diverse populations were related to higher levels of both CQ and CCS, future research should also further explore the relationship between these variables on levels of CQ and CCS.
Findings from this study suggest that the incorporation of CQ into the health education and health promotion field may be helpful in increasing professional competency and more specifically cultural competency when engaging with diverse cultural groups and working in cross-cultural settings. Since public health education degree preparation programmes (i.e. colleges, universities) have incorporated the concepts of cultural competence in the curriculum to prepare future public health practitioners, these programmes should also consider integrating concepts of CQ to help future health education specialists and other health education professionals develop CQ knowledge, CQ strategy, CQ drive and CQ action (Luquis, 2021; Luquis et al., 2022).
Limitations
Several limitations should be considered in interpreting the findings from this study. First, the overall response rate of less than 10% limits generalisation. It also raises the question of possible differences between respondents and non-respondents. Second, although our study had a high completion rate among responders, it is possible that those who did not complete the full survey became discouraged by the number of items in the CQ scale and/or the CCS as well as the relevance of the CQ statements to their current work as health education specialists.
Furthermore, the exploratory nature of the study prevented a detailed exploration of the relationships between variables. Finally, while the research teams sent multiple reminders to complete the survey and offered the opportunity to enter a draw as an incentive to increase participation, future studies should explore other strategies to increase return and completion rates among health education specialists. The above limitations notwithstanding, findings from the study suggest the need to regularly monitor CQ among health education specialists as they continue to develop their professional competency, especially cultural competency.