
Abstract
Objective:
Studies have shown that school leaders’ health literacy is key to supporting health development in school. During the COVID-19 pandemic, the importance of school leaders’ health literacy became evident, as school leadership was characterised with uncertainty and demanded high levels of alertness to the need to implement rapidly changing health-related measures at short notice. This study sought to explore school leaders’ health literacy, mental health and work-related characteristics in Danish public primary and lower secondary schools during the pandemic.
Methods:
Selecting schools from the national Danish register of institutions a sample of 220 complete responses was achieved in a cross-sectional survey. School leaders or a member of the school management team completed a self-administered version of the COVID-HL: School Principals Survey, which assessed health literacy, three domains of mental health, sense of coherence and workload. Data were analysed using chi-square tests and logistic regression.
Results:
The majority of school leaders (71.4%) demonstrated a sufficient level of health literacy. However, there was a significant difference in workload increase between those with sufficient (66.0%) and insufficient (81.6%) health literacy. A high general workload was associated with lower well-being, while an increase in workload during the COVID-19 pandemic was linked to psychosomatic complaints. Sense of coherence explained variations in well-being, emotional exhaustion and psychosomatic complaints.
Conclusion:
This study highlights the importance of enhancing the health literacy of Danish school leaders, enabling them to deal effectively with complex health-related information and make informed decisions during health crises. Strengthening health literacy is crucial to promoting overall health and well-being in schools under normal circumstances, as well as navigating health crises.
Introduction
Following the initial outbreak in December 2019, the global COVID-19 pandemic disrupted the regular functioning of schools, affecting around 1.5 billion students globally (UNESCO, 2023). In addition to its enormous impact on countries, communities and individuals worldwide, the pandemic took its toll on children and young people’s well-being, mental health and learning. It also posed challenges for teachers and school staff, in terms of both their own well-being and supporting their students (Lee, 2020; Marmot et al., 2021; O’Toole and Simovska, 2022).
Being a school leader in these unprecedented times was a highly demanding position loaded with uncertainty, an increased sense of responsibility and high levels of alertness to the need to implement ever-changing preventive measures at short notice (Duong et al., 2022; Leksy et al., 2023). While the well-being and mental health of students and teachers is a topic that has received much attention in policy and research, both before and during the pandemic, the well-being and mental health of school leaders seem to have been overlooked (Dadaczynski et al., 2022). This is alarming for several reasons. School leaders are responsible for general school governance and the organisation, implementation and sustainability of school-based disease prevention and health promotion efforts (e.g. Adams et al., 2023; Simovska and Prøsch, 2016). The limited research on the topic has shown that school leaders experience work-related stress and mental health problems more frequently compared to occupational reference groups or even the general population norm group (Dadaczynski et al., 2020, 2022; Hasselhorn and Nübling, 2004; Phillips et al., 2008). The COVID-19 pandemic likely exacerbated these trends by increasing the responsibilities related to school-based prevention of disease in the context of challenging societal conditions, high health risks and insufficient evidence about how the virus spread and the consequences of COVID-19 for different age groups in school communities.
The health risks of the pandemic were accelerated by an information epidemic, also known as an ‘infodemic’. An infodemic may be defined as a vast overflow of information within digital and physical environments, including false, misleading and unreliable messages that can induce fear, confusion and mistrust in public health authority among citizens, including children and young people (Eysenbach, 2020). This infodemic highlighted the need for schools to engage in the development of health literacy – that is, the ability to identify, obtain, critically assess and utilise information to make health-related decisions (Okan et al., 2020b, 2021). Again, school leaders carry the primary responsibility for creating organisational conditions that fostered the development of health literacy among teachers and other school staff, and for the school’s efforts to integrate health literacy as an educational goal (Carlsson, 2022; Okan et al., 2020a).
School leaders’ health literacy is critical to support health (literacy) development in schools (Adams et al. 2023). Research from Germany has identified a significant association between health literacy and implementation levels for the Health Promoting Schools initiative, even after controlling for sociodemographic and work characteristics (Dadaczynski et al., 2020). However, only a few studies have investigated the health literacy levels of school leaders and their association with various health indicators. In a cross-sectional survey, Lau et al. (2022) identified low COVID-19-related health literacy among 54% of school leaders from Hong Kong. Moreover, leaders with low health literacy also showed higher levels of work-related exhaustion and psychosomatic complaints. Before the COVID-19 pandemic, almost 30% of German school leaders who participated in an online survey were found to have limited health literacy, with a higher proportion among male leaders (Dadaczynski et al., 2022). Taking gender, age and type of school into account, limited health literacy was associated with a 1.9- to 2.4-fold increased risk for low well-being, as well as frequent emotional exhaustion and psychosomatic complaints.
Although the educational system in Denmark is highly decentralised and schools are governed on a local-municipal level, the latest system-wide educational reform (Danish Ministry of Education, 2013) has allocated even greater responsibility to school leaders than previously in terms of the implementation of the reform’s measures focused on improving academic outcomes and students’ well-being. School leaders are expected to assume the dual task of educational leadership – working with school development and supportive pedagogies – and strategic leadership – performing quality assurance and measuring and monitoring achievement and well-being against outcome goals set externally at the national or municipal level. Sometimes, there is tension between these tasks (Carlsson, 2022), intensifying the job’s demands, workload and, presumably, the risk of work-related stress and poor mental health among school leaders.
This exploratory study sought to investigate school leaders’ health literacy, mental health and work-related characteristics in Danish folkeskoler (public primary and lower secondary education for students aged 6–16). Sense of coherence (SOC) focuses on understanding factors that promote health and well-being. SOC is a theoretical framework that reflects an individual’s general orientation towards life and their ability to cope with stressors and maintain good mental and physical health (Antonovsky, 1979). We set out to address the following research questions:
What is the status of, and the association between, health literacy and mental health among school leaders in Danish schools?
Can differences in school leaders’ health literacy and mental health be identified based on sociodemographic and work-related characteristics, including sense of coherence?
Methods
Study design, population and ethics
As part of the international COVID-HL research network, we carried out a cross-sectional survey study in public primary and lower secondary schools in Denmark between December 2021 and February 2022. The school’s leader or another member of the school leadership (e.g. deputy leaders or members of the school management team) participated in the study. A complete list of all public schools was drawn from the public register of schools in the autumn of 2021 to create a stratified sample. The 1,109 registered schools were first stratified into the five Danish regions. Within each region, schools were sorted by their size in terms of number of students. For every three schools, one school was drawn randomly to the sample, with the two other schools drawn randomly as a first or second replacement school in case the management at the sample school did not wish to participate. To avoid sample size loss, a replacement school from the same stratum and of similar size was selected a priori. Thus, the study aimed at a final sample of 372 school leaders.
The survey was administered online using the survey platform SurveyXact (www.surveyxact.com), which complies with the Danish implementation of the European Data Protection Act concerning the collection and storing of sensitive personal data. The study was registered with the Institutional Review Board at Aarhus University. From this online platform, invitation letters were sent to the email addresses in the register’s entry for each school in the sample, providing information on the study’s objectives, rationale and background, as well as outlining the data management and data protection plan and underlining the voluntary nature of participation. The email requested that either the school leader or a deputy leader participate in the survey. The letter also stated that the Danish Association of School Leaders had endorsed the project. Within 1–2 weeks after the initial invitation, a reminder was sent out if the school had not completed the survey. After an additional 1–2 weeks, a similar invitation letter was sent to the first replacement school following the same procedure if the sampled school had not completed the survey, continuing with the second replacement school if the first replacement did not respond. To increase the survey response rate, a student assistant telephoned schools from the list of second replacement schools that had not completed the survey. This led to 220 complete responses within the sample of 372 schools, using both first and second replacement schools where relevant. The achieved sample displayed a minor underrepresentation of schools in the northern region of Denmark, which is the smallest of the five regions. Descriptive statistics for the completed sample are provided in Table 1.
Sample characteristics – absolute and relative frequencies (n = 220).
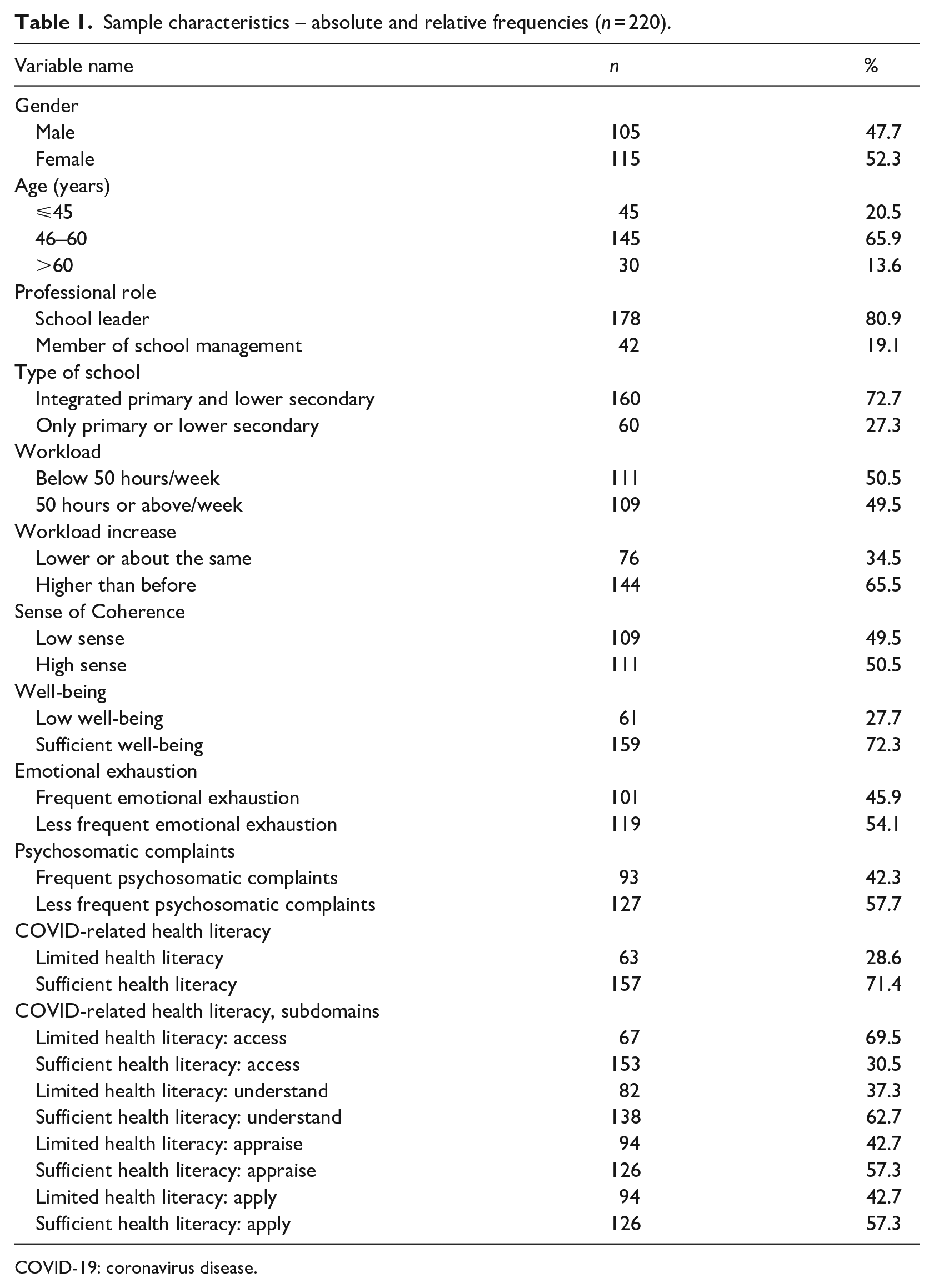
COVID-19: coronavirus disease.
Variables and instruments
The survey consisted of the Danish translation of the COVID-HL: School Principals Survey, with responses analysed according to the guidelines provided in the survey documentation (Dadaczynski et al., 2021).
Participants were asked to indicate their gender (male, female, other 1 ), age (⩽45 years, 46–60 years, >60 years) and professional role at the school (school leader or member of the management team).
The type of school was categorised as lower primary school (grades 0–3), primary school (grades 0–6), fully integrated (grades 0–9), primary and lower secondary (grades 4–9) or lower secondary (grades 7–9). These types were coded into a dichotomous variable indicating either all grades (integrated primary and lower secondary, the most common type of school in Denmark) or only some grades (only primary or lower secondary).
The school leaders’ workload was measured using two questions about weekly working hours. The first question asked, ‘How many hours do you currently work on average per week?’ with an option of selecting several hours. Although the official working week for public employees in Denmark is 37 hours, the answers were divided into leaders working below 50 hours a week and leaders working 50 hours or more a week, as 50 hours was just above the mean in the sample (49.3 hours) and Danish school leaders in general work more hours than an ordinary working week. The second question asked leaders whether their current weekly work hours were ‘lower’, ‘about the same’ or ‘higher’ than before the COVID-19 pandemic. This variable was coded into leaders working ‘lower or about the same’ as before, or ‘higher than before’.
COVID-related health literacy was measured with 22 statements introduced by ‘. . . how easy would you say it is to . . .’ followed by a statement related to the construct (e.g. ‘. . . find information about coronavirus on the Internet?’, ‘. . . to behave in a way to avoid infecting others?’) on a 4-point Likert-type scale (4 = very easy; 1 = very difficult). The scale showed good internal consistency (α = .96). Based on the scale, respondents were scored as having ‘insufficient health literacy’ (mean score < 3) or ‘sufficient health literacy’ (mean score ⩾ 3) by the general use of the scale (Lau et al., 2022; Okan et al., 2020a). The health literacy scale was further divided into four subdomains: access (six items, α = .85), understand (six items, α = .91), appraise (five items, α = .83) and apply (five items, α = .89), all showing high internal consistency reaching at least the same levels of Cronbach’s α as prescribed in the documentation for the scale (Dadaczynski et al., 2021; Okan et al., 2020a). Both the main scale and the subscales were dichotomised into ‘insufficient health literacy’ and ‘sufficient health literacy’ based on a cut-off score (<3 or ⩾3) following the general use of the scale in the literature (Okan et al., 2020a).
To measure psychological well-being, the WHO-5 scale was used (Bech, 2004). The scale consists of five positively worded items asking respondents about their well-being in the last 2 weeks (e.g. ‘Over the last two weeks . . . I woke up feeling fresh and rested’), scored from 0 points (‘At no time’) to 5 points (‘All of the time’). The scale is constructed by adding raw score points multiplied by four to create a scale ranging from 0 to 100. It has been suggested that a score of 50 or below indicates low well-being (Topp et al., 2015). Thus, the scale was accordingly divided into ‘low well-being’ and ‘sufficient well-being’, thereby not differentiating between different levels of low well-being. Internal consistency for the scale was similar to that reported in previous studies (α = .90).
Psychosomatic complaints were measured with the Burnout Assessment Tool (BAT) (Schaufeli et al., 2019, 2020), asking respondents, ‘How often do you suffer from the following complaints?’ and including five items, for example, ‘I suffer from headaches’, with five response options ranging from ‘Never’ (1) to ‘Always’ (5). A scale was created as sums of the five items with sufficient internal consistency (Cronbach’s α of .76). The scale was split in half by the median, with scores up to and including the median scored as ‘less frequent’ and scores above the median scored as ‘frequent’.
Exhaustion was measured using three statements from the BAT (Schaufeli et al., 2019, 2020). Respondents were asked on a scale from ‘never’ (1) to ‘always’ (5) to indicate how often the three statements (e.g. ‘At work, I feel mentally exhausted’) applied to them. Internal consistency for the scale was good (α = .85). A scale was created as the sums of scores and dichotomised into ‘frequent’ and ‘less frequent’ emotional exhaustion, divided by the median, which was included in the ‘less frequent’ group.
SOC was included as a measure of school leaders’ experience of their current work situation, asking participants to semantically differentiate between nine pairs of words concerning their current work situation (e.g. ‘manageable – unmanageable’) on a 7-point scale, where six of the items were inverted (Vogt et al., 2013). The scale provided a good level of internal consistency (α = .85). It was split into two groups labelled ‘low sense of coherence’ and ‘high sense of coherence’, including the median in the high sense group.
Data analyses
The first part of the analysis compared the COVID-19-related health literacy and mental health of school leaders using chi-square tests (χ2) to test for differences in statistical associations between the two levels of health literacy and school leaders’ mental health (Tables 3 and 4), as well as demographic characteristics (Table 2). Logistic regression was used to scrutinise the relationship between health literacy and demographic variables on the one side and school leaders’ mental health (outcome) on the other side with separate models for each mental health indicator (psychological well-being, psychosomatic complaints and exhaustion, Table 5). A 95% significance level was used in all analyses. All analyses were performed using the open-source statistical software R (R Core Team, 2023) within an RStudio environment (RStudio Team, 2015).
Health literacy levels of school leaders and the relation to sociodemographic factors, workload and sense of coherence (n = 220).
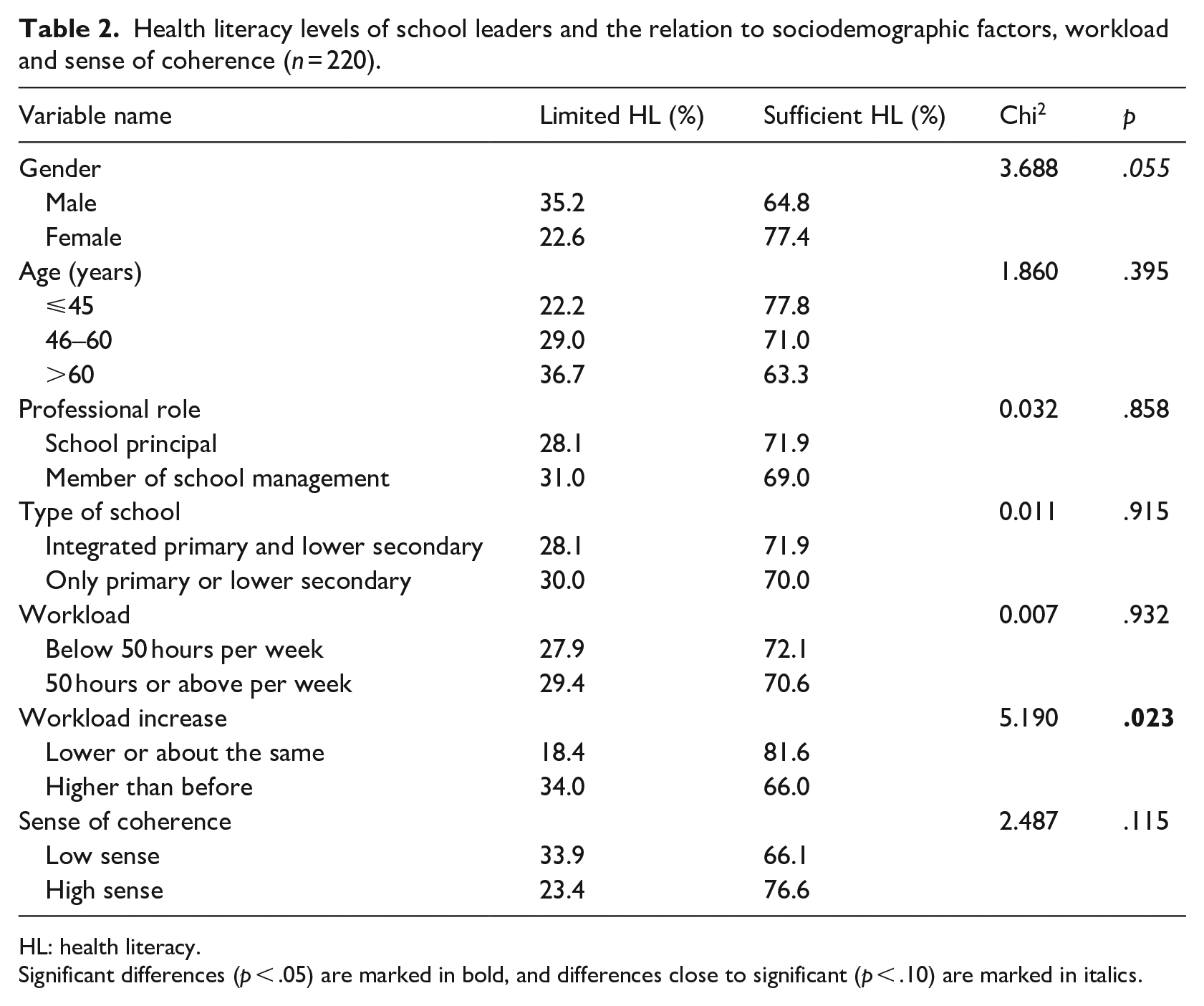
HL: health literacy.
Significant differences (p < .05) are marked in bold, and differences close to significant (p < .10) are marked in italics.
Results
Our sample (see Table 1) consisted of 52.3% female and 47.7% male leaders, with the majority being aged 46–60 (65.9%). Most of the responses to the survey (80.9%) were given by the school leader, with the remaining 19.1% being given by a management team member. Most responses (72.7%) were from integrated primary and lower secondary school leaders (grades 0–9).
As shown in the table, 49.5% of the responding school leaders worked 50 hours or more weekly, and 65.5% stated that the workload had increased during the COVID-19 pandemic. Given that the typical working week in Denmark is 37 hours, the findings show that the school leaders generally worked significantly more extended hours and that COVID-19 worsened the situation. Just 3 of the respondents reported that they worked 37 hours or less weekly, and only 13 respondents reported working 40 hours or less weekly.
Table 2 shows that the majority of the school leaders (71.4%) demonstrated a sufficient level of COVID health literacy, with female leaders showing slightly (but not statistically significant) higher levels of health literacy. There were no significant differences in health literacy by the type of school or professional role. There was, however, a significant difference related to the perceived workload increase during the COVID-19 pandemic. School leaders who reported an increased workload during the COVID-19 pandemic was likelier to show lower levels of COVID-19-related health literacy compared to school leaders who reported the same or no increase in the workload (Chi2 = 5.19; p = .023). Meanwhile, there was no correlation between health literacy and general workload.
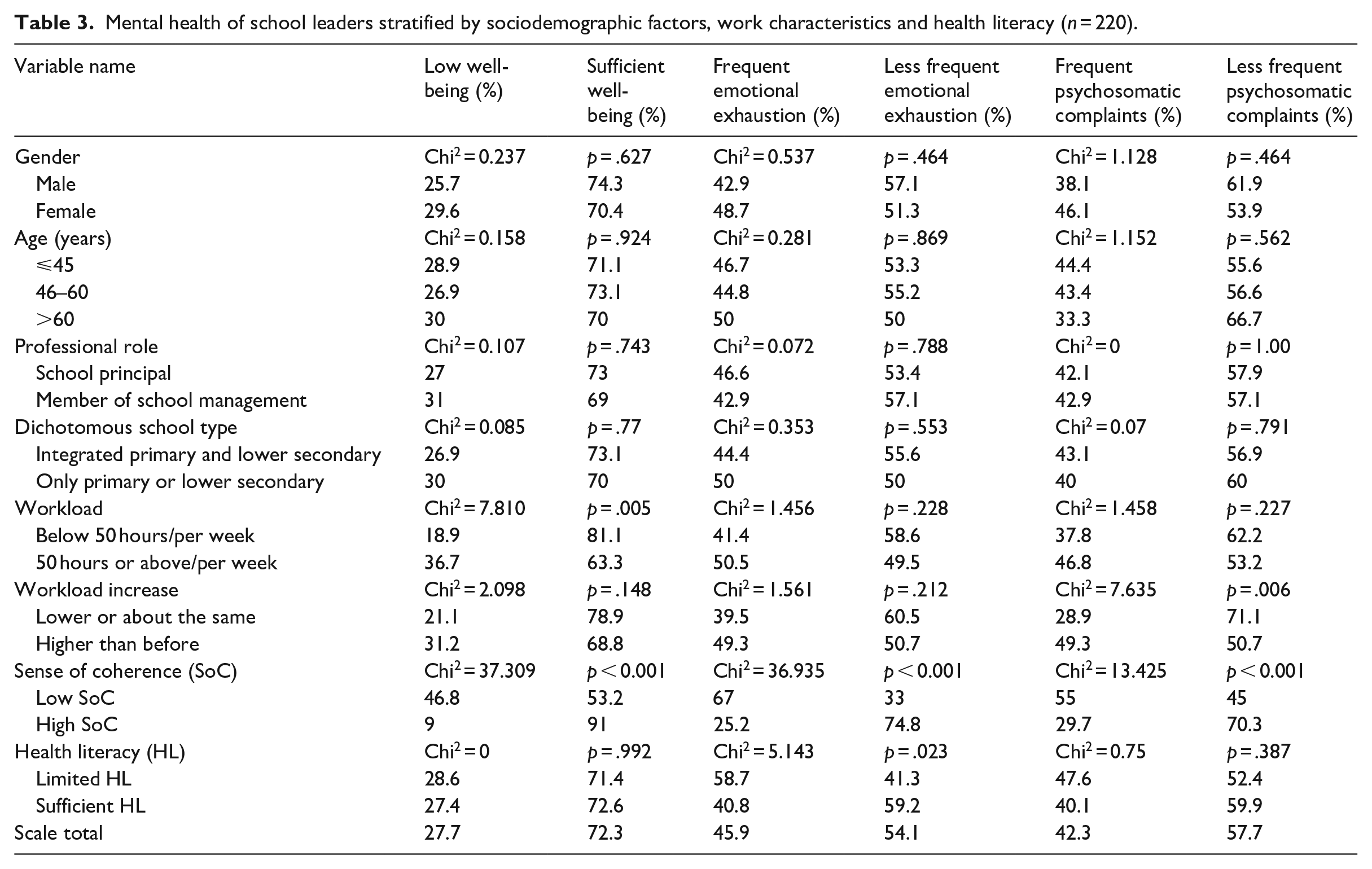
Table 3 provides an overview of the school leaders’ mental well-being. Although most respondents (72.3%) reported sufficient well-being, almost one-fourth of the leaders reported low well-being. A heavy workload of 50 or more hours weekly was significantly associated with lower mental well-being (Chi2 = 7.810; p = .005), and an increase in workload was significantly associated with frequent psychosomatic complaints (Chi2 = 7.635; p = .006). Limited health literacy was significantly associated with frequent emotional exhaustion (Chi2 = 5.143; p = .023), and low SOC was significantly associated with all the domains of mental well-being – low well-being (Chi2 = 37.309; p < .001), frequent emotional exhaustion (Chi2 = 36.935; p < .001) and psychosomatic complaints (Chi2 = 13.425; p < .001).
Mental health of school leaders stratified by sociodemographic factors, work characteristics and health literacy (n = 220).
Looking at different aspects of the mental health of school leaders (Table 4) in relation to the four measured subdomains within health literacy (ability to access, understand, appraise and apply information relevant to health and well-being), the results showed that the subdomain access was the only one not linked significantly to any of the mental health domains. Limited ability to apply health-related information was significantly related to frequent psychosomatic complaints (Chi2 = 4.588; p < 0.032). The trend was the same for the other aspects of well-being, although the associations did not amount to statistical significance. The domains of understanding (Chi2 = 7.603; p < 0.006) and appraising (Chi2 = 4.036; p < 0.045) were significantly related to emotional exhaustion, and a similar trend, although not statistically significant, was evident for psychosomatic complaints.
Mental health of school leaders stratified by subscales for health literacy (n = 220).
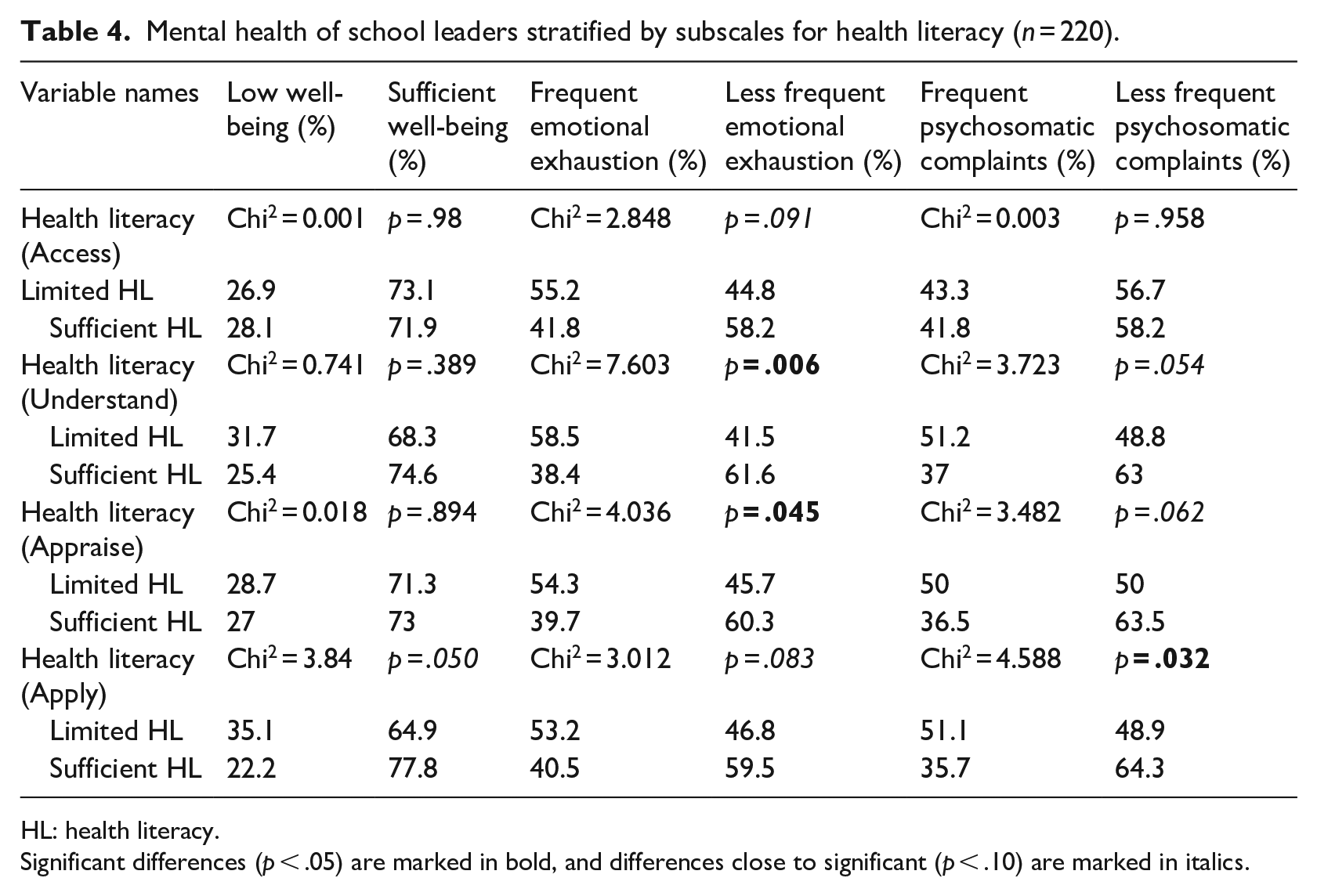
HL: health literacy.
Significant differences (p < .05) are marked in bold, and differences close to significant (p < .10) are marked in italics.
The findings presented in Table 5, showing multiple binary logistic regression analyses, confirmed the robustness of the previous results. The relation between health literacy and emotional exhaustion remained when controlling for SOC, workload and other background characteristics.
Multiple binary logistic regression analyses for the mental health of school leaders.
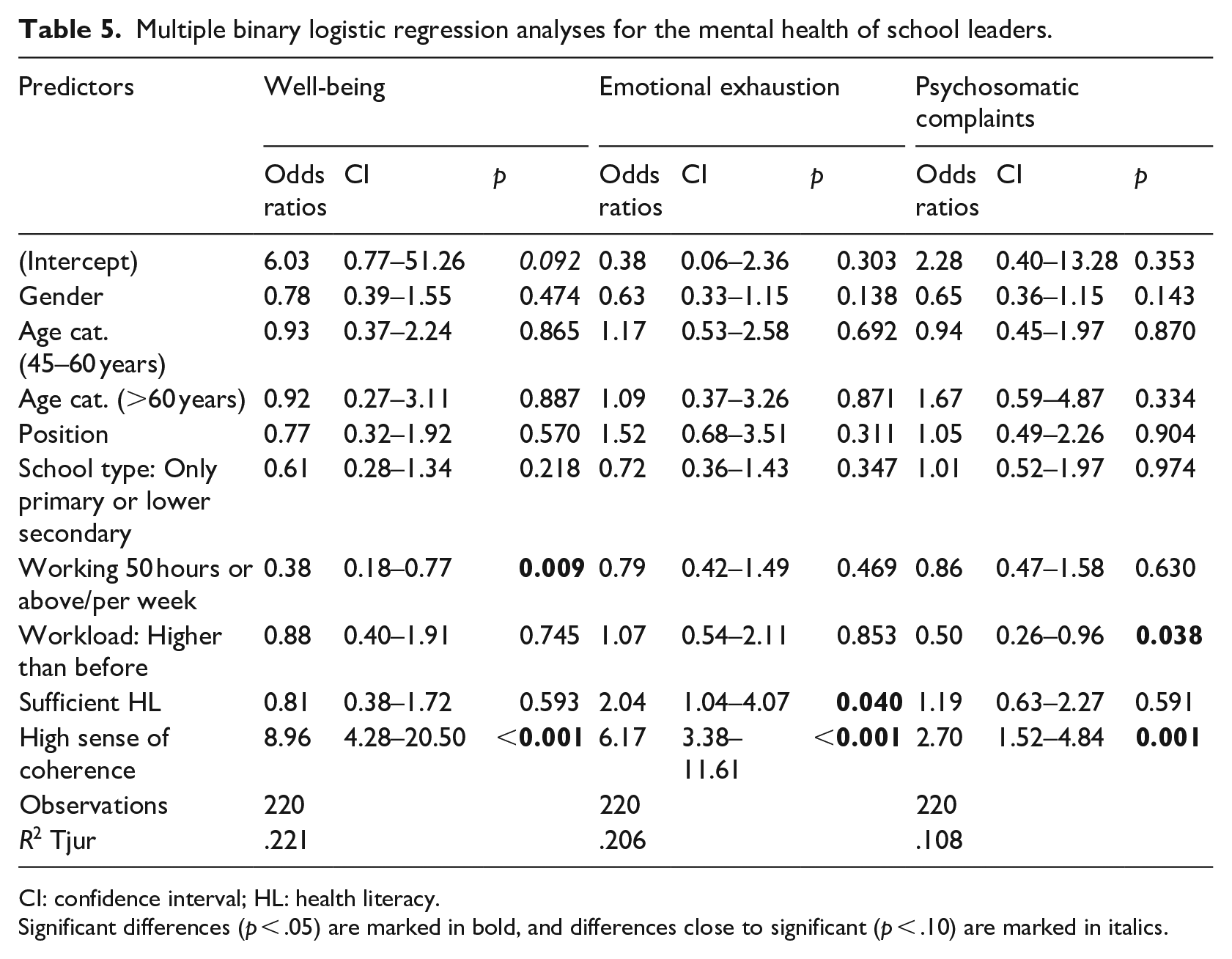
CI: confidence interval; HL: health literacy.
Significant differences (p < .05) are marked in bold, and differences close to significant (p < .10) are marked in italics.
Working hours predicted differences in well-being when controlling for health literacy and SOC. A perceived increase in workload explained the differences in psychosomatic complaints when controlling for workload, health literacy and SOC. SOC explained the difference in all three aspects measured – well-being, emotional exhaustion and psychosomatic complaints.
Discussion
The COVID-19 pandemic can be seen as an unprecedented crisis that put schools under intense pressure, especially school leaders, who have primary responsibility for the conduct and performance of these organisations. This is supported by research highlighting the impact of such demanding and complex conditions on the workload of school leaders, with limited support or resources to help them cope (e.g. Harris and Jones, 2020). In a recent systematic literature review, Chatzipanagiotou and Katsarou (2023) identified three key types of challenge for school leaders that became evident during the pandemic: (1) logistic challenges posed by the lack of infrastructure, resources and efficient planning in schools; (2) academic challenges (e.g. a transition to remote learning, guidance in online teaching practice); and (3) organisational challenges (e.g. ensuring a positive school climate, as well as physical and psychological well-being).
Although an emerging research base has suggested that work-related stress and mental health problems are widespread among school leaders, this occupational group is often overlooked in school health research and practice, which is also the case for research related to COVID-19. Similarly, health literacy, which has become the focus of public health research, policy and practice, has slowly found its way into the school setting in recent years. The fact that little is currently known about school leaders’ health literacy is remarkable, given that, during the COVID-19 pandemic, school leaders had to deal with large amounts of health-related information and make day-to-day decisions based on that information. Health literacy requires the ability to obtain, understand, critically assess and apply health-related information, on the one hand, for the development of health-promoting schools, also in times of crisis, and, on the other hand, as a resource for the leaders’ health and well-being (Dadaczynski et al., 2020; Glenn and Glenn, 2020).
School leaders are essential contributors to school-based health promotion and the development of organisational health literacy in schools (Adams et al., 2023; Kirchhoff et al., 2022). Usually, health literacy is approached from an individual perspective, aimed at promoting competencies, influencing attitudes and forming healthier behaviour. However, health literacy is a relational and contextual concept in which personal attributes must reflect the specific environment’s complexities and demands (Parker and Ratzan, 2010). This is where organisational health literacy in schools makes a difference, using institutional processes at the whole-school level to initiate social change within the school (Kirchhoff et al., 2022; Okan et al., 2021). School leaders are the central figures in creating such change in the school setting, which makes them indispensable in initiating and facilitating the development of organisational health literacy. To be able to lead this development, school leaders need a certain level of individual health literacy themselves.
This study showed that approximately 29% of the participating school leaders had limited COVID-19-related health literacy, which is lower than found in a survey from Hong Kong (Lau et al., 2022) but in line with the results reported in a German study conducted before the pandemic, concerning general health literacy among school leaders (Dadaczynski et al., 2022).
Stratified by sociodemographic and work characteristics, no differences in health literacy were identified according to gender, age, type of school or professional role. Given the scarcity of research in the field, the comparability of the findings is limited. Gender differences have only been reported in a few studies, with male educators more frequently reporting difficulties in acquiring and dealing with health information (Ahmadi and Montazeri, 2019; Dadaczynski et al., 2020). The results of this study point in a similar direction, with male respondents pointing to their limited health literacy about 12% more frequently than female respondents, although the effect size is not significant compared to previous studies. It has been argued in the literature that females make more use of health services, resulting in them being more experienced and better at handling health-related information (Owens, 2008) and having a more robust social motive for seeking health-related information (Bidmon and Terlutter, 2015).
Interestingly, the results of this study showed that health literacy was associated with an increase in perceived workload during the COVID-19 pandemic; that is, respondents with limited health literacy were significantly more likely to report a higher workload than before the pandemic. In interpreting this result, we argue that a limited ability to find and use health information could also be associated with work behaviours that can negatively affect one’s well-being, such as challenges in maintaining a healthy work–life balance. Evidence for this argument can be found in the study by Lau et al. (2022), where work intensification was associated with COVID-19-related health literacy in multiple linear regression analyses. Overall, these findings suggest that health literacy is more than a means to effectively implement measures of school health promotion and thereby improve student health outcomes and well-being. Health literacy can also be considered an asset for the health and well-being of school leaders and a resource for coping with work-related demands, mitigating stress, avoiding an unnecessarily heavy workload and protecting their health in general, including mental health and well-being.
Concerning mental health indicators, no sociodemographic differences were found in bivariate analyses. However, a heavy weekly workload (⩾50 hours) was associated with a higher frequency of low well-being. An association was found between an increased workload compared to before the pandemic and frequent psychosomatic complaints.
Concerning COVID-19-related health literacy, our findings highlighted that, in addition to the global score, it is essential to consider the sub-dimensions of health literacy. While respondents with limited overall health literacy were more likely to experience frequent emotional exhaustion, stratified analyses revealed a more nuanced picture. More frequent emotional exhaustion was associated with a limited ability to understand and critically evaluate health information. By contrast, a low ability to apply health information was more often found among respondents with low well-being (albeit the difference was not significant) and with frequent psychosomatic complaints. These results are of great importance since, with a few exceptions (Dadaczynski et al., 2022; Zhang et al., 2021), the relationship between the different sub-dimensions of health literacy and their health significance has received little attention from previous research. Simply providing school leadership with access to health-related information is insufficient, which highlights the need to develop professional development programmes aimed at the development of health literacy of school leaders and members of the school leadership.
Limitations
Although our sampling strategy aimed at reaching a representative cross-sectional sample of Danish school leaders, the survey response rate leaves room for selection bias. In combination with the cross-sectional nature of the study, this calls for caution when interpreting the results. The small sample size requires relatively large effects before the analyses show significant correlations. Given the sample size of 220 and with a normally assumed power of 0.80 and the used 95% significance level, an effect needs to be of the size w = 0.19 to be detectable in the cross-tabulations in Table 2 (Cohen, 1988). Furthermore, no Danish validations exist for the instruments used, so we used the general norms. Comparisons with other studies should therefore be carried out with caution, as translations of the scales might have influenced response patterns. However, the psychometric properties of the different measures seem to correspond well with the original measures, so there is no indication that the scales should not be expected to measure the same constructs in Denmark.
Conclusion
This is the first study in Denmark on school leaders’ health literacy and its associations with mental health and work-related stress, and other work characteristics. The findings indicate that there is a need to strengthen the health literacy of Danish school leaders if they are to be able to deal with complex health-related information and make decisions affecting the development and functioning of their schools during health crises, but also in terms of regular practices promoting health and well-being at the school. In this respect, health literacy has two functions: the first includes school leaders’ personal health literacy and how it enables them to manage complex health information better and integrate it into their leadership practices. The second shifts the perspective to understand school leaders’ health literacy as part of the school’s organisational health literacy. It concerns the ways in which that can help to promote the health and health literacy of students and teachers within the school, contributing to the whole-school approach to the promotion of health and well-being.
School-based health promotion is not new in Denmark – the country has been actively involved in the European Network of Health Promoting Schools since 1992, working with a whole-school approach and the development of health-related action competence, defined as students’ critical ability to take care of their health by addressing the contextual dynamics in school that affect health (Simovska et al., 2015). Although the concepts of action competence and health literacy share some similarities (Simovska and Paakkari, 2014), they are not identical. Health literacy is a relatively new topic in education in Denmark, and there are hardly any school-based health literacy programmes or policies supporting its development at the individual or organisational level. More research is needed, both longitudinal and cross-sectional, both qualitative and quantitative, to understand the complexities and potential causal pathways between school leaders’ workload, health literacy and mental health.
Although causal interpretations are not possible given the cross-sectional design, based on this study and related literature, we argue that research, policy and practice need to pay more attention to health literacy, mental health and work-related stress among school leaders. The development of school leaders’ health literacy can benefit their mental health and capacity to lead schools effectively during a pandemic, as well as in regular health promotion activities in schools.
Supplemental Material
sj-docx-2-hej-10.1177_00178969231211853 – Supplemental material for Relationships between COVID-related health literacy, mental health and workload of school leaders
Supplemental material, sj-docx-2-hej-10.1177_00178969231211853 for Relationships between COVID-related health literacy, mental health and workload of school leaders by Rune Müller Kristensen, Kevin Dadaczynski, Orkan Okan and Venka Simovska in Health Education Journal
Supplemental Material
sj-xlsx-1-hej-10.1177_00178969231211853 – Supplemental material for Relationships between COVID-related health literacy, mental health and workload of school leaders
Supplemental material, sj-xlsx-1-hej-10.1177_00178969231211853 for Relationships between COVID-related health literacy, mental health and workload of school leaders by Rune Müller Kristensen, Kevin Dadaczynski, Orkan Okan and Venka Simovska in Health Education Journal
Footnotes
Funding
The authors would like to thank The National Center for School Research at the Danish School of Education for funding a research assistant to set up the survey and a student assistant to contact schools. The authors received no additional financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.