
Abstract
Objective:
Despite a nationwide ban on tobacco sales to people under 18 years of age, adolescents can still buy tobacco products in Amsterdam. This study aimed to understand the influence of the retail environment in adolescents’ activity spaces on their tobacco-purchasing behaviour.
Method:
Interviews were conducted with 13 adolescents (aged 14–19 years) who went to school in Amsterdam and had ever bought tobacco products. Questions were based on the capability, opportunity, motivation, behaviour (COM-B) model. City maps showing all tobacco outlets were used to visualise respondents’ activity spaces and purchasing areas. Transcripts were analysed thematically.
Results:
Adolescents preferred purchasing tobacco at shops where they had successfully purchased it before, instead of going to just any shop close by. They purchased tobacco products mostly in small shops. Supermarkets were avoided, as employees complied with age-verification procedures. The city centre provided easy access because the density of small shops was high. In adolescents’ residential area, acquaintances behind the counter might facilitate tobacco purchase, while it was a barrier for minors who secretly smoked. At school, adolescents developed a collective knowledge of shops that sold tobacco products to minors either near school or further away. Tobacco was also bought on the black market because it was cheaper or because it was possible to buy specific products (e.g. snus).
Conclusion:
Tobacco purchasing by minors is less about the proximity and more about which stores in their activity spaces sell tobacco products to minors. Policies should therefore be aimed at the enforcement of age limits and reducing the number of small shops selling tobacco.
Introduction
Smoking is a preventable cause of many diseases in almost every organ (National Center for Chronic Disease Prevention and Health Promotion [US] Office on Smoking and Health, 2014). As smoking is most often initiated under the age of 18 years, adolescents are an important target group for smoking prevention (Nuyts et al., 2018). In 2021, 38% of Dutch 16-year-old adolescents have tried smoking, and 25% have tried e-cigarettes (Boer et al., 2022). The percentage of Dutch adolescents who have smoked tobacco products decreased significantly between 1999 and 2017, from 54% to 17%, but it has remained stable since then (Rombouts et al., 2020). This underlines the importance of improving tobacco control policies in order to create a tobacco-free generation (World Health Organization, Regional Office for Europe, 2017). Further restricting adolescents’ access to tobacco and e-cigarettes is a crucial step in reducing smoking initiation (Chen and Forster, 2006).
Despite a nationwide ban on sales of tobacco products and e-cigarettes to people under 18 years of age in the Netherlands, many adolescents know how to access these products (Nuyts et al., 2020a). The effectiveness of this ban has been found to be undermined by various purchasing strategies used by adolescents (DiFranza and Coleman, 2001; Hewer et al., 2021; Leão et al., 2019; Nuyts et al., 2020a; Papanastasiou et al., 2019; Robinson and Amos, 2010). For example, adolescents use tactics to look older to increase their chances of purchasing tobacco products, such as borrowing ID cards or dangling car keys (DiFranza and Coleman, 2001). In the Netherlands, this latter strategy works, as the minimum age to drive a car independently is the same as the minimum age for tobacco sales.
There is some evidence that adolescents’ tobacco-purchasing behaviour may be influenced by aspects of the tobacco retail environment, such as the type of tobacco retail outlets, retailer density and proximity and visibility of tobacco products and advertising in shops (Barnett et al., 2017; Finan et al., 2019; Gwon et al., 2016). In Europe, local shops, gas stations and night shops were mentioned by adolescents as places where they are able to purchase tobacco products as a minor, as they were less likely to comply with the legal minimum age of sale (Hewer et al., 2021; Nuyts et al., 2020a). A higher density of tobacco outlets is associated with a greater risk of smoking (Finan et al., 2019). In the USA, a reduction of tobacco outlet density was associated with lower accessibility and visibility of tobacco products (Luke et al., 2017). A high density may facilitate or stimulate tobacco purchases in three ways. First, it increases the accessibility of tobacco products, as there are more outlets to try and proximity to shops may increase. Second, it increases competition between outlets, which may lead to lower prices or less compliance with the age-of-sale regulations (Luke et al., 2017). Third, exposure to many visible tobacco points of sale may increase adolescents’ awareness of purchasing options and trigger purchasing behaviour (Nonnemaker et al., 2016). In the Netherlands, the regulations for vape products are the same as for tobacco products. The minimum legal sales age is 18 years for both, and the Netherlands has banned all tobacco and vaping advertising and displays in shops (tobacco specialist and vape shops are exempted). Tobacco retail outlets may still be recognised as such by adolescents.
There is limited empirical evidence on how adolescents perceive the tobacco retail environment and how they think that this may influence their tobacco-purchasing behaviour. Previous qualitative studies have shown that adolescents perceive tobacco products to be accessible so long as they are able to buy their products in at least one shop (Hewer et al., 2021; Nuyts et al., 2020a).
This study aimed to understand the influence of the retail environment within adolescents’ activity spaces on their tobacco- and e-cigarette-purchasing behaviour. The objectives of the study were (1) to describe the tobacco- and e-cigarette-purchasing behaviour of underage adolescents in Amsterdam, (2) to understand which types of shops they prefer and why and (3) to understand their motivations for purchasing tobacco and vape products in specific parts of the city. We carried out qualitative interviews with adolescents in Amsterdam. An innovative feature is that we used a map of Amsterdam with tobacco outlets to provide a visual tool for adolescents to explain where they often go to and where they purchase their tobacco and e-cigarette products (Walmsley and Lewis, 2014).
Methods
Study population
In total, nine interviews were conducted including single (N = 5) and paired interviews (N = 8) with 13 Dutch adolescents aged 14 to 19 years. For the 18- and 19-year-olds, information was collected retrospectively, by asking about their behaviour 1 or 2 years previously. With paired interviews, interaction between the two participants may occur, leading to a more complete perspective because they may complement each other, while participants can still individually answer the questions in-depth (Cartwright et al., 2016). This approach was also meant to lower the barrier to participate in an interview, as some adolescents feel more comfortable having a familiar person with them.
Four participants were recruited at a hockey club, nine participants at two youth centre locations and one participant was recruited via personal contacts of the first author (D.A.M.P.). D.A.M.P. visited sports clubs, parks and youth centres to invite participants through direct contact and to carry out the interviews during the same visit in a separate room. The inclusion criteria were checked verbally by the interviewer before the start of the interviews. The inclusion criteria were attending school in Amsterdam and having bought tobacco products, vape products or snus at least once. This did not necessarily mean that they themselves were currently using one of these products. It is illegal to sell those products to adolescents under 18 years of age in the Netherlands.
Ethical considerations
The medical ethics committee of the Academic Medical Centre decided that the Medical Research Involving Human Subjects Act does not apply to this study (W19_305 # 21.076). An information letter and informed consent was read and signed by all participants just before the interview. The informed consent of adolescents younger than 16 years was provided by their parents as well. Data were stored and processed in agreement with the General Data Protection Regulation (European Parliament, 2016). Identification of individual participants with the map was prevented by (1) the use of bigger circles around the home address and (2) not linking home or school location to specific participants or to each other.
Interview guide
The interview guide was informed by the capability, opportunity, motivation and behaviour model. Capability was subdivided into psychological and physical capability. Psychological capability means that adolescents know where and how to purchase tobacco, and physical capability concerns being actually able to purchase tobacco (e.g. being able to travel to a shop, and having the necessary financial means). Motivation includes all cognitive processes with a distinction made between reflective and automatic processes. Reflective motivation refers to rational reactions (making plans) for buying tobacco while automatic motivation includes irrational reactions (impulses). Opportunity includes factors outside the individual. It consists of physical opportunity, which arises from the built tobacco retail environment, including willingness of retailers to sell to minors (Michie et al., 2011).
The interview guide consisted of seven main questions together with follow-up questions. When 18- or 19-year-old participants were interviewed, the questions referred to the situation when they were still a minor. After addressing the questions about their specific tobacco-purchasing behaviour, the geographical opportunities of participants were addressed with a map of Amsterdam with the tobacco outlets indicated. This was used to discuss the specific tobacco outlets in participants’ activity spaces. The printed map was placed on the table between the interviewer and the participant(s). The interviewer asked the participants to identify specific locations on the map. Participants drew their physical activity space (e.g. where they went to school, where they lived and where they spent their spare time) and routes often taken by the participant to buy tobacco. This method made it possible to discuss the geographic aspects of their tobacco-purchasing behaviour in more detail. After that, more questions were asked to also address their capability and motivation towards tobacco purchasing at those locations previously indicated on the map.
Data collection
Interviews took place between 3 and 12 May 2022 in a public location. The interviews were held in Dutch, took between 20 and 45 minutes and were audio recorded. Participants were given the opportunity to ask questions before, during and after the interview and were assured that participation was voluntary and could cease at any time. Audio recordings were transcribed verbatim, but the quotes used in this paper were translated from Dutch to English.
Data analysis
The transcripts were read two or three times to become familiar with the text, before a thematic analysis (Braun and Clarke, 2006). Inductive coding was carried out in MAXQDA, where D.A.M.P. conducted open coding for all the participants individually by adding descriptive labels to text parts (Software, 2016). One transcript was also coded by T.R.D.v.D. to review consistency. Only small differences in coding were found and evaluated via discussion. Revisions in coding were made to all other transcripts. Descriptive codes were clustered together, and main themes were developed. The description of the themes is supported by illustrative quotes. Behind the quotes, the gender (female/male) and age of the participant were reported. We created a map of Amsterdam with the locations of tobacco outlets, schools and the approximate home addresses of the participants.
Results
Sample characteristics
Table 1 presents the demographic characteristics of the study population. Of the 13 adolescents, 3 were female. Figure 1 shows a map of Amsterdam with tobacco outlets and the participants’ school and home locations. One of the 13 participants lived in Diemen, which is an independent municipality in between Amsterdam and Amsterdam South-East. Participants indicated that they spend their free time all over Amsterdam, such as in parks, playgrounds, sports clubs, youth centres, and friends’ houses. The schools they attended were also located in different parts of the city.
Demographic and tobacco-purchase characteristics of the participants.
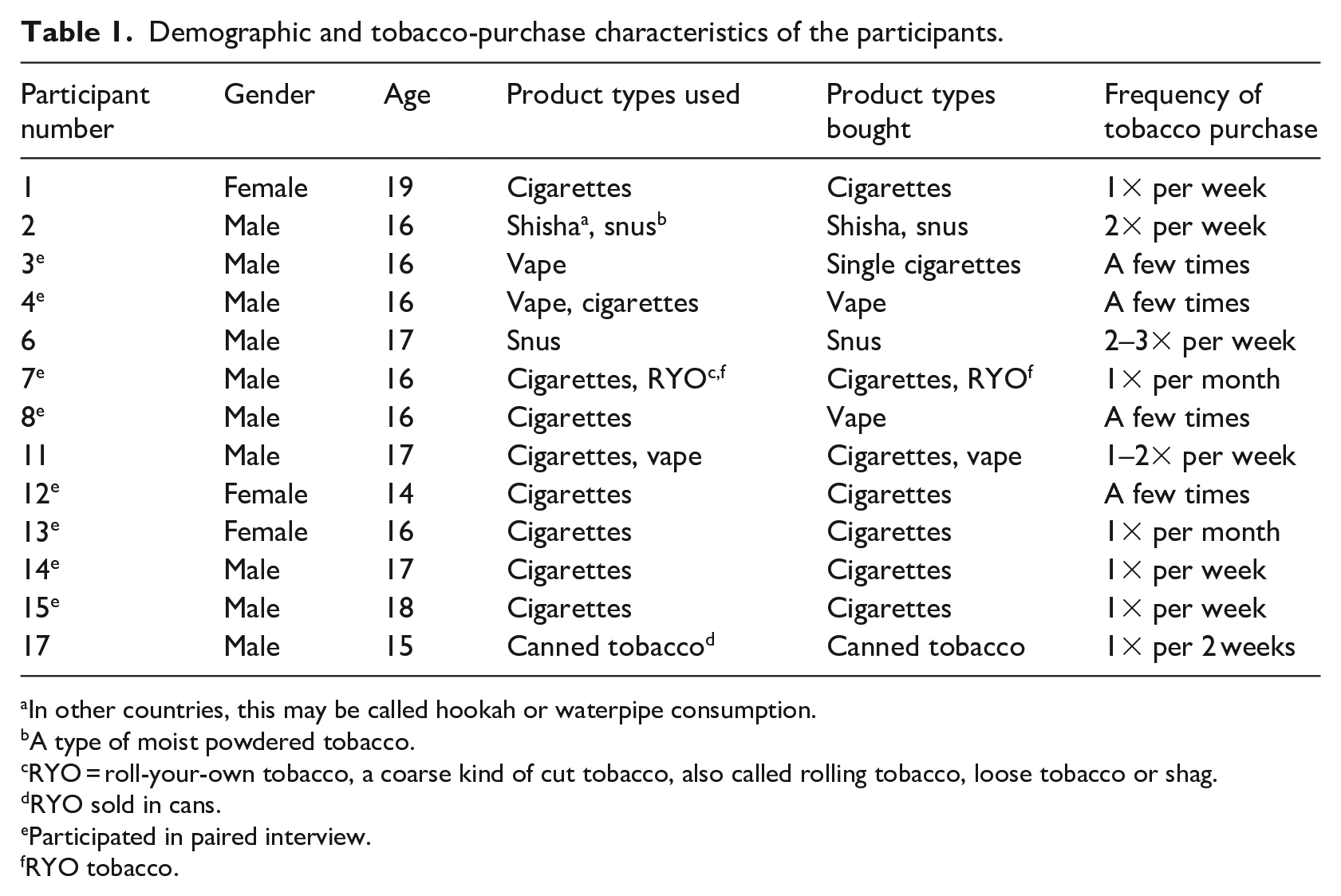
In other countries, this may be called hookah or waterpipe consumption.
A type of moist powdered tobacco.
RYO = roll-your-own tobacco, a coarse kind of cut tobacco, also called rolling tobacco, loose tobacco or shag.
RYO sold in cans.
Participated in paired interview.
RYO tobacco.
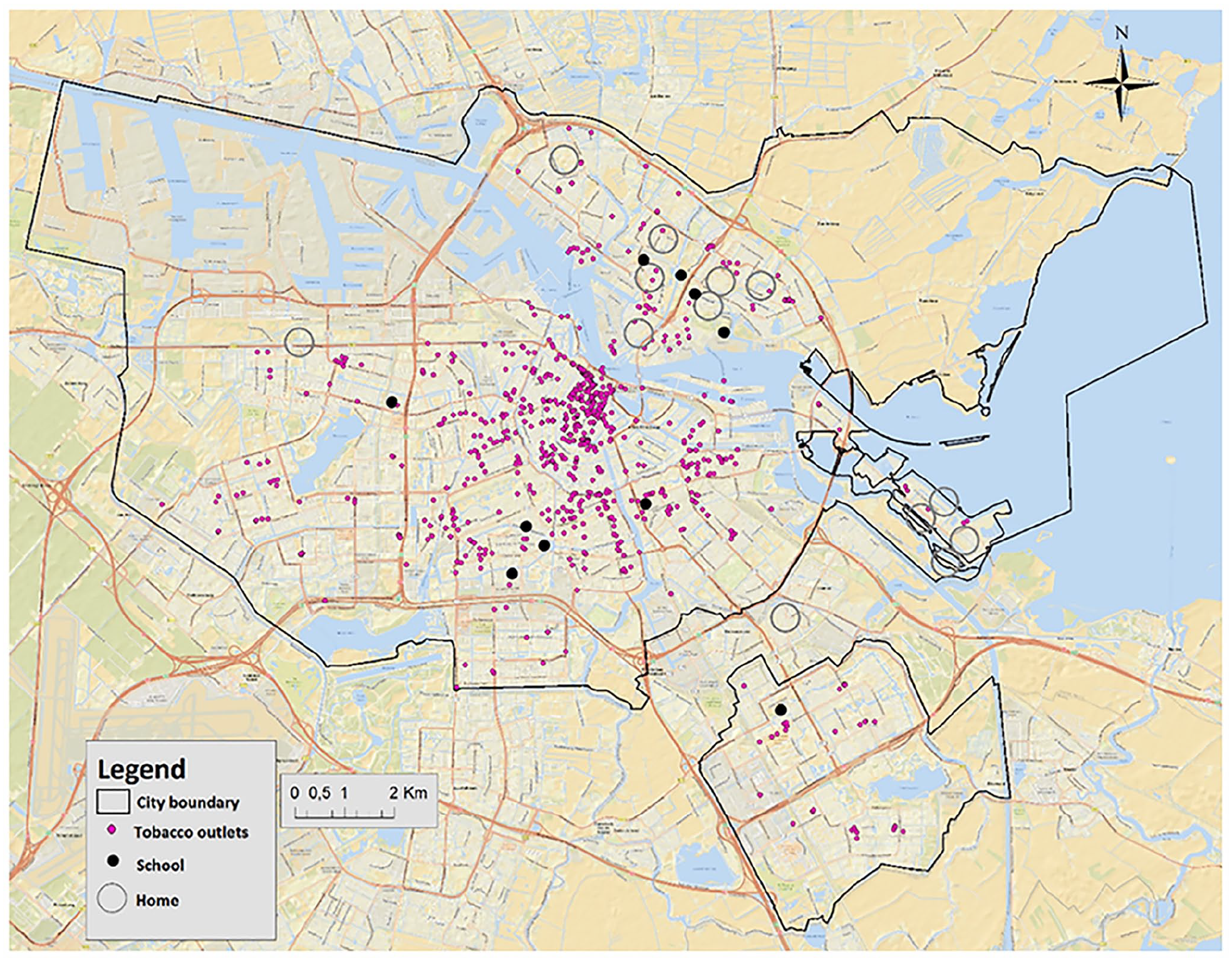
Map of Amsterdam with geographical information of participants.
Tobacco-purchasing behaviour
Table 1 also shows information on the tobacco products participants bought and how frequently they purchased tobacco. In total, nine participants bought tobacco, vapes and/or snus regularly (between once a month and twice or three times a week), and four adolescents had bought tobacco, vapes and/or snus a few times. Some adolescents bought cigarettes together with other friends because they experienced it as a social activity, while others preferred to go on their own because they noticed that they were not asked for ID when they came without friends. Participants bought a diverse spectrum of tobacco products, namely cigarettes, roll-your-own, canned tobacco, shisha, snus and vape products. In the rest of the results, when we refer to ‘tobacco products’, these include all e-cigarettes, vapes and other products mentioned by participants.
From this point forward, the results section describes the analysis of the transcripts and refers with superscripted numbers to quotes listed in Table 2.
Quotes from the participants.
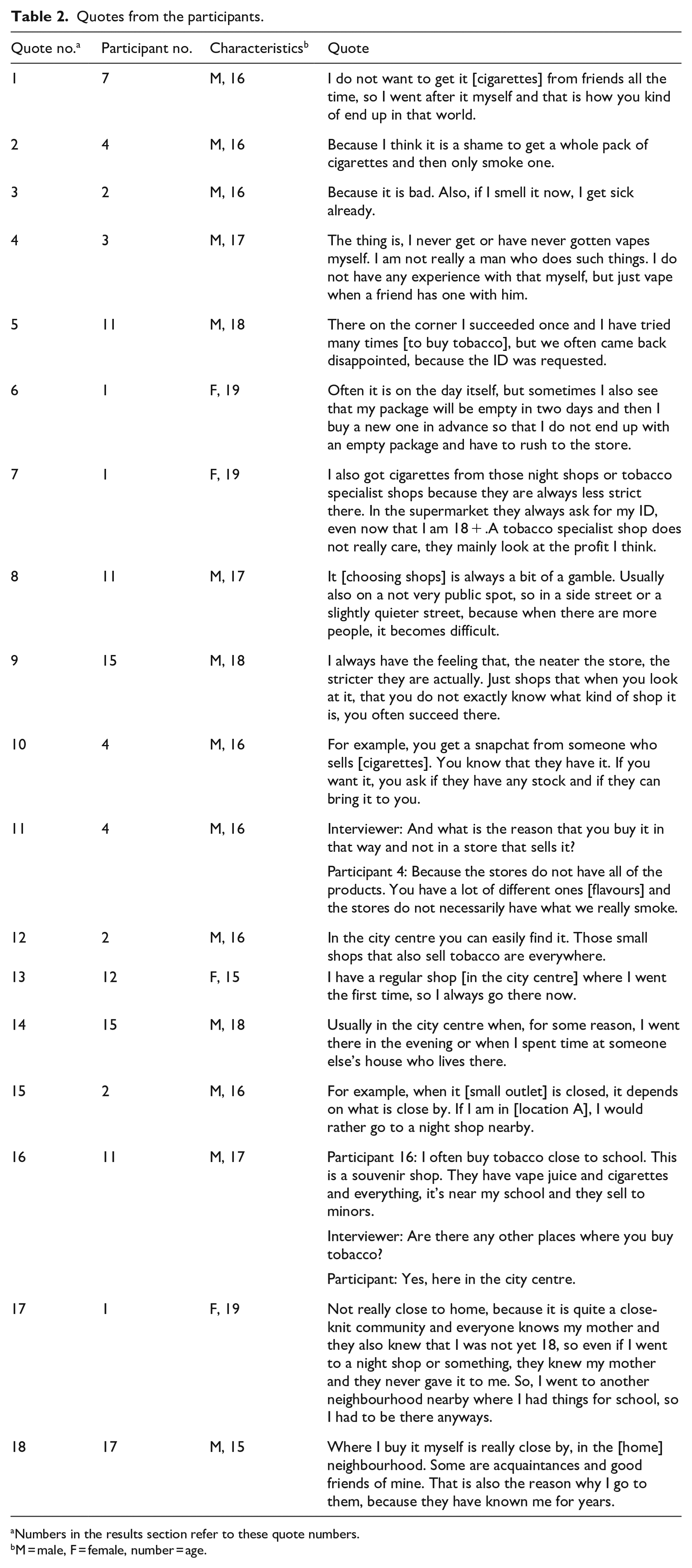
Numbers in the results section refer to these quote numbers.
M = male, F = female, number = age.
Motivations for tobacco-purchasing behaviour varied. Respondents bought tobacco for someone else, or they preferred to buy it for themselves because they did not want to use someone else’s cigarettes1 or ask for tobacco products. Participants identified several reasons why they did not always buy tobacco themselves: (1) They did not need a full pack and instead got individual cigarettes from friends2, (2) they did not want to spend money on something that is unhealthy3, (3) they thought that it did not suit them as a person to buy certain tobacco products4, or (4) the cashier asked for their ID5. Participants did not describe impulsive tobacco-purchasing behaviour, instead they planned their purchases. They scheduled tobacco purchases in advance when they wanted to do so with specific friends, so a time was arranged when they were together. When their cigarette pack was empty or almost empty, they thought about buying new products in advance6. Adolescents who wanted tobacco products for a specific event, such as a party, often went on Friday afternoon or evening, so they could smoke during the weekend.
Outlet characteristics
The types of shops where adolescents preferred to buy tobacco products were small shops, such as tobacco specialist shops, souvenir shops and night shops. Those shops were considered suitable locations because fewer age verification checks took place in them7. ID checks were considered the biggest hurdle in purchasing tobacco as a minor. Adolescents reported avoiding supermarkets because ID verification was executed well at supermarkets.
Various shops offered the opportunity to purchase tobacco products, but adolescents often went to a limited number of shops to purchase tobacco products. Several shop characteristics were reported to affect the chances of successful tobacco purchase. Participants explained that when there were more customers in the store, the cashier is more likely to ask for identification8. When shops looked messy, the participants felt their chances of being successful in buying tobacco were higher9. The age of the cashier also played a role. Some adolescents experienced that younger, maybe even underage, cashiers sold tobacco products more easily to them, while other adolescents had successful purchasing experiences with older cashiers.
Tobacco products were also bought on the black market. Adolescents came into contact with street sellers via social media, such as Snapchat or Facebook. They sent a message with their order and location, and the products were delivered10. Products bought on the black market included vape products, snus and cigarettes. Adolescents suspected that these were illegal products, for example, because cigarette packs did not adhere to plain packaging regulations. They bought these products because (1) they were friends with the person who was selling them, (2) it was experienced as an easy way to buy tobacco, (3) there was a large variety in products and flavours, like vape products and snus11 and (4) products were cheaper than in a shop, even when they had to pay delivery costs.
Location
The shops where adolescents preferred to buy tobacco were in various locations in the city (e.g. close to school, home or the city centre). The city centre was visited most often by the adolescents to purchase tobacco products. It was seen as the best place to purchase tobacco, due to the high density of tobacco specialist shops, souvenirs shops and night shops12. These small shops in the centre often also had a more diverse range of products, including vape products and snus. Some adolescents went to the city centre because it was common knowledge that one could easily buy tobacco at a specific shop there13. Other adolescents bought tobacco products in the city centre because they spent much of their free time there14. This entailed spending time with friends in parks or at playgrounds, which increased the opportunity to try shops in that area.
In the adolescents’ school area, shop preference was sometimes based on proximity15. Some participants mentioned that tobacco outlets in the school area were easily accessible in school breaks or after school. Adolescents accessed specific shops in the school area when classmates had experienced that there was no ID check. Adolescents who bought tobacco in the school area often had experience with purchasing at other locations as well16.
In the residential area, the chance to run into family members was higher than elsewhere. This was important to take into account when adolescents were trying to hide their smoking behaviour from their parents. Furthermore, when cashiers knew the parents of the adolescent, this could prevent them from selling tobacco to the adolescent17. Other adolescents, however, did prefer purchasing in their residential area because they knew the people behind the counter who were willing to sell tobacco to them. It was also a convenient and easily accessible location, as the residential area was one of the locations where they spent a lot of their spare time with friends18.
The visibility of tobacco products and/or advertisements seems to play a minor role in adolescents’ tobacco purchasing. While participants spent their free time all over Amsterdam and were often randomly exposed to various tobacco outlets, most participants deliberately choose the shops where they would purchase tobacco products. Participants preferred to go to shops they were familiar with, where they knew they would not be asked for ID, instead of going to a shop at random. Moreover, many tobacco outlets in the adolescents’ activity spaces were not noticed by them. Adolescents also ignored tobacco outlets if they had the feeling that it would not be possible to purchase tobacco products in them as a minor. This often did not result in trying out new places where tobacco could be purchased, unless adolescents were more experienced with tobacco purchasing.
Discussion
Key findings
This study explored the perceived influence of the tobacco retail environment in underage adolescents’ activity spaces on their tobacco-purchasing behaviour. Adolescents preferred small shops like tobacco specialist shops, souvenir shops and night shops. Supermarkets were avoided because employees there were likely to check IDs. The city centre was seen as the best place to buy tobacco because of the high density of small shops. In adolescents’ residential area, acquaintances behind the counter might facilitate tobacco purchase, while this posed a barrier for minors who secretly smoked and did not want their parents to know they bought cigarettes. In the school neighbourhood, adolescents developed a collective knowledge of shops where they could buy tobacco products, either close to school or farther away. Cigarettes, snus and vape products were also bought on the black market because it was cheaper or because they sold specific products. Participants who spent more spare time on the street were purchasing and/or smoking tobacco products in those areas.
Strengths and limitations
Besides the adolescents’ school and residential area, this study also assessed other activity spaces, such as sport clubs or public places where they hang out. The use of a map of the city showing all the tobacco outlets made it possible to talk in more detail and more concretely about the geography of their purchasing behaviour. This allowed the researchers to explore new aspects of the adolescent tobacco-purchasing behaviour, including perceived influences of proximity, density and visibility of tobacco products in the retail environments.
This study has some limitations. The external validity is limited, as our study area, the city of Amsterdam, is geographically different from other cities and villages in the Netherlands. Besides, most participants lived in Amsterdam-North, and it is uncertain whether their experience can be generalised to adolescents living in other parts of the city. Fewer tobacco outlets are located in this part of the city than in the city centre. However, participants did travel through the whole city, resulting in exposure to other areas of the city as well. Differences between different suburbs were not covered in this study. Furthermore, the sample size is rather small. However, a lot of overlap in codes was observed between the interviews, suggesting saturation on the main topics. Because of the small sample size, it is not possible to assess potential differences related to gender, socio-economic status or ethnicity. Our results warrant further study with a larger sample in order to further examine this topic and potential differences between subgroups. In addition, it has to be taken into account that social desirability bias could have affected the responses participants gave.
Comparisons with other studies and interpretation
Adolescents stated that they were less likely to be asked for ID in small shops than in chain stores, such as supermarkets. Previous studies in Europe also found low compliance with ID checks among small retailers and high compliance in supermarkets (DiFranza and Coleman, 2001; Hewer et al., 2021; Nuyts et al., 2020a; Robinson and Amos, 2010). One explanation for this may be that there is more supervision in chain stores to oversee compliance. Furthermore, the cashier of small shops is often the owner and directly benefits from higher tobacco sales. Moreover, small shops tend to have fewer customers, which, according to participants, is associated with greater success in purchasing tobacco products due to lack of social enforcement.
Participants reported that tobacco products were bought at places where adolescents spent their free time, which were often places other than the school environment. This shows the importance of the tobacco retail environment in activity spaces other than close to schools (Kowitt and Lipperman-Kreda, 2020). Much free time was spent in the city centre. The high density of tobacco outlets was one of the reasons mentioned for purchasing tobacco in the city centre. Previous studies have shown that the density of tobacco retail outlets in adolescents’ activity spaces is positively associated with exposure to tobacco outlets and daily tobacco use (Kowitt and Lipperman-Kreda, 2020; Lipperman-Kreda et al., 2012). A Scottish study found that a high density of tobacco retailers in the residential area had a greater influence on adolescents’ smoking behaviour than the density in the school environment (Shortt et al., 2016).
Proximity played a minor role in purchasing behaviour. Participants preferred to go to shops where they were able to purchase tobacco as a minor, regardless of distance. This may be due to the large amount of free time that adolescents tend to have and the ease with which adolescents can travel through Amsterdam (by bike, scooter or public transport). Moreover, they experienced the trip to purchase tobacco as an outing with friends. Similarly, a systematic review found no consistent evidence of an association between proximity of tobacco retail outlets to homes or schools and smoking behaviours among youth (Marsh et al., 2021).
The visibility of tobacco products and/or advertisements played a minor role in purchasing behaviour. Impulsive purchasing did not occur among participants who consciously decided where to purchase their tobacco products. Among adults, previous studies have shown that tobacco visibility functions as a trigger to purchase tobacco products, which is likely due to the fact that adults (18+) do not need to avoid ID verification and therefore do not need to plan where to purchase tobacco (Burton et al., 2015).
In several interviews, purchasing tobacco on the black market was described as an alternative way of purchasing tobacco products for minors. However, it is not clear what the scope of this phenomenon was, and it is rarely mentioned in international publications. In a 2017 study in Scotland, 18.6% of adolescents between 13 and 15 years of age knew that cigarettes were sold on the black market in their neighbourhood (Haw et al., 2020). Another study in Scotland showed that this manner of purchasing tobacco was more established in socially disadvantaged urban areas (Donaghy et al., 2013). Black market sales might be more common nowadays because of new opportunities offered by social media for direct sales.
Implications
Our findings imply that the prohibition of tobacco sales in supermarkets, which will come into effect in the Netherlands in 2024, may not have much influence on the tobacco-purchasing behaviour of minors. Nevertheless, the following policies may help minimise tobacco purchasing by minors. First, Smaller shops should be checked more frequently to test their compliance with the legal age of sale. The low compliance in small shops makes it possible for minors to buy tobacco products there. If the risk of receiving a fine increased in proportion to the profit of tobacco sales, small shops may stop selling tobacco products to minors (Elharrar et al., 2020). Second, tobacco licencing should be implemented with the aim of reducing the number of tobacco sales outlets. An effective licencing system might include distance between outlets requirements, buffers around schools, and limited hours of sale. A decrease in the number of tobacco outlets is not guaranteed to eliminate tobacco purchasing by minors, however, as some shops that sell tobacco to minors may remain. However, the chances of finding such shops may decrease if density decreases, especially if retailer licences with a high annual fee specifically discourage small shops from selling tobacco products (Chapman and Freeman, 2009). Moreover, the enforcement of a legal age of sale may be easier with fewer tobacco outlets and a comprehensive register of all points of sale.
Conclusion
This qualitative study among adolescents in Amsterdam found that adolescents actively visited small shops that were known to sell tobacco to minors, rather than going to a nearby outlet or to shops enroute to elsewhere. To reduce levels of tobacco purchasing among adolescents, a reduction in the number of outlets and stricter enforcement of the purchasing age limits are needed.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was part of the ‘Tobacco out of Sight’ project funded by the Dutch Lung Foundation, the Dutch Heart Foundation, the Dutch Cancer Society, the Dutch Thrombosis Foundation and the Dutch Diabetes Research Foundation, under project reference 2.1.19.007.