
Abstract
Objective:
Studies suggest that healthcare professionals often feel unprepared to deal with mental health issues in refugees and asylum seekers. The aim of this qualitative study was to examine the experiences of refugees and asylum seekers in relation to mental health and healthcare, to inform cultural competency training for undergraduate medical students.
Method:
Focus groups were conducted with 16 refugees and asylum seekers and staff from relevant charity organisations in Wales. We explored participants’ experiences in relation to mental health and healthcare, and training for healthcare professionals. The data were thematically analysed using an inductive approach.
Results:
Three overarching themes were identified: (1) recognition of the specific mental health needs of refugees and asylum seekers, (2) barriers preventing effective mental healthcare delivery for refugees and asylum seekers and (3) authentic learning experiences for medical students.
Conclusion:
To our knowledge, this is the first study to actively involve refugees and asylum seekers, along with individuals who work closely with this population, in considering the development of cultural competency training for healthcare students and professionals in relation to mental health. If we are to reduce the risks of exclusion from healthcare for refugees and asylum seekers, training in this area is essential. Findings from this study have informed the development of a guide for healthcare educators with a focus on refugee and asylum seeker mental health.
Introduction
With the global rate of refugees and asylum seekers (RASs) now standing at 27.1 and 4.6 million, respectively, at the end of 2021 (United Nations Higher Commissioner for Refugees, 2021), the number of forcibly displaced persons worldwide is at a record high. According to United Nations Higher Commissioner for Refugees (UNHCR, 2022) statistics, as of mid-2022 there were 231,597 refugees and 127,421 pending asylum cases in the United Kingdom.
Mental health problems are among the most commonly reported health issues experienced by RASs (Bogic et al., 2015), who often display physical, emotional and social manifestations of trauma (Satinsky et al., 2019). Common factors that contribute to distress are denial of the right to work, geographical dispersal and immigration detention (Giacco et al., 2018). The experiences of being a refugee or asylum seeker are heterogeneous (Bhugra, 2017), with individuals coming from diverse cultural and socioeconomic backgrounds, with varying pre- and post-migration experiences, and having a range of physical and mental health needs. This makes meeting the mental health needs of such individuals challenging for healthcare services (Murphy et al., 2002).
Cultural competency training in healthcare
One of the key strategies identified for addressing health disparities in society and ensuring equal access to healthcare is cultural competency training. Cultural competence is one’s ability to provide care to patients who have diverse beliefs, behaviours and values and tailor healthcare delivery to meet individual patient needs (Swihart et al., 2022).
Many RASs do not access mental health services due to cultural, social, linguistic and structural barriers (Crawley et al., 2011). Structural barriers include charging regulations, the refusal to register patients at general practitioner (GP) practices without proof of ID, and the complexities of navigating the UK healthcare system. Asif and Kienzler (2022) found that these barriers lead to risky help and health seeking, lack of or inadequate healthcare, and worse health outcomes among this population. RAS patients encountering negative experiences of seeking healthcare often report feelings of discrimination and a lack of confidence in healthcare services, leading to reduced uptake of services (Kibondo et al., 2000). Studies also suggest that healthcare professionals often feel unprepared to deal with mental health problems among RASs (Harris et al., 2020; Phillimore et al., 2007; Robertshaw et al., 2017).
Currently, there is little evidence about which cultural competency techniques are effective in health care and less evidence on when and how to implement them properly (Brach and Fraser, 2000). Within healthcare training, there continues to be a lack of knowledge and commitment to cultural competency, which in turn restricts the ability to help professionals and highlights the urgency for further research (Rukadikar et al., 2022). There is significant variation in cultural competency training available to healthcare workers with some methods including cross-cultural communication skills scenarios, individual self-awareness assessments and presentation of clinical cases during team meetings (McGregor et al., 2019). One of the most accepted definitions of culture competence comes from the study by Cross et al (1989), who characterise cultural competency by the combination of cultural knowledge, awareness and sensitivity. Despite a vast number of progressive definitions of cultural competence since then, ultimately cultural competence is endorsed through practice and is a dynamic and developmental process (Cross et al 1989; Villagran, 2022). The process of acquiring cultural competence involves the complex integration of knowledge, attitudes and skills over time, with the intention of improving communication between individuals resulting in more effective interactions with others (Clark et al., 2011).
This study used a deductive, bottom-up approach, through which cultural competence was examined through the lived experiences of RASs and staff working with them. By eliciting stakeholder perspectives in relation to mental health and healthcare experiences, we aimed to inform cultural competence training in healthcare in a way that is meaningful, that allows us to challenge our own biases and assumptions and is based on individual perspectives and diversity of lived experience. This study provides insight into the experiences of RASs, in relation to their mental health and access to healthcare, with a view to informing future cultural competency training for healthcare students and professionals. The study aimed to answer the following research questions:
What are the experiences of refugees and asylum seekers in relation to mental health and access to healthcare in the UK?
How can we improve the experiences of refugees and asylum seekers in relation to mental health through cultural competency training for healthcare professionals?
Materials and methods
Study design
Focus groups were conducted to allow for an in-depth exploration of the insights, perceptions and attitudes of both RASs, and staff members from charity organisations, who work with this population, in relation to their mental health needs, access to healthcare services and training for healthcare students and professionals. In this study four focus groups were conducted, with a total of seven RAS participants (randomly allocated to two focus groups) and nine staff members (also randomly allocated to two focus groups) from charity organisations. This qualitative study followed a constructivist approach with the aim of identifying the social, cultural and structural contexts that influence an individual’s experience.
Participant recruitment
Refugees, individuals seeking asylum and staff members, were recruited through Oasis Cardiff (https://www.oasiscardiff.org/) and ‘Diverse Cymru’ (https://www.diversecymru.org.uk/). Oasis Cardiff and Diverse Cymru are both charity organisations supporting RASs in Wales. Staff participants worked for these organisations in a variety of roles (for example, as mental health support workers, administrators and recovery practitioners). The research team attended Oasis and Diverse Cymru’s premises on a number of occasions to talk to RAS and staff about the study and invite individuals to participate. All staff members working for these organisations were invited to participate by email. The aim was to recruit between four to eight participants for each focus group.
All participants were aged 18 or over at the time of the study and had the capacity to provide written informed consent. All participants were individuals who self-identified as refugees or asylum seekers based on definitions provided by the Refugee Council (2021). RAS who spoke at least a basic level of English (so that they could understand the concept of the study, provide written informed consent and contribute to the focus groups) were invited to take part in the study.
Data collection
As some participants were limited in their ability to read English, the content of the information sheet was explained verbally to ensure participants were fully informed. All participants were given the option of discussing the project with the research team or a member of staff from the organisation through which they were recruited. All those who agreed to participate then gave informed written consent. Separate focus groups were conducted for RASs and for staff, with the aim of creating a safe space for participants to share their thoughts and experiences.
The focus group interview instrument (online supplemental appendix A) was designed following an inductive approach with the aim of allowing participants to guide the content of the discussion, for example by encouraging further discussion on certain topics/issues, including the sharing of feelings and personal experiences. Summary questions were asked to check accuracy throughout. Focus groups were run by either CS or SW who also took notes. The study team met regularly for reflexive discussion to challenge interpretations and potential biases and examine the data to iteratively guide the development of the interview instrument questions.
The focus group discussions lasted between 30 and 60 minutes. The smaller group size enabled participants to express, share and discuss their perspectives and experiences in a shorter space of time than might be possible with larger groups. Again, this can be of benefit where focus group discussions involve sensitive issues and experiences.
The focus groups were audio recorded and transcribed. All transcriptions were anonymised to ensure confidentiality.
Data analysis
The data were analysed using reflexive thematic analysis following Braun and Clarke’s (2006, 2021) six-step approach. Reflexive thematic analysis is a flexible interpretative approach to qualitative data analysis that facilitates the identification and analysis of patterns or themes within a data set (Braun and Clarke, 2012). It acknowledges the researchers’ active role in knowledge production (Braun and Clarke, 2019) and therefore a collaborative approach aimed at achieving richer interpretations of meaning, rather than consensus, is adopted. Themes are not predefined, rather they are produced by organising codes around a relative core commonality (Braun and Clarke, 2019). Reflexive thematic analysis allows researchers to respect the subjectivity of participants accounts, while acknowledging the researchers’ own interpretations.
To ensure familiarisation with the data, the transcripts were read multiple times and checked against the original audio recordings. Analysis involved all three members of the research team who each independently examined the transcripts. When re-reading the data generated no new meanings or patterns, semantic codes were created. NVivo (Version 11) was used to support the coding process. An experiential orientation to data interpretation was adopted in order to emphasise meaning making by participants. A predominantly inductive approach was taken whereby data were open-coded and respondent/data-based meanings were brought to the fore. Each member of the research team coded the data independently before attending team meetings to consider and discuss interpretations of the data, in the context the researchers’ beliefs and potential biases. Thematic patterns were generated and recorded according to the topics that were discussed in depth and at length by the groups. Themes were reviewed to ensure the data supported the theme. Findings are described using quotations as illustration.
Ethical approval was received from Cardiff University School of Medicine Research Ethics Committee. All data and materials were managed and securely stored in line with Cardiff University and Data Protection guidelines.
Results
Demographic information for the RASs who took part in the focus groups is presented in Table 1 below. Participants came from a variety of countries, had been in the United Kingdom for 2–20 years and aged between 21–80 years.
Demographic information for the seven refugee/asylum seeker participants.
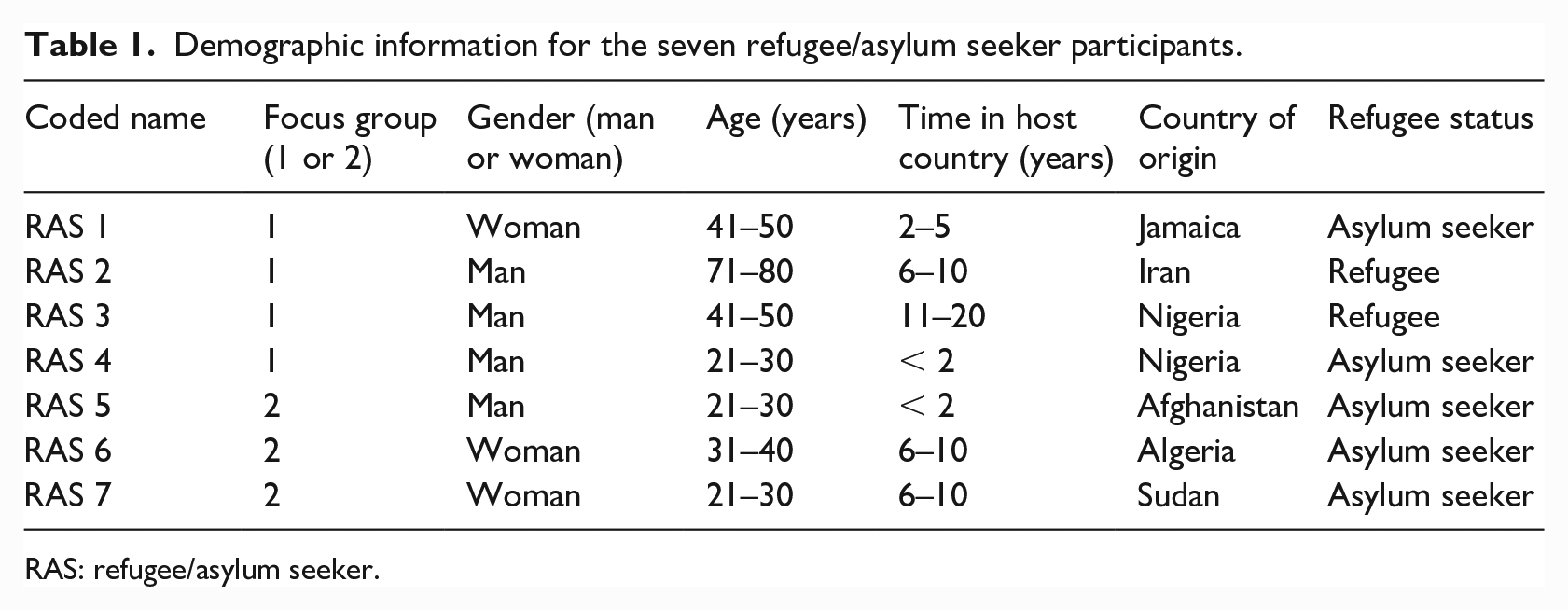
RAS: refugee/asylum seeker.
Participant perspectives shared during the focus groups reflected their differing backgrounds and experiences of migration. Following reflexive discussion and agreement within the research team, three overarching themes were identified: the specific mental health needs of RASs, barriers that prevent effective healthcare for RASs and authentic forms of cultural competency training.
The specific mental health needs of refugees and asylum seekers
This theme described the shared mental health needs of RASs, as expressed by both staff and RAS participants. Staff participants stated that many of the RASs that they worked with suffered from mental health conditions such as depression, anxiety, stress and post-traumatic stress disorder ‘You’ve got your depression, stress and anxiety around your specific asylum cases then you’ve got your complex, comorbid PTSD with that.’ (Staff 1)
RAS with longer resettlement times reported symptoms more closely associated with depression, including ‘[I] cry every night’ (RAS 3), whereas participants with shorter resettlement times reported symptoms more closely associated with post-traumatic stress disorder, such as ‘[I felt I was] going crazy’ (RAS 5) and having ‘flashbacks’ when thinking back to their pre-migration trauma (RAS 2).
Staff members and RAS participants themselves reported the impact of both pre-migration trauma and post-migration difficulties on mental health. Staff members stated that many RASs have mental health problems due to seeing the torture or murder of loved ones in their country of origin: ‘People will say have a look at this film and they’ll show you a decapitation of their family member.’ (Staff 2)
Separation from family members was also discussed by the RAS participants as impacting on their mental health: ‘You leave your family behind . . . and you’re here and you’re thinking what’s happening to my boy.’ (RAS 3)
It is worth noting that the migration process itself causes just as much, if not more distress and trauma: ‘When I came here on top of a ship, there were five, but one person died. He died beside my side . . . can you imagine what it’s like? You see the guy tangles in the propeller and he’s on a frantic sea and he’s going to be left there.’ (RAS 2)
Post-migration hardships were the most prominently discussed cause of distress and detriment to mental and physical health by the RAS participants, with a fear of deportation, ongoing difficulties in obtaining refugee status and poor living conditions being the most common ongoing difficulties: ‘I’ve been without a house since 2014 . . . Most times I have to put on damp clothes. Clothes that are very cold because they are in the shed outside’ (RAS 1) ‘long waiting . . . your health gets worse as you have to wait’ (RAS 6)
Despite significant pre-migration trauma, it was possible to see how post-migration experiences were equally, if not more, significant, to RASs, in terms of their impact on mental health. These post-migration experiences are also likely to impact on the ability of RASs to recover from pre-migration trauma.
Barriers that prevent effective healthcare for RASs
Language and culture
Consistent with previous research, language was highlighted as a major barrier to mental health, both by staff and RASs. Staff described experiences supporting RASs where language barriers meant they were unable to share their experiences and concerns. One of the staff participants described how a patient had to rely on his wife to tell his story, as her English was better than his own. This resulted in the patient becoming frustrated as his wife’s views on his mental health problems were very different to his own views. Due to the language barrier and the fact that the staff were relying on her viewpoint, the information given was not based on the individuals’ own perspective, as the staff later discovered: I could see he was getting more and more distressed because she was translating on his behalf, but she was throwing in her own experiences of what it was like to be supporting him with mental health issues. Then when she left the room, I actually found that he was telling me there were more complications that he didn’t want to put on his wife. (Staff 3)
There are many reasons why RASs may find it difficult to share experiences in relation to their mental health, and language is often an additional barrier. Participants pointed out that even professional translators did not solve all linguistic communication problems as there are variations in dialect used within their language: ‘. . . you go to the appointment [and] someone translates Arabic. We understand it, but it takes more than one, two times’ (RAS 7)
Staff members and RASs stated that mental illness was not recognised as an ‘illness’ in many cultures. This led many RAS patients to become confused when they were asked about their mental health or mental illness. Many RASs did not recognise themselves as having mental health problems, which then makes accessing mental health services even more difficult: I still remember an Eritrean man saying to me “What does depression mean?” because he had been asked . . . “Do I suffer from depression?”. He says ‘I don’t know what that is’, and I explained what it was, because of your symptoms because I knew quite well that he did. ‘We don’t have that word in our language’, so for a lot of people the word and what they’re going through, to them it’s normal because they don’t know any different. (Staff 4)
The way mental health symptoms were talked about, therefore, differed between RASs and staff participants. Staff participants used more familiar medical terminology to describe mental health symptoms, whereas RAS participants used physical actions, for example, acting out their head or heart being in pain, as they found this easier than attempting to explain their problem in English. Furthermore, RAS participants used colloquial rather than medical language to describe their mental health symptoms. This was clear when they described lack of sleep due to thinking about trauma that they had witnessed in the past: ‘I was going crazy’ (RAS 5) ‘In me, I cry every night’ (RAS 3)
Experiences of healthcare
Staff participants stated that some healthcare staff were not always aware of the services that are available when caring for RAS patients. This can result in negative healthcare experiences and reduce the likelihood of RASs engaging with healthcare services again in the future. Language and communication issues can also lead to negative healthcare experiences for RASs. GPs and health practitioners do actually have a legal requirement to use language line, but often they don’t know that that’s a legal requirement or they can’t access an interpreter so will use a family member. It’s quicker. The person is there. The person is available, and there can be issues that come out of that as well. (Staff 5)
Language barriers posed significant challenges for both patients and professionals, and can impact on patient experiences of care and patient safety. The use of interpreter services may address some of these challenges, although it may also introduce additional challenges in terms of accessibility, confidentiality and financial cost.
RAS participants explained that they felt that they are not believed, particularly when disclosing traumatic experiences, or felt that their experiences were not validated, and that this impacted on their interactions with healthcare staff. They reported having difficulty trusting healthcare professionals, resulting in a barrier to building an effective therapeutic relationship. One participant felt a doctor did not believe her when she tried to explain how traumatised she felt: ‘It’s like some of them don’t believe what you’re saying’ (RAS 1)
Together, these experiences impact on the likelihood of individuals accessing and engaging with healthcare services and further consolidate feelings of distrust in the healthcare profession.
Holistic care: psychological and social factors
A number of individuals within the RAS group discussed occasions when they felt healthcare professionals had tended to focus on treating their physical symptoms without consideration of their mental health status. They felt that insufficient consideration was given to the psychological and social factors that were impacting on their lives and their health. ‘The doctor no listen to what’s in my mind . . . The doctor just gives you the tablet. Just take the tablet’ (RAS 5)
Participants also highlighted the uniqueness of each individual’s own story in relation to their mental health problems and experiences: ‘Problems, our own problem . . . It depends on the individual . . . each refugee has their own needs and wants’ (RAS 3)
One participant said that a failure to take psychological factors into consideration could lead to healthcare professionals making false assumptions: ‘ . . . they don’t know some of the problems, what the individuals are going through . . . They’re just acting based on all this . . . so they judge on what they see in front of them’ (RAS 3)
RAS participants felt that such experiences with healthcare, and the focus on physical health, rather than mental health, made them less likely to engage with healthcare. They expressed the desire for a more holistic approach in which psychological, social and physical concerns are taken into account.
Authentic cultural competency training
Staff participants stated that training should be mandatory for healthcare students and staff in relation to cultural competency and mental health. Staff felt that mandating such training was an essential step towards meeting the mental health needs of refugees and asylum seekers in the future: We . . . have to deliver training to professionals, students and nurses and doctors . . . So, but not again it’s a choice, it’s not mandatory, it’s whoever wants to come on that training, so you’re not going to. That will never change, it will always stay the same until you make things mandatory. (Staff 1)
Participants stated that having patient involvement, with RASs talking about their experiences would improve students’ understanding of cultural differences and mental health problems and how to manage these: ‘People’s experience. No online learning. Online learning does not do it . . . It’s ticking boxes and then you get a certificate and ask them what they read two months down the line and most people won’t remember.’ (Staff 5)
Two RAS participants advocated for an authentic learning experience, whereby medical students attend refugee charity centres and interact with, and learn from, RASs themselves: ‘. . . a day out of the week . . . one of these offices can be used . . . so it’s sort of like a placement . . . to come to places like this and get the facts right’ (RAS 3) ‘. . . come in and listen to people and know people that are really going through’ (RAS 1)
This would also provide RASs with a chance to discuss their stories and problems, which many of the participants found beneficial. A number of participants felt that talking during the focus group itself has been a positive experience for them and that talking to healthcare students could also be of benefit to their own mental health as well as to students’ learning: ‘Good talking is better, like now’ (RAS 5)
A number of individuals from the staff member group suggested the use of case studies in cultural competency training as a means of providing a more authentic and impactful learning experience: ‘The experience has a more powerful effect than any Power-Point or anything like that. Hearing individual case-studies and hearing direct experiences is very, very valuable.’ (Staff 5)
Case studies could provide an opportunity for reflective discussion and problem solving, thereby increasing interactivity and promoting active learning (Mahdi et al., 2020).
Discussion
This study provides insights from RASs and staff who work closely supporting them in relation to mental health, access to healthcare and the development of cultural competency training for healthcare students and staff. Findings can support organisations involved in training healthcare staff and students in the development of cultural competency training generally, but also in relation to the specific topic of RAS mental health.
The ability of healthcare professionals to be able to recognise mental health conditions is important when working with this population as additional barriers may make diagnosis difficult (Crosby, 2013; Kirmayer et al., 2011). The mental health conditions described in focus groups are consistent with those found in the literature. RASs are at particular risk of developing mental health problems such as anxiety, depression and post-traumatic stress disorder (Blackmore et al., 2020). However, it is important to remember that the experiences of RASs are heterogeneous, and assumptions should not be made in relation to their health and healthcare (Fazel et al., 2005). In this study, participants with longer resettlement times reported symptoms associated with depression. These findings are consistent with the literature in that time spent in the host country is a strong predictor for mental health disorders (Bogic et al., 2012).
The high prevalence of mental health problems experienced by RASs is known to be due to the difficulties experienced before, during and after seeking asylum in another country. The number of people seeking asylum in the United Kingdom who are awaiting a decision on their case has increased by 408% between 2017 and 2022. The number of annual asylum applications in the United Kingdom has increased during this time (from 26,764 to 72,027 applications); however, in the same period, the backlog in processing cases has increased to five times its size (Home Office, Asylum and Resettlement Datasets, 2023; UK Parliament, 2023). Some of the asylum seekers who took part in our focus groups reported having been in Wales for nearly 10 years.
It is well established that RASs face many barriers in relation to accessing healthcare (Asif and Kienzler, 2022; Crawley et al., 2011; Kibondo et al., 2000). In line with previous studies, our study found that language and culture, including religious beliefs and health beliefs, were identified by RASs and staff as key issues when considering barriers to healthcare. Effective communication is fundamental to establishing an accurate diagnosis and ensuring patient safety. Several participants highlighted that the use of professional interpreters did not solve all linguistic communication problems. This is in line with the literature, which reveals that communication errors are common with interpreters, especially those with a different dialect or ethnicity to the patient (Blackwell et al., 2002).
There is a need for increased knowledge and awareness regarding cultural differences in the description and perception of mental health among diverse populations, taking into account health and religious beliefs. For some participants, the concept of mental illness or mental health was not one they were familiar with, and it is important that cultural competency training includes a focus on how to use language appropriately, and to explore patient’s experiences and belief systems, when discussing mental health.
RASs often do not feel comfortable disclosing traumatic experiences to healthcare professionals, and this has been identified as a barrier to receiving appropriate care (Giacco et al., 2014). Previous research has suggested that physicians often feel uncomfortable asking questions and communicating with RASs about their trauma histories (Bhatia and Wallace, 2007). This can leave doctors unaware of such trauma histories and associated health effects (Harris et al., 2020; Shannon et al., 2012).
For doctors to engage effectively with RASs who have experienced psychological trauma, an understanding of trauma-related symptoms and trauma history is required (Sher and New, 2016). This is an important consideration for cultural competency training, where we need to raise awareness of the impact of trauma on RASs, and its relationship to mental health outcomes. Cultural competency training needs to provide opportunities for students and professionals to become more comfortable discussing trauma histories in appropriately supervised and supportive settings.
This study highlighted a desire for a more holistic, trauma informed, approach to healthcare in which both emotional and physical concerns are considered. Holistic care requires the healthcare provider to consider the person as a whole and emphasises the connection between the human body, mind and spirit (Saha et al., 2008; Zamanzadeh et al., 2015).
The results of this study indicate that RASs and staff felt that cultural competency training for healthcare students and professionals should be mandatory. This is in line with the findings of Sen (2016) who found that making cultural competency training mandatory for all healthcare professionals can ensure the development of interpersonal and academic skills that enable staff to understand cultural differences (Sen 2016). Making training mandatory for healthcare staff and students can ensure safe and effective delivery of care to patients (Alcolado et al., 2014). However, evidence also suggests that where training is mandatory, motivation to learn decreases (Tziner et al., 1991). Individuals who are consulted about decisions regarding their attendance at training courses, including when and if they need to attend, are likely to be more motivated to learn during the training session (Machin and Treloar, 2004).
The suggestion of students learning through interactions with RASs, for example, with medical students undertaking placements in refugee charity centres, is supported by ‘situated learning theory’, which states that learning should be situated within an authentic activity, context and culture. Situated learning environments place students in authentic learning situations in a social community, where they are actively immersed in activity. Within this context, learning is often largely unintentional (Brown et al., 1989).
Our findings highlight the importance of designing and delivering authentic cultural competency learning experiences for healthcare students and staff. In health professional education, authentic learning is an instructional approach that allows students to explore, discuss and construct concepts and relationships in contexts that involve real-world problems, projects and issues relevant to the learner (Donovan et al., 1999). The ‘placements’ suggested by a number of participants, whereby students attend refugee charity centres to learn directly about the experiences of RASs, would be mutually beneficial to both students and RASs, creating an authentic experiential learning opportunity for students. It would allow medical and other health professional students to gain a first-hand insight into the cultural background and mental health needs of RASs, thereby increasing their cultural knowledge, awareness and comfort in interacting with patients from diverse backgrounds. Clearly there are challenges associated with this method of curricula delivery, and careful planning and support is required with the needs of RASs always being prioritised.
The suggested use of case studies to educate students is a well-established, evidence-based teaching method (Anderson and Krathwohl, 2000). However, it is important to recognise that case scenarios also risk perpetuating existing stereotypes. Using real-life cases to support cultural competency learning experiences in healthcare could improve students’ learning with regard to RASs’ mental health, where the scenarios are real, and co-created with those having first-hand experience of the issues that the case is designed to address.
Strengths and limitations
This study is the first of its kind to address the importance of cultural competency in relation to RAS mental health, from the perspectives and experiences of RASs themselves. It lays the foundations for future studies, involving RASs, to develop and expand on this work. This is particularly relevant considering recent international events, the impact of war and other political and social factors, and the continuing rise in the number of RASs worldwide.
The use of focus groups provided rich data and authentic descriptions from the staff members and RASs. The nature of focus groups allowed for the creation of a mutually supportive, and in some respects, empowering environment for the discussion of sensitive topics (Owen, 2001). The disclosure of sensitive information was vital to reflect the realities of the experiences of our participants and in turn, enhance the authenticity of this study and its findings.
However, the study focused on a relatively small number of RASs and staff participants, all from a single UK city. There are likely to be differences in the experiences of RASs across the United Kingdom, and across different countries, and it is important that the potential for geographical variations in experiences is considered. Future studies including participants from a range of different geographical locations may benefit from a greater breadth of data.
Importantly, this study did not collect specific information about participants’ mental health diagnoses, or whether RASs had been diagnosed pre- or post-migration. In addition, this study only included RASs and staff participants who were able to communicate in English, which excludes many who may have faced even more issues while accessing healthcare. Future studies would benefit from the involvement of professional interpreters and/or bilingual researchers.
Conclusion
To the best of our knowledge, this is the first study to actively involve RASs, along with individuals who work closely with them, in considering the development of cultural competency training for healthcare students and professionals in relation to mental health. Education and training in this area is essential if we are to reduce the risks of exclusion from healthcare for RASs.
Findings from this study have informed the development of A Guide for Healthcare Educators: Refugee and Asylum Seeker Mental Health (https://sway.office.com/dL2eCzSwiMwbZOgh?ref=Link), which provides advice to educators involved in developing cultural competency training.
While improving cultural competency training for healthcare professionals is only one component needed to improve mental health outcomes for RASs, system-wide improvements are required to support more far-reaching changes in this area.
Supplemental Material
sj-docx-1-hej-10.1177_00178969231182104 – Supplemental material for Cultural competency and mental health training for medical students: Learning from refugees and asylum seekers
Supplemental material, sj-docx-1-hej-10.1177_00178969231182104 for Cultural competency and mental health training for medical students: Learning from refugees and asylum seekers by Charlotte Silver, Sara Williams and Liz Forty in Health Education Journal
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.