
Abstract
Background:
Adopting healthy weight-related behaviours in emerging adulthood has long-term health benefits. Digital interventions using game-elements have the potential to improve diet and physical activity outcomes. Universities are influential settings in shifting emerging adults’ behaviour and can deliver health-promoting interventions to young adults.
Objectives:
To investigate the effect of an online intervention using quiz-games on nutrition knowledge, diet quality, physical activity and sitting time in a sample of university students.
Design:
Randomised, single-blind, controlled trial.
Setting:
Two UK Universities including a total of 88 students from different faculties.
Method:
The intervention group (n = 50) had access to 10 quiz-games and a website for 10 weeks. The control group (n = 38) received no such resources. Main outcomes were nutrition knowledge, diet quality, physical activity and sitting time assessed by self-administered questionnaires. Frequency and performance of the quiz-games played, and the effect of time (days) on performance after playing a quiz-game for the second time, were also investigated.
Results:
No significant differences were found between groups over time in any of the outcomes. The outcomes remained non-significant when engagement rates with the quiz-games were considered. Among the 35 game-players (n = 15 did not play any game), 15 played at least one quiz-game. Frequency of playing a quiz-game by all students ranged from 43 to 17 times, and mean scores (% of correct answers) ranged from 55% to 82%. When repeating a quiz-game within 8 days, the performance (score) was improved while after that point, performance remained the same or decreased.
Conclusion:
Online game-based interventions can be easily implemented in university settings. However, further research is needed on their design to enhance engagement and identify key factors affecting students’ behaviour to increase their effectiveness.
Introduction
Emerging adulthood, defined as the period from the late teens until early adulthood (18–25 years) has been described by Arnett (2000) as a distinct period in the life course characterised by higher independency, exploration and experimentation that may determine life choices in later adulthood. For many, it is also a period for weight-related behaviour changes as pooled evidence from longitudinal studies have shown changes in physical activity (Corder et al., 2019; Gropper et al., 2020) and dietary behaviour (Winpenny et al., 2017, 2018). The Project EAT among US adolescents showed a decrease in fruit and vegetable intake (FVI) (by >½ serving/day, N = 2,105) (Larson et al., 2007) and an increase in fast-food consumption (by 0.4 times per week in girls) (Bauer et al., 2009, N = 2,516) during the transition from high school to adolescence. The same cohort also showed a decline in weekly hours of moderate-to-vigorous activity (from 5.1 to 3.5 hours/week for girls) and an increase in time of computer use (from 10.4 to 14.2 hours/week for boys) (Nelson et al., 2006).
Adopting unhealthy eating and physical activity habits in early adulthood can have long-term health implications. The Adolescent Health study, also in the USA, which followed high school participants aged 16–17 years for 5 years, found an increase in obesity prevalence (from 13.1% to 23.6%, N = 3,657) which remained high 12 years later from baseline (Gordon-Larsen et al., 2010). The US CARDIA study showed that young adults aged 18–30 years with poor diets (e.g. high intakes of fast-food, meat and snacks) at baseline had a higher incidence of cardiometabolic risk over a 20-year study period when compared with participants following a diet closer to guidelines (Duffey et al., 2012). Engaging in regular physical activity also has long-term benefits, including reduced risks of obesity, coronary heart disease, type 2 diabetes and mental health conditions (Reiner et al., 2013) while long-term health benefits have been found in adults who became active in early adulthood and remained active over time despite being inactive as adolescents (Rangul et al., 2012).
Data from the 39 member countries of the Organisation for Economic Co-operation and Development (OECD, 2014) showed that about 58% of emerging adults entered tertiary education in 2012 with evidence suggesting unfavourable changes in weight-related behaviours during the transition from high school to tertiary education (Deforche et al., 2015; Gropper et al., 2020). An epidemiological study in Spain has found that two out of three university students failed to meet the recommended levels of physical activity (Arias-Palencia et al., 2015) while another cross-sectional study in the USA showed that about one-third of students consumed confectionary and fast-food once to twice a week, and less than 10% consumed more than two portions of fruit and vegetable per day (Yahia et al., 2015). In addition, a meta-analysis by Vadeboncoeur et al. (2015) including data from longitudinal studies (22 studies, N = 5,489) demonstrated that students gained an average of 1.36 kg during their first year of studies with similar individual studies indicating that weight gain (Pope et al., 2017) and unhealthy weight-related behaviours remained throughout university years (Small et al., 2013). University students have reported that a cluster of personal (e.g. previous habits, self-efficacy), social (e.g. behaviour and support of peers or close ones) and environmental (e.g. availability and accessibility of food or exercise facilities, living arrangements) factors impact their eating and physical activity behaviour (Deliens et al., 2014, 2015; Pelletier et al., 2014). Increased nutrition knowledge in students has also been associated with the development of healthy eating behaviours (Cooke and Papadaki, 2014; Kolodinsky et al., 2007); however, cross-sectional data indicate gaps in students’ knowledge in relation to foods containing fat, salt and fibre and optimal weight-management behaviours (Belogianni et al., 2021).
Digital interventions have been used to target dietary and physical activity behaviour in non-clinical populations (Gold et al., 2021). Examples include the use of mobile phones (e.g. texting), digital devices (e.g. pedometers) and Internet-based interventions. Gamification refers to the use of game-elements such as videos, rewards and social features in non-gaming systems to enhance user experience, motivation and engagement (Chan et al., 2019; Deterding et al., 2011). In the UK, emerging adults are peak users of video games (Statista, 2021) while the time users spent on gaming has been associated with adverse health indicators such as increased caffeine and junk food intake (Ream et al., 2013) and higher body mass index (BMI) (Huard Pelletier et al., 2020). Universities are influential settings in shifting emerging adults’ behaviour (Micallef et al., 2021) and therefore can favourably use the time young adults spend on gaming to deliver health-promoting interventions (Nelson et al., 2008). Digital interventions have the potential to improve diet and physical activity outcomes. However, more research is needed targeting specific populations and using designs that enhance motivation and adherence to the intervention (Gold et al., 2021). Due to its underpinning characteristics, gamification can be used in health-related contexts and as part of online interventions to make the learning process more appealing and increase participation (Kapp, 2012; Pereira et al., 2014).
Considering the weight-related behavioural changes occurring in emerging adulthood and the associated long-term health implications, emerging adulthood is an important timeframe for health promotion. The primary objective of this study was to investigate the short-term effect of an online intervention using game-elements (quiz-games) on nutrition knowledge, diet quality and physical activity in a sample of university students. Quiz-games’ characteristics including adherence (frequency) and performance (score) of games played and the effect of time (days) on performance after repeating a quiz-game were also investigated.
Materials and methods
Design and study population
A single-blind, randomised controlled trial (RCT) with two data collection points and two parallel arms was used to engage with the research questions and test the hypotheses – that university students’ engagement with playing the quiz-games as part of the online intervention would improve their nutrition knowledge, diet quality and physical activity behaviour. A detailed description of the study methodology can be found elsewhere (Belogianni et al., 2019).
Eligible students were those aged 18–34 years enrolled at the time of the study (2017–2018) in two London-based universities, and free of any medical or other condition that required special dietary treatment. Recruitment was open throughout the academic year. Students were screened for their readiness to perform a safe level of physical activity (Thomas et al., 1992) and their potential risk of having an eating disorder (Morgan et al., 1999) and those at risk were excluded from the study (n = 0). The sample size was calculated based on nutrition knowledge score using Kliemann et al.’s (2016) method. Kliemann et al. (2016) found that mean scores in nutrition knowledge were 79.3 (SE = 0.51, SD = 5) for students studying Dietetics and 67.7 (SE = 0.97, SD = 9) for students studying English in the UK, and the overall score difference was 11.5 points (95% confidence interval [CI]: 9.3–13.7). Additional evidence suggests that an 8%–9% (7.0–8.0 points) increase on the initial knowledge score significantly improves diet quality (Kullen et al., 2016). In the current research, students from all university faculties were invited to participate in this study; therefore, a standard deviation between 7 and 9 was expected in the mean scores of this mixed population. Setting the power at a 90% level and significance threshold at p < .05, a sample size of at least 35 participants in each group would satisfy the preceding criteria. Considering a 25% dropout rate, the overall sample size needed for this study was 88 participants.
A convenience sample of 88 participants entered the study and were randomly assigned to the intervention or the control group (Figure 1). Computer-generated random numbers (Urbaniak and Plous, 2015) based on a 4:3 allocation ratio (intervention: control) were used for randomisation as a higher dropout rate was expected from participants in the intervention group. Written consent was provided before students entered the study. The data collection points were at baseline and after a 10-week interventional period. Participants in the intervention group received access to the intervention while the control group had no access and did not receive any other educational materials. The study obtained approval by the Faculty Research Ethics Committee of Kingston University and St George’s, University of London (FREC 2017-12-009), and was registered in the ClinicalTrials.gov database (identifier NCT03028714). Students who completed the study received a £10 Amazon voucher token at the end.
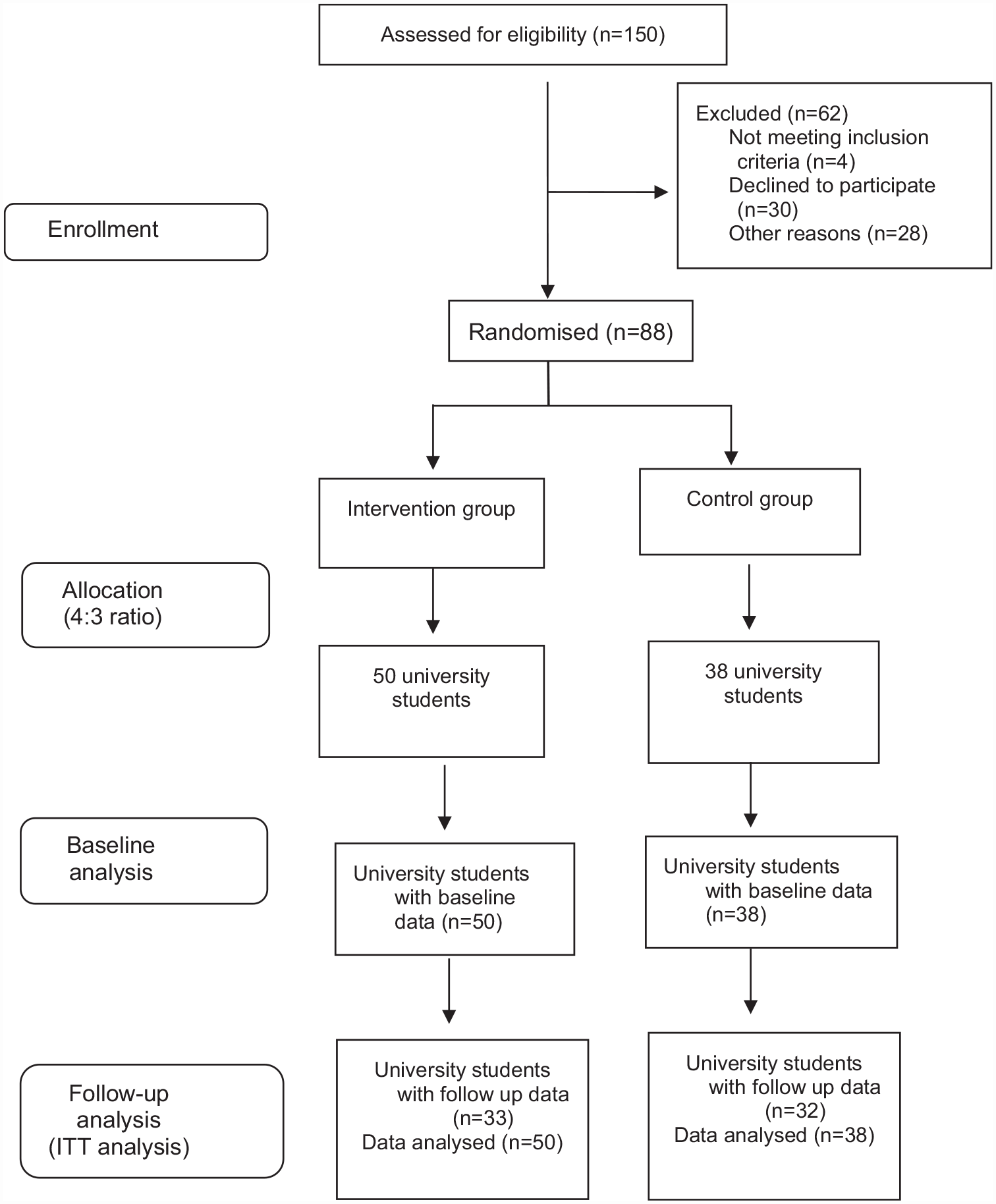
CONSORT flow diagram for the randomised controlled trial.
Intervention
The intervention included access to a website which contained information about the following topics: Activity and Exercise, Alcohol, Body weight, Eating on a budget, Fast-food, Fat, Food labels, Fruit and Vegetables, Meals and Snacks, Meat, Salt, Sugars and Sugary Drinks. Ten quiz-games relevant to the website content (one quiz for each topic except for Body weight and Eating on a Budget topics) were also included (Belogianni et al., 2019). Each quiz-game included 10 multiple-choice questions with a range of two to four answer options with only one correct response (see online Supplemental Table). The Kahoot! game-based learning platform was used to develop the online quiz-games (Dellos, 2015).
Gamification theory was informed the design of the intervention (Kapp, 2012), as the quizzes included the following game-elements: time – students had 30 seconds to answer each question; reward – students received points which increased their score when choosing the right answer; feedback – right and wrong answers appeared at the end of the quiz-game; social interaction – students could compete with each other when playing the same game (invited by the same host); and replay – students could repeat the quiz-game to improve their scores. Students were encouraged to play as many times as they wished to improve their knowledge and scores, as well as use the website as a reference tool to look for the correct answers. Music, videos and animated pictures were added to make the games more entertaining and engaging. Any electronic device was able to host the quizzes, and HTML iframes were used to pinch the quizzes to the website for easy access. Customised usernames and passwords were provided to students to access and play the games.
Prior to the study, the quiz-games were piloted with a class of undergraduate students to assess their feasibility. Electronic messages were sent twice per month to encourage students to play and improve their scores.
Outcome measures
Nutrition knowledge was assessed using the revised validated General Nutrition Knowledge Questionnaire (GNKQ-R) (Kliemann et al., 2016). The GNKQ-R tool includes questions in relation to dietary recommendations, food groups, healthy food choices, diet, disease and weight associations, and overall nutrition knowledge score ranging from 0 to 88. Each correct answer accounts for one point (otherwise null) and a higher score indicates higher nutrition knowledge.
Diet quality was assessed using a validated semi-quantitative food frequency questionnaire (FFQ) which calculates an index of diet quality (IDQ) (Leppälä et al., 2010). The FFQ includes 18 questions about frequency and amount of intake of whole grain products, fat-containing foods, dairy products, vegetables and fruits, sugary foods, and number of main meals skipped during the week. The IDQ score ranges from 0 to 15 points, with a higher score indicating higher diet quality.
Physical activity was assessed using the short form of the validated International Physical Activity Questionnaire (IPAQ-SF) (Craig et al., 2003). The IPAQ-SF includes questions about the frequency (days per week) and duration (minutes per day) of different types of activities (vigorous, moderate, walking) as well as sitting time (minutes per day). Physical activity was measured as total metabolic equivalent task (MET-minutes per week) from all types of activities (vigorous, moderate, walking).
Demographic and academic characteristics, including age, gender, ethnicity, study status (undergraduate/postgraduate), Faculty of study, being on a special diet (e.g. yes/no and type of diet if answered ‘yes’) and holding a nutrition qualification (yes/no and specific qualification if answered ‘yes’), were collected at baseline. Body mass (kg) and stature (m) were also measured by the principal investigator and BMI (kg/m2) was calculated at baseline.
Engagement with the quiz-games
Engagement was based on the frequency of playing the quiz-games (n). As the total number of quiz-games was 10, participants who played at least five quiz-games were considered adherent to the intervention. Because students were given the choice to play (or not) any quiz-game as many times as they wished, n (times playing) was calculated by adding the total number of quiz-games played, irrespective of whether it was the same or a different quiz-game.
Statistical analyses
IBM SPSS Statistics version 24 was used for the analysis of the data (IBM Corp, 2016). The significance level was set at p < .05. Descriptive statistics were used to describe the main characteristics of the study population and chi-square tests (or the Fisher’s exact test) and t-tests were performed to explore whether the two groups differed significantly on key variables at baseline. Descriptive statistics were also used to calculate the number of participants who played each quiz-game, the number of times each quiz-game was played, and the mean scores (% of correct answers) of each quiz-game. A receiver operating characteristic (ROC) analysis was undertaken to estimate the cut-off point (time in days) where the differences in scores ceased to improve for participants who played a quiz-game twice. The normality of variables were tested using the Kolmogorov–Smirnov test. The Mann–Whitney test was used to test for differences in outcomes between the two groups over time, and the Wilcoxon signed rank test was used to test for differences in outcomes within each group over time, using an intention to treat analysis. A mixed-design two-way repeated-measures analysis of variance (ANOVA) using a per protocol analysis was applied to investigate the effect of engagement rate with the quiz-games on the outcomes of measure over time.
Results
At baseline, participants of the two groups of the study did not significantly differ by age, gender, ethnicity, study status, faculty of study, BMI and following a special diet (Table 1). However, a higher number of participants holding a nutrition qualification was assigned to the control group (p = .033). Nutrition knowledge (p = .861), diet quality (p = .958), physical activity (p = .667) and sitting time (p = .237) also did not significantly differ between the two groups at baseline.
Baseline demographic, academic and anthropometric characteristics of study participants.
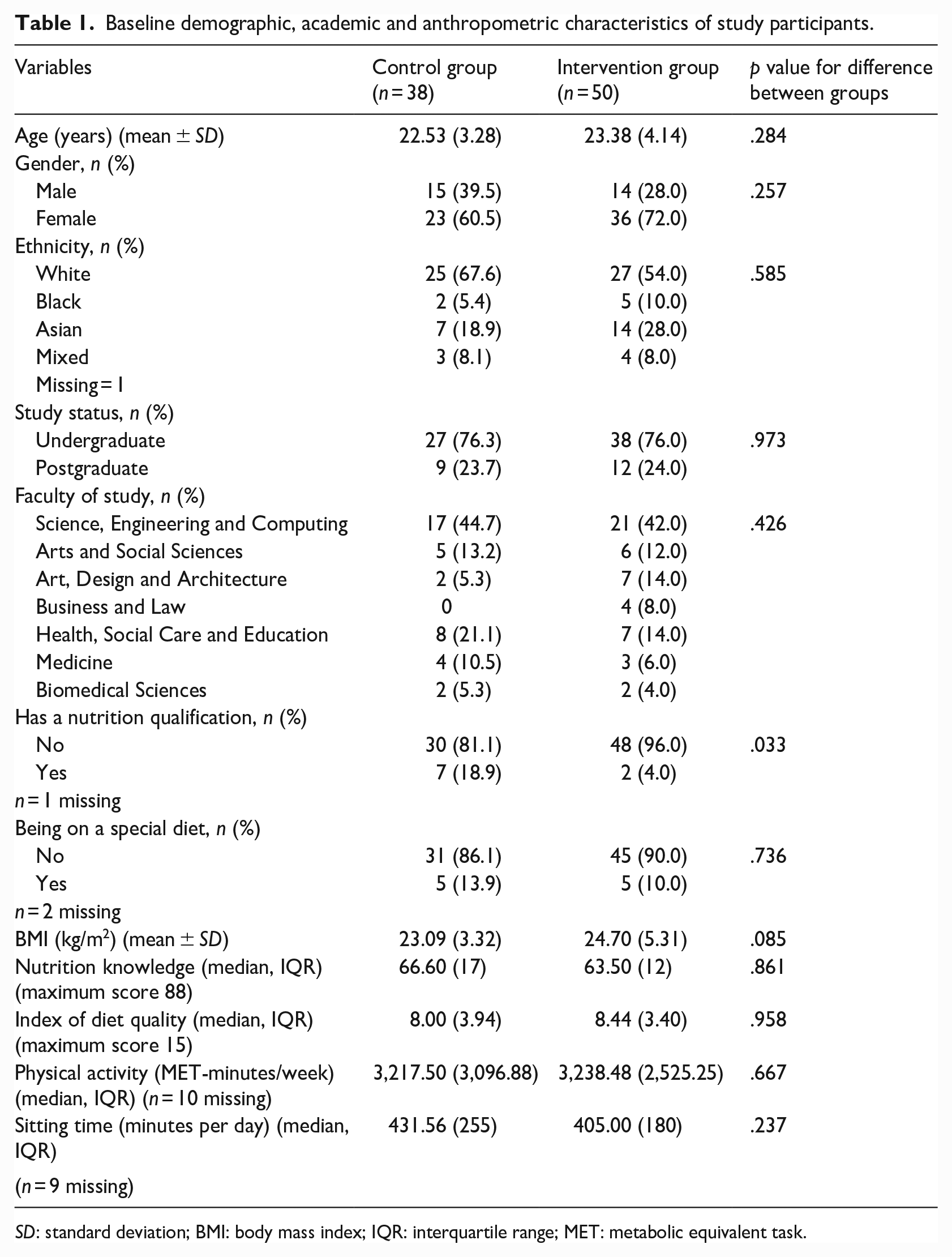
SD: standard deviation; BMI: body mass index; IQR: interquartile range; MET: metabolic equivalent task.
Of the 50 participants in the intervention group, 15 did not play any game and 35 were engaged to some extent with the quiz-games. On average, students played 6 out of 10 games with the Activity quiz-game being played by almost all students (n = 34) (Figure 2). Fast-food and Alcohol quiz-games were also played by a high number of students (n = 24), while Food labels and Salt quiz-games were played by the lowest number of participants (n = 16). Among the 35 game-players, 15 played at least one quiz-game. Activity was the most frequently played quiz-game being played 43 times in contrast with Food labels and Fruit and Vegetables quiz-games, which were only played 17 times each (Figure 2). The mean scores (as measured by % of correct answers) of the quiz-games ranged from 82% (Meals and Snacks) to 55% (Salt) (Figure 2). In total, 35 quiz-games were played twice, 6 quiz-games were played three times, one quiz-game was played four times and one quiz-game was played five times.
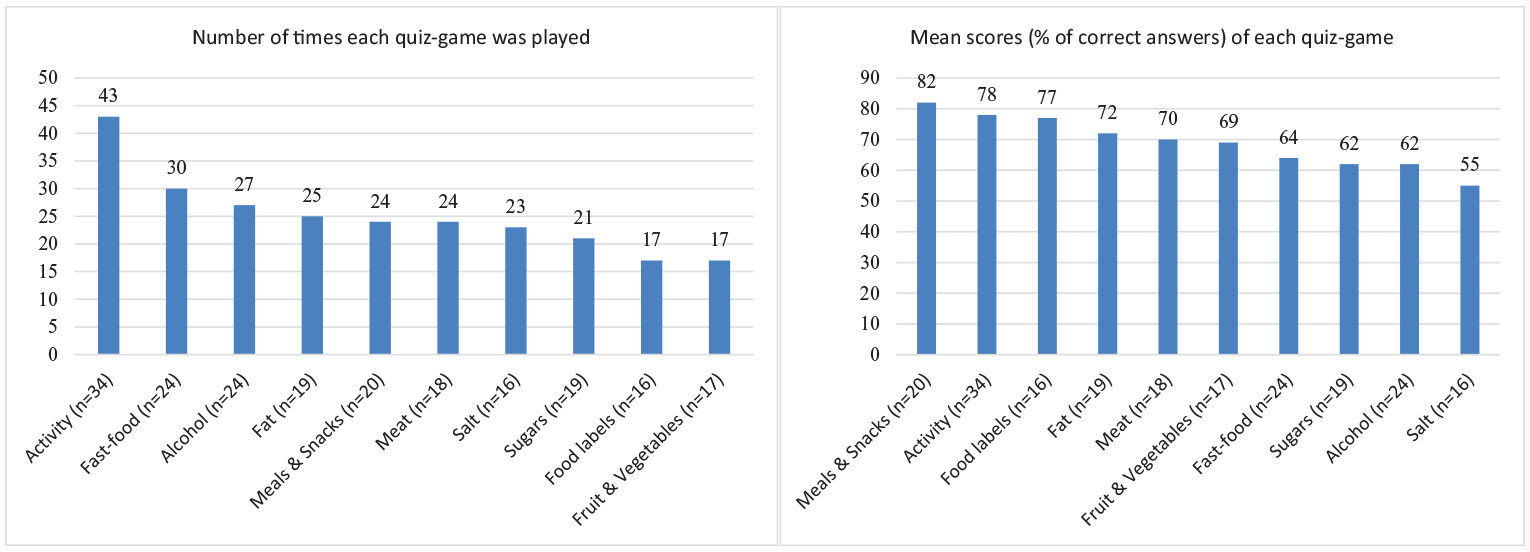
Number of times each quiz-game was played and mean scores (% of correct answers) on each quiz-game for participants in the intervention group who played each game (n).
Only the quiz-games which were played twice were used in the ROC analysis due to the low number of quiz-games played more than twice. The change in scores (score at second time minus score at first time) was converted into a new binary variable. When the second score was higher, the variable was coded as ‘positive’. When the second score was lower or remained the same, the variable was coded as ‘negative’. Based on this coding scheme, 18 students had a ‘negative’ change in scores, and their average number of days before repeating the quiz-game was 21.2 (SD = 21.3) while 17 students had a ‘positive’ change in scores, and their average number of days before repeating the quiz-game was 5.9 (SD = 9.3). The ROC curve analysis showed that 8 days was the cut-off point with the higher true positive rate (0.67) and lower false positive rate (0.29) (Figure 3), meaning that when participants played a quiz-game for the second time within 8 days, their performance (score) improved, while after that point, their performance remained the same or decreased.
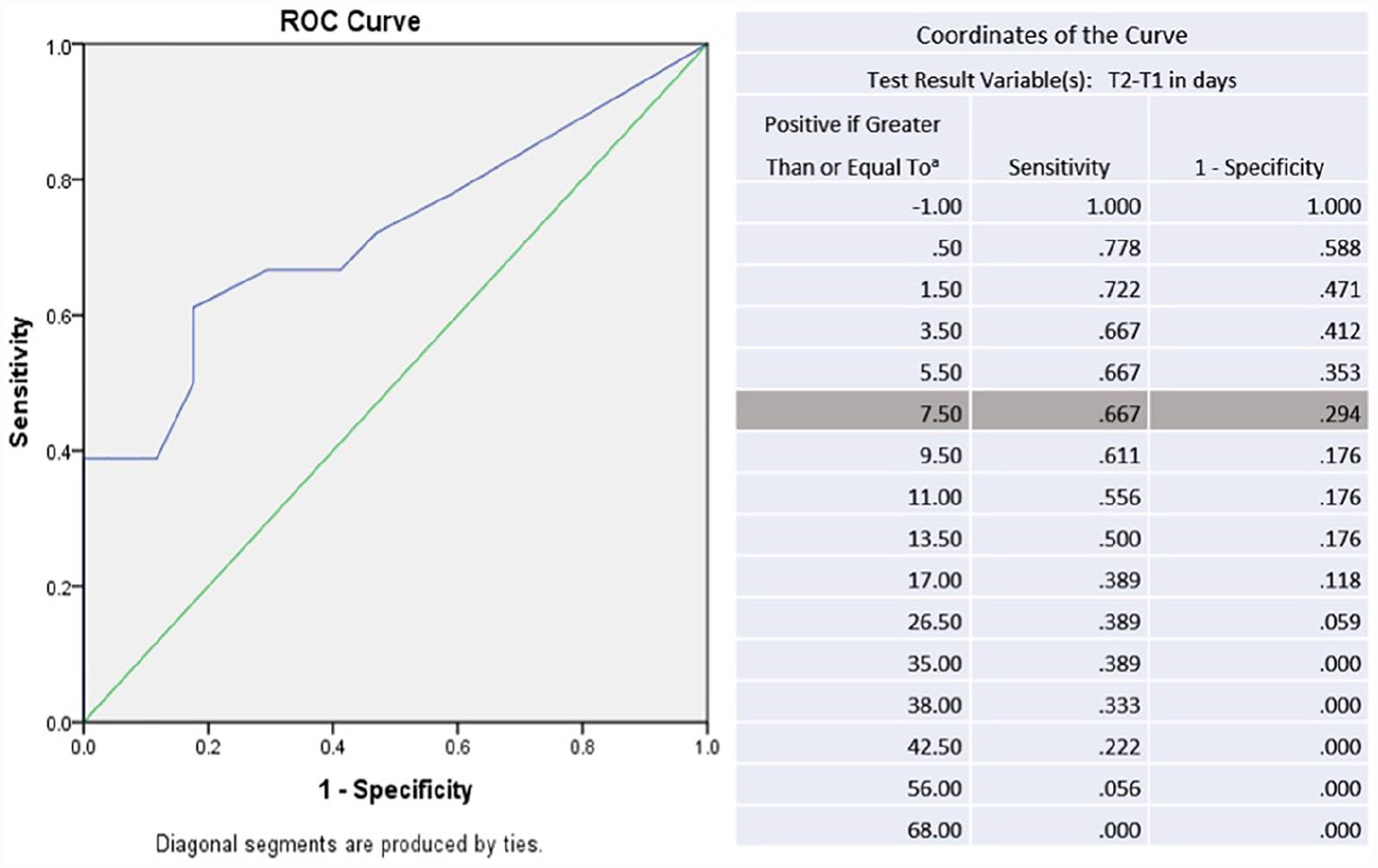
ROC curve used to estimate the cut-off point for the number of days where it was expected that when a player repeated the quiz-game, the score would remain the same or decrease. A cut-off point of 8 days seems to have the optimal sensitivity and one-specificity in this test.
No significant differences were found between the intervention and the control group over time on any of the outcomes of measure (Table 2). At the end of the intervention, students of both groups had significantly improved their nutrition knowledge compared to baseline (Table 2).
Comparison of nutrition knowledge, diet quality and physical activity outcomes of participants in the control and intervention groups over the study period.
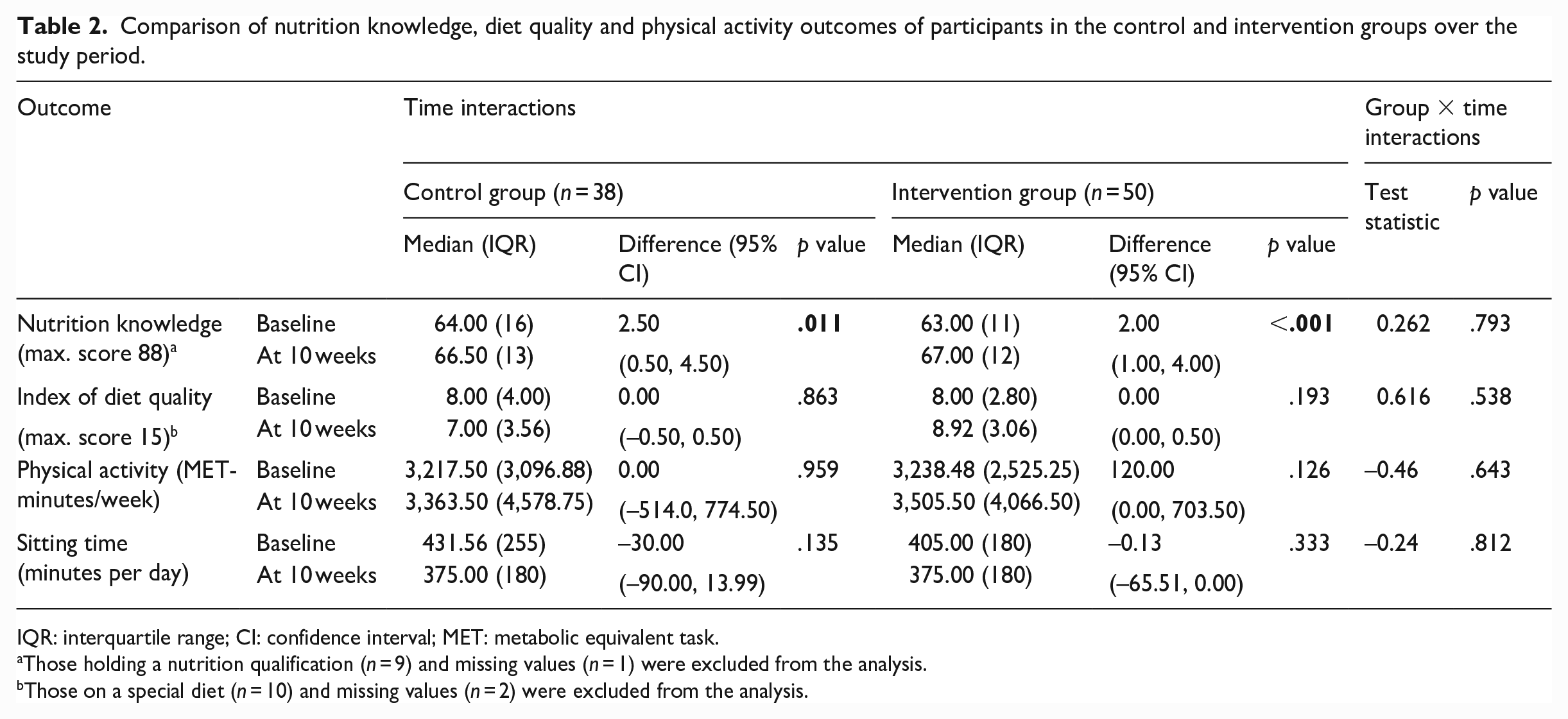
IQR: interquartile range; CI: confidence interval; MET: metabolic equivalent task.
Those holding a nutrition qualification (n = 9) and missing values (n = 1) were excluded from the analysis.
Those on a special diet (n = 10) and missing values (n = 2) were excluded from the analysis.
The engagement rate of the quiz-games had no effect on any of the outcomes of measure as no significant differences were found at the end of the intervention in nutrition knowledge, diet quality, physical activity and sitting time among adherent participants in the intervention group compared with those in the control group (Table 3).
The effect of engagement with the quiz-games on nutrition knowledge, diet quality, physical activity and sitting time over the study period. a
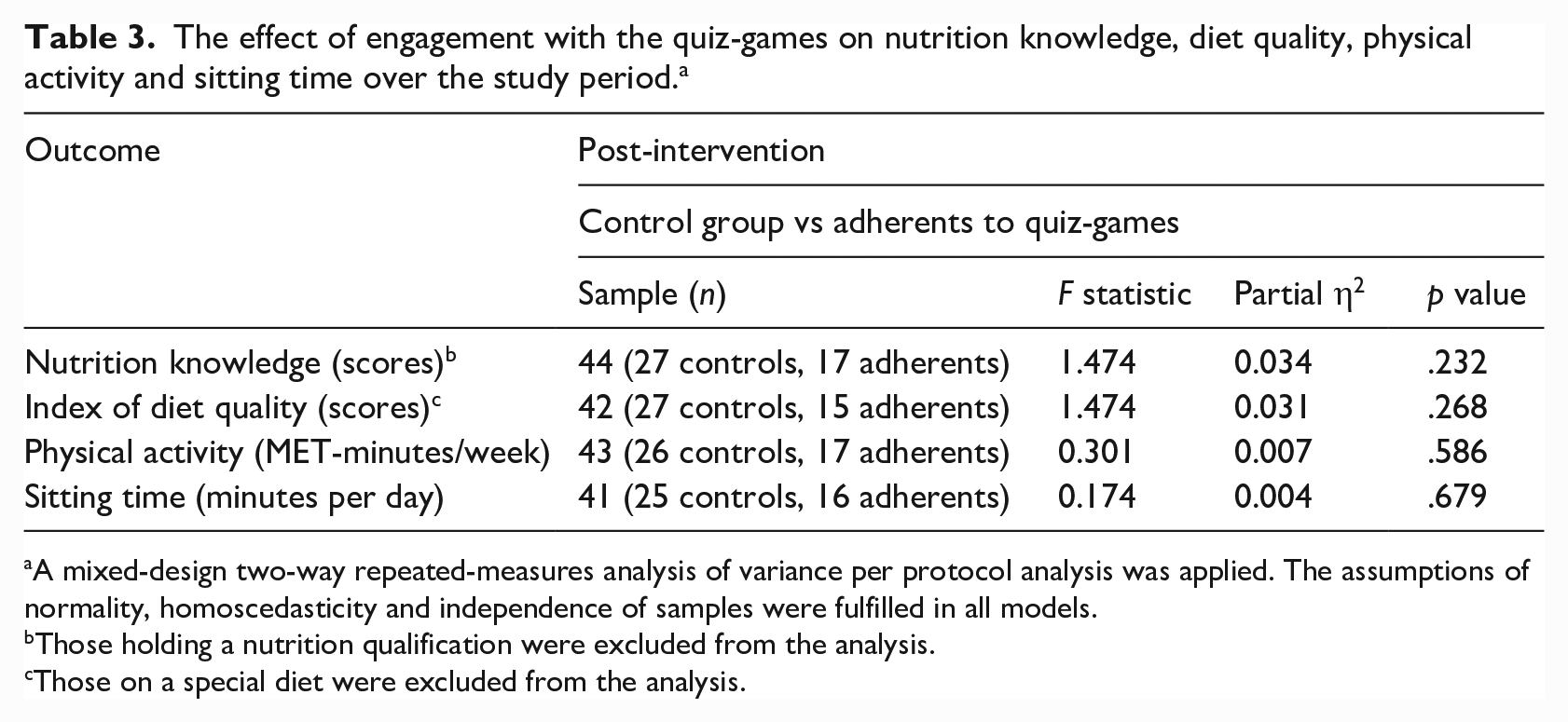
A mixed-design two-way repeated-measures analysis of variance per protocol analysis was applied. The assumptions of normality, homoscedasticity and independence of samples were fulfilled in all models.
Those holding a nutrition qualification were excluded from the analysis.
Those on a special diet were excluded from the analysis.
Discussion
The current study found no significant impact of the online quiz-games on nutrition knowledge, diet quality and physical activity between the two groups of the study over time. There was no statistically significant difference in the outcomes between the two groups of the study even when engagement rates with the quiz-games were considered. Similar digital interventions in non-clinical populations targeting both physical activity and dietary outcomes have shown small positive effects; however, digital interventions targeting diet or exercise alone have been found to be ineffective in a pooled analysis of 92 reviews including 42 meta-analyses (Gold et al., 2021).
With regard to study population, the RCT by Greene et al. (2012) that used a structured online intervention to improve FVI and physical activity among US university students found a small but significant increase in daily FVI intake at follow-up; however, no improvements were found in physical activity. The findings by Greene et al. (2012) are in line with those of an RCT conducted among Chinese students who also received a structured web-based intervention targeting FVI and physical activity with significant improvements in FVI only (Duan et al., 2017) suggesting that the structured and focused design of the interventions may have facilitated the positive dietary outcomes. The same study also found that the baseline stage of behavioural change, motivational indicators and social support played a significant role in actual behaviour change. This is consistent with findings from an intervention among Japanese university students using online quizzes to increase physical activity where only students inactive at baseline significantly increased their physical activity at the end of the intervention and follow-up period (Okazaki et al., 2014). In the current UK-based study, students from both groups did not have very low scores of nutrition knowledge, diet quality and physical activity at baseline. As a result, ceiling effects may have influenced the effect of the intervention on study outcomes.
Among the 50 students in the intervention group, 15 did not play any game and only 35 students played at least one quiz-game. When comparing the frequency of playing a quiz-game with the performance of the same quiz-game (Figure 2), one can assume that increasing knowledge to collect points was the main motive of students as the most frequent played games (e.g. Activity) had high performance and vice versa (e.g. Salt). As a result, the quiz-games seemed to have promoted surface learning in this study. Surface learning is characterised by accepting new information without processing them as opposed to deep learning which is characterised by critical thinking of the acquired knowledge, connecting to previous knowledge and integration of knowledge into real life (Biggs and Tang, 2011; Ramsden, 1992). The speculation that students memorised the information for a short period of time without processing the learning material in depth is also confirmed by the ROC analysis and the fact that scores decreased when repeating a quiz-game after 8 days. These outcomes are in line with other studies that have used the same platform (Kahoot!) to enhance learning of university students (Felszeghy et al., 2019; Neureiter et al., 2020). The studies found positive changes in the learning outcomes and students reported positive experiences with the platform, indicating the potential to use game-based quizzes as an auxiliary tool to recall a high amount of information in the short term. However, none of the studies assessed the learning outcomes in the long-term or whether and how students used the gained knowledge in practice.
Motivation may also impact adherence to the intervention. Despite evidence suggesting a positive correlation between adherence to digital interventions and improved weight-related outcomes (Donkin et al., 2011), many studies fail to report adherence data (Gold et al., 2021). In this study, adherence was estimated by measuring the number of times games played, with those playing at least five games considered as adherents. However, exposure to the website was not measured and adherence may have been underestimated as students who did not play any game could still have increased their knowledge by visiting the website. In addition, none of the students made use of the social feature of competing with each other, and all chose to play the quiz-games individually. Competition is important to keep motivation and engagement high with many studies arguing that gamification contexts need to be enhanced with game-design elements and tailored characteristics to increase their effectiveness (Chan et al., 2019). Moreover, the voluntary nature of the intervention and the fact that students who did not play any game still received the financial compensation at the end of the study may also explain the low engagement rates with the quiz-games.
The short duration of the intervention and the lack of follow-up assessment are other study limitations as participants may have needed more time to engage with the intervention and process the given information before a measurable impact presents itself. The intention to treat analysis approach used in this study tends to de-emphasise the magnitude of the intervention on outcomes, and the use of self-reported questionnaires may have decreased the accuracy of the collected data. Despite the small sample size, an effort was made to recruit participants throughout the academic year to consider seasonal factors that have been found to affect weight-related behaviours of students (Deliens et al., 2014, 2015; Small et al., 2013). Finally, although positive associations have been found between knowledge and dietary changes (Spronk et al., 2014), dietary, physical activity and sedentary behaviour in university students is affected by a cluster of factors not considered in this study (e.g. social, financial and environmental) (Deliens et al., 2014, 2015) and therefore, multicomponent interventions may be more appropriate to achieve substantial lifestyle behaviour changes in this population (Belogianni and Baldwin, 2019).
Conclusion
Online quiz-games seem to be well-accepted and easy to implement in student populations; however, they may not be sufficient to provide robust changes in knowledge and weight-related behavioural outcomes. Therefore, further investigation is needed to identify the specific gamification features that have the potential to promote dietary and physical activity outcomes. Researchers should further evaluate students’ motivation to change their lifestyle behaviours as well as their motivation to engage with the games to get a better understanding of the characteristics of successful game-based interventions. Adding social and interactive activities (e.g. cooking classes, workshops), adjusting the university environment (e.g. by enhancing the availability of healthy foods in cafeterias and improving access to gyms) and using game-based learning with social features may be key elements in successful interventions to improve knowledge and promote healthy weight-related behaviours among university students.
Supplemental Material
sj-docx-1-hej-10.1177_00178969231179032 – Supplemental material for An online game-based intervention using quizzes to improve nutrition and physical activity outcomes among university students
Supplemental material, sj-docx-1-hej-10.1177_00178969231179032 for An online game-based intervention using quizzes to improve nutrition and physical activity outcomes among university students by Katerina Belogianni, Ann Ooms, Anastasia Lykou, Dimitra Nikoletou and Hannah Jayne Moir in Health Education Journal
Footnotes
Acknowledgements
The authors thank students and staff at the two universities involved in the study as well as the Kahoot! Support team.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: H.J.M. is a senior medical writer with EMJ, London, UK.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: K.B. received a studentship by Kingston University to pursue a doctorate associated with this study; however, no external funding was received for the research itself.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.