
Abstract
Objective:
Latino day labourers (LDLs) in the USA are at increased risk for non-fatal and fatal occupational injuries, which are compounded by stressors that include wage theft, job insecurity and discrimination. This paper describes the development and refinement of Vales+Tú (You are Worthy of More), an injury prevention programme currently being evaluated as part of a cluster randomised trial in which health promotion is taken directly to the ‘corners’ (e.g. street corners, home improvement store parking lots, and public parks) where workers gather to seek employment.
Design:
Vales+Tú comprises two corner-based intervention approaches, group problem-solving (small group discussions) and brief motivational interviewing (one-on-one dialogue), that aim to activate LDL agency to control their safety and that of their peers.
Setting:
Corners in Houston, Texas, where LDLs seek employment.
Method:
Intervention Mapping informed the refinement of Vales+Tú for the current trial. We provide a narrative review of the development process based on needs assessment and formative development activities (surveys, focus group discussions and pilot tests).
Results:
In addition to documenting the need for LDL injury prevention, with 20.2%–41.6% of Houston-based LDLs surveyed between 2013–2014 and 2019 reporting a severe work-related injury in the past year, we describe key facets of the Vales+Tú corner-based intervention approaches – including their theoretical basis and LDL-centred activities, as well as enhancements made informed by formative evaluation.
Conclusion:
The community-engaged development process of Vales+Tú resulted in two practical intervention approaches that can be adopted by worker centres and other organisations to promote LDL worker safety.
Introduction
In the USA, the majority of Latino day labourers (LDLs) are recently arrived immigrants who work in a variety of low-paying jobs, with many working in the broadly defined construction industry (Hill et al., 2019; Valenzuela et al., 2006). Within the construction sector, LDLs are over-represented in several high-risk occupational trade groups, including drywall installers (60%), roofers (52%), painters (50%) and labourers (43%) (Center for Construction Research and Training [CCRT], 2021). In addition to the higher injury risks associated with construction-related occupations, Latino workers in the USA experienced the highest occupational fatality rate (4.5 per 100,000 full-time equivalent [FTE]) in 2021 compared to other racial/ethnic groups and to the US all-worker occupational fatality rate (3.6 per 100,000 [FTE]) (Bureau of Labor Statistics [BLS], 2022).
Beyond the inherent occupational hazards associated with the nature of their work, LDLs are at increased risk for occupational injuries due to their informal work arrangements, immigration status, language barriers and lack of formal safety training (Burgel et al., 2015; Fernández-Esquer et al., 2021; Valenzuela et al., 2006). Several studies have also documented the negative impact of LDLs’ exploitative work conditions on their physical and mental health. Repeat exposure to everyday stressors such as wage theft, job insecurity, discrimination, lack of access to workers’ compensation and low wages have been found to be significantly associated with increased LDL alcohol consumption, psychological distress and physical injury (Fernández-Esquer et al., 2021; Hill et al., 2019; Negi, 2013). Given their compounding occupational, economic and psychosocial risks, culturally tailored interventions targeted to their working conditions are urgently needed to address LDL occupational health disparities.
To assist LDLs in reducing their risk for workplace injury and related adverse health outcomes, a community partnership among LDL advocates, university researchers and community-based organisations in Harris County, Texas, was established to create Vales+Tú (You are Worthy of More). Initially developed and pilot tested in 2015 (Fernández-Esquer et al., 2022), Vales+Tú aims to promote LDL health and safety and reduce workplace injury via an explicit focus on LDL agency and empowerment. Given the daily structural barriers and stressors that confront LDL health and safety described above, the lack of compliance by some employers to Occupational Safety and Health Administration (OSHA) requirements and the constant rotation by LDLs among various employers and job settings, Vales+Tú places intentional emphasis on valuing the LDL lived experience and harnessing and activating LDL agency to protect and advocate for their own health and the health of their peers, recognising the ever-shifting job context that makes targeting any one employer a challenge. In fostering LDL agency and collective efficacy for worker safety, the programme centres on community health worker-led groups and one-on-one approaches that bring health promotion directly to the public spaces, or ‘corners’ (e.g. street corners, parking lots of home improvement stores and public parks) where workers gather to seek employment in jobs that include construction, landscaping, painting and other manual labour jobs.
In continuing to co-learn about best approaches for Vales+Tú’s corner-based approach for activating LDL agency for injury prevention, the programme recently underwent further refinement for a large-scale cluster randomised controlled trial that is currently under way. The purpose of this paper was to describe the development and refinement of Vales+Tú as guided by Intervention Mapping, a widely used systematic health promotion programme planning framework that incorporates theory, evidence and community input throughout the planning process (Bartholomew-Eldredge et al., 2016). In describing the development process of Vales+Tú, we provide a narrative review of our previous needs assessments and pilot testing as well as refinements to the programme based on recent formative research.
Methods
The development of Vales+Tú took place over two primary phases: (1) a pilot testing phase in 2015 (Fernández-Esquer et al., 2022), and (2) a cluster randomised controlled trial phase (2018–2023). We used Intervention Mapping to organise and report our previous needs assessments efforts and pilot testing of Vales+Tú, and then to further refine and enhance the programme for the current trial. Intervention Mapping provides a robust framework for health promotion planning in relation to the at-risk population and environment and has been applied across a variety of health topics, populations and settings (Bartholomew-Eldredge et al., 2016).
In describing our development and refinement process of Vales+Tú, we report on Intervention Mapping Steps 1–4, which consist of conducting a needs assessment and developing a logic model of the problem (Step 1), stating programme outcomes and objectives (Step 2), designing the programme (Step 3) and producing the programme (Step 4) (Bartholomew-Eldredge et al., 2016). Steps 5 (preparing the implementation plan) and Step 6 (developing the evaluation plan) are beyond the scope of this paper. The basis for our narrative description of the Vales+Tú development and refinement process consists of a review of findings from (1) needs assessments on risk factors for occupational injury conducted in 2008, 2013–2014 and 2019, which included interviewer-administered surveys with LDLs and corner-based observations; (2) a comprehensive pilot test (#1) of Vales+Tú that assessed the feasibility and acceptability of the intervention based on interviewer-administered surveys conducted in 2015; and (3) formative refinement activities to further enhance Vales+Tú for a current large-scale community trial (2018–2023) that included two participatory inquiry workshops with members from a community advisory board (CAB) (a community-facilitated logic model session to review and enhance the intervention logic model, and role-playing activity to collectively review and enhance the Vales+Tú intervention strategies); and a second corner-based pilot test (#2) conducted in 2020 that focused on assessing aspects of the delivery of intervention activities (e.g. flow, timing and content of activities based on field staff input) with LDLs in preparation for the cluster randomised trial.
Figure 1 presents a summary of the different research phases and activities that informed the development and refinement of Vales+Tú, including the study designs, study populations and methods (for further detail, see Fernández-Esquer et al., 2015, 2019a, 2019b, 2021, 2022). In addition to our primary studies, we also cite the empirical literature and describe below the theoretical foundations that guided our approach and development process. These activities align with the Intervention Mapping Core Processes for intervention planning (Bartholomew-Eldredge et al., 2016). Study aims and protocols for all previous and current Vales+Tú studies were reviewed and approved by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston (UTHealth) School of Public Health, with informed consent procedures that emphasised the voluntary and confidential nature of study participation, and the provision of gift card incentives (US$25–US$75) in recognition of participants’ time.
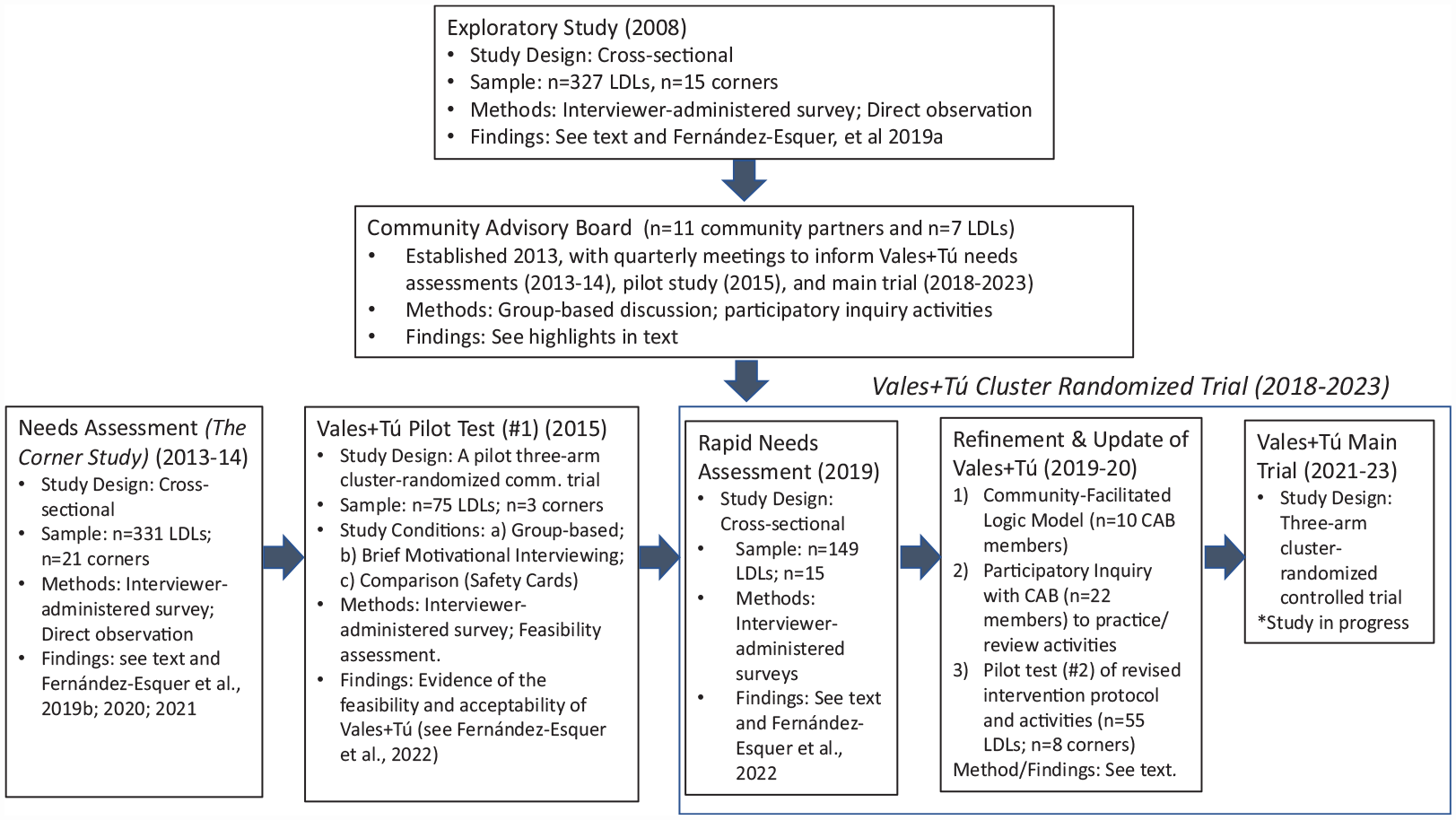
Needs assessment and formative development activities of Vales+Tú injury prevention programme.
Results
Vales+Tú overview
The Vales+Tú programme, originally developed and pilot tested in Houston, Texas, in 2015, pioneers two different behaviour change approaches adaptable to the corner conditions of day labour work: (1) a small group, participatory learning and action approach (‘Group Problem-Solving’ approach), and (2) a one-on-one, change talk process focused on the LDL own risk reduction priorities (‘Brief Motivational Interviewing’ approach) (Fernández-Esquer et al., 2022).
The group problem-solving (GPS) approach was informed by our team’s extensive corner observations (Fernández-Esquer et al., 2015, 2019a, 2019b, 2021), which revealed that small groups represent the natural organisation of LDLs who congregate in clusters of approximately four to seven workers as they wait to be hired at the corner. Small group activities have been found to facilitate discussions around a problem that a group can tackle and solve together (Martinez et al., 2014). Previous research suggests the approach can effectively disseminate safety knowledge and skills, while reinforcing safety peer norms (Forst et al., 2013).
The brief motivational interviewing (BMI) approach incorporates techniques commonly used in motivational interviewing to elicit change talk through the use of open-ended questions, reflections and summaries (Apodaca et al., 2016). Through change talk, the community health worker (alternatively known as promotor) encourages the LDLs to reflect on their own experiences, needs and priorities. The dialogue aims to identify personally relevant risk-reducing behaviour and safety strategies that the LDLs can use to replace or modify current practices.
Vales+Tú’s primary theoretical orientation is based on two complementary perspectives that emphasise agency and self-determination among individuals and groups. Bandura’s (2006) theory of human agency proposes that behaviour is the result of personal dispositions, psychological determinants and environmental factors. Freire’s (1973) approach to empowerment and collective action complements this perspective and holds that individuals and groups have the capacity to decide and implement skills needed to resolve problems that are important to them. In building from these theoretical foundations, Vales+Tú is based on the premise that structural and social conditions in the lives of LDLs amplify the dangers they confront at work and increase their risk for injury (Fernández-Esquer et al., 2019a); Vales+Tú aims to support LDLs in addressing these dangers. Importantly, Vales+Tú’s corner-based approach is context specific and incorporates a health promotion interweaving into settings and environments design approach by embedding health promotion within an everyday context familiar to the priority population (Springer et al., 2017).
Description of Vales+Tú intervention development
Below, we summarise our intervention development process for Vales+Tú as organised by Steps 1–4 of the Intervention Mapping planning framework.
Step 1: Assess needs and develop a logic model of the problem
CAB: Intervention Mapping. Step 1 consists of conducting a needs and asset assessment of the health topic, risk populations, community and context to develop a deep understanding of the behavioural, social, environmental and intrapersonal factors that contribute to the health problem, as informed by a logic model of the problem, or risk model (Bartholomew-Eldredge et al., 2016).
A first task of Step 1 involved establishing a planning group. Informed by a community-engaged research orientation that emphasises collaborative and equitable partnerships and co-learning in all research phases (Wallerstein et al., 2018), the Vales+Tú CAB was initially established in 2013 based on a partnership of LDL advocates, community health researchers at UTHealth School of Public Health and leaders from community-based organisations that included Fe & Justicia Workers Center, Living Hope Wheelchair Association, Familias Inmigrantes y Estudiantes en la Lucha (FIEL) and CRECEN Community in Action. The composition of the Vales+Tú CAB follows the linkage system concept, which consists of bringing together diverse perspectives within a resource group, potential implementers and priority population for health promotion planning (Bartholomew-Eldredge et al., 2016). After careful selection and screening, 27 local organisations and community experts were invited to serve on the CAB. Ultimately, 11 community partners remained in the CAB for the duration of the project, along with seven LDLs. For both the initial development of Vales+Tú programme and its later refinement, we engaged the Vales+Tú CAB in quarterly meetings to guide and provide feedback on the programme’s activities, and establish programme priorities for reducing injury and promoting LDL safety and health. CAB members voted on the priorities of the pilot programme and provided key input on the needs assessment approach, including identifying corners, selecting the name/logo of the programme, exploring LDL needs and prioritising the health outcomes to be targeted by the programme.
Needs assessment
The development of Vales+Tú was informed by three separate needs assessments of work-related injury among LDLs who seek work on the corners of the Houston Metropolitan area. These included an exploratory study conducted in 2008 of n = 327 LDLs based at n = 15 corners (Fernández-Esquer et al., 2019a), a more expansive needs assessment conducted between November 2013 and July 2014 of n = 331 LDLs from n = 21 corners (Fernández-Esquer et al., 2019b, 2020, 2021), and a rapid needs assessment conducted in 2019 of n = 149 LDLs based at n = 15 corners aimed at assessing current experiences of injury among LDLs and pilot testing measures developed for the community trial of Vales+Tú (Fernández-Esquer et al., 2022). Methods for these assessments align with the Intervention Mapping core processes (Bartholomew-Eldredge et al., 2016) and included the following: question posing about the problem (e.g. What is the extent of work-related injury among LDLs? What are the most common types of work-related injury? What are the behaviours, determinants and environmental factors that contribute to work-related injury?); exploring with the CAB the barriers and facilitating factors for LDL health and quality of life; conducting reviews of the empirical literature and theory; and collecting primary data through surveys, interviews and focus groups with LDLs. Below, we share selected Vales+Tú needs assessment findings and present our initial risk model or logic model of the problem.
The health problem: work-related injury
In building from a growing literature base on the magnitude of work-related injury for Latino workers (Burgel et al., 2015; CCRT, 2021; Centers for Disease Control and Prevention [CDC], 2008; Valenzuela et al., 2006), the Vales+Tú assessments aimed to describe the context of LDLs, the prevalence of work-related injury, and the factors that contribute to work-related injury and adverse health (Fernández-Esquer et al., 2019b, 2020, 2021). Key findings from the 2013–2014 assessment (n = 331 LDLs) indicated approximately one in five LDLs (20.2%) experienced a work-related injury in the past year, underscoring the high prevalence of injuries among this population (Fernández-Esquer et al., 2020). The most prevalent types of injury included injuries caused by falling (23.9%), moving heavy objects (21.6%) or being struck by an object (20.5%). Despite their high prevalence, LDL injuries were often not reported to anyone due to fear of being fired, with a high percentage of injuries (64.4%) resulting in missed workdays, temporary incapacitation (54.0%) and permanent incapacitation (34.5%) (Fernández-Esquer et al., 2020). The 2019 assessment (n = 149 LDLs) indicated 41.6% of LDLs reported a severe work-related injury in the past 12 months (Fernández-Esquer et al., 2022), underscoring the ongoing need for injury prevention approaches.
Risk context and risk factors for work-related injury
The three needs assessments, along with CAB input and review of the empirical literature, contributed to the identification of the contextual and environmental factors, risk behaviours and personal determinants associated with increased injury among LDLs. In understanding the context of work-related injury, our needs assessment findings indicated that situational stress, that is, frequency that LDLs experienced lack of food and money, job deprivation (e.g. unable to find work), employment trouble (e.g. wage theft, conflict with boss), interpersonal trouble (e.g. fights with family) and immigration-related stress (i.e. deportation-related worry, disappointment about life in the USA and fear of venturing out as an immigrant) had a detrimental effect on LDL mental health and workplace safety, resulting in increased risk of occupational injury (Fernández-Esquer et al., 2019a, 2021). Other environmental factors found to increase the risk of injury among LDLs include lack of safety training, inadequate safety equipment and wage theft (Burgel et al., 2015; Fernández-Esquer et al., 2021; Valenzuela et al., 2006). Based on a review of the literature, work-related risks that contribute to increased injury also include job inexperience, physical job demands, lack of personal protective equipment (PPE) and working long hours (Dong et al., 2015; Nakata, 2011). The needs assessments also established the feasibility of reaching LDLs on the corners. Finally, key intrapersonal factors posited to increase work-related injury included low self-efficacy and skills for work-related safety practices and worksite hazard identification; low knowledge about social support services; low perceived risk (susceptibility and severity) of worksite injury; low normative beliefs for safety behaviours; and low perceived social support.
Logic model of the problem
Based on the needs assessments, literature review and CAB input, a logic model of the problem was developed (otherwise known as ‘a risk model’), which provides a conceptual model of the individual-level factors (e.g. behaviours) and environmental conditions posited to influence LDL work-related injury and adverse mental health (Figure 2). With recognition of the environmental and social factors that may amplify hazardous conditions at work, the model is informed by structural, occupational and health inequalities associated with the worker at the worksite, including worksite exposures resulting in illness or injury (Adler and Snibbe, 2003; Quesada et al., 2011). A social ecological model of health behaviour (Sallis and Owen, 2015) guided the planning group to explore individual-level and environmental-level factors that lead to adverse health or social outcomes.
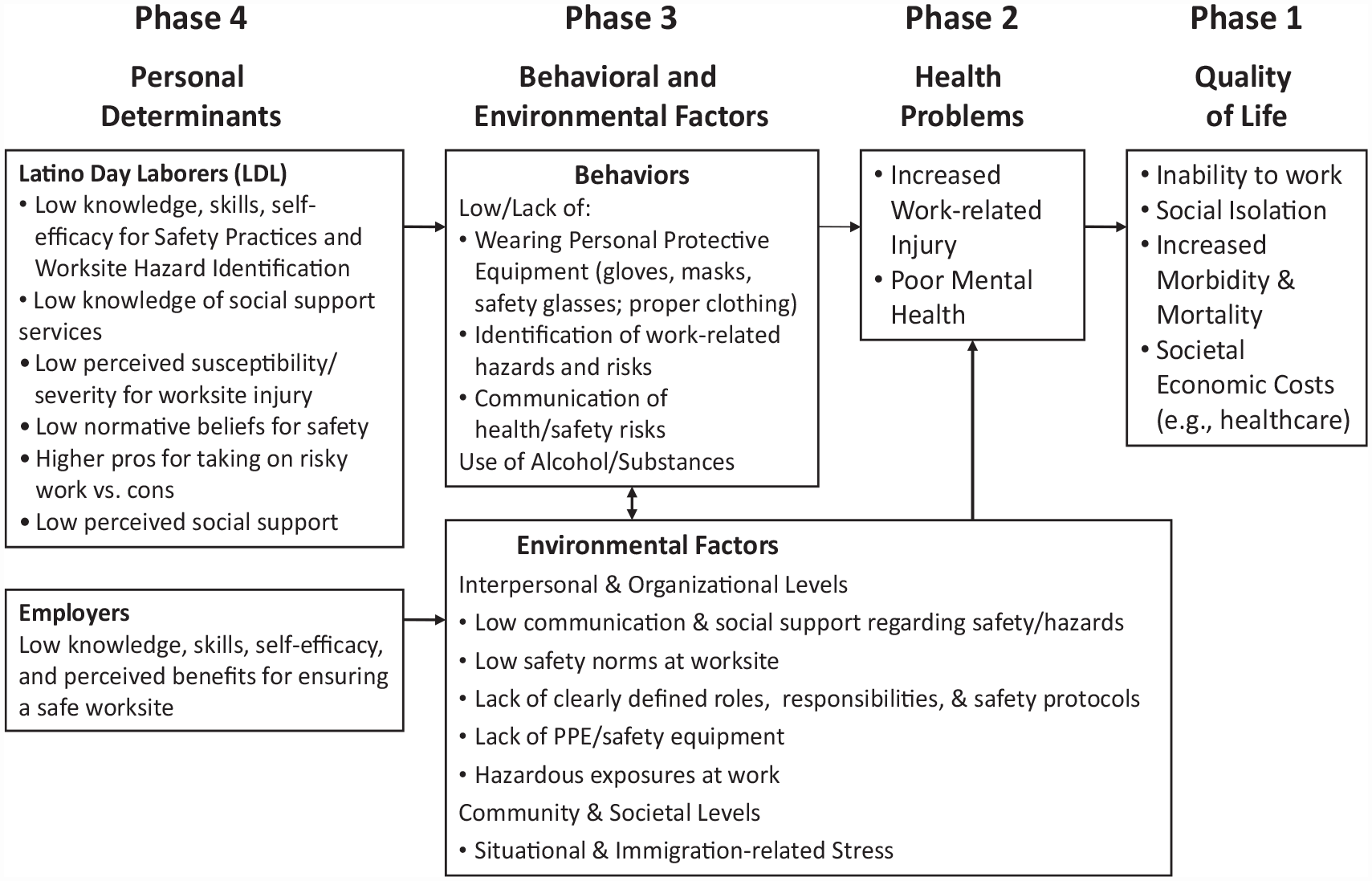
Logic model of the problem, Vales+Tú injury risk reduction programme.
Step 2: State programme outcomes and objectives and create initial logic model of change
In Intervention Mapping Step 2, we moved from the logic model of the problem to the creation of a logic model of change (otherwise known as the intervention logic model) aimed at reducing work-related injury and enhancing mental and psychosocial health among LDLs. Below we provide a summary of key content for our logic model of change; in Step 4, we share our full intervention logic model.
Behavioural and environmental outcomes
Building from the Vales+Tú pilot injury reduction programme that was developed with LDLs and pilot tested in 2015, in 2019, we engaged a subgroup of the CAB (n = 10 members) in a community-facilitated logic model session (Lien et al., 2011) to create the logic model of change for more formal testing of Vales+Tú for the current cluster randomised trial. Key targeted behavioural outcomes or practices to reduce various types of work-related injury based on our logic model of the problem included the following: wearing PPE (gloves, masks, safety glasses, proper clothing) (O’Connor et al., 2005), identification of work-related risks (Teran et al., 2015) and communication of work-related hazards (Hallowell and Yugar-Arias, 2016). Key social and environmental outcomes that may be influenced by the LDLs included the following: communication regarding safety with peers and supervisors and strengthening of peer safety norms (interpersonal level); reduction of hazardous exposures and conditions at work that lead to injury (organisational level); and enhancement of social support for LDLs for health and safety and making social services available (community level).
Performance objectives
Performance objectives are the specific actions (i.e. steps) an individual or group can follow to implement the identified risk reduction behaviours and/or health-promoting environmental conditions (Bartholomew-Eldredge et al., 2016). By law, employers are responsible for providing safe workplaces and complying with standard established by OSHA. Best practices for effective injury and illness prevention recognise the importance of worker involvement in safety programmes and practices (OSHA, 2016). A unique contribution of Vales+Tú centres on valuing, building and activating agency within LDLs to take control and action for their own safety and the safety of their peers. In developing this LDL-centred approach, a challenge that confronted our planning team was developing an approach that can promote LDL safety across the various types of jobs they perform. In addressing this challenge, performance objectives (Bartholomew-Eldredge et al., 2016) provided a framework for promoting risk reduction actions that can be applied across various types of work and settings. Similar to health communication campaigns such as Stop, Drop and Roll within the field of fire injury prevention (US Fire Administration (USFA), 2020), we aimed to create a simple mnemonic that encompasses key preventive actions aimed at increasing worker safety and reducing work-related hazards.
In developing the performance objectives, we conducted a thematic analysis of Mi Promesa based on the 2015 pilot study. Mi Promesa represents the promise or public commitment made by each LDL to increase their safety at work. Results from coding of the safety behaviours reported by LDLs found that these behaviours could be grouped within three overarching themes related to communication, planning and acting; in Spanish, comunicar, planear and actuar. We abbreviated these performance objectives as ‘ComPA’, meaning to communicate safety concerns and needs with peers and supervisors; plan to be safe before getting to the worksite and during job; and take action to promote safety, act cautiously and remove hazards. In addition to their foundation in best practices expressed by the LDLs, ComPA actions are consistent with OSHA recommendations for construction worker safety (OSHA, 2016). ComPA also aims to promote the theme of LDL unity and support, as ComPA is another way of saying compadre or compañero – a term used to indicate friendship in Spanish.
Personal determinants
Personal determinants are intrapersonal factors that aim to respond to the question of why an individual or group would implement the health-promoting or risk-reducing behaviour and targeted performance objectives (Bartholomew-Eldredge et al., 2016). With a primary theoretical foundation in health belief model (HBM) and theory of human agency/social cognitive theory (SCT), the specific determinants posited to influence risk reduction actions included perceived severity and susceptibility for work-related injury (HBM); knowledge about ways to prevent injury and reduce hazards at work (SCT); outcome expectations and perceived benefits for taking action to be safe at work (SCT/HBM); self-efficacy for taking action to be safe at work (HBM/SCT); perceived social support for being safe at work (SCT); normative beliefs among LDLs for safety at work (SCT); and behavioural intentions to take action to implement work-related safety practices (theory of planned behaviour).
Step 3: Design the programme
Intervention Mapping Step 3 consisted of designing the overall health promotion programme, which includes identifying and developing key programme themes and intervention activities that include change methods and practical applications for delivering methods. In designing Vales+Tú, our planning group developed two intervention approaches that could fit within the confines of the corner: a GPS approach, and a one-on-one, BMI approach. Below, we provide a summary of key themes integrated into both interventions, as well as the change methods and practical applications.
Themes
The overarching theme and title for the intervention, Vales+Tú, is a Spanish expression meaning you are worthy of more (Figure 3). This name was jointly developed by the research and corner outreach teams and selected based on input from LDLs and the CAB. The project name highlights the personal worth of each worker and the value of their safety and health. This personal worth is tied to their ability and individual agency to stay healthy for the benefit of their family, their co-workers or compañeros and their community. This theme also emphasises that LDLs are change agents to promote working conditions for themselves and their co-workers.

Vales+Tú logo.
Theoretical change methods and practical applications
Within the Intervention Mapping framework, a change method is defined as a general process for influencing changes in the determinants of the targeted health behaviour and environmental conditions; a practical application is a technique for operationalising the change method in ways that fit with the priority population and intervention context (Bartholomew-Eldredge et al., 2016). In Table 1, we provide a summary of the key theoretical change methods and practical applications for Vales+Tú, as organised by the GPS and BMI intervention approaches.
Theoretical change methods and practical applications, Vales+Tú worker safety intervention.
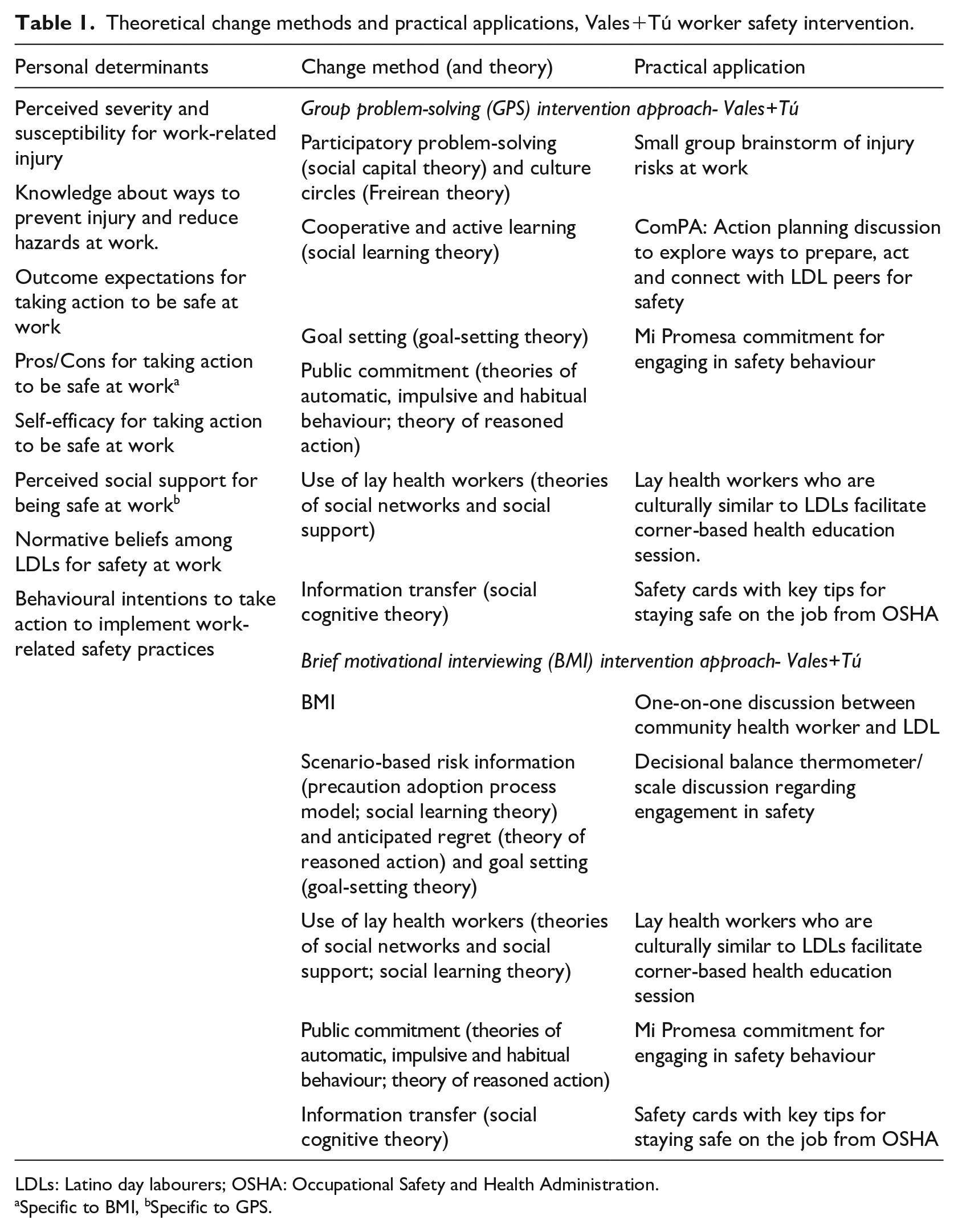
LDLs: Latino day labourers; OSHA: Occupational Safety and Health Administration.
Specific to BMI, bSpecific to GPS.
Key theoretical change methods of the GPS approach include participatory problem-solving (social capital theory), active and cooperative learning (SCT), goal setting (goal-setting theory) and culture circles (Freirean theory) – which together create a space in which to explore, value and build on existing knowledge of participants through critical dialogue to enhance learning and create meaning (Humphries, 2019). Practical applications for delivering these methods comprise small group discussions in which LDLs reflect on the risky work conditions that they routinely experience and brainstorm safety strategies that they can implement to mitigate their hazardous work environment. The group activity culminates with each individual developing an action plan (Mi Promesa) for prioritising worker safety and improving their quality of life as organised by the ComPA framework.
BMI integrates elements of motivational interviewing (Field et al., 2005, 2010) and was adapted to the culture, context and risk reduction needs of the local LDL population. BMI recognises that LDLs face a motivational conflict of accepting dangerous work or refusing work to maintain their safety. BMI consists of a one-on-one conversation with LDLs, led by a trained community health promoter, that allows an exchange of ideas to explore their personal risk dilemmas, engage in problem-solving to reduce risks and commit to specific actions consistent with maintaining their safety at work. In guiding the discussion, the BMI approach explores three stages of their workday during which the LDLs may be empowered to maximise their safety. The conversation focuses on decisional balancing, looking at the pros and cons of taking risks at work. The natural culmination of the BMI approach is the development of Mi Promesa in which the LDLs commit to use a risk reduction strategy during the workday. BMI is intended to enhance motivation for action through the development of discrepancy reduction while enhancing internal locus of control and self-efficacy through the process of creating implementation intentions.
Both approaches incorporate the information transfer change method via dissemination of safety cards developed by OSHA. They also culminate with the creation of a public commitment by each LDL of self-identified actions and goals to enhance their own and their peers’ safety and well-being, as delivered via the Mi Promesa activity (Table 1). Personal commitments have been shown to increase compliance with various health behaviours (Bartholomew-Eldredge et al., 2016). Both GPS and BMI intervention approaches are being delivered for the current trial in Spanish by lay community health workers who were extensively trained in popular education and motivational interviewing, respectively, and who are familiar with LDL culture and context.
Step 4: Produce the programme
Intervention Mapping Step 4 consisted of producing the programme, with key activities that include developing intervention materials and pre-testing and pilot testing the intervention prior to full implementation. In 2015, a three-arm cluster randomised community trial was conducted among 75 LDLs (n = 25 LDLs per condition) to pilot test the Vales+Tú GPS and BMI strategies in comparison with a standard of care control (OSHA safety cards), with interviewer-administered surveys conducted at baseline (in person) and at 2-week follow-up (by phone). Both strategies were led by lay community health workers (promotores) who were recruited from the LDL community and/or partner social service agencies, who spoke Spanish as their first language, and who participated in a full day of training (consisting of 8 hours), followed by approximately 30 hours of rehearsal practice to master the delivery of the Vales+Tú interventions.
The GPS condition consisted of a promoter-led discussion on the identification of potential dangers at work followed by work risk scenarios in which LDLs explored strategies to reduce or prevent worksite hazards and promote their health and safety, with emphasis on the importance of helping each other to stay safe. The BMI condition, also led by a promotor, included a decisional balance activity to explore the benefits and disadvantages of taking jobs with greater danger, followed by a discussion of the importance of reducing workplace dangers, and the development of an action plan to reduce workplace danger. Both GPS and BMI conditions, which lasted between 30 and 45 minutes, concluded with a public commitment activity (Mi Promesa) in which the LDL is invited to make a pledge on actions they will take to stay safe. The intervention approach was found to be both feasible (e.g. 40%–74% of LDLs who were approached expressed interest in participating in the intervention; 88% of participants were reached for post-test survey) and acceptable (90%–100% of participants rated their experience with the GPS and BMI activities as ‘good’ or ‘excellent’).
In refining the Vales+Tú intervention approaches for the current large-scale cluster randomised trial, we reviewed and updated health and safety resource materials from the 2015 pilot test (Fernández-Esquer et al., 2022) and implemented additional formative evaluation activities that included a participatory inquiry workshop with CAB members and our academic partners (n = 22) in early 2020, and a second abbreviated pilot test to test the delivery of the revised approaches with a sample of LDLs (n = 55) conducted in late autumn 2020. The participatory inquiry CAB workshop consisted of a mock implementation of the GPS and BMI approaches followed by critical reflection and discussion to identify further opportunities for improvement. Once refinements had been made, we piloted the GPS and BMI approaches with LDLs recruited from eight randomly selected corners to assess the flow, timing and overall delivery of the activities, with enhancements to the delivery of GPS and BMI made based on discussions with our field staff. Table 2 presents the resulting refinements and enhancements to the delivery of Vales+Tú GPS and BMI approaches.
Refinements and enhancements made to Vales+Tú worker safety intervention.
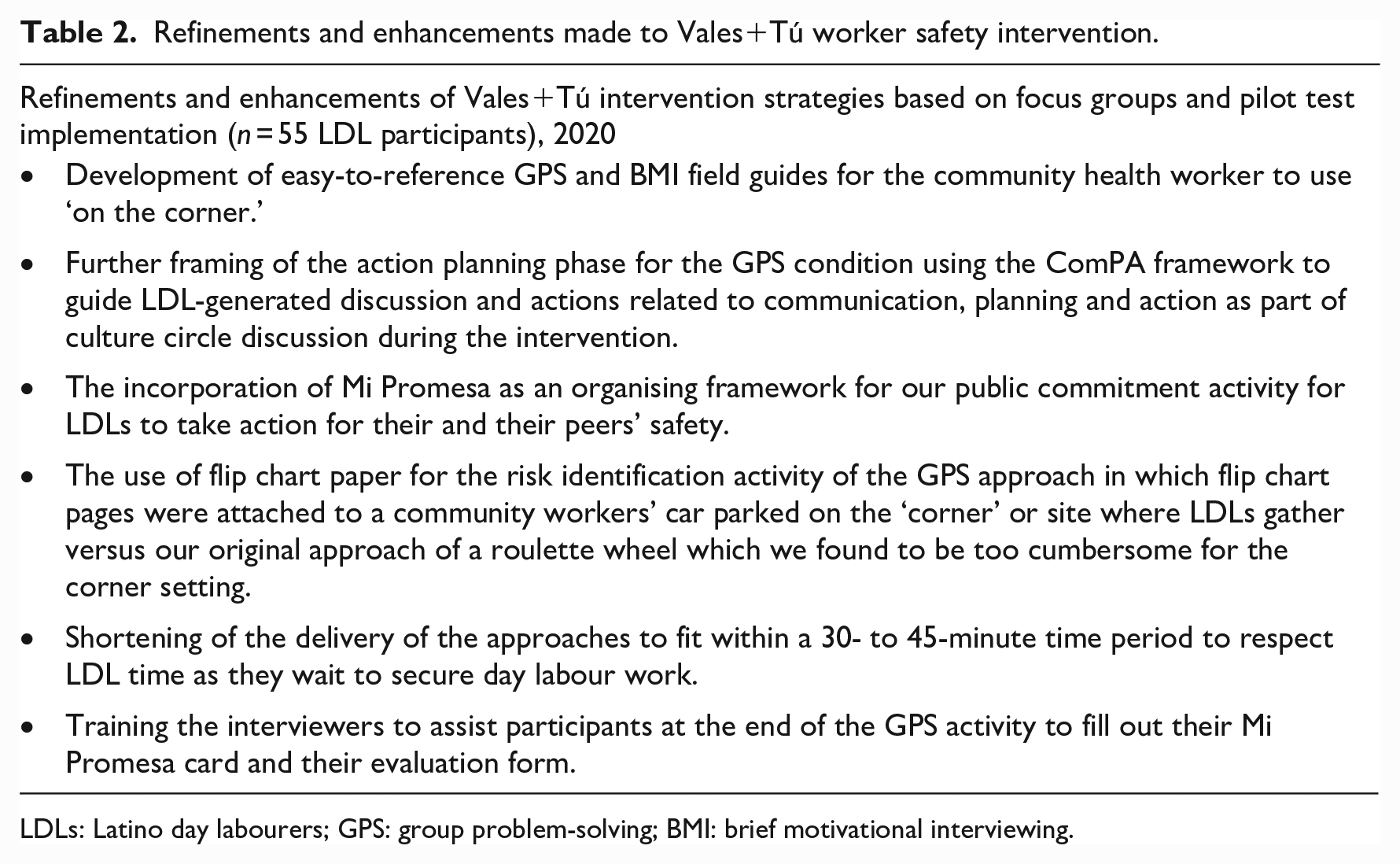
LDLs: Latino day labourers; GPS: group problem-solving; BMI: brief motivational interviewing.
Full intervention logic model
The final intervention logic model for Vales+Tú is presented in Figure 4. This logic model begins with an explicit focus on reducing hazards that lead to workplace injuries and adverse mental health conditions, including anxiety and depression, and increasing positive social cohesion among LDLs and their co-workers, job satisfaction and LDL empowerment. In promoting these outcomes, Vales+Tú includes the two corner-based, promoter-led approaches, GPS and BMI, that are currently being evaluated as part of a cluster randomised trial.
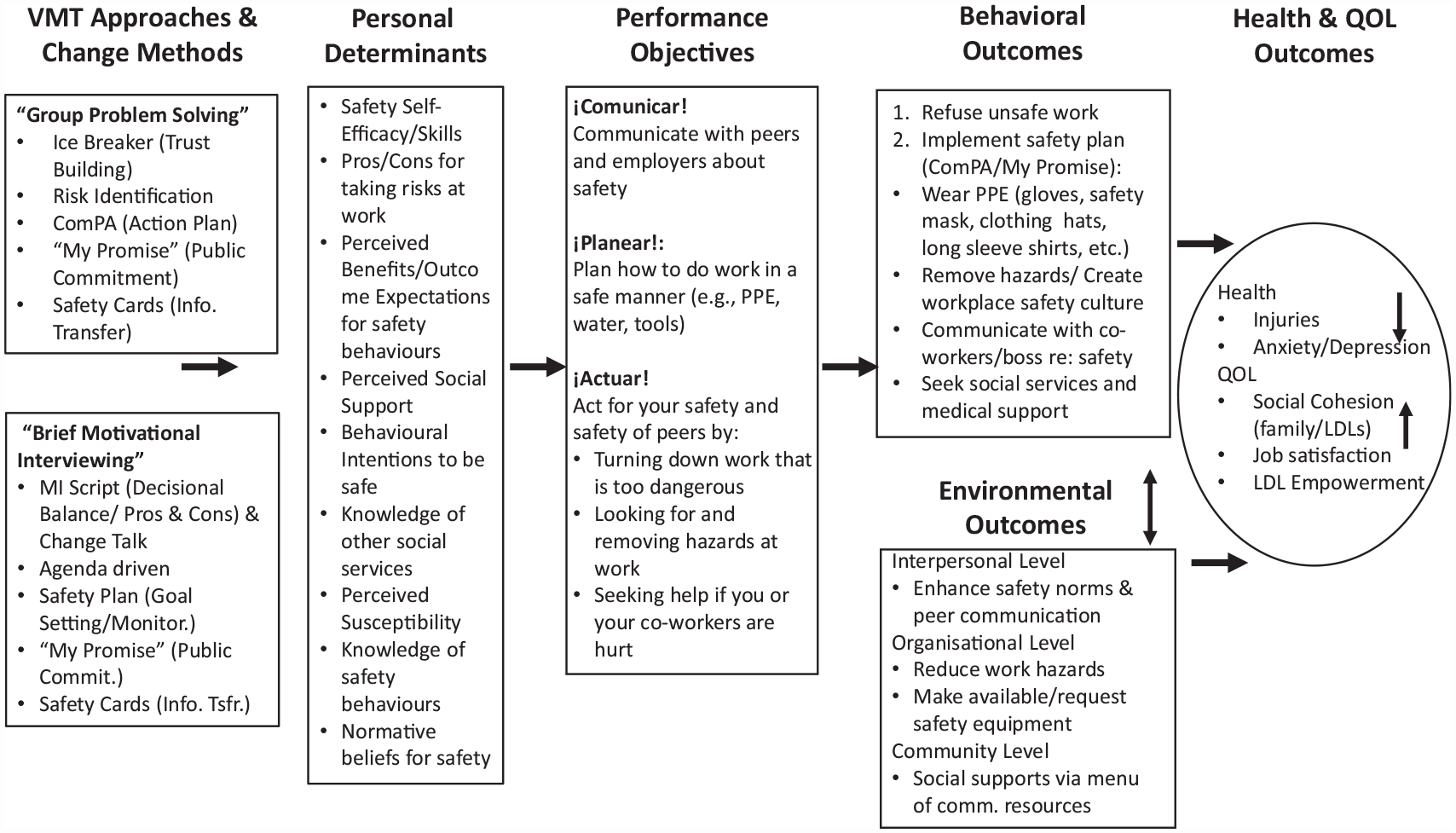
Vales+Tú (VMT) intervention logic model.
The GPS approach being tested includes an ice breaker/trust-building activity, a risk identification activity in which LDLs brainstorm key hazards and other social conditions that increase their exposure to adverse health outcomes, an action planning activity organised by the ComPA framework and a final Mi Promesa public commitment activity in which LDL participants share prevention actions they will take to increase their and their co-workers’ health and safety.
The BMI approach being tested includes an exploration of the LDL’s interest and motivation for selected injury prevention situations, validation of the problems faced by LDLs, an opportunity to select from a menu of health behaviour change options and Mi Promesa. These activities aim to enhance targeted intrapersonal factors (e.g. perceived benefits, self-efficacy and behavioural intentions) for promoting workplace safety as guided by the ComPA framework that leads to the application of/use of risk reduction strategies to prevent work-related injuries (Figure 4).
Discussion
This paper has presented the conceptual background and described the process of engaging researchers and community partners in developing the Vales+Tú programme for formal testing in a cluster randomised trial. In this process, we engaged multiple perspectives and explored multiple sources of data on workers’ experience with dangers at work and the factors that facilitate or prevent this exposure. The Intervention Mapping framework provided a systematic approach for describing our intervention development process, including reporting on our needs assessment activities and the development and refinement of our multi-component interventions for the challenging LDL corner context.
A critical aspect of our work is the emphasis on LDL lived experience and understanding of the conditions they face. Rather than emphasising knowledge transmission, the Vales+Tú programme highlights workers’ ability to individually and collectively analyse their workplace problems and formulate an action plan that fits their priorities. In addition to encouraging findings from our pilot study (Fernández-Esquer et al., 2022), the two Vales+Tú intervention approaches, GPS and BMI, are grounded in previous health promotion research and practice. Popular education approaches within the small group context, which often incorporate group-based social learning games, brainstorming, simulation and problem-solving activities, have been found to improve health through the empowerment of individuals and communities, with evidence for increasing self-esteem, social support and sense of community across diverse populations and health issues (Martinez et al., 2014; Wiggins et al., 2012). One-on-one discussion approaches led by lay or community health workers have also been found effective in promoting risk reduction practices among Latino adults for a range of health issues (e.g. Corkery et al., 1997; Navarro et al., 1998; Woodruff et al., 2002). Herein, we combine these approaches to develop interventions that take into account LDL lived experiences and that integrate interactive approaches to problem-solving by leveraging the familiarity and expertise of peer coaches.
While our previous needs assessments, pilot study and recent formative evaluation provide foundation for the feasibility of the GPS and BMI approaches, we recognise the challenges of intervention work with our proposed context and topic area, including the fluid nature of the corners where LDLs gather, the brief nature of the proposed intervention approaches and the structural barriers LDLs face and that put them at greater risk for injury on the job. Despite these challenges, we see great opportunity for supporting LDLs in reducing work-related injury and hazards by fostering dialogue, action and social cohesion via empowerment-based approaches that reach out to LDLs in their everyday contexts. The Vales+Tú corner-based GPS and BMI approaches exemplify some of this potential.
Conclusion
The collaborative partnership that was established as the foundation of the Vales+Tú programme has resulted in two practical intervention approaches to prevent LDL injury and promote LDL safety and health that can be adopted by worker centres and other organisations working with LDLs or similar groups. Given the practical theoretical approaches guiding these intervention approaches, lay health workers can be trained to deliver the Vales+Tú intervention in many settings, including the corners where LDLs gather to look for work. The conceptual frameworks guiding Vales+Tú can also inform additional intervention work to prevent LDL injury. Importantly, the process for developing Vales+Tú underscores the value of formative evaluation and active engagement of the priority population in developing population-specific health promotion interventions. By sharing our developmental work, we hope to advance ongoing co-learning about how to best support the agency of LDLs for injury prevention in ways that value their local knowledge and fit within their everyday work context.
Footnotes
Acknowledgements
We would like to extend our sincere gratitude to the Latino Day laborers who participated in this study and to the members of the study’s Community Advisory Board for their guidance and insights.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the research reported in this publication was supported by the National Institute On Minority Health And Health Disparities of the US National Institutes of Health under Award Number R01MD016328 (PI: Fernández-Esquer). The content is solely the responsibility of the authors and does not necessarily represent the official views of the US National Institutes of Health.