
Abstract
Background:
Little is known about the health literacy of children living with long-term conditions. This study aimed to gain insight into the life of children with a long-term condition in the context of health literacy, specifically their understanding of their health and the barriers and facilitators to sharing information about their condition with others.
Design:
Child-centred qualitative arts-based approach with children aged 6–12 years.
Setting:
Children participating in the study came from three countries – the UK, Australia and New Zealand.
Method:
A participatory arts-based qualitative child-centred approach prompted children to draw, label and use stickers, body-outlines and collage to describe elements central to health literacy. This encompassed their long-term condition, their understanding of their condition, its management and decision-making associated with sharing information about their condition with others. The sessions were audio-recorded, and reflexive thematic analysis was undertaken.
Results:
Four central themes related to key elements of child health literacy: (1) pragmatic understanding – what it feels like and what happens in my body; (2) management regime – what do I have to do to keep on going; (3) information sharing – I don’t tell random people; and (4) benefits of sharing – they’ve got my back.
Conclusion:
Children indicated a pragmatic or process type understanding of their condition and its management. Children were discerning about who they shared information about their condition with, but tended to establish a network of well-informed peers capable of providing support if needed. Despite gaps in children’s health literacy, parents and families have an important role to play in checking children’s understandings and developing critical health literacy.
Background
Health literacy
Health literacy is acknowledged to be a key health determinant which has the capacity to reduce health inequality (Beauchamp et al., 2015). Nutbeam and Muscat (2021) define health literacy as the personal knowledge and competencies mediated by organisational structures and availability of resources that enable people to access, understand, appraise and use information and services in ways which promote and maintain good health and wellbeing for themselves and those around them. (p. 1582)
Over the last two decades, the concept of health literacy has evolved from an initial focus on fundamental literacy skills (reading and writing) and their correlation with understanding of health information and outcomes, to a conceptualisation of health literacy as a solution that recognises empowerment and extends beyond the acquisition of basic health knowledge (Velardo and Drummond, 2017). Nutbeam (2000) proposes a hierarchy of three types of health literacy: functional, interactive and critical health literacy. Functional health literacy includes the literacy and numeracy skills required to understand basic health information. Interactive health literacy embraces the more advanced literacy and social skills needed to interact with others, communicate and apply learning to changed situations. Critical health literacy is the ability to critically evaluate and reflect upon information to make decisions about health. Nutbeam suggests that progression between these domains leads to increasing autonomy and personal empowerment for self-management (Bhagat et al., 2018).
Children’s health literacy
There is a growing body of literature exploring the role of health literacy in improving children and young people’s health behaviours and outcomes (Bánfai-Csonka et al., 2022; Bröder et al., 2017, 2019; Guo et al., 2018; Riemann et al., 2021; Velardo and Drummond, 2017). Recent research has highlighted how good health literacy can empower children to understand their world and daily life to make informed and positive health decisions (Bánfai-Csonka et al., 2022; Bröder et al., 2017). Despite this initial work, there is a lack of clear definition concerning child-specific health literacy (Paakkari and Paakkari, 2012), and many studies fail to engage with the voice and experience of the child in addressing health literacy for this population sub-group (Bánfai-Csonka et al., 2022). A widely acknowledged definition of child health literacy by Paakkari and Paakkari (2012), however, is that it is ‘a broad range of knowledge and competencies that seek to encompass, evaluate, construct and use . . . theoretical knowledge, practical knowledge, critical thinking, self-awareness, and citizenship’ (p. 136).
The progressive broadening of discourse around health literacy, prompted by the work of Nutbeam (2000) as detailed above, suggests that children have the capacity to develop, apply and share the knowledge of their condition within their family and within education, health and social arenas. While the specific challenges of working with younger children to develop health literacy remains to be explored, Bánfai-Csonka et al. (2022) and Nash et al. (2018, 2019, 2020, 2021) highlight how children exposed to early health literacy interventions can become more active in healthcare decision-making (Bánfai Csonka et al., 2022) and signals the importance of developing health literacy initiatives for children (Nash et al., 2021). This work suggests that developing health literacy early in one’s life course can lead to improved health behaviours and outcomes in later life.
Children health literacy and living with a long-term condition
The provision of genuinely meaningful care to children and their families requires a well-developed sense of what it is like for a child to live with a long-term condition in their life (Bray et al., 2015, 2022; Carter et al., 2014; Carter and Ford, 2013). Unfortunately, much health research has tended to ignore the broader factors such as ‘distributed health literacy’ or how children and young people manage health conditions within their social networks as they grow up (Muscat et al., 2022). One of many facets of everyday experience is the complex balance a child maintains between their developing understanding of their condition as a new or different mode of being in the world and the degree to which they choose to share – or keep secret – information about that condition from those with whom their world is shared. It is through this balancing act that the development of the child’s social network with respect to a health condition takes shape (Lambert and Keogh, 2015).
Central to a successful transition from childhood to adolescence is the establishment and maintenance of supportive relationships with peers and others (Freeborn et al., 2013; Lambert and Keogh, 2015; Scholes et al., 2013). For many children experiencing a long-term condition, the physical signs and symptoms of their condition and/or the therapeutic regimen can mean children are vulnerable to self-doubt and avoidance of activities of both a health and social nature (Brazeau et al., 2018; Gauntlett-Gilbert and Connell, 2012). Some children may develop a disturbed sense of belonging (Wo et al., 2018) in the face of judgements made by their peers (Rising Holmström and Söderberg, 2022; Scholes et al., 2013). Research endorses a strong sense of relief, support and empowerment experienced by children who are able to share information about their condition (Shorey and Ng, 2020). However, there is very little discussion in the literature of children’s health literacy linked to living with and managing a long-term condition, particularly among younger children, regarding the process that a child engages with in deciding to share that understanding with others.
The aim of this international collaborative study, therefore, was to undertake a closer examination of childhood health literacy in the context of living with a long-term condition. To better understand the health literacy of children living with a long-term condition (at any point beyond the first 3 months following diagnosis), the following research questions were addressed: What is the experience of young children (6–12 years) living with and managing a long-term condition? What barriers and facilitators do children perceive to exist when sharing or considering sharing information about their condition with others?
Methods
Study design
A participatory arts-based child-centred approach was chosen to provide children with opportunities for creative expression, engagement, communication and control over what they shared with the researchers. The use of a qualitative arts-based approach aimed to assist in the generation of rich data that would provide insights into the children’s experiences of their long-term condition (Ångström-Brännström and Norberg, 2014; Carter and Ford, 2013).
Importantly, the overall research design, methods and recruitment materials were developed through consultation with three children and young people aged 9–14 years of age in the UK, known to the researchers. This consultation took place face-to-face and via email. Importantly, children and young people identified the need for alterations to some of the text on the flyers and information sheet to enhance accessibility while also suggesting the arts materials that would be of greatest help to children and young people in the data collection processes.
During the course of the study, COVID-19 restrictions were introduced in each country. This meant that although much of the data collection took place face to face, during the latter stages of work a number of online data collection activities had to take place using video-based platforms (Zoom or MS Teams). In the case of data collection via a video-based platform, families were asked to provide their own art materials (pens, stickers, collage materials).
When data collection moved online during COVID-19, these children and young people advised the researchers how to position cameras and plan the activities within a slightly shorter timeframe to keep participants engaged.
Sampling and recruitment
Children aged 6–12 years in the UK, New Zealand (NZ) and Australia (Aus) were invited to take part in the study; slightly different approaches to recruitment were adopted in the different countries depending on the local ethics approvals and best choice of methods. In general terms, a flyer was placed on social media platforms and in child health clinics, and distributed via professional networks and chronic illness support groups.
Children were eligible to participate if they were aged 6–12 years, had a diagnosis of a long-term condition and were at any point in their disease trajectory beyond the first 3 months following diagnosis. Children were only considered for inclusion if their long-term condition required at least one daily intervention of some form (e.g. monitoring of blood glucose levels, medication, physiotherapy). The 6- to 12-year age group was identified as a key group to focus on, given the absence of research in this area and children being at a key stage in developing their understanding of life and living with a long-term condition. Children were excluded if they were judged by a clinician or parent as being too unwell to participate, or experienced cognitive impairment to the extent that it would impact on their ability to engage with the study.
Across the three countries, a total of 16 children aged 6–12 years were recruited.
Data collection
Children in the study were provided with art materials (pens, stickers, collage materials etc.) and encouraged to use these, as needed, to complete three tasks as part of an interview.
1. A body outline on a piece of paper was used to explore their understanding of their condition. Children were encouraged to draw and use the materials to show what parts of their body were affected by their condition. Children had a choice of body outline to work with. As the children drew on the picture, the researcher was able to ask for further details about the drawing by asking questions such as the following:
‘Are there times that having [condition] makes you feel sick or poorly? Can you please tell me which bits of your body sometimes feel sick’ or ‘Are any bits of your body feeling sick right now and if so, can you show me which parts’, ‘Can you show me on the body outline what is happening inside your body when you are feeling sick or poorly? Can you show me how the medicine you take every day works inside your body?’
2. Children were then asked to identify 6–10 people (e.g. mother, father, sibling, friend, nurse, doctor) who were important to them. Children were given the choice of drawing these people or selecting an artefact (e.g. a Lego figure, a felt figure, a sticker) to be that person. The children were then asked about which of these people know about their condition, how they found out, who told that person about their condition, people’s responses and the child’s feelings about information being shared about their condition. The following questions were used to understand the child’s decision-making:
‘You have lots of special people, can you tell me which of these people know about your [condition]?’ ‘Do you think that you can remember what you told [person’s name or role] about your condition? Do you remember what [person’s name or role] did or what he/she said when they found out about your condition?’ ‘Why do you think you told important/special person A this and important/special person B that?’
3. As a means of recognising and exploring children’s expertise and understanding of their condition, study participants were asked to write a letter, story or postcard to share with a friendly person from another planet. Children were told,
‘Let’s pretend that someone friendly from another planet comes to earth one day and they want to know about your condition. They come and see you because you are an expert, you know all about [condition] and you can tell them all about it. So they can remember everything and take the information back to their planet, they want you to write a letter/story/postcard or tell me and I will write it down’.
In the case of the face-to-face and online data collection, the interview with each child lasted between 20 and 45 minutes and was audio-recorded and transcribed to enable data analysis. In some cases, parents were present during the interview or nearby – the presence of a parent was left to the discretion of the children. Children had the option of retaining their artwork, after it had been photographed or gifting it to the research study.
Analysis of the children’s experiences
Data from the interviews with children were primarily qualitative in character (comprising transcripts of interviews and visual images created by the child). Following the interviews, the transcripts from the audio-recorded data were subjected to more formal analysis using Braun and Clarke’s procedure for Thematic Analysis (Braun and Clarke, 2006). The initial analysis of in-country data was undertaken by the respective research teams and tentative codes were developed. The entire team met frequently using video conferencing technology and engaged in further iterative and inductive construction of themes. The drawings facilitated the discussion and complemented the interview data that had been gathered. While the pictures were not formally analysed, they were used to complement what the child had told us in their responses to questions. Similarities and contrasts between the perspectives of young people across the three research locations were identified. To protect confidentiality, children are identified by means of pseudonyms (Table 1).
Participant demographic characteristics.
Rigour
Throughout this study, the international research team were in regular communication, including video-conference meetings to establish a highly detailed research and procedures. The study design was pilot tested in the UK and minor changes made to engage children more actively. Once data had been collected, the entire research team met frequently to discuss the analysis and interpretation: queries were shared and consensus reached. An audit trail of the process of analysis was maintained across each stage.
Ethical approval
Ethical approval for the study was granted by Edge Hill University (Ref: CYPF 15), Federation University (Ref: A18-120), and Auckland University of Technology (Ref: 19/162) prior to the commencement of the study. All children taking part in the study received parent/carer/guardian consent for them to participate in the study. The child’s written assent was obtained prior to data collection. The researchers worked carefully with children to ensure they understood that they could end participation at any time with no negative consequences. Time was spent explaining how the information would be used and any safeguarding boundaries.
Findings
The experience of living with and managing a long-term condition was embodied through three central themes: (1) pragmatic understanding – what it feels like and what happens in my body; (2) management regime – what do I have to do to keep on going; (3) information sharing – I don’t tell random people; and (4) benefits of sharing – they’ve got my back.
Pragmatic understanding – what it feels like and what happens in my body
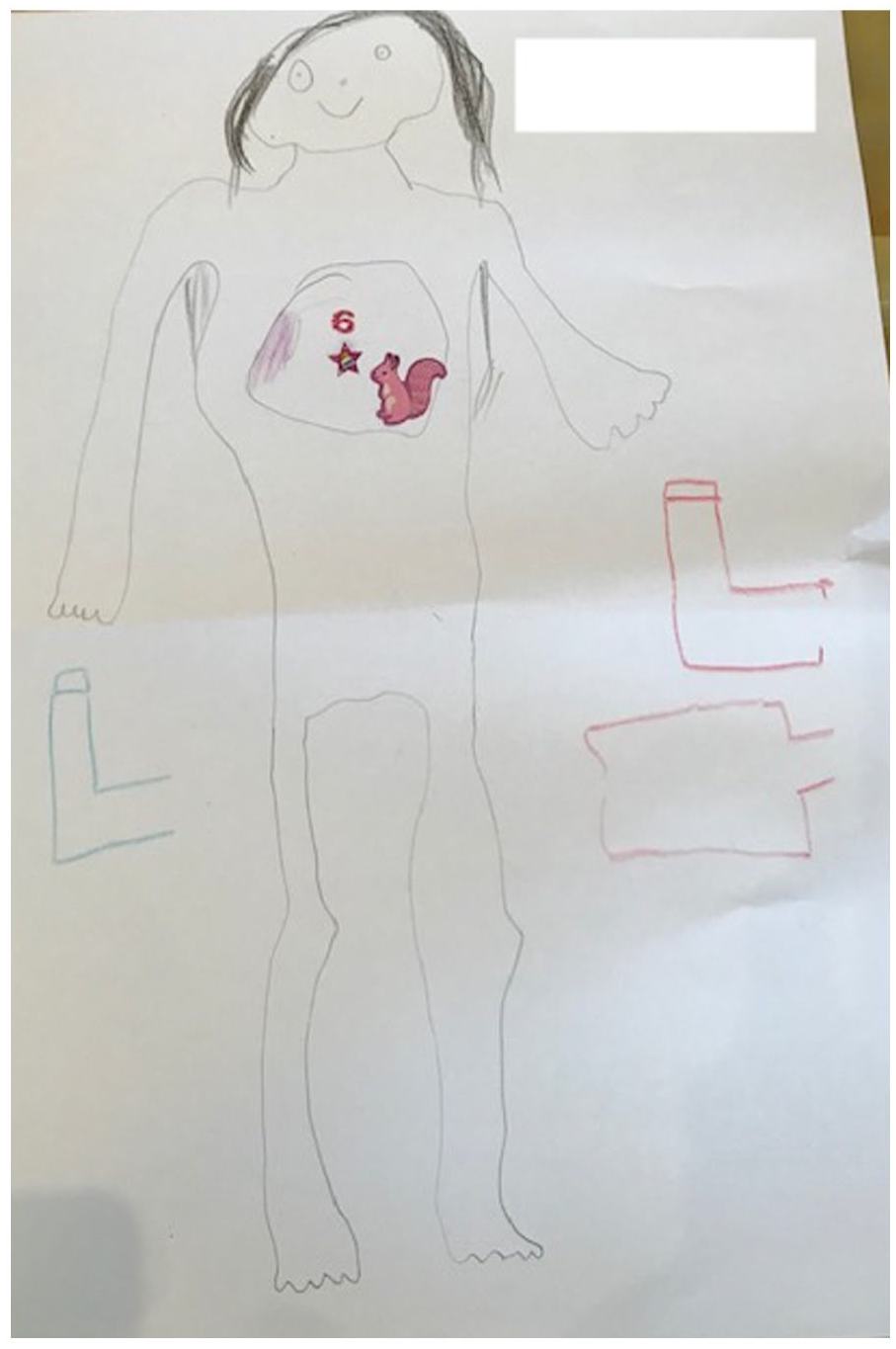
The children talked about their long-term condition and its management pragmatically; many of these descriptions were embodied and informed by their own experiences, feelings and the information that had been shared with them. Although some descriptions were not technically accurate, they had an internal logic. Lily, for example, explained how asthma ‘infects your heart and you might have a headache’. Her more detailed explanation grounded this description in her experience of what asthma felt like: I feel like I am out of breath because I’ve been running about, and I’ve used all my breath to run about with. I feel like my heart is beating too fast. That’s why I have drawn two hearts on your drawing. (Lily, asthma, UK)
The children’s images also presented and emphasised the symptoms they experienced with their condition.
In Figure 1, Jordan (asthma, Aus) emphasises the cardiac symptoms and headache.
Jordan (asthma, Aus) emphasises cardiac symptoms and headache.
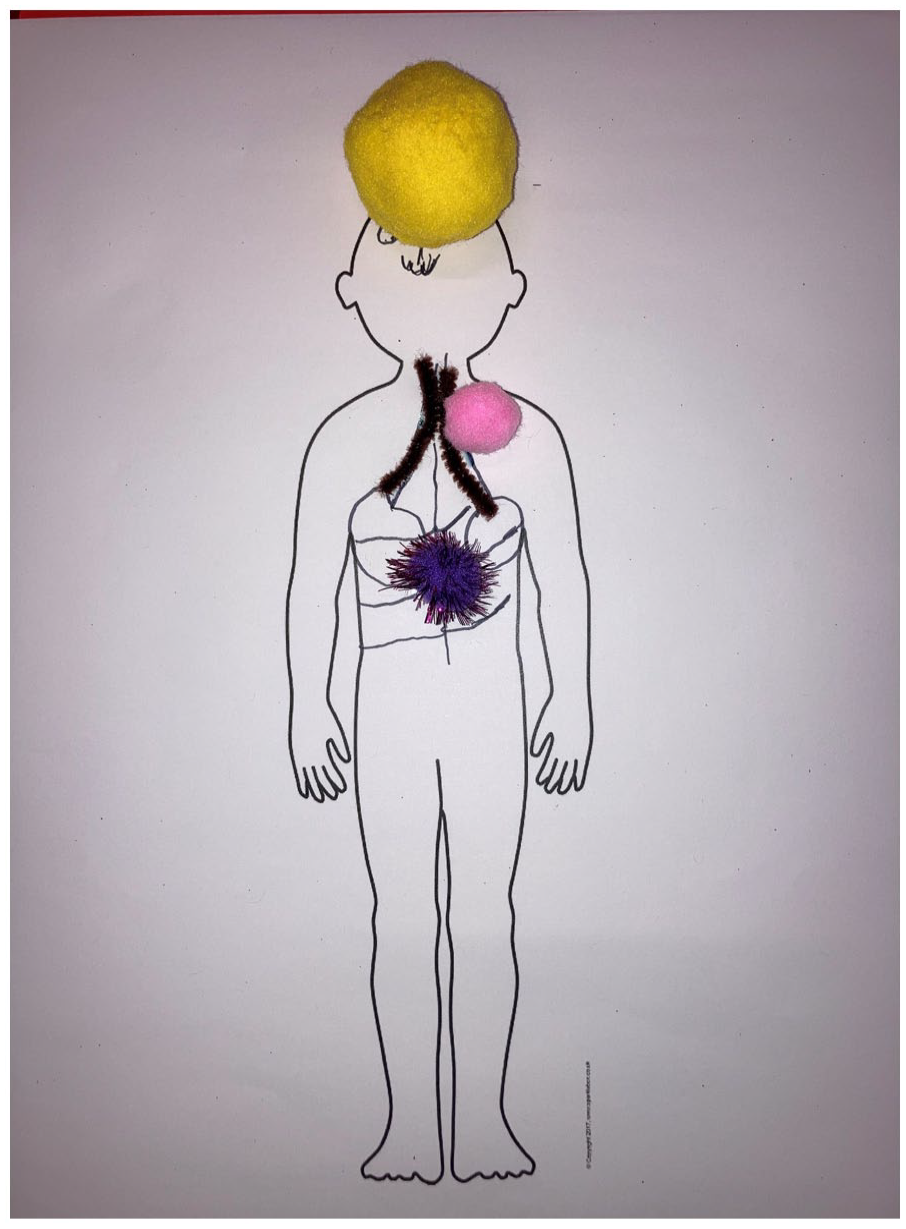
Jude talked about how asthma makes it ‘kind of like hard to like breathe’, while Rachael told us ‘your lungs like kind of close up’ and David noted that asthma is ‘a cough’. The children also understood that certain factors could act as triggers, with asthma being caused by ‘lots of dust is going into your lungs’ (NZ 2) and diabetes happening because ‘my pancreas doesn’t work so I have to have insulin to inject myself with’ (NZ 3). Owen used figurative language to explain what happens when seizure activity is experienced (Figure 2). The messages get muddled up in my brain . . .. So, it is like a postman delivering mail but it goes to a different house. (Owen, UK)
Owen (asthma and epilepsy, UK) emphasises cognitive symptoms.
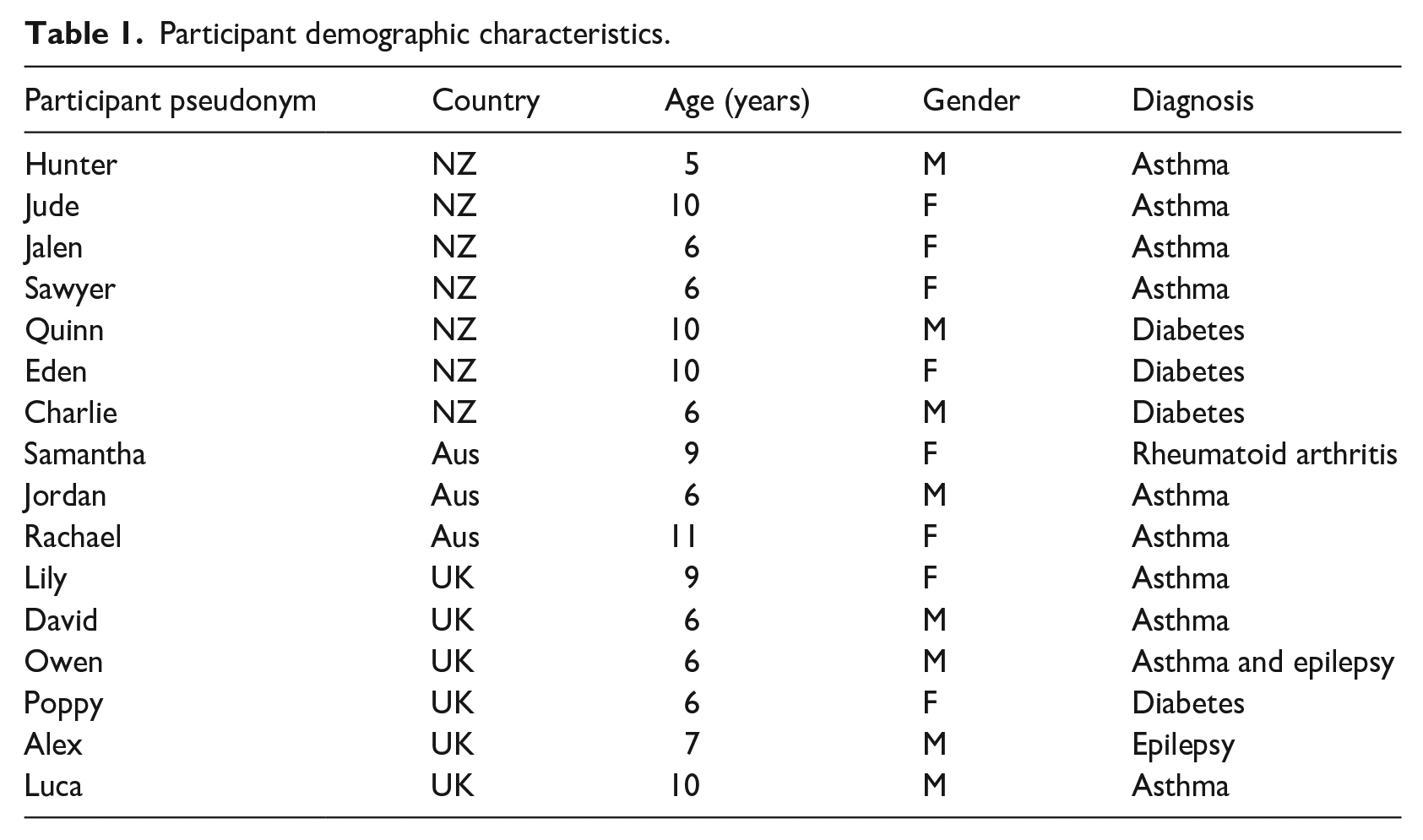
Some children wove sophisticated language and detailed explanations into their descriptions of their condition, drawing on medicalised explanations: Because my pancreas doesn’t work and then I also can put 10 basals which give me insulin over a period of time if my sugar’s high. And if my sugar gets too high then I can, um start getting sick. And like, I’ll start I’ll throw up if I have ketones. And if I’m really low, I can go into a coma and die if I don’t get an injection. Sounds a little dramatic. (Eden, NZ)
However, despite this robust description, Eden could not identify where the pancreas, the cause of his problems, was in his body outline (Figure 3). As was the case with other children, his understanding had limits. The children’s pragmatic and embodied understanding was sufficient for them, and they left the deeper understanding of their long-term condition to their parent or guardian.
Eden (diabetes, NZ) shows limited explanation.
Management regime: what do I have to do to keep on going?
Children showed a pragmatic understanding of their management regime and had a propensity to focus on the interventions needed in order for them to keep going or to keep up with their peers. Jordan linked the use of his inhaler to a change in the size of his airways, explaining, ‘the tubes that make you breath and lead to your lungs. The tubes to the lungs get smaller and with the asthma pump the tubes get bigger’. Most children tended to think of their medication and/or health management in a formulaic way and described their management regime with little apparent understanding of how their medication worked: I have to take two puffs of that in the inhaler [for asthma], and I’m supposed to take it about twice, twice a day and I take it like at, definitely at night sometimes . . . I do take it in the morning as well. (Rachael, Aus)
Jalen explained, I think the blue one’s to like help straight away the purple one’s to like, do it in a day but I don’t know what the orange one means. I think I’m meant to take it every day. (Jalen NZ)
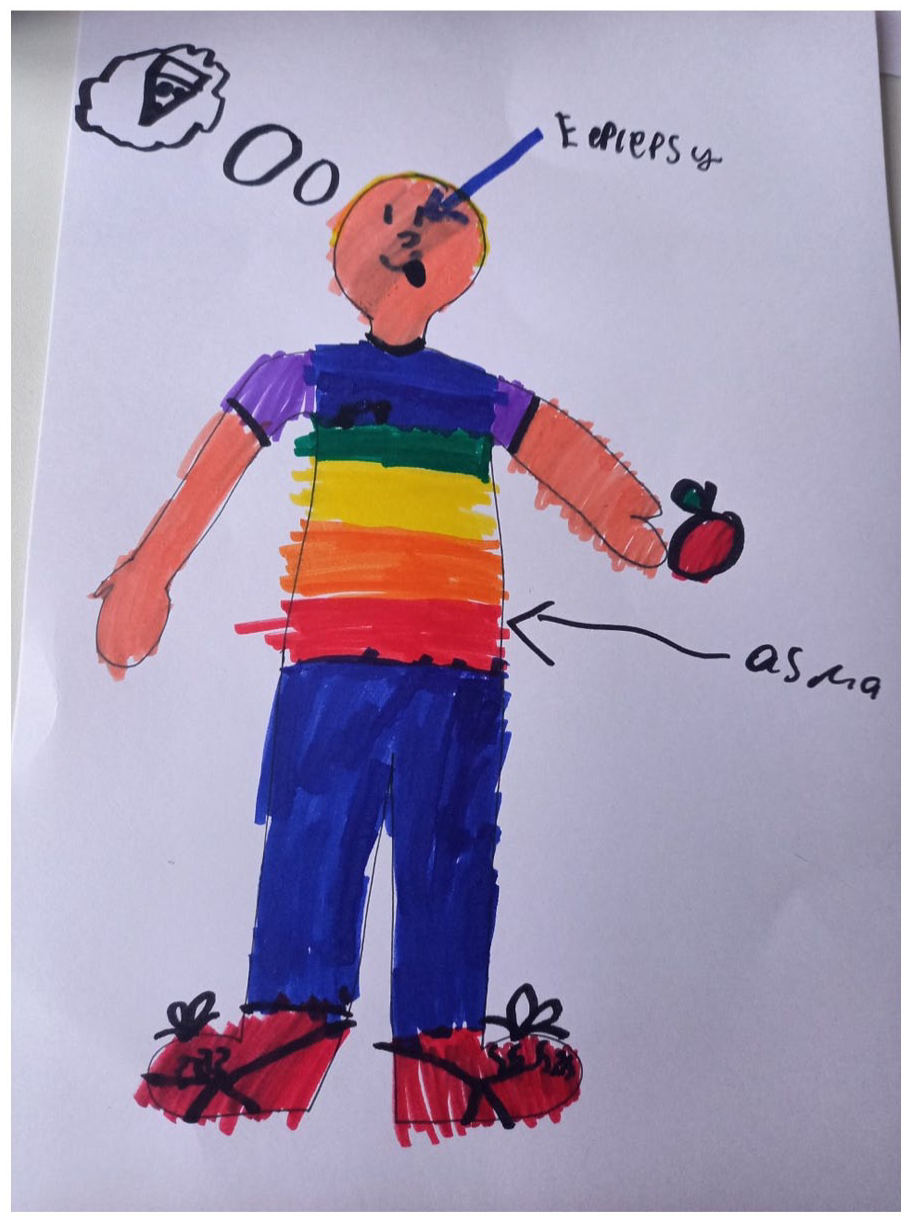
This focus on the process of management was also to be seen in several of the creative works the children produced (Figures 4 and 5).
Jalen (asthma, NZ) emphasises elements of management.
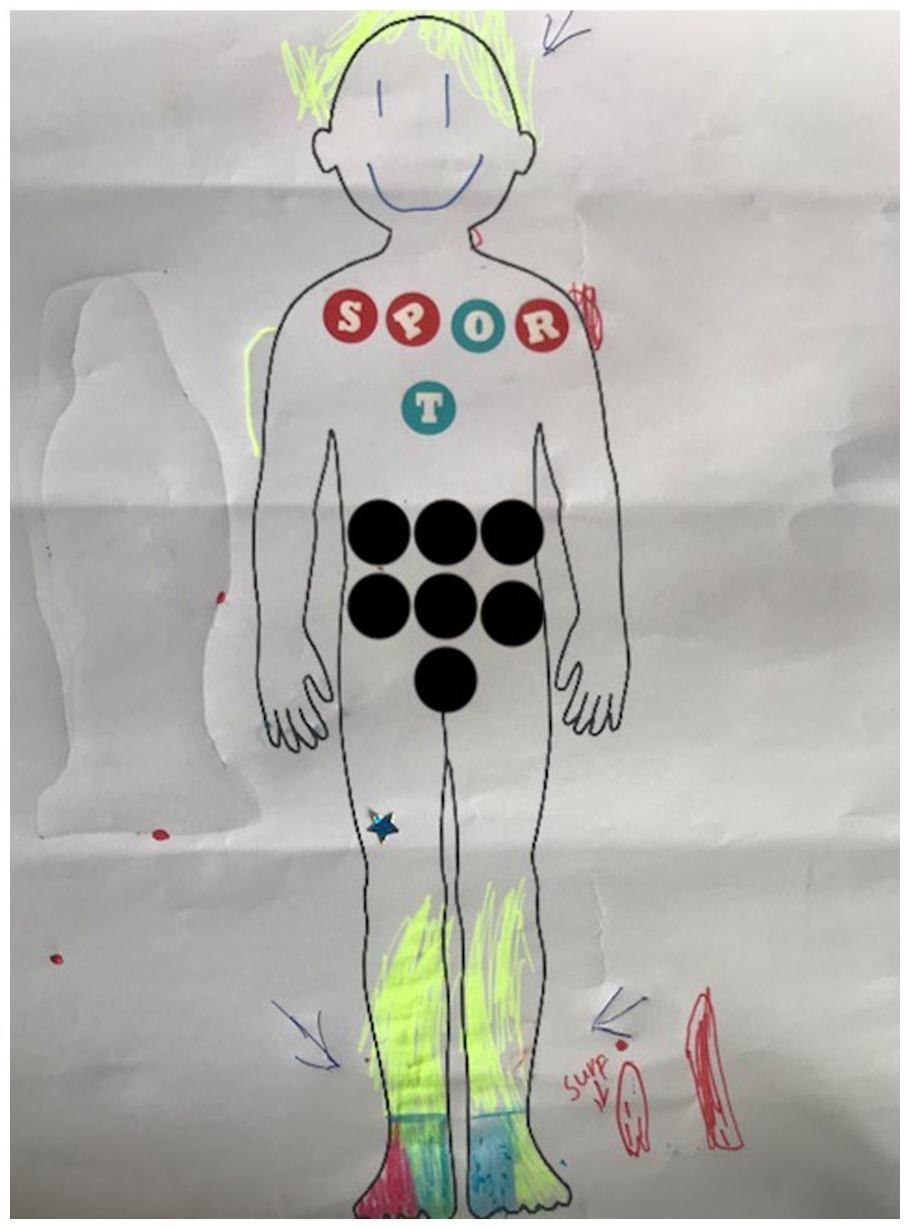
Quinn (diabetes, NZ) emphasises elements of management.
Children gave accounts of how they believed their medications worked. These offered some insight into places where their understanding was muddled. David thought water was key to removing his asthma: Yeah drinks (water) they do help ‘coz they like suck up the asthma. What happens is when we swallow it, it takes the asthma with it. (David, UK)
Lily talked about her medication being a ‘special air’: [My medication for asthma] . . . If my heart is all blocked up or something it unblocks it because I think there is special air in it, and I breathe it in and then all my other air goes out into the spacer. So, swapping my air for the special air. (Lily, UK)
Children also acknowledged that, at times, their management regime made them feel unwell. Despite this, they were prepared to engage in the treatment. You gotta take it (Ventolin) in – like the right amount because if you take too much, you’ll get dizzy . . . cause like when I have it, I feel like I need to faint and I get, like, a bunch of head rushes and stuff. And then after I have it because it’s like the Ventolin. There’s something in it and it makes it just it just makes it kinda makes this shake (demonstrates shaking reaction). But I’m trying to make it get better. (Rachael, Aus)
Overall, children described their experiences of managing their condition using pragmatic and prescribed terminologies and routines. Associating elements of their management regime with the colour, shape and size of treatment modalities provided opportunities for children to link symptoms with a specific treatment.
Information sharing: I don’t tell random people
Children showed selectiveness regarding who they told about their long-term condition. Most reported feeling comfortable to tell family and close friends but there was a sense of not wanting to share their condition openly with everyone. Lily (asthma, UK) explained, ‘I want to choose who I tell . . . it’s not really any of their business’. There were times, however, when the children experienced an acute exacerbation of their condition and displayed obvious symptoms that were witnessed by other children. In situations like this, children within the wider social network would unavoidably become aware of the child’s illness. Quinn talked of the tension between feeling comfortable telling some people and not wishing to tell everyone: Um but I don’t really tell them because when I say, mention the word. When I say diabetes, they say what? I’ve never heard of it and then I carry on and then they just say I don’t know what you’re talking about. So, I don’t really say it to people. I only say it to my friends that know about it. (Quinn, NZ)
Owen aptly represented the communication strategy he adopted in his drawing of his social network, showing how he told different people different things (Figure 6). He highlighted how his cricket team has a different level of understanding to his wider close social network.
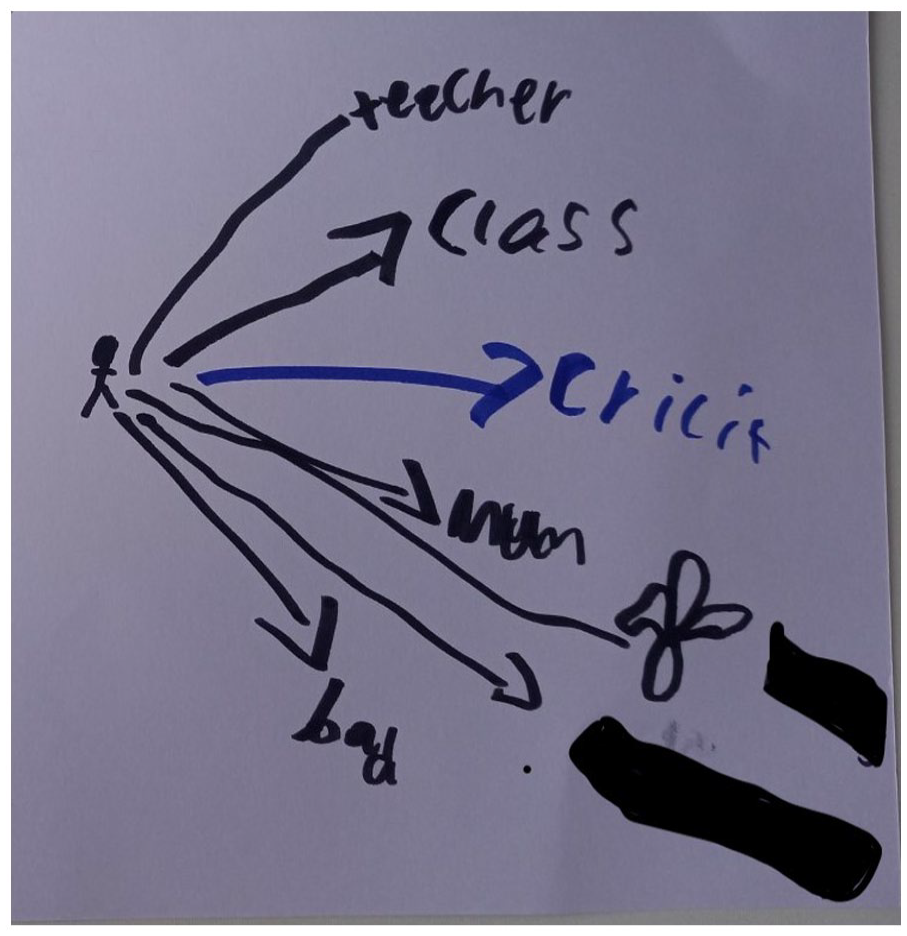
Owen (asthma and epilepsy, UK) tells his cricket team something different to other social contacts.
Among all the children, there was a sense of wanting to avoid judgement by others. Barriers to information sharing occurred when peers expressed concern about ‘catching’ their long-term illness, seemed confused about what it was or reacted in a way that made the child feel sad and isolated. Samantha shares a sense of being different or more vulnerable which meant she was guarded about openly sharing her condition with everyone: At an old school I had to tell my class because, we had ‘show and tell’ and I had to show them something . . . my operation and stuff. And then a guy wouldn’t, wouldn’t go near me . . . ‘cause he thought that it was contagious. I hoped that they [the other children] probably forgot ‘cause they didn’t know how to pronounce it, but they made me feel pretty sad because I . . . I’d never thought that they would react like that. (Samantha, Aus)
Sharing information about their own condition with others outside of their immediate family was something that each child had engaged in as an ongoing process across their life journey. Despite this familiarity, Rachael explained how she adopted a cautious approach when making decisions about sharing: I don’t tell random people. Like there’s not many people at my school [who know]. I had to tell my sport teacher because I can’t do some sport. That’s the only person who really knows. (Rachael, Aus)
Children experienced or seemingly feared misunderstanding by others. As a result, they developed a capacity to discern those individuals who were socially close to them from those who were outside their network of social importance.
Benefits of sharing: they’ve got my back
While cautious, children reported sharing information about their condition with their peers carried some benefits. While the children shared information with close friends, they found it often easier to share with children who had the same condition, recognising they may be able to provide support through the provision of medication or first aid. Poppy’s artwork (Figure 7) highlighted that it was her family – including the dog – and one good friend that knew about the condition.
I’ve got a pretty big friendship group and a couple of them know about it. Like I have another friend called [friend’s name] and she’s also got asthma. So, like, if I’ve if I’ve forgotten my Ventolin or anything she’s like, got hers, or if we had to go to first aid, and if I had to, like, make a plan for first aid like, she would come with me and stuff. And my other friends, I don’t know. I just don’t. I just don’t like mention it, like, not because I’m embarrassed or anything just because [it] just doesn’t come up in, like, natural conversation or anything. (Jordan, AUS)
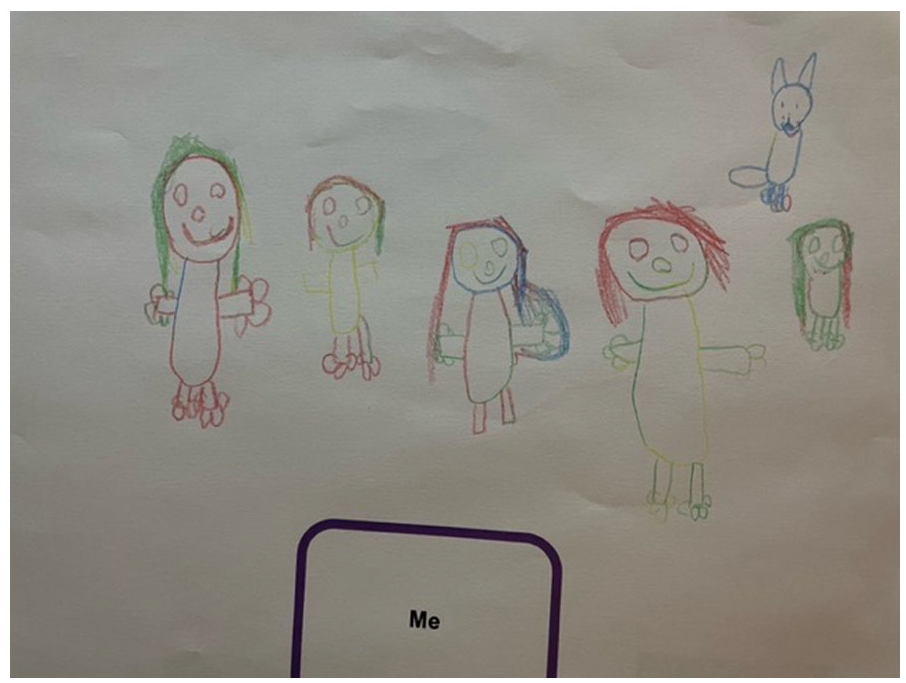
Poppy (diabetes, UK) indicates the social network they rely on.
Quinn suggested that children who did not have the same condition were not reliable when it came to support: I said, ‘I’m low’ when I got back up to class and they [my best friend] said ‘I’ll come with you’. Whereas with my other friends who aren’t really my best friends they said ‘okay we’ll see you later’ which is kind of dangerous for me if I’m low. (Quinn, NZ)
Trust was the key criterion children used to base their decision on who to share with. This was captured in a comment by Samantha: ‘I just think . . . can I trust you . . . I just . . . I don’t wanna hurt’ (Samantha, Aus). Linked to this was the sense of safety that a trusted friend would ‘have my back’ and provide the necessary support to keep them safe. Sharing information had the capacity to provide children help with treatment and accessing adult help, a sense of comfort and support during periods of exacerbation of their condition and a sense of safely knowing that their peers were looking out for them.
Discussion
Recent research has highlighted the importance of health literacy for children in the early phases of development, and the positive influence it has on long-term outcomes (Bröder et al., 2019). Importantly, health literacy is a modifiable factor that can be developed through education (Nutbeam and McGill, 2019). Despite this, there has been limited research to inform our understanding of ‘what’ it is that children understand about their illness, the way a young child makes decisions about ‘who’ they share information about their illness with, and ‘how’ they share that information with (Bray et al., 2015, 2022; Carter et al., 2017). Existing studies tend to take the perspective of older children (Lambert and Keogh, 2015; Woodgate et al., 2022). However, this study offers a nuanced and close examination of the experiences of young children living with a long-term condition across three countries, providing rich insights into key elements of health literacy from the perspective of the children themselves.
Children in this study showed a pragmatic understanding of their condition and its management as evidenced through their arts-based creations and explanations. Demonstrating a working understanding of their respective condition and management regime, our findings are consistent with previous studies with children (Bray et al., 2015; Carter et al., 2017) and studies examining health literacy in adult populations (Edwards et al., 2012). Children tended to have a mechanical or process-like understanding of their condition, focusing on ‘how it felt for them’ and the management strategies they have used in the past, to get on with their lives. The use of practical rather than technical descriptions of the physiological mechanisms that underpin a young person’s understanding of their condition has been identified by Kirk and Hinton (2019) who noted that children limited their understanding of the condition as a strategy to limit the perceived impact of their long-term condition.
The relatively limited sophistication in understanding of their condition shown by children in this study might suggest a merely rudimentary or functional capability in terms of Nutbeam’s (2000) framework. However, we suggest that children are indeed capable of being critically literate. Children in our study demonstrated how they engaged in listening to their body, following their management regime, and shared information to allow them to live as ‘normal’ lives as possible. The application of this understanding to their own situation, based on an assessment of their symptoms and administration of the appropriate treatment in a variety of real-world contexts is suggestive of critical literacy or something very much like it. This echoes findings in a previous study by Curtis-Tyler (2011) who proposed avoiding age-based assumptions about children’s understanding and contribution to their care. Importantly however, our study suggests that a child’s ability to be critical is highly contextual.
While the voices of younger children are often overlooked, there is literature that is rich with different strategies that are frequently employed by young people to increase their sense of normalcy (Cartwright et al., 2015; Kirk and Hinton, 2019; Tong et al., 2012). Several studies suggest that younger children seek to conceal their condition from others as a means of managing their perceived sense of difference (Barned et al., 2016; Benson et al., 2015; Kirk and Hinton, 2019). The children in the study, however, reported applying their health knowledge to simply get on with life and take their condition in their stride. Although, at times, they used covert techniques of surveillance and subsequent management, children did not report using strategies to hide their symptoms and their condition.
Children in this study, while not averse to sharing information about their condition with others, described how this was not something they did with everyone. This finding points to a subtle but important difference when compared to the literature that suggest children will go to great lengths to conceal their condition from their peer group (Barned et al., 2016; Kirk and Hinton, 2019). Other studies report concealment techniques ranging from ceasing therapeutic regimes (Curtis-Tyler, 2011) and social withdrawal from peer groups (Heaton et al., 2016) in order for children to present themselves as normal (Heaton et al., 2016; Kirk and Hinton, 2019). Kaushansky et al. (2016) found that adolescents tended to view their condition as irrelevant to their relationships and while they did not hide it, they did not broadcast it widely. Children in this study as with the older children in Kaushansky et al.’s (2016) study were comfortable sharing with family, friends and peers they reported as being ‘close’. There are synergies here with the notion of distributed competencies outlined by Muscat et al. (2022). Children in our study seemed to cautiously craft a network of key social contacts: family, friends, schools and sports clubs that might both support and/or compensate for a child’s developing health literacy; providing a resource that may operate to buffer lower levels of health literacy.
Consistent with previous research (Green, 2007), it was evident the children’s understanding of their condition was informed by parents, predominately their mothers. We suggest that the at times limited understanding of their condition by children in our study may be the end result of a healthcare system that relies on parents ‘picking up the slack’ or making up for any shortfall in their child’s understanding. We noted too that children often sought an approving glance or acknowledgement of their responses from their parents – particularly mothers – while engaged in our study. Although there is typically an intense period of engagement between healthcare professionals and parents at the child’s initial diagnosis about the child’s condition (Smith et al., 2015), this is not always repeated or updated subsequently (Miller et al., 2009), and if it is the child, may not be involved. Further work is therefore required to identify better ways of engaging and supporting the development of health literacy among children.
Limitations
The qualitative nature of this study, the purposive sampling utilised, and small number of participants involved means we cannot generalise findings to other contexts. It is also important to appreciate that advertising the study through specific professional networks as well as private health clinics may have created unintended selection bias.
Conclusion
This study used an arts-based approach to understand and provide a closer examination of the daily life of children with a long-term condition through a framework of health literacy. As such, it offers a deeper insight into what younger children (6–12 years) understand and consider to be most important about their long-term health condition. Children’s pictures and subsequent elaboration upon them revealed a sound working understanding of their respective condition and the desire to get on with their lives. Children were able to assess their own symptoms and respond appropriately, suggesting that with support many children can achieve more critical levels of health literacy. There is growing evidence that developing health literacy across the life course affects an individual’s ability to manage their long-term condition. Developing a child’s understanding of their condition is something health professionals can address through strategically timed targeted opportunities for learning.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.