
Abstract
Background:
Health literacy is an important public health concern and can be defined as ‘the degree or extent to which the individuals have the capacity to obtain, process and understand basic health information and services to make appropriate health decisions’. Research on health literacy among recent immigrants to Canada is not that extensive.
Objective:
The purpose of this paper was to describe health literacy status among Nepalese immigrants residing in Calgary, Alberta, Canada.
Methods:
In 2019, a cross-sectional study, using a self-administered questionnaire, was conducted among Nepalese immigrants in Calgary. The questionnaire comprised 38 questions including sociodemographic information, self-rated health status, having a chronic disease or not, health literacy, sources of health information and preference to gain health information.
Results:
We received 401 responses: 49.63% were from women, 51.37% were aged 36–55 years, 37.00% had graduate-level education, 44.96% had immigrated to Canada less than 5 years ago and 81.05% were employed full-time/part-time or self-employed. Findings revealed that 17.21% of survey participants had limited health literacy, followed by 40.15% who had marginal health literacy. The majority of the survey participants (71.82%) either always or often got health information from healthcare professionals, followed by online resources (56.61%).
Conclusion:
Noteworthy levels of limited health literacy and marginal health literacy were observed among the Nepalese immigrant population. Multidirectional, culturally tailored, community-led, collaborative initiatives are needed to improve health literacy among the immigrant population, to lessen health disparities and to promote better health outcomes.
Background
Health literacy is an important public health concern, which can be defined as ‘the degree or extent to which individuals have the ability to find, understand, and use information and services to make informed health-related decision and actions for themselves and others’ (Santana et al., 2021). It comprises the ability to understand labelling and instructions on prescribed medicines, health and medical education leaflets, appointment slips, the guidance of doctors and other health professionals, consent forms and the capability to navigate complex healthcare systems. Health literacy enables people to make well-informed decisions, which, in turn, improves their health status and empowers them (Park et al., 2018). Various studies have proven that limited health literacy may lead to poor health outcomes, greater health disparities, increased health costs and lower use of preventive health services (Berkman et al., 2011; Sheridan et al., 2011). In Canada, health literacy is seen as an essential determinant of health, which is associated with other social determinants that impact health improvement, eliminating inequalities, and health empowerment. Due to limited health literacy levels, poor choices may be made about food habits, a medical or health issue may go unchecked and deteriorate, important questions for care providers (e.g. treatment options) may go unasked and individuals may struggle to navigate an unfamiliar healthcare system (Hersh et al., 2015; Murray et al., 2008).
A variety of sociodemographic characteristics such as age, ethnicity and/or identity, sex, educational level, employment, income level, language, social support and cultural beliefs, all influence health literacy (Paasche-Orlow and Wolf, 2007). Being an immigrant is associated with many of these factors; thus, immigrants may be vulnerable to limited health literacy. A study by the Canadian Public Health Association in 2014 showed that 60% of immigrants had a health literacy competence level below the level required to cope with the demands of everyday living (Chiarelli, 2006). This may be attributable to the challenges they face when integrating into the country stemming from socio-cultural differences, as well as relatively low proficiency in English or French (Ng and Omariba, 2014). Research has shown that in the case of chronic diseases and overall self-reported health status at the time of arrival, immigrants arriving in Canada are healthier. However, the health status of immigrants has been found to decline over time due to factors such as settlement challenges, pressure of acculturation for social and professional integration, economic hardship and discrimination. These lead to migration-related stress and force immigrants to opt for risky health behaviour by prioritising settlement needs over those to do with health. Having limited health literacy may create further difficulties to make better decisions in such challenging situations (Todd and Hoffman-Goetz, 2011). People with limited health literacy levels report accessing more health services, increased hospitalisation rates and increased healthcare costs (emergency care and inpatient admission). Older people, minority populations, immigrant populations and low-income populations are particularly vulnerable to limited health literacy (Bajgain et al., 2020). Health literacy on certain topics such as sexual and mental health literacy in the context of the host country may be different from that in the home country, which can further lower the health literacy level of an immigrant (Svensson et al., 2017).
Health information resources are crucial for individuals to understand and participate in care. Research reveals that, although there are major sources of health information available, many people are unable to acquire, comprehend and apply these (Benjamin-Garner et al., 2002). A US study shows that adults may struggle to comprehend and apply health information, and those who find it most difficult to access health information are more likely to have higher hospitalisation rates and lower usage of preventive interventions (Nielsen-Bohlman et al., 2004). Traditionally, the primary source of health information has been a trusted health professional. Alternative sources have become more available with the growth of media coverage and the rapid development of the Internet (Hesse et al., 2005).
According to 2016 census in Canada, among the 7.5 million immigrants living in Canada (22% of total population), 1.9 million were of South Asian origin (Statistics Canada, 2017). In recent years, the flow of South Asian immigrants to Canada has further increased. It is predicted that South Asians may become the largest visible minority population group by the year 2036 with over 3 million (Morency et al., 2017). South Asian immigrants experience significant barriers to accessing healthcare that may be associated with a low level of understanding of the Canadian health system and services (Islam and Étongue, 2014). Despite this, research on health literacy among immigrants in Canada is scarce, although research among South Asian communities in the Greater Toronto Area has shown that these groups are among the most vulnerable in Canada when it comes to health-related inequalities (Islam and Étongue, 2014). Many of their members may be unaware of the healthcare options available or how the healthcare system operates in Canada (Islam and Étongue, 2014). Although studies have been conducted on some immigrant groups, health literacy among members of the Nepalese community has not been investigated at this point. This study therefore aimed to identify levels of health literacy among Nepalese immigrants residing in Calgary, Canada. The results may assist policymakers, practitioners and other stakeholders to develop new strategies and policies to promote equal access to good quality healthcare.
Materials and methods
Study design and setting
A cross-sectional study, using a self-administered questionnaire, was conducted in 2019 to assess levels of health literacy among Nepalese immigrants in Calgary, Alberta. We used convenience and snowball sampling, and 401 self-administered questionnaires were completed as part of the study. Ethical approval for the study was provided by the Conjoint Health Research Ethics Board, University of Calgary (REB 15-2325).
Study population and data collection
The population for this study comprised Nepalese immigrants aged 18 years and older residing in Calgary, who were able to read and write in English, and willing to participate in the survey. Data collection took place between January 2019 and June 2019. Recruitment was undertaken in collaboration with the Nepalese Community Society of Calgary (NCSC) and other local Nepalese community groups.
Potential participants were connected via email and social media as well as word of mouth. Initial participants were encouraged to share information about the study with additional contacts based on their personal social networks as they completed the enrolment process.
Potential participants were notified about the study’s goal and objectives by researchers through telephone or in person. Along with an informed consent form, the self-administered questionnaire was distributed among interested and eligible participants. Upon completion, participants returned the questionnaire along with signed informed consent. A follow-up note was sent once to non-responding participants 2 weeks after the first survey distribution. Of the 500 questionnaires distributed to potential participants, 401 surveys were completed and returned.
Survey tool
The questionnaire was developed through discussions within the research team. It comprised questions eliciting sociodemographic information, self-rated health status, health literacy, sources of health information and preferences for gaining health information. The survey questionnaire was pilot tested with a small number of Nepalese community members in Calgary and was revised by the research team prior to final administration.
Variables
The sociodemographic information elicited include age, sex, marital status, family size, education, employment status and income. Data were also collected on whether individuals had a family doctor and extended health insurance coverage, length of stay in Canada, self-reported health status and chronic disease condition.
Health literacy was measured using a brief health literacy measurement tool developed by Chew et al. and further modified by Haun et al. (Chew et al., 2004; Haun et al., 2009). Using this four-item tool, respondents were categorised into three levels of health literacy – limited, marginal and adequate (Chew et al., 2004; Haun et al., 2009). A limited level of literacy implied being unable to adequately understand simple health information/instructions (e.g. the information provided on prescription bottles/appointment slips). A marginal level of literacy entailed being able to understand simple health information and integrate easily identifiable pieces of information but not complex ones (e.g. computed tomography [CT] scan procedure brochure and drug interactions). An adequate level of health literacy indicated proficiency in understanding complicated health information and making informed decisions afterwards (Chew et al., 2004; Haun et al., 2009).
To assess health-seeking information, participants were asked ‘how frequently they had sought health information from different sources’. Participants could indicate whether or not they had used specific sources of information (e.g. from a healthcare professional through direct contact or by telephone; leaflets or pamphlets at a healthcare centre and books; from media resources such as television/radio/newspapers, Google/web pages and social media; interpersonal sources such as friends/family, self-help/patient group/peer group and community-level sources). Sources of health-seeking information were recorded using a 5-point Likert-type scale from ‘always’ to ‘never’.
Participants were then asked, ‘who they wished to get information from’. Sources could include health professionals through direct contact or by telephone; leaflets or pamphlets at a healthcare centre and books; media resources such as television/radio/newspapers, Google/web pages and social media; interpersonal sources such as friends/family, self-help/patient group/peer group and community-level sources. Again, preferences for gaining health information were measured on a 5-point scale.
Statistical analysis
The descriptive analysis was undertaken on categorical data and presented in frequencies and percentages. A chi-square test for association was used to determine the association between health literacy and the sociodemographic characteristics of participants. Analyses were conducted using STATA version 14.2, and values of p < .05 were considered statistically significant.
Results
Characteristics of survey participants
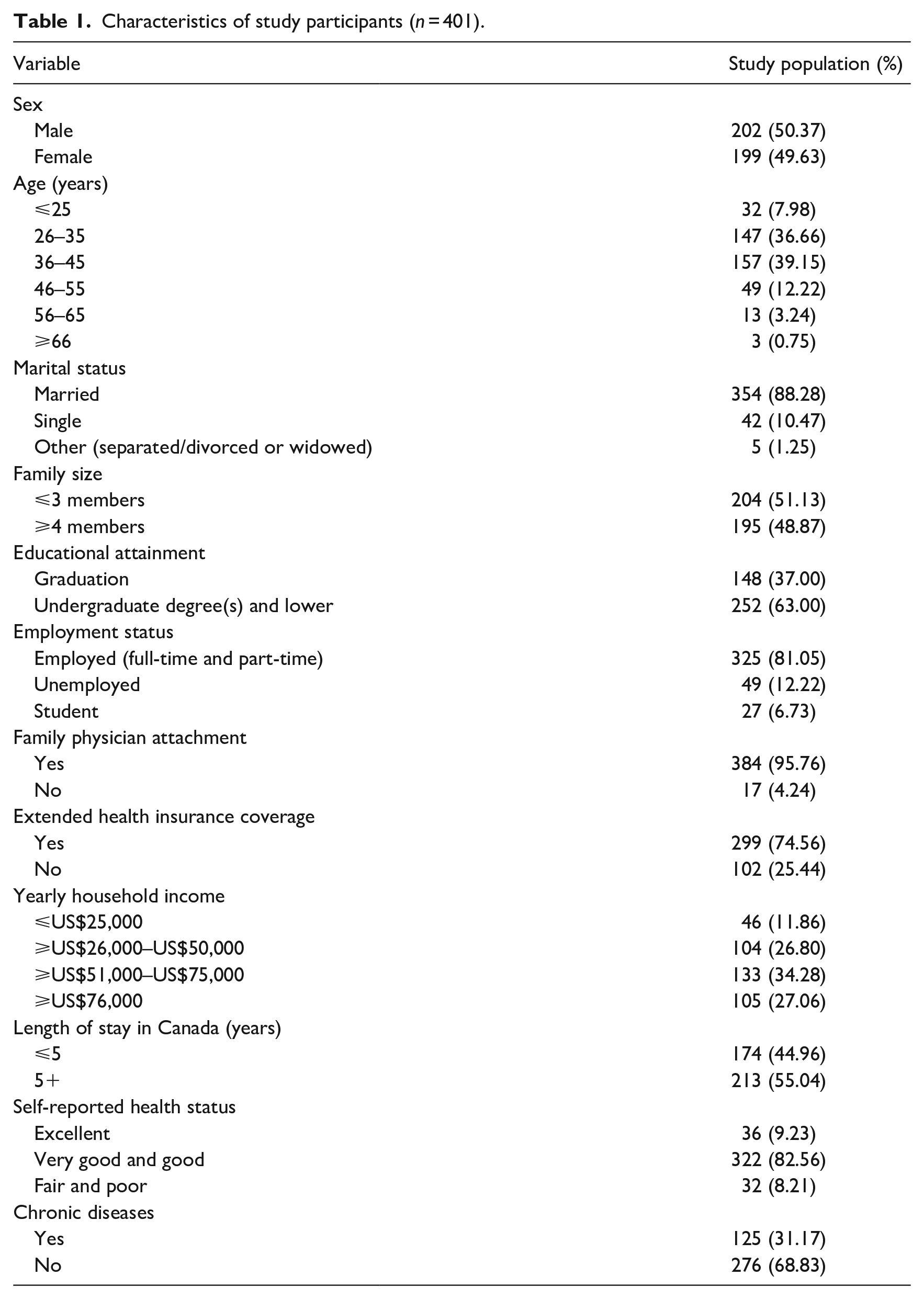
The sample population comprised an almost equal proportion of male (50.37%, n = 202) and female (49.63%, n = 199) participants. Most of the survey participants (75.81%, n = 304) were aged between 26 and 45 years, married (88.28%, n = 354) and reported to have an undergraduate or a lower level of educational degree (63%, n = 252). Over one-third of participants (81.05%, n = 325) reported their employment status as working full-time or part-time. Most of the participants (95.76%, n = 384) had a regular family doctor and extended health insurance coverage (74.56%, n = 299). Over one-third (34.28%, n = 133) of participants reported a yearly income of between US$51,000 and US$75,000. The majority of participants (82.56%, n = 322) believed that they were doing very good to good with their health, but about one-third (31.17%, n = 125) of the participants reported that they were suffering from at least one chronic disease (Table 1).
Characteristics of study participants (n = 401).
Health literacy levels
A total of 17.21% (n = 69) of the survey participants had limited health literacy, followed by 40.15% (n = 161) with marginal health literacy. The remaining 42.64% (n = 171) of the respondents had adequate health literacy. The association between health literacy and selected demographic characteristics is shown in Table 2. There were statistically significant associations between health literacy levels and participants’ gender, age group, education level, employment status, having extended health insurance coverage or not, income level and self-reported health status. Women were significantly more likely to have a low level of health literacy compared to men. Having undergraduate or a lower level of educational degrees and not having extended health insurance coverage were associated with having limited health literacy. Age group, employment status, income level and self-reported health status were significantly associated with low levels of health literacy. On the other hand, health literacy was not associated with participants’ marital status, family size, having a family physician, length of stay in Canada and having a chronic disease.
HL levels and associated demographic factors among Nepalese immigrants to Calgary, Alberta in 2019 (n = 401).
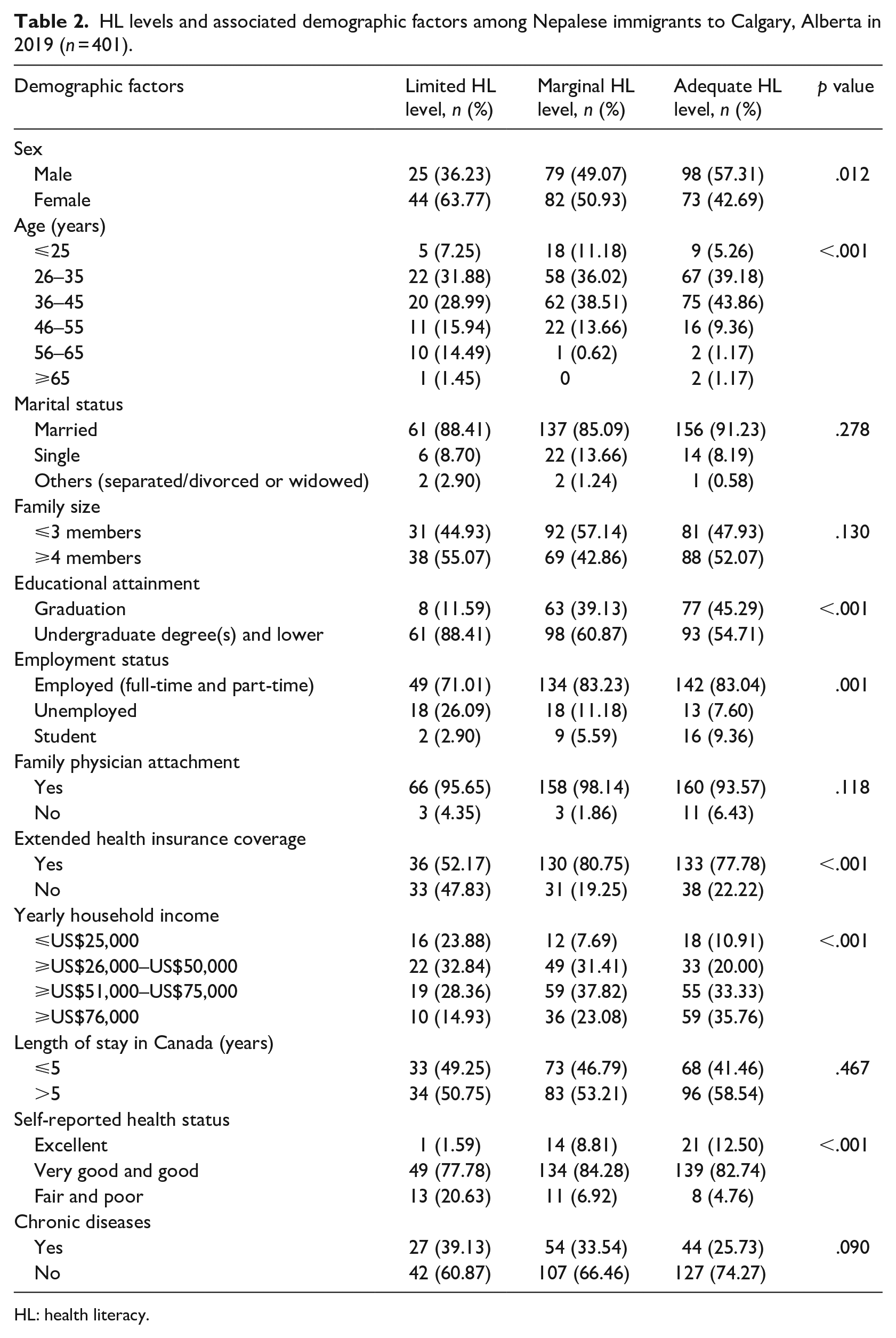
HL: health literacy.
Sources of health information
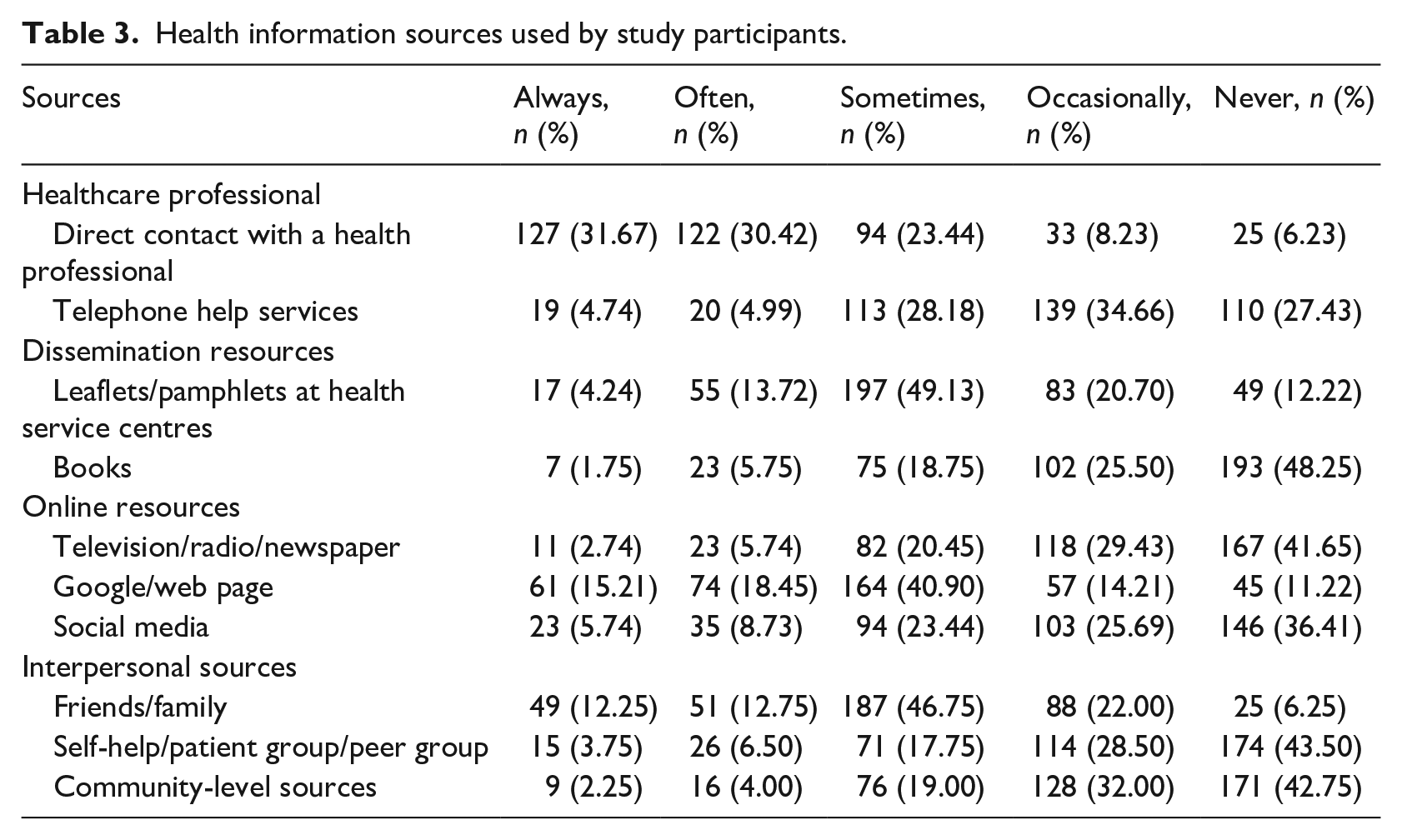
We asked participants about sources of health information. Table 3 details the responses. The majority of the participants (71.82%, n = 288) either always or often got health information from healthcare professionals, followed by online resources (56.61%, n = 227) such as television, radio, Google and social media. Dissemination sources, on the other hand, for example, leaflets and books, were not used much by them, as more than half (60.47%, n = 242) of them reported never having received health information from these sources. A total of 18.25% (n = 73) of the participants reported always getting information from interpersonal sources such as friends or peer groups.
Health information sources used by study participants.
Preferences for gaining health information
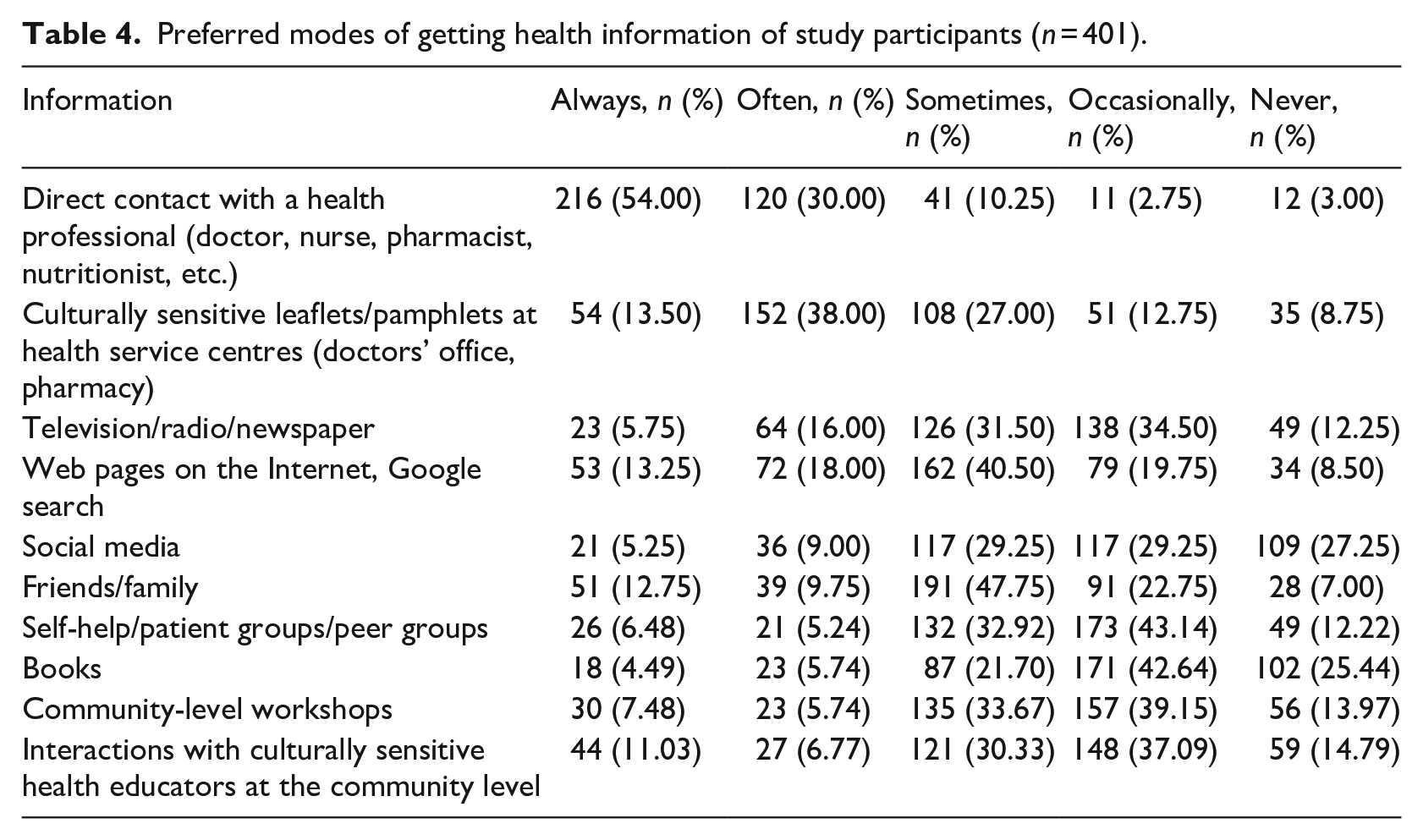
Over half of the participants (54%, n = 216) reported that their preferred sources of health information would be direct contact with a health professional (e.g. doctors, nurses, pharmacists and nutritionists). Others preferred to receive health information from leaflets/pamphlets at doctor’s office and other health service centres (13.50%, n = 54), the Internet and Google searches (13.25%, n = 53), family and friends (12.75%, n = 51) and interactions with culturally sensitive health educators at the community level (11.03%, n = 44). Over a quarter of the participants reported social media and books as their least preferred source of health information, 27.25% (n = 109) and 25.44% (n = 102), respectively. Details on preferred sources of health information among participants can be found in Table 4.
Preferred modes of getting health information of study participants (n = 401).
Discussion
This study investigated levels of health literacy among Nepalese immigrants in Calgary, Canada. Overall, 17.21% of respondents had limited health literacy, while a further 40.15% had marginal health literacy. Sociodemographic characteristics such as gender, age, education, employment status and income were significantly associated with health literacy among participants.
Health literacy is important for immigrants, particularly when they may encounter additional barriers to healthcare access due to cultural, language and systemic differences (Turin et al., 2020a, 2020b). Earlier studies in Canada reveal that immigrants tend to have limited health literacy (Ng and Omariba, 2014) compared to others. Studies in other countries have reported similar findings. An Australian study found that health literacy level was lower among immigrants from non-English-speaking countries (Ross, 2021). This may be due to the difficulties comprehending the language in which health information is made available in the host country (Yu and Mishra, 2020). Findings in our sample showed that women had a lower health literacy level than men, which aligns with the findings of previous studies showing a correlation between gender and health literacy in immigrant populations (Morawa and Erim, 2014; Müller and Koch, 2017). Female immigrants from Nepal are often expected to take care of the family, thereby limiting exposure to the language, culture and healthcare systems of the host country (Tsai et al., 2018). Consistent with previous research, our study demonstrated that having low income and not having extended health insurance were also significantly associated with lower levels of health literacy (Becerra et al., 2017). The reason behind these associations is not well understood and needs further investigation (Svendsen et al., 2020). We also found a significant association between the level of education and health literacy, a finding replicated elsewhere in the literature (Lee et al., 2015).
The World Health Organization (WHO) has noted that difficulty accessing educational information is a critical contributor to limited health literacy in immigrant communities (Kickbusch et al., 2013). In this study, the majority of participants (72.82%), either always or often, relied on healthcare professionals for health information, followed by sources such as radio, television and social media (56.61%). Research in other minority communities has shown similar patterns (e.g. Gutierrez et al., 2014). Furthermore, it has been suggested that cultural differences may influence the choices of health information sources (Askola et al., 2010). For example, a US study found that non-Japanese Asia Pacific patients were more inclined towards interpersonal communication with healthcare professionals or their friends as health information sources compared to Caucasians who preferred scientific information sources such as books and newsletters, and Japanese who opted for mainstream media and commercial sources (Kakai et al., 2003).
More than half of the respondents (60.47%) in this study had never sought health information from sources such as leaflets, pamphlets and books at health centres. In Canada, digitised public health information and written materials are two of the most popular ways to provide health information to the public but accessing them will be difficult for those who have limited access to computers and the Internet and/or who are less proficient using digital sources (Mason et al., 2021). There is a need for better understanding of the most acceptable sources of health information for immigrants (perhaps in audio-visual and interactive forms), and action is needed to present health information in the forms most likely to enhance uptake (Khalid et al., 2022a).
When information source preferences were examined, more than half of the respondents (54%) preferred to receive health information from a health professional. This finding aligns with other research identifying physicians as leading sources of information, followed by friends and families (Lai et al., 2017). Basic healthcare is covered by public insurance to residents of Canada, which can reduce the financial obstacles to physician consultation (Mason et al., 2021). Having materials available in Nepalese languages in health centres was the second highest preference among participants, followed by gaining information from the Internet and family and friends. Other research has shown that family members are a common source of health information among Asian immigrants to the USA (Jang et al., 2018).
Strengths and limitations
To our knowledge, this is the first study to evaluate health literacy among Nepalese immigrants and their health information sources in Canada. The study makes a contribution to understandings of health literacy in minority ethnic communities and to understanding the various ways in which the population accesses health information. A distinct strength of the study was the use of a community-engaged approach (Smikowski et al., 2009; Turin et al., 2021b), ensuring meaningful community involvement (Turin et al., 2021a; Turin et al., 2022b).
The study team consisted of Nepalese community scholars and citizen researchers, who linked us to a Nepalese community organisation and general community members during the planning and execution phases of the work. This allowed us to build a trusting relationship with the Nepalese immigrant community in Calgary. Our community scholars and citizen researchers were also strongly positioned as insider researchers who were also community champions. Other academic team members contributed to insider ownership of the research through capacity building, facilitating and steering the research process. In addition, we used a self-administered questionnaire that participants filled out in their own time, often at home when they had the time to think carefully about concepts of health literacy and answer reflectively and fully.
Despite the strengths of the study, some limitations also need to be kept in mind. This being a cross-sectional study, it lacks the ability to establish a causal relationship between the various sociodemographic factors and health literacy levels we identified. Another limitation is the lack of generalisability in the study findings beyond the target sample due to the use of snowball sampling. Participants in this study were limited to Nepalese immigrants residing in the Calgary region and were not representative of other immigrants to Canada. However, findings offer valuable insights relevant to other regions of Canada where Nepalese immigrants are concentrated including Toronto and Vancouver.
Conclusion
This study identified relatively limited levels of health literacy among members of an immigrant community in one area of Canada as well as sociodemographic differences that need to be taken into account when developing future more tailored approaches to improving health literacy. Understanding the information sources used and preferred by community members is central in this respect. The need for culturally relevant translated health information resources is signalled by study findings as is the need for a multidimensional community-led approach (Khalid et al., 2022b; Turin et al., 2022a).
Footnotes
Acknowledgements
We acknowledge the engagement and support received from Nepali-Canadian grassroots community members in Calgary. We also appreciate the encouragement we received from the socio-cultural organisations belonging to this community.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported partially by a start-up grant to T.C.T. (principal investigator and corresponding author)