
Abstract
Objectives:
Digital interventions are increasingly used to support behaviour change. In the prevention of chronic work-related skin diseases, the sustainable implementation of appropriate skin protection behaviour following tertiary individual prevention is important. However, there exists no intervention to support the maintenance of these behaviour changes until now. We report the systematic development of a technology-based maintenance programme to support patients to sustainably implement skin protection behaviour and to overcome barriers.
Design:
Complex intervention development based on a five-step multi-methods process.
Setting:
Tertiary individual prevention of work-related skin disease in Germany.
Methods:
Intervention development comprised the following steps: literature review, qualitative focus groups with stakeholders, quantitative assessment of the patients’ needs, development of a programme theory, and intervention development and concept validation.
Results:
We developed a concept for a complex intervention based on results from the literature review, with seven reviews meeting the criteria; qualitative focus groups involving three dermatologists, five health educators, two psychologists and three employees of an accident insurance institution; and a quantitative needs assessment with 72 patients. Key requirements were derived from this process: for example, the need to develop an app to self-monitor skin protection behaviour and skin condition and to inform the individual about ways of dealing with barriers encountered during the uptake and maintenance of skin protection behaviour. In addition, patients will participate in an individual goal-setting exercise to identify individual behavioural goals.
Conclusion:
A technology-based approach to the prevention of work-related skin diseases was developed. During the process of development, the perspectives of relevant stakeholders and the target group were considered in a participatory way.
Background
The management of chronic diseases such as diabetes mellitus or cardiovascular disease often requires specific health behaviours in patients, for example, following a specific diet or doing physical exercise. Implementing and strengthening of such behaviour can improve health-relevant outcomes such as weight and may thus positively influence the course of a disease (Danaei et al., 2009; Piepoli et al., 2014). However, changing and maintaining health behaviour is often a challenging process because it requires adapting daily routines and various barriers to doing this can arise. Behaviour change theories such as Schwarzer’s (1992) Health Action Process Approach (HAPA) aim to explain these processes and can be used to identify strategies to support behaviour change. Schwarzer conceives behaviour change as a process which includes a motivational and volitional phase. Intention formation precedes the practical implementation of a new behaviour through the interaction between three social cognitive variables: risk perception, outcome expectation and motivational self-efficacy. In the subsequent volitional phase, behaviour change is planned (action and coping planning) and then carried out (Schwarzer, 2008).
In recent times, digitalisation has profoundly influenced health care structures and patient care, and new technologies are increasingly used in health care settings. Digital health solutions have been developed for the prevention, diagnosis and monitoring of health-related outcomes and disease progression (Bhavnani et al., 2016; Gopal et al., 2019). A specific field of application is the adoption and maintenance of new health behaviours (Sawesi et al., 2016). Different digital and mobile health (mHealth) applications such as smartphone apps, podcasts, SMS as well as telephone consultations have been developed and evaluated for use in different contexts including health-related nutrition and physical activity (Sorgente et al., 2017; Webb et al., 2010). These interventions hold the potential to promote better self-control and self-monitoring of behaviour by reminders and tailored feedback systems as well as to improve interactions between health professionals and patients. Furthermore, they allow easy accessibility of health-related contents at any time for a large number of users. Compared to face-to-face interventions, they may also be more cost-effective (Sorgente et al., 2017; Webb et al., 2010).
Work-related skin diseases are among the most frequently reported work-related diseases in Europe in recent decades (Mahler et al., 2017), hand eczema being the most frequent clinical diagnosis (>85%) (Brans and John, 2016). Work-related skin diseases often result from long-lasting and frequent wet work wearing occlusive gloves and contact with irritating or potentially allergenic substances (Jacobsen et al., 2022), and genetic dispositions such as atopic dermatitis can trigger these diseases. Workers in health care settings, the metal industry, hairdressing and construction are some of the most affected high-risk professions (Brans and John, 2016). These diseases often lead to reduced quality of life and cause a high socioeconomic burden due to incapacity to work and lower productivity (Cvetkovski et al., 2005; Hutchings et al., 2001).
Due to the high prevalence of work-related skin diseases, a wide range of prevention approaches have been developed in Germany. In the case of severe and/or repeatedly relapsing work-related skin disease, the German Social Accident Insurance offers insured persons a 3-week period of inpatient rehabilitation (tertiary individual prevention [TIP]) (Brans and Skudlik, 2019). In the management of these diseases, appropriate skin protection behaviour can positively influence the skin condition and the disease progression. Because of this, health education and counselling are pivotal elements of this programme with the aim to positively influence health-related sets of cognitions (e.g. action planning) and to promote the uptake and practice of an optimised skin protection behaviour as part of the patients’ professional and private daily life. However, implementing skin protection measures is complex and may require several behavioural components like intensified skin care, handling and wearing appropriate protective gloves, as well as reducing handwashing procedures (Brans and Skudlik, 2019). Tackling barriers in real-life workplace settings may further facilitate the uptake of new appropriate skin protection behaviours. However, due to the often chronic course of work-related skin disease, and in case of atopic dermatitis, the sustainable implementation of skin protection measures following the TIP programme is of utmost importance.
To date, however, there is no specific intervention in occupational dermatology to support the uptake of skin protection behaviour. Since TIP patients tend to live across the whole country, the use of a technology-based programme was chosen as strategy instead of a face-to-face intervention. In this paper, we report the systematic development of such a maintenance programme based on O’Cathain et al.’s (2019) logic model. The aim of the intervention was to support patients to sustainably implement skin protection behaviour in their professional and private daily lives and to overcome possible barriers.
Process of intervention development
Digital interventions are complex interventions characterised by several components interacting with each other (Skivington et al., 2021). The development of such interventions should be theoretically informed (O’Cathain et al., 2019). The UK Medical Research Council (MRC) guideline (Skivington et al., 2021) recommends the use of a cyclical approach consisting of the following four steps: (1) development (e.g. identification of underlying evidence), (2) feasibility (e.g. testing feasibility and acceptability), (3) evaluation (e.g. assessing effectiveness and the change process) and (4) implementation (e.g. dissemination and monitoring).
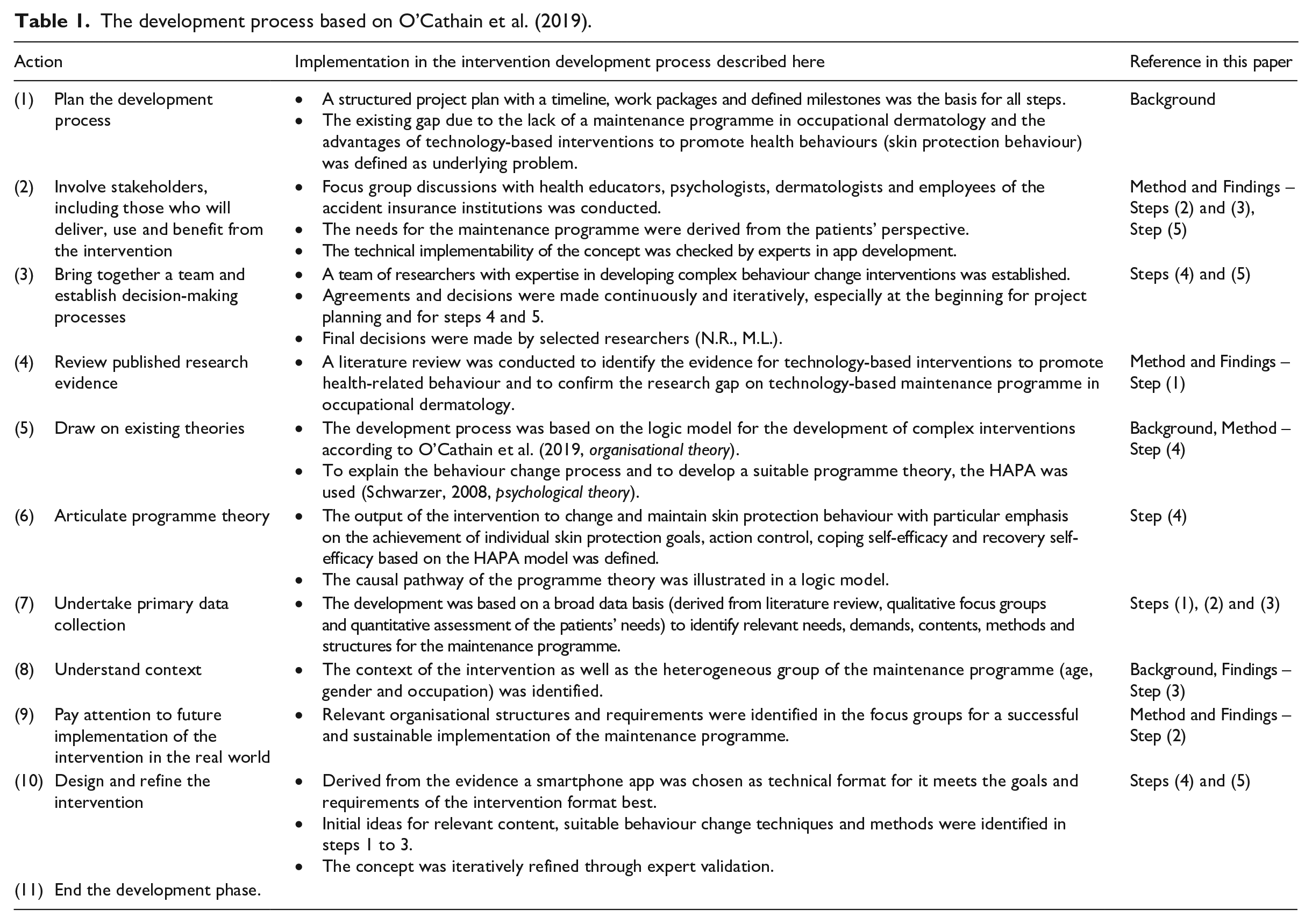
For the first phase of intervention development, O’Cathain et al. (2019) have proposed the use of a logic model consisting of 11 actions (Table 1). The development process is characterised by a dynamic and iterative exchange between the developing researchers, stakeholders and target group. Informed by this approach, the development phase of this intervention consisted of a multi-stage process characterised by the following five steps (Figure 1 and Table 1).
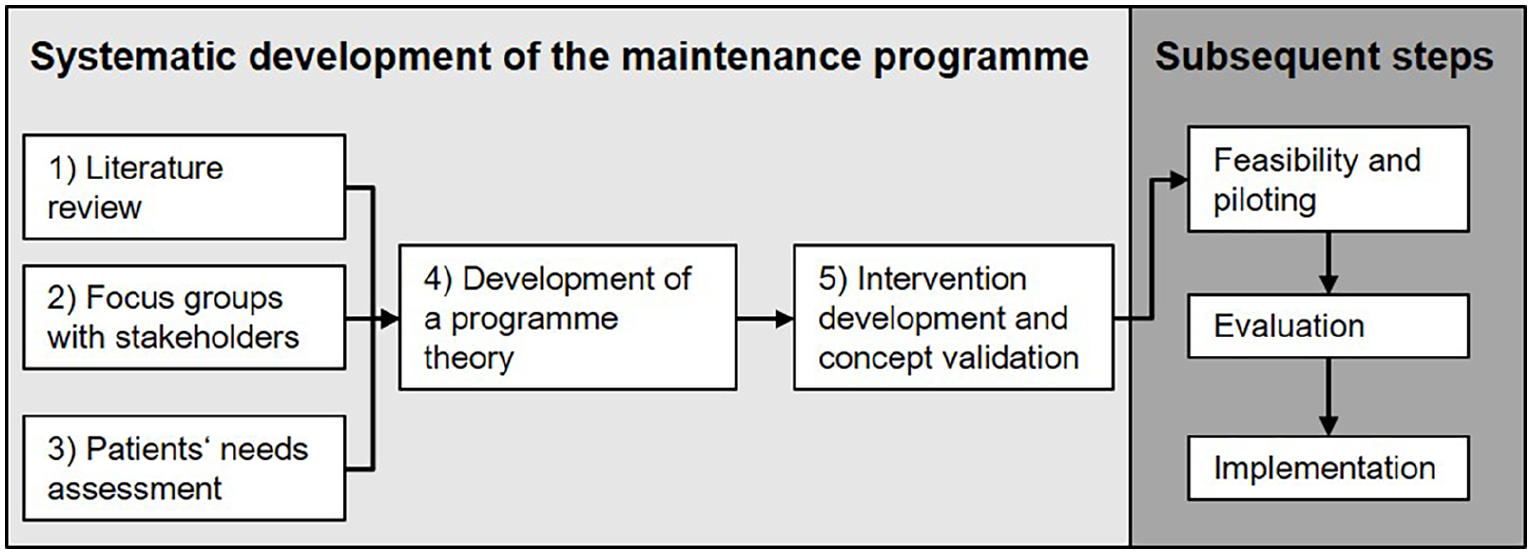
Steps in the development phase based on Skivington et al. (2021).
The development process based on O’Cathain et al. (2019).
Step 1 – literature review to identify existing evidence
Method
Health behaviours can be maintained and supported by different strategies and devices. In order to gain insight into the effectiveness of technology-based interventions to promote health behaviour, a MEDLINE literature review was conducted using PubMed. PICOS (Population, Intervention, Comparison, Outcome, Study Design) elements were used to define the objective of the review as well as inclusion and exclusion criteria for study selection (Centre for Reviews and Dissemination, 2009; Table S1, Supplementary Material). Since there is no technology-based maintenance programme in occupational dermatology, studies that promote behavioural change for adults in other health-related behaviours were searched for.
We included studies of chronic diseases amenable to treatment by behaviour change, such as obesity, adiposity, diabetes and cardiovascular diseases. Studies dealing with pharmacological interventions, mental health disorders or diseases such as HIV were excluded. Because the number of published reviews concerning technology-based interventions for health behaviour has increased rapidly in the last years (Shea et al., 2017), only systematic reviews were included. Therefore, for the literature search, the filter ‘review’ was included. Furthermore, only reviews with a controlled study design published in the English or German language were considered. Reviews reporting somatic, health-related outcomes (e.g. weight loss), quality of life or self-efficacy were only included if behavioural outcomes were also presented. A review was excluded if no behavioural outcomes were reported.
Figure 2 shows the study selection procedure. Uncertainties regarding the selection of studies were discussed until consensus was reached between two researchers (N.R., M.L.). When an assessment of relevance based on the titles and abstracts could not directly be undertaken, the reviews were included in step 1 followed by full-text review. A total of seven reviews (n = 7) were included.
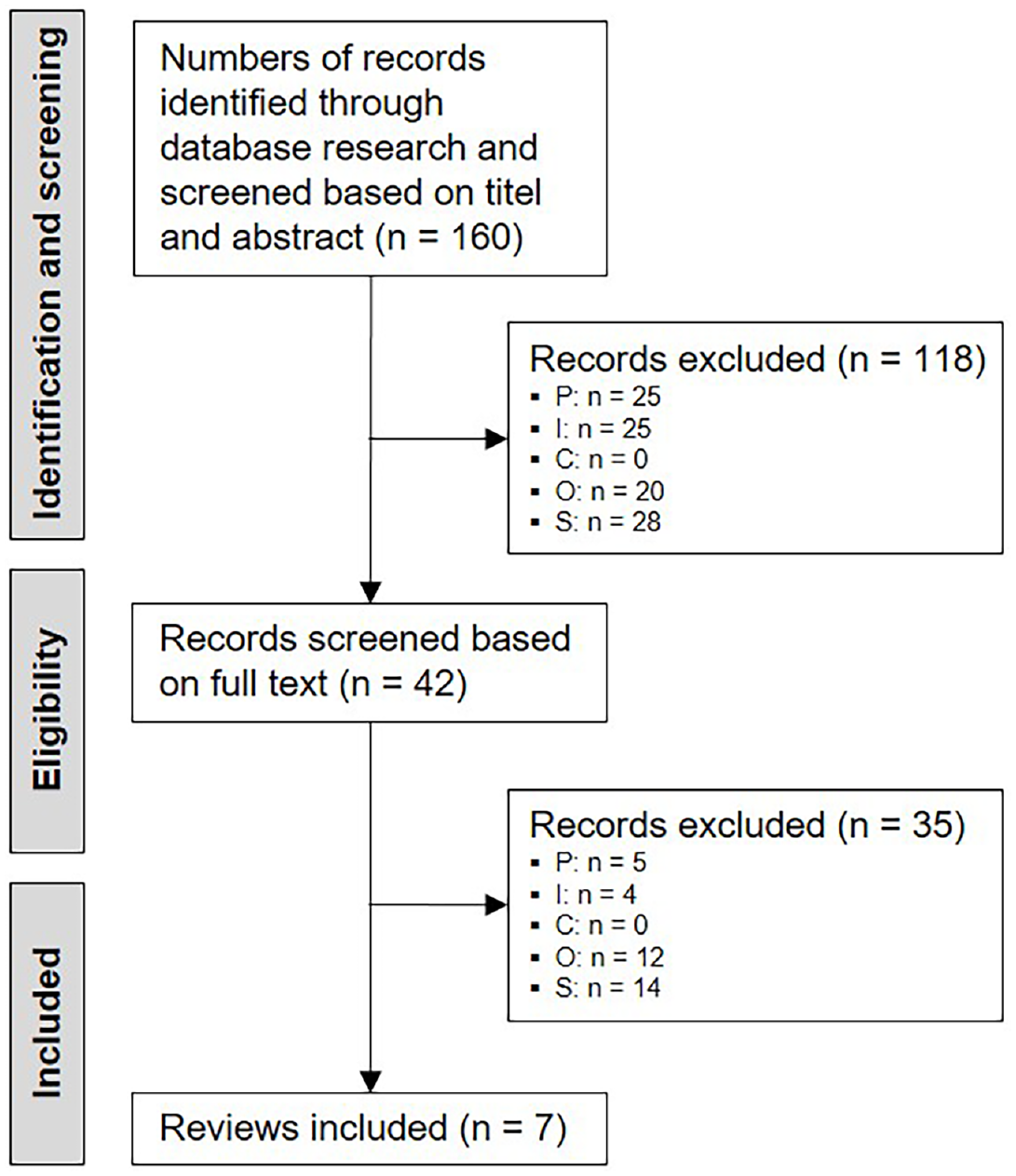
PRISMA flow diagram (Liberati et al., 2009).
Findings
Because of their heterogeneity, almost all the authors stated that the studies in the included reviews were difficult to compare. Thus, no clear conclusions can be drawn regarding the evidence of technology-based interventions to promote health-related behaviour (Cassimatis and Kavanagh, 2012; Palacios et al., 2017; Pfaeffli Dale et al., 2016; Vandelanotte et al., 2007; Wang et al., 2017). Therefore, we report the results of the reviews narratively. The review characteristics, field of application and the technologies used are shown in Table S2 (Supplementary Material).
When comparing a technology-based intervention to no intervention, studies show that some technology-based interventions improved physical activity or dietary behaviour in intervention groups compared to waiting list cohorts or control groups without any intervention (van den Berg et al., 2007; Vandelanotte et al., 2007). Usually, short-term intervention effects could be detected. Longer-term effects could not be shown or showed smaller effect sizes (Palacios et al., 2017) which raises questions concerning their clinical relevance (van den Berg et al., 2007; Vandelanotte et al., 2007).
When comparing technology-based interventions to standard care (e.g. face-to-face interventions) or comparing different technology-based interventions, no significant differences were reported. Accordingly, the type of technology or intervention format itself does not seem to be decisive for intervention effectiveness. Furthermore, interventions often consist of several components, so that results cannot always be clearly attributed to individual elements (Cassimatis and Kavanagh, 2012; van den Berg et al., 2007; Vandelanotte et al., 2007).
Pfaeffli Dale et al. (2016) report that the positive effects of SMS on smoking cessation or nicotine consumption cannot be directly transferred to other complex health behaviours such as physical activity or diet. Wang et al. (2017) conclude from their review that text messages and apps are particularly suitable for behavioural change. While text messages primarily convey knowledge and health tips, apps can promote disease and behaviour control through more complex, interactive methods. The range of application and the design possibilities of apps are higher compared to text messages. Furthermore, apps are mainly used for long-term interventions, whereas text messages are considered suitable for short-term interventions.
In addition to intervention format, the frequency of single intervention elements may be an important factor when changing behaviour. Some reviews concluded that regular contact at the beginning of the intervention, but which reduces over time, seems to be a reasonable intervention strategy (van den Berg et al., 2007; Vandelanotte et al., 2007).
Underlying theoretical models to explain health behaviour change were utilised in almost all studies (Palacios et al., 2017; Pfaeffli Dale et al., 2016; van den Berg et al., 2007; van Vugt et al., 2013; Vandelanotte et al., 2007). Palacios et al. (2017) point out that the same theories should also be used for evaluation because individual constructs can serve as mediators of behavioural outcomes (Pfaeffli Dale et al., 2016). In general, theory-based interventions are often more effective compared to interventions without an underlying theory from which relevant content and behaviour change techniques can be derived (Vandelanotte et al., 2007). The most common behaviour change techniques are goal setting, self-monitoring of behaviour, feedback on behaviour, action planning, coping planning, information about health consequences and prompts/cues (Palacios et al., 2017; Pfaeffli Dale et al., 2016; van Vugt et al., 2013).
Interactive self-monitoring and feedback applications are often tailored to users and delivered electronically or face-to-face. There is evidence that tailored feedback and personalisation can achieve better physical activity outcomes (Palacios et al., 2017; Vandelanotte et al., 2007), but the terms tailoring and personalisation are not used consistently. Whereas some studies aim to tailor their feedback by mentioning the participant’s name in the message, other studies create individualised feedback on behaviour for each user (Pfaeffli Dale et al., 2016; van den Berg et al., 2007).
In the literature, technology-based interventions are associated with high dropout rates. Therefore, components like reminder messages or gamifications that increase motivation and satisfaction are important (Palacios et al., 2017; van den Berg et al., 2007). These features can increase adherence, which in turn influence outcomes. There is evidence that an intensive use of technology is associated with better outcomes (Palacios et al., 2017; Vandelanotte et al., 2007).
Overall, the results of the reviews as well as the underlying primary studies are inconsistent and partly contradictory. Thus, the evidence regarding the effectiveness of technology-based intervention formats that can be derived from these studies is weak (van den Berg et al., 2007; Vandelanotte et al., 2007; Wang et al., 2017). Heterogeneous results may be due, for instance, to different measuring instruments and different intervention designs which limit the comparability of results (Cassimatis and Kavanagh, 2012; van den Berg et al., 2007; Vandelanotte et al., 2007).
Although the evidence base on technology-based health behaviour change interventions is largely unclear, we were able to derive some implications for the development of our app-based programme in occupational dermatology. The most important implication is that apps seem particularly suitable for changing health behaviour compared to other technologies. Furthermore, the effectiveness of technology-based interventions depends on a number of different factors that need to be taken into account during intervention development. These include strategies to increase user adherence through personalisation and tailoring, reminder systems in which messages reduce over time and the use of a theory-based approach. Finally, we decided to focus on the use the behaviour change techniques ‘goal setting’, ‘self-monitoring of behaviour’, ‘feedback on behaviour’ and ‘information about health consequences’, which are among the most common behaviour change techniques used in technology-based behaviour change interventions.
Step 2 – focus groups with stakeholders
Method
To identify the demand for a technology-based maintenance programme, three semi-structured focus group discussions (Döring, 2016) were conducted between November 2020 and February 2021 with members of professional groups involved in the care of patients with work-related skin disease. Three dermatologists participated in the first focus group, five health educators and two psychologists in the second and three employees from a major German statutory social accident insurance institution in the third.
The focus groups were intended to identify demand for the maintenance programme from the perspective of different professional groups. For step 2, we chose to use a qualitative method because it was our goal to elicit different opinions as well as experience-based attitudes. Consensus reaching was explicitly not a goal (Lamnek and Krell, 2016). Intervention contents and methods as well as structural requirements were addressed in order to develop a suitable intervention.
N.R. led the discussion using the questions in Table S3 (Supplementary Material) and M.L. made a record of the discussions using MindMaps (Pelz et al., 2004) and validated the content with the group after each session. After the focus groups had been conducted, the results were analysed separately for each professional group. The results were then summarised for content, methods and structural requirements. The participants were recruited from the Institute for Interdisciplinary Dermatological Prevention and Rehabilitation (Osnabrück, Germany) and from the German Social Accident Insurance for the Health and Welfare Services (BGW).
Findings
All stakeholders made reference to the three categories: content, methods and structural requirements. However, different issues emerged in different focus groups. For example, while the dermatologists focused particularly on the pathogenesis and treatment of work-related skin disease, employees at the accident insurance institution identified important conditions for the implementation of the maintenance programme. The health educators and psychologists identified techniques to present the content in a way appropriate for the target group (e.g. through the use of diagrams and podcasts).
Intervention contents
According to stakeholders, it is important to include material on the correct use of creams and gloves. Patients should be able to distinguish between the different creams that are applied in different settings and for different skin conditions (e.g. dry skin or blisters) and should know how to use gloves appropriately at work and in private life. To ensure intention to adopt a new behaviour was kept in mind; it was seen as advisable to create individual goals.
Stress was given to the importance of internal risk factors (e.g. in the case of atopic dermatitis) and the associated need to implement skin protection measures in the long term, even if the skin condition had improved. It was also recommended to keep track of the patient’s behaviour and disease progression, for example, by tracking the frequency of skin protection measures. Stakeholders’ experience shows that patients often pose organisational questions about their skin care, for example, regarding the roles of different occupational groups and how to deal with problems (e.g. if the employer does not provide appropriate protective gloves). These frequently asked questions should be answered as part of the technology-based maintenance programme.
Method of intervention
To utilise different sensory channels and increase accessibility for people with reading difficulties, content should be provided visually (e.g. videos) and/or auditorily (e.g. via podcasts). These should be unlocked successively one after the other to maintain motivation and adherence throughout the period of maintenance. Personalised reminders or motivational feedback were also considered helpful. Optimised skin protection behaviour and skin condition could be visualised via diagrams and photos.
Structures and requirements
To aid the use of the maintenance programme, staff working in accident insurance institutions should be informed about the contents and functions of the technology so as to advise and refer patients to the technology according to their needs. To aid use, patients should already be introduced to the technology as part of the TIP. The technology should not be used for monitoring purposes by the accident insurance provider, but should instead provide a personal opportunity and motivation for patients to develop a new routine in their skin protection behaviour. Finally, the technology should be intuitive to use and easily accessible in daily life. Using the app should not be seen as burden but rather a support for skin protection behaviour.
Step 3 – patients’ needs assessment
Method
The literature review revealed that technology-based interventions are often associated with low adherence and high dropout rates. To increase acceptance and motivation to use the intervention and ensure better intervention outcomes, users should be involved in all phases of intervention development (Alberts et al., 2020; Kernebeck et al., 2021). A participatory development process would enable the assessment of target groups’ needs in order to take them into account during intervention development.
For this reason, patients who had provided written informed consent in accordance with the ethical standards of the Declaration of Helsinki took part in a written follow-up survey as part of quality assurance measures following the TIP. The aim of this ongoing survey is to monitor patients’ satisfaction and to assess ways of optimising the rehabilitation programme. In the analysis presented in this paper, results from patients who participated in the TIP between January and June 2019 are included. The survey aimed at identifying the patients’ needs following discharge in terms of a technology-based maintenance programme as well as technical requirements for implementation. A quantitative approach was used for the ongoing survey asking questions, for example, about the accessibility of different devices such as smartphones. The questionnaire was distributed in July 2019 and included questions on the implementation of skin protection behaviours following discharge, favoured technological formats and ways of providing further support. Descriptive data were analysed using IBM SPSS version 26.
Findings
Of 194 questionnaires distributed, 72 were returned (response rate: 38%). Of these, 37 (51%) came from women and 35 (49%) from men (49%). Participants’ average age at the time of the survey was 49 years (range 24–64 years, SD = ±11). The majority of respondents worked in the health care sector (n = 31, 44%) followed by metals industry (n = 16, 23%).
The majority (54%, n = 38) reported difficulties in implementing skin protection measures after returning to work. Patients identified the need for support and help if the skin condition deteriorates again, if they do not receive support from their employer in terms of their skin disease, or if recommended protective gloves or creams are not provided. They also expressed the need for strategies to deal with itching or stress.
Slightly more than half of participants (54%, n = 39) felt the need to refresh the contents learned from seminars on the correct implementation of skin protection, skin cleansing and skin care. Webinars including other patients, but also explanatory videos showing, for example, the correct removal of gloves, or podcasts explaining the correct application of skin protection measures were rated as highly popular.
No technology proved equally accessible for all patients. However, access to Internet-enabled smartphones (93%, n = 63) was higher compared to computers (85%, n = 58).
Step 4 – development of programme theory
Based on the results of steps 1–3, a smartphone app was considered most suitable approach to use. Intervention development focused on the volitional phase of the HAPA model with the aim of optimising skin protection behaviour by setting and achieving individual skin protection goals, strengthening action control and dealing with barriers and relapse through coping self-efficacy and recovery self-efficacy (Schwarzer, 2008).
The conceptual underpinnings of two major intervention components were developed: (1) smartphone app and (2) individual goal-setting interviews. Specific behaviour change techniques derived from Michie et al.’s (2013) taxonomy and HAPA constructs were assigned to the programme contents by two researchers who had received online training in coding behaviour change techniques (N.R., M.L.). Thus, theory-based behaviour change strategies were translated into practical strategies for the app. To aid implementation in specific contexts and settings, intervention development was supplemented by the identified structural requirements identified in step 2.
The programme theory was translated into a logic model for the maintenance programme that illustrates the causal pathways within the behaviour change process (Figure 3). The logic model serves as the basis for subsequent programme development and the piloting of the app. It will be revised informed by the results of the next process steps (Skivington et al., 2021).
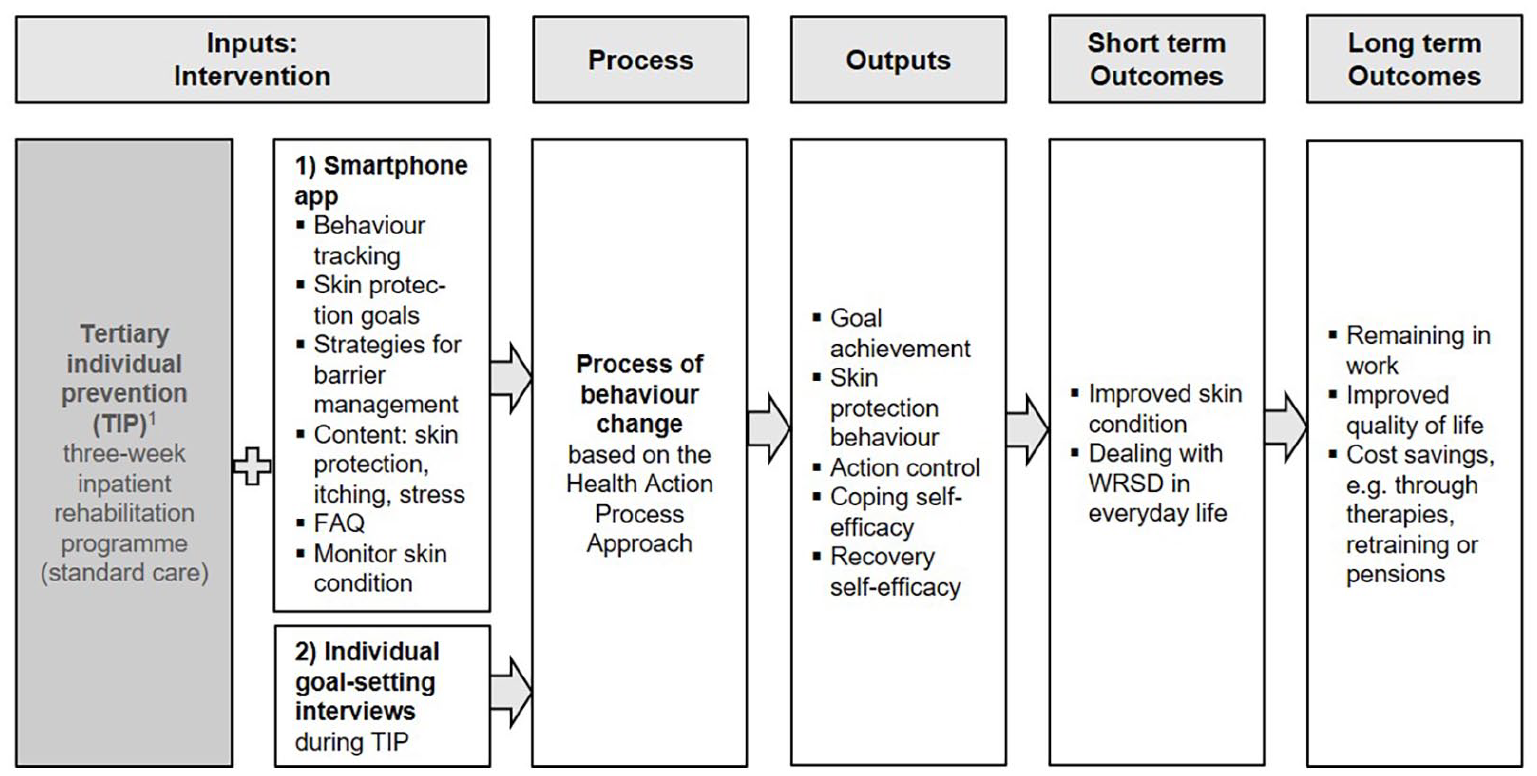
Logic model.
Step 5 – intervention development and concept validation
After specifying the programme theory, a preliminary intervention concept was developed. For each intervention component, a specific intervention goal was defined and the components were specified in terms of frequencies and sequences.
The conceptual approach was then presented and further revised by members of the project team in two rounds of meetings with health educators and psychologists as well as with app development experts. In the first round of meetings, face validity regarding completeness and stringency was checked by six health educators and one health psychologist, all of whom were experts in the development of behaviour change interventions. The conceptual approach was adapted accordingly and then presented to three app development experts in a second round of meetings. The focus here was on checking and discussing feasibility from the technical point of view.
Next, two researchers (N.R., M.L.) developed the specific contents. This included the preparation of text for content repetition and the creation of feedback messages. To ensure the comprehensibility and correctness, the content was reviewed by other members of the project team and again revised by the researchers.
To ensure quality assurance in the future implementation phases of the project, the intervention and specific intervention components will be developed into a written intervention manual (O’Cathain et al., 2019; Skivington et al., 2021).
Discussion
This paper has reported on the systematic development of a technology-based maintenance programme to help patients with work-related skin diseases implement appropriate skin protection measures at work and in daily life. To the best of our knowledge, this is the first paper to report on the development of an app-based maintenance programme for use in an occupational dermatological setting.
The results from the literature review show that the evidence regarding the effectiveness of technology-based interventions to change health behaviour in different settings is scarce. External validity is also limited as it cannot clearly be deduced from existing publications which technology is most suitable to be transferred to new fields of application. However, Wang et al. (2017) state that compared to other technical devices, apps are particularly suitable for health behaviour change. Various advantages include the use of interactive methods, automatic feedback and possibilities for personalisation and tailoring. Furthermore, access of our specific target group to smartphones is high. We assume that these results can be transferred to a wider cohort of patients with work-related skin disease but not to patients suffering from other chronic diseases. Since smartphones are an integral part of daily life, the maintenance programme may easily delivered via app to a large part of the target group.
Because of high dropout rates in technology-based interventions, other factors to influence app use, adherence and effectiveness, should be considered in the development process (Palacios et al., 2017; Vandelanotte et al., 2007). These might include feedback on the desired behaviour, reminder systems, consideration of the needs of the specific target group and detailed introduction on how to use the app (Yu et al., 2015). In their meta-analysis, Head et al. (2013) found that tailored and targeted messages (d = 0.442, p < 0.001) had larger effect sizes compared to tailored messages (d = 0.274, p < .001) or targeted messages (d = 0.073, not significant) alone. Intervention effectiveness is higher when messages include individual variables such as physiological parameters (e.g. weight) and are personalised with the patient’s name. Furthermore, interventions are more effective when the frequency of messages decreases over the intervention period (d = 0.523, p < .001) or can be determined by the users themselves (d = 0.425, p < .01).
Lyzwinski et al. (2018) identified in their review of user preferences for mHealth interventions for weight loss a number of factors influencing usage. To increase app adherence, simple use, visual appeal, opportunities for personalisation and elements for entertainment such as gamification were cited as most important criteria. These results are consistent with those of Palacios et al. (2017), Vandelanotte et al. (2007) and van den Berg et al. (2007) and are key to success in intervention development. Lyzwinski et al. (2018) also identify technical requirements that should be taken into account when programming the app – they include simple navigation and visual appeal. Regardless, studies show that intervention use is higher for apps than for websites (Carter et al., 2013) or paper-based interventions (Burke et al., 2011). However, it is best to assume that these aspects alone are not sufficient to achieve acceptable usage because app adherence is likely influenced by other factors such as users’ motivation to change their health-related behaviour (Vandelanotte et al. 2007).
Strengths and limitations
The systematic and theory-based approach to developing the maintenance programme in line with existing evidence is a strength of this work. O’Cathain et al.’s (2019) core principles and actions were used as framework to consider different perspectives of relevant stakeholders and members of the target group participatory. Furthermore, this paper reports on how iterative development and revisions led the maintenance programme to address the justified critique of lack of transparency in terms of detailed information on development (Duncan et al., 2020).
Limitations include the fact that the literature review was conducted on only one database MEDLINE via PubMed. A comprehensive systematic review using additional databases (e.g. PSYNDEX or CINAHL) with snowballing was not part of this project. That said, it seems reasonable to assume that we were able to identify a large amount of relevant literature by the choice of database as well as by focusing on reviews. Nevertheless, further literature searches are to be recommended in future.
The results of any needs assessment may be influenced by personal interests of participating patients in technology-based maintenance programme, or by socially desirability effects. Therefore, response bias in this study cannot be excluded. Furthermore, a written questionnaire alone is not sufficient to elicit the full spectrum of perspectives within a target group. Thus, in the subsequent piloting of the app, the target group’s perspectives will need to be obtained, for example, by focus groups and surveys, to adapt the intervention to their needs.
Next steps
Subsequent steps will focus on piloting the app and the goal-setting interviews in line with Skivington et al.’s (2021) recommendations. As a part of this process, the intervention will be tested and formatively evaluated by patients alongside further technical development. It will be important to consider the views of the target group beyond intervention development to ensure long-term app adherence and reduce dropout. Thereby, the feasibility of implementation in the context of the TIP will need to be tested at the process and structural level (Donabedian, 2005). Following the recommendations by Palacios et al. (2017), appropriate instruments are currently being developed and tested to evaluate the effectiveness of the app based on the underlying theory of behaviour change. It must also be explored in relevant contexts whether an app is suitable for this new field of application. Finally, a detailed description of the app based on the ‘template for intervention description and replication’ will be published after piloting and feasibility testing (TIDieR, Hoffmann et al., 2014).
Supplemental Material
sj-docx-1-hej-10.1177_10963480221116049 – Supplemental material for Development of an app-based maintenance programme to promote skin protection behaviour for patients with work-related skin diseases
Supplemental material, sj-docx-1-hej-10.1177_10963480221116049 for Development of an app-based maintenance programme to promote skin protection behaviour for patients with work-related skin diseases by Nele Ristow, Annika Wilke, Swen Malte John and Michaela Ludewig in Health Education Journal
Footnotes
Acknowledgements
We acknowledge support from the Deutsche Forschungsgemeinschaft (DFG) and the Open Access Publishing Fund of Osnabrück University. We would also like to thank Stefanie Awe from the Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege, BGW (Institution for Statutory Accident Insurance and Prevention in the Health and Welfare Services) for supporting the organisation of focus group discussions.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. Funding for the project Technologiebasierte Nachbetreuung in der berufsdermatologischen Prävention der BK Nr. 5101 (TecNaP): Systematische Bedarfsanalyse und Konzeption eines Angebotes zur Unterstützung der Patientinnen und Patienten beim aktiven Transfer von Hautschutzmaßnahmen in den beruflichen und privaten Alltag (TecNaP), project (FF_1457) was provided by the BGW.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.