
Abstract
Objectives:
The incidence of type 2 diabetes in UK Black African and Caribbean communities is up to three times higher than in the general population, and engagement with self-management advice is poorer. This study explores the perspective of those living with diabetes to understand how the cultural salience of advice could be improved.
Design:
Participants were recruited via community venues, faith institutions and primary care. Eight focus groups were conducted with 41 individuals (Black African n = 23, Black Caribbean n = 18). Grounded theory methods were used for analysis.
Results:
Although motivated to manage the condition, individuals experienced a misalignment between elements of the care provision and cultural norms. Explanatory models of diabetes differed from the biomedical model reducing trust in treatment protocols. A lack of cultural salience reduced the accessibility of advice. Furthermore, elements of self-management advice were seen to conflict directly with some cultural traditions and practices. Individuals had to reconcile the two perspectives in order to proceed with self-management, often prioritising cultural norms and advice from informal sources over healthcare advice. Building personal relationships with the healthcare team improved trust and engagement.
Conclusion:
Findings suggest the needs in these communities were not being fully met. The healthcare interaction was pivotal in improving trust and engagement and reducing misinformation. However, appropriately informed community support also offers the potential to mitigate misalignment and to improve equity of access.
Introduction
The threefold higher incidence of type 2 diabetes in UK African and Caribbean (AfC) communities compared to the general population (Health Survey for England, 2006), coupled with lower engagement with self-management (Winkley et al., 2015), presents a challenge for healthcare professionals. People of Black ethnicity are less likely to have annual testing, and while policy changes are raising standards for all people living with diabetes, the inequities between individuals of Black ethnicity and the general population persist (James et al., 2012; Whyte et al., 2019). Providing care and health promotion that is individualised and sensitive to cultural beliefs and habits is a key public health objective to increase engagement and reduce inequities (National Institute for Clinical Excellence, 2018). Furthermore, improving the cultural salience of care has been shown to improve diabetes-related knowledge and control (Creamer et al., 2016).
Health behaviour is shaped by culture, ‘the learned, shared, and transmitted knowledge of values, beliefs, norms and lifeways of a particular group that guides an individual or group in their thinking, decisions and actions in patterned ways’ (Leininger, 1991: 5–68). Health professionals in the UK consider language issues and knowledge of dietary practices to be key barriers to offering culturally sensitive care for minority ethnic communities (Wilson et al., 2012). However, ‘surface’ issues (like language) belie the multi-dimensional complexity of the influence of ‘deep structure’ cultural issues on engagement. These deeper issues are the cultural, historical, social, environmental and psychological factors that influence target behaviour in a given population (Resnicow et al., 1999). Resnicow et al. suggest that though surface issues influence initial engagement, it is the more nuanced understanding of deep cultural factors that influence salience and ultimately the efficacy of interventions and care. This understanding has informed the development of many successful interventions to support African American communities to achieve a range of health objectives (Berkley-Patton et al., 2019; Resnicow et al., 2004; Summers et al., 2013).
Theoretical models designed to inform the development of culturally sensitive care, all highlight the need to listen to members of the community that any service is intended to serve (Liu et al., 2012). Tension between cultural beliefs and practices and the provision of care has been suggested to present challenges for healthcare professionals providing diabetes care to AfC communities (Goff et al., 2020). However, research exploring the patient perspective is lacking (Majeed-Ariss et al., 2015). In addition, considering heterogeneity within UK Black communities is important; there are significant differences in migration patterns, countries of origin, religion and generational status across these groups. All these factors impact lifestyle habits, dietary choices and health behaviour (Leung and Stanner, 2011).
To help understand how best to provide support, the focus of research to date has been on health beliefs and cultural drivers (Alloh et al., 2019; Brown et al., 2007; Scott, 2001). In order to improve cultural competency of care, however, we need to understand how these factors intersect with the healthcare provision and how they influence adherence to recommendations. This study therefore focuses on the patient perspective and aims to explore factors which may facilitate engagement of Black AfC communities with self-management advice. The findings are of potential interest for both healthcare professionals and researchers designing health interventions to support these communities. The data were collected as part of the HEAL-D study (Goff et al., 2019).
Materials and methods
Study design
Experiences of diabetes self-management were explored using qualitative focus groups and an inductive approach to data analysis. Ethical approval was granted by the UK Health Research Authority (IRAS 1994991). This study is reported according to the consolidated criteria for reporting qualitative research (COREQ) guidelines.
Participants and setting
A purposive sample of adults of self-identified Black African (BA) or Black Caribbean (BC) ethnicity was recruited. 1 Inclusion criteria included a clinical diagnosis of type 2 diabetes, English speaking and living in London. Recruitment methods comprised mailings and leaflets distributed via general practitioner (GP) surgeries and Black majority churches and mosques, and at local cultural events. Attention was given to involving members of the community who were less likely to access the research process, and community advocates facilitated engagement.
Qualitative procedures
Eight focus groups, comprising four to eight participants, and stratified by gender and ethnicity, were conducted in community venues. Focus group methodology was chosen to explore similarities and differences of opinion between the participants. Each session lasted 2 hours, and each was audio recorded and transcribed. The topic guide was loosely structured to facilitate free discussion, and it covered four key topics – general attitudes to diabetes and diabetes care, dietary factors, attitudes to weight, and attitudes towards activity. Classic grounded theory methods were used for the data analysis (Timonen et al., 2018). Accordingly, coding proceeded from open-coding, through to selective and theoretical coding with Misalignment, Reconciling Perspectives and Trust being key categories. Emergent themes were grounded in the data using Glaser’s concept-indicator approach, and Spradley’s notion of semantic relationships was used to help identify inter-relationships between categories (Glaser, 1998; Spradley, 1979). NVivo software was used to organise the data. One author carried out the analysis (A.P.M.), and final concepts and themes were discussed and agreed with input from two further authors (L.M.G. and C.A.R.).
Results
The characteristics of the 41 participants are detailed in Table 1. Participants were primarily first-generation immigrants, and 44% were not educated above the age of 16.
Participant characteristics.
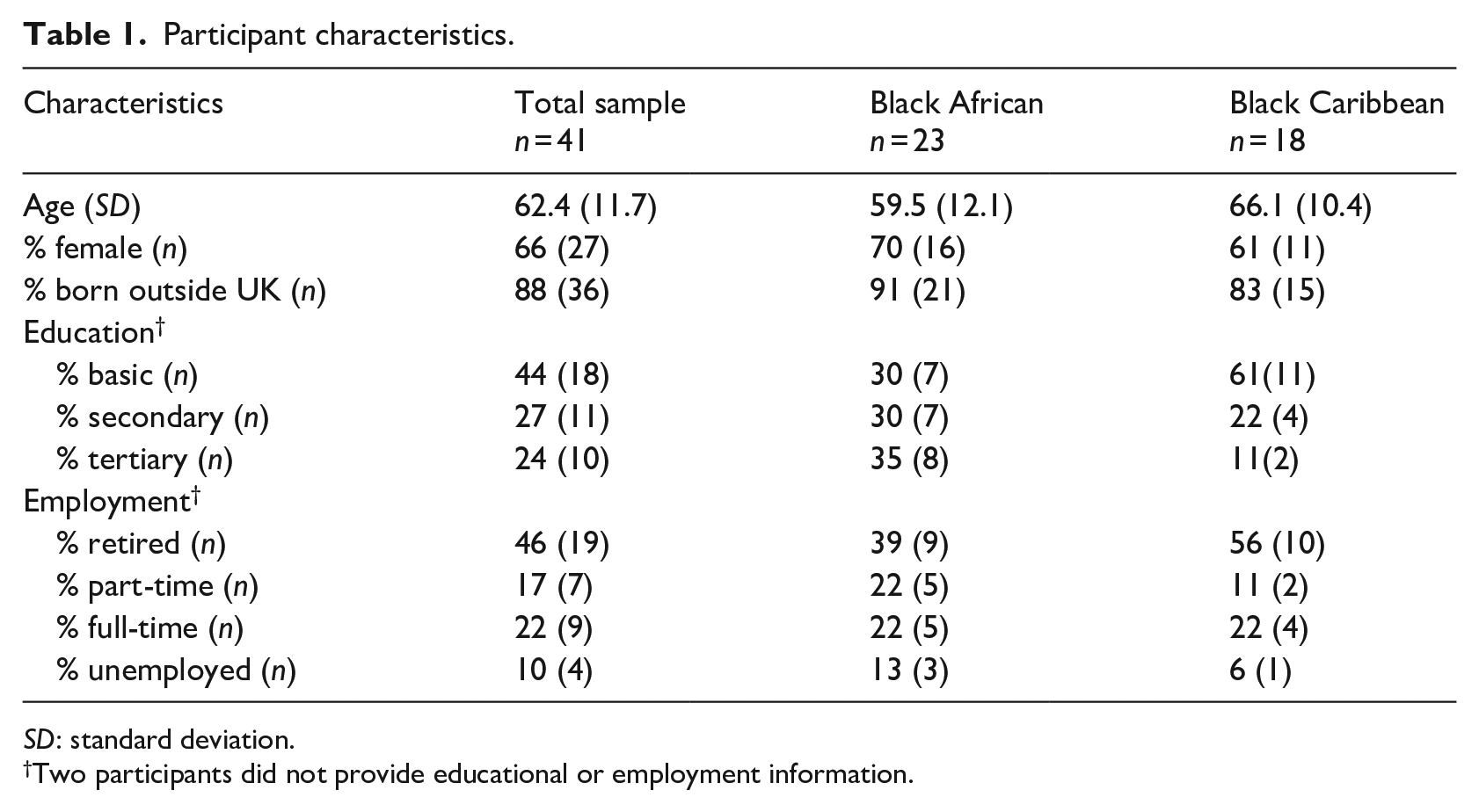
SD: standard deviation.
Two participants did not provide educational or employment information.
The key evident themes of Misalignment, Reconciling Perspectives and Trust are illustrated below.
Misalignment
Participants were engaged with medical care, but self-management advice presented challenges in the context of cultural influences on beliefs and health-related lifestyle norms. The influence of generational status appeared minimal, with even second-generation participants from both groups showing strong attachment to cultural norms and experiencing some degree of misalignment.
Tug of war with traditions
Cultural identity was strongly associated with dietary norms – traditional carbohydrates forming the mainstay of meals, oil and seasoning being used for flavour; consuming large portions and eating ‘’til you belly full’. Advice to reduce carbohydrate was felt to conflict with valued cultural practices and practically, changes were hard to make as starchy carbohydrates were central to staple recipes and socialisation. Many focus group participants described a taboo associated with diabetes which coupled with normative pressure to eat large portions of traditional starchy staples created a dilemma for those who would rather that others were not aware of their diagnosis. The social stigma was most evident among BA participants, although present in both ethnicities. Collectively, these factors created additional social pressures for those trying to change habits.
They will say, why are you having that small amala? Can we feed you? People were looking at me! (BA woman, age 72, Nigeria)
Even the most motivated struggled as they felt they need to give up traditional foods, as the following participant described: It has meant that for a lot of our food, I just don’t eat it anymore [. . .] It goes against everything everyone says you’re supposed to eat [. . .] So, for me it has meant a lot of don’t eat it. That has been the bottom line. For me it has been one of, OK . . . deprivation. (BA woman, age 50, Nigeria)
Advice to lose weight was difficult to reconcile with cultural associations of weight with prosperity and health in both genders, and with attractiveness and desirable maturity in women. This was a complex issue with the more health literate participants recognising that it was good not to carry excess weight. Yet, even knowing this, women still felt pressure from the perception of others: As you hit an age in terms of maturity . . . you want to look substantial. You don’t want to be perceived to be almost a young girl. (BA woman, age 63, Uganda)
A preference for using traditional natural remedies to treat diabetes was also evident for most participants of both ethnicities. They had faith in these approaches that were used widely among contemporaries. Conversely, their healthcare team prioritised medication as a first-line treatment, and individuals were advised against traditional remedies because of contraindications.
[The] doctor will advise you, say ‘I don’t give you, don’t take it’ he said ‘what I advise you to take, what I don’t prescribe you don’t take [. . .] you need to be careful of your organs. (BA, man, age 57, Sierra Leone)
Knowledge provision lacking cultural salience and sensitivity to existing beliefs
Knowledge needs were not fully met because the provision of information did not adequately address cultural lifestyle norms, nor was it sensitive to cultural nuances in understanding and illness representations. Knowledge and beliefs were culturally situated, and participants described explanatory models of illness that did not completely reflect the biomedical point of view (see online supplemental data). Participants reported fear and stigma associated with diagnosis and a tendency either to associate diabetes with external causes or not to be sure why it occurs. This inevitably reduced intention to follow advice when the links between the causes of diabetes and the treatment advice were not obvious. This was particularly the case for older male participants of both ethnicities.
People don’t know what give you ‘sugar’ – it must be the traits of the family or if it’s something you eat, or what? I don’t know. (BC man, age 84, Jamaica)
Confusion was evident in a number of areas, and knowledge gaps were identified (Figure 1). Translating dietary advice to traditional cultural foods was a key challenge as dietary advice was perceived to lack cultural relevance. Participants described a situation in which foods that were familiar to them were not generally discussed in conventionally structured education sessions. This left individuals uncertain about how portion size related to traditional starches. In some cases, lack of familiarity with nutritional classification meant that traditional starches were not necessarily identified as carbohydrate and hence were excluded from dietary change. Both ethnicities reported this issue. The quote below illustrates this, and this Caribbean participant went on to describe how, as a result of this confusion, she carried on eating larger portions of traditional starches as normal and just cut back on sugar.
I was telling them [in structured education] about breadfruit, they didn’t know what I was talking about, so they didn’t give us anything on West Indian foods. It was all about English foods! [. . .] so although you tried to soak some of it in, when I went home I was thinking ‘what levels of sugar are there in yam?’ (BC woman, age 54, UK)
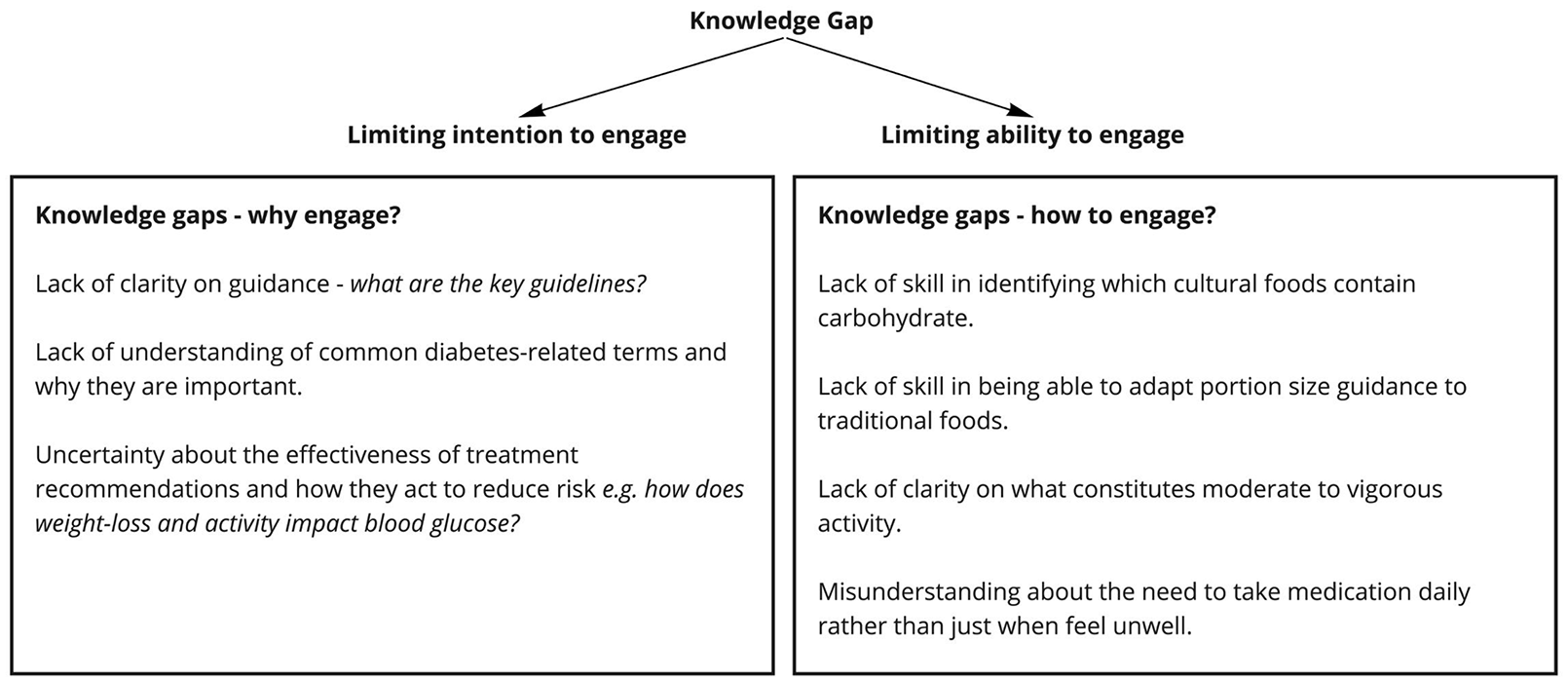
Knowledge gaps influenced intention and ability to engage with self-management advice.
While the health benefits of being active were recognised, individuals did not always appreciate the need to regularly meet the moderate/vigorous intensity recommended to support blood glucose control, nor what activities would meet the recommendations. When the doctor recommended use of leisure facilities, like the gym, this did not resonate with women. On the contrary, walking and dancing held cultural salience for both women and men.
Going to the gym is not in our culture, not in our culture at all. (BA woman, age 70, Nigeria) The people sing and dance and clap, even the old people they dance a lot. (BC man, age 49, Jamaica)
Expectations of care
Participants valued UK healthcare provision. Expectations of care, however, included an anticipation that cultural beliefs and practices, and Black identity should be respected. The automatic use of body mass index (BMI) charts considered inappropriate for the Black body shape and lack of appreciation of the importance of dietary and cooking traditions were examples of things participants found alienating.
They say that we’re obese because we’re heavy-boned and this and that because you’re measuring a black lady on a European chart. How are we obese? You’re telling us incorrect information because you’re going by British standards. [Our] English counterpart, they’ve not got batty [Creole: buttocks] . . . you’re going by a European chart . . . (BC woman, age 52, UK) They sent me to a dietitian, and she was saying, ‘Oh, you can have chicken, but literally just take it out of the packet and put it in the grill’, I had to let her know I’m proper West Indian and we season and fry our food and I can’t help that! (BC woman, age 54, UK)
Participants showed no strong desire for healthcare practitioners to be culturally matched with their own ethnicity, just that their healthcare providers could give them practical pertinent advice – ‘It’s all about the information [. . .] so it wouldn’t bother me. I don’t think I’d notice [their ethnicity]’.
Participants valued building a relationship with their doctor and felt short appointment times limited the chance to do so – ‘when I go the doctor [sic] its 5, 10 minutes then you have to go. Everyday it’s the same thing’ – and participants wanted to meet rather than receive information in writing: If we get to do the natural thing, come to you personal and sit down – you have explain. That’s what the doctor said come and see me. He doesn’t just written. He said I must come in and see him – I said I doesn’t want insulin. (BC man, age 76, Jamaica)
Furthermore, some individuals did not seem comfortable expressing needs and raising misunderstandings. The participant below explained how she did not understand the technical terms used, but did not seek clarification: . . . some big words. So, you know, big fancy words. With the diabetes, sometimes they say some word, like a BMI . . . You know, you just take the word and go . . . (BC woman, age 73, Jamaica)
For these participants, a direct prescriptive approach was preferred and some were left confused by the lack of clarity: And there are no real tools you’re being told you really must exercise. What does that mean? You really must lose weight. What does that mean? There are no tools when you’re being told that. (BA woman, age 50, Nigeria)
The degree of misalignment varied among individuals depending on the faith they have in the biomedical explanatory model and the degree to which they were personally influenced by community social norms. So, those whose knowledge and understanding of diabetes was similar to that of the healthcare provider and who had dietary and lifestyle habits more acculturated to the UK experienced less misalignment than those whose beliefs and habits were strongly driven by their ethnic identity.
Reconciling perspectives
Individuals went through a dynamic process of absorbing, facilitating knowledge and filtering as they reconciled the healthcare advice with their own perspective (Figure 2).
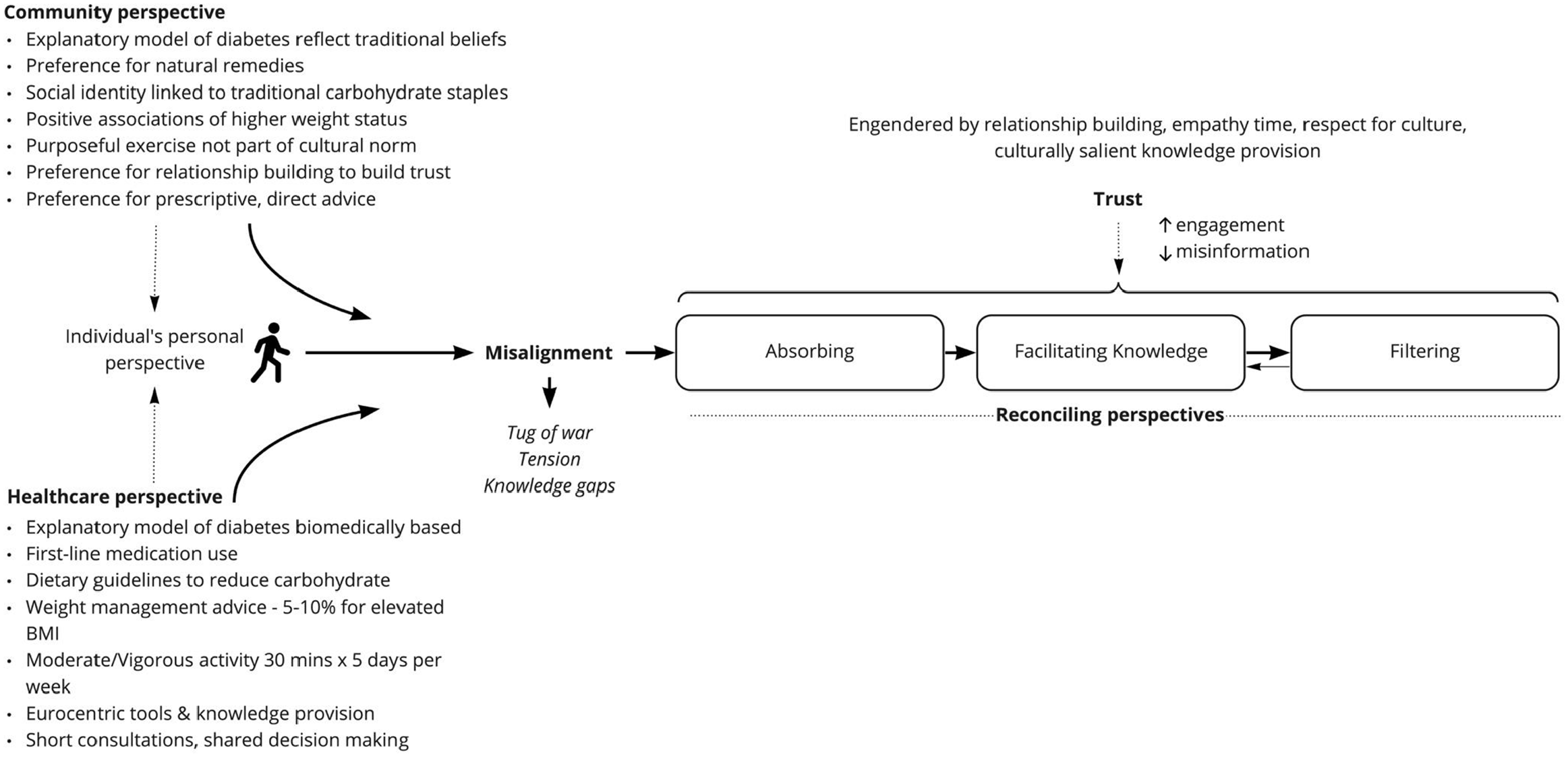
Illustration of the theory of reconciling perspectives.
Absorbing
Participants described absorbing the diagnosis in the context of their existing knowledge. The majority had witnessed the worst of diabetes: I had a bad experience . . . She was in a diabetic coma; she was in a coma for five years. It was very, very serious for us . . . Her muscles just collapsed and she died. That was a serious one to me . . . Awful thing [and] our friend lost his leg. (BC man, age 71, Guyana)
Yet this fear was often not acknowledged in the routine diagnosis, leaving individuals in shock and uncertain about the future: She said, ‘Do you drink?’ I said, ‘No’. ‘Do you smoke?’ I said, ‘No’. She said, ‘You’ve got diabetes’, and she just write me the tablets I should take. She never even told me it was type two diabetes. (BC man, age 75, Jamaica)
Those who had positive faith in the healthcare advice engaged quickly – ‘I knew it was a silent killer . . . I said no I will follow the doctor’s instructions’. However, those uncertain about the value of treatments and whether the condition could be controlled could disengage if not supported sensitively, for as long as a few years – ‘Every medicine I was prescribed at the time, I’d just dump it’. The main differentiator in the behaviour patterns here was related to health literacy and faith in care, and the patterns were consistent across ethnicities.
Facilitating knowledge
Those with less trust and faith in the treatment approaches offered turned to trusted sources in the community to verify what their health professionals advised. This included seeking more advice about medication and dietary advice or simply getting clarification on the technical terms used by their healthcare team, from people they trust. A reliance on trusted informal sources perpetuated misunderstanding in some cases, making adherence to recommendations less likely. The following participant explains how she changed her medication dosage unilaterally giving weight to advice from a trusted health professional within the family, over her doctor: She [Dr] put me on the tablets, one in the morning one in the evening but I have a nephew of mine in Trinidad that’s a doctor. So, I discuss this with him and he say what she’s given me . . . that for that level of sugar that’s too much. So, I started taking one a day. (BA woman, age 61, Nigeria)
Individuals reported listening to their body to understand when their blood sugar was high, rather than seeking empirical data, and taking medication sporadically in response to symptoms.
They put me on the tablets. So, I take one in the morning, one in the evening, sometimes I just take one and I just feel all right. (BC woman, age 60, Jamaica)
Informal sources, such as members of the church, provided an opportunity to ask questions and to seek clarity when individuals may have been reluctant to do this in the healthcare setting. Furthermore, faith settings, both church and mosque, were acceptable venues to receive medical information and created security.
When we get together our church, when we test [blood sugar] in back, she will explain, tell us, what does ketone mean . . . BMI then we get it more . . . I get it clearer. (BC woman, age 73, Jamaica) It’s very nice that this type of thing [healthcare advice] being delivered in the mosque giving awareness to other people that feel shy. (BA woman, no demographic data provided).
Those with more faith in healthcare however sought additional guidance from their healthcare team and researched medically aligned resources such as those provided by Diabetes UK. Even so, the most engaged individuals still lamented the difficulty in finding culturally relevant information about food.
I want to see more articles talking about the people that have done research on African foods [. . .] when you are trying to picture the African foods you want to look at it in terms of quantity, you can’t see that information for African foods. (BA man, age 41, Nigeria)
Filtering
Individuals decided how they personally would integrate the healthcare advice with their own perspective. The majority of participants felt the tug of war with traditions strongly, and they responded differently depending on their desire and external pressure to follow norms. Some remained resistant to the healthcare advice, being unwilling to significantly alter their habits and prioritising advice from trusted informal sources. These participants formed a significant percentage of the sample – ‘I can’t leave my African food. No matter what the doctor say’.
The next most common group of individuals interpreted the advice to be incompatible with their desire to follow cultural norms around weight and explained they would follow the health advice to a degree but only as far as it fitted within their cultural identity. This might involve losing weight, but not to the degree that it was noticeable; or reducing portion size, but resisting substituting foods or cooking in different ways. The quote below came from a participant who was very motivated and focused on his health yet was uncomfortable with losing weight to the extent others would notice.
Any weight loss that will be significantly noticeable, I don’t think I want to go to that extent. [. . .] because the culture from where I’m from, I can’t see my friend and say, ‘Oh, I’m diabetic’ . . . definitely weight, you are looking to start a different – explaining people . . . or you start avoiding people, avoiding places. (BA man, age 41, Nigeria)
A smaller group of participants with higher health literacy, including individuals of both ethnicities, prioritised health and were willing do whatever it took to manage their diabetes – this included giving up foods they loved or rationalising that, despite identifying with cultural body image ideals, they will strive to lose weight for the sake of their health – ‘In my mind, every time I lose a pound or two I’m less likely to get a foot ulcer’.
Trust and the positive influence of the patient–practitioner relationship
The inter-relational nature of the healthcare interaction had the potential to positively influence the outcomes of the process of reconciling perspectives. When there was a connected relationship, the participants placed more trust in the healthcare professional, they were more likely to discuss concerns, did not change the medicine doses unilaterally, more actively considered suggestions that contradicted the traditional perspective and were more motivated to do their best to follow the guidance.
So, myself and my doctor we have very good rapport. He called me, he said look at your record. ‘So, I’m saying that when you lost your business, that’s not the end of everything, you can bounce back but you need to have good health’. He encouraged me. (BA man, age 58, Nigeria)
Factors that increased trust included giving the patient time, relating to them as an individual, showing empathy, respecting cultural practices and beliefs with salient relevant advice, tailoring explanations and offering encouragement. The participant below described the change in her motivation when her dietitian made the advice more relevant to her cultural habits.
My first dietitian that I saw she said ‘oh don’t take this, don’t take that’ . . . then I was so anxious. [It] make me not want to listen. But the second dietitian I spoke to she knew our food. She had a model of fufu so it make me more welcome . . . that makes me more compliant listening to her because she knows what we eat. (BA woman, no demographic detail provided)
Discussion
This study explored the perspective of individuals of AfC heritage living with type 2 diabetes in the UK. Our findings suggest that cultural drivers strongly influence health beliefs, knowledge about diabetes, expectations of care and health behaviours. This culturally influenced perspective was at odds with a biomedically situated care provision and information provision shaped primarily for the general UK population. In the absence of the healthcare professional addressing these issues and building trust, individuals living with diabetes needed to reconcile the advice provided with their own cultural beliefs and practices in order to engage in self-management. In practice, individuals find it hard to fill the knowledge gaps and all but those with high health literacy, prioritise cultural affiliation over adherence to advice. These personal factors intersect with ethnicity and were evident in both BA and BC participants; while individuals need lifestyle advice pertinent to their personal cultural heritage, our data suggest health literacy, trust and the strength of ethnic identity transcend the ethnicity groupings commonly used in healthcare and may be pertinent factors to consider in developing support for these communities.
Identification of a potential disparity between individual lived experience of illness and the perspective of healthcare professionals identified in early medical anthropology studies (Kleinman, 1978) is central to the development of person-centred care in modern medicine (Hudon et al., 2012; Royal College of General Practitioners, 2021). Our data suggest this disparity may be accentuated in intercultural interaction where culturally situated experiences and influences shape both health beliefs and health behaviour. Evidence from systematic reviews suggests that in other ethnic minority communities in high-income countries, those living with type 2 diabetes share a similar experience to that of the UK AfC individuals that was identified in our data – with differences in beliefs about causes of diabetes and lack of common understanding about the treatments and controllability hampering understanding of advice (Majeed-Ariss et al., 2015; Wilson et al., 2012; Zeh et al., 2014). Alloh et al. (2021), in their study of West African immigrants, further suggest that the influence of social norms and health beliefs is diminished with UK residence and diabetes diagnosis in the UK setting. These data, together with ours, highlight the need for healthcare practitioners to actively address and explore individual health beliefs and psychosocial factors in order to improve engagement with diabetes self-management advice.
Furthermore, the particularly challenging issue of the diabetes advice perceived as conflicting with valued cultural dietary and health-related norms in our data has recently been described in UK South Asian communities (Patel et al., 2021). In their 2021 study, Patel et al. also reported that for those with strong cultural identity, cultural traditions were given preference over diabetes self-management advice unless the misaligned understandings were addressed by the healthcare team. An unresolved intercultural mismatch between the healthcare professional’s perspectives and those of the patient can result in disengagement, frustration and distrust (Degrie et al., 2017; Rothlind et al., 2018).
Gaps in knowledge due to lack of salience of advice have previously been reported in BC communities, although prior to the more recent shift to prioritising culturally competent care (Scott, 1997, 1998). Around 20 years has passed since these earlier reports, and our data highlight both that this disparity continues and that despite motivation to engage, this lack of knowledge hampers the ability of individuals to adhere to guidance. Our data suggest these issues are also evident for those of BA ancestry.
The data also highlight the importance of information-seeking behaviour to help supplement the healthcare information provision which is perceived to be incomplete. For all individuals, this proved challenging but particularly so for those with lower health literacy with less trust in their healthcare team. The trust placed in informal sources shown by participants of both ethnicities has previously been reported in BC communities in the UK (Scott, 1998). However, our data highlight that reliance on trusted sources outside the healthcare team may both reduce adherence and perpetuate misinformation but also may be positive and helpful. The value of leveraging trusted community support in diabetes self-management for communities of African heritage is evident in the USA (Creamer et al., 2016), with interventions in faith-based settings being shown to be particularly helpful (Ammerman et al., 2002; Summers et al., 2013). Community partnerships with Black majority churches have also been suggested as a valuable approach to supporting Black British communities (Harding et al., 2018). Empowering trusted members of the community to support self-management in partnership with healthcare has potential to reduce the misalignment patients experience and to provide a trusting environment for improving knowledge. However, community advocates still need to be equipped with culturally relevant, evidence-based tools to address the specific gaps in knowledge identified.
Our data suggest that when trust is established between the patient and healthcare team, it can help improve engagement and nudge adherence to recommendations. Participants did not expect healthcare practitioners to have a perfect understanding of their cultural traditions, nor did they express any need for cultural concordance. Nevertheless, they did expect first, that healthcare professionals should respect the difficulty of receiving a diabetes diagnosis, given the context of their, often harsh, experience of diabetes. Second, they expected healthcare professionals to understand that self-management might pose a particular challenge in the context of social norms and beliefs. This is an important aspect of person-centred care (Hudon et al., 2012), and the powerful positive effects of trust between doctor and patient are well-described in the literature (Birkhauer et al., 2017; Brown et al., 2017). Moreover, traditional African cultures are relationship-driven, collectivist cultures (Di Noia et al., 2013) and therefore it is unsurprising that when individuals felt they were given time to develop a personal relationship with their doctor, this appeared to improve both engagement and trust. The importance of building personal relationships in healthcare consultations is supported in the literature on both intercultural (Degrie et al., 2017; Rothlind et al., 2018) and ethnicity-concordant interactions (Birkhauer et al., 2017; Mazzi et al., 2016). However, our data also suggest that shared decision-making, central to the philosophy of person-centred care, may not sit comfortably with the natural less-assertive communication style of some who have expectations of a more paternalistic approach. Navigating these differences can be positively influenced by putting an emphasis on patient empowerment and helping improve patient health literacy (World Health Organisation, 2013). However, recognising and addressing cultural preferences is also important for healthcare practitioners providing culturally competent care (Purnell, 2002).
Qualitative methods in particular are well suited to exploring the participant perspective and grounded theory, emphasises an inductive approach to capture the key concerns (Glaser, 1998). In this study, an effort was made to recruit a diverse sample. Inevitably, however, acculturating influences mean that the findings present a current snapshot, and representative views will change as more second-generation individuals develop diabetes. In addition, the London Boroughs where the research was conducted have a high density of minority ethnic communities, many of whom tend to live in more economically and social deprived circumstances (Joseph Rowntree Foundation, 2017). The experience of participants may not therefore, necessarily reflect that in other settings where healthcare teams may have less experience of supporting minority ethnic communities and where the social conditions may be more affluent. We also recognise that there is considerable diversity between and within communities of BC and BA heritage, and as such, these are homogenising ethnic groupings. Our objective, however, was to consider how best to support members of these communities within the healthcare setting, limiting the degree of granularity to that which is practically useful.
Conclusion
This study highlights that despite policy advances to address health inequalities, those in UK AfC communities still experience inequities. The findings suggest potential opportunities to improve the cultural salience of type 2 diabetes self-management advice. The healthcare interaction can be pivotal in improving trust, engagement and reducing misinformation. In addition, appropriately informed community support offers potential to improve equity of access. These findings may be of value to healthcare practitioners supporting these communities as well as to health researchers.
Supplemental Material
sj-docx-1-hej-10.1177_00178969221108563 – Supplemental material for Misalignment: understanding the challenge of engaging with self-management advice for people living with diabetes in UK Black African and Caribbean communities
Supplemental material, sj-docx-1-hej-10.1177_00178969221108563 for Misalignment: understanding the challenge of engaging with self-management advice for people living with diabetes in UK Black African and Caribbean communities by Amanda P Moore, Carol A Rivas, Seeromanie Harding and Louise M Goff in Health Education Journal
Footnotes
Acknowledgements
Thanks go to The Muslim Association of Nigeria; Baitul Rahman Masjid Mosque; The Latter Rain Outpouring Revival Church, Peckham; and St John’s Church, Peckham.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. This study was supported by a National Institute of Health Research (NIHR) Career Development Fellowship awarded to Louise Goff (CDF-2015-08-006). Amanda Moore was supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care South London at King’s College Hospital NHS Foundation Trust. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.