
Abstract
Objective:
Engaging in healthy behaviour while studying at university is a defining factor in terms of its impact on a person’s later health in life. Therefore, university students are a priority when it comes to health education interventions. This article describes the development and implementation of a web-based health programme intervention to enable students to acquire knowledge and strategies to allow them to make decisions that favour their health by adopting healthy and positive behaviours.
Design:
The design of the Health On You programme was based on the PRECEDE-PROCEED model and used an online platform designed to facilitate self-learning using interactive teaching strategies. The programme included six modules focusing on the following topics – Drinking responsibly; Living free of smoke; Saying no to illicit drugs and to self-medication; Balanced, Healthy and Sustainable Diet; Moving Yourself; and Preventing Sexually Transmitted Infections.
Setting:
Data collection took place in a public university in northern Portugal.
Method:
In 2021, a cross-sectional study was carried out with a convenience sample of 37 students attending a Portuguese university to assess the implementation process.
Results:
Overall assessment of the programme was fairly positive – 5.00 (with 5 being the highest mark), as well as for each of its developed modules (mean scores, 4.66–5.00).
Conclusion:
The Health On You programme appeared to be an innovative web-based health intervention due to the broad-based approach it adopted, both in terms of the topics tackled and the variety of teaching and learning strategies used to address each of the modules.
Introduction
Research on health education in higher education is growing both nationally and internationally, with universities and colleges being seen as places in which to encourage the development of lifelong healthy behaviours (Amare et al., 2019; Arsandaux et al., 2020; Bennett and Holloway, 2017; Xu et al., 2019). The focus on health education in higher education has been stimulated by a number of developments including the Sustainable Development Goals (SDG), especially SDG3 and its guarantee of access to good quality health and well-being for all. In the USA, Healthy People 2030 (US Department of Health and Human Services, 2021) sees young adults, and in particular university students, as a priority social group, and Healthy Campus 2020 (American College Health Association, 2018) has developed guidelines to encourage the implementation of wellness and health programmes in universities.
In the scientific literature, several studies with computer-based or web-based EPS programmes have demonstrated feasibility, acceptability and effectiveness among university students (Bailey et al., 2012; Broekhuizen et al., 2012; Hutchesson et al., 2015; Oosterveen et al., 2017; Webb et al., 2010) and positive effects on health behaviour (Visser et al., 2020; Webb et al., 2010). To date, these programmes have mostly implemented in non-formal settings since, although they take the form of systematically organised educational activities, they are often carried out outside the official education system and are, therefore, not mandatory (Inter-agency Network for Education in Emergencies, 2010). Scientific studies that include web-based health education strategies in a non-formal context are increasingly common (Gabarron et al., 2018; Hsu et al., 2018). Health education actions in higher education are increasingly urgent because, on the one hand, the number of young adults in this context has been increasing over the years; and on the other hand, higher education institutions have the infrastructure (in the form of technology, facilities and specialised professionals) to become health-promoting spaces capable of fostering change in individual and collective health behaviours.
Against this background, this article describes the process of developing and implementing a web-based health education to provide university students with the knowledge and strategies to enable them to make healthy decisions and adopt positive health behaviours in their everyday lives.
Programme design
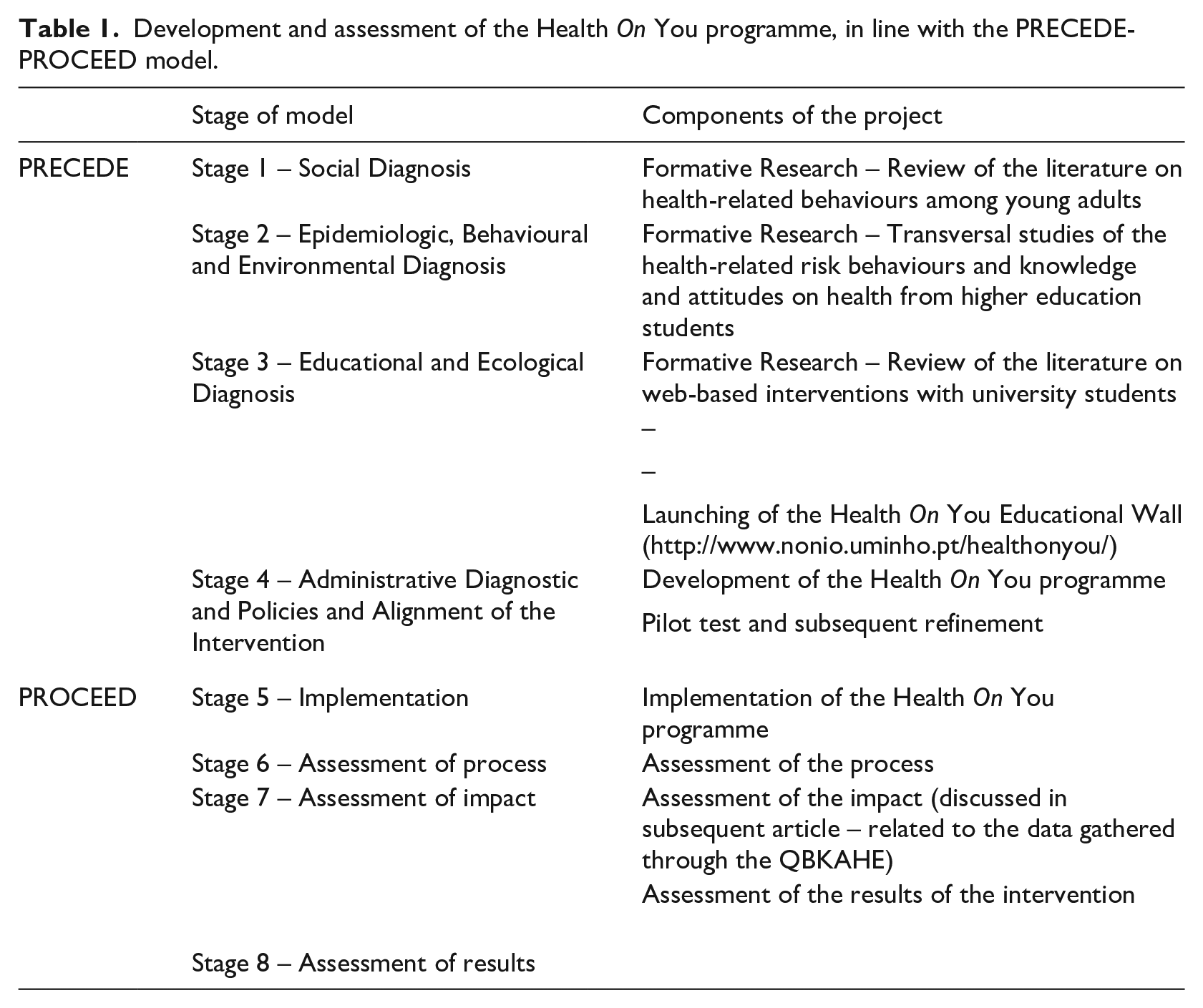
The development of the Health On You programme was informed by the PRECEDE-PROCEED model (Green and Kreuter, 2005). This model has frequently been used for intervention development in health education for university students (Ashton et al., 2017; Whatnall et al., 2019). It is implemented in eight stages: the first four stages (PRECEDE) serve the purpose of planning and evaluating the needs of those involved, while the PROCEED component (the second four stages) involves implementation, process evaluation, progress with results and impact.
Table 1 offers a general overview of the PRECEDE-PROCEED model and a description of how each component was implemented in this study.
Development and assessment of the Health On You programme, in line with the PRECEDE-PROCEED model.
Intervention development
Stage 1: social diagnosis
Stage 1 focused on identifying the necessary information to guide intervention development, specifically for higher education students. In this regard, a number of literature reviews took place in relation to previously identified risk behaviours among higher education students (excessive consumption of tobacco, alcohol and illicit drugs; self-medication; unbalanced diets or eating habits; insufficient physical exercise’ and unprotected sex). The studies identified in these reviews highlighted the need to create a health education programme for delivery in higher education.
Stage 2: epidemiologic, behavioural and environmental diagnosis
Environmental and behavioural factors were explored in this stage, which focused on an analysis of risk behaviours for students’ health (Alves et al., 2021a, 2021b, 2021c, 2021d, 2022; Alves and Precioso, 2020) and identified the environmental factors on campus that might negatively affect the students’ health, such as vending machines selling high-calorie food and nearby restaurants offering unbalanced meals, coffee shops and bars selling alcoholic drinks, and tobacco sales in kiosks. Health-related services on campus were also identified, including areas for physical activity and a canteen with meals carefully planned by a nutritionist. This information enabled an understanding of how environmental factors might or might not support unhealthy habits and provided evidence for environmental and political change.
Stage 3: educational and ecological diagnosis
Stage 3 was based on the logic model derived from stage 2, and identified from the available literature predispositional (information and beliefs/attitudes), reinforcing (abilities and resources/instruments) and facilitating factors (influence of the social environment and surrounding people) that could impact health behaviour (Green and Kreuter, 2005). The studies reviewed at this stage included those focusing on knowledge and attitudes towards adopting healthy behaviours and the influence of peers on certain risk practices (Alves et al., 2021a, 2021b, 2021c, 2021d, 2022; Alves and Precioso, 2020).
At this stage, the review of available literature intended to identify the potential efficacy of web-based interventions and those that were most relevant to university students. When it comes to changing health behaviour (Cugelman et al., 2011; Kohl et al., 2013; Webb et al., 2010), this type of intervention is increasingly common and had numerous benefits when delivered via the Internet: 24/7 accessibility; a pace of delivery tailored to each individual; the guarantee of anonymity (a very valuable aspect for young adults who may be ashamed when asked particular questions, for example, on the use of condoms); the possibility of maintaining and updating interventions; and the possibility of providing individual and personalised forms of learning (Cugelman et al., 2011).
The intervention described here was derived from other web-implemented interventions developed for university students, such as M-PASS (Barretto et al., 2011; Bingham et al., 2011), a brief, theory-based motivational intervention consisting of four web-based sessions to prevent and reduce risky drinking among first-year college students. It was also informed by AlcoholEdu (Paschall et al., 2011), a five module Internet-based alcohol misuse prevention course aimed at first-year students. Other programmes that informed its development were (for tobacco) the web-based programme Questions Sharing and Interactive Assignments (QSIA) (Essa-Hadad et al., 2015) and (for marijuana) the Cannabis eCHECKUP TO GO (also called e-TOKE) (San Diego State University Research Foundation, 2009), a brief online intervention offering individualised feedback about perceived use norms, the money spent on cannabis, consequences of its consumption and strategies to reduce the latter. The Eating Advice to Students (EATS) (Whatnall et al., 2019) web-based nutrition intervention for university students also adopted the approach utilised here, as did the Web-based Nutritional Health Education Module (El-Refaay et al., 2017), which has been described by experts and university students as comprehensive and focused on strategies that encourage students to adopt healthy eating habits. More generic approaches that informed the development of Health On You included Active Transition (Kwan et al., 2013), a password protected website hosted on the university portal, designed as an informative 6-week forum in which weekly topics are presented on behavioural, normative and control beliefs related to physical activity (goal setting, action planning, relapse prevention and behavioural maintenance), and F.O.R.E. Play (Moore et al., 2012), which was developed to provide students with information or a means obtaining it on the prevalence and prevention of HIV and other sexually transmitted infections.
Stage 4: administrative and policy diagnosis, and alignment with the intervention
Stage 4 centred on determining the intervention components deemed necessary to carry out an awareness-raising campaign on the need for changes in behaviours identified in previous stages, taking into account available organisational and administrative resources. According to the authors of the PRECEDE-PROCEED model, this phase requires engagement with behaviour change theories to support intervention goals. In this case, intervention development was based on the Triadic Theory of Influence (TTI) (Flay and Petraitis, 1994) because its meta-theoretical structure allows the grouping together of multiple theories relevant to behaviour change among young adults (Ashton et al., 2017). The guidelines developed by Brendryen et al. (2013) influenced the work.
During this stage, a project logo was developed, as well as the programme’s educational wall (see http://www.nonio.uminho.pt/healthonyou/) and digital platform, containing links to additional information, tips on the adoption of healthy behaviours, interactive questionnaires for behavioural self-assessment, and access to the digital platform on which the intervention programme was hosted.
The programme
The Health On You programme is a theory-based web-based intervention to promote the adoption of positive health behaviours by students in higher education. It aims to promote university students’ understanding of information, skills and behaviours related to tobacco use, alcohol use, illicit drug use, medication, eating habits, physical exercise and sexuality. It also aims to make available psychosocial strategies to bring about change in health-related behaviours. Subsequent to the intervention, students are expected to adopt more positive health behaviours, by applying the preventive strategies learned. In addition, students involved in this programme are expected to positively influence the health behaviours of their peers.
The different intervention components were made available on the password protected thinkific.com platform. This platform allows for updating and the addition of new contents, including data-collection instruments to monitor participants’ activity and store the data generated throughout the study.
The Health On You programme itself comprises six modules sub-divided into a series of mini-sessions, focused on the abovementioned topics: Responsible Drinking; Living smoke-free; Saying no to illicit drugs and to self-medication; Balanced, Healthy and Sustainable Diet; Being active; and Preventing Sexually Transmitted Infections. In an introductory session, a welcome message is shown, and an explanation given on how the platform works. The objectives of the intervention are stated, and a motivational message pops up to inspire participants.
The short sessions were designed to be interactive so as to promote the adoption of healthy behaviours and help young people resist the social pressure(s) they experience at university. During the programme, different pedagogical practices and strategies are used to promote positive health-related behaviours: Campus Focus, in the form of a graphic, shows the prevalence of particular health-related behaviours in higher education settings. Website Health aims to complement the information provided in a specific module and allows web interactivity. Top 10 consists of a list of practical and relevant health tips. Voices consists of a number of short testimonials by university student testimonials. Preventive Strategies is a list of advice on the prevention of certain risk behaviours. Strategies for Change comprises a checklist for behaviour change. To reflect upon contains questions to trigger self-reflection and thought about health-related behaviours. Finally, Health Videos comprises a series of videos developed specifically for this programme containing a number of motivational strategies.
A bibliography is attached to each module to satisfy the needs of those wanting more information, along with a questionnaire designed to evaluate the module. A detailed description of all the intervention components is available as an online Supplemental File.
Methods
The study was approved by the Ethics Committee for Research in Social and Human Sciences (CEICSH) at the University of Minho Ethics Council, under protocol CEICSH 009/2019. Implementation took place between April and May 2021, after obtaining students’ informed written consent to participate in the programme.
Participants and recruitment
Participants were recruited from one higher education institution in the North of Portugal. An email was sent to all (N = 64) students attending three Master’s degree courses in the social sciences and humanities, inviting them to participate. Of this potential sample, 37 consented to participate in the study, yielding a response rate of 57.8% from all programme candidates. The students who participated in the programme were almost young women (n = 36, 97.3%) aged 21 to 23. All were full-time students living with their parents or family members and were predominantly single and not in a romantic relationship (n = 23, 62.2%).
Instruments
Our assessment of the intervention was divided into three parts: diagnosis (related to previous conditions), monitoring (with a focus on process evaluation) and results (concerned with students’ overall appreciation of the programme).
Diagnosis – Identification of Expectations
Before beginning the programme, participants were invited/asked to complete a questionnaire consisting of three open questions, which allowed an assessment of (1) motivations (‘What is your motivation to participate in this Programme?’), (2) expectations (‘Complete the sentence: After participating in this programme, I will be able to . . .’) and (3) anticipated obstacles (‘What is your main obstacle to participate in this Programme?’). In addition, the students were invited to complete a second questionnaire on ‘Health Behaviours, and Knowledge and Attitudes in Higher Education’ to assess the intervention’s potential impact on future health knowledge, attitudes and behaviours.
Monitoring – Assessment of Modules Scale
This scale, adapted from Jardim and Pereira (2006), was administered at the end of each module, allowing students to express their opinions on 23 items divided into five categories as follows: (1) overall appreciation of the module – 5 items (e.g. ‘The organisation of this module was . . .’); (2) objectives – 4 items (e.g. ‘The suitability of the strategy achieve the objectives was . . .’); (3) contents – 7 items (e.g. ‘The theoretical knowledge transmitted was . . .’); (4) activities – 4 items (e.g. ‘The practical usefulness of the proposed activities was . . .’); (5) development – 3 items (e.g. ‘The stimuli given to continue to strengthen the developed skills were . . .’). Each of these items was evaluated using a 5-point Likert-type scale (‘bad’, ‘poor’, ‘satisfactory’, ‘good’ and ‘very good’). In addition, sociodemographic questions were included to understand the relevance of each module to student characteristics.
Results – Scale of Assessment for the Implementation of Programme
This scale was utilised to assess the programme’s quality (adapted from Jardim and Pereira, 2006). In all, 28 items were selected and placed in five categories as follows: (1) overall appreciation of the module – 6 items (e.g. ‘The results achieved were . . .’); (2) objectives – 4 items (e.g. ‘The clarity of the objectives of the programme was . . .’); (3) contents – 10 items (e.g. ‘The overall coherence/interconnection of the themes was . . .’); (4) activities – 5 items (e.g. ‘The activities carried out in the modules were in general . . .’); and (5) development – 3 items (e.g. ‘The stimuli given to continue to deepen the developed skills were . . .’). Each item was evaluated using a Likert-type scale (‘bad’, ‘poor’, ‘satisfactory’, ‘good’ and ‘very good’). In addition, students were asked to complete the Questionnaire about Health Behaviours, Knowledge and Attitudes in Higher Education again to analyse differences before and after the intervention.
Procedure and data analysis
All intervention components were individually pre-tested with five volunteer students to ensure understanding and interest in the sessions, clarity of language and visual presentation. Changes made following the pre-testing included improving the colour scheme used, adding instructions on how to use the platform and reducing the amount of detailed information provided by using videos specifically made for the purpose. The health education specialists involved in the pre-testing considered the objectives of the sessions clear and the contents adequate and up-to-date. The platform design was considered appropriate in terms of font size and style, as well as the use of bold to highlight the most critical content. The students considered that the programme was beneficial to their peers and that the contents covered would promote an increase in knowledge, as well as support the adoption of positive health behaviours. No difficulties were reported on the use of the platform.
In total, 35 hours (over 2 months) were expected to be needed to complete the programme, depending on the depth of understanding desired by each student. One month after the start of the programme, reminder emails were sent to participants to encourage its completion, and following its completion, all participants received another email with a certificate of course completion. All participants had a designated tutor in the form of the principal investigator of this project, to interact with and who provided online support throughout the programme.
The Identification of Expectations Questionnaire (IEQ) was filled in and answered immediately after accessing the programme, before the beginning of the first module; while the Assessment of Modules Scale (SAM) and Scale of Assessment for the Implementation of Programme (SAIP) were filled in at the end of each module and at the end of the programme, respectively. Completing these scales took around 5 minutes.
The Statistical Package for the Social Sciences (SPSS) (version 26.0) was used to analyse the data gathered. In what follows, the higher the average on a scale, the higher the satisfaction with each of the categories within that scale (0–5 range). The QIE’s open questions were subjected to content analysis to create explanatory categories for each of the questions.
Results
The analysis confirmed that student expectations regarding the programme were broadly of three types: to improve the professional skills to help others (referred to by 19 out of 37 students), to live a healthier life and improve health-related behaviours (referred by 15 students out of 37), and to increase knowledge (referred by 12 students out of 37).
Every participant pointed out that their main motivation for participating in the programme had been to learn, whether about their health and lifestyle or about intervention programmes that might include their family members, friends and the overall community. The only obstacle mentioned by participants was the lack of time to take part in it while undertaking their other academic and professional activities or carrying other responsibilities.
Table 2 summarises the average ranking given to the components of each module and the programme overall, showing quite good positive satisfaction. The answers indicated that the participants were positive in their overall appreciation of the modules (mean scores, 4.66–5.00), and considered the objectives, contents and activities in each module appropriate (mean scores, 3.45–4.59; 4.76–5.00; 3.45–4.54, respectively).
Rankings for global appreciation, objectives, contents, activities and development of modules and programme components. a
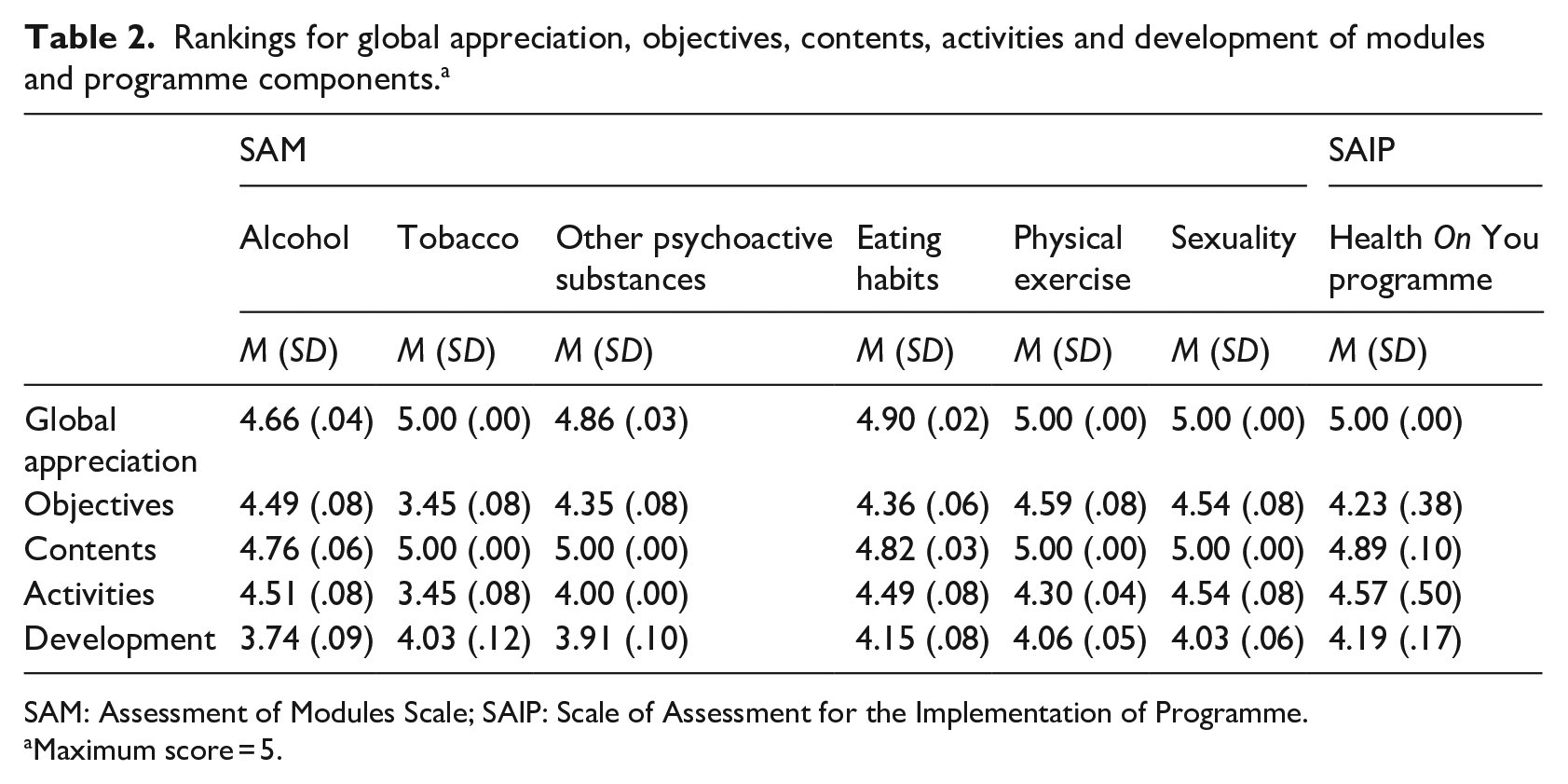
SAM: Assessment of Modules Scale; SAIP: Scale of Assessment for the Implementation of Programme.
Maximum score = 5.
Discussion
Health education in higher education is key to preventing the adoption of risk or harmful health behaviours among students. This study describes the development and preliminary evaluation of the Health On You programme as a solution to the challenges university students may face in adopting positive health behaviours. The expectations and motivations of participants aligned with those of other studies, in which students considered it valuable to acquire knowledge about health and have access to health education resources (Xukai, 2019).
This study showed the value of intervention focused on multiple behaviours, taking into account the fact that an ideal intervention should aim to simultaneously change and improve several risk behaviours (Prochaska et al., 2008) and evidence locally of the existence of complex risk behaviour profiles among university-age students (Alves et al., 2021b). Our analysis of existing health education intervention programmes in higher education revealed that scientific articles rarely describe in-depth the development, implementation and evaluation of the intervention (Barretto et al., 2011; Bartholomew et al., 2016; Fernandez et al., 2019). In this study, we attempted to remedy this deficit using the PRECEDE-PROCEED model as our guide. The implemented methodology can be used by other researchers and professionals in the field to increase the transparency and credibility of the intervention development process and the obtained results. Findings from this study showed that one of the main barriers mentioned by the students to adopting healthy behaviours was lack of time. Although the developed programme sought to address this dimension, it makes sense for higher education institutions to invest in organisational development to allow for this. Given the association between well-being and avoidance of health risk behaviours, the future development of the Health On You programme would benefit from the inclusion of a module on well-being in higher education, to enable the acquisition of skills relevant to life at university and to address topics such as emotional regulation, self-esteem, critical thinking and assertiveness.
Socio-educational programmes to promote positive health behaviours should aid the development of social and personal skills to deal with situations and social contexts of risk, especially the skills needed to resist emerging peer pressure, which means strengthen assertiveness and self-efficacy (Mbuthia et al., 2017; Pinchevsky et al., 2012). The Health On You Programme engaged with these issues with a focus on how to create healthy habits and prevent risky behaviours. However, future work might benefit from the use of a peer education model as a means of promoting healthy behaviours (Webel et al., 2010; Yan et al., 2014). The use of strategies such as peer counselling (Quintiliani and Whiteley, 2016) and peer support (Crisp et al., 2020) may also be justified, with the Health On You programme being used to train older students to become health-promoting agents in higher education settings.
Limitations
A key limitation of the study derived from students’ voluntary participation. Since the involvement in the programme was voluntary, this may suggest that participating students were more interested in and receptive to the adoption of positive health behaviours. This may have left out those students who would benefit from this type of programme because they have a higher prevalence of risk behaviours. In addition to this limitation, the study included a relatively small sample and no control group. So, although the study allows us to draw preliminary conclusions to guide future intervention studies, the results should be interpreted with caution. In terms of programme design, one of the disadvantages of using a web-based format was that it was difficult to measure the quantity and quality of interaction participants had with the web programme, despite the opportunity to comment on each of the sessions. Moreover, even though incentives were provided to encourage students to participate in group forums on the sessions, few comments were made. Furthermore, participants should have been asked what they thought about the web-based intervention format, and the inclusion of this information would have helped validate (or otherwise) the format adopted by the intervention.
Conclusion
Higher education institutions are key settings in which to help students develop healthy lifestyles. In the same way as academic learning, they provide opportunities for the development of health skills and understandings that will be valuable in later life. Web-based interventions such as the Health On You programme have the potential to be implemented nationally. The results of this study reveal an overall positive appreciation of the programme with the potential to facilitate lifestyle changes and reduce risky health behaviours among university students.
Supplemental Material
sj-docx-1-hej-10.1177_00178969221107876 – Supplemental material for Health On You programme: Development and implementation of web-based health education intervention for university students
Supplemental material, sj-docx-1-hej-10.1177_00178969221107876 for Health On You programme: Development and implementation of web-based health education intervention for university students by Regina F Alves in Health Education Journal
Footnotes
Acknowledgements
The authors thank the reviewers, the journal’s editor-in-chief and José Precioso for their thoughtful comments and help in improving the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. This work was supported by the Foundation for Science and Technology – FCT (Ministry of Education and Science, Portugal) (SFRH/BD/120758/2016).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.