
Abstract
Objective:
To examine the impact of a self-determination theory-informed school-based lunchtime games intervention on wellbeing and symptoms of anxiety and depression among adolescent girls in Ireland.
Design:
Non-randomised controlled intervention design.
Method:
This self-determination theory-informed intervention consisted of lunchtime games for girls aged 13 ± 0.7 years, 3 days a week. After a 2-week ‘sampling’ period, students self-selected to 0, 1, 2 or 3 days of lunchtime games. Intervention and control groups were compared by pre- and post-testing. Participants were included in the intervention design via a survey to ascertain the most popular games and activities at the outset.
Results:
Participating in games twice a week led to significant decreases (p < .01) in symptoms of anxiety and depression while the control group showed significant increases (p < .01) in symptoms of anxiety and depression. Mental wellbeing significantly (p < .01) increased among those who participated two and three times a week. Increases in mental wellbeing were similar in effect size to increases in self-efficacy.
Conclusion:
Higher frequencies of physical activity led to increased mental health. Self-efficacy may act as an underlying mechanism for increases in mental health through physical activity.
Introduction
A number of lifestyle-related health problems have increased among children and adolescents over the past 20 years in high-income countries, especially in Northern Europe (Potrebny et al., 2017), with symptoms of anxiety, depression and stress being the most common (NICE, 2011; Rehm and Shield, 2019). Together, these issues account for 10%–14% of the global burden of disease (Schofield et al., 2019; World Health Organization, 2018), with further evidence indicating that mental health issues account for 183.9 million disability-adjusted life years (Schofield et al., 2019). The Global Burden of Disease study (James et al., 2018) reported that anxiety and depressive disorders are among the top four leading causes of the disease burden among young people in Western Europe. Internationally, a larger proportion of young women report mental health issues when compared with young men, although both follow a similar pattern of increase over time (Dooley et al., 2019; Murphy et al., 2020). Ireland has among the highest reported rates of depression among adolescents in Europe (Eurostat Statistics Explained, 2018). One-third of Irish young people, aged 12–19 years, were found to be suffering from either depression or anxiety, with girls reporting higher levels of mental health difficulties than their male counterparts (Dooley et al., 2019; Murphy et al., 2020). In a positive sense, wellbeing is a key indicator of health and refers to an individual’s optimal psychological functioning (Deci and Ryan, 2008; Dodge et al., 2012).
Evidence to support the positive physiological benefits of physical activity is well established. A body of evidence is also growing to support the benefits of physical activity for positive mental health outcomes, such as wellbeing, and the prevention of negative mental health outcomes, such as depression and anxiety (Biddle et al., 2019; Murphy et al., 2020). Many children and adolescents fail to meet the recommended levels of physical activity internationally, and specifically in high-income countries (Hallal et al., 2012; WHO, 2011), with Ireland being no exception (Murphy et al., 2020; Woods et al., 2019). Recent cross-sectional analyses found 10% and 8% of Irish young people aged 12–19 years achieved the recommended levels of physical activity (Murphy et al., 2020; Woods et al., 2019). Physical activity levels were also found to decline with age in both boys and girls as symptoms of anxiety and depression increased (Dooley et al., 2019; Murphy et al., 2020), suggesting an association between increased levels of physical activity and increased mental health as has been previously identified in cross-sectional (McMahon et al., 2017) and experimental (Gordon et al., 2021; Goldfield et al., 2015) studies. Internationally, and in Ireland, women have consistently reported higher symptoms of depression and anxiety, and lower levels of wellbeing and physical activity (Dooley et al., 2019; Murphy et al., 2020; Woods et al., 2019). Reductions in physical activity throughout adolescence are also more common in girls than boys (Bradley et al., 2011; Woods et al., 2010). Suggested factors for this reduction in physical activity are a lack of enjoyment, lack of purpose or meaning in the activity, and unfair treatment or negative relationships with coaches (Farmer et al., 2018), all of which may lead to lowered self-esteem, therefore negatively impacting mental health outcomes psycho-socially and behaviourally. Consistent findings of lower physical activity participation by girls, coupled with a lower proficiency of movement skills (O’Brien et al., 2016) and poorer mental health outcomes, suggest that there is a need for more and specifically tailored physical activity interventions for Irish adolescent girls.
Interventions to improve physical activity levels have been trialled across a variety of contexts with varying degrees of success. One of the most promising areas, due to the ease of recruitment and controlled environment, is the school setting. A key area of school-based physical activity research that has gained momentum is the implementation of strategies during school breaks (Hyndman et al., 2012, 2014). Several interventions targeting school breaks have successfully attempted to counteract declining physical activity by implementing active supervision (Sallis et al., 2003), school break periods with a weekly activity theme (Stellino et al., 2010) and the provision of sports or games (Verstraete et al., 2006). These interventions have generally fostered structured physical activity with specified locations, time schedules, adult supervision and the facilitation of sport and fitness (Sener, 2006).
Limited information currently exists about the psychosocial mechanisms responsible for improving wellbeing and physical activity levels among children and adolescents (Michie et al., 2018), although one meta-analysis has identified the potential importance of self-perceptions, social connectedness and emotions experienced while participating in physical activity (Lubans et al., 2016). To advance wellbeing and physical activity promotion, it has been proposed that psychosocial variables be included in all aspects of the design of interventions (Michie et al., 2018; Van Sluijs and Kriemler, 2016). One model encompassing psychosocial variables that has been previously used to aid in the design of physical activity interventions is the self-determination theory (Deci and Ryan, 2004). Collectively, sub-theories within the self-determination theory specify that the satisfaction of human’s psychological needs for competence, autonomy and relatedness is essential for optimal motivation and wellbeing. In support of the self-determination theory, adolescents’ physical activity has consistently been predicted by autonomous motivation (Owen et al., 2014). The aim of self-determination theory-informed interventions is to engender needs-supportive social conditions, wherein the enhancement of physical activity and wellbeing is realised indirectly through needs-support and satisfaction, and autonomous motivation (Fortier et al., 2012; Ryan and Deci, 2017).
The primary aim of this study was to examine the impact of self-determination theory-informed school-based lunchtime games intervention on the wellbeing and symptoms of anxiety and depression of Irish adolescent women. Secondary aims were to examine the impact of frequency of physical activity on both physical and psychological markers of health while also examining some of the potential changes in secondary outcomes that may lead to changes in mental health and wellbeing.
Methods
Study design
This study took the form of a non-randomised, exploratory, controlled before-and-after design. The study took place from September 2019 to December 2019. The design, conduct and reporting of the trial adhere to the Transparent Reporting of Evaluations with Non-randomised Designs (TREND) statement (Des Jarlais et al., 2004). This non-randomised trial was designed to examine the impact that frequency of physical activity has on positive and negative mental health outcomes. The intervention consisted of lunchtime games 3 days a week for 40 minutes. The intervention lasted for 10 weeks as previous reviews have found interventions lasting 8–12 weeks to be the most effective (Biddle and Asare, 2011; Biddle et al., 2019) and fit into the current school calendar. The 10 weeks included a 1-week ‘sampling’ period at the beginning and a ‘free-week’ due to school holidays in the middle as can be seen in Figure 1. After the ‘sampling’ period, students aged 13 ± 0.7 years self-selected to 0, 1, 2 or 3 days of lunchtime games. Those who self-selected to 0 acted as the control group. Intervention and control groups were compared through pre- and post-testing. The control group had lunchtime as normal which consisted of remaining in their ‘base’ classroom while eating lunch. There were no options for further physical activity at lunchtime.
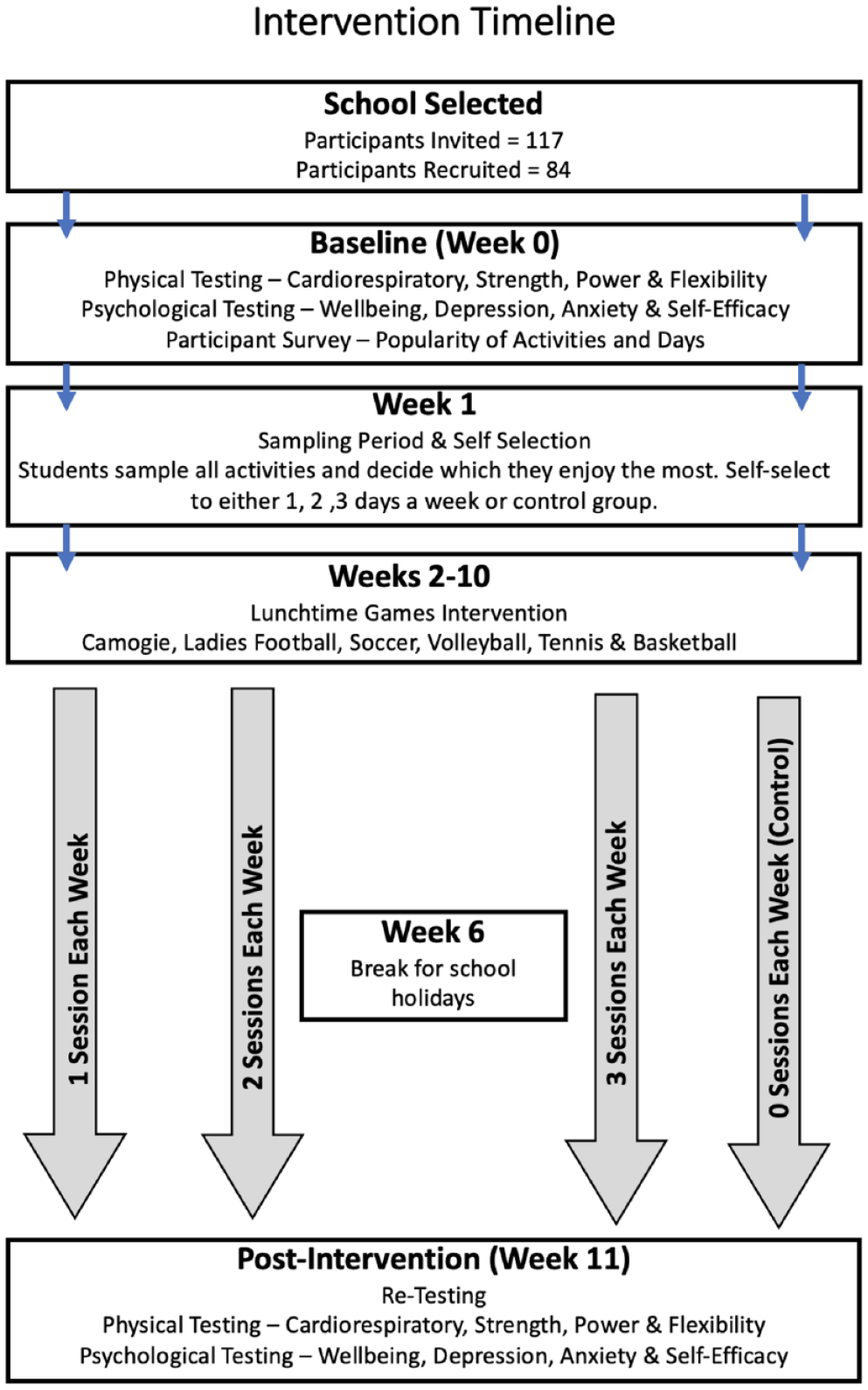
Intervention timeline.
Intervention overview
Autonomy was provided by including participants in the intervention design via a survey to ascertain the most popular games and activities at the outset. A breakdown of choices can be seen in Figure 2. The activities offered were camogie (an indigenous sport to women in Ireland similar to field hockey), football, soccer, tennis, volleyball and badminton. Two activities were offered at each lunchtime and participants could select whichever one they preferred. Lunchtime games were based on small-group activities of —four to six participants per group to allow for connections to develop between participants. Each lunchtime session included a 5- to 10-minute period in the middle when participants focused on developing a skill that was relevant to the game being played that day . This allowed participants to develop a level of competence. Activities were led by the first author, a physical education teacher at the school, and two other teachers who were experienced coaches. Transition year ‘assistants’ (fourth year students participating in a voluntary coach education module) also aided in the delivery of activities with at least two assistants involved in each activity. Transition year assistants had completed an introduction to coaching course prior to their involvement in the intervention activities.
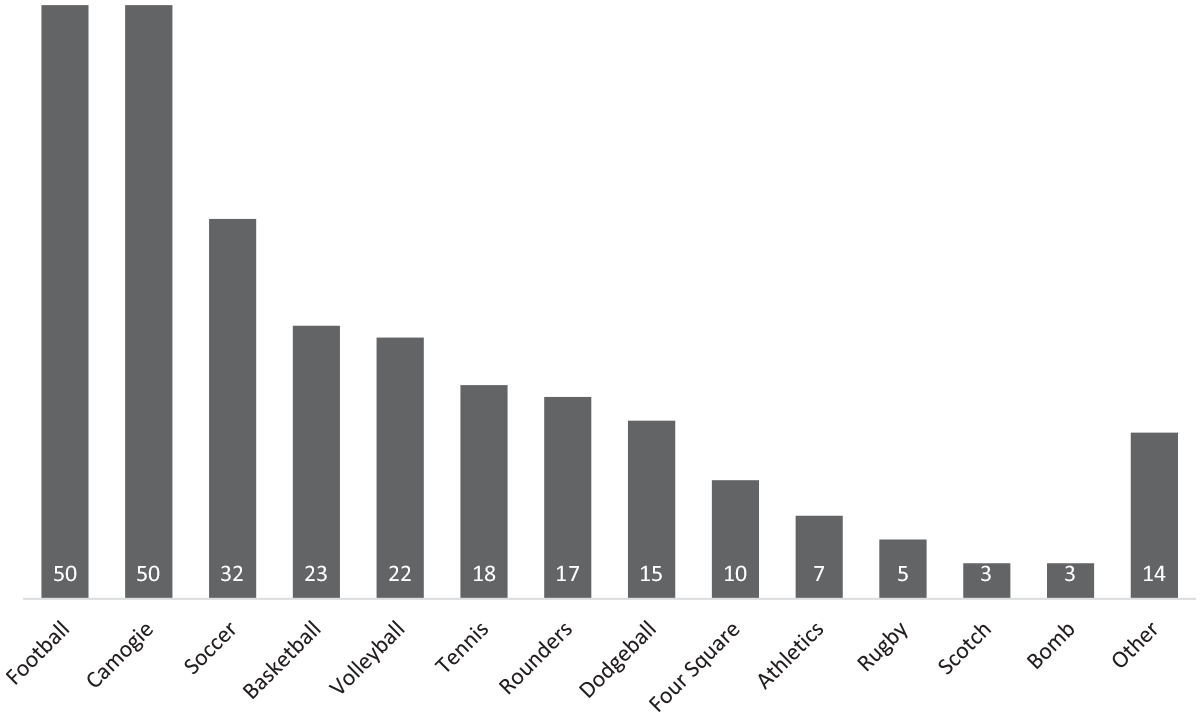
Survey of most popular activities and days of the week.
Selection and recruitment
Convenience sampling was used to identify an all-girls Catholic secondary school located in the south-east of Ireland close to where the lead researcher was based as a physical education teacher. An approach was made to the school principal by the research team through a phone call and subsequent on-site meeting. All first year students received a plain language statement outlining the purpose of the research, along with a participant and parental consent form. A total of 85 students (72% response rate) returned signed informed parental consent forms along with their own assent to participate in the study (Figure 2).
Intervention outcome measures
Pre- and post-tests included physical, psychological and behavioural measurements. The primary outcome variables of the lunchtime games intervention were wellbeing, symptoms of depression and symptoms of anxiety. The secondary outcome variables were self-efficacy and health-related physical fitness. A summary of the measures can be seen in Table 1.
Mental health outcomes pre- and post-intervention.

Significant difference (p ⩽ .05).
Psychological
Participants completed a self-report questionnaire, which included well-established and validated instruments, all of which are detailed below. All the questionnaires were administered through an online form and could be completed via tablet or mobile phone. The majority of participants chose to use their mobile phone. Participants filled in the questionnaire during a timetabled wellbeing class. 1 The lead researcher was present throughout to answer any potential questions that might arise. Questionnaires were completed between 3 and 5 days after physical testing, depending on when wellbeing classes were timetabled. The psychological variables measured consisted of positive psychological domains (wellbeing and self-efficacy) and negative psychological domains (depression and anxiety).
Wellbeing
Wellbeing was assessed using the Warwick Edinburgh Mental Wellbeing Scale (WEMWS) (Tennant et al., 2007), which measures positive psychological wellbeing through a 14-item self-report questionnaire. Responses to each item range from 1 to 5, with overall scores ranging from 14 to 70, where 70 represents the best possible level of wellbeing. Cronbach’s alpha in our sample was .83, indicating good internal reliability. The psychometric properties of the WEMWS have been confirmed in both adult (Tennant et al., 2007) and adolescent samples (Clarke et al., 2011).
Self-efficacy
Self-efficacy was measured using the general self-efficacy scale (Chen et al., 2001) which seeks to measure differences among individuals in their tendency to view themselves as capable of meeting task demands in a broad array of contexts (Chen et al., 2001). Cronbach’s alpha in our sample was .86, indicating good internal reliability. The general self-efficacy scale has been shown to have very good test–retest reliability and validity in both adult populations and among adolescents (Luszczynska et al., 2005).
Depressive symptoms
The severity of depressive symptoms was measured using the Beck Depression Inventory (BDI) (Beck et al., 1988). Items of this instrument assess specific symptoms of depression experienced over the preceding 2 weeks. The BDI includes an item measuring loss of libido, which was excluded from the questionnaire as it is considered inappropriate for use in school (Kendall et al., 1987). Each question was scored from 0 to 3, indicating the severity of the symptom, with total scores ranging from 0 to 60. Cronbach’s alpha in our sample was .94, indicating excellent internal reliability (Beck and Steer, 1984). The reliability and validity of the BDI have been confirmed in clinical and community samples of adolescents (Steer et al., 1995; Teri, 1982).
Anxiety symptoms
Symptoms of anxiety were assessed using the Beck Anxiety Inventory (BAI) (Steer and Beck, 1997), a 21-item self-report questionnaire. Responses to each item range from 0 to 3, with scores ranging from 0 to 63, with higher scores indicating increased levels of anxiety. Cronbach’s alpha in our sample was .93, indicating excellent internal reliability (Ulusoy et al., 1998). The BDI has been shown to have good reliability and validity in adolescent samples (Fydrich et al., 1992; Steer et al., 1995).
Physical fitness
Health-related physical fitness comprises multiple components including cardiorespiratory endurance (CRE), musculoskeletal fitness (muscular strength, endurance and power), flexibility and body composition, which have been identified as powerful markers of future health among children and adolescents (Ortega et al., 2008; Ruiz et al., 2009). There is a consistent body of evidence supporting the favourable effects of moderate to high levels of physical fitness on health-related outcomes, including cognitive abilities in childhood and adolescence (Bezold et al., 2014). The health-related physical fitness measurements used were based on recent guidelines for fitness testing in adolescents in Irish schools (O’Keeffe et al., 2020). CRE was measured using the 20-m multistage test (beep test); muscular strength using a hand grip dynamometer; muscular endurance using the front plank; lower body power using the standing long jump; and flexibility using the sit and reach test. All tests were carried out during physical education class by the lead researcher. Participants had a minimum of three attempts at each test to practice the movement and their best score went forward for analysis.
Physical activity
Habitual physical activity was assessed via a modified version of the Take PART questionnaire by measuring the number of days during the past 14 that participants had accumulated 60 minutes of moderate-to-vigorous physical activity (MVPA), which was previously validated in an Irish adolescent population (Woods et al., 2009). The original Take PART questionnaire measured the number of days in the past 7 that participants were active. This was modified to 14 as previous investigations of associations between mental health outcomes and frequency of physical activity have been based on 14-day scales (McMahon et al., 2017; Murphy et al., 2020). The survey item was as follows: ‘During a typical 2 week period, on how may days were you physically active for a total of at least 60 minutes? For each day, add up all the time you spent in physical activity like walking, riding a bicycle, etc. Count up the days with at least 60 minutes of physical activity in a typical 2-week period’. A graphic summarising moderate-to-vigorous physical activity, with examples, was also included in the questionnaire to aid participants in gauging the intensity of their exercise. Responses ranged from 0 to 14 days.
Data analysis
Mean scores on the psychological variables (BDI, BAI, SE, WEMWS) in the four groups (0, 1, 2 or 3 times per week) were compared using two-way repeated-measures multivariate analysis of covariance (MANCOVA) to control for the effects of initial psychological variables and groupings at the outset. Mean scores on the physical fitness measures in the four groups were also compared using two-way repeated-measures MANCOVA to control for initial physical fitness measures at the outset. Post hoc between-groups comparisons were carried out using Tukey’s honestly significant difference (HSD) and Bonferroni correction to account for multiple testing. Cohen’s d was used for calculating and reporting effect sizes. Confidence intervals were set at 95%. Linear models with fixed effects for ‘days meeting physical activity recommendations’ were conducted to assess the impact of the intervention on each psychological variable. Linear regression was used to test for the moderating effects of initial wellbeing, depression, anxiety and self-efficacy on the impact of the intervention.
All analyses were conducted in R (R Core Team, 2013), and figures were produced using the package ggplot2 (Wickham, 2011). The study was approved by the Dublin City University Ethics Committee (DCUREC/2019/107).
Results
In total, 85 students participated in the study: 24 attended games one time per week, 22 attended two times per week, 18 attended three times per week and 21 attended 0 days per week, thus acting as the control group (Table 1).
Psychological variables
No significant differences were found between sub-groups in terms of symptoms of depression, symptoms of anxiety, self-efficacy or wellbeing at the outset (Table 1).
Depression
A significant increase in symptoms of depression was observed in the control group (p = .01). No significant differences were observed in those who participated on either 1 (p = .02) or 3 (p = .05) days per week. A significant decrease was observed in those who participated on 2 days per week (p = .001).
Anxiety
A significant increase in symptoms of anxiety was observed in the control group (p = .009). No significant differences were observed in those who participated on either 1 (p = .7) or 3 (p = .3) days per week. A significant increase was observed in those who participated on 2 days per week (p = .003).
Wellbeing
No significant differences were observed in either the control group (p = .1) or among those who participated once per week (p = .06) for wellbeing. Significant differences were observed in those who participated both two (p = .01, d = 0.67 ± 0.54; medium) and three times (p = .001, d = 0.8 ± 0.50; large) per week for wellbeing.
Self-efficacy
No significant differences were observed in either the control group (p = .4) or among those who participated once per week (p = .7) for self-efficacy. Significant differences were observed in those who participated both two (p = .002, d = 0.76 ± 0.51; medium) and three times (p = .001, d = 0.9 ± 0.61; large) per week for self-efficacy.
A linear model with fixed effects for ‘days meeting physical activity recommendations’ found that the impacts of the intervention remained significant (p < .001) even when controlling for frequency of physical activity in all of the psychological variables. A further linear model controlling for wellbeing, depression, anxiety and self-efficacy at the outset of the intervention found that the impact of the intervention remained significant (p < .001).
Physical fitness
Pearson’s product moment was used to examine the association between physical fitness measures and psychological variables at the outset. A significant moderate association was found between symptoms of depression and body mass index (p = .006, r = .3), while a significant weak inverse association was found between symptoms of depression and muscular endurance (p = .04, r = −.22). A significant weak inverse association was found between symptoms of anxiety and lower body power (p = .04, r = −.22). A significant weak inverse association was found between wellbeing and body mass index (p = .01, r = −.27), while a significant weak association was found between wellbeing and muscular endurance (p = .02, r = .25). No significant associations were found between any physical fitness measures and self-efficacy (Table 2).
Associations between mental health outcomes and components of physical fitness.

r (±95% confidence interval).
Significant correlation (p ⩽ .05).
Significant differences in CRE and muscular endurance were found between sub-groups at the outset, with the control group scoring significantly lower on both measures, while the group that participated three times per week scored significantly higher on both. Significant reductions in muscular endurance were found in all groups post-intervention, while the control group showed significantly higher CRE. The control group and those who participated one time per week also showed a significant increase in body mass index. Those who participated one, two and three times per week had significant increases in flexibility, while those who participated three times per week had a significant decrease in muscular strength (Table 3).
Changes in physical fitness.

Significant difference (p ⩽ .05).
Discussion
The current study took the form of a non-randomised exploratory trial looking at the impact of a self-determination theory-informed lunchtime games-based intervention on mental health and wellbeing outcomes in Irish adolescent girls. Overall, the intervention had significant positive impacts on mental health and wellbeing indicators with little-to-no effect on components of physical fitness.
Participants who attended lunchtime games two times per week had significant reductions in symptoms of anxiety and depression, while those who attended three times did not. This suggests there is a ceiling effect or ‘sweet spot’ in terms of the frequency of activity that is required to protect against anxiety and depression, in line with previous findings from European and Irish adolescent cohorts (McMahon et al., 2017; Murphy et al., 2020). Dose–response curves suggest symptoms of anxiety and depression reach their lowest in adolescents when meeting physical activity recommendations on 8–9 days out of every 14 with no benefits being found in those with a higher frequency (McMahon et al., 2017; Murphy et al., 2020).
Elsewhere, it has been suggested that meeting physical activity recommendations on 14 days out of 14 may be associated with neurotic or compulsive behaviours and potential eating disorders, particularly in young women (Davis et al., 1997; Smith et al., 2013), therefore leading to elevated symptoms of anxiety. Controlled motivation has also been suggested as having a negative impact on the mental health benefits that can be derived from physical activity (White et al., 2018) such as when forced to engage in activity, through the use of negative consequences or as punishment, on a higher frequency of days by a coach or parent. Participants in the group that attended three times per week were meeting physical activity recommendations 9 days out of every 14 and so may not have benefited from the increased activity through the intervention. Ceiling effects of physical activity on wellbeing have not been found for European adolescent boys (McMahon et al., 2017) or Irish adolescent boys or girls (Murphy et al., 2020) in terms of wellbeing, which is in line with the current findings of increases in those who attended two and three times per week, regardless of the external frequency of activity.
Previous adolescent-focused physical activity interventions have shown inconsistent findings with respect to mental health outcomes. A recent meta-analysis of interventions with physical activity components showed no overall impact on anxiety or depression directly post-intervention or at follow-up (Neill et al., 2020). These findings must be taken with caution, however, as most participants had pre-existing known comorbidities such as previous traumatic experiences or obesity. One such intervention showing a reduction in symptoms of anxiety and depression involved a physical activity programme that was delivered through a cognitive behavioural skills programme (Melnyk et al., 2009), which had an impact on the context of physical activity. Other interventions have focused solely on the type and intensity of physical activity, including both aerobic and resistance training (Goldfield et al., 2018) and found neither to have a significant impact. The authors suggested that exercise interventions for adolescents should include higher levels of cognitive engagement when being physically active (Goldfield et al., 2018).
A review of the mechanisms underpinning changes in mental health and wellbeing through physical activity was conducted by Lubans et al. (2016). They suggested three interlinking hypotheses, including neurobiological processes, psychosocial processes and behavioural processes. Most neurobiological explanations have focused on brain-derived neurotrophic factor (BDNF). While BDNF was not measured in the current study, a recent randomised controlled trial found no significant changes in BDNF after a 22-week intervention that looked at various types of exercise (Goldfield et al., 2018). This suggests there may be another neurobiological process responsible for potential changes, or that psychosocial and behavioural processes play a more significant role than hitherto documented in this relationship, as was highlighted in a previous meta-analysis (White et al., 2017).
The similarity in effect size between improvements in wellbeing and self-efficacy highlights the potential psychosocial processes that underlie the mechanisms of physical activity and wellbeing promotion. Previous meta-analytic evidence found that when controlling for total physical activity, the life domain within which physical activity took place had a significant effect on mental health outcomes with leisure-time physical activity having the largest positive association (White et al., 2017). This suggests psychosocial processes, such as choice of activity (autonomy), a sense of belonging (relatedness) and increases in self-confidence or esteem (competence), play a significant role in the development of mental health and wellbeing through physical activity. A systematic review and meta-analysis of the association between self-determined motivation and physical activity in adolescents found a moderate positive association between autonomous forms of motivation and physical activity, whereas controlled forms of motivation had weak, negative associations with physical activity (Owen et al., 2014). This is in agreement with Lubans et al. (2016), who suggested that increases in self-perceptions and social connectedness are key psychosocial contributors to global self-esteem, resilience and subjective wellbeing, and therefore increased mental health.
Another school-based physical activity intervention has been found to have indirect effects through autonomy-support and needs satisfaction, indicating that needs satisfaction at a domain level (such as physical activity) may transfer its effects to wellbeing at a global day-to-day level (Shannon et al., 2018). Increases in self-esteem through physical activity may be an underlying mechanism for increases in wellbeing as previous qualitative evidence has demonstrated that positive affect and physical activity were associated with feelings of achievement and progress (White et al., 2018). Meaningful experiences in physical activity have previously been attributed to young people’s perceptions of their own high motor competence (Gray et al., 2008), suggesting that improvements, accomplishments and learning all contribute to greater enjoyment of physical activity experiences. This aligns with Scanlan and Lewthwaite’s (1986) model of sport enjoyment based on the two continua of intrinsic–extrinsic and achievement–non-achievement. Increasing task-specific self-esteem through increased movement competence may lead to enhanced overall self-esteem, thus developing higher levels of subjective wellbeing in adolescents.
Limitations
As participants voluntarily assigned themselves to groups, or to act as controls, motivation to participate must be considered a potential confounding variable in this study, not least because it is an important correlate and potential determinant of engaging in and sustaining physical activity (Ng et al., 2012). Those who selected 0 days per week had significantly lower levels of CRE and met physical activity guidelines on fewer days than those in other groups, indicating that they were already less active and less fit than other participants. The study sought to include autonomy and intrinsic motivation by allowing participants to choose what activities were included in the intervention. However, as the intervention was based on the most popular games, this may have led to the exclusion of potential participants who were most in need of extra physical activity as they would prefer to engage in less popular or less-accessible activities. Future interventions should look to target potentially ‘at-risk’ sub-groups who may have lower levels of physical activity and/or wellbeing by tailoring the activities to their specific interests instead of popular choices of the group at large. The design of the current study was specific to adolescents in a particular setting. Therefore, adaptation would be necessary for use with alternative populations or in different contexts. It was not possible to conduct a follow-up to test whether the effects reported maintained longitudinally due to restrictions in place for COVID-19. While every effort was made to reduce the potential for contamination, the design of this study would have been improved through the use of a clustered randomised control trial including additional participants.
Conclusion
In conclusion, this non-randomised study shows that a self-determination theory-informed lunchtime games–based programme can decrease symptoms of anxiety and depression in girls while also increasing their wellbeing. It also suggests that the school setting provides opportunities to intervene with children and adolescents and has a positive effect on both physical activity and wellbeing. Similar effect sizes for both self-efficacy and wellbeing suggest that increased self-efficacy may be an important underlying mechanism for increasing wellbeing through physical activity. The lack of change in physical fitness also suggests that lower intensities of physical activity, coupled with the right contextual factors may be enough to elicit change in markers of mental health in adolescents. Future research should look to embed the self-determination theory in interventions, so the impact of autonomy, competence and relatedness can be further explored to determine the contextual factors that best support wellbeing in adolescents through physical activity.
Footnotes
Acknowledgements
We thank the trial participants, whose willingness to take part made this study possible. We also thank the participating school for facilitating testing and completion of questionnaires during school time.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.