
Abstract
Objective:
To gain insight into the extent of body mass index (BMI) change during an academic year for children with overweight or obesity at entry to an early learning programme with nutrition and physical activity components (Head Start). We explored whether meeting with families to discuss weight and nutrition and age of entry in the programme were associated with movement towards healthy weight via a reduction in BMI.
Design:
Quantitative analyses of administrative Head Start data of children aged 3–5 years old who entered the programme with a BMI labelled as overweight or obese.
Setting:
Children who participated in a Head Start early learning programme in the Southwest USA.
Method:
Descriptive analyses of BMI changes over the Head Start programme year. Ordinary least square regression analyses were run to explore whether a meeting with a family regarding their child’s weight and nutrition (i.e. a family service event) and age of entry predicted BMI change over the programme year.
Results:
Children with BMI labelled as overweight or obese, on average, reduced BMI over the academic year. Unexpectedly, having a family service event was related to an increase in BMI over the school year. Earlier age of entry predicted reduced BMI over the programme year.
Conclusion:
Head Start programming appears well suited to support decreases in prevalence of childhood obesity and that earlier entry was better. A meeting with families regarding their child’s weight and nutrition predicted an increase in BMI, though several factors indicated the need for more nuanced research on the types and intensity of these events.
Introduction
Nearly 14% of US preschool-aged children and 19% of 6- to 11-year-old children are classified as overweight or obese. Obesity in childhood is associated with immediate and longitudinal physical and psychological risks, such as high blood pressure, asthma, diabetes, anxiety and low self-esteem (Centers for Disease Control and Prevention (CDC), 2020; Gordon-Larsen et al., 2010; Rundle et al., 2020; Ward et al., 2017; Weihrauch-Blüher et al., 2019). Children in households with low incomes have higher rates of being categorised as obese than their peers in families with higher incomes [CDC, 2021]. While of national concern, findings were also relevant to Southern Californian communities, particularly those with high levels of poverty. In the current study’s focal county, children who are economically disadvantaged have one in four health risk, such as high blood pressure, high cholesterol, type 2 diabetes and/or heart disease, compared to a 1 in 10 risk for their more economically advantaged peers (Orange County’s Healthier Together, 2020). Importantly, children whose families experience downwards socioeconomic mobility or consistently earn low incomes have higher body mass index (BMI) percentiles as they approach adolescence (Kendzor et al., 2012). Furthermore, Latine 1 children are also more likely than their white or Asian peers to experience childhood obesity (Robert Wood Johnson Foundation, 2019), especially if the Latine children are from low-income households (CDC, 2021). In Southern California, Latine children are the largest ethnic/racial group and the most likely to live in poverty (KIDS Data, n.d.).
Early education and health promotion
Early childhood programmes are a potential pathway to start children on healthy trajectories (Larson et al., 2011; Ling et al., 2016). The US CDC recommends young children eat healthy food and stay physically active. Furthermore, the programme standards for most early childhood programmes require health education including nutrition and physical education. Existing findings are mixed as to the extent to which centre-based childcare promotes healthier lifestyles, for example, through nutrition standards and physical activity, and/or prevents, reduces or increases young children’s experience of being overweight or obese (Alberdi et al., 2016; Andreyeva et al., 2021; Dooley et al., 2021; McGrady et al., 2010; Swyden et al., 2017; Trivedi, 2021). While some studies have found an association between use of childcare and increases in BMI for children in centre-based care (Murphy et al., 2021) and for very young children (under age 2 years) (Gubbels et al., 2010), there is evidence that Head Start programme participation can reduce BMI (Lumeng et al., 2015).
In addition to the early learning setting itself, the engagement of parents in early childhood programmes is an important consideration. In a meta-analysis of prevention and management interventions for preschool-age children, the most effective childcare management interventions included parents in active roles with hands-on training (Ling et al., 2016). Effective weight-loss interventions have been associated with the use of social cognitive or social learning theories (Nixon et al., 2012), a focus on individual targeted strategies (Mehdizadeh et al., 2020), and the use of strategies to improve both child and parent perceived competence in nutrition (Nixon et al., 2012).
Implementing holistic approaches to the complexity of childhood overweightness and obesity is important due to the multiple factors involved such as nutrition and physical activity in the immediate environment (e.g. home, school) and more distal factors such as access to healthy food (in location and price) and recreation, that are influenced by policy (Pereira et al., 2019). Findings from systematic reviews of ecological weight reduction approaches with children indicate that interventions that engage multiple levels (e.g. school, family) are important for promoting healthier weight, although effect sizes are sometimes small (Kiraly et al., 2017; Quattrin et al., 2012; Vo et al., 2019).
In this study, we examined one of the major early childhood programmes in the USA – Head Start, a federally funded comprehensive preschool programme that serves low-income families through a whole family well-being approach that includes nutrition and well-being services (Dahlin et al., 2020). This holistic early childhood programme provides health, education and psychosocial services to support short- and long-term optimal outcomes for children and their families, including requirements to serve healthy meals at school and to incorporate physical activity (Office of Head Start, 2016). These in-programme features are an important support to promote healthy weight.
Head Start, nutrition and weight management
As part of its programming, Head Start collects BMI data within 45 days of the child entering the programme, then identifies and monitors children whose BMI percentiles are in the range of underweight, overweight or obese (Miller et al., 2021; Tovar et al., 2021). In addition to providing nutritious meals and physical activity in the programme, Head Start may also address the multi-faceted contributors to weight gain in young children. As a two-generation programme focusing on children and their caregivers, Head Start attempts to address family and community-level contributors and risk factors for obesity, including access (or lack of access) to healthy food (Alberdi et al., 2016; Hawkins and Law, 2006). Head Start also engages with families to create family goals and plans that support child and family well-being (Office of Head Start, 2016). This additional feature may be particularly salient for promoting awareness and access to healthy food options, nutrition guidance and physical activity opportunities, both in the programme and at home. For instance, Head Start offers services to connect families to food, as well as employment support services that may help parents in findings jobs with better hours (which may open up time to access healthy meals). In addition, Head Start works to support more physical activity for families. In a study of Head Start health managers, the majority reported having policies in place related to physical activity, with more than half reporting at least one health curriculum in use in the programme, nearly all programmes addressing the topic of health with families and more than half having weight management services for families (Martin and Karoly, 2016).
Upon entry to Head Start, families meet with programme staff to identify family goals and create a family partnership agreement that identifies ways to meet those goals. Families and staff remain in continuous contact during the year, connecting in ‘family service events’ around specific concerns. In this paper, we examine family service events initiated by the programme to express concern that the child’s BMI is in the range of overweight or obese. Meeting with parents around a specific goal related to child weight concerns may be an effective strategy, as the inclusion of parents is an important component of interventions aimed at increasing children’s healthful behaviours and/or weight loss (Ling et al., 2016; Nixon et al., 2012).
Head Start has shown healthy weight changes for participants during the programme year (Frisvold and Lumeng, 2011; Lumeng et al., 2015), but little is known about the components of Head Start that may facilitate children in reaching healthy BMIs or whether earlier entry is better than later. Thus, this study sought to explore the role of the family service event in which the programme connects with the family to set goals around child weight, BMI or nutrition, and whether the age the child entered Head Start (at age 3 or 4 years) was related to changes in BMI for children identified by the programme as overweight or obese. To our knowledge, family service events focused on weight, nutrition and physical activity have not been actively explored in previous literature, but may shed insight into how Head Start programming-as-usual and its family engagement approach, rather than an outside intervention, may support avenues towards healthy weight for children who participate.
Current study
This study explored whether children in a Head Start programme with BMI in the overweight or obese ranges in a large county in California reduced their BMI over time in the programme. We then examined whether the Head Start staff met with families (via what is called a family service event) to discuss weight and nutrition and whether the age of enrolment into the Head Start programme was associated with movement towards healthy weight via reduction in BMI. Data came from a Head Start programme that serves a predominately Latine population, reflective of the community in which it is situated.
We hypothesised that enrolment in Head Start would be associated with reductions in BMI over time because of both the nutritious meals and physical activities provided to children during the programme year and the holistic child and family services Head Start offered. Among children who entered Head Start with a BMI labelled as overweight or obese, we hypothesised that those who had a family service event related to weight or nutrition would decrease in BMI more than children without because, theoretically, the programme would be more attuned to providing family services directly related to weight and health concerns. While some evidence has suggested an association between very early entry into childcare and increased BMI (Gubbels et al., 2010), starting younger may be better for children who attended Head Start specifically, because of the full array of child and family service available it offers. Therefore, we asked, for children who entered Head Start with BMI in the range of overweight or obese as defined by the US Centers for Disease Control:
To what extent did BMI change over the academic year?
Did having a family service event (i.e. a Head Start staff-family meeting) focused on concerns about a child’s nutrition or weight predict changes in BMI during the academic year?
Did children’s BMI change more when children started Head Start at age 3 compared to ages 4 or 5?
Method
Study population
We used administrative data from a large urban Head Start programme, covering years 2013–2017 for 26 Head Start centres. For this study, we restricted the sample to children with at least two reports of BMI at the 85th percentile or higher at time points at least 90 days apart for an unduplicated count of 1,120 children. The first time point was collected at the time the child entered the Head Start programme, when their weight and height were measured and BMI calculated. Information on the type of scale and use of a stadiometer was not available in the dataset. The second time point, using the same method of BMI measurement, was, on average, about 6 months after the first time point.
All children identified as Latine. The majority of parents spoke Spanish as a primary language (74.44% with a family service event; 68.45% without a family service event). Unsurprisingly, given that Head Start eligibility mandated families earn below the federal poverty level unless the child has a disability, nearly all families reported incomes that fell under the federal poverty level. For both groups of children (with overweight and with obesity), nearly half had a parent who had not completed high school. See Table 1 for a detailed description of the sample.
Sample Characteristics.
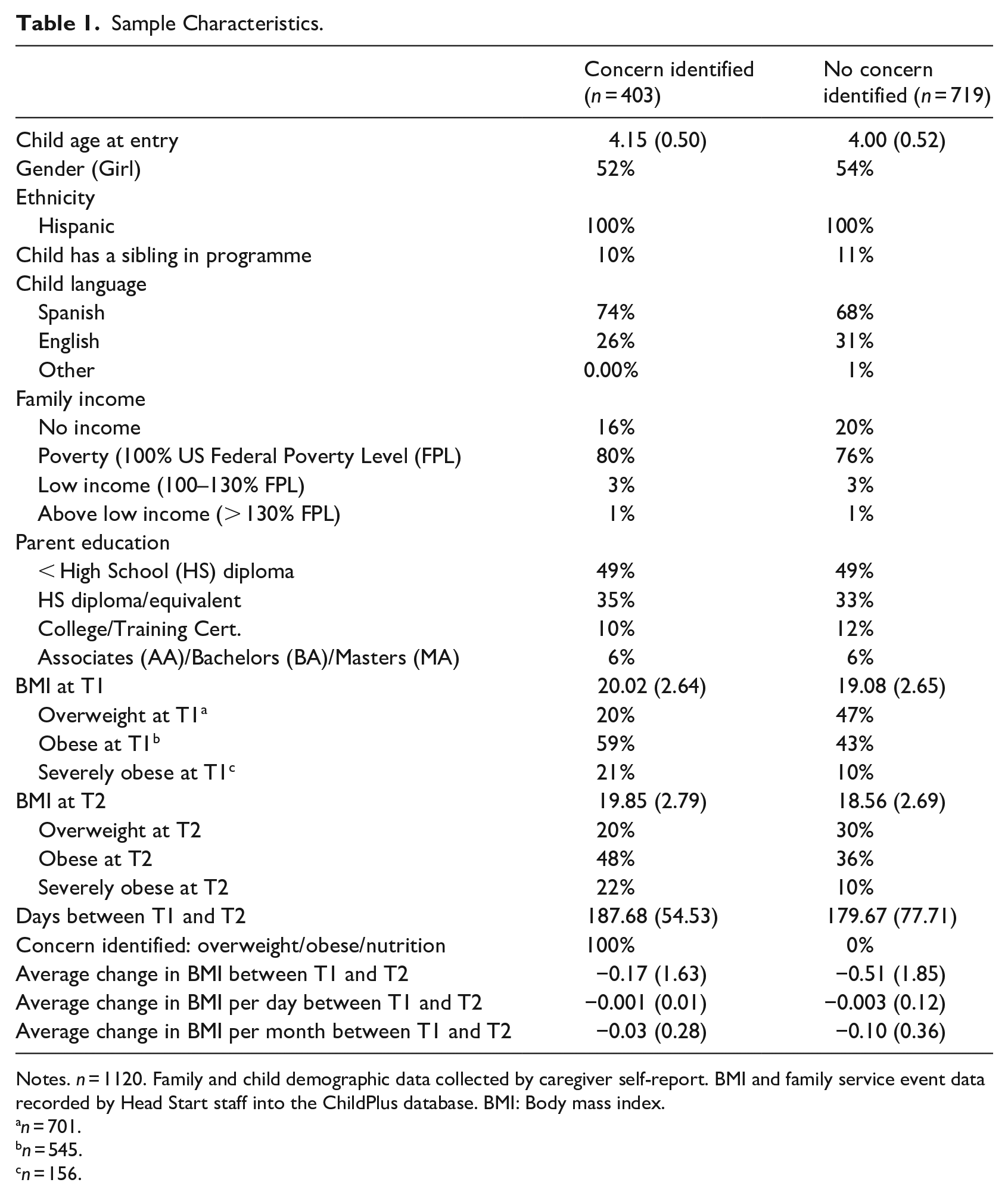
Notes. n = 1120. Family and child demographic data collected by caregiver self-report. BMI and family service event data recorded by Head Start staff into the ChildPlus database. BMI: Body mass index.
n = 701.
n = 545.
n = 156.
In comparing children who had a family service event related to weight concerns, several differences were found. First, children who had a weight concern-related family service event had higher BMIs (M = 20.02, SD = 2.64) than those without a plan (M = 19.08, SD = 2.65), t(1,120) =-5.72, p < .01 at time 1. Parents of children who had a family service event were slightly older (M = 34.08, SD = 0.34) than those who did not (M = 32.71; SD = 0.26). Children with and without a family service event focused on weight did not significantly differ by family income, parent education level, parent employment, or having siblings in Head Start.
Measures
BMI
Head Start staff collected BMI data when the child entered the Head Start programme in summer or autumn of the programme year (July–November) and again in spring of the programme year (March–June) the following year. These data were entered into the programme’s ChildPlus database. We used BMI raw score, rather than BMI z-scores, as BMI raw scores have been considered better for assessing change over time (Ansari et al., 2015; Cole et al., 2005). To account for differing time points between collection of BMI data, we created a variable to capture the change in BMI per month as our outcome variable by taking the difference of the two time points and dividing by the number of months between them.
Overweight/obese/severely obese
We used definitions from the US CDC (2019) to define the obese and overweight categories to reflect commonly used reference points and align with definitions used by the programme. We were interested in whether Head Start, with its full array of services, would be beneficial for children with BMI in the overweight, obese and severely obese ranges. However, we were especially interested in children categorised as having severe obesity, as this places these children at greater risk for dyslipidaemia, hypertension, Type II diabetes and fatty liver disease than their peers with milder levels of obesity (Bender et al., 2020). We used the recommended approach of calculating severe obesity at 120% of 95th percentile (Bender et al., 2020; Kelly et al., 2013), in which case severe obesity was coded as 1. Another variable labelled obese was coded as 1 if the child’s BMI was at or over 95th percentile, but under 120% of 95th percentile. A third variable, overweight, was coded as 1 if BMI was at or more than 85th percentile but under 95th percentile.
Obese or overweight family service event
A child’s BMI was obtained when they entered Head Start. If a child’s record indicated that their BMI was considered obese or overweight, the parent was contacted by programme staff (e.g. family health manager, family partnership advocate) via the family’s preferred contact method (e.g. email, text, telephone call or in-person meeting). We define this communication between staff and family as a ‘family service event’. In the programme’s administrative system, if a weight-related family service event was scheduled, a 1 was assigned. Otherwise, the family service event variable was scored as 0.
When engaging with families through a family service event, the Head Start programme staff sought to share the concern and then co-construct an approach to reduce child BMI. Because Head Start focuses on family partnerships, what the approach looked like differed by each family’s goals and preferences. It may have simply been general nutrition advice (e.g. healthy recipes) and recommendations for physical activity, but it might have included referrals or services from a registered dietician or healthcare provider. Head Start staff are expected to follow up with families regarding family service events, though the frequency and intensity are not available through the administrative data that we, as researchers, received.
Covariates
At enrolment, parents self-reported demographic information for themselves and their children during intake with Head Start staff. The following information came from parental self-report during these meetings: family income, parent’s primary language, parent’s employment status, parental education level, Women, Infants and Children (WIC) participation, 2 Supplemental Nutrition Assistance Programme (SNAP) 3 use, subsidised care receipt, child race/ethnicity and child age. We used the full database to identify if a child had a sibling in the programme, coding a 1 if the child’s family ID was attached to one or more other children in the dataset.
Data analysis
We conducted ordinary least squares regressions in Stata 15.1 to examine whether BMI classified as severely obese, obese, or overweight and a weight-related family service event predicted BMI loss during the programme year. We controlled for several family demographic characteristics including income, parental language, employment, education level and whether there was a sibling in the programme. Our reference group for these analyses were children whose BMI percentiles were in the overweight range. Standard errors were clustered at the site level to account for the clustering of children in sites.
Results
First, all children in the sample, on average, reduced their BMI over the programme year. Children who entered the programme with a BMI in the severely obese range experienced a greater reduction of BMI per month on average (M =-0.97, SD = 3.31) than children who entered obese (M =-0.39, SD = 1.48) or overweight (M =-0.18 SD = 1.18) and this difference was statistically significant χ2(316) = 464.77, p < .001. Children with no family service event around weight concerns (M =-0.51, SD = 1.85) had larger reduction of their BMI than those with a family service event related to weight (M =-0.17, SD = 1.63), t(1120) =-3.03, p < .01.
Second, we asked if having a family service event focused on a concern about a child’s nutrition or weight (1 = yes; 0 = no) predicted changes in BMI during the academic year when controlling for whether the child was overweight, obese or severely obese. Contrary to our hypothesis, receipt of a family service event related to weight predicted an increase in BMI per month between BMI measurements (β = 0.09, p < .001). As can be seen in Table 2, reduction in BMI was also predicted by having a sibling in the programme (β =-0.10, p < .05) and receiving a childcare subsidy (β =-0.11, p < .05). Participation in WIC predicted an increase in BMI per month over the academic year (β = 0.09, p < .01). All other variables were not statistically significant.
Family Service Event as a Predictor of BMI Change over Programme Year.
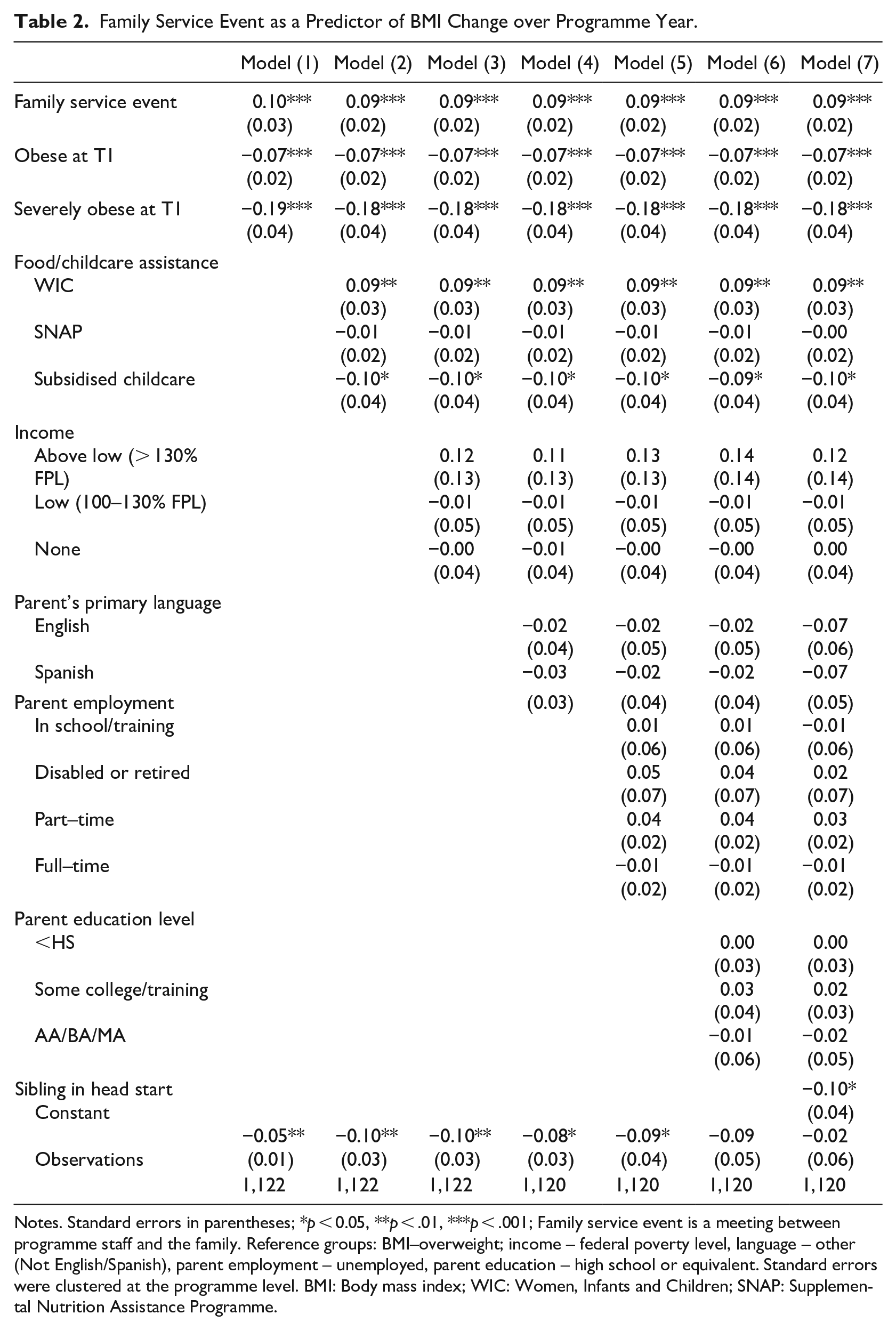
Notes. Standard errors in parentheses; *p < 0.05, **p < .01, ***p < .001; Family service event is a meeting between programme staff and the family. Reference groups: BMI–overweight; income – federal poverty level, language – other (Not English/Spanish), parent employment – unemployed, parent education – high school or equivalent. Standard errors were clustered at the programme level. BMI: Body mass index; WIC: Women, Infants and Children; SNAP: Supplemental Nutrition Assistance Programme.
Our third research question explored the relation between age of entry into Head Start (age 3, 4, or 5) and the extent of BMI change over the academic year (on average a 6-month window between BMI measures). As expected, entry to Head Start at age three predicted a greater reduction in BMI per month of the programme year (β =-0.08, p < .05) than starting later (See Table 3). There were no significant findings for entry at age four or five. In this model, having a family service event related to a child’s weight predicted an increase in BMI per month between a child’s BMI measurements (β = 0.08, p < .01), as did familial participation in WIC (β = 0.08, p < .01). However, having a sibling in the programme (β =-0.10, p < .001) and receiving a childcare subsidy (β =-0.11, p < .05) continued to predict lower BMI per month. All other variables were not statistically significant.
Age of Entry as a Predictor of BMI Loss in Spring of Programme Year.
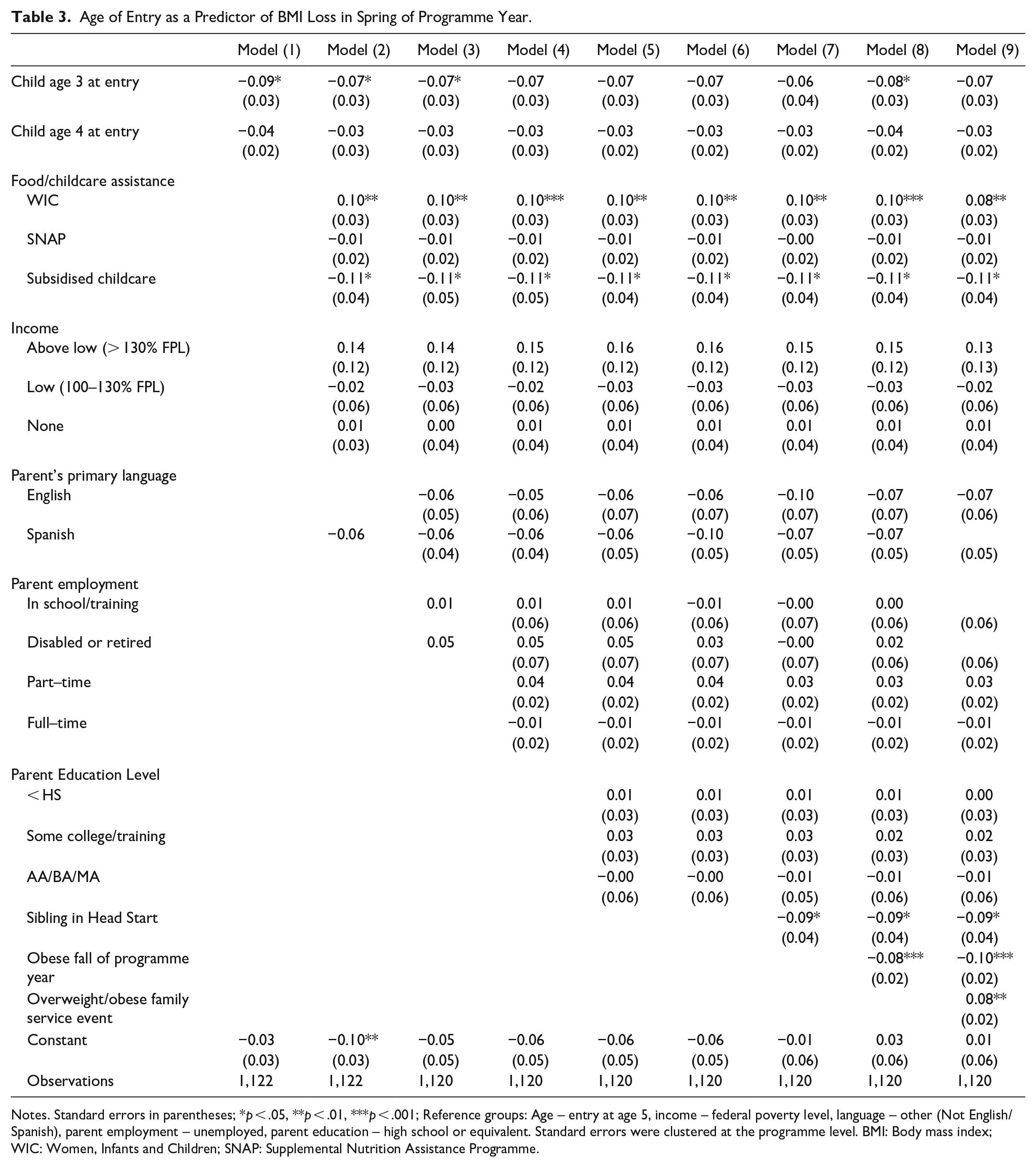
Notes. Standard errors in parentheses; *p < .05, **p < .01, ***p < .001; Reference groups: Age – entry at age 5, income – federal poverty level, language – other (Not English/Spanish), parent employment – unemployed, parent education – high school or equivalent. Standard errors were clustered at the programme level. BMI: Body mass index; WIC: Women, Infants and Children; SNAP: Supplemental Nutrition Assistance Programme.
Discussion
Children who entered the Head Start programme year with BMI classified as obese, on average, reduced their BMI during the programme year at a rate of about 0.07 per month. Children considered overweight similarly reduced their BMI about 0.03 per month. Head Start participation seemed especially useful for children who entered the programme with a BMI in the severely obese range–association between this designation and weight loss per month (0.18) was higher than those who entered Head Start in the obese range, although these children too got leaner. Obesity, and particularly severe obesity, is associated with a host of health problems (e.g. type II diabetes, hypertension). The finding that both children with obesity and severe obesity reduced their BMI over the Head Start year is a promising one, indicating that Head Start participation was related to healthy changes. Further, children who entered Head Start at an earlier age had a greater reduction in BMI, suggesting the importance of early access to Head Start services and programming.
A reduction in BMI was also associated with receipt of a childcare subsidy. Head Start programme participation is of no cost to families, thus it is likely these families used the subsidy to provide their children with additional hours of childcare beyond Head Start. This was consistent with previous research findings that preschool programmes are related to promoting healthy weight for children (Alberdi et al., 2016; Koleilat et al., 2012) and that participation in out-of-school activities, rather than parental care, is associated with reduced risk for obesity (Mahoney, 2011). Further, the Head Start programme had multiple programme factors that support a reduction in BMI, such as a nutritious meal programme and physical activity requirements for attendees (Office of Head Start, 2020). Having a sibling in Head Start also predicted a reduction in BMI over the programme year. It may have been that having more than one child in Head Start created multiple touch points for the programme to build relationships with families, which may have then supported more productive family service events.
We hypothesised that Head Start’s focus on family partnerships would position it well to support reductions in BMI through specific service events focused on children who entered the programme with BMI considered overweight, obese, or severely obese. These service events consisted of communication with families through email, telephone calls and meetings to discuss programme-initiated concerns that a child may be experiencing obesity or overweightness and create family goals in this area. Head Start’s approach to tailor contact, conversations and strategies to individual family units meant that families may have received different ‘interventions’ in order to find the best fit the family. Unexpectedly, the use of these events was associated with an increase in BMI over the school year. We can think of several possible reasons why.
To begin with, the available family service event data were not very descriptive, serving solely as a proxy for parent-programme interventions to reduce child BMI. Unfortunately, we lacked information about the level of support or intensity of these family events. For instance, a family event could have simply entailed a meeting to note a concern and share resources or could have involved long-term planning to meet goals around BMI reduction. The literature points to intensity of engagement with families as a key factor in successful prevention and management interventions for young children (Ling et al., 2016; Nixon et al., 2012). Head Start staff reported a wide range of strategies for communicating BMI information to families; while also reporting a range of parental reactions (Tovar et al., 2021). With these administrative data, we were unable to determine the receptiveness of families or how staff communicated information. Furthermore, details about the intensity, dose and duration of these family service events would be extremely useful to informing our analysis and findings, but our data, drawn from administrative records, do not provide such detail. It was also worth noting the BMI of children with a family service event was higher than those without one. It was possible that other family characteristics influenced both the likelihood of the family service event and lifestyle habits of children. Existing research has found that children with BMI categorised as obese tend to experience more obesity over time (National Academies of Sciences, Engineering, and Medicine, 2016). Our finding of BMI reduction was promising.
The use of WIC services was also associated with an increase in BMI over the programme year. This was surprising as previous research has found WIC service receipt to be related to lower obesity prevalence, greater food security and increased healthy eating behaviours (Chiasson et al., 2013; Daepp et al., 2019; Jansen et al., 2017). Our findings may have been related to the ‘insurance hypothesis’ whereby some individuals employ adaptive strategies to buffer against food insecurity (Nettle et al., 2017). In such cases, families who have experienced food insecurity may overeat when food becomes available (i.e. via WIC) as a means to protect against future food insecurity. Qualitative research with WIC participants indicates that some families may be too stressed, lack knowledge of healthy eating behaviours, or may not believe their child is overweight (Chamberlin et al., 2002). Understanding the beliefs and behaviours of parents, especially low-income parents using government services WIC and Head Start, may shed more light on mechanisms that could have driven this positive association with increased BMI over the Head Start year.
Limitations
It is worth noting some of the limitations of this study. Most importantly, the data come from an administrative dataset. Details about BMI measurement such as scale type are not available. Health data included in Head Start administrative sets have been questioned in terms of precision of the weight and height data collected, particularly when conducted by Head Start teachers and not a health professional, due to flexibility in measurement guidance by Head Start and variation in collection practices across programmes (Miller et al., 2021; Tovar et al., 2021). For instance, in a national survey of Head Start Health or Nutrition managers, only 25% of respondents reported using a scale that required calibration and 35% did not use a stadiometer (Tovar et al., 2021).
Second, this study only included children who entered Head Start with BMI in the 85th percent or higher and thus were considered overweight or obese. Because of this, changes in BMI cannot be compared to changes in children with lower initial BMI or those with higher BMI but not yet in the overweight range when they enrolled in Head Start.
Third, not all children in this administrative dataset had two BMI timepoints and, thus, were not included in the sample. The group of children excluded had a higher proportion of children with a sibling in Head Start, a lower proportion of children whose primary language was Spanish, a higher proportion of children whose primary language was English, and were in families who earned, on average, lower household income than the children included in the sample. These children may have differed in additional ways from those with two time points in ways we cannot measure.
Fourth, although we clustered standard errors at the site level to account for differences between sites, there may be within site differences (e.g. classroom teacher) that may have helped or hindered family connection to the programme. Finally, few details about the content and scope of the family service event were available, limiting our ability to differentiate activities that might promote healthier BMI or not. Even with these limitations, these data, capitalising on administrative data that all Head Start programmes must record, suggest potential benefits for children who are overweight, obese or severely obese in Head Start.
Conclusion
Amid concern around increased prevalence of childhood obesity in the USA, policymakers have been interested in mechanisms to support healthy weight trajectories for children (Frieden et al., 2010; Powell et al., 2017). We found that participation in a Head Start programme was associated with a reduction in BMI for children who entered the programme with a BMI classified as overweight, obese or severely obese. Importantly, these children came from demographic groups with the highest rates of obesity (families with incomes below the poverty line and Latine). In addition, earlier may be better, as we found entry in Head Start at 3 years of age predicted reduced BMI, whereas entry at 4 or 5 years did not. Although unexpected that a family service event focused on the concern of a child’s weight was associated with an increase in BMI, future research is needed to understand the level of service provided (e.g. information sharing versus an ongoing goal-driven plan for weight loss) and family characteristics that may pose barriers to reducing BMI. These data suggest that Head Start addresses another type of family risk, childhood obesity, especially when participating at the earliest start of preschool.
Footnotes
Acknowledgements
The authors express their gratitude to the Head Start programme who graciously agreed to provide the data for this study as part of a research-practice partnership.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the John Randolph Haynes & Dora Haynes Foundation.