
Abstract
Background:
Evidence supporting physical activity (PA) as an effective modality in the prevention and management of non-communicable diseases is robust. Medical doctors are ideally placed to translate this into practice; however, realising this has proved challenging. To ensure doctors are well prepared, the training of medical students to be proficient in PA counselling seems essential. This study aimed to explore the PA counselling practice of junior doctors, to gain insight into how undergraduate training might influence their future practice.
Methods:
Interviews were conducted with 11 junior doctors recruited by purposive sampling from across seven different medical schools. All junior doctors were currently undertaking their post-graduate training in North-West England. Interviews were digitally recorded, transcribed verbatim and analysed using thematic analysis.
Results:
Themes developed from the data were PA attitudes and practices, and barriers and facilitators to PA counselling in clinical practice.
Conclusion:
The PA counselling practice of junior doctors was found to be inadequate, and attitudes towards PA promotion were particularly discouraging while in the hospital setting. Lack of training in PA counselling at both the undergraduate and postgraduate level and lack of support from consultants were major hindrances. However, unexplored opportunities exist for junior doctors to incorporate PA counselling into primary and secondary care and thus transform the practice of the next generation of doctors.
Introduction
Globally, physical inactivity (PI) is a major risk factor for non-communicable diseases (NCDs), including cardiovascular pathologies, some cancers, type 2 diabetes and ultimately mortality (González et al., 2017; Lee et al., 2012). The total international healthcare expenditure in 2013, due to PI, was approximately US$53.8 billion (Ding et al., 2016). Consequently, to mitigate the detrimental effects on health precipitated by PI (Kohl et al., 2012) and reduce the financial burden on healthcare services, promoting physical activity (PA) is vital (Scarborough et al., 2011).
In England alone, it is estimated that about 37% of adults do not meet the recommended guidelines of achieving 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity PA per week (Sport England, 2019). This is despite the championing of Make Every Contact Count (MECC), a UK initiative to further promote PA and other healthy behaviours (Public Health England [PHE], 2016). MECC’s ambition has been for all health professionals to include, during their consultations with the public, brief conversations that promote positive lifestyle changes.
Evidence shows that one in four people would be more active if advised to be so by a general practitioner or nurse (Orrow et al., 2012). Despite this, a survey in the UK found that about 80% of primary care physicians reported reduced confidence in undertaking PA counselling with their patients, which was largely attributed to the lack of awareness of the UK national PA guidelines (Chatterjee et al., 2017). Other reasons for the poor uptake of PA counselling in clinical practice include time constraints, insufficient incentives and inadequate training (Chatterjee et al., 2017; Douglas et al., 2006; Wheeler et al., 2017). This has led to advocacy for more education on exercise medicine within the medical curriculum particularly at undergraduate level, as this may produce doctors more competent in PA promotion (Dunlop and Murray, 2013). This is supported by previous research which found that classes teaching PA for health were often omitted from medical students’ training (Weiler et al., 2012), suggesting that newly qualified doctors may not be fully prepared and equipped to undertake PA counselling with their patients.
After graduating from medical school, qualified UK doctors enter a 2-year postgraduate foundation programme in which they complete a series of approved training posts as junior doctors within the National Health Service (NHS) (UK Foundation Programme [UFP], 2016). This training provides the opportunity for junior doctors to develop their knowledge and skills under the supervision of a senior doctor before becoming autonomous practitioners (UFP, 2019). During this period, junior doctors also undertake clinical assessments to demonstrate their proficiency in duties that they will need to perform to progress to general practice (GP) or specialty training (UFP, 2016). One of these competencies is the ability to incorporate health promotion and illness prevention in their consultations. To satisfy the minimum level of competence, junior doctors need to counsel their patients on positive lifestyle behaviour. This can include advising patients about the possible ill effects of inactivity (UFP, 2016). The foundation programme therefore provides junior doctors with another opportunity to develop the skills and confidence to undertake PA counselling.
While the phenomenon of PA counselling in clinical practice has been studied among medical students and practicing primary care physicians, the authors were not aware of studies exploring solely the views and PA counselling practice of junior doctors. Gaining this knowledge can provide an insight into newly qualified doctors’ perceptions of PA promotion as well as any barriers and enablers to undertaking this. Having a better understanding of this phenomenon can support the development of both the undergraduate and postgraduate foundation training curriculum to enhance the competence in PA promotion of future doctors. Against this background, the aims of this study were to:
explore the PA counselling attitudes and practices of junior doctors;
understand barriers to PA counselling practice among junior doctors;
understand enablers and facilitators to PA counselling among junior doctors
Methodology
A purposive sample of 11 junior doctors from seven different English medical schools was obtained. All participants were under 35 years of age and were in their second year of their postgraduate medical practice. All were undergoing their foundation training in five different medical specialties in one of the health trusts in the North-West of England.
Participants self-selected by responding to posters placed on the notice board of the postgraduate foundation school and emails sent to participants’ email addresses by the foundation school’s administrative coordinator. All posters included an overview of the study and highlighted the eligibility criteria.
A qualitative, exploratory study using semi-structured interviews was chosen as this facilitates more depth of insight into the phenomenon under study and allows for the elaboration of information that may not have previously been considered by the researcher (Gill et al., 2008) (see Supplemental Material for interview schedule).
Interviews lasted approximately 40–60 minutes and took place between August and September 2018. Written consent was obtained prior to the interviews. Ethical approval for the study was granted from the NHS Health Research Authority and the Manchester University NHS Trust (IRAS: 247445, MFT PIN: B00258) and Manchester Metropolitan University (Ethics Reference 993).
Inclusion and exclusion criteria
Participants who were more than 4 months into the foundation training programme took part in this study. This was to ensure that participants had undertaken induction training and were thus familiar with their new working environment. This meant that junior doctors in year 1 could not be a part of the study because they were only 5 weeks into their foundation training programme at the time of data collection. Junior doctors who did not obtain their undergraduate medical degree in the UK were excluded as the study aimed to gain insights into the extent of PA education in the UK undergraduate medical curriculum (Table 1)
Participants’ characteristics.
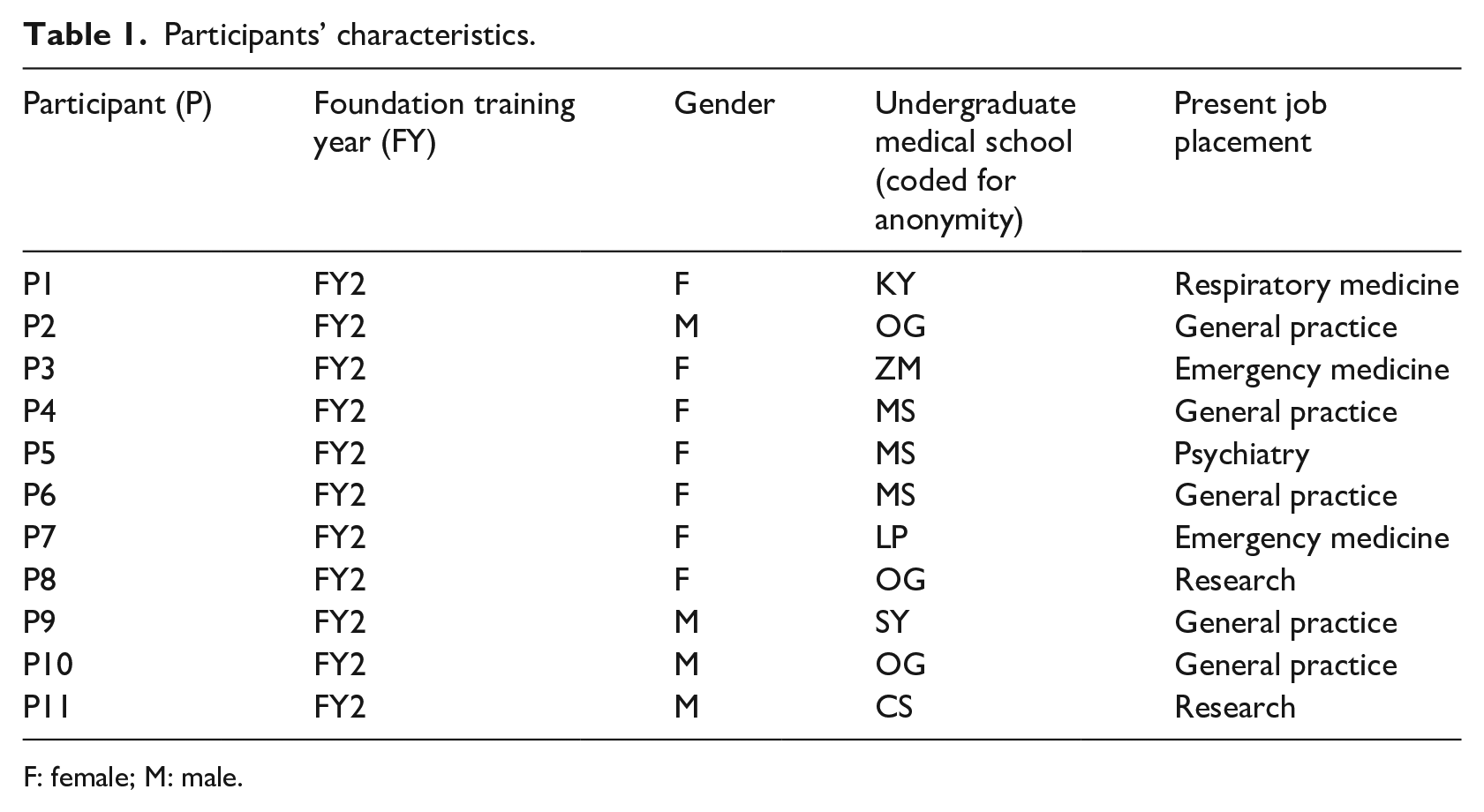
F: female; M: male.
Data analysis
Interviews were digitally recorded and transcribed verbatim. Data analysis followed the six-stage process identified by Braun and Clarke (2006). The interviews were conducted by J.O., the first author, who is a medical doctor and at the time of conducting this research was undertaking a master’s degree. Together with the second author (S.E.H.), a physiotherapist and experienced qualitative researcher, the data analysis was undertaken.
Initially, to familiarise themselves with the data, both authors read and re-read the transcripts of the interview before separately generating initial codes based on recurring topics or salient points highlighted in the text. Then, following discussion between them, codes that were deemed similar were organised together to form sub-themes before related sub-themes were combined to produce overarching themes. These overarching themes were labelled appropriately to capture the essence of what the data were portraying.
Throughout the above process, any divergences in coding or differences in interpretation between researchers were discussed, and further review of the raw data was undertaken. Modifications were then made until a consensus was achieved. Analysis of the data confirmed data saturation had been achieved when no new themes were emerging (Braun and Clarke, 2006).
Findings
Three overarching themes were identified: PA counselling attitudes and practices, barriers to PA counselling and enablers of PA counselling (Table 2).
Thematic analysis.
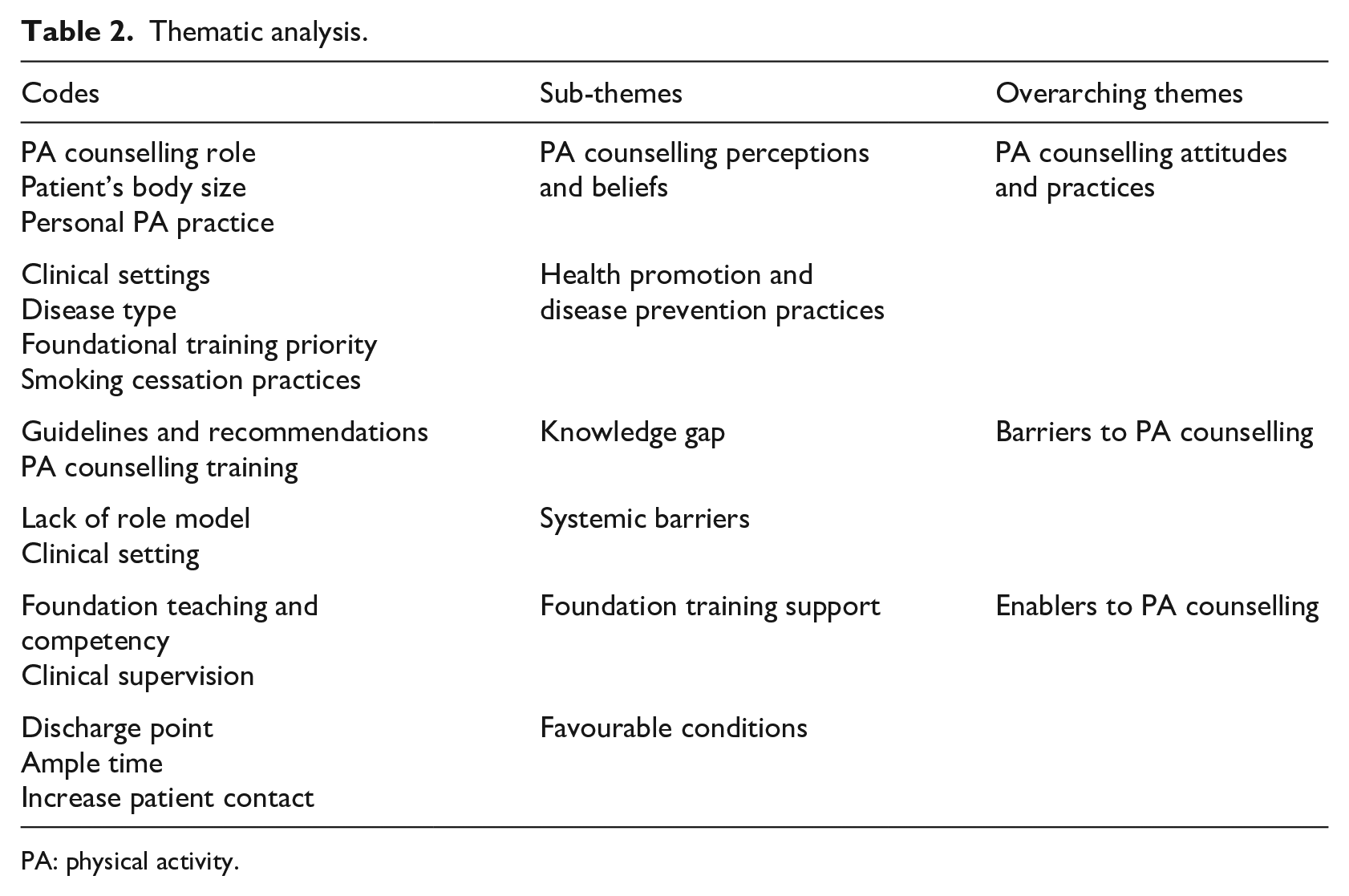
PA: physical activity.
PA counselling attitudes and practices
PA counselling perceptions and beliefs
There was broad consensus among participants that PA was integral to good health with an awareness of both the physical and mental benefits. However, participants had diverse views about the relevance of PA in clinical practice. Most participants felt that PA counselling would be more beneficial as a disease prevention intervention than as treatment for a condition and suggested that primary care rather than the hospital setting was the optimal place for this to take place. These views seemed influenced by what participants deemed to be the working practices of the clinical setting they found themselves in. For participants in a hospital setting, diagnosis and treatment of illnesses were seen as the priority, and thus, PA for prevention was not considered a concern: It is not that it is not possible [PA counselling], instead, it is overlooked. In secondary care, they come in with a problem and we fix it and that is the main objective. (P3)
However, some participants highlighted that PA counselling could be initiated in hospitals as a treatment intervention, but they felt that consultants often did not emphasise the importance of PA to their patients in these clinical situations: I think it should be encouraged but, probably said as a side note to other things. For instance, in depression, PA is really beneficial, yet they [the consultants] will say we will start you on an antidepressant before they say actually . . . try and be more active. (P2)
In particular, participants felt that patients admitted for obesity-related illnesses in hospital settings could benefit from advice on PA. However, they did not often provide this because they felt uncomfortable doing so: … I find it a lot awkward to ask people if they are overweight or if they do any physical activity because a patient may take offence to the fact that you are calling them fat. (P1) In respiratory medicine, I saw patients who could become physically active, but with a history of chronic obstructive disease. They were obese and I knew they could exercise, but they were a difficult person to have a conversation with. Instead of talking about physical activity, I chickened out and talked about smoking. However, I should have talked to them about the fact that their weight was making them ill. (P5)
Despite consensus among participants about the health benefits of preventive and therapeutic PA counselling, there were differing views as to who was responsible for providing these conversations, particularly in the hospital setting. Although some participants said they could be involved in PA counselling in hospitals, others felt it was more fitting to the role of other health professionals even though they felt that smoking cessation and dietary advice were their own responsibility.
In the hospital setting, physical activity is kind of categorised as the duties of physiotherapist or occupational therapist. (P2) I probably tell my patient about smoking cessation and healthy diet but nothing on physical activity. Even though I think much should be said …. I ask myself if it is my role because in my head I just think their GP will talk to them about it. Also, I feel in surgery or acute medicine, it is consultant led and they will give the advice. You just feel like it’s not my job. (P4)
Despite this, participants did acknowledge that they were well placed to impart this information as patients respected their advice: It is true that the doctor could have a bigger role in emphasising how important PA is for prevention of so many diseases. I have seen patient ask me questions about physiotherapy related things, and I will just say what the physio has said but wouldn’t believe it until it came out of my mouth. And this is because you are in a privileged position, that you are well trusted as a doctor. In fact, I think I am letting my patient down for not talking to them about PA. (P9)
Health promotion and disease prevention practices
Although their competency assessment in health promotion and disease prevention provided the participants with the opportunity to undertake PA counselling, most participants chose to advise on smoking cessation instead. One reason for this was that participants felt that the evidence in support of smoking cessation in the prevention and management of illnesses was more robust than PA: We talk about smoking cessation easily. If you know someone is a smoker, I think I will be more likely to say give up smoking compared to say to someone who is inactive to exercise. Because I think the problem with smoking cessation is much greater than inactivity in the short term. . . the evidence is overwhelming that if you stop smoking you can slow progression of diseases. I think stopping smoking is more important than exercise that is why I am good in smoking cessation advice. (P8)
The majority of participants perceived the essence of their training to be illness diagnosis and disease management rather than health promotion: I think the most important thing in foundation school is how to spot an ill patient first and foremost. Doctors will prefer to be trained on something that will stop them missing something that might mean bad outcomes for a patient. I think the importance of PA has slipped down a little bit because we are more scared of missing an ill patient rather than preventing an illness a patient does not have from happening in the future. (P10)
Due to their busy work schedule since qualifying as doctors, it was apparent that participants’ leisure time spent undertaking PA had reduced. Although not a consensus among participants, some felt this could undermine the effectiveness of any PA counselling they undertook as the success of their advice could be influenced by patients’ perceptions of themselves as role models for PA: for me when I was at uni, I would play sport three times a week and then I will walk from my house to university every day. However, I cannot do that now because I drive to work. Basically, the job and change in lifestyle has affected my level of activity. (P7) Firstly, what I do influences what I say and how I appear to them. For example, if I was clearly nearly inactive and I am telling them to exercise, I will look like a hypocrite and they won’t take such advice seriously. It’s like anything, if a doctor tells a patient to stop smoking and then the patients goes and sees the doctor smoking, it may influence the patient’s decision in a way. (P6)
Barriers to PA counselling
Knowledge gaps
Although PA counselling was not routinely undertaken by participants when in the hospital setting, it was clear that the lack of undergraduate education in this area made it hard to incorporate PA advice while consulting with patients: For instance, there was a guy I came in contact with whose HBA1c was borderline. We talked about diet and exercise. He said he had started walking in the park. I just further advised him to find something he enjoyed and then he should do it. I did not make any recommendations. I feel I could have done more. However, there is no physical activity teaching in med school. Up till now I never saw the importance of giving brief advice on PA to a patient. I think there is a gap in the curriculum in this regards. (P5)
Although the majority of participants were aware of aspects of the PA recommendations, some seemed to lack knowledge of how much PA to advise on and for how long: … on the ward, you can spend about 30-40 minutes with a patient because you do ward rounds and keep going back to take blood samples. I think there is much opportunity to give physical activity counselling. However, not knowing how to do this is the issue. . .You get taught how to deliver bad news, how to do smoking counselling but you don’t get taught on evidence bases to engage in a conversation about weight and activity. And I personally would not know what to recommend to patients. (P2)
Systemic barriers
Systemic barriers such as time pressure, particularly in hospital settings, and lack of clinical support in terms of mentorship and clinical supervision also created a barrier to PA education and counselling: You learn by seeing what other people do. For example, your consultant . . . you don’t see them making the point either. (P11)
However, for participants who had seen consultants engage with PA counselling, how they had approached this influenced the participant’s motivation to do so in a likewise manner: I have felt much more empowered to have such conversation having seen it done well and I have also seen it done badly and I have seen a patient make a complaint as a consequence of it. I think that negatively impacted my view on it and I will not want any patient to have complaints about me at this point in my career. (P1)
Enablers of PA counselling
Foundation training support
Along with additional training as undergraduates, some participants suggested that being taught about PA counselling during their postgraduate foundation training could positively influence PA counselling practices. They suggested that making it a compulsory part of their clinical assessment might encourage them to approach PA discussion with patients: A lot of people think physical activity is important but they have not really thought about talking to a patient about it. I think a lot of time foundation teaching reminds you of something and then you can take it into practice . . . (P7)
Favourable conditions
Participants highlighted how foundation training provided them with an environment that could be favourable to undertaking PA counselling. This was particularly the case in general practice (GP), as they were allowed longer consultation times than qualified general practitioners and with patients who were more medically stable. In addition, the model of consultation adopted in GP settings encouraged PA counselling: In primary care, I have a really long appointment and I can give physical activity advice. As a doctor, I think it is more feasible because we have more time. As a GP, it is more difficult because of time pressures. (P3)
However, even the hospital setting could provide opportunities to promote PA. Some participants said they had more time with patients compared to senior colleagues: …. junior doctors are probably the clinicians with most patient contact. I think there is no time to set aside or specific times to talk to the patient in hospital care. However, whilst taking blood you can talk about smoking cessation. It is being opportunistic on the job to talk about preventive practices. (P5)
They also felt that discharge was an opportune time to approach PA counselling especially as it could prevent readmission: The point of discharge could be teachable moments to give physical activity advice. It is probably not utilised, and we are probably missing an opportunity. The point of discharge could be a time to drive home the need to be physically active particularly if it was a risk factor for their admission. I probably have overlooked it in hospital care. (P4)
In addition, it was highlighted that the discharge planning process could also be leveraged to provide PA counselling: For instance, when you have to write discharge summaries you have to say …. have you given the patient smoking advice or does the patient smoke. . .there is a part that reminds you to consider that aspect. So, there could also be a part that reminds you of giving brief physical activity advice to patients. (P11)
Discussion
Although participants were aware of the health benefits of PA, they underestimated the implications of PI for health when compared to smoking. This appeared to have a negative effect on their attitude towards PA counselling, although recent evidence suggests that increasing PA levels can reduce mortality by as much as smoking cessation (Byberg et al., 2009; Holme and Anderssen, 2015).
Those participants who did attempt to provide PA counselling lacked the self-assurance to provide definitive advice in terms of timing, type, frequency and duration of PA because of limited awareness of the recommended guidelines. This resonates with previous research, which found that low confidence secondary to insufficient knowledge about PA guidelines was a major reason why family physicians were unable to provide specific advice about PA interventions (Chatterjee et al., 2017; Wheeler et al., 2017). Lack of knowledge about PA clinical guidelines among participants could also be a reflection of the apparent low prioritisation given to PA education in UK medical schools (Weiler et al., 2012).
While there exists the challenge of introducing PA for health into an already full medical curriculum, the UK can learn best practice from other universities elsewhere in the world that have successfully incorporated exercise medicine into the undergraduate medical curriculum (see, for example, Noormohammadpour et al., 2018; Trilk and Phillips, 2013). As part of the Movement for Movement initiative, work has also taken place in the UK to produce resources for UK medical schools to help embed PA into their curricula (Gates et al., 2016, 2018b). Although the impact of this initiative is yet to be evaluated, progress so far has been encouraging (Gates et al., 2018a).
As participants were more likely to engage in smoking cessation counselling, this was also their preferred choice when undertaking their clinical assessment in health promotion. Nevertheless, participants expressed a desire to converse more with their patients about PA but felt the need for more mentorship from senior colleagues to support them to undertake this. This suggests that if senior staff could become effective role models by translating the knowledge acquired by doctors in their undergraduate training into practice, this could positively influence junior doctors’ undertaking of PA counselling. Making PA counselling a compulsory competence as part of postgraduate clinical assessments would provide an additional opportunity to improve doctors’ commitments to providing PA advice in the clinical setting.
Physically active physicians have been found to be more likely to endorse PA to their patients because they are more self-assured in talking about what they have themselves found valuable (Lobelo et al., 2009). In this study, participants who had reduced PA levels due to work commitments claimed that this could be deleterious to their PA promotion practices. However, previous research has also found that despite meeting PA recommended guidelines, medical students lack the ability to undertake PA counselling (Mandic et al., 2017). This suggests that the extent to which a doctor is physically active may not, on its own, lead to competency and self-assurance in approaching PA counselling. Nevertheless, encouraging and supporting doctors to have an active lifestyle alongside training in PA promotion may strengthen their resolve to put it into practice.
While most studies concerning PA counselling in clinical practice have focused on PA promotion in primary care, mainly general practitioner locations, little is known about its feasibility and practice in a typical hospital setting (Hébert et al., 2012). In this study, many participants felt that PA counselling was the role of other health professionals, particularly physiotherapists, as they were perceived to have more time to undertake this. While previous research has shown higher levels of PA promotion among physiotherapists, as compared to physicians, physiotherapists have also highlighted many barriers to its undertaking, including insufficiency of time (Lowe et al., 2017). In fact, some of the participants claimed they had more contact time with patients when working in hospitals compared to other doctors. As this suggests that lack of time is not a major hindrance to junior doctors, the opportunity for them to incorporate PA counselling, at this time, is enhanced. Nevertheless, participants highlighted that their priority on hospital placements was towards the diagnosis and medical management of illnesses and not PA counselling. Failing to recognise the impact a patient’s lifestyle and behaviour have on their health has previously been identified as a reason for scarce PA promotion in the NHS (Weiler and Stamatakis, 2010). Besides, although the benefits of PA counselling as an intervention for patients with established diseases have been highlighted, the lack of doctors undertaking this in hospitals may be because of the misconception that PA is only a preventive measure (Sallis et al., 2015). As hospitals offer a setting in which to strengthen further the public health message on PA, additional research that incorporates these settings would therefore seem pertinent to establish ways to facilitate doctors’ undertaking of PA.
Participants highlighted that for PA promotion in hospital settings to be effective, it should be introduced as part of the discharge process. Generally, discharge planning aims to reduce the length of stay in hospitals while also minimising unplanned readmissions (Gonçalves-Bradley et al., 2016). This is consistent with the participants’ perceptions about PA being a tool to prevent readmission, particularly among patients admitted for a disease where PI was a risk factor. While the discharge process involves a multidisciplinary approach, junior doctors are primarily charged with its coordination (Katikireddi and Cloud, 2008). Having the responsibility for discharge in this way creates another opportunity for junior doctors to promote PA.
Limitations and strengths of the study
While a sample of 11 participants may be considered small, this study aimed to provide an in-depth understanding of a phenomenon rather than generalise (Creswell, 2014). Given that junior doctors from only one hospital trust were interviewed and participants were self-selecting, this limits the generalisability of the findings, as did the range of clinical placements included.
Implications for future research
While there has been much focus on PA promotion in primary care clinical settings, findings from this study suggest additional opportunities exist to promote PA counselling in secondary care. However, further research will be needed to gain more insight into this. In particular, to facilitate doctors’ adherence to PA counselling in the clinical arena, a cultural shift in doctors’ perceptions towards PA is required to transform future practice. Additional studies, particularly in the area of implementation research, are needed to understand the changing behavioural attitudes of doctors towards PA counselling in the clinical arena and how this translates into practice.
Conclusion
Findings from this study show that the PA counselling practices of junior doctors are limited and attitudes towards PA promotion were particularly discouraging while in the hospital setting. This suggests that many junior doctors may lack the confidence to discuss PA for health with their patients as they begin further training in GP or as a specialty trainee. While lack of training and support from consultants were major hindrances noted, this study also revealed that unexplored opportunities exist for junior doctors to incorporate PA counselling in both primary and secondary care.
Supplemental Material
sj-pdf-1-hej-10.1177_0017896921999074 – Supplemental material for Physical activity counselling among junior doctors in the UK: A qualitative study
Supplemental material, sj-pdf-1-hej-10.1177_0017896921999074 for Physical activity counselling among junior doctors in the UK: A qualitative study by Jimisayo Osinaike and Sandra Elaine Hartley in Health Education Journal
Footnotes
Acknowledgements
We thank Jenny Caunt for her support throughout the research. The authors declare that they have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.