
Abstract
Objective:
Evidence suggests the increased prevalence of diabetes among South Asian (SA) adolescents is due to their genetic risk profile. The South Asian Adolescent Diabetes Awareness Program (SAADAP) is a pilot intervention for SA youth in Canada with a family history of type 2 diabetes mellitus (T2DM). We sought to investigate changes in (1) diabetes knowledge and associated risk factors, (2) risk perception and (3) health behaviours among adolescents participating in SAADAP.
Design:
One-group pre-test, post-test design informed by a commitment to community-based participatory research (CBPR).
Setting:
Sixty-eight adolescents aged 13–17 years with a family history of T2DM participated in SAADAP in a clinical-community setting in Canada.
Method:
Pre–post questionnaires were administered to evaluate diabetes knowledge and associated risk factors, risk perceptions and health behaviours. Analyses were restricted to 49 participants who attended at least four diabetes education sessions.
Results:
The mean age of adolescents was 14.5 years, and 57.1% self-identified as girls. The difference in knowledge about the definition, symptoms and complications of T2DM from baseline to post-intervention was 3.32 out of 21 (p < .001) among SA youth. There was significant increase in learning about diabetes risk factors (p < .001) from baseline to post-intervention. Almost 60% of participants exhibited no change in their risk perception after intervention. Approximately two-thirds of the participants self-reported positive changes in health behaviours after completing the programme.
Conclusion:
SAADAP showed promising outcomes in raising knowledge and improving health behaviours in SA adolescents with a family history of diabetes. Larger controlled trials with longer follow-up are recommended to support and expand on the current findings.
Keywords
Introduction
South Asian (SA) diasporic communities living in Canada report disproportionately high rates of type 2 diabetes mellitus (T2DM) (26.7%) compared to their white counterparts (11.6%) (Banerjee and Shah, 2018, 2020). As a result of migration due to social, economic and political factors, SA families in Canada can trace their heritage to India, Pakistan, Sri Lanka, Bangladesh, Nepal, the Caribbean, Africa, the Middle East and/or other parts of the world (Shukla, 2001). There is evidence of a heightened risk of prediabetes at an early age among members of such communities in Canada (Fazli et al., 2019).
T2DM is a highly heritable condition, with many SA adolescents having a parent or grandparent with T2DM (Qi et al., 2015). This family history reflects genetic susceptibility, as well lifestyle and social factors shared within families (Pandey et al., 2013). SA adolescents have been shown to have greater insulin resistance than white children, even after adjustment for body mass index (BMI) and visceral adiposity (Anand et al., 2016). From a behavioural perspective, studies have reported SA adolescents tend to consume greater amounts of carbohydrate, partially with a high glycaemic index (e.g. roti and rice) coupled with lower levels of physical activity (Banerjee et al., 2015; Merchant et al., 2007). Social and economic conditions are increasingly being viewed as primary influencers and predictors of diabetes outcomes in SA communities tied to their pre- and post-migration experiences (Banerjee and Shah, 2020). Factors such as access to health and healthcare, social and community context, neighbourhood and built environment, education and economic stability collectively contribute to higher risk of SA adolescents developing T2DM. (Namdarimoghaddam, 2020). These can manifest through limited opportunities for physical activity and healthy eating in this racialised population (Banerjee and Shah, 2018; Fazli et al., 2019; Misra and Ganda, 2007).
Culturally grounded interventions focused on lifestyle strategies must begin early in SA communities living in Canada to prevent the onset of T2DM (Thomas et al., 2012). Community-based educational interventions such as the Indian Diabetes Prevention Program (IDPP) have shown that increases in physical activity and healthy diet can reduce T2DM incidence in SA adults, and that these benefits surpass those afforded by pharmacological therapy (Ramachandran et al., 2007, 2010). However, to date, the availability and evaluation of diabetes education programmes focusing on SA adolescents are limited in the scientific literature. Given that adolescence represents a critical period for the onset of adverse diabetes-related conditions, intervening during this developmental period is a strategic and promising opportunity for prevention (Wolf et al., 2021). The few diabetes education programmes tailored for Black, Latino and Indigenous adolescents with a family history of T2DM show knowledge, lifestyle behaviours and selected anthropometric outcomes to be positive (Holcomb et al., 1998; McKenzie et al., 1998; Marlow et al., 1998). These interventions have taken into account social determinants including culture, built environment, education, working conditions and access to healthcare that contribute to disproportionate rates of T2DM in ethno-racial and low socio-economic status communities (Williams et al., 2017).
The first of its kind, the South Asian Adolescent Diabetes Program (SAADAP) was developed in Canada to provide a culturally grounded infrastructure to support SA youth with a family history of T2DM. The goal of this pilot community–based programme was for SA youth to acquire a combination of awareness and knowledge of their risk, skills, resources and experiential strategies to make physical activity and healthy eating an accessible, integral and routine part of life. Success in the implementation of any diabetes education programme is dependent on context-specific information. Therefore, a unique aspect of this programme was the importance of helping SA youth to enhance their knowledge and awareness of the social determinants of diabetes in their diasporic communities while offering strategies for lifestyle change. Understanding the social and environmental factors shifts away from solely focusing on symptomatology and treatment of the disease as in traditional diabetes interventions (Harper et al., 2019). This alternative approach seeks to dispel diabetes-related stigma experienced by SA communities that includes being culturally blamed and shamed by healthcare professionals for having a high burden of diabetes (Beverly et al., 2019; Greenhalgh et al., 2015).
The purpose of this pilot study, therefore, was to investigate changes in (1) diabetes knowledge and associated risk factors, (2) risk perception and (3) health behaviour among SA adolescents participating in the programme .
Methods
Research design
We used a one-group pre-test, post-test design to evaluate the pilot SAADAP intervention in a style guided by community-based participatory research (CBPR) (Horowitz et al., 2008). An established SA Youth Advisory Group worked together with the intervention team to design a community-driven, culturally and youth-appropriate evidence-based diabetes education programme to benefit SA adolescents with a family history of T2DM. The primary role of the advisory group was to provide insight and feedback on programme design, implementation and evaluation. The study was approved by the University of Toronto Research Ethics Board (REB # 35077).
Theoretical framework
The SAADAP approach is rooted in Critical Consciousness Raising (CCR) (Wiggins and Perez, 2017), which seeks to go beyond the individual to identify and evaluate the social determinants of T2DM. Health education programmes that have a secure theoretical background show promising results (Horowitz et al., 2008). CCR is a concept derived from popular education, also known as Freirean education, and may be used to promote SA adolescents’ awareness of the social and environmental factors in their lives that impact their risk in developing T2DM. Through a process of critical consciousness raising, SA individuals and groups are able to redefine themselves and their diabetes risk in a more positive, health-promoting and affirming manner based on their own perspectives and social realities as opposed to those assigned to them by others (Harper et al., 2019). This process of gaining critical consciousness and an understanding of one’s social environment, coupled with active engagement in one’s community and a heightened sense of competence, was a critical aspect of the diabetes education programme evaluated here.
Recruitment and selection criteria
Prospective study participants aged 13–17 years with a family history of T2DM were identified and recruited through SA adult patients accessing services at a diabetes and endocrinology clinic in the Peel Region of Ontario, Canada. This site was chosen since the SA population comprises 27.7% of the local population and experiences a high T2DM disease burden (Desai et al., 2021) . Classification of family history was based on participants having at least one biological parent and grandparent diagnosed with T2DM (Berentzen et al., 2016). Staff at the collaborating clinic presented parents and/or grandparents with T2DM with the opportunity to enrol their children/grandchildren in SAADAP.
Information pamphlets were distributed at the clinic. Interested individuals were directed to a multi-lingual SAADAP team member who was present in the clinic waiting room. The research coordinator followed up with patients who self-identified as SA and their children/grandchildren over telephone to confirm eligibility. Adolescents were excluded if they were in receipt of treatment for T2DM themselves, had been diagnosed with type 1 diabetes mellitus or had a pre-existing condition that could interfere with physical activity participation. Informed assent and parental consent were obtained from eligible SA adolescents in person at the clinic prior to baseline data collection.
Each participant received a CA$10 Amazon gift card after completing each questionnaire in this study. For adolescents, participation in the SAADAP was considered community involvement hours that formed part of the Ontario Ministry of Education high school graduation requirement.
Intervention
The SAADAP curriculum was adapted from the Diabetes Prevention Program (Diabetes Prevention Program Research, 2002), the Indian Diabetes Prevention Program (Ramachandran et al., 2006) and the Diabetes Community Lifestyle Improvement Program (Weber et al., 2016). It included educational components about T2DM risk, prevention and behavioural self-management. One of the key objectives of the curriculum included increasing baseline knowledge and awareness of T2DM based on local social and environmental conditions that encompassed factors such as income, education, housing and access to nutritious food and physical activity opportunities (Walker et al., 2015).
The programme was delivered across a 10-week time frame in a clinical-community setting. Participants were required to attend in-person weekly sessions run by SA registered dietitians and registered kinesiologists between October 2018 and December 2018 (n = 40) or between January 2019 and March 2019 (n = 40). Eight 1.5-hour sessions were delivered across six groups of 10–15 adolescents (Steinsbekk et al., 2012). Every session contained experiential learning components such as healthy cooking and exercise demonstrations, interactive games, critical discussion of the social and environmental determinants of T2DM, intention and goal setting.
The exercise curriculum included structured components that include engaging in aerobic activities, anaerobic activities and resistance exercises. The exercise sessions were designed to support ongoing active living with family and friends with minimal cost and equipment. The nutrition education centred on traditional and non-traditional forms of SA cooking. There was a field trip to a prominent chain grocery store that sold SA foods to learn how to read labels on food products and make healthier and affordable food choices. A parent or grandparent was invited to attend the last group session with each participant, and siblings were also encouraged to be part of the final interactive cooking session. This session fostered social support from family members and created a supportive social environment, which may further contribute to sustained health behaviour changes to prevent and manage T2DM (Williams et al., 2017).
In addition, every participant had access to two individual consultations (at weeks 1 and 10 of the intervention) each with a dietician and a kinesiologist to create a tailored diet and exercise programme in relation to available resources, time, socio-economic circumstances, religious and cultural needs.
Data collection
Each participant completed a series of on-line questionnaires prior to participating in the SAADAP programme and a second follow-up questionnaire 1 week after the 10-week intervention. All questionnaires had been evaluated for face and content validity using a modified Delphi Panel approach involving clinical experts in the diabetes field. The questionnaires were also pilot tested for completion time and comprehension by the Youth Advisory Group to ensure they were appropriate for the adolescent audience.
Completion of the questionnaires took approximately 20–30 minutes. Age, gender and household income were collected at baseline. The instruments used to measure diabetes-related knowledge, risk perception and health behaviours are described below.
Knowledge
Definition, Symptoms and Complications: Diabetes knowledge was assessed by an adapted version of the Brief Diabetes Knowledge Test (BDKT) (Fitzgerald et al., 2016), a validated tool used in a wide variety of populations. This indicator evaluated participants’ knowledge of the definition, symptoms and long-term complications of T2DM. Items included true or false questions and questions with one correct answer and two detractors. Correct items were given a score of 1 and incorrect items were scored 0. Sub-question scores were summed from the Diabetes Knowledge question, producing a possible range from 0 to 21.
Risk Factors: Relevant biological, behavioural and psychosocial diabetes risk factors were assessed in line with approaches used in previous studies (Kim et al., 2007). Survey items to assess social and environmental factors were created by the study investigators who are experts in this content area. Change in knowledge of diabetes risk factors was reported per dimension. Each dimension was summed to a maximum score of 6 for Biological factors (e.g. family history), 4 for Behavioural factors (e.g. not exercising enough), 4 for Psychological factors (e.g. depression), 3 for Social factors (e.g. having a low family income) and 3 for environmental factors (e.g. poor housing).
Risk perception
This measure was assessed via participants’ rating of their risk of getting diabetes by the time they reached their parent’s age as almost no chance (less than 1%), slight chance (1%–5%), moderate chance (6%–20%) or high chance (greater than 20%) (Kim et al., 2007).
All change scores were calculated as post-intervention scores minus baseline scores. Positive scores represented enhanced risk perception after the workshops. A negative value denoted decreased perceived risk, 0 meant no change and a positive value signified an increase in risk perception
Health behaviour
A post-intervention questionnaire was administered to evaluate self-reported behaviour changes following the SAADAP. The question asked was, ‘Since completing the SAADAP, what changes you have you made?’ Adolescents had the option of checking up to a maximum of 18 protective behaviours related to physical activity and dietary patterns to reduce their risk of T2DM. This question was developed by the study team based on previous research and in line with Canadian clinical practice guidelines for the prevention of diabetes (Lipscombe et al., 2014).
Analysis
Normally distributed data are reported in terms of means and standard deviation (SD), non-normally distributed data are reported with medians and interquartile range (IQR) and categorical data are expressed as frequencies with percentages.
To measure change in diabetes knowledge scores from baseline to post-intervention, we fitted a mixed model with a random intercept for participants. This model, unlike linear regression, accounts for the fact that the study followed the same participants before and after the diabetes education counselling sessions, thus making observations correlated and not independently distributed at the participant level. Mixed models comprised fixed and random effects. The fixed effects of our model included visit (categorical variable with two levels: baseline or post-intervention), age (continuous variable), gender (categorical variable with two levels: female or male) and time of intervention (categorical variable with two levels: September 2018–December 2018 or January 2019–March 2019). There were no interaction terms in the model (an interaction between age and gender was tested but was not significant, so removed from the model). To adjust for participants’ baseline score affecting their change score outcome, a random effect for participant was added. This allowed us to resolve this non-independence by assuming a different ‘baseline’ knowledge score for each participant. For both the univariate analyses and the multivariate analyses (adjusted for age and gender), diabetes knowledge outcomes were included as the dependent continuous variable.
All analyses were restricted to participants who had attended at least four of the eight diabetes education sessions. Research on diabetes prevention programmes offered in a community-clinical setting suggests that participants who attend four or more core sessions tend to achieve better outcomes (Vojta et al., 2013). A value of p < .05 was considered statistically significant. All questionnaire data were analysed using SAS 9.4 TS Level 1M3. Proc mixed was used for all mixed model analyses with a random statement for the participants.
Results
Baseline characteristics
Eighty SA adolescents with a family history of T2DM were recruited for the pilot programme, of which 68 (85.0%) agreed to participate with informed assent and parental consent. Forty-nine (72.1%) attended four or more of the SAADAP sessions, with an average attendance of six sessions. Within this group, 43 adolescents (87.8%) completed the questionnaires at baseline and post-intervention.
The mean age of participants was 14.5 years (Median 14–16); 57.1% were girls Approximately 59.2% reported their household income. Among those who did, 38.7% reported having a household income greater than $60,000. Many participants, about 40%, felt that they had a moderate chance of getting diabetes by the time they reach their parents’ age. Over one-third of participants believed that they had a high chance of getting diabetes at that age, and about a quarter thought they had a slight chance. Table 1 details participants’ baseline characteristics.
Participant characteristics at baseline (n = 49).
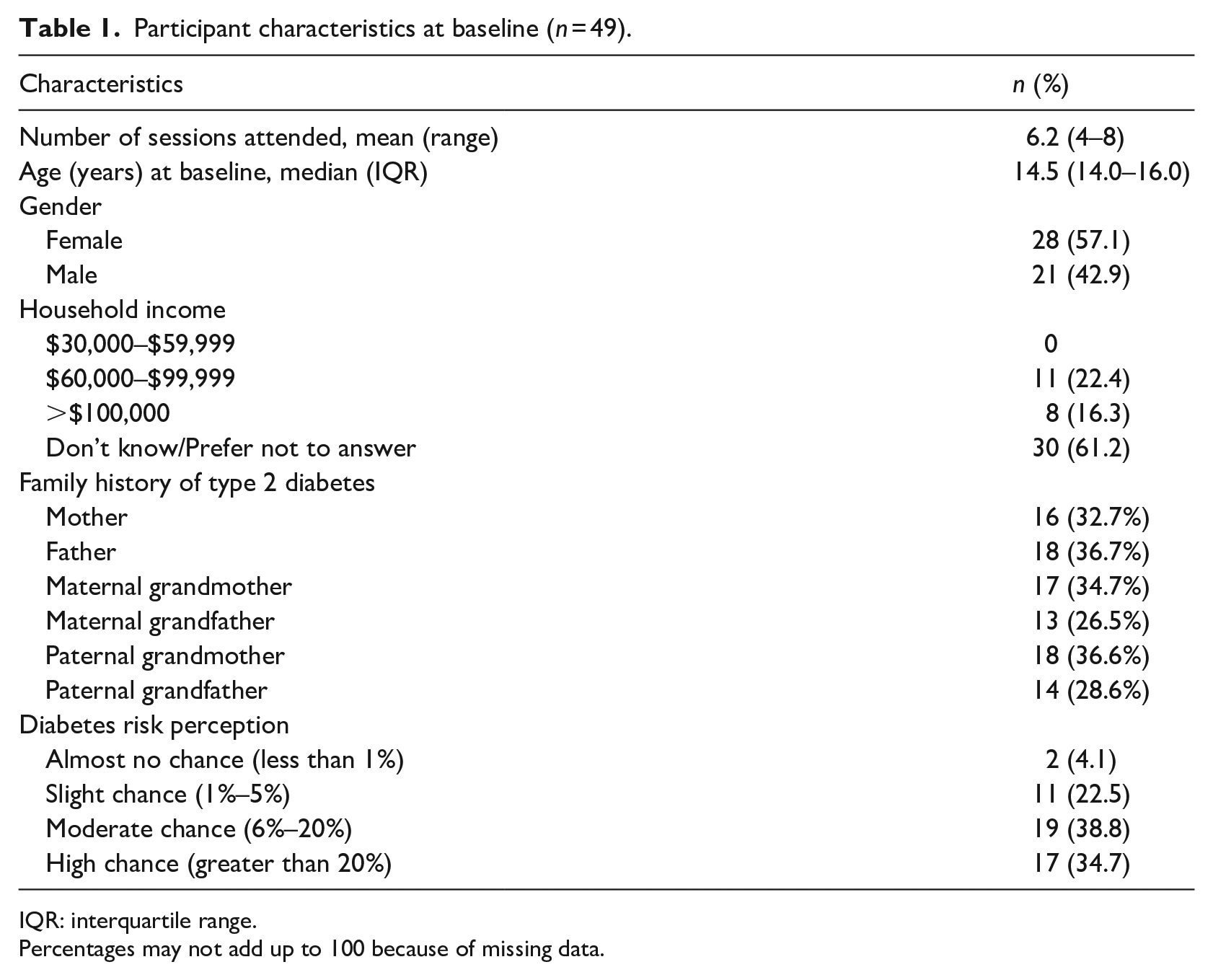
IQR: interquartile range.
Percentages may not add up to 100 because of missing data.
Change in knowledge – definition, symptoms and complications
Figure 1 shows that the diabetes knowledge score in understanding the definition, symptoms and complications increases at the post-intervention visit. Adjusting for gender and age, the difference in diabetes knowledge scores post-intervention from baseline on average for the cohort was 3.32 out of 21 (p < .001).
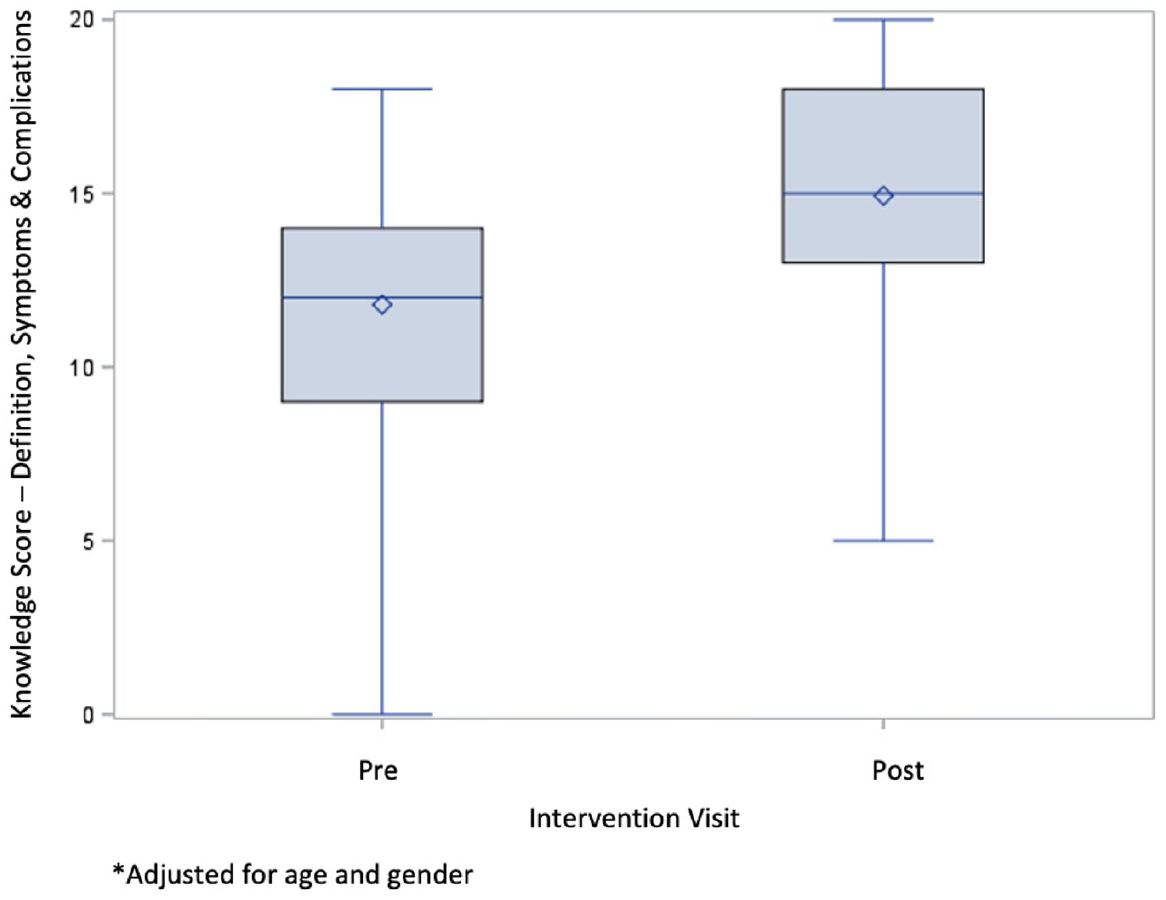
Change in diabetes knowledge in definition, symptoms and complications (pre–post intervention) (n = 43).
Change in diabetes knowledge – risk factors
In Table 2, the total and dimension mean risk factor scores are shown, each adjusted for gender and age. There was a significant increase in the total risk factor knowledge score (p < .001). The diabetes knowledge scores for the Social dimension increased by a score of 1.0 and the Environmental dimension increased by 0.7 out of 3, both being statistically significant (p < .001). The Psychological dimension score increased by a score of 0.35 out of 4, although this was not significant (p = .315). The diabetes awareness score for Biological dimension decreased post-intervention by 0.6 out of 6 (p = .014). Similarly, the score for the Behavioural dimension decreased post-intervention; however, this effect was not statistically significant.
Change in diabetes knowledge of risk factors (post-intervention–baseline risk) (n = 43).
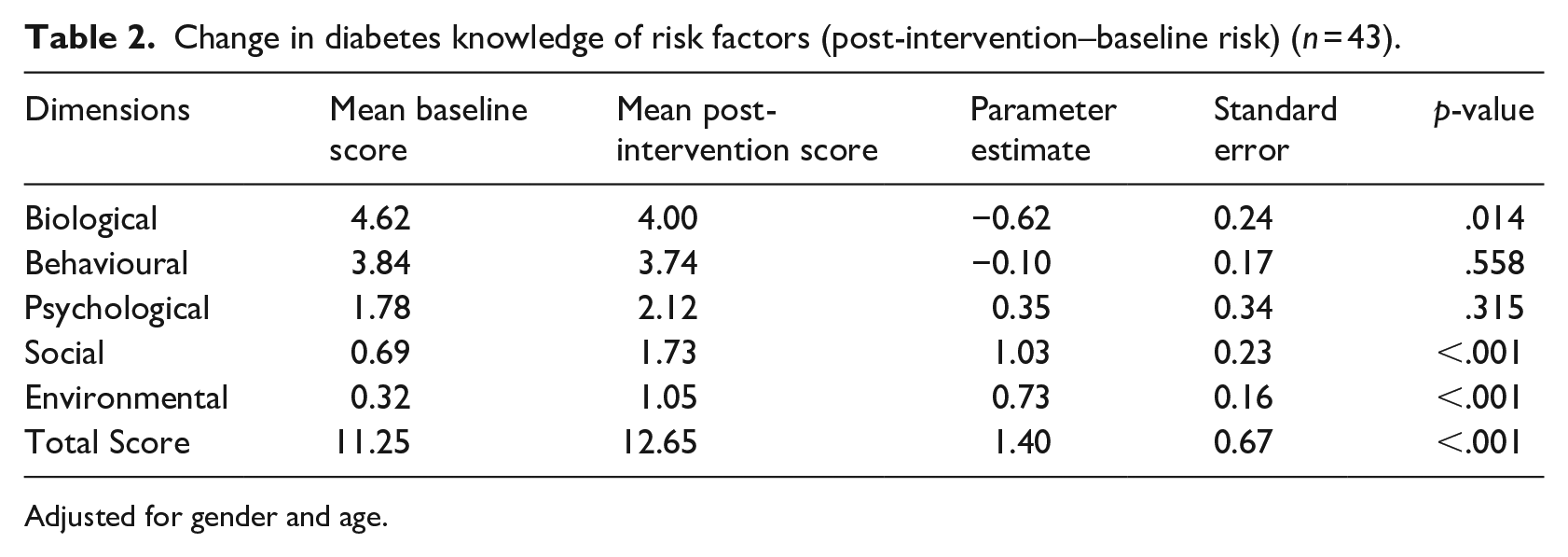
Adjusted for gender and age.
Change in perceived diabetes risk
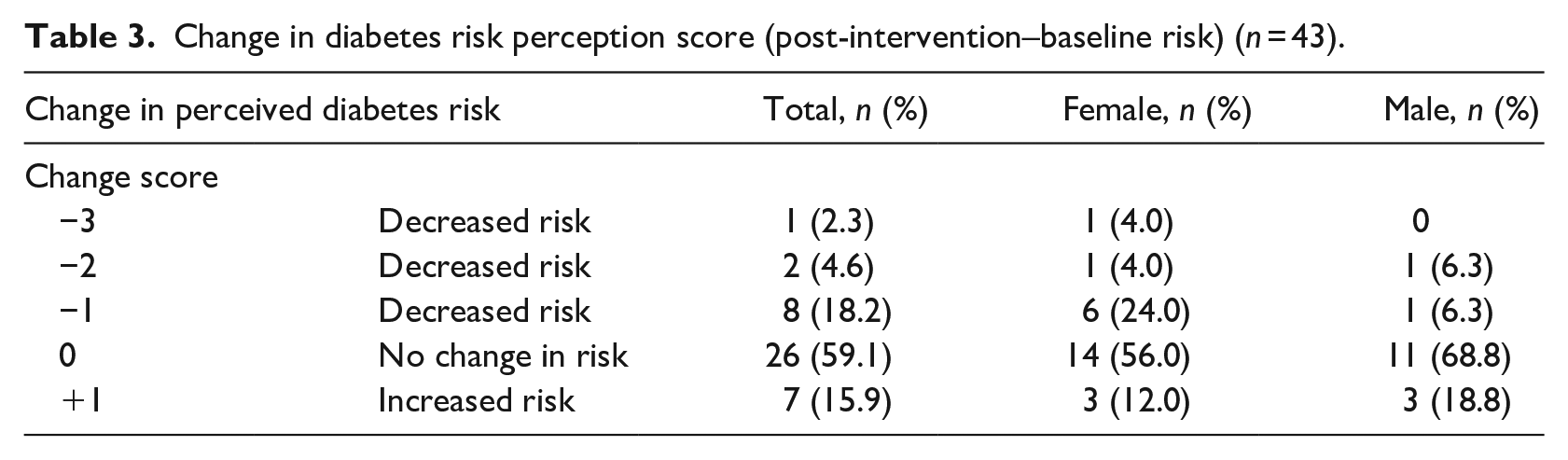
Almost 60% of participants reported no perceived change in diabetes risk after intervention, and a quarter of participants had decreased perceived risk, with a higher percentage of them being girls. Among approximately 16% of participants, perceived risk slightly increased at their follow-up visit, although this change was not statistically significant (χ2 = 3.11, df =4, p = .54) (see Table 3).
Change in diabetes risk perception score (post-intervention–baseline risk) (n = 43).
Change in self-reported health behaviours
Tables 4 and 5 summarise responses for self-reports of specific physical activity and dietary change after completing the intervention. Almost three-quarters of participants increased their physical activity overall (73.2%), encouraged their family to become more active (70.7%) and walked more frequently to get to places (70.7%). Most adolescents reduced their intake of sweets and junk food (80.5%), ate out less often (85.4%) and encouraged family members to eat healthier (80.5%).
Self-reported physical activity changes (post-intervention) (n = 43).
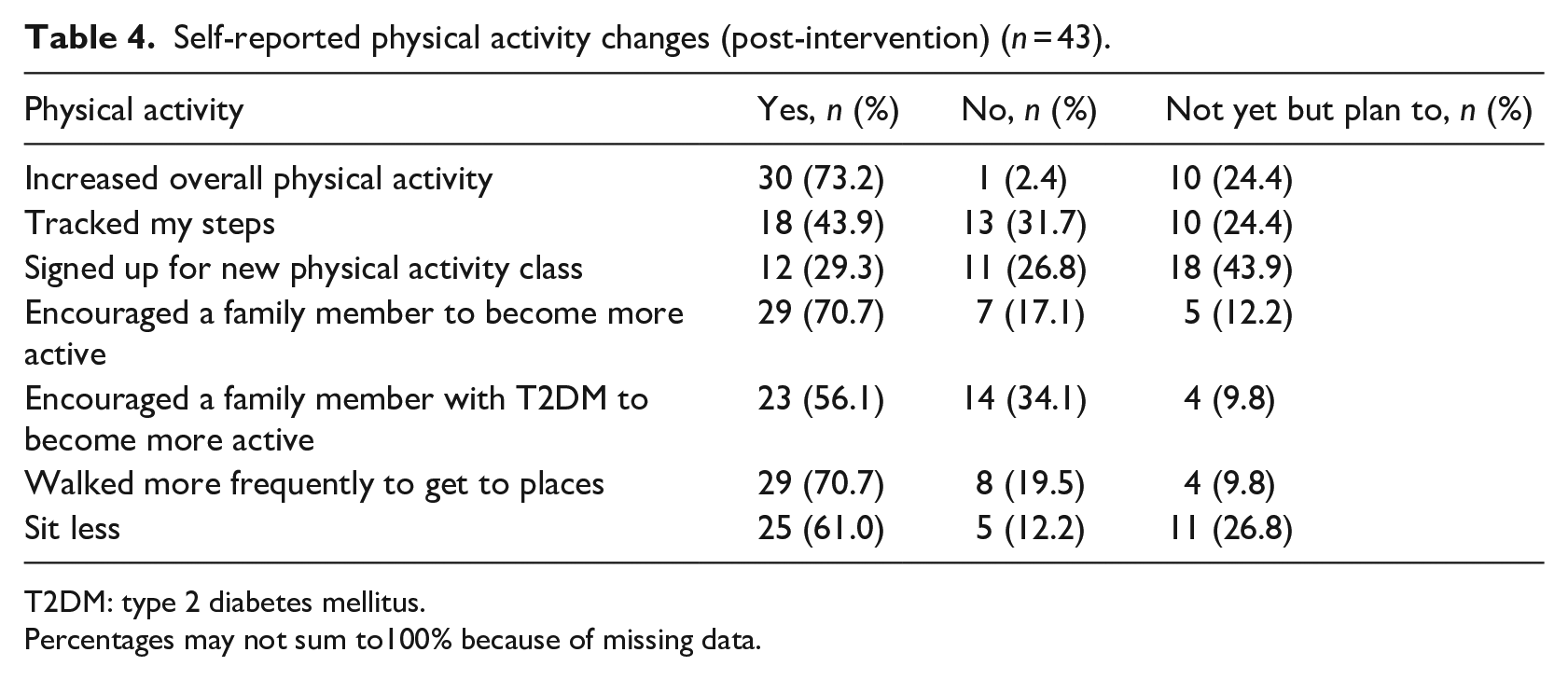
T2DM: type 2 diabetes mellitus.
Percentages may not sum to100% because of missing data.
Self-report of specific dietary changes (post-intervention) (n = 43).
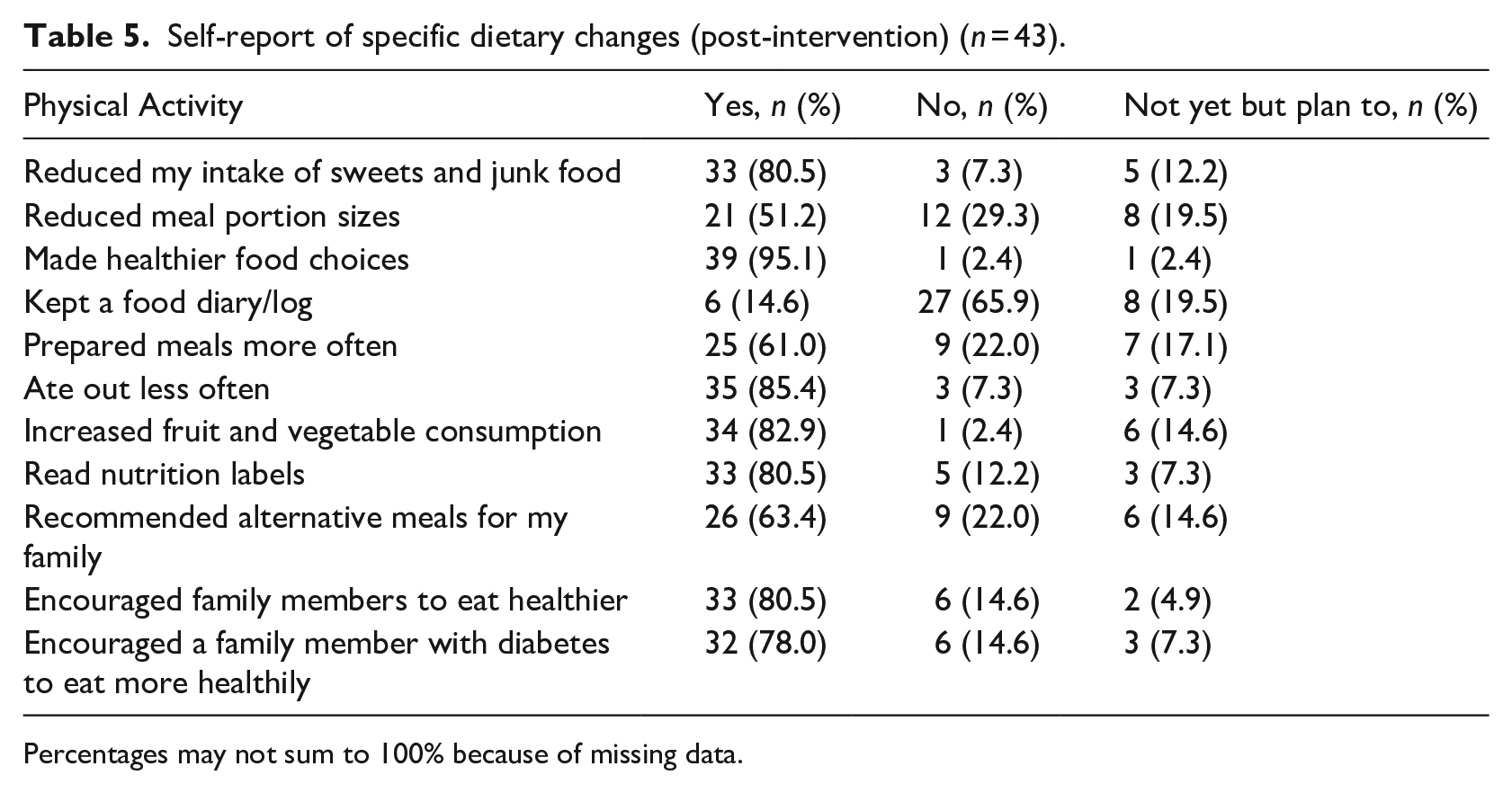
Percentages may not sum to 100% because of missing data.
Discussion
This pilot project is the first of its kind. The SAADAP was created, developed and implemented by SA academics and healthcare professionals with SA youth with a family history of T2DM living in the Peel Region of Ontario. This community-based and culturally relevant diabetes education intervention resulted in positive impacts on knowledge, risk perception and self-reported behaviours. An important and unique feature of the programme was its commitment to addressing social determinants in the disproportionate prevalence of T2DM in SA communities living in Canada. Overall, our findings show that after the intervention participants gained an enhanced understanding of T2DM as deriving from a complex interplay of social, environmental and genetic factors relevant to the SA population.
In line with previous studies in SA adults (Bhurji et al., 2016; Hawthorne, 2001), we observed an improvement in knowledge of the symptomatology and complications of T2DM among SA youth following the intervention. With regard to possible risk factors, awareness of the biological and behavioural factors was high for adolescents at baseline and remained relatively unchanged. This finding aligns with a survey study by Mahajerin et al. reporting high school students tend to have a high level of risk factor recognition, identifying obesity, physical activity, junk food, family history and race/ethnicity (Mahajerin et al., 2008). This high baseline level of awareness could be due to health promotion and disease prevention initiatives having a primary emphasis on genetic and lifestyle factors that increase T2DM risk in the general and SA populations (Bellary et al., 2008; Raphael et al., 2019).
It is well established that there are other non-biomedical factors that contribute to high rates of T2DM in the SA population (Banerjee and Shah, 2018; Walker et al., 2016), and awareness of relevant social and environmental factors was poor among the majority of SA adolescents upon entry to our programme. Disparities in income, education, poor housing and social support result in otherwise preventable cases of diabetes for immigrant groups (Gary-Webb et al., 2014). Knowledge of these factors at the end of the programme was significantly improved, suggesting that participants developed their critical consciousness about the contextual factors influencing the higher rates of T2DM. In the process of developing critical consciousness, SA adolescents unlearned dominant narratives regarding their risk for diabetes centred on their genetic predisposition and cultural behaviour (Greenhalgh et al., 2015; Raphael et al., 2019). They acquired a broader understanding of the social and ecologic context in which individuals are born, grow, live, work and age (Hill et al., 2013), which is increasingly recognised as contributing to the rising incidence of T2DM in the SA population. An individual with a higher level of critical reflection may be less likely to have a fatalistic attitude and feel stigmatised, which is common in SA communities (Patel et al., 2015) for situations created by social and environmental factors (Christens et al., 2013).
Critical consciousness strategies have been incorporated in HIV prevention interventions specifically for racialised youth and shown to elevate perception of health risk to a position of empowerment that promotes feelings of control and participation in healthy behaviours (Harper et al., 2019). Our study findings indicate the SAADAP is acceptable to young people within this racialised community and helps to promote behaviour change in nutrition and physical activity, important components of diabetes prevention (Ramachandran et al., 2006). Furthermore, a high number of adolescents indicated the programme also helped them to facilitate lifestyle change among family members diagnosed with T2DM. This could be attributed to the SAADAP incorporating strategies that are immersive and experiential rather than didactic, leading to health behaviour change among the adolescents and within their families (Bhurji et al., 2016). Further work is necessary, however, to examine the development of critical consciousness as a process that involves changes in knowledge and perspectives, as well as behaviours at the individual, family and community levels.
A high proportion of participants felt they had a moderate to high chance of getting diabetes by the time they reach their parents’ age at baseline. This was in contrast to studies showing low risk perception is prevalent among SA adults even with known risk factors such as family history (Mukerji et al., 2016). Most participants exhibited no perceived change in diabetes risk after intervention, however, with risk perception increasing for some. Perceptions of higher risk in turn may be important motivating factors for preventive health behaviour (Harrison et al., 2003). Future research should examine whether there is a correlation between diabetes risk perception and prevention efforts (e.g. engaging in physical activity and healthy eating) in SA families and communities at risk of diabetes.
Limitations
There are several limitations that should be taken into account in the interpretation of the findings reported here. First, generalisability was limited because of the restricted sample of 49 adolescents with a family history of T2DM in the Peel Region of Ontario for analysis. Second, while the analysis evaluated change in knowledge and risk perception outcomes pre-to-post SAADAP, adolescents were not randomised to the programme, and thus these estimates of change cannot be interpreted as causal. Third, the impact of the SAADAP could be estimated only for those who attended four sessions or more. However, these participants were similar to those who attended fewer than four sessions on most baseline characteristics, suggesting that the findings are not substantially biased by differential attrition. In addition to attrition, missing data on some variables reduced the sample size available for analysis. Although several steps were made to ensure that questions could be answered with anonymity, it is likely that some participants withheld pertinent information on socio-demographic characteristics. Finally, the self-reported data on health behaviour changes could be vulnerable to social desirability bias. SA adolescents may overreport the number of health behaviour changes made if they are aware of the importance of these changes and wish to appear adherent to recommendations. Given the novel and exploratory nature of the pilot study, the findings derived from significance tests should therefore be confirmed in large-scale and trial studies.
Strengths
This study has major strengths in that the SAADAP reflects the shared vision and knowledge across multiple groups of SA stakeholders: researchers, healthcare professionals, community-based organisations, public health students and community members. The pilot programme was developed and delivered to a high-risk racialised community in a manner informed by evidence-based public health initiatives such as the Diabetes Prevention Program and Indian Diabetes Prevention Program. SAADAP is an accessible and culturally grounded programme to increase knowledge about T2DM prevention that encourages physical activity and healthy eating to attenuate risk among South Asian communities in Canada. Study findings support the development of health education activities not currently available to enable SA youth to better understand relevant structural issues within the local community. Pilot findings will also aid in the design of a future clinical trial to evaluate SAADAP.
Footnotes
Acknowledgements
We thank members of the Youth Advisory Group and Steering Committee for their ongoing participation in this project. We acknowledge LMC Diabetes & Endocrinology for providing access to SA patients for recruitment. We thank Ravnit Dhak, Lalitha Bhagavatheeswaran and Erika Kouzoukas for their support in the design and delivery of SAADAP. We thank Nuzha Hafleen and Harsh Naik for assisting in the statistical analysis. Finally, we thank youth participants and their parents for their willingness to engage in research to reduce diabetes risk within the local SA community.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. We are grateful to the Lawson Foundation for funding this project as part of their Child & Youth Diabetes Strategy (GRT 2016-119; GRT 2019-23; GRT 2020-43).