
Abstract
Objective:
The effectiveness of health education for patients has often been suboptimal. The neglect of a focus on empowerment and the presence of implementation barriers have been put forward as possible explanations for this. This study aimed to gain insight into how to co-create and develop an empowerment theory-based health education intervention for urological cancer patients.
Design:
Bravo’s empowerment intervention model provided the theoretical foundations for the work undertaken with urological cancer patients in the Netherlands, using a participatory interactive learning and action approach.
Method:
Insights into needs regarding health education were obtained through semi-structured interviews with patients (n = 22) and health professionals (n = 17). Subsequently, eight co-creation sessions (n = 30) were organised to translate these needs into a health education intervention.
Results:
An intervention in the form of digital patient information was developed. The information offered provides a view of the different care steps based on clinical guidelines but personalised in different ways. By connecting patients’ empowerment needs to the information provided, and by taking health professionals’ perspectives into account, barriers to health education were made visible and addressed.
Conclusion:
Patient empowerment theory proved valuable in better aligning a participatory research process with the empowerment needs of urological cancer patients. The programme theory developed may offer a valuable template for the development of future health education interventions.
Keywords
Introduction
Patients are increasingly expected to be responsible for their own disease and care management, but often experience difficulties in doing so (Jerant et al., 2005). Lack of relevant knowledge, the complexity of the benefits and disadvantages of treatments, and uncertainties regarding the care process limit the capacity to make informed choices (Balogh et al., 2011; Schulz and Nakamoto, 2013). Health education interventions are designed to increase patients’ knowledge about disease and care management (Davison and Degner, 1997; Wilkes et al., 2000) and are expected to lead to more informed and empowered patients (e.g. Bergsma, 2004; Prigge et al., 2015). The empowerment of patients could subsequently shift power and responsibilities from health professionals to patients. This shift may improve the quality of care through, for instance, better treatment decision-making and the use of self-management opportunities (e.g. Anderson et al., 2009; McCorkle et al., 2011; Schmidt et al., 2015), leading to improved health outcomes (Powers and Bendall, 2004).
The effectiveness of current health education interventions has, however, been suboptimal (e.g. Kuijpers et al., 2013; Mason et al., 2008). One possible explanation is that health education interventions are limited in scope or not consistently adopted (Loudon et al., 2014). Besides implementation challenges, the impact on patient empowerment is often suboptimal (Kuijpers et al., 2013; Mason et al., 2008), itself the result of a neglect of empowerment conceptualisations in the health education literature. The concept of patient empowerment is multilayered and multidimensional, making it difficult to apply the concept consistently and operationally (Gibson, 1991). In the most commonly accepted definitions, the focus is on one of the following: (1) empowerment as a transformative process; (2) the principles and ethos of empowerment; or (3) empowerment interventions (Bravo et al., 2015). Consequently, empowerment carries different connotations in different contexts and among different population groups (Jupp et al., 2010; Zimmerman, 2000).
There is a pressing need, however, for greater insight into how health education interventions might contribute to patients’ empowerment and what information should be provided and in what way. When designing an intervention, it is valuable to use programme theory, which consists of a set of statements that explain why, how and under what conditions the effects of the programme are expected to occur (Sidani and Sechrest, 1999). Through programme theory, research inputs and activities can be aligned to help to achieve the intended outcomes (Funnell and Rogers, 2011; Scheirer, 1987). A good quality programme theory is therefore the key to a successful intervention. In the light of this, this study aimed to gain insight into how to co-create and develop an empowering theory-based health education intervention using programme theory. Our focus was on developing an online health education intervention for urological cancer patients. The incidence of urological (prostate, bladder and kidney) cancer in the Netherlands is relatively high (around 20%) compared to other cancer types, with 22,754 cases in 2017 making it one of the most prevalent diseases (IKNL, 2015). Urological cancer patients often have to cope with (long-term) physical and psychosocial consequences that affect their quality of life (Sanda et al., 2008). In particular, the chronic nature of the disease and the diversity of treatment options call for greater patient empowerment (McAllister et al., 2012).
Methods
To develop an online empowering health education intervention, an intervention design study was conducted between December 2015 and March 2017. The study took the form of a collaboration between the Vrije Universiteit Amsterdam, the European Association of Urology (EAU), and the Prostaatkankerstichting and Leven met blaas-of nierkanker foundations. A transdisciplinary project team 1 was established to guide the study. Project team members met before the start of each project phase to discuss the plans and to reflect on the outcomes of the previous phase.
Developing the initial programme theory
To develop the programme theory for the health education intervention for patients, Bravo et al.’s (2015) patient empowerment intervention model was used as a starting point (Figure 1). This model, developed to enable the design and evaluation of empowerment interventions, seeks to integrate existing definitions and constructions (Prigge et al., 2015; Small et al., 2013; Thomas and Velthouse, 1990). According to the model, patients’ empowerment level is informed by the ethos present at three different levels: (1) the patient, (2) the health provider and (3) the health system through the implementation of individual- and group-focused interventions.
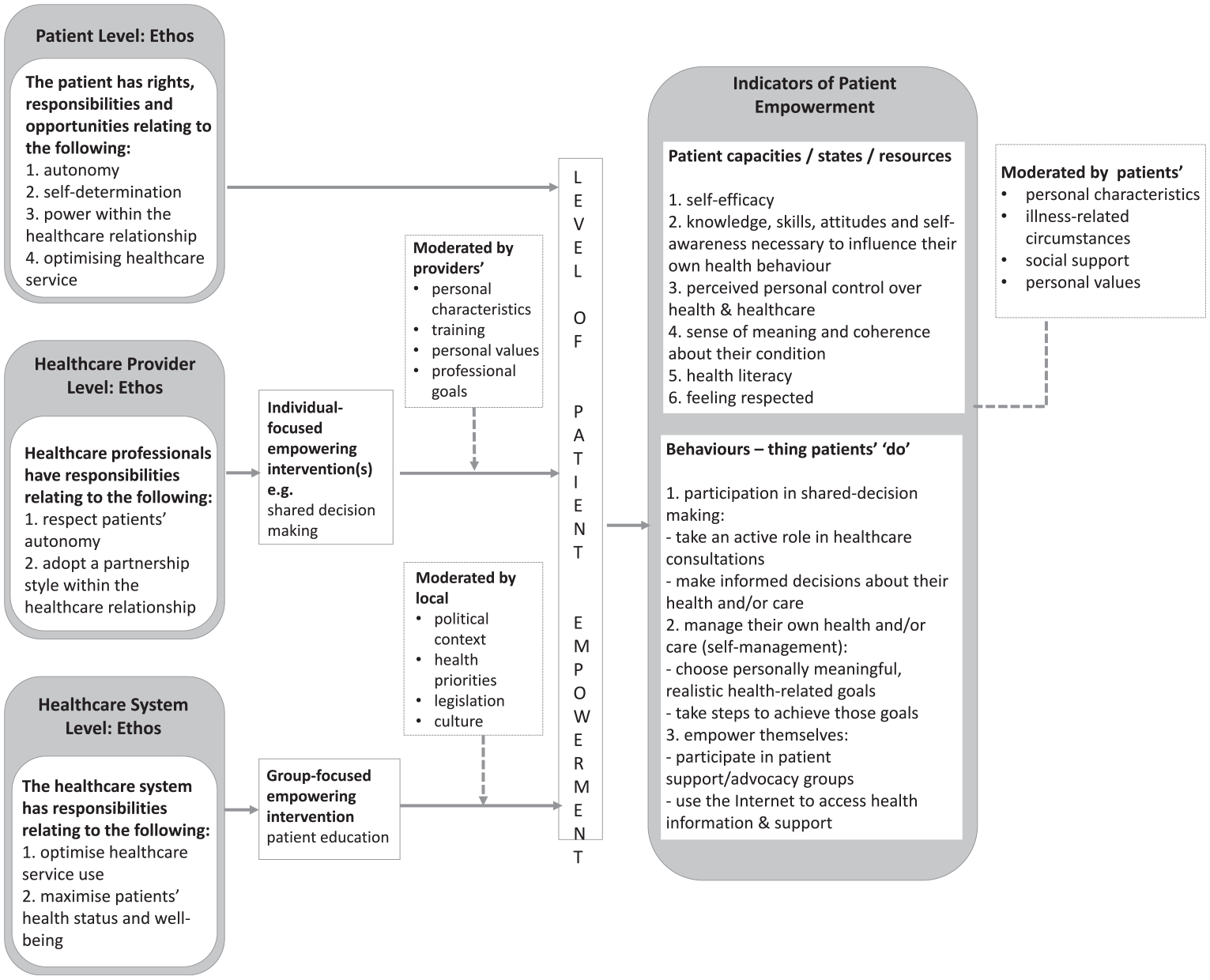
Conceptualisation of patient empowerment based on the patient empowerment model of Bravo et al. (2015).
The level of empowerment can be determined by two types of indicators: patients’ capacities or the resources for empowerment (states), and patients’ empowerment behaviours. States focus on the needs of patients in terms of capacities and resources to become empowered. Behaviours reflect a response to the state of empowerment and comprise actions that increase the level of empowerment. They include shared decision-making, self-management and the empowerment of patients by themselves. Bravo et al. (2015) hypothesise that the relationship between state and behaviour is reciprocal, meaning that one person’s resources influence his or her behaviours, which in turn impact the extent to which certain resources are gained.
Together, the indicators affect patients’ quality of life and well-being, and subsequently their clinical outcomes. These indicators have not been included in the conceptual model since the outcomes were not within the scope of this study.
Designing the programme theory
Because patients live with a disease every day, they have experiential knowledge regarding their empowerment needs (Caron-Flinterman et al., 2005). Choudhury et al. (2020) addressed this issue by involving patients in the development of a health education intervention, so that the intervention might reflect patients’ state of empowerment. In this study, a participatory research approach was adopted whereby the experiential knowledge and empowerment needs of the target group formed the basis for the research (e.g. Bergsma, 2004; Sheely, 2018).
The participatory process used was informed by an Interactive Learning and Action (ILA) approach, which involved developing trust among stakeholders, stimulating learning and generating a shared vision (Betten et al., 2013). The ILA approach has been found to be a valuable approach to empowering vulnerable groups such as patients by articulating and integrating experiential knowledge (Caron-Flinterman et al., 2005). The process comprised four phases: (1) setting the conditions, (2) determining patients’ and health professionals’ needs regarding health education, (3) integrating these existing needs into a health education intervention, and (4) developing and implementing the intervention.
Phase 1: setting the conditions
During this first phase, the context of the project and relevant conditions for the involvement of patients were identified, based on the current literature and discussion between the project team members and the relevant stakeholders. Stakeholders were selected based on the advice of the project team members and snowballing and consisted of medical experts in the field of urological cancer, representatives of the Dutch Nederlandse Vereniging van Urologie and Federatie Medisch Specialisten organisations, and the chairpersons of two Dutch patient organisations. Contact with the stakeholders was established to obtain a general idea about the challenges that arise from current health education interventions for urological cancer patients in the Netherlands.
Phase 2: determining patients’ and health professionals’ needs
Semi-structured interviews were conducted with 22 patients with urological cancer and 17 health professionals (urologists and specialist nurses). Patients were recruited via the two Dutch patient organisations by way of emails, newsletters and social media. In addition, flyers were distributed in hospitals in the Netherlands. Health professionals were recruited via the network of the EAU and its Dutch counterpart, the Nederlandse Vereniging van Urologie. When we were recruiting, our aim was to ensure a balanced representation of health professionals working at different hospitals treating urological cancer patients in the Netherlands. Supplemental online appendices 1 and 2 provide an overview of the characteristics of patients and health professionals interviewed. The interviews were conducted face to face (n = 29) and by telephone (n = 10) and took approximately an hour to an hour and a half to complete. An interview guide 2 was used to structure the interviews (available in online supplemental appendices 3 and 4). For patients, the interviews consisted of a timeline interview in which patients discussed their condition and care management in chronological order. Each step was related to their experiences of and needs for information and empowerment (including the elements of the conceptualisation of patient empowerment depicted in Figure 1). The same topics were discussed with health professionals, although no timeline was used.
Phase 3: integrating needs into an intervention
For each urological cancer domain, 3 two co-creation sessions were organised. In total, 30 patients and health professionals joined the sessions (see online supplemental appendix 5 for participants’ characteristics). Many participants attended both sessions for each cancer type. Each session lasted 3 hours and was moderated by the first author and a colleague. In the first session, the structure, format and required content for the health education intervention were described, informed by phase 2. During these sessions, it was unanimously decided to develop digital patient information based on the different steps in the care pathway and structured in different layers. Before the second session on each cancer domain, draft texts in support of this approach were developed by professional writers. These texts were then ordered according to how they might form different sections within the future digital patient information but were initially drafted as Word documents. In each second session, the participants commented on the drafts prepared. The draft texts were reviewed regarding length, readability, comprehensibility and accuracy, and whether the content of the texts aligned (or did not align) with local variations between hospitals. If additional information was needed, suggestions for sources were given. Furthermore, participants also considered whether additional topics and relevant resources needed to be added.
Phase 4: developing and implementing the intervention
Based on the outcomes of phase 3, a final template for the health education intervention – in the form of digital patient information – was developed by professional writers. Feedback on this template was obtained via the participants in phase 3 (n = 24) and the members of the project team. Subsequently, potential implementation steps were discussed and decided upon with the project team. Before implementation, the digital patient information was tested with a broad group of patients and health professionals via general meetings at the patient organisations 4 and a professional conference. 5 A majority of patients and health professionals were appreciative of the information developed.
Data analysis
The interviews were transcribed verbatim. Subsequently, the transcripts were analysed using the qualitative data analysis programme MAXqda 2007. First, deductive analysis took place, based on the main concepts in the conceptual model. Second, insights relating to the main concepts were identified via an inductive approach comprising three steps: (1) open coding: identifying, categorising and describing insights; (2) axial coding: creating subcategories; and (3) selective coding: developing a storyline (Thomas, 2006). The coding scheme is shown in online appendix 6. Extensive notes made during the co-creation sessions provided input regarding on whether the different stakeholders’ views complemented each other and were integrated into decisions about the development of the health education intervention.
Ethical considerations
According to Dutch law, the approval of a formal medical ethics committee was not required because this study was non-invasive, and participants were over 18 years old. The study, however, complied with the national Code of Ethics for Research in the Social and Behavioural Sciences involving Human Participants (VCWE, 2016). All respondents received written and verbal information about the aims of the study and that they could withdraw from the study at any time without giving reasons. All data were anonymised before analysis and stored securely via Surfdrive, a cloud service for higher education and research in the Netherlands.
Results
The findings are structured and described in accordance with the phases of the ILA: (1) patients’ and health professionals’ needs regarding health education (phases 1 and 2), (2) integrating the needs into an intervention (phase 3), and (3) developing and implementing the intervention (phase 4).
Patients’ and health professionals’ needs
The articulated needs of patients and health professionals regarding health education are described in line with the elements of the conceptualisation of patient empowerment shown in Figure 1.
Ethos
Patients’ views on autonomy, self-determination and power within the health care relationship impacted their empowerment level. Almost all the patients we consulted indicated their wish to be involved in the care and decision-making processes. However, the extent to which they wanted to be so differed depending on their self-determination. Most of them viewed decision-making as a shared responsibility. Yet, regarding their involvement, most patients described the wish to be informed, attributing a reactive attitude to themselves.
A few patients, who were mostly affiliated with a patient organisation, saw a more extended responsibility that involved arranging the best care for themselves by, for example, asking for second opinions and contacting health insurance companies. Regarding self-determination, many patients indicated that it is important to speak up for yourself, because as a patient you are subject to the care process and the potential consequences of it. The power relationship between patients and health professionals differed depending on the personality, skills and views of both parties. Assertive patients, who would like to be in control, ensured that a more equal relationship was established by testing health professionals’ knowledge against other resources such as the clinical guidelines or a second opinion (sometimes from abroad).
An information imbalance, patients’ dependence on their health professional, and patients’ emotions that hindered them during conversations, contributed to a negative power balance. As one patient said, And then I did not really know what was going to happen. Since it was a shock that I was admitted for 3 days, I also did not ask for it [what was going to happen]. (Female patient, invasive bladder cancer)
During interviews with the health professionals, respect for patients’ autonomy and the care relationship were discussed. Many of the health professionals, especially the specialist nurses, regarded decisions as being the patient’s choice. However, some health professionals indicated that they felt they were responsible for helping patients to make a well-informed choice by indirectly steering their decision-making. The ethos of the health care system level was less explicitly identified. However, the responsibility of the health care system to optimise the use of health services was revealed by the hospitals’ development of treatment-decision aids, which aimed to help patients make informed choices that fitted their needs.
Empowerment behaviours
Empowerment behaviours relate to the ‘things patient do’. Bravo et al. (2015) make a distinction between (1) shared decision-making, which means taking an active role in consultation and making informed decisions; (2) self-management, which means choosing meaningful and realistic goals and taking steps to achieve them; and (3) patients’ empowerment of themselves.
Shared decision-making
The patients we consulted thought that shared decision-making was important, but half of them felt they did not have a real choice in their care management. In the opinion of some of the patients, not all health professionals wanted patients to play a role in decision-making: I don’t think health professionals like patients to have their own ideas . . . I have the feeling that health professionals are very resistant to assertive patients or patients who know what they want. They find empowered patients difficult to cope with. (Male patient, non-invasive bladder cancer)
Moreover, patients considered good knowledge as essential to becoming involved in decision-making. At the time of writing, much of the information provided to patients related to anticipated treatment steps, and less information was provided about diagnostic and treatment options, which was considered essential for making well-informed decisions.
Although the health professionals also thought that shared decision-making was important, many of them (particularly the urologists) found it challenging to answer ‘even more questions’ in the limited time available. Other challenges related to the support of less educated and health-literate patients and differences in patients’ experiences regarding quality of life. This was also implicitly expressed by the fact that the interviewed patients experienced the impact of the disease progress and care management differently. To enable patients to make an informed decision, information about available treatment options should be included as well as information about (differences in) potential impact on their quality of life.
Self-management
Patients needed information about managing both the physical and the psychological consequences of the disease. Most of them articulated the wish to have more knowledge about the side effects of treatments, such as erectile dysfunction, fatigue, and problems with incontinence and concentration, to enable them to control these side effects or find a way to live with them. Stress and depression were frequently mentioned as the psychological consequences of the disease. Because of the limited support available, patients sought psychological help themselves or developed ways to cope with these consequences: Sometimes you will be referred to psychosocial support, but mostly you have to seek help yourself . . . It would be good if every patient has a contact person who informs about what is going to happen and helps to deal with the emotional consequences. (Male patient, kidney cancer)
Empowering themselves
Although most of the patients we consulted looked for more information, the degree to which they did so depended on how they were coping. A few patients did not look for information because they did not want to feel like a patient, did not want to know everything, or had already given up. The Internet was the main information source but patient organisations and (occasionally) peers were also mentioned. Having more knowledge helped motivate patients to become more involved in their care management and gave them more control over their condition.
Retrospectively, I think that by being active [searching for information] you get a grip on the situation. Otherwise, you just let it happen. There are a lot of things you cannot control, but by doing these things [like searching for information], you have the idea you can do something for yourself. (Male patient, invasive bladder cancer)
Empowering interventions
Following Bravo et al.’s (2015) model, empowering interventions could be implemented by health professionals (individual-focused) or health care systems (group-focused). Concerning the former, the need to facilitate shared decision-making was voiced by both patients and health professionals. Many of the interviewed patients believed that improving their conversational skills, having examples of questions they could ask, and having access to aids to assist with treatment decision-making could help them to articulate their point of view and have an equal conversation with health professionals. In addition to shared decision-making, some patients indicated the need for health coaching on how to cope with the impact of the disease on daily life. The need for group-focused empowering interventions was expressed in relation to health education – to be delivered via information materials – about care management and the possible diagnoses and available treatment options. Various patients explicitly mentioned the provision of health education as an important step towards shared decision-making.
Empowerment capacities, states and resources
Regarding their empowerment capacities, states and resources, patients mentioned the following aspects: (1) knowledge, skills and attitudes; (2) perceived personal control; and (3) feeling respected.
Many patients considered a relationship with a health professional that was based on respect and mutual trust and that allowed all options to be openly discussed to be extremely important. Feeling respected and having a basic level of knowledge about disease and care were regarded as critical conditions for optimal shared decision-making.
I mean, when you have read enough information beforehand, you will have a clearer idea. Then you will be better prepared and able to hold the discussion and for instance ask: ‘Why are we not doing this or considering this option?’ (Male patient, invasive bladder cancer)
Health literacy and self-efficacy were mentioned only in the context of other potential patients. A few patients and health professionals believed that less educated patients were less able to become empowered, since they were less knowledgeable about their disease process and care management and how they could influence their own health-related behaviour.
Moderators relating to health professionals and patients
Only a few moderators relating to patients were explicitly mentioned. These moderators had a lot of overlap with elements of patients’ ethos, such as the assertiveness of patients. A moderator that was implicitly mentioned was the stage of the disease: since patients’ need for information changed with progression. This moderator was in turn related to patients’ coping strategies, which changed over time. Moderators relating to health professionals were also implicitly mentioned. Information provision was influenced by providers’ professional goals. A few urologists, for example, mentioned that it was not their role to explain future care steps or to provide patients with (written) information. They said nurses should carry out these tasks.
Integrating needs into an intervention
Overall, the participants who attended the first co-creation session for each disease domain preferred an online individualised group-focused empowering intervention that provided an overview of reliable information on the different steps in the disease and care management and which included information about and tools to facilitate shared decision-making (e.g. treatment-decision aids, tools for patient–doctor conversations). This preference – which was in line with the needs expressed in phase 1 – underlines the importance of layered information so that information resources are personalised instead of being developed for the ‘general’ patient in line with existing information sources.
During the co-creation sessions, patients and health professionals gave different but complementary types of input on the future health education intervention that could be developed. While patients valued the intelligibility and connotations of the wording, health professionals paid more attention to the correctness of the texts. A consensus was reached regarding wording that was both comprehensible and correct. Example might include the use of wording ‘return of the disease’ instead of ‘relapse’, and ‘cell research’ rather than ‘cytology’. Patients also stressed the importance of complete, transparent, personal and ultimately empowering information. Personalisation was also important with patients stressing the need for information about distinctive symptoms for men and women and illustrated materials for each sex. The need for comprehensive information was highlighted by, for example, the request to add information about experimental treatment options and treatments offered abroad. Health professionals, on the contrary, emphasised the relevance of the information to the Dutch context, organisational differences or uniformity within the patient group. The relevance of certain diagnostic and treatment options was discussed, for instance. In addition, health professionals mentioned feasibility and implementation issues, such as the need to embed new health educational provision within current arrangements for information provision.
When deciding on the content of the information materials, there was a need to balance these perspectives. An example of such balance was the decision to mention the existence of experimental and alternative therapies in the materials, but without addressing specific therapies, and by adding the recommendation to discuss these therapies with the treating physician. This decision balanced patients’ need to be informed about these possibilities with health professionals’ concern about information that could become outdated or was not evidence based. Another example was mentioning the urgency of certain care steps, including patients’ wish to have a time indication for the expected care process and health professionals’ perspective that it was sometimes hard to give a precise time indication due to existing uncertainties in care management.
Developing and implementing the intervention
Based on the identified needs, a template for a health education intervention for urological cancer patients in the form of digital patient information was developed in the form of a simplified care pathway. This contributed to the integration and uniformity of available knowledge, in line with the (inter)national standards. There were small differences in the steps depending on the type of urological cancer that is being considered, but the pathways generally consisted of the following steps: (1) symptoms, (2) consultation, (3) diagnosis, (4) discussion of diagnostic results, (5) treatment, (6) follow-up and (7) possible recurrence.
For each step in the care pathway, customised information was provided using multilayered webpages via which patients could determine for themselves (by clicking or using hyperlinks) the information they would like to receive and how detailed they wanted it to be. The information provided was stratified for patient type and disease stage. The aim was also to layer the information so as to make it suitable for different educational backgrounds. This was done by first mentioning only basic information, with links provided to more detailed information. In the future, audio-visuals will be added to further meet the needs of less literate patients.
Personalisation was also stressed to help patients integrate and interpret the information. The patient information also included tools to facilitate shared decision-making (e.g. treatment-decision aids, tools for patient–doctor conversations) and self-management (e.g. tips on using stoma equipment and coping with the impact the disease had on daily life).
Discussion
Study findings reveal how the combination of programme theory and a participatory process strengthened the development of an empowerment theory-based health education intervention for urological cancer patients. As a result, one of the current barriers to developing successful health education interventions – namely, the neglect of empowerment as part of it – was addressed. Importantly, the experiential knowledge of and the need for empowerment of the members of the target group formed the basis of the research process. By actively involving patients in the development of the health education programme, the intervention better reflected their empowerment.
In line with other studies, participants regarded shared decision-making and self-management as highly desirable outcomes of empowerment (e.g. Anderson and Funnell, 2010; Aujoulat et al., 2007). At the time of writing, however, health education interventions too often only advise on expected diagnostic and treatment steps, which does not sufficiently support patients to make informed choices. An empowering health education intervention consisting of digital patient information which (1) was personalised at different levels; (2) provided a uniform overview of relevant information on different care steps based on clinical guidelines; and which (3) contained information and tools facilitating shared decision-making and self-management was well received. Details of the intervention are now available on www.allesoverurologie.nl (the website of the Dutch Association of Urology) and www.thuisarts.nl (a Dutch website containing reliable health information); and will be integrated into patient records in the two hospitals participating in the study.
Multiple studies stress how patients’ empowerment may imply a personal change in patients’ health-related behaviour (Aujoulat et al., 2007; Bravo et al., 2015; Chamberlin and Schene, 1997; Feste and Anderson, 1995). The digital patient information we developed aimed to bring about such a change by increasing patients’ knowledge and skills, which was considered an important step for taking part in shared decision-making and self-management. Personal change in health-related behaviour should not, however, be seen in isolation from other influencing factors, such as patients’ ethos, personal values and social context. As Schulz and Nakamoto (2005, 2013) emphasise, empowerment must be accompanied by a volitional component, which is referred to as the ‘meaning’ dimension in the empowerment model of Thomas and Velthouse (1990). In addition to patients’ motivation influencing their ability to change, so does their health literacy. By using layered digital information, the health education intervention aims to target a diverse group of patients with different values and levels of health literacy. The intervention assumes, however, that patients want additional information and have ICT resources and skills. Due to these prerequisites, the intervention excludes patients who do not have these resources and skills and/or do not seek additional health-related information. We know from earlier research that these kinds of patients tend to have a lower level of income, education or literacy, which might exacerbate their vulnerability (Helsper and Reisdorf, 2017; Helsper and Van Deursen, 2017). Because of this, the implementation of eHealth information and services may further widen health-related disparities (Bodie and Dutta, 2008; Neter and Brainin, 2012). To counteract the exclusion of members of this vulnerable group as much as possible, information is provided for each step of the clinical care pathway and the intervention will be integrated into electronic patient records. Health professionals will therefore be better able to assist vulnerable patients to obtain access to and use the patient information. This support will help in generating an interactive process of communication and education in which knowledge and power are shared. This interactive process is similar to what Aujoulat et al. (2007) define as the inter-personal dimension of empowerment. To further stimulate this process, the intervention also provides tools to support patient–health professional interaction.
Strengths and limitations
A key strength of this study derives from the fact that the intervention design utilised was based on programme theory. The theory-based design enables future evaluation of the patient information developed. This design process may also provide a valuable template for developing empowerment interventions for other disease types. The intervention itself could not, however, be used as such a template since it had been personalised for the specific needs of urological cancer patients. A further limitation in terms of generalisability is that the intervention presumed that patients were aware of the possibility and had the wish to be involved in health decision-making and care. Other types of information provision, which may be more valuable for patients who do not expect to be so involved, were excluded from the study design.
Conclusion
This study revealed how the combination of the use of a programme theory in which patient empowerment is conceptualised and a participatory process in which the needs of patients and professionals were articulated, enabled the development of an empowerment theory–based health education intervention for urological cancer patients in The Netherlands. Follow-up work is needed, however, to determine the extent to which (and in what ways) the intervention led to increased empowerment of the patient group. The programme theory developed through this study may prove useful as a template for developing future health education interventions.
Supplemental Material
sj-pdf-1-hej-10.1177_00178969211035169 – Supplemental material for Co-creating an empowering health education intervention for urological cancer patients
Supplemental material, sj-pdf-1-hej-10.1177_00178969211035169 for Co-creating an empowering health education intervention for urological cancer patients by Violet Petit-Steeghs, Carina ACM Pittens, Jurriaan Oosterman and Jacqueline EW Broerse in Health Education Journal
Footnotes
Acknowledgements
We are grateful to the patients and health professionals who shared their experiences with us during the study. We also thank Eveline Smit, Liesje Yu and Matthias Seenok for helping with data collection, and the project group for their valuable contributions.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article. The project was supported by The Netherlands Organisation for Health Research and Development (ZonMW) (project number 516022514). ZonMW was not involved in the study design, collection, analysis and interpretation of data; the writing of the article; nor the decision to submit the paper for the publication.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.