
Abstract
Objective:
The stigmatisation of incarceration has significant negative effects on the health and well-being of individuals and communities. At the University of British Columbia in Canada, an undergraduate course on prison health included instruction by people with lived experience of incarceration as part of a teaching approach aimed to reduce stigma. In this study, we sought to understand the impact of this course as described by students.
Design:
Qualitative interviews with students who completed the course in 2017 were conducted by another former student of the course. Interviews were transcribed and interpretive descriptive methods were used to elucidate findings.
Results:
Nine former students participated in the study, eight (89%) were women and the median age was 23 years. Analysis yielded the following themes: (1) learning from people with lived experience, (2) de-mystifying through knowledge and understanding, (3) broadened perspectives and self-reflection, (4) future choices and actions and (5) changing views on incarceration.
Conclusion:
Findings suggest that approaches to address stigma in teaching prison health in an undergraduate course provided students with a deepened understanding of health inequities and determinants of health; increased feelings of compassion and interest in health equity for populations impacted by incarceration; and fostered opportunities for reflection, critical thinking and broadened perspectives.
Background
On any given day in Canada, approximately 39,000 adults are in custody and 104,000 adults are supervised in the community through programmes such as probation, community supervision and parole (Statistics Canada, 2018). People engaged by the criminal justice system have a higher burden of mental and physical health needs and experience increased rates of injury and mortality compared to the general population (Kouyoumdjian et al., 2016). However, people with a history of incarceration experience barriers to healthcare services and negative health outcomes due to the stigma associated with criminal justice involvement (Abbott et al., 2017; Fahmy et al., 2018; Joudrey et al., 2019; Schnittker and John, 2007).
Gray (2002) describes stigma as both felt and enacted: Felt stigma (internal stigma or self-stigmatisation) refers to the shame and expectation of discrimination that prevents people from talking about their experiences and stops them seeking help. Enacted stigma (external stigma, discrimination) refers to the experience of unfair treatment of others.
Both felt and enacted stigma related to incarceration play a role in access to healthcare services for people who have experienced incarceration. Fahmy et al. (2018) found that even in the context of Canada’s universal healthcare system, discrimination based on history of incarceration was a barrier to accessing primary healthcare. Previous negative interactions with healthcare and the anticipation of stigma and discrimination may also prevent people from accessing needed services (Moore et al., 2016).
Addressing stigma in healthcare settings and in the general population is an important component of health and healthcare equity. Reducing stigma is often approached through education, contact or a combination of both (Corrigan et al., 2012; Griffiths et al., 2014; National Acadamies of Science, 2016; Nyblade et al., 2019). Contact refers to an interaction between members of different groups. Intergroup contact theory posits that direct contact between groups can reduce prejudice and conflict and promote inclusion (Hewstone and Swart, 2011; Pettigrew, 1998; Pettigrew et al., 2011; Pettigrew and Tropp, 2006; Turner et al., 2007). The theory points to four conditions that make contact most effective in reducing prejudice: (1) having equal status, (2) engaging in cooperation, (3) sharing common goals and (4) receiving support from social and institutional authorities (Pettigrew, 1998; Pettigrew and Tropp, 2006).
Contact is often a key component of anti-stigma approaches to teaching and learning. Anti-stigma approaches are interventions which ‘present factual information about the stigmatised condition with the goal of correcting misinformation or contradicting negative attitudes and beliefs’ (National Acadamies of Science, 2016). Previous research on the experiences of undergraduate students demonstrated that anti-stigma approaches to teaching that included interaction with people who experience stigma increased compassion, self-awareness and stereotype rejection. (Alipanopoulos et al., 2020; Boag and Wilson, 2014; Calaway et al., 2016; Patten et al., 2012; Sword et al., 2004; Zrinyi and Balogh, 2004). In this study, we set out to apply an anti-stigma approach guided by intergroup contact theory to an undergraduate course in prison health with the aim of reducing prejudice and harmful attitudes of oppression among learners. This study explores the experiences and learning reported by undergraduate students in this course.
Context
The Collaborating Centre for Prison Health and Education (CCPHE) was established in 2006 at the University of British Columbia (UBC) in Vancouver, Canada ‘to foster collaboration and partnerships between universities, prisons and the justice system, and communities, to reduce disparities that negatively affect those who are in custody or in the process of (re)integrating into society’ (The Collaborating Centre for Prison Health & Education, n.d.). As part of the CCPHE’s mission, a fourth-year undergraduate course on ‘Prison Health’ was developed and offered in the UBC School of Population and Public Health. The aim of the course was to introduce undergraduate students, many of whom will go on to careers in health and medicine, to the health and healthcare inequities experienced by people who are engaged by the criminal justice system. The course ran for the first time from January to April 2017, and to-date has repeated during the same months in 2018, 2019 and 2020. Students attend lectures provided by interdisciplinary faculty, members of community organisations, correctional institutions and people who have experienced incarceration. Course readings are assigned based on the specific topic of focus for each week’s class (e.g. women’s health in prison, healthcare services delivery in correctional settings, mental health and substance use). Assigned readings include articles from academic literature, reports and documents from government or stakeholder organisations such as the World Health Organization and the Elizabeth Fry Society and from Arresting Hope (Fels et al., 2014), a book which includes first-hand accounts of women incarcerated in BC and from prison staff. Students are also provided with a list of optional readings related to the weekly topic for interest and self-directed learning. Students explore course topics through in-class and online discussion, group projects, case studies and reflective writing.
The course has aimed to foster the four conditions for reducing prejudice outlined in intercontact theory (Pettigrew, 1998; Pettigrew and Tropp, 2006). Guest speakers who have experienced incarceration share their expertise with student learners as course instructors. Though the hierarchy of student–instructor is not strictly equal status, this change in roles reflects a potential shift in power dynamics. Cooperation and collaboration have been a central tenant of the course in which academics, service providers and people with lived experience often presented in the same day and provided input into student discussion groups and activities. Instructors, guest speakers and students shared the common goal of student learning and reflection. Finally, support from social and institutional authorities has been made explicit, as the course is a well-recognised and popular course in the School of Population and Public Health, with wait-listed students each year. In addition, the participation of guest speakers from community organisations, staff from correctional institutions and researchers gave support to engagement and collaboration.
Boag and Wilson (2014) and Calaway et al. (2016) found that undergraduates participating in prison tours showed increased positive attitudes and empathy with people engaged by the criminal justice system. Medical students who engaged with people who have experienced incarceration as part of their training demonstrated increased rejection of negative stereotypes and interest in future work with populations affected by the criminal justice system (Brooker et al., 2018). In addition, among students in programmes where incarcerated and non-incarcerated learn as peers such as Inside-Out Prison Exchange Program in USA and Walls to Bridges in Canada, participation helped to dispel fears and stereotypes, reduced negative or punitive mindsets and created an increased empathy, sense of connection and drive for social change (Hilinski-Rosick and Blackmer, 2014; Martinovic et al., 2018; Pollack, 2016). Our study aims to add to the literature by examining the impact of anti-stigma approaches around incarceration to learning in a university classroom, rather than correctional setting. In addition, we examined the impact of people sharing their lived experiences of incarceration in an educator role. We were able to identify three other undergraduate-level prison health courses: one at McMaster University, one at John Hopkins Bloomberg School of Public Health and a third at Brown University. However, there have been no peer-reviewed, published findings on the impact of these courses. This study aimed to explore the impact of prison health education, which included instruction by people with lived experience of incarceration, as described by undergraduate students who participated in the course.
Methods
Study design, sample and recruitment
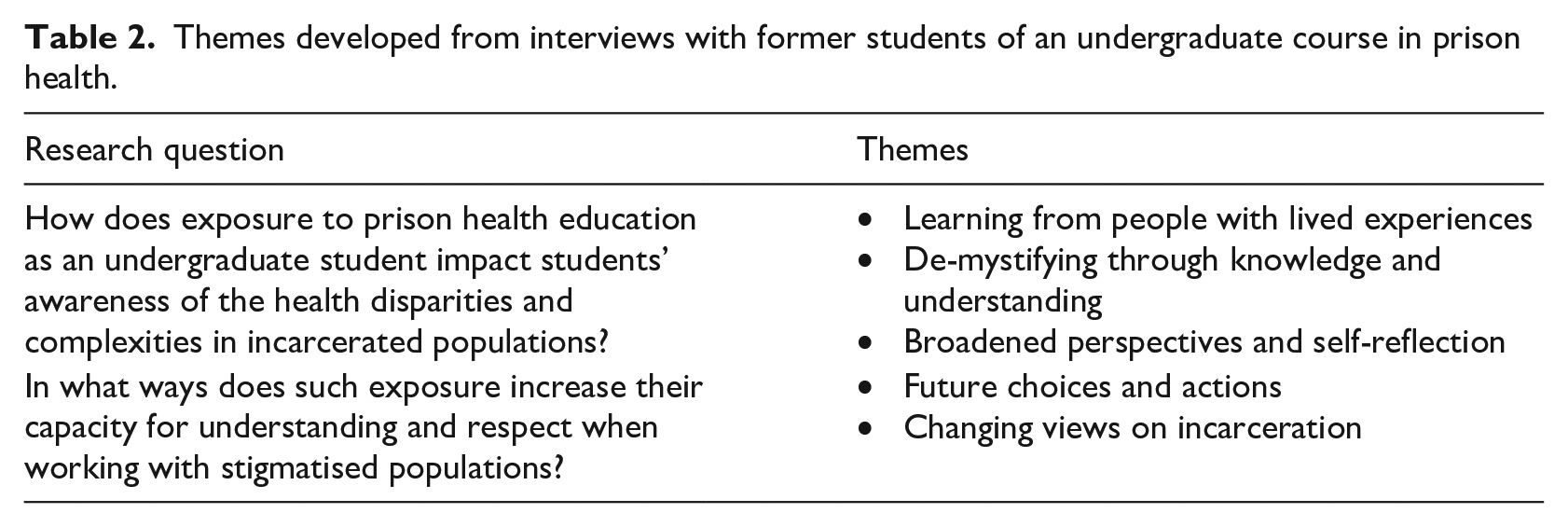
This qualitative study was designed to answer the following research questions: (1) how does exposure to prison health education as an undergraduate student impact students’ awareness of the health disparities and complexities in incarcerated populations, and (2) in what ways does such exposure increase students’ capacity for understanding and respect when working with stigmatised populations?
The research team consisted of a research assistant who had completed the course as a student (R.B.C.) the course instructor (R.E.M.) two academic faculty members who had participated in the course as guest-lecturers (L.D., J.A.B.), a third academic faculty member (Carl Leggo) and a graduate student (K.E.M.) who was the teaching assistant in subsequent years of the course. An email was sent in July 2017 from the course instructor to all students who completed the prison health course between January and April 2017 inviting them to participate in the study.
Students interested in participating contacted the research assistant to set up a date and time for either an in-person or a phone-based interview. Two subsequent emails were sent specifically to recruit male participants, as there had been no responses to the first email from male students. All students who expressed their interest in participating by contacting the research assistant were interviewed for this study. The University of British Columbia Behavioural Research Ethics Board granted a certificate of approval for the study (#H17-01170).
Data collection
Individual interviews were conducted by telephone or in-person depending on the participant’s preference. Written consent was obtained prior to the interview, which was audio recorded. A semi-structured script with open-ended questions was developed by the research assistant with input from others on the research team. Research questions explored four main areas: (1) experience prior to the course (e.g. what previous experiences have you had that are related to prison health or prisons in general), (2) description of experience in the course (e.g. what surprised you the most about the course), (3) specifics about the course (e.g. which elements of the course helped you engage with the course material) and (4) impact of the course (e.g. from your experiences in [the course], how has your view of incarceration and the prison system changed, and in what way(s) has [the course] made you feel more equipped to work with a marginalised population)? Participants additionally completed a demographic survey following their interview. Interviews were conducted by the research assistant, who was a student in the course in 2017, and were about an hour in length. Audio recordings were transcribed verbatim with all personal identifiers removed.
Data analysis
All transcriptions were analysed using Interpretive Descriptive (ID) methodology (Thorne, 2016). ID is designed to answer complex questions situated within real-world contexts and generates practical knowledge rather than building new or extending existing theories. This approach was chosen to focus findings on meaningful application to practice, in this case anti-stigma approaches to teaching about prison health. Following the coding of all interview transcripts by the research assistant, the course instructor and the other faculty co-authors reviewed and coded transcripts to ensure that common themes and contrasting observations were identified and compared. Specific attention was paid to student awareness of and perspectives on health disparities, health equity, stigma and respect. In iterative discussion, the research team drew initial themes developed from coding into higher-level conceptualisations until consensus on final themes was reached. NVivo software was used to organise the data analysis by developing a structure of units to categorise reoccurring ideas and develop a thematic structure.
Findings
Main findings
There were 9 participants in this study (Table 1), of whom 8 (89%) were women; this was higher than in the overall class in which 8 of the 35 students were men (23%). The age range of study participants was 20–28 years.
Characteristics of study participants.
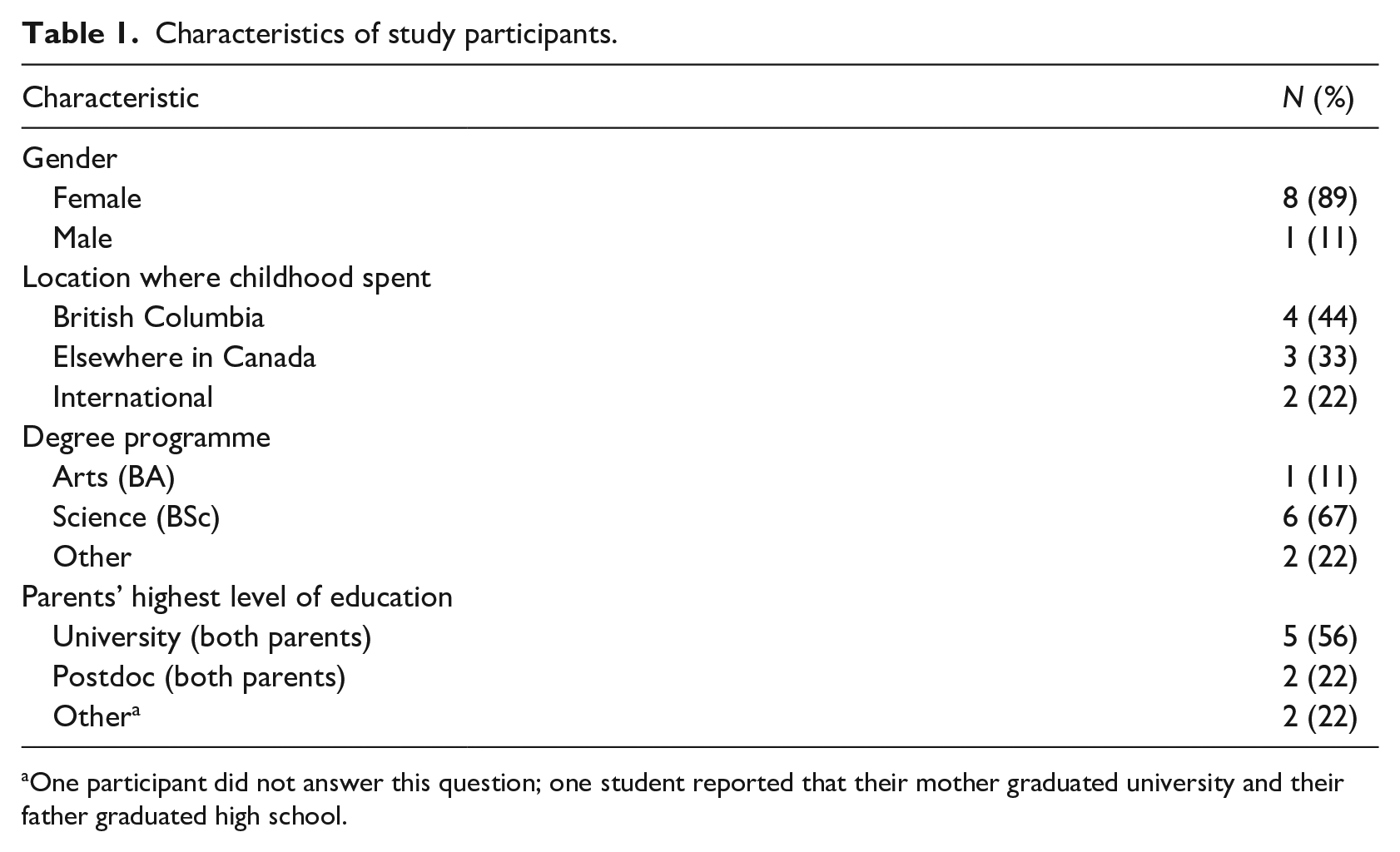
One participant did not answer this question; one student reported that their mother graduated university and their father graduated high school.
In response to our research questions, five major themes were developed (Table 2). Students described the course as an opportunity for: (1) learning from people with lived experience, (2) de-mystifying through knowledge and understanding, (3) broadened perspectives and self-reflection, (4) future choices and actions and (5) changing views on incarceration. In the following description of themes, we have included examples of participants’ responses with their self-identified gender and age (e.g. F 22).
Themes developed from interviews with former students of an undergraduate course in prison health.
Learning from people with lived experience
Participants unanimously expressed an appreciation for guest instructors with lived experience of incarceration: When people would come in who’d actually [experienced incarceration] and could speak to . . . what you were reading in the textbook . . . to actually put a face to that, was really. . . significant to me. – F 24
In addition, study participants remarked that the guest speakers shared parts of their lives that in a different context might not be easily talked about. Students talked about the accepting environment of the classroom as not just supporting this sharing but also in allowing students to reflect and explore their own attitudes in the context of this contact. One student described the classroom as a ‘safe space’ for learning and growth. Participants indicated that they felt the course offered a unique opportunity to learn about a topic that they had limited exposure to. Nearly all students expressed that their gained knowledge had relevance to everyday life.
De-mystifying through knowledge and understanding
Most participants indicated that prior to the prison health course, their understanding of incarceration and people who experience incarceration came from the news, social media and other portrayals. Study participants had very limited knowledge of the incarceration system in Canada prior to taking the course. Learning about the complexities of incarceration ‘opened up another world’ (F 23) for students and caused participants to reflect on some of the issues that surprised them.
I didn’t know that it’s a totally different [health] system, and I was like why are they different? Young people and old people, we’re still under the public system, right, but why is it for [people in prison] . . . they’re separated? – F 20
In addition, the stories shared by guest speakers were important in addressing stereotypes students may have entered the class with. One student talked the interviewer through this process: Some part of me instinctually felt fear, but after he told us his story, that part subsided real quick, and you know became logical again. – M 28
Guest instructors with lived experience of incarceration gave students opportunity to reflect not only on the challenges in the guest presenters’ stories but also the hope and opportunity.
Broadened perspectives and self-reflection
Students reflected on how the course helped them to expand or change their perspectives and develop a deeper understanding and appreciation of the topics addressed. For example, the literature read by students during the course, such as Arresting Hope (Fels et al., 2014) and Prison and Health (Enggist et al., 2014), offered alternative perspectives on incarceration, which did not conform with hegemonic discourses on the treatment of people engaged by the criminal justice system. Furthermore, the guest instructors who shared their personal narratives with students, gave students the opportunity to learn ‘what is on the other side’ (M 28) of stereotypes they had heard or held. As demonstrated by one student’s reflection, participants’ broadened perspectives increased their capacity for using multiple lenses to examine complex issues: I think the most important part about this course, is teaching people the meta-cognitive skill of being more open to other viewpoints . . . ’cause that skill-set, other than just [in a] prison setting, it could be used everywhere else in your daily life. M 28
As demonstrated by the following quote, participants exhibited self-reflection in their responses to the stories shared with them as part of the course: I just think that having this knowledge . . . makes you think like oh they’re real people and they have issues just like us and it makes you . . . reflect on the fact that you’ve had a lot of advantages in your life – F 22
Words such as ‘grateful’, ‘fortunate’ and ‘thankful’ were used by students often as they reflected on their own lives as a result of the course. Although participants described some class sessions as emotionally ‘heavy’, they expressed that the overall learning experience enabled them to develop a stronger sense of their own position of privilege in society.
Future choices and actions
Participants expressed that having academic and professional guests who were experienced working with incarcerated populations in Canada illustrated the possibilities for making change. Furthermore, it gave participants hope that they might be able to contribute to ameliorating the health challenges faced by people who experience incarceration within the correctional setting and beyond. In addition, for some participants, the course directly influenced the possibilities they saw in their future careers: I’m hoping that at some point in my career I can definitely work in the prison system somehow . . . I felt like I never would have thought about that beforehand. – F 24
Much of the impact of engaging with people with lived experience of incarceration was a change in what students expected of themselves in their daily lives.
When you’re downtown people always approach you and ask for money, or sometimes they just wanna chat, and you know now that I’ve taken the course . . . I try to talk to them a little bit more, or at least acknowledge them. – F 22
Changing views about incarceration
For many participants, the possibility of using a rehabilitative approach to incarceration, as opposed to primarily punitive methods, was a novelty. The course’s use of unconventional examples of incarceration structures, such as some of the programmes discussed in Arresting Hope (Fels et al., 2014) exposed students to alternative methods of incarceration aimed to support rather than further punish. Participants expressed how rehabilitative methods would give incarcerated individuals access to needed resources and tools and help to improve outcomes in the community after their release.
Furthermore, participants expressed a sense that solitary confinement was being used as a tool to punish incarcerated individuals beyond their sentence and that a system of incarceration without rehabilitation fosters recidivism. Throughout student interviews, the idea of rehabilitation surfaced time and time again in response to breaking the cycle of reincarceration.
What’s the point of having someone inside and 5 years later releas[ing] them back out to the world where they have nothing, and then you know what will they do? – M 28
Found poem
As a type of summary of study findings, we include a found poem, ‘Thrown Into the Deep End’ (Figure 1), which was written by the late Carl Leggo, an academic poet and co-investigator, as he lingered over one transcript. The found poem, which uses one student’s words, provides a poignant illumination of all the study themes, their interactions with one another and the sometimes-difficult process of reflection, growth and shedding of previously held beliefs.
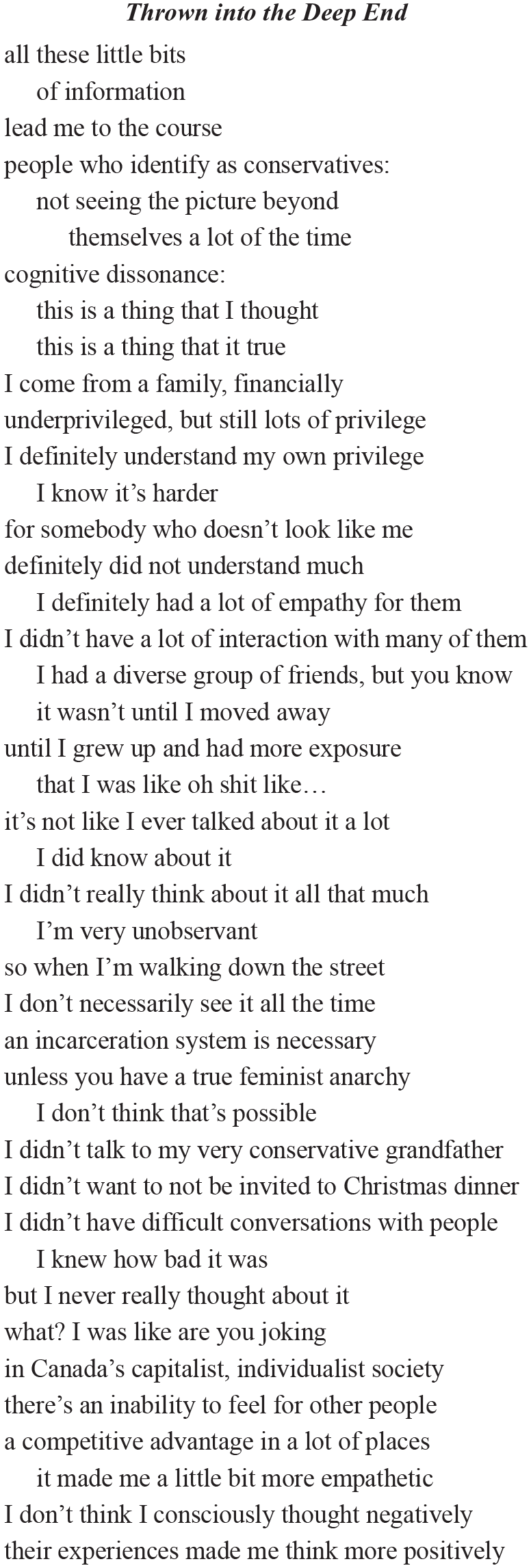
Thrown into the deep end.
Discussion
Implications
The UBC Prison Health course is one of only a small number of undergraduate prison health courses delivered in North America. Experiences and perspectives described by students in this study highlight that anti-stigma approaches and inter-group contact can have a positive impact on undergraduate learning about prison health in a classroom setting.
In particular, the course gave students an opportunity to better understand the criminal justice system and the health inequities and social determinants of health associated with incarceration. Guest presenters who shared their personal narratives with students played a central role in facilitating a shift of perspective among students in the course. Learning from people with lived experience of incarceration helped to create power dynamics, which reflected equal status and cooperation, both important conditions to increase empathy and stereotype rejection (Pettigrew, 1998; Pettigrew and Tropp, 2006). Furthermore, individuals with lived experience holding positions of expertise and authority in the class is a form of explicit support by institutional authorities, a third condition for reducing prejudice. This change is consistent with the finding by Shannon et al. (2009) that encountering an educator who had a disability promoted attitudinal shift among undergraduate students.
Students reported that learning from people with lived experience of incarceration was a powerful learning opportunity facilitated by creating a ‘safe space’, which allowed them to meaningfully reflect on their own attitudes and beliefs in the context of what they learned. Developing a compassionate, collaborative environment was an intention of the course to address the concerns expressed by other researchers that students will avoid meaningful discussion through perception of a socially desirable ‘right’ answer to complex issues involving stigmatised populations (Batson et al., 1997; Monroe and Martinez-Martí, 2008; Weaver and Yun, 2011).
Students specifically highlighted how learning from people with lived experience of incarceration worked to counter the portrayals they had seen in media. Elsewhere, it has been found that entertainment media as a source of knowledge produces more negative attitudes of stigmatised groups (Sword et al., 2004), and the media has been known to provide the general public with a predominantly negative view of incarcerated populations (Motley and Sturgill, 2013). Stigma and discrimination serves as a barrier to adequate healthcare services (Fahmy et al., 2018; Frank et al., 2014; Moore and Tangney, 2017; Redmond et al., 2019). Discrimination in community can have a direct and devastating effect on the health and well-being of people who experience incarceration. Discrimination based on criminal record has been demonstrated in employment and housing (Canadian Civil Liberties Association, 2014; Evans et al., 2019; Pager et al., 2009; Pager and Shepherd, 2008) and is associated with depression and anxiety and social isolation (Assari et al., 2018). Increased opportunities for meaningful intergroup contact in the context of health education may help to address stigma among learners some of whom are future healthcare providers and all are members of society.
Participants highlighted how guest presentations and course readings offered alternative perspectives to the predominant discourse on criminal justice they had been exposed to. Reflecting on these counter-narratives through writing assignments and group discussions required participants to use perspective-taking, a key mechanism of intergroup contact’s ability to influence attitudes (Batson and Ahmad, 2009). Perspective-taking has previously been demonstrated as an influencing factor in the attitudinal change of undergraduate students (Patterson and Hulton, 2012) and allowed participants to image themselves in the situations described by guest speakers. Furthermore, the perspective-taking and resulting emotional response experienced by participants is in line with the parameters of empathy (Batson and Ahmad, 2009; Boag and Carnelley, 2016) and echoes the mechanisms for attitudinal change observed in Boag and Wilson’s (2014) exploration of undergraduate students’ experience of a prison tour. The prison health course also engaged students in reflective learning, which required them to examine experiences and compare them against presuppositions, values and beliefs, then assess gaps and the need for future learning (Kuiper and Pesut, 2004; Ryan, 2015) Participants highlighted the value of reflection in facilitating their learning in the course, as well as a practice they could incorporate moving forward as a component of lifelong learning.
As seen in previous research on the effects of an anti-stigma approach to education which include contact with people who experience stigma (Brooker et al., 2018; Patten et al., 2012), participants expressed a desire to explore future opportunities to work with and advocate for incarcerated individuals and other stigmatised groups. One participant has already begun volunteering at a youth detention centre. Further evidence of a transformation in study participants’ practices was confirmed by students’ desire to see more rehabilitative methods of implementing justice, similar to the findings by Calaway et al. (2016). Students’ rejection of a solely punitive approach to incarceration illustrates the course’s ability to not only address stigma and negative stereotypes, but also to develop respectful, person-centred perspectives. Overall, participants in the prison health course expressed increased empathy and understanding, and interest in addressing health inequities for people and populations impacted by the criminal justice system.
Limitations
One of the main limitations of the study was the use of convenience sampling. Strong engagement with course material was likely a bias for self-selecting to participate in an interview and may have generated a sample of students who were positively impacted by the course experience. In addition, since prison health was an elective course, students enrolled were perhaps more likely to be open to the ideas put forward and to engage in critical reflection. Given the qualitative inquiry and the small sample size, our findings are not generalisable to all undergraduate students, but the themes identified may be of relevance to similar students.
Only one male student participated in an interview, and although the majority of the course participants were women, the study sample did not fully represent the gender balance of the course. However, the themes determined from the male participant’s interview resonated with those from interviews with female participants.
Both parents of almost all study participants had attended university, suggesting that participants had experienced a relatively privileged upbringing. This factor may have positively contributed to attitudinal change, as previous research has shown that students with greater personal experience of stigmatised people are less impacted by intergroup contact (Calaway et al., 2016; Zrinyi and Balogh, 2004).
There was no formal member checking of findings of this study, however, this limitation was to some extent addressed by engagement of a previous student of the course in the analysis. Participants’ answers may have been influenced by perceived social desirability particularly due to awareness of the course instructor’s involvement in this study. (Batson et al., 1997; Monroe and Martinez-Martí, 2008; Weaver and Yun, 2011). We attempted to minimise this through peer interviews conducted by another student in the course. Finally, analysis may have been influenced by the connection to the course felt by the course instructor and research assistant (a former student). This was mitigated by engaging other team members in the iterative and collaborative development of themes.
Future research
Future research that measures student attitudes before and after experiencing intergroup contact with people who have experienced incarceration would add knowledge to our understanding of the impact that prison health education may have at the undergraduate level. New research could shed light on the experiences of people engaged by the criminal justice system through the intergroup contact process. This knowledge is important to ensure feelings of judgement or re-traumatisation are mitigated during the cross-group encounter, especially in consideration of the vulnerability some people may feel when sharing their personal narratives.
Conclusion
This study demonstrates the value of anti-stigma approaches to health education, which include intergroup contact in addressing stereotypes and myths around incarceration and promoting empathy among undergraduate students from a variety of degree programmes. Students who participated in interviews for this research project reported that as a result of the course they shared a desire to apply what they had learned about and from people who had experienced incarceration in advocacy or their future careers demonstrating the potential for long-term and far-reaching effects. Expanded access to similar courses has the potential to generate a stronger public response to health inequities. This may be particularly valuable for undergraduate students likely to go on to professional degrees in health and social sectors such as medicine, nursing and social work.
Footnotes
Acknowledgements
The authors acknowledge that they live and work on the traditional, ancestral and unceded territory of the Coast Salish peoples; Skwxwú7mesh (Squamish), Stó:lō and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) and xʷməθkʷəy̓əm (Musqueam) Nations. They also acknowledge guest presenters who shared their experiences and stories to give invaluable learning opportunities to students of the Prison Health course. Finally, they acknowledge Dr. Carl Leggo (1953–2019), coauthor, colleague and friend.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.