
Abstract
Objective:
e-Bug is a teaching resource that addresses the UK 5-year National Action Plan on antimicrobial resistance (AMR) that pledges to work with educators and local authorities to ensure young people understand infection prevention and control (IPC) and AMR. This study aimed to evaluate the effectiveness and acceptability of the e-Bug face-to-face train-the-trainer intervention with school and community educators.
Design:
Service evaluation of an educational intervention via surveys.
Setting:
Workshops were organised by Public Health England (PHE) and collaborators in seven regions of the UK during 2018–2019.
Method:
Pre- and post-intervention surveys measured satisfaction with training, knowledge of IPC and AMR, and confidence to teach others. Statistical analyses included multilevel and ordinal logistic regression models to measure change in educator knowledge and confidence.
Results:
In all, 262 educators participated: primary (46%), secondary (17%), college (2%), healthcare (29%) and community (7%). Educators had high pre-intervention knowledge of topics, with significant improvement (p < .05) in confidence to teach all topics and some significant IPC knowledge improvement, post-intervention. There was strong evidence for a difference in confidence change between educator types, with primary educators improving the most. Ninety-five percent of educators rated the train-the-trainer workshop positively, valued the interactive workshops and felt confident to use the resources.
Conclusion:
Confident and knowledgeable educators, achieved via e-Bug train-the-trainer workshops, will enhance education of IPC and AMR topics in schools and communities, and therefore support the UK 5-year AMR action plan. The intervention will be monitored with long-term follow-up surveys to explore how training has been disseminated and to evaluate long-term benefits.
Introduction
Antimicrobial resistance (AMR) is a significant threat to the health of the public (World Health Organization, 2015) and a key priority for Public Health England (PHE, 2019b). UK public surveys suggest a sustained misunderstanding of AMR (McNulty et al., 2007, 2019), and schools are a vital setting to correct this. The UK 5-year National Action Plan on AMR aims to enable ‘all school children to understand how to wash hands, prevent infections and use antimicrobials appropriately’ by working with school educators and local authorities (HM Government, 2019b).
Infection prevention and control (IPC) interventions have the potential to reduce childhood infection and, consequently, reduce school absenteeism (Willmott et al., 2016) and antibiotic prescribing (Lemiengre et al., 2018; Vodicka et al., 2013). Antibiotics education is currently limited in the UK National Curriculum, particularly for primary schools (Hayes et al., 2020), and occurs at higher secondary education which is not mandatory for all students (HM Government, 2013). Statutory guidance from September 2020 for England will include Relationships and Sex Education (RSE) and Health Education, which will include topics on hygiene, infection prevention and antibiotics for primary and secondary education (HM Government, 2019a).
There is limited research on educators’ teaching of IPC and AMR. Primary teachers in New Zealand and India have reported a lack of knowledge around antibiotics and antibiotic resistance (Kotwani et al., 2016; Norris et al., 2009). In a recent study, English primary educators had good knowledge of oral hygiene and tooth brushing but lacked awareness of the effects of sugar on oral health (Eley et al., 2020). English and Canadian secondary educators felt they lacked the capability to teach about sexually transmitted infections (STIs) (Cohen et al., 2004; Westwood and Mullan, 2007). Therefore, educator training may be needed to improve knowledge, confidence and skills to teach about IPC and AMR.
Three-quarters of antibiotic prescribing occurs in community settings in England (Public Health England, 2019a), and Antimicrobial Stewardship (AMS) can include the education of patients and the community (Carson and Patrick, 2015; Eley et al., 2018; Rogers Van Katwyk et al., 2018). Educational activities have been undertaken with specific community and vulnerable groups, including uniformed youth groups (PHE, 2019a), young parents and adults with learning disabilities (Eley et al., 2018).
e-Bug is an educational resource used internationally, developed and promoted by PHE to educate young people in schools and communities about microbes, transmission of infection and correct use of antibiotics (e-Bug, 2020). e-Bug materials are endorsed by the National Institute for Health and Care Excellence (NICE, 2017), and their use in schools and the community significantly improves young people’s knowledge of hygiene and antibiotic topics (Eley et al., 2019b; Lecky et al., 2010). Following research with school nurses (Hoekstra et al., 2016), an e-Learning training package was developed and hosted on the e-Bug website in 2016. Evaluation of the e-Learning found that a high proportion of educators self-reported their knowledge of IPC and AMR topics to be low before the e-Learning, and 80% perceived their knowledge to improve after completing the e-Learning (Eley et al., 2019a). Educators suggested adapting the training to follow a ‘cascade model’ whereby educators disseminate training to colleagues (Eley et al., 2019a). PHE developed and piloted a face-to-face train-the-trainer intervention in 2017, based on these recommendations, to further increase uptake of e-Bug and education on IPC and AMR in schools and the community.
The aims of this service evaluation were to measure educator knowledge of and confidence to teach others about IPC and AMR before and after receiving the e-Bug train-the-trainer intervention and to assess the acceptability of the workshops through trainee feedback.
Methods
The intervention
A half-day training workshop was developed and piloted with educators in Gloucestershire, England, in 2017. The final workshop consisted of three stages (Figure 1), including introductory information about IPC and AMR, interactive demonstrations, and discussion and action planning. Following the workshop, participants received an ‘Approved e-Bug Educator’ certificate and complementary resource booklets. Participants were encouraged to train other educators in line with a cascade model, whereby training is disseminated to other educators in a workplace/educational setting (Kennedy, 2005). Further support was offered by the PHE e-Bug team where needed, including supplying training materials. Workshops were tailored to the needs of the group; all included information on four core topics (microbes, hand hygiene, respiratory hygiene, antibiotics), and optional topics were included depending on interest and need. The workshops were delivered by PHE staff experienced in delivering training with a background in public health, health psychology and microbiology.
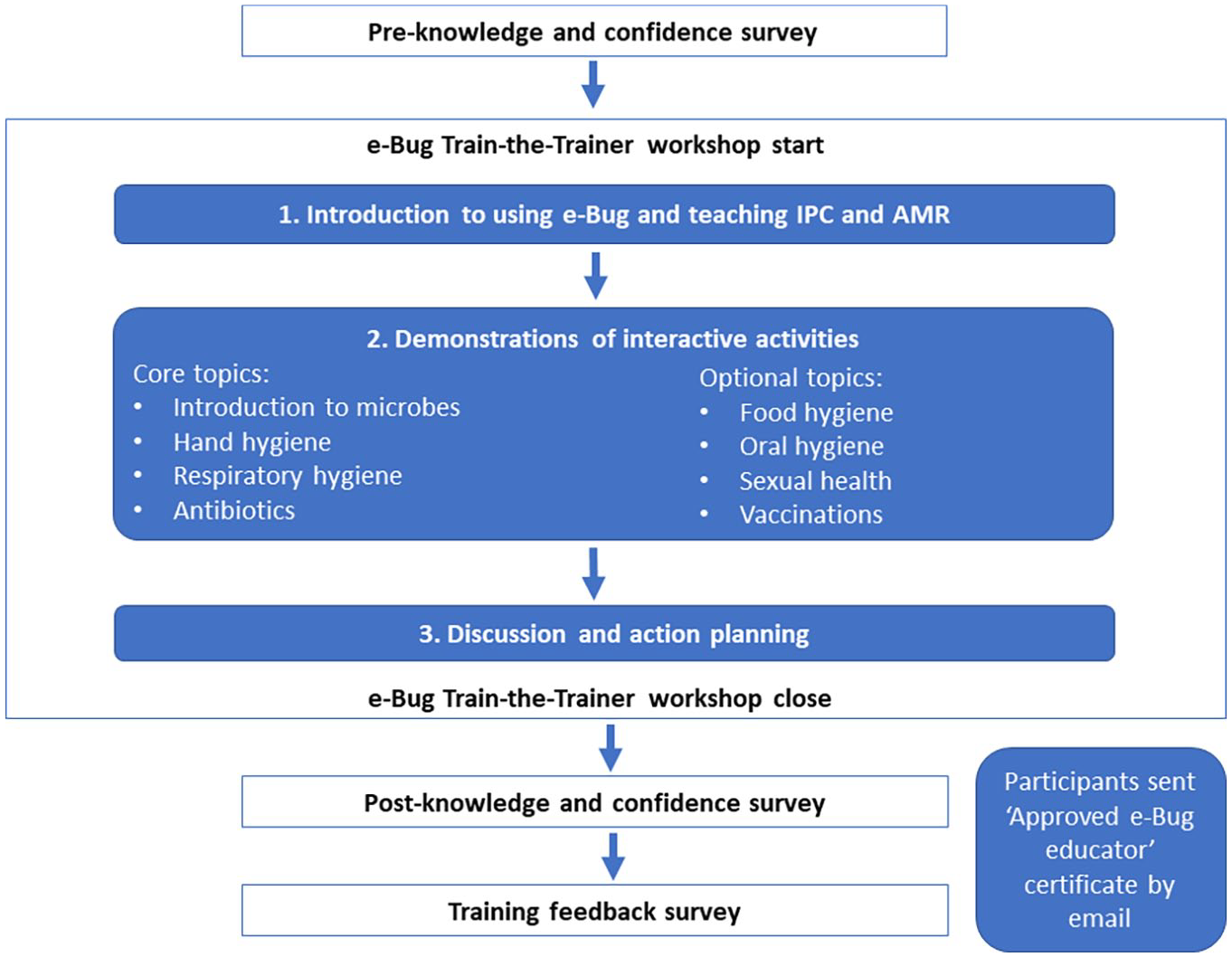
Data collection process map and workshop stages.
Setting and recruitment
Thirteen workshops were organised between June 2018 and 2019, across seven regions of the UK with the support of collaborators (see Supplementary Material). Educators were not recruited from Wales for this evaluation, as the intervention was implemented across Welsh local authorities in 2017 and training workshops were arranged by the Welsh Network of Healthy Schools Schemes (WNHSS).
Collaborators supported the recruitment of educators by promoting the workshops via mailing lists, dedicated websites and social media platforms. Workshop attendees were invited to participate in the survey evaluation to provide data to improve the workshops and for use in publications. Of the 266 workshop participants, 262 opted to complete the pre- and post-knowledge and confidence survey and 165 completed the training feedback survey.
Survey design
For the pre- and post-knowledge and confidence survey, 12 questions covered knowledge of core topics and a further 8 covered additional topics, based on questions validated in previous PHE evaluations (Eley et al., 2018, 2019b; Young et al., 2017). Likert scale questions were developed to measure participants’ confidence to teach about IPC and AMR topics, from very confident (could answer questions and lead discussion) to very unconfident (would choose not to teach it). This questioning method was based on the validated Sex Education Confidence Survey (Balkin, 2008). Questions on additional topics were only answered by participants who received training on them. The pre-intervention survey (see online Supplementary Material) also contained demographic questions, including occupation, age and qualifications. Identifying information was used solely for the purposes of matching the pre- and post-knowledge and confidence survey, and then anonymised. A training feedback survey was developed and tested during piloting and included open-ended and Likert scale questions on the value, design and content of the workshops (see online Supplementary Material).
Data collection
Surveys were distributed and collected by members of the PHE project team (Figure 1). The knowledge and confidence surveys were completed on paper before the start of the workshop and again afterwards. The intervention feedback survey was completed by participants anonymously after the post-knowledge and confidence survey.
Data analysis
Pre- and post-knowledge and confidence survey
Quantitative data were input into Epidata v4.6.0.0 and Stata v15 for data analysis. Three- or two-level multilevel models depending on feasibility and parsimony, or panel models if necessary, were used to evaluate the change in knowledge and confidence of educators following intervention. Single-variable analysis was performed to measure association of the outcome with period (before/after intervention), and multivariable analysis was performed to adjust the association for other fixed effects in the model, including the demographic data collected. Results persisted in the multivariable analysis; therefore, single-variable analysis is only presented. To determine whether change in knowledge or confidence varied significantly between educator types, an interaction between period and type was included. For binary outcome data (knowledge questions), logistic regression was used; for Likert scale confidence data, ordinal logistic regression was performed, and a sensitivity analysis of linear regression was completed to check robustness to assumptions. A likelihood ratio test, if possible, or Wald test was performed to obtain p-values, and the statistical significance level was set at 5%.
Training feedback survey
Data were input into Microsoft Excel and descriptive statistics were completed for Likert scale questions. Qualitative open responses were inputted into NVivo 11, and the software was used as a tool to perform thematic analysis. Two researchers explored themes emerging from the data and then agreed on a thematic framework. Quotes were selected based on representativeness to the themes.
Ethics
As a service evaluation study, approval through National Research Ethics Service was not required. PHE Research Ethics and Governance Group provided approval following governance review; an ethical review was not required due to the study being an evaluation of a teaching resource. All participants who completed the surveys were aged over 18 years and had been informed of the purpose of the survey during the intervention. Consent was deemed accepted on completion of the surveys. Survey responses were collected in line with the Data Protection Act 1998 and Caldicott 1999 regulations on handling and distributing sensitive participant information.
Results
Participants
Of the 266 educators who attended train-the-trainer sessions, 262 (98%) participated in the evaluation from regions of England, Scotland and Northern Ireland, including various teaching backgrounds (Table 1). Educator types included primary (46%), secondary (17%), college (2%), healthcare professionals (29%) and community educators (7%). There were a higher proportion of women (88%) in comparison with men (9%), and three-quarters held a bachelor’s or master’s degree. Sixty-eight percent of educators received training on additional topics.
Characteristics of participants (N = 262).
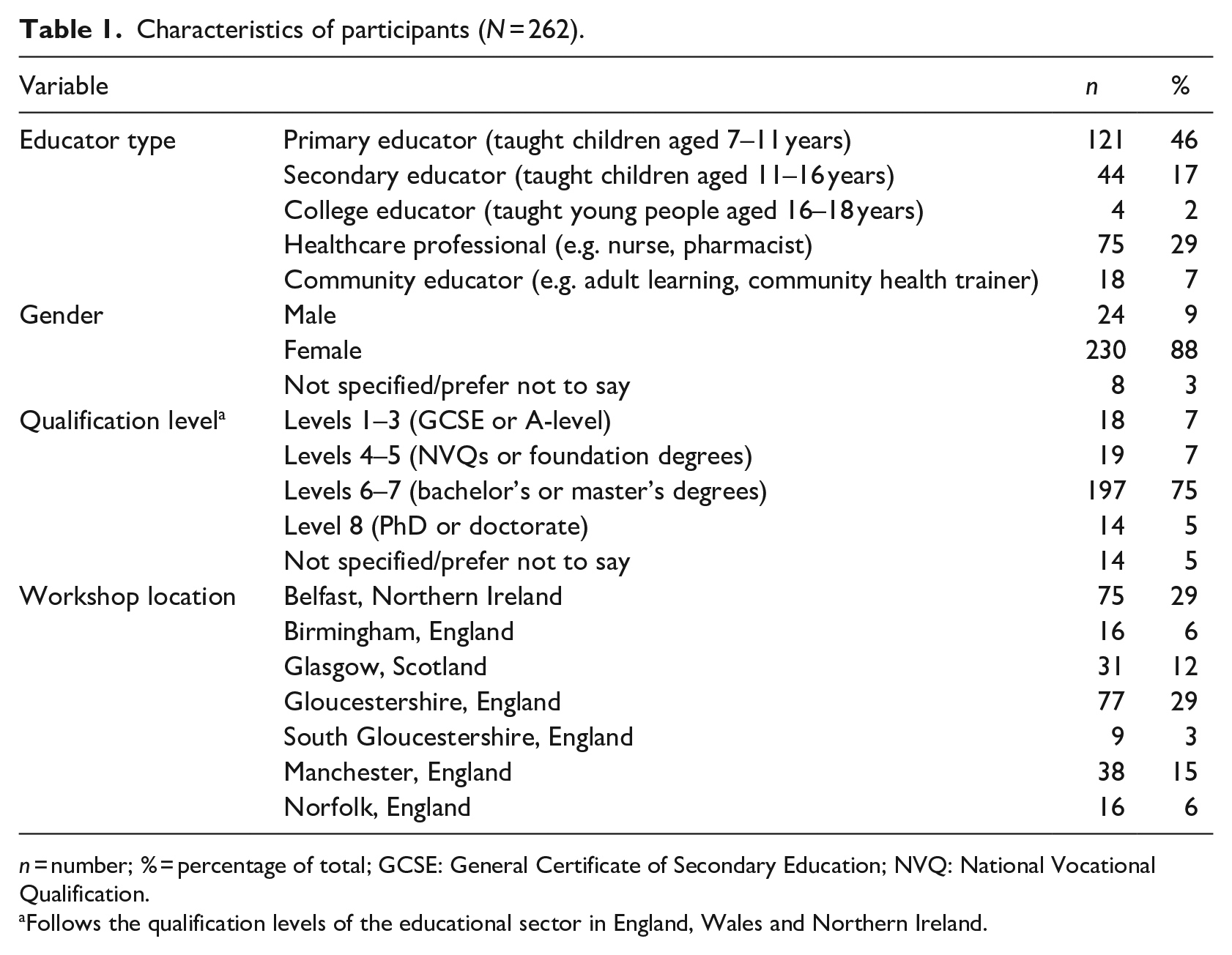
n = number; % = percentage of total; GCSE: General Certificate of Secondary Education; NVQ: National Vocational Qualification.
Follows the qualification levels of the educational sector in England, Wales and Northern Ireland.
Educator knowledge
All but 3 of the 20 questions covering core and additional topics had pre-intervention knowledge >70%. Pre-knowledge was particularly high for handwashing (100% correct knowledge of when handwashing was needed), and all questions around antibiotics had >88% correct knowledge. Four questions showed strong evidence (p < .05) of improvement post-intervention (Figure 2) and, of these, three did not differ significantly between educator types. Correct knowledge of the questions ‘which is not a microbe?’ improved from 74% to 89.3% and ‘why do we need to use soap to wash hands?’ almost doubled from 45.3% to 89%. Pre-knowledge of the question ‘what is the best way to stop microbes spreading?’ was initially very high (95.2%) and improved to 99.1% post-intervention. For the question ‘which is the smallest microbe’, there was very strong evidence (p < .001) for a difference in improvement by educator type, with most benefit for primary educators.
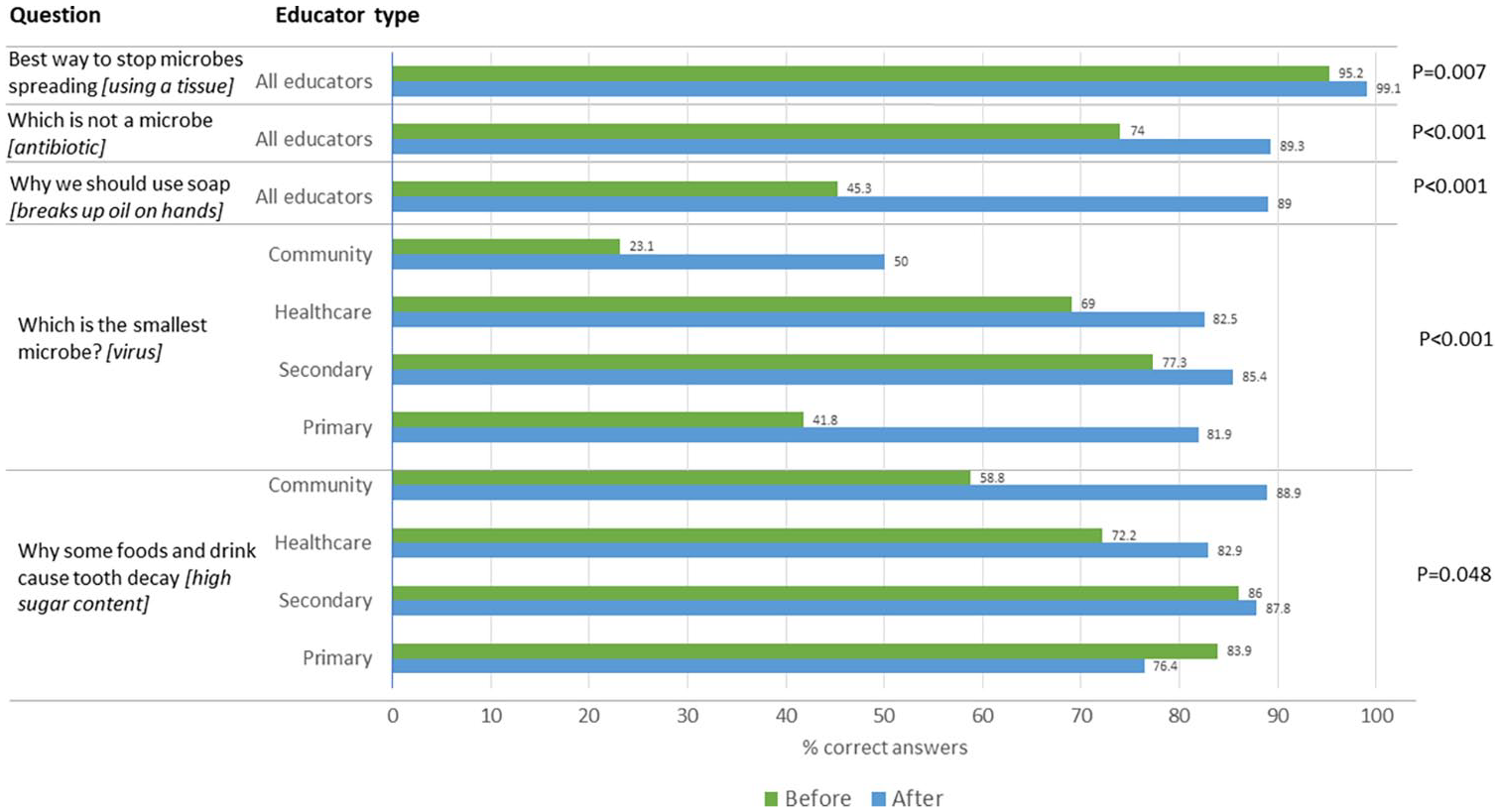
Results of the single-variable analysis where significant knowledge change of educators was observed.
Educator confidence
Pre-intervention confidence to teach others about IPC and AMR differed by educator type, and primary and community educators reported overall lower confidence. The proportion of primary educators who felt unconfident or very unconfident (where they would struggle or choose not to teach a topic) was 23% for respiratory hygiene, 31% for microbes and 53% for antibiotics. Post-intervention, 86% of primary educators felt confident or very confident (where they could lead discussion with little aides) to teach about antibiotics. In comparison, 71% of healthcare professionals felt confident or very confident to teach antibiotics pre-intervention, and this increased by 16% post-intervention to 87%.
Pre-intervention, 38% and 37% of educators were unconfident or very unconfident to teach about vaccination and sexual health, and this improved to 71% and 73% confident or very confident after intervention, respectively. In comparison, confidence to teach about hand hygiene, food hygiene and oral hygiene was higher pre-intervention (84%, 65% and 66%, respectively). Post-intervention, the proportion of educators who felt confident or very confident to teach was 98% for hand hygiene, 90% for food hygiene and 89% for oral hygiene.
There was a significant improvement (p < .05) in participants’ confidence to teach all topics post-intervention. There was very strong evidence (p < .001) for a change in confidence to teach about hand hygiene and additional topics (vaccination, sexual health, food hygiene and oral hygiene) post-intervention; however, this did not differ significantly according to educator type (Figure 3). In comparison, there was a significant difference observed in the change in confidence between educator types to teach core topics – microbes, respiratory hygiene and antibiotics (Figure 4). In all cases, primary and community educators had the biggest change in confidence; however, the results were subject to uncertainty due to the small sample of some educator types (college and community), which led to wide confidence intervals.
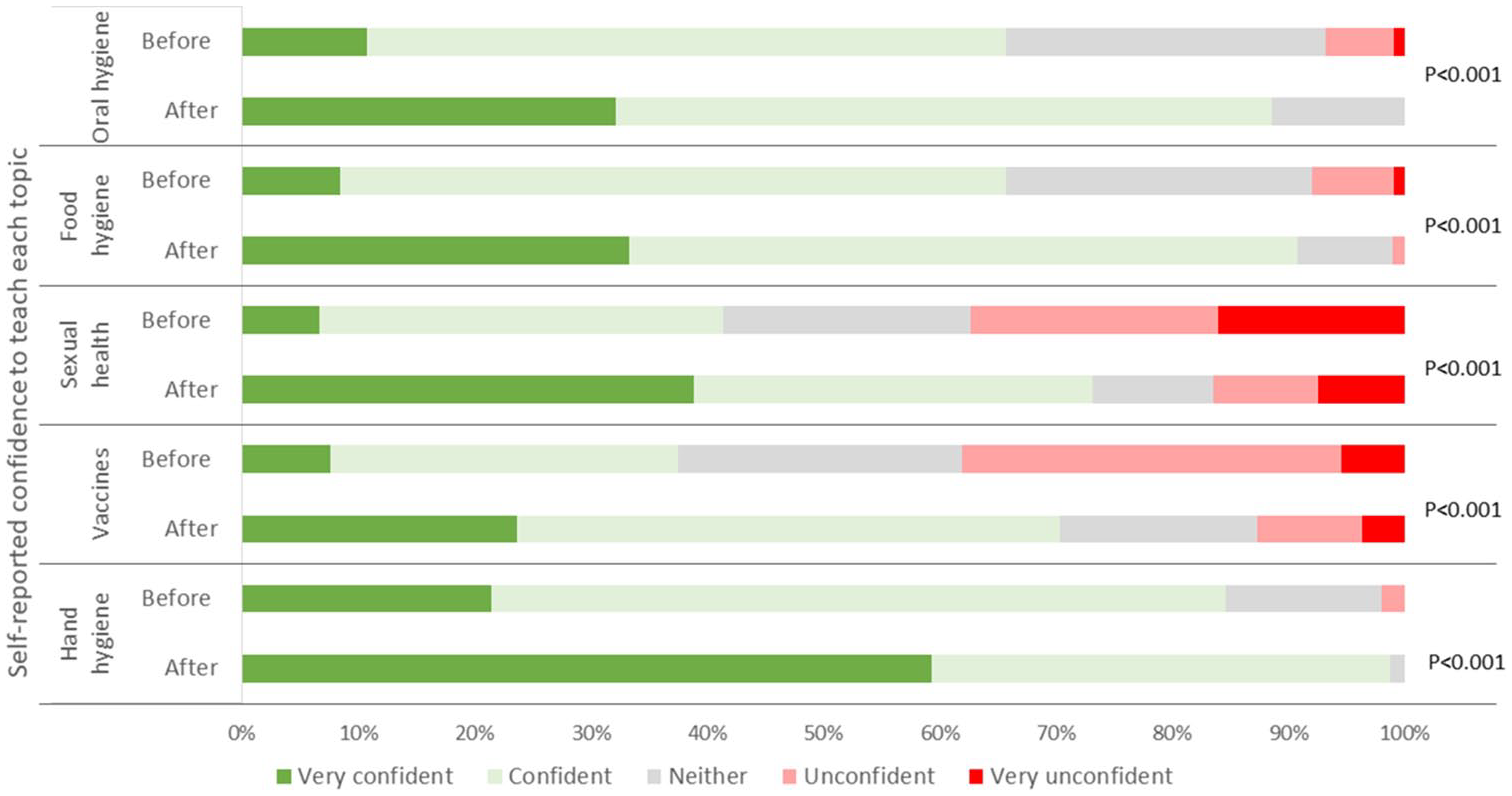
Single-variable analysis of change in confidence to teach infection prevention topics, not differing significantly by educator type.
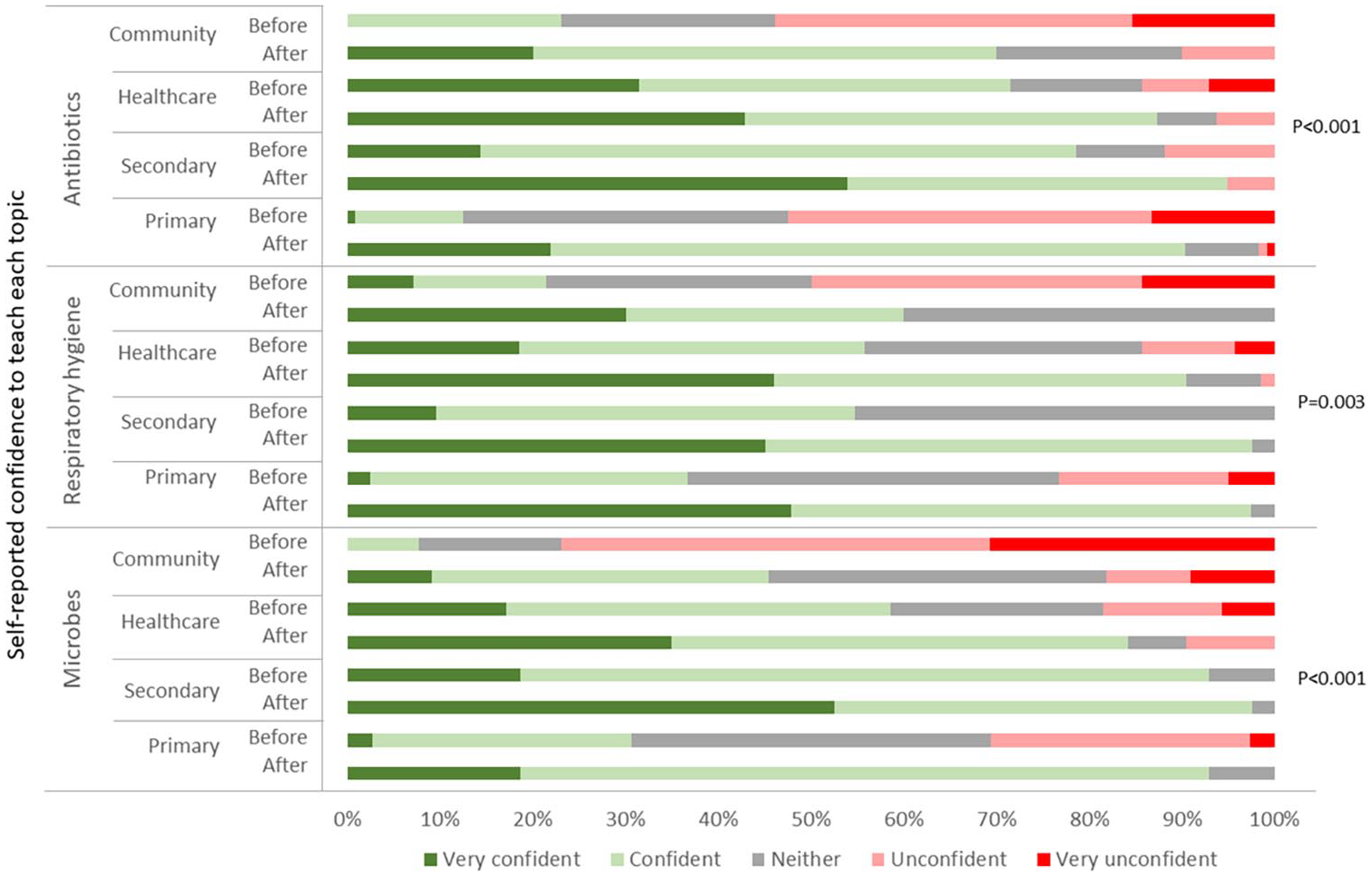
Single-variable analysis of change in confidence to teach infection and antibiotic topics, differing significantly by educator type.
Workshop feedback
Of the 262 educators, 135 provided feedback on the train-the-trainer workshops. The workshop was rated ‘excellent’ or ‘good’ by 95%, the balance of activities to discussion was reported to be ‘excellent’ by 64% and the workshop length was reported to be ‘just right’ by 89%. Half of the educators reported they would use the e-Bug resources on a termly basis, 19% monthly, 8% weekly and 22% would use them at least once a year.
Themes from the open-ended responses supported the positive view of the train-the-trainer workshop. Educators reported that the workshops were informative and engaging and that the interactive and ‘hands-on’ demonstrations could be recreated and adapted for their setting. A primary educator (participant 77) described the workshop as follows: ‘Lots of information backed up by practical ideas plus resources to ensure we can take them back to school’; a secondary educator (participant 109) reported, ‘All activities can be easily used at KS3/4 particularly KS3 at this time of year. Activities were short and engaging’.
Educators valued the skill and knowledge of trainers in providing further information and leading discussions. A community educator (participant 56) reported, ‘Both trainers very skilled. Kept it moving, very knowledgeable and approachable, encouraged discussion and used questioning to check understanding’.
Educators reflected on their skills gained from the workshop, particularly the confidence to teach the topics covered and improved awareness of the topics and e-Bug resources. Educators reported intentions to return to their school or community and deliver education or train colleagues. A primary educator (participant 120) said, ‘It has raised my confidence in teaching in this area. Also, I will be able to disseminate info to my colleagues’; a secondary educator (participant 177) described the workshops as ‘Very useful – Feel confident that I could incorporate resources and do them in the classroom tomorrow’.
Weaknesses of the training reported by participants included the fact that some struggled to understand advanced topics and terminology, including antibiotic resistance, and felt that information could be simplified for non-scientists. A community educator (participant 6) said, ‘I do not have a background in science so do not have much experience in the terminology used. Maybe to simplify some for lower ability individuals’. Some participants felt that more information on antibiotic resistance was needed; a community educator (participant 26) reported, ‘. . . I still feel I have little understanding and confidence regarding antibiotic resistance’. Some participants felt that more time could be given to education and group discussion; a healthcare professional (participant 136) reported, ‘The time available I feel squashed some of the possible audience discussions. I feel the adults need the education as much as the students’.
Discussion
Main findings
The e-Bug train-the-trainer intervention significantly improved the confidence of educators to teach IPC and AMR topics, and the interactive nature of the training was valued. Educators’ pre-intervention knowledge was high for most topics and there was less improvement in knowledge observed post-intervention. It is not surprising that knowledge was initially high, as half of the participants were either healthcare professionals or secondary school educators, and therefore trained or experienced in science and health topics. Where knowledge improved, it was greatest for primary and community educators who did not specialise in science. When additional topics were added to the training, the content covered was reduced so that the length remained the same (half-day), which could explain the lack of significant knowledge gain for some topics. Feedback from those without a science background suggested the technical information around antibiotic and antibiotic resistance topics may be pitched too high, and some educators felt the training should be longer to cover more information.
Comparison with existing literature
The authors believe this is the first study to evaluate a face-to-face training intervention for educators to improve teaching of IPC and AMR topics in schools and communities. Similar to the original e-Bug e-Learning, educators self-reported a gain in skills including confidence and self-reported knowledge of e-Bug (Eley et al., 2019a). Pre-intervention knowledge of antibiotics was high in our study in comparison with previous research (Kotwani et al., 2016; Norris et al., 2009); however, this may be due to the self-selection of participants and the high number of those with science training. Previous work has found that secondary educators lack confidence and feel uncomfortable teaching sexual health topics (Cohen et al., 2004; Westwood and Mullan, 2007); similarly, this study found low confidence to teach about sexual health pre-intervention, but this increased significantly post-intervention.
The high pre-intervention knowledge and confidence that was observed around oral health is supported by Eley’s (2020) previous work with primary educators (Eley et al., 2020); however, in the present study, educators had good knowledge of the effect of sugar on oral health pre-intervention, which may be due to the sample including healthcare professionals. Previous work with primary educators in New Zealand (Norris et al., 2009) identified a lack of confidence to teach about antibiotics, which was also observed in our study. Lack of confidence is commonly cited as the biggest barrier for primary educators in teaching primary science (Murphy et al., 2007), which may be exacerbated by a lack of science content in Primary Teacher Training at college or undergraduate level (Wellcome, 2017).
Educator training workshops have been an effective intervention for similar topics, including physical education (Hivner et al., 2019). HIV and AIDS workshops have significantly improved the knowledge and teaching confidence of secondary school educators (Sarma et al., 2013), and workshops for healthcare professionals have improved hand hygiene behaviour (Bellissimo-Rodrigues et al., 2015; Tartari et al., 2019). Through the high number of healthcare professionals attending the workshops, our study supports the observation that interventions designed for the educational setting may be transferable to healthcare or community settings. Activities designed for children could be transferable to adult audiences, as demonstrated by Eley et al.’s (2018) use of e-Bug to improve knowledge of young parents in a children’s centre setting (Eley et al., 2018).
Strengths and limitations
A strength of this study is that the workshops were based on the NICE-endorsed e-Bug resources (National Institute for Health and Care Excellence, 2017) and developed with the input of educators. This sample of participants may have had an existing interest and high knowledge of the topic as they had opted to attend workshops. The high proportion of female participants may reflect the target audience; 85% of primary educators (World Bank, 2020) and 77% of the National Health Service (NHS) workforce (The Kings Fund, 2018) in the UK are women. School educators and healthcare professionals require formal qualifications for their role, which may explain the high qualification levels observed and high pre-intervention knowledge.
Ninety-eight percent of those who attended the workshops completed the pre- and post-knowledge and confidence survey, and 52% provided anonymous feedback. The high number completing the former survey is a strength as the knowledge and confidence data are representative of individuals who took part in the intervention, whereas the intervention feedback may not be. The lower sample size for intervention feedback may be because this survey was provided last. Participants may have chosen not to complete it because of fatigue or lack of time, and therefore future studies should use one merged survey to improve completion rate. The feedback was altogether positive; however, the half who did not provide feedback may have had a different experience from those who did complete it.
A strength of the sampling is the large number of participants, representing regions of England, Scotland and Northern Ireland. Furthermore, the inclusion of a mix of educator types including healthcare professionals provided interesting insight into the different value of the training by educator type. The low sample size of different educator types led to some uncertainty in statistical analyses and may prevent generalisability.
Implications and future work
Implications for local authorities
As the national curriculum in England will include more education on hygiene and antibiotics from 2020 (HM Government, 2019a), educators’ lack of confidence to teach these topics needs to be addressed through teacher training and the provision of evidence-based resources, as modelled in this study. e-Bug train-the-trainer workshops can also support educators in teaching IPC topics to children during pandemic situations, such as the coronavirus disease 2019 (COVID-19).
The implementation of e-Bug train-the-trainer workshops through local authorities and other agencies is a potentially effective way of expanding this intervention. All UK local authorities should consider uptake of the training or integration into existing practice, and the PHE e-Bug team have developed guidance and tools to support this, including free online training for educators (Future Learn, 2020).
Implications for PHE
The evaluation has provided evidence for revision of the train-the-trainer workshop content to increase accessibility for those without a science background. Although many participants were happy with the length of the half-day training, further information should be given to educators lacking a science background (primary and community). The knowledge survey will be reviewed with educators and healthcare professionals to ensure questions are pitched to the right level and not misinterpreted.
This study shows that training can improve healthcare professionals’ and community educators’ confidence to deliver education. PHE could explore the integration of e-Bug train-the-trainer in healthcare settings and encourage healthcare professionals to train colleagues and educate patients. Train-the-trainer workshops facilitated by PHE currently exist for general practice staff and have been shown to improve antibiotic prescribing in primary care settings (McNulty et al., 2018).
Future work
Qualitative feedback suggested educators intended to deliver education using e-Bug. Therefore, PHE plan to incorporate long-term follow-up based on the COM-B (capability, Opportunity, Motivation, Behaviour) model of behaviour change (Michie et al., 2011) to understand barriers and facilitators to delivering education or training others. In similar studies, while training may have improved confidence to teach, the subsequent implementation of education may not occur due to the lack of motivation, time and resources (Bellissimo-Rodrigues et al., 2015). Future evaluation of impact could be measured through a case–control study, as demonstrated by Sarma and colleagues with an HIV-related training intervention for school educators (Sarma et al., 2013). A study in progress in South Gloucestershire may provide insight into the impact of the training of educators on the handwashing behaviour of primary students following education; however, the sample size of educators in this study is small (South Gloucestershire Council, 2013). As the wider e-Bug project is an international collaboration, expansion and adaptation of training elsewhere in Europe is currently taking place.
Conclusion
The e-Bug train-the-trainer intervention improves educators’ confidence to deliver IPC and AMR education regardless of their professional and qualification background and therefore supports the aims of the UK AMR National Action Plan. Confident educators will help to engage and provide young people with the capability to prevent and self-care for infections, to use antimicrobials appropriately and to subsequently help reduce rates of AMR. Training content will be reviewed to improve the knowledge of educators, including more information for those who lack formal science training. Local authorities across the UK are being encouraged to implement the train-the-trainer workshop in their schools and communities.
Supplemental Material
HEJ-20-0169_Supplementary_(1) – Supplemental material for Improving educator’s knowledge and confidence to teach infection prevention and antimicrobial resistance
Supplemental material, HEJ-20-0169_Supplementary_(1) for Improving educator’s knowledge and confidence to teach infection prevention and antimicrobial resistance by Catherine Hayes, Charlotte Eley, Carla Brown, Rowshonara Syeda, Neville Q Verlander, Magda Hann and Cliodna McNulty in Health Education Journal
Footnotes
Acknowledgements
We thank our collaborators, including the Public Health Agency, Gloucestershire County Council, Manchester University, Birmingham Clinical Commissioning Group, Health Protection Scotland, the Scottish Antimicrobial Prescribing Group (SAPG), Rebecca Owens at the Open University, Independent Living Skills and South Gloucestershire Council, for enabling delivery and supporting data collection for the evaluation. We also thank Public Health Wales and the Welsh Network of Healthy Schools Schemes (WNHSS) for implementing this intervention in Wales and providing feedback. We thank Alicia Demirjian and Emily Cooper within the Primary Care and Interventions Unit for their comments to the manuscript and Julie Brooke for manuscript support. Thanks to all educators for taking part in this service evaluation and for feedback on the intervention.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research authorship, and/or publication of this article. At the time of data collection, all authors except N.Q.V. worked on the e-Bug programme and were involved in delivery of the train-the-trainer workshops.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. Development and delivery of the intervention were supported and funded by Public Health England. Accommodation and travel for PHE staff to deliver training was in some cases supported by collaborating organisations.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.