
Abstract
Objectives:
Breastfeeding is the optimal method of infant nutrition. Despite this, rates of breastfeeding in high-income countries are low and mirror wider health inequalities with women from under-served populations being least likely to breastfeed. In the UK, adolescent mothers from areas of high socio-economic deprivation are among the least likely groups to initiate and continue breastfeeding. This study aimed to examine young women’s experiences of breastfeeding, with a particular focus on information provision and relationships with healthcare practitioners.
Methods, design and setting:
Data were collected through qualitative focus groups and interviews with 27 adolescent mothers from areas of socio-economic deprivation in Belfast (Northern Ireland), Bristol (South West England) and Middlesbrough (North East England). Questions focused on the support young mothers receive for breastfeeding with a particular focus on the importance of healthcare practitioners in breastfeeding practices.
Results:
Although young mothers were well-informed about the benefits of breastfeeding, they lacked basic information which led to early cessation. Moreover, mismatched cultural health capital between healthcare practitioners and adolescent mothers led to perceived strained relationships wherein young mothers felt undermined and not listened to. We suggest that this arises from an intersection of age-related lack of confidence and low cultural health capital arising from differences in socio-economic status.
Conclusions:
Recommendations are offered for a more holistic approach to young mothers’ maternal health and the use of peer supporters.
Introduction
Breastfeeding is the optimal method of infant nutrition, linked with a variety of health benefits for mothers and infants including reduced risk of diabetes, sudden infant death and some cancers (World Health Organization [WHO], 2003). WHO (2003) recommends exclusive breastfeeding for the first 6 months of an infant’s life and combined feeding for the first 2 years, a recommendation reflected in public health guidance globally.
Despite this, rates of breastfeeding in high-income countries fall far below the recommendation of the WHO and public health agencies. The UK’s most recent Infant Feeding Survey demonstrated that while 81% of babies are breastfed at least once, only 1%–2% of infants are exclusively breastfed at 6 months old (McAndrew et al., 2012) and less than 1% of 12-month-old infants receive any breastmilk at all (Victora et al., 2016). This has been, in part, attributed to the UK’s ‘anti-breastfeeding culture’ in which breastfeeding is only deemed acceptable under particular circumstances such as being done discreetly to very young babies and women’s bodies showing no visible signs of lactation such as breast enlargement or milk seepage (Kitzinger, 1994: 82; Morris et al., 2016).
Moreover, patterns of breastfeeding mirror wider health inequalities with low-income mothers, young mothers, women who left education early and those working in routine occupations being the least likely to breastfeed (McAndrew et al., 2012). This patterning is reflected in most other developed countries too. For example, Stolzer and Zeece (2006: 129) noted that in the USA breastfeeding rates are ‘significantly lower’ among economically and socially disadvantaged populations while Arora et al. (2012) found that Australian mothers with higher levels of education were more likely to exclusively breastfeed until their child was 6 months old.
In this article, we focus on adolescent mothers living in areas of high socio-economic deprivation in the UK who are among the least likely groups to breastfeed. Only 11% of UK mothers aged under-20 still breastfeed at six months, compared with 45% of those over 35 (McAndrew et al., 2012). This compounds existing health inequalities affecting young mothers and their children. For example, the Royal College of Midwives, Public Health England and Department of Health (2014: 4) suggests that children of teenage mothers are 25% more likely than babies of older mothers to be born at a low birthweight and have an infant mortality rate 60% higher than babies of mothers aged 20–39.
Research demonstrates that young mothers are well-informed about the health benefits of breastfeeding (Condon et al., 2012: 158) but face barriers including reluctance to breastfeed in public (Dyson et al., 2010), low tolerance of pain (Wambach and Koehn, 2004), complications with work or education (Spear, 2006), and the incompatibility of breastfeeding with cultural norms (Condon et al., 2012). While research has identified effective breastfeeding support for women more widely (e.g. Guise et al., 2003), adolescent mothers face different challenges (Hunter et al., 2014) and require specific support interventions at particular times post-partum (Muelbert and Giugliani, 2018). For example, while breastfeeding groups are beneficial for mothers generally, Fox et al. (2015) noted adolescent mothers’ discomfort in groups which are not age-specific.
Dykes et al. (2003) identified five key areas of breastfeeding support benefitting young mothers: instrumental, informational, network, esteem and emotional. Within this, effective support from healthcare practitioners is particularly pertinent and associated with longer breastfeeding and better breastfeeding experiences (Wambach and Koehn, 2004). Clark and Price (2018) similarly argued that support from healthcare practitioners can ‘empower’ adolescent mothers to breastfeed. McVeigh and Smith (2000) suggested that support from healthcare practitioners can translate into social support from family and partners, though Hunter and Magill-Cuerden (2014) stressed the need for this support to fit into young mothers’ wider lives, which can often be complex.
However, healthcare practitioner support for breastfeeding is not always effective. While tensions between healthcare practitioners and maternity service users occur in other demographic populations, research has suggested that the wider stigma around young motherhood (e.g. Yardley, 2008) can translate into specific forms of strained relationships and the experiences of young mothers cannot simply be conflated as a sub-set of those of mothers more generally (Hunter and Magill-Cuerden, 2014). In the USA, Stolzer and Zeece (2006) have highlighted the inadequacy of practitioners’ knowledge of lactation which translated into poor advice for disadvantaged mothers. In UK maternity services, research has demonstrated that young mothers feel they are treated less favourably because of their age and perceived themselves to be ignored by midwives (MacLeod and Weaver, 2002). Similarly, participants in Whitley and Kirmayer’s (2008) research felt stigmatised by healthcare practitioners because they had become parents ‘young’, which placed them at increased risk of post-natal depression and further social exclusion. For Dykes et al.’s (2003: 395–396) sample of young mothers, having healthcare practitioners who were on the same ‘wavelength’ was important though the roots of this wavelength matching have not been drawn out.
In this article, we propose the theory of ‘cultural health capital’ (Shim, 2010) as a lens through which to understand the uneasy relationship between healthcare practitioners and adolescent mothers around breastfeeding support. Cultural health capital is rooted in Bourdieu’s (1977) wider notion of cultural capital, which maintains that particular practices, including style of dress, ways of speaking, eating habits, leisure activities and so on, are forms of capital through which a person can accumulate status and power. People who participate in practices with higher cultural capital (e.g. listening to classical rather than popular music) are often regarded as ‘more intelligent or gifted’ (DiMaggio, 1982: 190) and have better educational outcomes. As such, cultural capital maps onto, and reproduces, wider patterns of inequality, with those from lower socio-economic and other disadvantaged groups accumulating less cultural capital which translates into fewer opportunities, lower attainment, and less social mobility.
The concept of cultural health capital looks specifically at the ways higher cultural capital can be mobilised in healthcare contexts and be beneficial for health. Shim (2010: 3) proposed cultural health capital as a collection of skills and attributes enabling healthcare users to ‘optimise their relationships with health professionals and the care they receive’. Among these skills are self-discipline, proactive approaches to health, the ability to navigate the healthcare system, and effective communication with practitioners. As such, people with existing high cultural capital are able to transpose this into healthcare settings and navigate the system to their advantage. Deployment of these skills in healthcare interactions can grant users increased access to care and treatments, and greater participation in joint decision-making (Dubbin et al., 2013). While cultural health capital has some overlaps with health literacy, it goes beyond this. Whereas health literacy focuses on patients having technical vocabulary through which to communicate effectively with practitioners, cultural health capital is about a wider presentation of self as a responsible, engaged, good patient. This can lead to practitioners’ ‘more favorable estimations of their patients, and subsequently to additional attention and health care’ (Dubbin et al., 2013: 114).
Cultural health capital has been shown to be an important factor in health promotion and public health (e.g. Abel, 2007; Dubbin et al., 2013) but has yet to be applied to breastfeeding support. In maternity services more generally, it has been demonstrated that women with lower cultural health capital have worse experiences. One participant in Phillimore’s (2015: 575) research on migrant women in a ‘superdiverse’ UK city, for example, commented that maternity services were ‘geared up for white middle class women’.
This article suggests that cultural health capital is a useful framework through which to more holistically understand and theorise young mothers’ breastfeeding support experiences and needs. In other words, while age is a key factor in women’s experiences of breastfeeding support, the complexity of these experiences is not always captured by age alone but arises from a coalescence of age, socio-economic status and local cultural norms (e.g. Condon et al., 2012) which is well-captured by the notion of cultural health capital. We argue that practitioners need to be sensitive to the potentially lower cultural health capital of disadvantaged groups which can result in healthcare practitioners not being on the same ‘wavelength’ as healthcare users and, consequently, being perceived as unsupportive. In doing so, this article draws on the lived experiences of young mothers in their own words, which Dykes et al. (2003: 392) have argued is necessary for developing effective support services.
Methods
Findings presented here are drawn from two qualitative studies. The first focused on general health beliefs and behaviours of young mothers living in areas of social and economic deprivation (Hackshaw-McGeagh et al., 2018) and the second examined three case examples of young mothers’ breastfeeding experiences. The findings presented here are drawn from a sub-set of findings from the first study and the full dataset from the second study.
For the first study, 27 young mothers (women with at least 1 child by age 21, participants ages ranged from 16 to 24 years) were recruited from areas of high socio-economic deprivation in three UK cities – Belfast, Northern Ireland (n = 9), Bristol, South West England (n = 13), and Middlesbrough, North East England (n = 5). Twenty-six of the participants were white British, 1 was mixed race, 21 had one child, 4 had two children and 2 had three children. Participants’ children were between 5 years old and newborn and three participants were pregnant at the time of the research. Participants were recruited through parent support organisations which sent out recruitment material on behalf of the project team. The inclusion criteria were that participants were female with at least one child before the age of 21 and had capacity to consent. There was no lower age limit for participation. Women who had children after the age of 21 were excluded as they do not fall into the ‘adolescent’ category. Where women had a child under the age of 21, then subsequent children after 21, they were still eligible to participate. All recruitment material was checked by parental support organisations’ staff to ensure it was comprehensible and accessible to the sample population.
Following informed consent, which was collected at an introductory session, participants took photographs over the course of a week which demonstrated a typical 7-day period in their lives as young mothers. Although the focus of the first study was on health beliefs and behaviours, participants took photographs which depicted their weekly activities more broadly to illustrate the contexts in which health-related decisions are made. Photos were used to facilitate discussions within focus groups and are not separately analysed here. We used photo elicitation to (1) give participants a degree of ownership of the project, (2) engage the participants deeply in the project and (3) informally begin conversations and as a prompt for discussion. Given the regular political and practice scrutiny young motherhood is subject to, we were keen to avoid directly questioning participants in case this was perceived as confrontational. Photo elicitation provided a way through which we were able to access women’s stories and experiences in a non-threatening and non-judgemental way. Photo-elicitation has been used with lesbian, gay, bisexual, and transgender (LGBT) communities (Johnson, 2007) and homeless populations (Radley et al., 2005) as a tool to reduce pre-established barriers or to access and engage harder to reach minorities, enabling participants to tell their stories and enabling researchers to access information that might otherwise be out of reach (Reavey, 2012).
Following this period of photo elicitation, two focus groups were held in each area. At the first, participants’ photographs were shared and their depictions of everyday life as young mothers were discussed. These were informal discussions prompted by participants’ photographs and guided by a topic guide where necessary. The topic guide covered themes such as experiences of telling people about a pregnancy, experiences of judgement and the challenges and opportunities of young motherhood. The second focus group occurred approximately a month after focus group 1 and focused specifically on health beliefs and behaviours including diet and exercise. Sixteen of the original 27 participants returned for focus group 2. Breastfeeding was discussed in both focus groups. Focus group discussions were structured by a topic guide, audio-recorded and later transcribed by a sub-contracted transcriber. Focus groups were conducted by the authors with support from researcher assistants and lasted approximately 2 hours.
Focus group data were analysed thematically using the framework approach (Ritchie et al., 2014). This method of analysis consists of six stages: familiarisation, identification of thematic coding framework, indexing, charting, mapping and interpretation. Data pertaining specifically to breastfeeding were extracted from the wider dataset and analysed separately using the same framework approach. This analysis identified that 19 participants mentioned breastfeeding during focus groups. Of those, 11 participants did not attempt breastfeeding at all, while 8 participants breastfed for durations between a few hours and 15 months. Healthcare practitioner support was identified as a particularly salient theme.
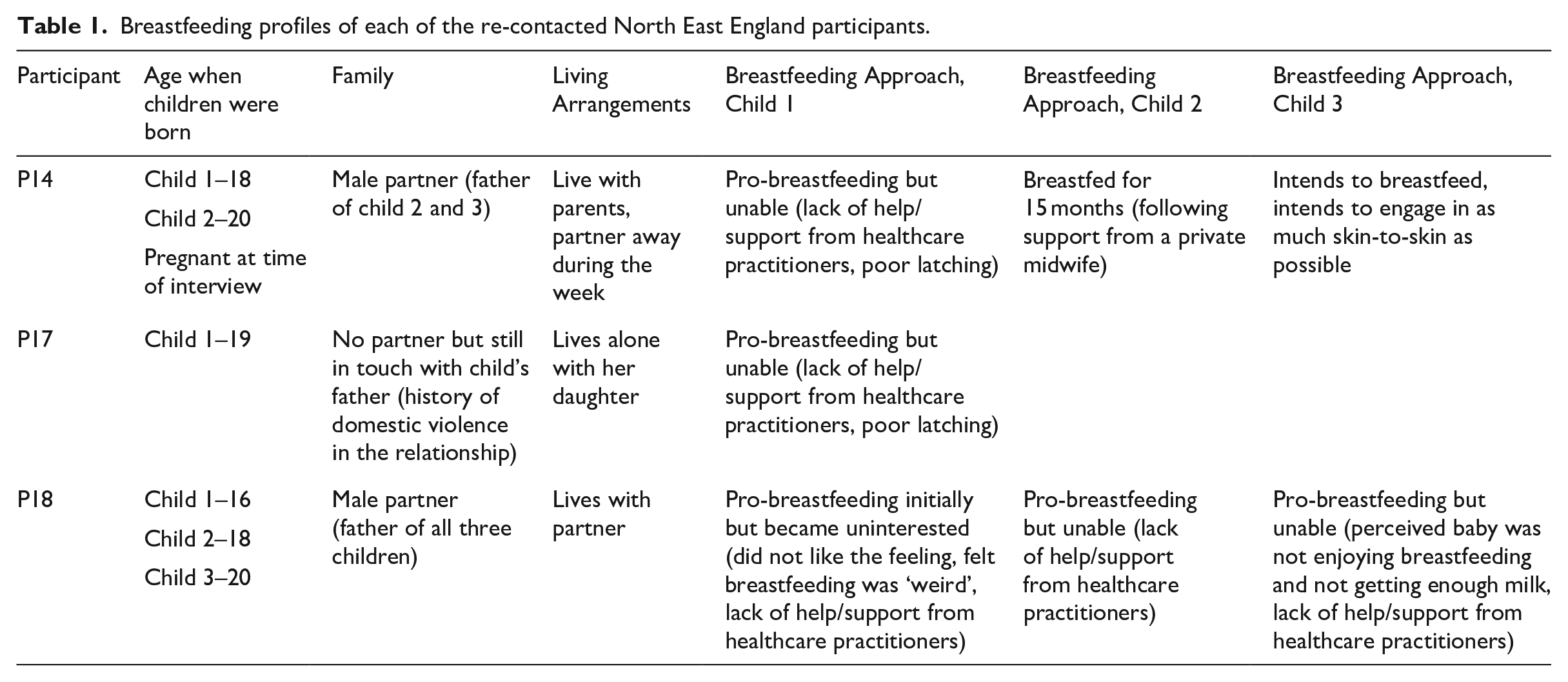
The second study built on the breastfeeding data from study one and focused on breastfeeding services in North East England through three ‘case examples’; these cases were selected because of the diversity of their breastfeeding experiences (Table 1). The intention of this follow-up study was to interrogate the breastfeeding data further and draw out in-depth stories from women with divergent breastfeeding experiences. These three participants were re-contacted and participated in in-depth semi-structured interviews about breastfeeding where they were questioned about breastfeeding support and relationships with healthcare practitioners. Interviews were conducted by HB and lasted around 60 minutes each. The data from these three follow-up interviews were combined with the overall dataset and are not analysed as a separate dataset here. These three case studies enabled us to explore and expand the salient themes from the first study in more detail. We found that the data from these case studies confirmed the focus group findings around infant feeding. In addition, these case studies enabled us to gather specific data about breastfeeding provision in the North East of England to recommend specific service provisions.
Breastfeeding profiles of each of the re-contacted North East England participants.
Ethics approval was granted by Durham University in December 2014 (for the first study) and July 2016 (for the second). Participants were not paid for their participation, but travel expenses were reimbursed. Free childcare and catering were provided for all focus groups and interviews. For anonymity purposes, participants have been given shorthand codes where, for example, P1 denotes Participant 1.
Findings
The research examined young women’s experiences of breastfeeding, with a specific focus on information provision and relationships with healthcare practitioners. Our findings focus on three key findings: (1) participants’ attitudes towards breastfeeding, (2) the information participants’ received about breastfeeding, and (3) interactions with healthcare practitioners. We draw on the framework of cultural health capital to analyse this final point in more detail.
Attitudes towards breastfeeding
Echoing findings of existing research, participants were well-informed about the benefits of breastfeeding for themselves and their children. Based on this understanding of the benefits of breastfeeding, around half of the participants made the decision to breastfeed during the third trimester of their pregnancy and attempted to breastfeed once they had given birth. However, all but one participant from whom breastfeeding data were collected were unable to breastfeed for as long as they had hoped. While we did not specifically explore women’s breastfeeding problems, participants described being unable to breastfeed because of concerns about milk supply quality, inability to latch or perceptions that their baby was not enjoying or benefitting from breastfeeding. Participants also expressed anxiety about being unable to monitor how much breastmilk their children were receiving, which was addressed by formula feeding:
You always think when you bottle feed you know how much they’re getting whereas with breastfeeding you can’t measure it. You don’t even know if they’re getting fed. (P14)
Five participants who opted not to attempt breastfeeding implied they did so, partly, because of work or educational commitments which they saw as incompatible with breastfeeding. Similar to Condon et al.’s (2012) work, some participants described breastfeeding as ‘not normal’ (P13) among their peers and in their community, which led them to opt not to breastfeed.
While previous research has suggested that public breastfeeding represents a deep-rooted challenge for adolescent mothers (Dyson et al., 2010), participants’ perspectives were more nuanced in this study. While some participants’ stories echoed existing research and demonstrated reluctance to publicly breastfeed (e.g. P10), three participants described public breastfeeding as never having been an issue (e.g. P14), even demonstrating a degree of defiance (e.g. P6):
I didn’t want to go out and just breast feed in front of everybody, I’m not comfortable with that. (P10) When I had Sophie, I breastfed her for 14 or 15 months and I never ever once felt judged or anything like that. (P14) Its [public breastfeeding] just something you’ve got to do. (P6)
Information about breastfeeding
Participants triangulated information about breastfeeding from a variety of formal and informal sources. Social media was repeatedly cited by participants as an important source of information on children’s health generally and breastfeeding specifically. Participant 14 commented,
I joined Facebook pages more than anything to see how they got on with it [breastfeeding] and if it was possible. (P14)
All participants from whom breastfeeding data were collected described receiving only scant information from formal sources such as healthcare practitioners and organisations and, moreover, perceived this information as inadequate because while it repeated the ‘breast is best’ message, it lacked practical information about, for example, what breastmilk should look like:
I was like there’s only this tiny, tiny little bit of yellow milk, what’s that? I can’t give him that, it’s yellow. I didn’t realise that’s the most important part. (P14)
Also notably absent from formal sources was information about combination feeding (i.e. combining breastmilk with bottle feeding formula):
I was of the understanding that you had to keep your baby on formula once you’d given it . . . that giving them breastmilk would mess up their digestion, you know, giving them different. . . . I didn’t have a clue. (P18)
These omissions meant that when participants experienced breastfeeding problems, which the majority did, they ceased breastfeeding altogether. In other words, because participants were unaware that combination feeding was possible, once infants had been given formula they were not then given breastmilk again. As a result, the vast majority of participants stopped giving any breastmilk at all within the first 6 months, contrary to public health recommendations. Given that the participants were well-informed about the health benefits of breastfeeding many reported feeling guilty or regretful about stopping breastfeeding early with some even describing symptoms of depression:
I got really upset and I went back to the doctor’s because I was so depressed that I couldn’t breastfeed him. (P7)
Relationships with practitioners: focus on cultural health capital
Participants drew attention to the importance of the healthcare practitioners delivering breastfeeding support services. Eighteen of 27 participants described having had strained relationships with healthcare practitioners stemming from a feeling of being undermined or not listened to, which is a common experience for populations with low cultural health capital (Shim, 2010). Of the other nine participants, three described positive relationships with individual healthcare practitioners but understood this as exceptional and attributed these positive relationships to very specific factors including having paid privately, having previously lodged a formal complaint and the healthcare practitioner themselves being a mother. The more common experience of not being listened to was felt by both breastfeeding mothers and those who formula fed. Some participants who wanted to breastfeed but had problems establishing feeding described healthcare practitioners recommending formula feeding too readily contrary to their wishes to persevere with breastfeeding:
The nurses at the hospital were absolutely terrible . . . if he wouldn’t latch on, they would just be like, ‘try and give him a bottle’. But I’d be the one to be like, no, he’s going to do it. (P7)
Conversely, participants who did not want to breastfeed described feeling under significant pressure to do so:
I told them I wanted to change her on to bottles and they tried to force me to stay on the breast . . . I actually sat and cried because they tried to force me to stay [on the breast]. (P17)
This perceived pressure to shift feeding methods was symptomatic of more general strained relationships with healthcare practitioners. Where participants described positive relationships with healthcare practitioners, these were based on legitimisation of, and support for, the choice to formula feed and on-going support for breastfeeding:
The midwife that delivered him she said, ‘do you want me to get a bottle, are you breast feeding?’, and I said to her, ‘look, I’ll try it’, and she said to me, ‘you don’t want to do you?’, and I said, ‘not really’. She said ‘if you don’t want to you haven’t got to’, and that was nice for somebody to actually to say that to me. (P9) My health visitor . . . was pro-breastfeeding so she made sure she was there quite a lot and I had her number if I needed anything. (P14)
Although Participant 14 was positive about her health visitor, she also expressed desire for breastfeeding support from people a similar age, as did other participants:
With [child] I wish I had had someone my age to show me. (P14) They should get people in to show you how [to breastfeed] . . . other young mums you can talk to. (P17)
While some participants attributed problematic relationships with healthcare practitioners to age-related lack of confidence, age alone did not capture the full complexities of navigating breastfeeding support as a young mother from a socio-economically deprived area. Uneasy relationships between adolescent mothers and healthcare practitioners were also impacted by discriminatory assumptions about young mothers, power imbalances and ineffective communication. As such, the intersection of age, socio-economic status and cultural norms which rendered breastfeeding as abnormal can be captured through the lens of participants’ low cultural health capital which placed them on a different wavelength (Dykes et al., 2003) to healthcare practitioners and made effective communication challenging.
Many participants were acutely aware of the potential stigma surrounding young motherhood (see Hunter et al., 2014), which emerges from a coalescence and conflation of age and socio-economic status where being a young mother was associated with poverty, unemployment, low educational attainment and lack of career prospects (Ellis-Sloan, 2014). These intersections and overlaps between age, socio-economic status and locality were visible in participants’ narratives about breastfeeding support:
I think it’s an age thing as well though because when I went to my antenatal classes . . . in like [name of socio-economically privileged area]. . .the age of pregnancy out there . . . where I live, everybody else is sort of doctors and lawyers and married and all that kind of stuff . . . and then there was me [laughter] and I felt really, not ashamed but I felt really quite embarrassed when I turned up to the my classes, because I was so young compared to all of them . . . I didn’t want to breastfeed, it didn’t interest me. But the lady that took the group . . . she just looked at me in disgust really when I said I didn’t want to breastfeed because I was the only one that didn’t . . . But they all did, and they probably looked at me as if I was really young. (P9)
For many participants, then, comparatively low cultural health capital, stemming from both age and socio-economic status, meant they lacked the vocabulary and confidence to become active participants in their own maternal, care. For example, a focus group discussion between Participants 1, 2 and 3 went as follows:
[Doctors] don’t take any notice of you, they’re the worst (P3) Doctors are crap. (P2) Doctors don’t take no notice of you. (P1) They just think, ‘young mother’. (P2)
In terms of breastfeeding specifically, this resulted in perceived sub-optimal support where several participants described healthcare practitioners as ‘arseholes’ (P7), a ‘nightmare’ (P17), and their support as ‘absolutely awful’ (P14). Moreover, a number of participants described acquiescing to suggestions about feeding which were contrary to their wishes because of their limited capacity for resistance:
I just took it, like the nurses. That’s what the midwives were telling me to do [give infant a bottle] so I just did it. You’re not going to argue . . . Then what I said to them is I wanted to try and breastfeed again, and they were . . . they were quite arrogant. Me being 18 at the time it was just do as they say. (P14)
Discussion
This article contributes to research on breastfeeding support by focusing on socio-economically deprived adolescent mothers in the UK, who have some of the lowest breastfeeding rates globally. We have shown that while young mothers are well-informed about the benefits of breastfeeding, they lack basic practical information, which leads to early cessation and the seeking of information, particularly through social media, which is not evidence-based.
Specifically, young mothers would benefit from information about what breastfeeding feels like, what breastmilk looks like, and better information about combination feeding. While we echo Dykes et al.’s (2003) recommendation for increased informational and practical support for adolescent mothers, this support should be available through a variety of media, particularly social networking sites which young mothers relied on for health and breastfeeding information. Research has previously demonstrated the capacity for successful health education and promotion through social media (Korda and Itani, 2013) and Daly et al. (2016) found that specific pregnancy and post-natal support applications (in their case Baby Buddy) are particularly well-used by mothers under 20 and those in disadvantaged areas. Future research would benefit from focusing on particular gaps in adolescent mothers’ knowledge which may lead to early breastfeeding cessation to inform the content of this social media support. While this article goes some way to doing this, a longitudinal approach, which could capture adolescent mothers’ feeding experiences and decisions in ‘real time’, would help feed into longer-term improvements in breastfeeding information. Moreover, future research could usefully focus on how changing attitudes to breastfeeding affect and are affected by diverse groups of women and their cultural health capital.
In addition, we demonstrated that the healthcare practitioners offering information and support to adolescent mothers are central to breastfeeding practices. Young mothers’ often reported strained relationships with healthcare practitioners, which are not a result of age alone but a complex intersection of age, socio-economic status, and local norms about breastfeeding which can be understood through the framework of cultural health capital (see Shim, 2010). Cultural health capital provides a more holistic framework for understanding young mothers’ breastfeeding support experiences given it captures the intersections, overlaps, and co-production of diverse factors rather than foregrounding one particular variable, such as age. Young mothers’ low cultural health capital is most notably manifested as a limited capacity to communicate their wishes effectively, which can lead to a limited scope for active participation in their treatment, which in turn can be perceived as poor treatment (e.g. MacLeod and Weaver, 2002; Whitley and Kirmayer, 2008). Increasing cultural health capital may potentially increase rates of breastfeeding through women being better able to communicate with healthcare practitioners to overcome challenges. However, cultural health capital is structural, meaning it stems from the systematically rooted inequality and exclusion of particular groups, rather than being the result of individual behaviour or choices. As such, cultural health capital is not easily addressed by singular interventions and, moreover, women’s choice not to breastfeed needs to be given space and respected in practice.
Recommendations for health promotion practice
Given the above findings, health practitioners and services providers should take a holistic approach to breastfeeding support for adolescents focusing on young mothers’ wider life worlds (Condon et al., 2012) and being mindful of the cultural backgrounds which might lead to low cultural health capital. Specifically, health providers might recruit and train peer supporters or mentors who are/were themselves adolescent mothers, who understand its complexities, and will not add to the strains young mothers\already experience (Hunter et al., 2014). Previous research has demonstrated that peer support for breastfeeding is effective in increasing adolescent mothers’ exclusive breastfeeding duration (Di Meglio et al., 2010) and improving their breastfeeding experiences (Nesbitt et al., 2012). Matching service users with practitioners who have similar profiles and/or life experiences (in this case peer supporters) has been shown to be beneficial for healthcare relationships (e.g. Ahmed et al., 1991). These peer mentors would be best placed in advisory roles (e.g. answering ‘basic’ questions) which complement healthcare practitioners’ clinical focus and would not add additional time constraints to already over-stretched practitioners. Through these peer mentors, young women could be better empowered to actively participate in their maternity care.
Limitations
This study has a number of limitations. First, it did not collect data from healthcare practitioners themselves, which means that the factors underpinning the perceived strained relationships between themselves and young mothers, for example, the pressures of short consultation times, have not been fully explored.
Second, the data comprise retrospective verbal accounts from young mothers about their breastfeeding experiences. This kind of research carries the risk of participants misremembering as Linton and Melin (1982) demonstrated in the case of chronic pain. Future research would benefit from using real-time methods which, enabled by advances in technology, is a likely future direction for experiential social and behavioural research (Schwartz, 2007).
Third, all but one of the participants were white and all were native British or Irish, which gives a relatively homogeneous picture of adolescent mothers’ experiences. This also means that we have not explored the full capacity of cultural health capital for capturing intersecting marginalities such as ethnicity and migrant status. Future research would benefit from exploring more diverse breastfeeding support experiences.
Conclusion
This article used the framework offered by cultural health capital as a lens through to explore young mothers’ experiences of breastfeeding information and support. We have shown that while young mothers are well-informed about the benefits of breastfeeding, they lack basic information which may lead to early cessation. Moreover, young mothers’ reported poor relationships with healthcare practitioners which we argue results from intersections between age and socio-economic status, leading to low cultural health capital. Future research would benefit from engaging with the perceptions of healthcare practitioners and involving young, socio-economically deprived mothers in research on effective breastfeeding interventions.
Footnotes
Acknowledgements
We thank participants who shared their personal stories and experiences with us and the gatekeeper organisations who were instrumental in supporting the research. Thanks too to Rhona Beynon at Bristol University, who undertook some of the data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The initial research was funded by a Grant from Cancer Research UK (Grant Reference: C53270/A19689) and the follow-up project was funding by an Economic and Social Research Council Impact Acceleration Account Award provided by Durham University (no specific grant number given).