
Abstract
Objective:
This article reports on a qualitative evaluation of the Love Life, Smokefree Sports primary school pilot intervention. This 8-week programme used sports and physical activity sessions to convey Smokefree messages to 120 children aged 10 and 11 in two primary schools in Sheffield in 2018. The study aimed to understand children’s experiences of participating in the programme. Its objectives were to explore children’s recall of the health promotion messages associated with each of the learning sessions; explore children’s perceptions of the meaningfulness of those messages in the context of their everyday lives; and identify and understand any contextual factors that might impact upon children’s recall and/or the meaningfulness of the Smokefree messages.
Method:
Qualitative data were generated with 25 children through focus groups after the programme concluded. Data were analysed thematically using cross-sectional, categorical indexing.
Results:
Learning from the programme was particularly likely to be described as meaningful by children when they could interact with material and visual representations of complex ideas and when sessions involved strongly embodied experiences. However, children did not always find it easy to relate learning to their everyday lives and sometimes struggled to reconcile pre-existing, contextualised understandings with intervention messages. We mobilise the concept of critical health literacy as a theoretical lens through which to interpret these findings.
Conclusion:
Health education should be meaningful in the context of children’s everyday lives. Starting from the premise that children are active critical health literacy practitioners and working with them to design and evaluate health education initiatives can promote this.
Introduction
Currently estimated to result in around 7 million deaths a year (World Health Organization [WHO], 2018), tobacco smoking is a major risk factor for non-communicable diseases such as asthma, coronary heart disease (CHD), chronic obstructive pulmonary disease (COPD), type 2 diabetes, stroke and an array of cancers (Khani et al., 2018; Onor et al., 2017; US Department of Health and Human Services, 2014). Although around 20% of the world’s population are thought to smoke tobacco (WHO, 2018), recent decades have seen a general decline in the prevalence of tobacco smoking, particularly in higher income countries including Australia, Canada, New Zealand, the UK and the USA (Islami et al., 2015). Bans on tobacco advertising, legislative restrictions on smoking in public places, warning labels and smoking cessation services are all thought to have contributed to reduced numbers of people using tobacco products (Gravely et al., 2017).
Tobacco smoking typically begins prior to adulthood (Amos et al., 2009; US Department of Health and Human Services, 2014). Over 200,000 children in the UK (Hopkinson et al., 2014), and more than 1 million young people in the USA (Choi and Stommel, 2017) begin tobacco smoking each year. Across Europe, the prevalence of smoking initiation in younger adolescents is increasing (Marcon et al., 2018), and globally, between 82,000 and 99,000 young people start smoking every day (Schwab, 2011). Rates of tobacco smoking are consistently greater among people of lower socioeconomic position (SEP; Hiscock et al., 2012b; Loring, 2014). Those from disadvantaged backgrounds are more likely to try tobacco smoking and less likely to succeed in quitting (Hiscock et al., 2012a; Smith et al., 2018). Furthermore, exposure to secondhand smoke (SHS) is more frequently experienced by low SEP populations (Moore et al., 2012; Nazar et al., 2016) and linked to a greater likelihood of tobacco use by both children (Taylor-Robinson et al., 2017) and adolescents (Xi et al., 2016). Worryingly, those who start smoking early are also the least likely to quit (Khuder et al., 1999). Consequently, addressing tobacco smoking among young people is a global public health priority (Lando et al., 2010).
Tobacco-related interventions with young people have utilised motivational strategies, pharmacological therapy, physical activity and Internet and mobile technologies (Gabble et al., 2015) to promote smoking cessation (Fanshawe et al., 2017; Harvey and Chadi, 2016) and prevent smoking uptake (Carson et al., 2011). School-based programmes are increasingly popular (Thomas et al., 2013) and have been deemed particularly effective in comparison with interventions delivered in ‘medical clinics, family or other settings’ (Gabble et al., 2015: 10). In Europe, school-based interventions, such as the But I don’t smoke, Unplugged and Smokefree Class Competition programmes, have demonstrated varying degrees of effectiveness in preventing uptake of smoking among young people (National Institute for Health and Care Excellence [NICE], 2010).
The Love Life pilot intervention
The Love Life, Smokefree Sports programme is a UK-based preventive tobacco intervention, informed by work conducted with more than 30 primary schools in the North West of England between 2010 and 2013 (McGee et al., 2016; Trigwell et al., 2015). Delivered in primary schools over six physical education learning periods, the programme utilised sports, games and physical activities to convey a range of anti-smoking messages (Table 1). The term Smokefree is used to describe places where smoking is prohibited and people who do not smoke. This article reports on the delivery of the programme’s pilot phase which took place in two primary schools in Sheffield, UK, between March and July 2018. The programme was delivered by Zest, a community-based organisation in Sheffield. Zest runs a leisure centre, a library and health, work, youth and young people’s services for the community. It delivers the city-wide Children and Young People’s Stop Smoking Service, which includes a Smokefree Schools Programme. Three members of staff and two volunteers led the sessions, all had experience of working with primary-age children in a sports context and held sports coaching qualifications. A total of 120 children (50% boys and 50% girls) from two urban primary schools participated in the study. The schools were chosen as they were both feeder schools for secondary schools which had (1) previously engaged with the Smokefree Schools Programme, (2) were in areas of high smoking prevalence (and socioeconomic deprivation as measured by the Index of Multiple Deprivation [IMD] for Lower Layer Super Output Areas), and (3) represented a good geographic spread. Sessions were adjusted to fit around the time available within the school timetable. At one school, sessions were 30 minutes long with 26–28 pupils in each session (each session was delivered three times). At the other school, sessions were 1 hour long with 41 pupils in each session.
Aims and formats of the Love Life, Smokefree Sports programme sessions.
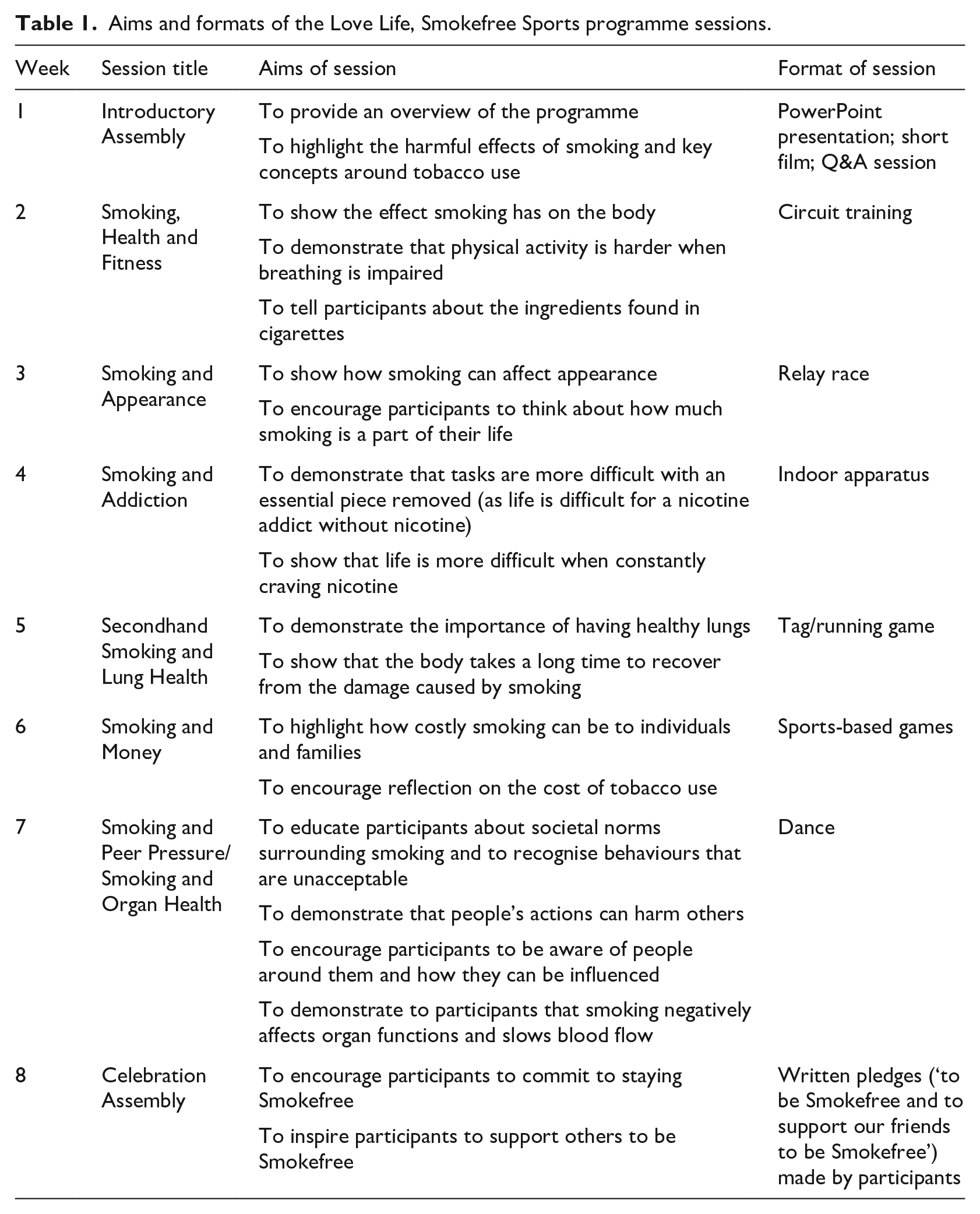
Like the original programme in the North West of England, the intervention design was guided by the socioecological model of health, the health belief model, the theory of planned behaviour and social cognitive learning (McGee et al., 2016; Trigwell et al., 2015) and the key themes addressed were broadly the same. Both interventions were delivered in areas of high deprivation, replaced regular physical education sessions (six in the Love Life and five in the original programme) and included a final celebration assembly and a Smokefree pledge. In this way, both the content and the dose of the two interventions were broadly similar. There were, however, a number of differences. First, the Love Life programme included an Introductory Assembly not present in the North West programme. This was deemed a useful way to provide general information to engage the children in the Smokefree message and introduce the programme team members. Second, unlike the original programme, the Love Life programme included sessions on Smoking and Appearance and Secondhand Smoking. This was informed by Zest’s experience of delivering Smokefree peer educator courses for secondary school-age children, in which these topics were included and well received. Third, while teachers and Smokefree Sports coaches delivered the original intervention, the Love Life programme was delivered solely by Smokefree Sports coaches. Offering to take the physical education sessions on teachers’ behalf was considered an important incentive for school participation. Finally, while the original intervention offered branded collateral for participating schools, engaged local sports stars and teams to help and provided a full training programme for teachers, these elements were not replicated in the Love Life intervention due to a more limited budget and capacity.
The study aimed to understand children’s experiences of participating in the Love Life, Smokefree primary school pilot intervention. Its objectives were to explore children’s recall of the health promotion messages that were associated with each of the learning sessions; explore children’s perceptions of the meaningfulness of those messages in the context of their everyday lives; and identify and understand any contextual factors that might impact upon children’s recall and/or the meaningfulness of the Smokefree messages. Our approach was informed by an understanding of children as active agents able to provide knowledgeable commentary on their own lives (Brady et al., 2015). We mobilise the concept of critical health literacy, defined as ‘the ability to assess the quality and relevance of information and advice to one’s own situation’ (Harris et al., 2015: 4), as an analytical framework to illuminate children’s interaction with the programme and implications for health education.
Evaluation method
Sample and recruitment
A total of 25 children (16 girls and 9 boys), aged 10 and 11, participated in focus groups 2 weeks after the final Smokefree session (approximately 8 weeks after their first encounter with the programme). Children from both primary schools, which had been the sites for the pilot intervention, took part in the study. Three focus groups were held in the first school and two in the second due to the differing class sizes and the number of participants in the programme in each school. On the request of the head teachers, it was agreed that classroom teachers would select pupils to participate in the focus groups.
Parents were sent an information letter outlining the study and the implications of their child’s involvement and an opt-out form to sign and return to school if they did not wish their child to participate. No parents opted their children out of participating. Following this, children were invited to participate in a focus group discussion. They were provided with child-friendly information letters and consent forms and the opportunity to ask questions before deciding if they wished to participate (Alderson and Morrow, 2011). Ethical approval for the study was granted by the University of Sheffield Ethics Committee.
Focus groups
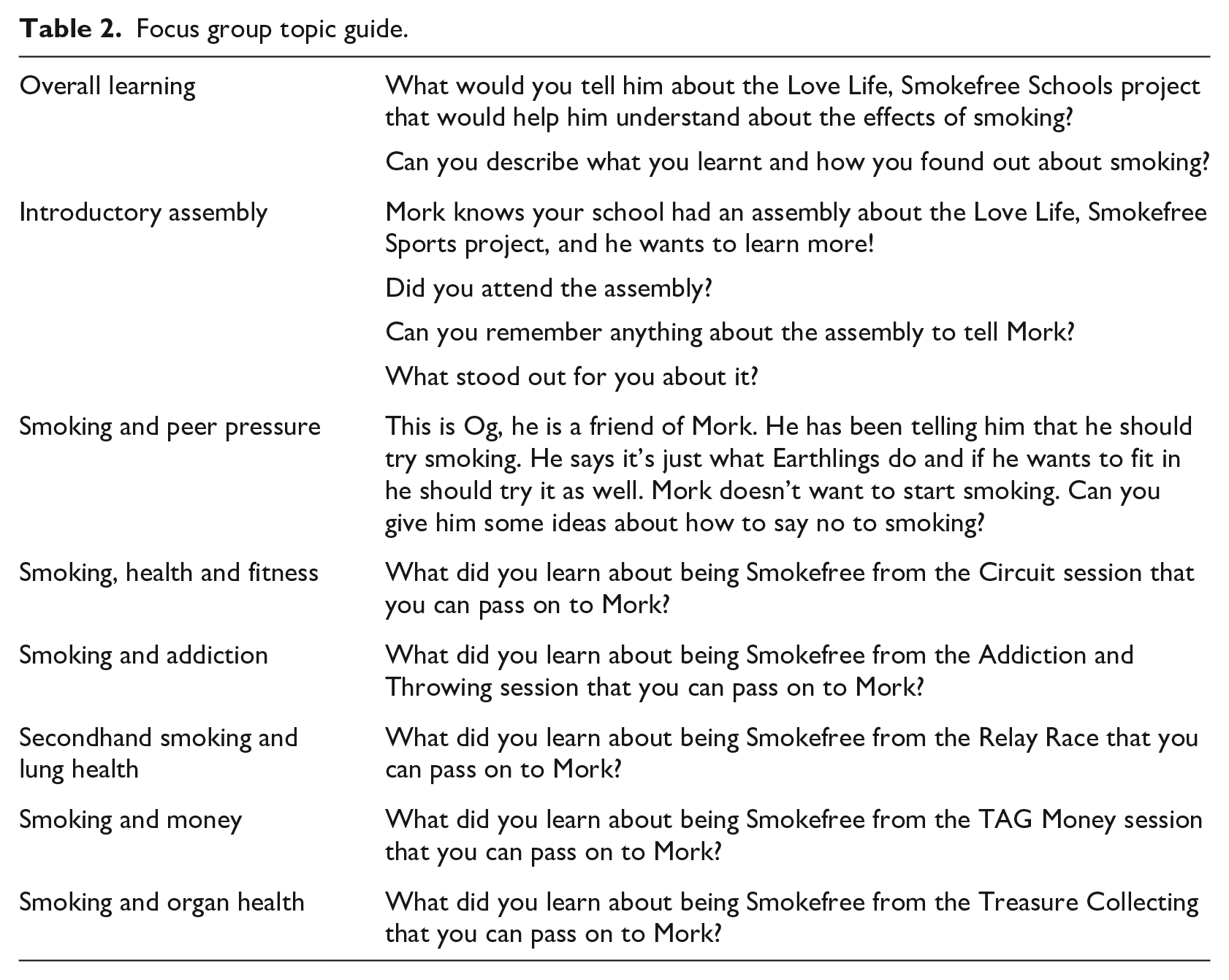
Each mixed-sex focus group comprised five participants and was facilitated by an intervention team member and a research team member. Discussions lasted approximately 30 minutes and took place in an art room, away from the main classroom. Focus groups were chosen with the aim of supporting the interaction of peers and with the intention of reducing the inevitable power differentials between adult researchers and child participants (Clark et al., 2014). Topic guides were developed jointly by university researchers and the intervention delivery team. Questions took the form of children explaining their learning to an alien (Mork) and his friends using flash cards (Table 2). This approach positions children as authoritative ‘knowers’ (James and James, 2004), encouraging them to articulate their understandings of the key messages conveyed during intervention sessions. The approach was, therefore, designed to access children’s meaning making and to foreground their own interpretations of the health promotion messages to which they had been exposed.
Focus group topic guide.
Analytical strategy
Focus groups were audio-recorded and transcribed verbatim. Pseudonyms were applied to minimise any opportunity for individual children to be identified. Data analysis followed the procedure outlined by Braun and Clarke (2006: 87): familiarisation with data, generation of initial codes, search for themes, review of themes, definition of themes and production of the report. Themes were generated as they helped to describe, illuminate and interpret the data (Vaismoradi et al., 2013: 403) adopting both an inductive and a deductive approach. There were some difficulties with the quality of the recorded data, and it was not always possible for the transcriber to identify a specific child within a conversation. This is noted in the data extracts as ‘Child’ or ‘Name?’.
Findings
Overall, children were very positive about their participation in the programme. They valued the intervention and felt that it had resulted in meaningful learning. However, they often did not recall the relationship between session activities and intervention messages. We highlight three key areas that lend insight into the meaningfulness of health education messages – effective representation of complex ideas, embodied learning and challenges to meaningfulness.
Utilising visual and material representations of complex ideas with children
Visual and material representations of complex ideas proved both popular with and meaningful for children. Children particularly enjoyed and readily recalled their learning from the presentation of a ‘tar jar’ in their school assembly:
It showed how much you put in your body . . .
It was in a year . . . and also . . .
[. . .]
It was like this gross thing that your slime comes out of when you put too much activator and trust me, it was disgusting. [Other voice interrupts/talking over]. It goes all over the place.
It’s 10 times worse than [. . .]
It were like a bonfire lollipop, but melted,
Thank you Tamsin.
Oh, and also we talked about those chemical that are inside it, like what people put into their body. And I didn’t know that there was arsenic in it.
Yeah, which is poison.
(Focus Group [FG] 2)
Another child noted,
I liked how they presented it. They didn’t make boring like, my God, there are over seven thousand chemicals in this, get on with your work. They made it interesting. That helped us understand it [. . .] They didn’t just do it all boring, like writing on a blackboard. They showed us the things, so that was interesting. (Child, FG1)
Following prompting, most children recalled this session clearly and could articulate the learning associated with it. Children spoke with enthusiasm about the knowledge that they had acquired about the harmful chemicals that could be inhaled through smoking. They described having known ‘a bit’ about the harmful properties of cigarette smoking prior to the intervention, which one child attributed to television coverage that had ‘showed me like the label on a cigarette that told me all the bits where everything is’ (FG2). However, they were intrigued and horrified by the information they had been given about toxins in cigarettes: ‘It has over seven thousand toxic chemicals’ (FG2), ‘rat poison and toilet cleaner and stuff’ (FG2), ‘arsenic’ (FG1) and ‘I don’t know what it’s called but there was this really addictive one’ (FG4).
Similarly, in the Smoking and Appearance session, simulated visual representations of an intervention team member before and after smoking (with yellow teeth, grey skin, dark circles under eyes, tooth loss, wrinkles and spots, etc.) as part of a running game were recalled in great detail and the children described this activity as fun:
I think this is how we went, so basically, we had loads of cards of (intervention team member) with an edited face of her if she did smoke and her face which she looks normal, yeah. And what would happen is we choose teams, and I think it’s the smoking team and the non-smoking team. The non-smoking team would go around and switch them around to the normal ones and then the smoking team would go around and try to switch them back to the smoking. (Crystal, FG3)
When discussing this activity, children from both schools articulated a clear understanding of some of the potential effects of smoking on appearance. Children were aware that ‘your appearance would change’ (FG2), faces might ‘start to wrinkle before’ (FG3), ‘your teeth can decay’ and ‘you can get yellow fingers’ (FG2).
Providing opportunities for embodied, experiential learning
Embodied, experiential learning opportunities also afforded powerful, meaningful frameworks for children’s learning when they helped to reinforce key intervention messages. Their discussions of the Smoking, Health and Fitness sessions, in which they were invited to experience for themselves the effects of smoking on the respiratory system, were particularly noteworthy:
Well, we had like these masks on and we did, like, I think it was for a minute, we did like every exercise and it showed us how, like you could feel if you were doing sports and if you were addicted to smoking.
Yes, definitely. Staci?
And how hard, if you were going to be doing sports, how hard it would be to be breathing.
(FG4, emphasis added)
Similarly, Crystal described both her enjoyment of the session and her appreciation of how the session promoted an experiential rather than merely intellectual understanding of the impact of smoking on the body:
I enjoyed the session, I learnt a lot [. . .] Because that session was like fun to test out how I, it actually feels because I always feel like what was, what does it actually feel like, because you can see people sometimes struggling. So like, how does it really feel? And it actually showed me how it feels and I don’t want to feel that feeling in my life. (Crystal, FG3, emphasis added)
However, in all the focus groups, when children discussed the relationship between smoking and fitness, this was generally articulated in relation to sport – and to people (themselves and/or others) whom they characterised as sporty or to elite sportsmanship – rather than children’s everyday lives or mundane play activities like walking, cycling or playing. Juliana, for example, noted that as a smoker, ‘I wouldn’t be able to do as much sports as I would be able to’ (FG4). Similarly, another girl related her learning to aspiring professional footballers: ‘[It’s] not good for you and [. . .] it can make stuff hard, say, if you’ve got someone, say, who wants to become a footballer, it’s going to make it harder for you because if you smoke it’s not easy’ (Child, FG3).
Furthermore, activities in which the embodied experiences were simply an appendage to rather than reinforcing the intervention message were not successful. The Smoking and Addiction session, for example, proved very difficult for children to recall, even when prompted by an intervention team member, who described what physical activities had been undertaken:
I can remember something with the ball, but I can’t remember if that’s the lesson.
Do you remember from watching it Austin?
I remember people batting the ball and then just running around that’s it. Around, like people going fast people going back, but I can’t remember the lesson.
(FG3)
Even with further prompting, the children appeared confused about the learning associated with this session: addiction was only occasionally referred to and did not seem to be clearly understood. Here then, in contrast to wearing the masks in the Smoking, Health and Fitness session, which afforded children the opportunity to experience the message themselves (physical activity is harder when breathing is impaired by smoking), the embodied activities in the Smoking and Addiction session did not help to reinforce the message that ‘life is more difficult when constantly craving nicotine’.
Relating learning to everyday life
Following the intervention, although children could articulate a number of key learning messages, they still had some reservations which suggest the need for ongoing reinforcement to enable them to think these messages through within the context of their everyday lives. Gemma’s discussion of peer pressure, for example, clearly highlighted the need for ongoing support. Despite describing the responses she had learned (‘you don’t need to smoke, you can just be yourself’ and ‘they think they are going to be the coolest people ever because they smoke but that’s not the point. It’s really bad for you’), Gemma was still left wondering how these clear-cut messages might play out in imagined potential future scenarios:
Do you have any questions about what’s going to happen now? Yes, Gemma?
If you smoke when you’re older and you like say, what’s the age to smoke again?
Legally, do you mean to buy cigarettes? When you are an adult?
Like I’m scared if somebody is going to like . . . like say if I’ve got a friend who does it, I feel that they are going to be like a bit disappointed that I’m not going to be doing it like them.
(FG3)
Gemma’s question in the focus group could highlight a lack of opportunity to ask questions and consider the potential gap between ideal strategies and the perceived realities of life in the intervention itself. In a similar vein, children considered ideas about the association between smoking and weight loss in the focus groups:
And it (smoking) gets you thinner. It gets you thinner though because instead of eating all you are doing is just lifting and smoking . . . Just going up-down, up-down . . . and you can’t taste much. (Ember, FG1)
Children struggled to accept the intervention team member’s response, ‘Well I think that thing about smoking making you thinner is a bit of a myth’, confronting as it did the received wisdom from their mothers or their perceptions about the impact of smoking on mothers’ weight: ‘When my mum smokes, she’s thin. And when she tries to stop, she gets a bit bigger, fatter. Yeah, ‘cause it does make you lose weight’ (Zahra, FG1).
Discussion about their mothers’ smoking also reflected the long-standing understanding that women’s smoking can be an important coping strategy in the face of the multiple demands placed on them (Graham, 1987): ‘She’s (her mother) got an electric one and she only smokes once per week, if she really needs to. Me and my sister, we make her really, really mad. That’s when she needs it’ (Zahra, FG1). The format of the intervention, therefore, left apparently little room for children to raise issues that mattered to them, which had arisen through their lived experiences.
There was also some confusion evident when children felt that the outcome of the activities undertaken in the session did not make sense. Although in the session on Smoking and Appearance an additional disadvantage was imposed upon one team to symbolise the effects of smoking (making them hop rather than run), this team still triumphed in the challenge. Children were understandably annoyed about what they perceived to be a nonsensical final outcome:
Why did that team, why did we give that team hopping? Why did we say that this team has to hop?
Because you could see the advantage that you can see when people do not smoke.
So, we gave, one team was the smoking team; one team was the non-smoking team. And the smoking team, we said, oh yeah, you’ve got to do the hopping. So, we gave you a disadvantage.
We still won, didn’t we?
But you had a disadvantage.
Yes, we all went mad about it.
(FG1)
Similarly, in the session on Smoking and Money, there was confusion when the outcome of the team game was not as expected. Children were not always clear that collecting cigarettes, which they had learned were expensive, did not augment the value of the (symbolic) possessions they were accruing in the game. They also pointed out that a team that was required to crawl during one activity, to represent the disadvantage of being smokers, had nevertheless still triumphed over their opponents.
Discussion
Learning from the Smokefree programme was particularly likely to be described as meaningful by children when they were able to interact with material and visual representations of complex ideas and when sessions were associated with strongly embodied experiences which emphasised key intervention messages. However, children did not always find it easy to relate their learning to their everyday lives and sometimes struggled to reconcile pre-existing, contextualised understandings with intervention messages.
Children’s enthusiasm about the information they had gleaned through material and visual representations coheres with previous research emphasising the effectiveness of pictures in increasing children’s comprehension and recall of health communications, particularly when they promote an emotional response (Houts et al., 2006). Children’s enjoyment of and learning from the most interactive elements of the Smokefree programme also echo findings from McGee et al.’s (2016) Smokefree evaluation and supports the UK’s National Institute for Health and Clinical Excellence (NICE) recommendations that smoking prevention interventions geared towards children should be interactive and participatory (NICE, 2008). Similarly, the fact that children enjoyed and valued the strongly embodied learning opportunities coheres with other studies which emphasise the importance of somatic, bodily experiences in developing health-relevant understandings (Fairbrother et al., 2016). It also offers further evidence of the opportunities afforded by sport as an educational platform for smoking prevention (Centers for Disease Control and Prevention, 2011; The Community Connector, n.d.; Trigwell et al., 2015; WHO, n.d.). However, an important finding from our study, and one not reported elsewhere, was that children in all the focus groups articulated the impact of smoking on fitness in relation to sporty people or elite sportspeople.
This important finding demonstrates a key limitation of the applicability of the message for those who do not consider themselves ‘sporty’ or potential sportspeople. It highlights a need to open up for discussion or to create activities demonstrating the negative impact of smoking on everyday physical activities like walking to school or playing out with friends. Furthermore, our study demonstrates that not all embodied activities promoted meaningful learning. In contrast to activities which mirrored the intervention message, those in which the embodied experience proved tangential to the message were unhelpful. An additional challenge, and one also identified in McGee et al.’s (2016) study, was that despite their evident learning about the health impact of smoking, some children still thought that they may smoke in the future due to stress or social acceptability though the majority of children stated that participation in the Smokefree Sports had made them more determined not to smoke in the future. However, while McGee et al. (2016) argue that Smokefree campaigns can help to ‘dispel myths’ and ‘facilitate children in making a rational and logical decision not to smoke’ (p. 12), we would argue that through acknowledging that they may smoke in the future, children in our study demonstrate a nuanced understanding of the myriad influences on health behaviour including stress and social norms (Graham, 1987). They realise that behaviours are not solely governed by rational, logical decision-making processes based on understanding health information.
As Harris et al. (2015) argue, a health education model that emphasises only information giving and understanding (functional health literacy) ‘decontextualizes information – not allowing for barriers and facilitators to the use of information that may be beyond a person’s control’ (p. 4). The authors contrast this with critical health literacy which they define as ‘the ability to assess the quality and relevance of information and advice to one’s own situation’ (p. 4). This helps to move beyond the giving and receiving of information towards a more nuanced picture. However, building upon the work by Fairbrother et al. (2016), Samerski (2019) critiques a conceptualisation of critical health literacy which often ‘still takes an individualistic approach depicting citizens as cognitive agents instead of as emotional, social and embodied beings’ (p. 2). Samerski (2019) further argues that health literacy ‘depends on concrete situations, the resources at hand and, in many cases, is prompted and shaped by personal experience and somatic (bodily) knowledge’ (p. 2). Such a conceptualisation of critical health literacy coheres closely with children’s interaction with the Smokefree programme. The data clearly demonstrate that children assemble their understandings gleaned through visual and material representations, the experiential elements of the programme and their contextualised understandings based on past and envisaged experiences (Bhagat et al., 2018; Im and Swan, 2019). In this way, they demonstrate their active engagement in critical health literacy practices.
Limitations
No process evaluation of the pilot project was possible and discussion with children occurred 8 weeks after the initiation of the intervention meaning recall was often difficult. Although children generally described the sessions as fun and informative, it is important to note that a member of the intervention team was present during the focus groups and children may have felt compelled to give a ‘positive take’ on their experience (Punch, 2002). However, the fact that children articulated questions with which they were still grappling after the intervention and also their frustration, for example, when games did not have what they perceived to be the ‘right’ outcome, suggests that children felt able to express their thoughts during the focus groups. It is also possible that recruitment bias influenced the data generated and therefore the interpretations that can be derived. Often in schools those children who are most eloquent and/or the ‘best behaved’ are put forward by teachers as appropriate informants (Heath et al., 2007).
Implications
With respect to the Love Life, Smokefree Sports intervention, evaluation findings have a number of specific implications. First, there may be value in focusing the intervention on those messages that are most clear to children, notably, smoking can make breathing difficult and can therefore impede children’s ability to participate in physical activities; smoking is expensive; and smoking can have a negative impact upon individuals’ appearances. Second, health promotion messages may have greater resonance for children if they relate more clearly to activities of daily life (such as walking, playing and cycling) rather than focusing on children’s ability to participate in ‘sport’. Finally, our study also suggests that interventions such as Smokefree Sports need to provide opportunities for children’s additional and particular concerns to be integrated into, and considered within, the programme’s scope (such as parental smoking).
This study also raises important implications for research, practice and policy in relation to child health education more broadly. In relation to research, it has contributed to the dearth of literature exploring critical health literacy (Harris et al., 2015), particularly in relation to children (Fairbrother et al., 2016; Velardo and Drummond, 2017). It has underscored that children are active health literacy practitioners, they strive to make sense of their learning for their everyday lives and they welcome the opportunity to share their contextualised understandings in order to make links. The area is ripe for further research.
In terms of practice, the study has highlighted the importance of understanding children’s perspectives of health education interventions. It has shown the importance of promoting opportunities for children to critique, question and make links to personal experience and familial, contextualised understandings (Bröder et al., 2020). Such an approach aligns with a community empowerment model which seeks to ‘encourage dialogue and active engagement among participants’ through discussion and participatory activities (Im and Swan, 2019: 40). This helps to go some way towards acknowledging and working with rather than negating the complexities and nuances of everyday life, where neat health education messages may not always sit easily. Involving children at the early stage in the intervention development process can help to ensure that their views are mobilised in the design of the intervention (Bhagat et al., 2018; Trigwell et al., 2015). This could help sensitise the intervention team to salient issues for children with the aim of promoting meaningful opportunities for learning and discussion of learning. However, this requires significant policy investment to facilitate longer lead in times for health education interventions to maximise children’s involvement at an early stage.
Conclusion
This study has provided important insights for smoking prevention programmes and health education geared towards children more broadly. It has demonstrated that providing opportunities to interact with visual and material representations of complex ideas and creating strongly embodied experiences which emphasise key messages can promote meaningful learning for children. Furthermore, children should be encouraged to draw upon, and relate learning to, their pre-existing, contextualised understandings. Affording children opportunities to engage in critical health literacy is paramount for meaningful health education. Neglecting to do so risks inadvertently exacerbating inequalities in health since children for whom key intervention messages may be the most difficult to reconcile with their everyday experiences may struggle most to take them on board.
Footnotes
Acknowledgements
The authors acknowledge the contribution of all pupils who participated in the study. They would also like to thank Lou Wright, Megan Ohri, Megan Drury and Stephanie Dunscombe for their role in designing and facilitating the focus groups.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.