
Abstract
Background:
The broad nature of young people’s development is internationally acknowledged, which includes physical, mental, spiritual, moral and social elements. In England, schools have a legal obligation to promote spiritual, moral, social and cultural (SMSC) development. It has been suggested that personal, social, health and economic (PSHE) education, a broad form of school-based health education, may contribute to building SMSC development in young people.
Objective:
To examine the association between PSHE education in schools and outcomes of an SMSC nature.
Method:
The study drew on data collected as part of the 2014 World Health Organization Health Behaviour in School-aged Children (HBSC) study for England. Data were collected from young people aged 11, 13 and 15 years, using anonymous self-completed surveys administered during school lessons. The analysis drew on responses from 3,731 young people. Multilevel modelling was used to examine the association between PSHE education and variables of an SMSC nature, while controlling for demographic variables.
Results:
Overall, the majority of young people who reported receiving PSHE education were positive about the benefits of this school-based health education. Positive perceptions of PSHE education were significantly associated with increased spirituality among young people, reduced engagement in both fighting and bullying perpetration and increased general self-efficacy.
Conclusion:
This paper highlights the important role that health education in a school context may have for young people’s broader development, and contributes to the national evidence base advocating for compulsory PSHE education in schools.
Introduction
The notion of health, well-being and the development of young people is broad and comprehensive, with the constitution of the World Health Organization (WHO; 1946) acknowledging the importance of social well-being in regard to health. Furthermore, Articles 27 and 32 of The Convention on the Rights of The Child (UN General Assembly, 1989) recognise the significance of young people’s physical, mental, spiritual, moral and social development.
In England, schools have a legal responsibility to contribute to this broader sense of development. It has featured in legislation dating back to the Education Act 1944, which described ‘the spiritual, moral, mental, and physical development of the community’; it was the Education (Schools) Act 1992 which adopted the widely accepted expression ‘spiritual, moral, social and cultural development’, sometimes shortened to SMSC. The importance of SMSC development has since been reiterated in the Education Act 2002; furthermore, schools in England are currently assessed on how effectively they promote SMSC by the Office for Standards in Education Services (Ofsted).
There are many overlaps between the different aspects of SMSC development. Eaude (2008) highlights the links between moral and social development in particular, describing how an individual’s moral actions are intrinsic to their social interactions. It has been widely acknowledged that defining SMSC development is complex (White, 1994). However, definitions have been proposed from varying sources, including government agencies, academics and practitioners to facilitate the integration and evaluation of SMSC in schools (Bigger, 1999; Eaude, 2008; Ofsted, 2004, 2017).
The concept of spirituality has been noted in particular ‘for its intangibility’ (Adams et al., 2015: 201) and abstract nature (Weathers et al., 2016). Spirituality can be thought of as the exploration and reflection of beliefs (Brown, 1998; Ofsted, 2017), building relationships and connections (Benson et al., 2003; Michaelson et al., 2016; Weathers et al., 2016), finding meaning and purpose (Benson et al., 2003; Ofsted, 2004) and developing a sense of identity (Brown, 1998; Ofsted, 2004). A framework has been proposed to support the conceptualisation of spirituality in which it is thought to span four domains: to oneself, to others, to the environment and to the transcendent (Fisher, 2011; Michaelson et al., 2016). Spirituality moves beyond religiosity, particularly important in the diverse context of schools; nonetheless, a person’s religion may foster spiritual development (King et al., 2014; Lepherd, 2015). Overall, spirituality has been conceptualised and demonstrated to be a health asset for young people, ‘a “developmental engine” that works by fostering the search for connectedness, meaning and purpose’ (Brooks et al., 2018: 387).
At the basic level, moral development comprises recognising the difference between right and wrong, which should be reflected in young people’s behaviour (Ofsted, 2017). However, moral development is more than simply following rules; it also entails schooling the young person to make and analyse moral judgements, and gain an understanding and awareness of different views (Eaude, 2008; Ofsted, 2004).
In social development, young people are taught the ability to successfully engage with others – both in the school environment and in the broader societal context (Ofsted, 2004, 2017). Social development inculcates in young people the skills to navigate relationships, which include listening, understanding, giving respect, collaborative working and conflict resolution (Brown, 1998).
A young person’s cultural development encompasses both understanding and appreciating their own and other cultures (Ofsted, 2017). Cultural development fosters respect and open-mindedness, and challenges prejudice and discrimination (Brown, 1998). Bigger (1999) highlights the importance of cultural development for young people today, who live and attend schools in multicultural societies and are exposed to international news on a daily basis.
The SMSC development of young people is thought to be pivotal to their future and often emphasises their relationship with the community and society more broadly. For instance, King et al. (2014) suggest that spirituality contributes to young people’s social identity and enables ‘them to matter to self, family, and society’ (p. 189), while Brown (1998) suggests it provides skills ‘needed to cope with life at home, school and in the community’ (p. 162). Furthermore, cross-cultural evidence demonstrates a link between spirituality and young people’s health and well-being (Brooks et al., 2018; Eaude, 2009; Michaelson et al., 2016). It has also been suggested that a positive SMSC development may promote learning and increased attainment at school (Eaude, 2008; National Curriculum Council, 1993), supported in part by guidance which demonstrates a link between pupils’ emotional and social well-being and attainment (Brooks, 2014).
The development of SMSC is broad and extends beyond the bounds of the national curriculum, hence it can be integrated in schools in a number of ways. Eaude (2008) describes the wider environment as including the school ethos, classroom displays celebrating diversity, and quiet areas for reflection as well as collective worship. A number of core subjects have recognisable links with SMSC, including religious education and philosophy, while languages and art allow exploration of different cultures and beliefs. In England, Ofsted (2004, 2013) and The PSHE Association (2018) recognise the role that personal, social, health and economic (PSHE) education can play in promoting SMSC development.
PSHE is a comprehensive form of health education delivered at school which is thought to prepare young people ‘for life and work in this changing world, helping to keep pupils safe, healthy and boosting their life chances’ (PSHE Association, 2017: 3). The school environment has been acknowledged as a key setting for health education (Langford et al., 2014). Traditionally, health education in schools often focused on risk behaviours and behaviour change but more recent programmes, such as PSHE, highlight the ways to maintain and promote health (Bruselius-Jensen et al., 2017). While many schools provide PSHE education, the position of PSHE education is hotly contested, and at the time of publication, PSHE education was non-statutory for state schools in England. However, while the provision of PSHE itself is not compulsory, a number of topics often taught in PSHE education lessons are; for example, the National Curriculum states that sex and relationships education and drug education are statutory requirements in secondary schools (Department for Education, 2014).1
Evidence suggests that PSHE education, or similar school-based health education, may be linked with improved health and well-being and educational attainment (Department for Education, 2015). A Cochrane review of the WHO Health Promoting Schools framework, in which health education such as PSHE is at its core, has identified associations with body mass index (BMI) reduction, increased physical activity, increased fruit and vegetable consumption, decreased cigarette use and reduced reports of bullying (Langford et al., 2014). Meta-analyses of education programmes related to social, emotional and behavioural skills (Durlak et al., 2011; Sklad et al., 2012) identified positive effects including improved social skills, reduced anti-social behaviours and increased well-being. In addition, programmes delivered school-wide, as is PSHE education, have been shown to be more effective than interventions targeted at a selective group of at-risk young people (Farahmand et al., 2011).
The Department of Education (2015) highlights the potential benefit of PSHE education on educational outcomes: ‘A virtuous circle can be achieved, whereby pupils with better health and well-being can achieve better academically, which in turn leads to greater success’. (p. 3). A longitudinal analysis confirmed a positive association between higher levels of emotional, behavioural, social and school well-being and academic achievement (Gutman and Vorhaus, 2012).
Evidence indicates that health education, such as PSHE, may have positive impacts on health, well-being and school attainment (Durlak et al., 2011; Murray et al., 2007; Sklad et al., 2012); furthermore, programmes related to social and emotional skills have proven successful. After undertaking a literature review, however, we identified no studies that examined the association between school-based health education and SMSC development.
This paper, therefore, will contribute to the current evidence base surrounding health education in school, and PSHE education more specifically. Consistent with suggestions from Ofsted (Ofsted, 2004, 2013), the analysis will explore whether PSHE lessons are associated with outcomes of an SMSC nature while controlling for demographic variables, in order to identify whether health education is associated with SMSC development. Rather than compare those who received PSHE education with those who did not, this paper examines young people who rated their PSHE provision positively and indicated that the lessons had an impact against those who rated PSHE education poorly.
Method
Participants and procedure
This study draws on data collected as part of the 2014 Health Behaviour in School-aged Children (HBSC) study conducted in England. HBSC is an international survey-based study, collecting data on the health and well-being, health behaviours and social context of young people from across Europe and North America (Inchley et al., 2016). Data are gathered through anonymous, self-completed questionnaires administered during school lessons. At present, 47 countries are involved in the HBSC study, with national research teams running the study in each participating country.
The sample frame for the HBSC study is young people attending school aged 11, 13 and 15 years of age. Full details of the sampling technique can be found in the HBSC international protocol (Currie et al., 2014). The sample in England is further stratified by region and school type, ensuring a large representative sample of young people from across independent and state schools. In total, 5,335 young people took part in the 2014 HBSC study in England (see Brooks et al. [2015] for a detailed description of the sample characteristics). This study draws on data from 3,731 young people, who responded to questions about their PSHE education at school.
The 2014 HBSC study in England received ethical approval from the University of Hertfordshire Health and Human Sciences Ethics Committee with Delegated Authority (HSK/SF/UH/00007). Permission was initially sought from schools, after which letters were sent to both students and parents/guardians with an opt-out form for those who did not wish to participate. Immediately prior to students completing the survey, it was reiterated that their involvement was voluntary and they could withdraw from the study. For further details see Brooks et al. (2015).
Measures
The value of PSHE education
Young people’s perception of the effectiveness of PSHE education on their health-related behaviours was assessed through four items: (1) PSHE classes have improved my skills and abilities to care for other people’s health; (2) PSHE classes have taught me to consider the importance of health in society more broadly; (3) PSHE classes have taught me to think about the advantages and disadvantages of different health behaviours (e.g. physical activity, diet); and (4) PSHE classes have improved my skills and abilities to care for my own health.
Young people rated each item on a four-point Likert-type scale, ranging from ‘strongly agree’ to ‘strongly disagree’. A factor analysis of these variables based on the non-parametric Spearman’s correlation matrix revealed that a one-factor solution could account for 77% of the variation in the variables with near-equal weights for the four questions. This implies that using an equally weighted average of the four PSHE items would provide an appropriate overall measure of the value of PSHE education. The Cronbach’s alpha for this scale was 0.913.
The following measures were selected from the 2014 HBSC survey as being relevant to SMSC development.
Spirituality
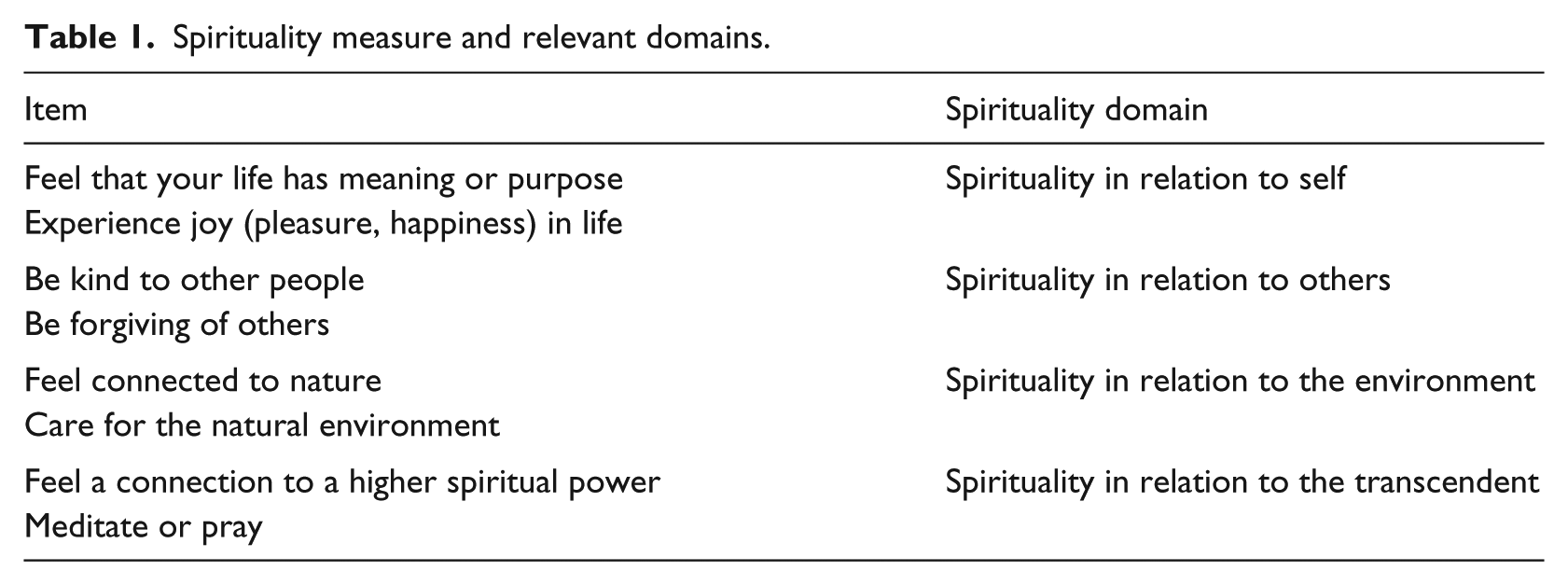
Using a measure adapted from Fisher’s Spiritual Wellbeing scale (Gomez and Fisher, 2003), spirituality was assessed via eight items with young people rating them on a scale of 1–5, with only the extremities labelled as ‘not at all important’ and ‘very important’ (Michaelson et al., 2016). In line with Michaelson et al. (2016), factor analysis revealed that a four-factor solution was appropriate, accounting for 86% of the variation. Consequently, four domains of spirituality were included in the analysis (Table 1). For each domain, an average of two questions was created, leading to a value between 1 and 5. In accordance with Michaelson et al. (2016), spirituality scores were categorised as ‘not important’ (scores of 2 or below), ‘somewhat important’ (scores above 2 and below 4) and ‘important’ (scores of 4 and above).
Spirituality measure and relevant domains.
General self-efficacy
The general self-efficacy is measured via the General Self-Efficacy Scale (Schwarzer and Jerusalem, 1995), made up of 10 items including ‘I can always manage to solve difficult problems if I try hard enough’ and ‘I can remain calm when facing difficulties because I can rely on my coping abilities’. Responses ranged from ‘Not at all true’ (scoring 1), ‘Hardly true’ (scoring 2), ‘Moderately true’ (scoring 3) to ‘Absolutely true’ (scoring 4). An average score is calculated subject to a minimum of seven items having answers.
Bullying perpetration
The HBSC study draws on questions from the Revised Olweus Bully/Victim Questionnaire (Olweus, 1996). Respondents were asked, ‘How often have you taken part in bullying another student(s) at school in the past couple of months?’ with response options varying from ‘I have not bullied another student at school in the past couple of months’ to ‘several times a week’.
Fighting
Respondents were asked, ‘During the past 12 months, how many times were you in a physical fight?’ Responses ranged from ‘I have not been in a physical fight in the past 12 months’ to ‘4 times or more’.
Demographic variables
The model controlled for the effect of demographic variables, including gender, age, ethnicity and family affluence (Currie et al., 2008).
Statistical analysis
The data are hierarchical in nature as they were collected from pupils grouped into classes and then into schools, and hence multilevel modelling was employed. The modelling accounted for weights in the dataset that allowed for minor deviations between the sample and population characteristics. A multilevel proportional odds model was fitted for bullying perpetration; however, the four spirituality domains and fighting violated the proportional odds assumption and hence separate binary logistic multilevel models were employed. A multilevel model for continuous outcomes was fitted for general self-efficacy.
As the effect of PSHE education is of prime importance, its main effect was retained in the models irrespective of the actual size of its effect. Likewise, demographic variables were retained to control for their effects. Interactions were considered, but to avoid the addition of spurious terms they were only included if the associated p value was less than 0.1%, the Akaike information criterion (AIC) improved by at least 10 and the estimation process yielded reasonable results. The same criteria were applied when considering the inclusion of random slopes.
The binary logistic and continuous multilevel models were analysed using the lme4 package (version 1.1-13) in R (version 3.4.1) via RStudio (version 1.0.143). The ordinal package (version 2015.6-28) in the same versions of R and RStudio were used to fit the proportional odds multilevel model.
Results
Descriptive analysis
Overall, the respondents were positive about the impact of PSHE education (Table 2). The four items were combined into an overall score assessing the value of PSHE education, which resulted in a mean score of 2.151 (standard deviation [SD]: 0.709). Of the 5,335 young people who took part in the study, 3,731 gave valid answers to all the four items assessing PSHE. The missing responses were examined in further detail; all schools had missing and non-missing data, with no obvious indication that the students with missing data differed from those with non-missing data.
Descriptive statistics for measures of PSHE education.
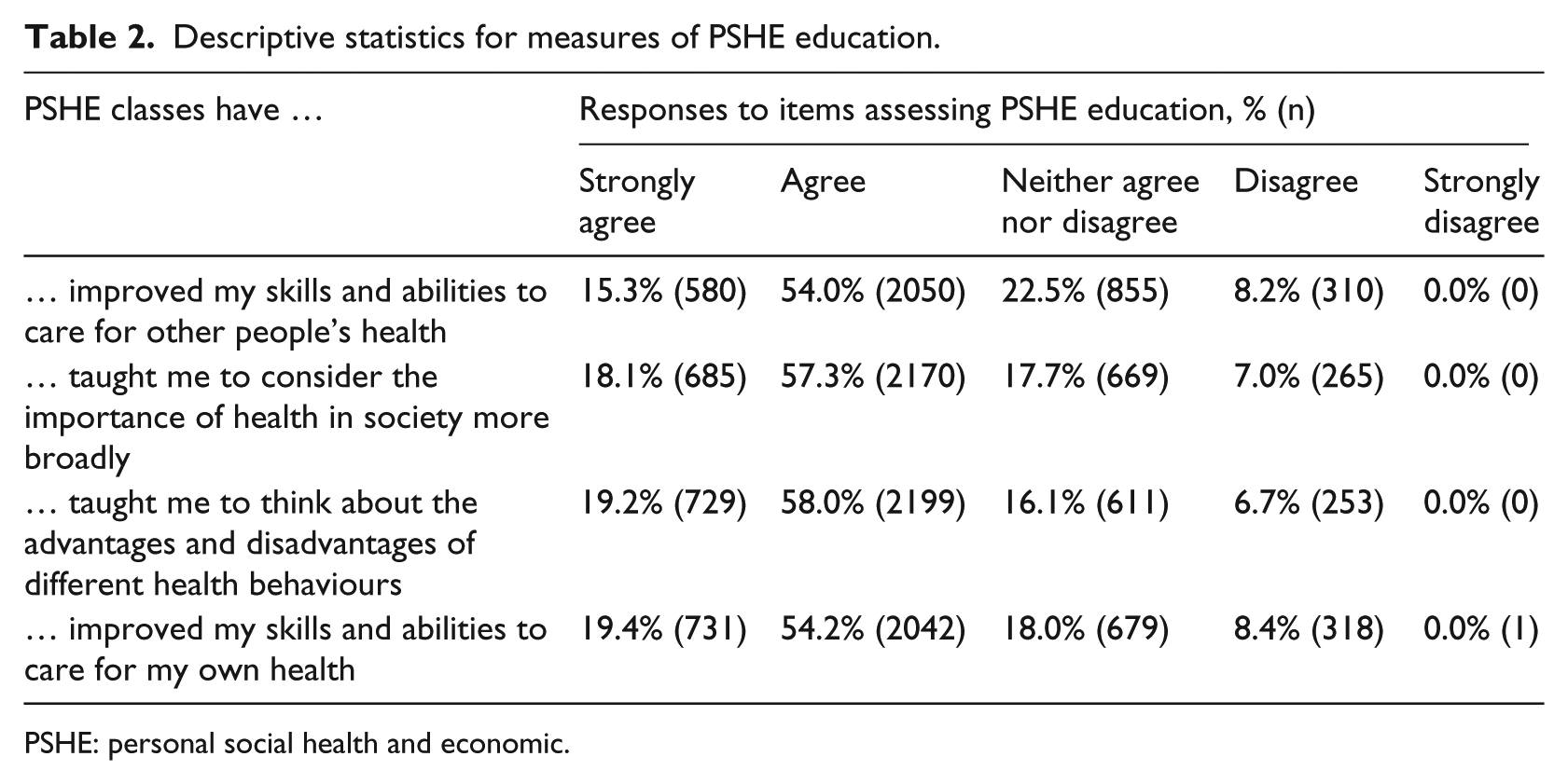
PSHE: personal social health and economic.
Statistical models
The purpose of the statistical model was to illustrate the relationship between PSHE education and measures of SMSC development while controlling for demographic variables. As such, the results section focuses on the association between PSHE education and SMSC variables. Supplementary material (online only) contains data examining the association between SMSC variables and demographic factors. The results report the effect on the outcome in question, which is associated with PSHE education improving by 1 SD. This can be conceptualised as a moderate positive change in PSHE education.
Spirituality
PSHE education was significantly associated with all four domains of spirituality (Table 3). An improvement in the score for PSHE education by 1 SD significantly increased the odds of being in the ‘important’ category for all four aspects, with increases varying from 35% for relation to self to 59% for relation to environment. Furthermore, the domains related to the environment and to the transcendent also noted increased odds of being in the combined ‘somewhat important’ or ‘important’ categories of 49% and 47%, respectively.
The effect of PSHE education improving by one SD on the four spirituality domains, including relevant OR, 95% CI and p values.
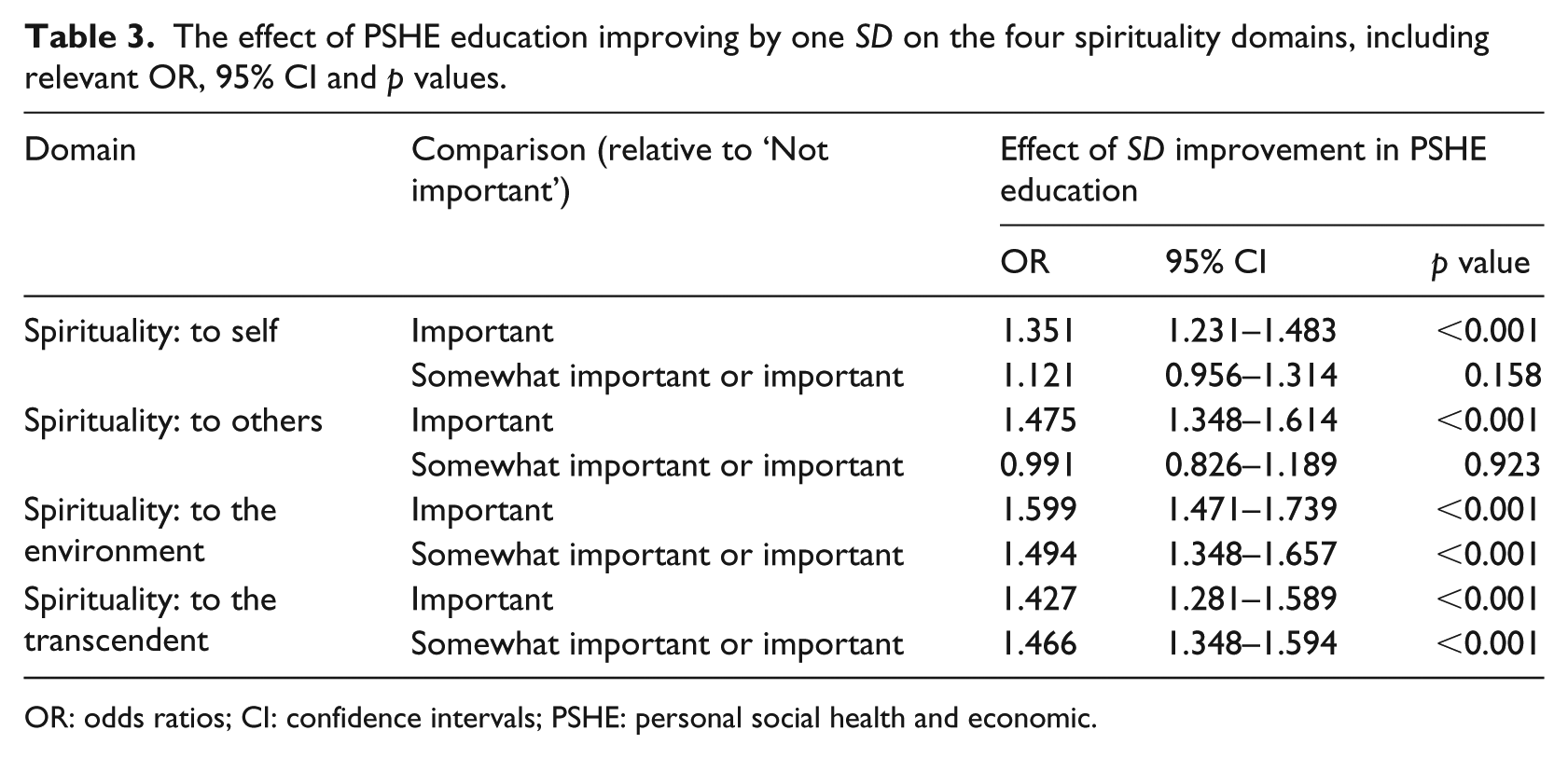
OR: odds ratios; CI: confidence intervals; PSHE: personal social health and economic.
Bullying perpetration
The score assigned to PSHE education was significantly associated with bullying perpetration. The response options vary from not bullying another student in the past couple of months to bullying perpetration several times a week. As the score for PSHE education improves by 1 SD the odds of being in a more frequent category for bullying others reduces, becoming 86% of what they were previously (OR 0.857, 95% confidence interval (CI) [0.779–0.942), p = 0.001]).
Fighting
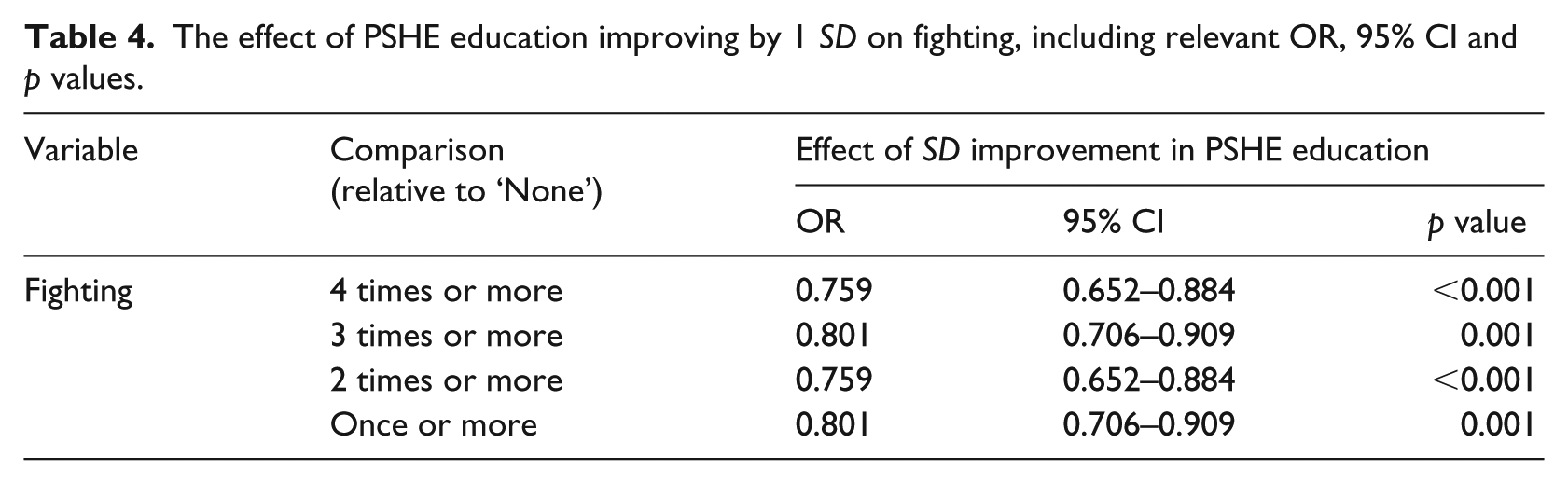
The measure of PSHE education was significantly associated with fighting at school. As the PSHE score improves by 1 SD the odds of reporting being in a fight reduce by 76% for being in fights four or more times to 80% for three times or more (Table 4).
The effect of PSHE education improving by 1 SD on fighting, including relevant OR, 95% CI and p values.
General self-efficacy
In the HBSC survey, a mean general self-efficacy score of 3.03 (SD: 0.508) was identified. If PSHE education improved by 1 SD, the general self-efficacy score increased significantly by 0.082 (95% CI [0.059, 0.104], p < 0.001); this equates to a fairly small increase of 17% of an SD. When modelling general self-efficacy, significant random slopes at both levels 2 and 3 were established. Consequently, the effect varies between classes/schools with estimates ranging from values not significantly different from 0 to an increase of 24.9 (50% of an SD).
Discussion
Health education in a school context may play a fundamental role in promoting the SMSC development of young people. This study drew on a large, representative sample of 11–15-year-olds in England, identifying associations between health education and variables of an SMSC nature. According to our findings, positive perceptions of PSHE education were significantly associated with young people’s spirituality, lesser engagement in fighting/bullying behaviours and increased self-efficacy.
Spirituality is a broad, multifaceted concept, and the measure utilised in this study encompasses four domains of spirituality in line with current conceptual frameworks (Fisher, 2011; Michaelson et al., 2016). Young people who reported benefitting from PSHE education were more likely to identify with all four domains of spirituality. Of interest, the strongest association was identified for spirituality in relation to the environment. The proportions of young people that indicate the environment domain is important has been shown to decline internationally with age among both boys and girls (Michaelson et al., 2016); this study highlights the broader role PSHE education may play in helping young people form beliefs about the wider community and the natural world.
Bullying perpetration and fighting span SMSC, touching on young people’s spiritual relationship with others, moral development, social skills and cultural tolerance, with indications that higher levels of spirituality are linked to decreases in victimisation (Dutkova et al., 2017). PSHE education was significantly associated with lower levels of self-reported bullying perpetration and fighting. These findings coincide with those of the Cochrane review, which found reductions in bullying victimisation associated with the WHO Health Promoting Schools framework (Langford et al., 2014), as well as international meta-analyses, which identified decreases in anti-social behaviour following social, emotional and behavioural education programmes (Durlak et al., 2011; Sklad et al., 2012).
General self-efficacy can be thought of as contributing towards a positive social skill, and is the ‘belief in one’s competence to cope with a broad range of stressful or challenging demands’ (Luszczynska et al., 2005b: 439). Respondents who reported PSHE was beneficial were more likely to have higher levels of self-efficacy. Considering the positive associations demonstrated cross-culturally between general self-efficacy and a number of constructs, such as improved self-esteem, optimism and academic success (Luszczynska et al., 2005a), this positions school-based health education, like PSHE, as an important and effective intervention. Self-efficacy is believed to develop via social learning processes like modelling and social persuasion (Bandura, 2012), and health education may provide an environment for these to be carried out.
Developing SMSC skills may have positive implications on young peoples’ health and well-being, educational attainment and future life chances. PSHE education (or PSHE-type interventions) has been associated with attainment at school (Barnard et al., 2017). It has been suggested that these positive results operate via the mechanisms of primary outcomes associated with PSHE, such as better emotional health, reductions in bullying and reduced involvement in risk behaviours such as tobacco and alcohol use. Thus, PSHE education leads to greater pro-social behaviour, increased self-esteem and confidence and greater care for the self and others – outcomes that could be considered as mapping directly onto SMSC. Furthermore, The Collaborative for Academic, Social, and Emotional Learning (CASEL, 2018) has stressed the importance of social and emotional learning (SEL) for the ability to set and achieve goals and to make responsible decisions; skills that would undoubtedly enhance learning, and resonate with the general self-efficacy trait identified in this study. Barnard et al. (2017) also suggest that PSHE lessons may ‘create an environment where students feel able to take cognitive risks’, which they argue would lead to enhanced learning.
The present findings contribute to the international evidence base pointing towards the positive implications of health education at school, with existing links found between health education and physical health, emotional well-being, health behaviours and risk behaviours (Durlak et al., 2011; Langford et al., 2014; Sklad et al., 2012). Furthermore, considering that the SMSC development of young people is an underlying theme within the Convention on the Rights of the Child (UN General Assembly, 1989), establishing a link between health education and SMSC in young people has potential relevance well beyond the context of PSHE in England.
While the majority of respondents were positive about PSHE education (Table 2), there was a considerable proportion of young people who did not report benefitting from these lessons. The non-statutory nature of PSHE results in high variability across schools, including variation in individual schools’ vision of PSHE and its purpose (Willis and Wolstenholme, 2016). This is demonstrated by variations in the delivery of topics in PSHE, with economic and careers education being rated least favourably (Brooks et al., 2015). This paper contributes to the evidence base surrounding views that there is a need to involve young people in the evaluation of PSHE education so as to identify what topics are important and beneficial for the lives of young people today (Formby and Wolstenholme, 2012; Willis et al., 2013).
Limitations
This paper is a product of the HBSC study in England; a unique, cross-sectional survey which provides a broad picture of adolescent health, well-being and health behaviours situated in their social contexts. The methodology provided the possibility to explore the impact of PSHE education on adolescent SMSC development with a large, representative sample of young people in England, while controlling for demographic variables. However, findings from this study should be interpreted with knowledge of its limitations. This paper drew on data from the HBSC study for England, which relies on self-reported data and may be subject to social desirability bias. Despite this, self-report data are considered to hold the most valid information when studying how young people view their health and well-being. While the HBSC England dataset provided a large representative sample, the variables relating to SMSC development were to some extent pre-assigned and the SMSC measures identified are by no means exhaustive. In particular, we acknowledge Fisher’s (2016) critique of measuring spirituality among young people; however, within the frame of a large-scale survey-based study it was practical to use an 8-item scale (Michaelson et al., 2016).
Furthermore, the study reveals associations between PSHE education and various outcomes of an SMSC nature, but the nature of cross-sectional research does not allow us to draw conclusions about causal relationships. It is not clear whether young people who reported benefitting from PSHE lessons had already possessed some predisposition to spirituality, less engagement with fighting and bullying behaviours initially, and that was the reason they acknowledged the positive impact of PSHE lessons. Moreover, it is feasible that external factors may influence young people’s appraisal of both PSHE and their SMSC development. While the study did examine variation at the school and class levels, the influence of specific school level variables was unexplored. More investigation is needed to expand current knowledge about the role and mechanism of health education for adolescent SMSC development, with particular note of the school-level factors to provide a full and comprehensive picture.
This study explored the association between young people’s perception of PSHE education and factors of an SMSC nature. PSHE education currently has a non-statutory status, and although widely accepted in many schools, its content and mode of delivery are at the discretion of individual schools. This study is unable to compare those receiving and not receiving PSHE. The positive SMSC outcomes identified in this paper corroborate existing work demonstrating the broader impact of health education at school (Durlak et al., 2011; Sklad et al., 2012); however, future work must consider those with and without PSHE education provision in order to ascertain its impact.
Conclusion
In a national context, PSHE education may play some part in schools successfully meeting both the Ofsted and Education Act 2002 requirements related to SMSC development. As mentioned previously, the non-statutory nature of PSHE education in England is highly contested (PSHE Association, 2017; Willis and Wolstenholme, 2016). The current findings add weight to the argument that PSHE education should be mandatory.
This study did not compare those with and without PSHE, but examined self-reported PSHE provision, indicating that the quality of health education is imperative. Unfortunately, the Ofsted (2013) report entitled Not Yet Good Enough deemed PSHE to be inadequate or requiring improvement in 40% of schools, highlighting poor leadership, lack of teacher expertise and limited curriculum time. The topics delivered in health education are often considered to be of lower priority compared with other aspects of the curriculum (Dewhirst et al., 2014); this is believed to be a consequence of the current results-driven culture which forces a focus on measurable academic outcomes, particularly evident in secondary schools (Formby and Wolstenholme, 2012; Willis and Wolstenholme, 2016).
While the prioritising of educational attainment over health education is counterintuitive, as Bonell et al. (2014) explain, ‘education and health are synergistic’ (p. 1). Students who report positive health and well-being are more likely to have higher levels of school attainment, identified both nationally (Gutman and Vorhaus, 2012) and internationally (Bradley and Greene, 2013; Suhrcke and De Paz Nieves, 2011). Furthermore, there is a promising relationship between health programmes at school and educational outcomes (Durlak et al., 2011; Murray et al., 2007). In line with this, Ofsted (2013) recognised that schools graded highly for PSHE education were more likely to have an outstanding rating for overall effectiveness. And as the 2012 Annual Report of the Chief Medical Officer for England explains, PSHE education ‘forms a bridge between health and education by building resilience and wellbeing’ (Department of Health, 2013).
Providing good-quality health education at school is a worthwhile investment of time and resources, with the potential to reap a number of benefits for young people. This paper focused specifically on the positive impact of PSHE education on adolescent SMSC development; however, considering the pre-established links with health and well-being (Brooks et al., 2018) and attainment (Brooks, 2014; Eaude, 2008), the positive impact of health education is likely to be both long-lasting and far-reaching.
Supplemental Material
Supplementary-material-0150 – Supplemental material for The role of school-based health education in adolescent spiritual moral, social and cultural development
Supplemental material, Supplementary-material-0150 for The role of school-based health education in adolescent spiritual moral, social and cultural development by Kayleigh L Chester, Ellen Klemera, Josefine Magnusson, Neil H Spencer and Fiona M Brooks in Health Education Journal
Footnotes
Acknowledgements
The authors thank the young people and schools that participated in the 2013/2014 HBSC study in England.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The 2013/2014 Health Behaviour in School-aged Children (HBSC) study for England was funded by the Department of Health, England.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.