
Abstract
In the following article, the restorative potential of the environment in a cancer rehabilitation programme is analysed and discussed. The programme was developed as a transdisciplinary cooperation of psychologists, theologians, philosophers, and artists. To investigate the importance of environments, six qualitative focus group interviews were performed with 36 Danish cancer patients (30 females; six males) who attended the programme either at The Danish Knowledge Centre for Rehabilitation and Palliative Care (REHPA), a former hospital building adapted for rehabilitation, or at Løgumkloster Refugium, an old monastery, used as a place for retreat. The data were analysed using a content analysis that took a psychodynamic and hermeneutic approach as its point of departure. Outcomes associated with the environment that enhanced the well-being of the patients were feelings: a) of being close to nature, b) of being protected, c) of the spirit of place, and d) of experiencing narratives of peace. Our programme supports the idea, that environments in which cancer rehabilitation takes place can trigger different emotions and fulfil different existential needs. Aesthetic, historical, and spiritual aspects of an environment can help individuals to respond to existential challenges and can induce hope. Our study contributes knowledge about the interplay between existential well-being and aspects of the environment.
Introduction
More than a century ago, in 1886, the art historian Heinrich Wölfflin wrote a dissertation entitled “Prolegomena to a Psychology of Architecture”. 1 He attempted to show that architectural forms are catalysts for expressions of certain moods. Wölfflin aimed to explain how the subject’s experienced impression of a building was mirrored by the physical expression of the object. For example, a certain relation between height and weight is often experienced as an expression of power, and a human being can feel uplifted when the ceiling is high and oppressed when it is low. Recent health-related research, in line with Wölfflin, looks at the effect of buildings on human emotions and well-being2, 3, 4.
Recently, the psychologist Roger Ulrich 5 tested a conceptual model showing that aggression in psychiatric facilities may be reduced by designing the physical environment with features that evidence shows to be stress-reducing, such as, a) reduction of crowding (e.g., low social density) and environmental stress (e.g., noise reduction), and b) positive distractions (e.g., access to garden or to views of green spaces). His findings suggested that designing (psychiatric) environments with a focus on these features can reduce the safety threat posed by aggressive behaviour. Ulrich’s results contribute to the growing body of research dealing with the influence of treatment environments on patients’ wellbeing.
Being in a natural environment has received particular attention, and Attentive Restoration Theory 6 can be applied to explain how the healing and restorative effects of nature are linked to human attention. Kaplan & Kaplan described psychological attention processes taking place in nature. The healing effect of nature is defined by two different kinds of attention: focused attention and spontaneous attention. During our everyday life, we switch between these two kinds of attention, depending on our environment and the tasks we are involved in. Spontaneous attention in particular has a restoring and recuperating effect on our body and mind. When we are in a natural environment, our senses are stimulated, and we automatically employ spontaneous attention, which means, that we can relax and rest.
When there is a meeting of minds from areas of environment, psychology and health science, there is an opening onto the human lifeworld and its expectations. However, research in health-related environments and rehabilitation often lacks knowledge about the existential needs of patients when they are in treatment. 7 Our surroundings always evoke emotions, but seriously ill and vulnerable patients are especially responsive to their surroundings. 8 Research evidence shows that having to live with a serious or life-threatening illness gives rise to existential concerns. Yet the different ways in which environments of rehabilitation influence the processes of existential rehabilitation have rarely been investigated.
In this paper, we will analyse and discuss the restorative potential of environments in a rehabilitation programme for patients in a challenging life situation. Our programme was explicitly designed to address existential rehabilitation needs (for example the fear of dying) of individuals who have or have had cancer (in the following referred to as patients with cancer) and that was tested and evaluated with two groups of patients in two different environments.
Focusing on the interrelationship between the meaning of the programme as perceived by the patients and the environments in which the programme was being held, this paper will attempt to explore the following question:
How do patients with cancer, who are facing a challenging life situation, perceive the restorative potential of a rehabilitation environment?
Methods
The programme
On the basis of insights from the existing literature and from previous experiences among the authors,9, 10, 11, 12, 13 the programme focused on group counselling combined with art therapy in specifically selected surroundings. ‘Healing dialogue, art and environment’ might summarise the programme. The course was designed within the tradition of existential philosophy and psychology and addressed basic questions of existence: the purpose of life, fear of death, angst. The framework of the programme assumed that environmental aspects were accorded considerable significance for existential distress and growth.
The researchers, drawing experience from their backgrounds as psychologists, theologians, philosophers, and artists, designed the programme together, but took different roles in the implementation. The group counselling was performed by a psychologist and a pastor, the art therapy by an artist. The focus group interviews with theparticipants were performed by a philosopher and a sociologist, who were part of the research group, but had not participated in the programme.
Recruitment
The programme focused on cancer patients’ existential needs and well-being. Participation was voluntary and was prompted by promotional material. The two courses were attended by a total of 40 patients (the maximum number of 20 participants on each course), aged 31–76 years, seven male and 33 female patients with different forms of cancer (curable and non-curable). Each course lasted five days (Monday to Friday) and they took place in June and in October 2018. Thirty-six patients participated in the focus group interviews, which were conducted on the last day of the course. Four patients were absent on the last day due to health or for personal reasons.

Løgumkloster Refugium.
Settings
The two chosen environments were:
Løgumkloster (https://www.loegumkloster-refugium.dk), an old monastery used as a retreat and centre for rehabilitation.
Løgumkloster writes on its homepage: Løgumkloster Retræt can contribute to your life in many ways. On one hand, there is space for enrichment and reflection and on the other for relationships and dialogue about major and minor questions of everyday life. The retreat is open all the year round. If you need a respite for one or more days, a stay at the Retreat can be an unique opportunity for anyone.
REHPA (http://www.rehpa.dk), Danish Knowledge Centre for Rehabilitation and Palliative Care. REHPA offers courses aimed at patients with rehabilitation and palliative care needs. The course facilities are situated in Nyborg, behind the local hospital in specially adapted facilities featuring a view of the nearby medieval castle and in beautiful natural surroundings. The modern rehabilitation facilities, including rooms for group activities, training spaces and a café, are sited on the ground floor, separated from the hospital. Private accommodation is on the third floor of the hospital, which previously housed offices and administrations facilities, and here there are recreation rooms and a dining room. Getting from the rehabilitation facilities to the third floor requires patients to walk past the hospital. REHPA’s facilities, the third floor in particular, have been designed and furnished with the design principles of ‘healing architecture’ in mind. These principles were developed on the basis of a literature review of ways in which the physical environment influences individuals dealing with life-threatening illness. The five design principles include: functionality, light-sound-air-temperature, nature, privacy and relations, and atmosphere. 14
REHPA, living room, 3rd floor.
Both course venues are placed in attractive natural surroundings. The retreat is located close to a river and a forest, while REHPA is close to the sea. Today, Løgumkloster serves as a place of retreat for the public and offers courses throughout the year. REHPA is a national knowledge centre and offers courses aimed at patients with life-threatening illnesses, or those needing rehabilitation or palliation.
Ethical considerations
The study was approved by the Research and Innovation Organization (RIO) of the University of Southern Denmark (Journal nr.10.104). All patients were provided with written and verbal information about the research project before attending the course and gave their informed written consent.
Analysis
The overall evaluation of the programme was carried out using participant observation and focus group interviews with 36 patients (30 female, six male).15, 16 The patients were provided with photos of the various activities and the surroundings. The interviews lasted up to sixty minutes and were transcribed verbatim and validated by the focus group moderators. The evaluation of the overall elements of the course (such as group therapy and art therapy) are described elsewhere. In this paper, we have specific focus on the restorative impact of the rehabilitation environment on the patients’ existential well-being.
Methodological framework and procedure of the analysis
The data from the focus group interviews were read several times, and all passages regarding the environment were extracted.
As a first step, the transcripts from the focus group interviews were analysed using a psychodynamic approach. 17 This meant that special attention was given to the topics and emotions that were of significance to the patients’ existential well-being and which were evoked by the two different course environments. As a second step, a more detailed and in-depth content analysis 18 was carried out, whereby the transcribed material was coded with a focus on the overall research question cited in the introduction.
Step 1: Comparative analysis of communication within the focus groups
To understand how the group processes differed in the two venues, the transcripts were reviewed on the basis of three selected questions of a question guide developed by interactional group psychoanalysts. 19 These were:
What are the patients (of this group) talking about? (For example: Do they mention specific topics?)
Are there any rules or norms common to the group? (For example: Do they show a propensity for agreement? Is there a strong focus on the interviewer?)
Which emotions are mentioned by the patients? (For example: anger, dissatisfaction, happiness)
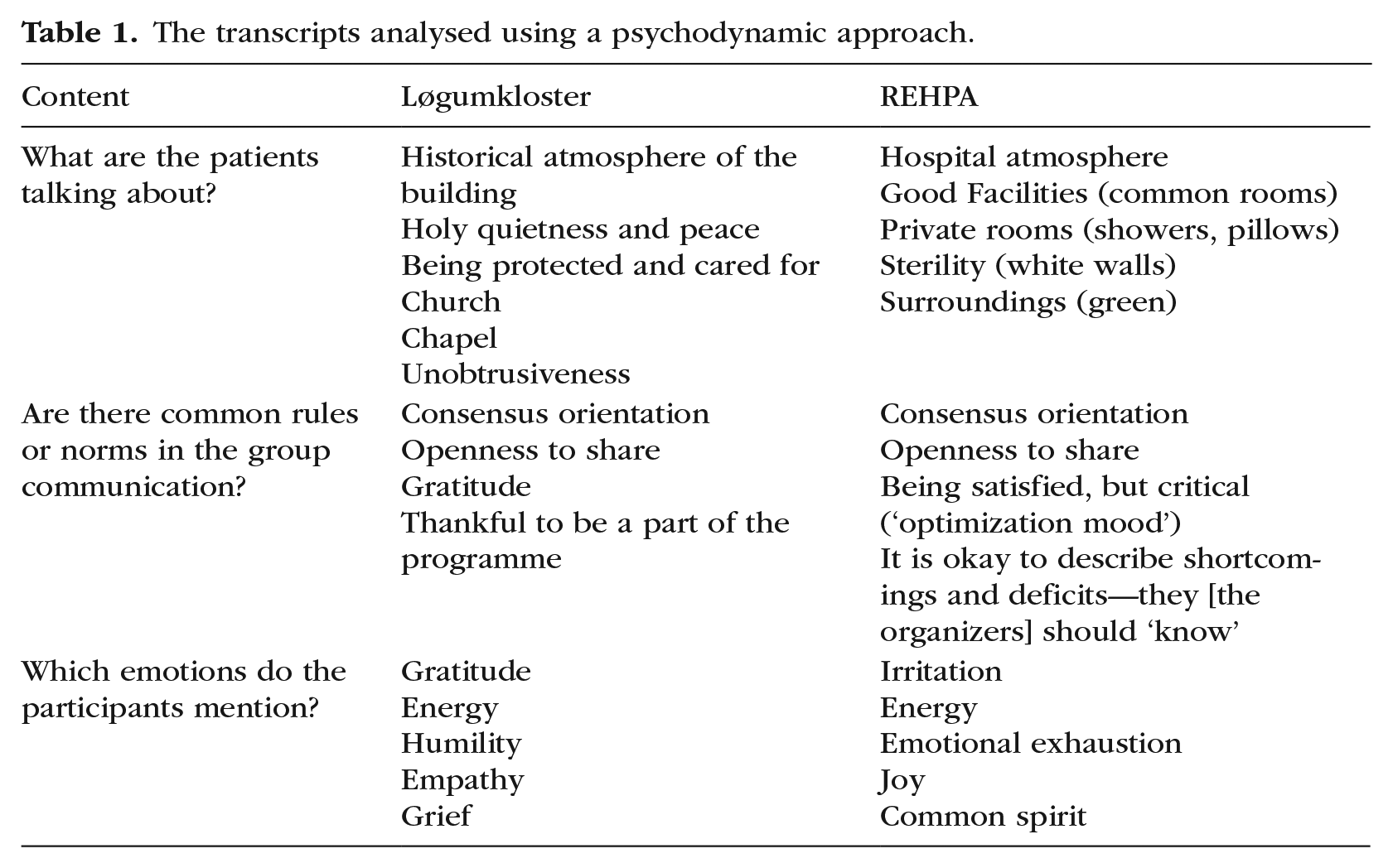
The six focus group interviews were conducted on the last day of the course following four days of intense getting-to-know each other and course engangement. The atmosphere was trustful and relaxed; the members of all focus groups aimed at reaching a consensus, but they also expressed different opinions. Regarding the emotions, it was noticeable that the patients in Løgumkloster expressed a higher level of gratitude about the programme (see Table 1).
The transcripts analysed using a psychodynamic approach.
Step 2: Analysis of the restorative aspects of environment
The second step of the analysis of the data material included a content analysis, 20 where the transcribed material was analyzed with a focus on the restorative effects of the natural surroundings and the architecture, as indicated by the participants. The comparison of the two venues was less important in this analysis since the aim was to identify whether overall benefits to patients’ well-being could be derived from their environment. Working with the material revealed a variety of important beneficial aspects of atmosphere and environment such as: feeling close to nature; feeling protected; sensing the soul of the place; and experiencing narratives of peace.
Close to nature
Being able to have access to their natural world and to have a view of their natural surroundings was mentioned as important by all participants. In Nyborg, a woman took daily biking rides to the sea (‘I have been to the water every single day!’), while a man went out jogging, and almost all took walks during the day on the castle wall. In Løgumkloster, they all enjoyed the gardens and some went for walks or jogged in the nearby forest.
Of particular importance were the bedrooms and the beginning of the day, as many participants had experienced prolonged periods without sleep in their life with disease. At Løgumkloster, the bedrooms were sited at the ground level with a view of fields and river and open countryside and direct physical access to the surrounding environment. The horses in the nearby meadow particularly caught the positive attention of many.
“Waking up to the view of two horses and to the sound of singing birds.” “If I wake up during the night and look through the window, I see the horses.”
The bedrooms in Nyborg were situated on the third floor, where the participants had access to a living room with a balcony providing a pleasant view of the surrounding gardens and woodland. The living room and the balcony were designed with an eye to light and air and this was appreciated by the participants. The balcony was mentioned as a place for talks and relaxation.
“I have relaxed on the balcony and talked to others.” “It was a quiet and relaxing place.”
The courses were held in the summer and autumn. Both seasons were mentioned by the participants, always in a positive manner with an emphasis either on the summer temperature or on the autumn colors.
Feeling protected
While the patients’ morning experience was shaped by their visual access to nature or life outside, the experience of well-being during the day was influenced by different emotions. In Løgumkloster, the group therapy sessions on the first day had started by a communal reading of the first chapter of The Brothers Lionheart by the Swedish author Astrid Lindgren. In this novel, an older brother comforts his dying little brother by telling him about an idyllic land beyond the stars and beyond death, called Nangijala. The image of Nangijala was taken up by the participants to describe the environment they were in as evoking a sense of security and inner feelings of being protected.
“This is a place where I can feel small and protected.” “The atmosphere was respectful, there is a lot of dignity.” “These rooms must know something about it [the 1000 year tradition of spiritual care], since they built what we need—this protection and this magnificence [. . .]. The rooms allow you to feel protected and comforted.”
The spirit of place
At both venues, the group rooms were described as cheerful, and some mentioned candles and flowers in the rooms as having a positive impact. At Nyborg, where all participants had emphasised having access to their natural surroundings as positive, the overriding consensus was that their individual accommodation evoked negative emotions caused by the sterile atmosphere of the rooms with the bare whiteness of their clean walls.
“The atmosphere was sterile, all that white colour on the walls. Why did the walls have to be white, anyway?” “I was sitting in a cell, a white, empty cell.” “It gives you the pip, all that hospital stuff.”
The hospital atmosphere conveyed by the building aroused some aversion and brought back memories of treatment and admission to the world of disease. As the participants otherwise expressed satisfaction with the rehabilitation course, it is important to underline, that the colour white seem to be of particular importance, especially when they brought back memories of hospital.
Communicating narratives of peace
In Løgumkloster, various Christian rituals (a service of prayer, the singing of hymns) were available during the day for those interested. Before breakfast, a morning assembly was held in a small chapel, while the evensong was held in the large church, as part of a daily public event. On the way to these events along a corridor, signs requested people to ‘walk calmly and speak softly’. Morning prayer and evensong were not part of the programme but offered as options to the course participants. For a number of the participants, the Christian atmosphere elicited a sense of being worthy: “I do not walk into a religion, I walk into a room. I can distinguish this”. “I have got the feeling that I am worthy”. “The quietness of the place calmed my troubled mind”.
The peaceful atmosphere was described as being of utmost importance. The participants especially stressed the influence of the historical aspects of the Christian building as a space that created an inner silence, humility and personal gratitude. They emphasized the importance of the dignity of the monastery building, especially the chapel for the morning prayers, where an atmosphere of quiet concentration and reverence prevailed: “The old church is conveying a thousand years of knowledge and of tradition as a place of sanctuary”. “What was it this place could offer?[. . .]. How could the monks be so creative [. . .]? My conclusion is that it was because they were living in quietness”
“I think it’s [. . .] almost as if it’s all in the bricks—the whole business about being in something historical and something divine or something respectfully human somehow.” It seemed as if narratives of peace and sanctuary were embedded in the very bricks of these historic walls. The individual life story was merged with the holiness of the place, making the individual destiny less important in the larger scheme of things, and this provide peace for the individual.
When we sum up the various aspects of analysis, a number of environmental aspects can be characterized as supportive. Starting with the overall spirit of place, our participants cited being embedded in history as being important. A new building close to a hospital can evoke memories of an individual history of disease but can also represent a tradition of care. As for the monastery, the feeling of being a part of something that was bigger than the individual life story seems to promote a form of reverent humility in the face of immensities of time and space and an awareness and acceptance of the fragility of life against the power of the human spirit. The views onto the world outside and access to nature was also perceived as significant. Having visual access to nature, historic buildings and animals is mentioned as enhancing existential well-being.
Discussion
Our analysis identified environmental elements of importance in an existential cancer rehabilitation programme working with group and art therapy. Our analysis lays the foundation for a twofold interpretation of aspects of importance for the well-being of cancer patients. The first covers psychological aspects of containing, holding and protecting, while the second aspect is a more philosophical understanding of an opening to the world around us—and beyond.
Containment, protection, and control
A one-week programme requires that the patients experience a warm welcome and the feeling of being ‘at home’. The start of the day is, therefore, of immediate importance for their well-being. The need to feel comfortable and safe during a residential programme might be especially pronounced for patients who have undergone the alienating experience of admission to hospitals without any privacy. Cancer patients often experience that they lose control of their lives when confronted with their diagnosis, but these existential aspects are seldom investigated. 21 Our results show that different aspects of the environment can support the experience of finding themselves in a safe place. Given that we also have palliative patients and ‘palliare’ means to alleviate without curing and to cover with a coat. The environment seems to have a double function—to contain feelings and to provide a sense of security. All patients emphasised the importance of the view. The view can provide a link to history (e.g., castle walls), to creatures (e.g., horses) or visual access to the natural world. Regarding the effects of the view of and from patients’ rooms, in the 1980s the environmental psychologist Roger Ulrich started the tradition of evidence-based healthcare design (EBD). 22 He demonstrated that patients with a view of the natural world (trees) had shorter postoperative stays than matched patients in similar rooms with a window looking onto a brick wall. His research has been the starting point of gathering evidence that the view from a window can provide opportunities for restitution and well-being. 23
When looking into healthcare design and well-being, the aspect of light and privacy often figures. 24 However, these aspects were of less importance in our study. All patients had single rooms for the week, but these rooms were mostly referred to when discussing the comfort of the interior furnishings, for example the poor quality of the pillows or the lack of a private bathroom. However, complaints about the poor quality of the pillows might be an expression of a more general wish to be cared for when going on a rehabilitation course. Being cared for or being held is a cultural and spiritual narrative, and the term safekeeping went through almost all quotes of the patients. Most of the patients had a secular background, and were not practising religion in their every day life. However, they felt particulary secure and sheltered at Løgumkloster. This might simply be explained through the architecture of the building. The old monastery has thick walls imbued with history, while the retreat is built as a quad around a garden offering safety, peace and space for privacy. There seemed to be an interplay between existential meaning and the religion narrative in the building.
The place was able to contain the individual. In psychology, the term containing or containment refers to a psychoanalytic process in which therapists initially record and hold the projections and emotions of patients without reacting to them. 25 In a second step, the psychotherapist transforms what is unbearable for the patient into something bearable and gives it back in a third step. At Løgumkloster, the walls and the building seem to have contained the difficult emotions of the patients. At Nyborg, other individuals were mentioned as important, for example staff working as volunteers during the evening activities.
The experiences encouraged by these environments can also be interpreted as attempts to tackle, reduce or come to terms with the anxiety that derives from a sudden and shocking awareness of the finite nature of existence. 26 Patients explained that when encountering the monastery’s 1,000 years of history, their own destiny and personal life story were suddenly seen in a larger perspective that made them feel dignified and humbled at the same time. We have to be aware that almost all patients described themselves as not religious persons.
While containment as a psychological interpretation found expression in the protective influence of the environment, an existential phenomenological perspective can point to a spiritual dimension of these environments. The Danish theologian and philosopher, K.E. Løgstrup 27 describes aesthetic impressions as a way of connecting to the world through our senses, which links with the historical start of this paper and Wölfflins ideas. Seen against the background of Løgstrup’s ideas, participants could be said to be experiencing environments as protective sanctuaries; for example, when the old monastery walls were experienced as opening up ‘a larger perspective’, this may have indicated a turning away from an introspective fixation on existential pain and loss of dignity, towards a more receptive acceptance of the world. As pointed out by Løgstrup, aesthetic expressions can open up and tune what he calls ‘universal emotions’ such as anxiety, grief, happiness, and love. Such emotions are, of course, individual and related to the individual’s situated being, but they are also universal as human experiences. Impressions received from the environment seem to have the potential for opening up the universal dimension of the emotions which accompany a life-threatening illness by transcending the feeling of being isolated selves. Taking this spiritual dimension into account, restorative and calming surroundings, which can contain cancer patients’ emotions, have the potential for inducing hope. This is not a concrete hope for changed life conditions such as cure or prolongation of life but ‘an absolute hope’ 28 —a hopeful way of being found in connectedness to the world.
It is a hope which knows the given conditions for our existence but it does not limit itself by those. It is a hope which transcends death.
29
Limitations
Our results are generated by observations of a restricted number of patients. We deliberately decided to try our programme on a smaller scale in order to gain an understanding of contextual, relational, and situational issues of significance for processes of change. In addition, different patients participated in the two venues, and this reduced the comparative aspects of our results. We have also be aware that most of our participants were females, showing that a programme addressing counselling and art mostly appeals to women. However, the quotations cited were uttered by the participants and might in this way be applicable to others who experience existential concerns and difficulties as a consequence of their illness trajectory.
Conclusion and implications for practice
The research question for this study was how patients do perceive the restorative potential of environment in an existentially challenging life situation. The environments described effected inner moods, experiences and expectations in very different ways. This study contributes new knowledge to ways in which environments might support existential and spiritual wellbeing, might provide containment for challenging emotions, and induce hope.
Footnotes
1
H. Wölfflin, Prolegomena zu einer Psychologie der Architektur. [Prolegomena to a psychology of architecture] (München: Mann, 1886).
2
B. Cold, Aesthetics, Well-Being and Health. Essays within architecture and environmental aesthetics (Burlington: Ashgate, 2001).
3
R. S. Ulrich, C. Zimring, X. Zhu, J. DuBose, H. B. Seo, Y. S. Choi., X. Quan, and A. Joseph, ‘A review of the research literature on evidence-based healthcare design’, Herd 1.3 (2008): 61–125.
4
K. K. Roessler, ‘Healthy Architecture! Can environments evoke emotional responses?’, Global Journal of Health Science 4.4 (2012): 83–9.
5
R. S. Ulrich, L. Bogren, S. K. Gardiner, and S. Lundin, ‘Psychiatric ward design can reduce aggressive behaviour’, Journal of Environmental Psychology 57 (2018): 53–66.
6
R. Kaplan and S. Kaplan, The experience of nature: A psychological perspective (Cambridge: University Press, 1989).
7
S. Blaschke, ‘The role of nature in cancer patients’ lives: a systematic review and qualitative meta-synthesis’, BMC Cancer 17.1 (2017): 370.
8
M. Browall, I. Koinberg, H. Falk, and H. Wijk, ‘Patients’ experience of important factors in healthcare environment in oncology care’, International Journal of Qualitative Studies in Health and Well-Being 8 (2013): 20870.
9
H. Peoples, N. Nissen, Å. Brandt and K. la Cour, ‘Belonging and quality of life as perceived by people with advanced cancer who live at home’, Journal of Occupational Science 25.2 (2018): 200–13.
10
K. K. Roessler and F. W. Lindemann, ‘How to cope with anxiety in hospital settings: Evaluation of a professional training’, Expository Times 126.2 (2014): 63–70.
11
N. C. Hvidt, T. B. Mikkelsen, A. D. O. Zwisler, J. B. Tofte, and E. Assing Hvidt, ‘Spiritual, religious, and existential concerns of cancer survivors in a secular country with focus on age, gender and emotional challenges’, Journal of Supportive Cancer Care 27.12 (2019):4713–4721.
12
K. la Cour, S. Josephsson, and M. Luborsky, ‘Creating connections to life during life-threatening illness: Creative activity experienced by Elderly Peple and Occupational Therapists’, Scandinavian Journal of Occupational Therapy 12.3 (2005): 98–109.
13
K. la Cour, ‘Possibility spaces in every day life: On creative potentials in interventions for people with life-threatening incurable diseases’, Positive Approaches to Health. (Hauppauge: Nova Science Publishers, 2007), 37–46.
14
K. Falk and H. U. Timm, Arkitektur & lindring [Healing Architecture], (Nyborg: REHPA, 2018).
15
C. A. Davies, Reflexive ethnography : a guide to researching selves and others, 2nd ed. (London, New York: Routledge, 2008).
16
C. S. Davis, Focus groups: applying communication theory through design, facilitation, and analysis (New York: Routledge, 2017).
17
U. Streeck and F. Leichsenring, Handbuch psychoanalytisch-interaktioneller Therapie. Behandlung von Patienten mit strukturellen Störungen und schweren Persönlichkeitsstörungen [Handbook of psychoanalytic-interactional therapy. Treatment of patients with personality disorders] (Göttingen: Vandenhoeck & Ruprecht, 2009).
18
K. Malterud, ‘Qualitative research: standards, challenges, and guidelines’, The Lancet 358(9280), (2001): 483–8.
19
Streeck and Leichsenring (2009).
20
Malterud, (2001).
21
Blaschke (2017).
22
R. S. Ulrich, ‘View through a window may influence recovery from surgery’, Science, 224.4647 (1984): 420e1.
23
E. R. C. M. Huisman, E. Morales, J. van Hoof and H. S. M. Kort, ‘Healing environment: A review of the impact of physical environmental factors on users’, Building and Environment 58 (2012): 70–80.
24
R. Gifford, Environmental Psychology (Victoria: Optimal Books, 2014).
25
W. Bion, Learning from experience. (London, 1961).
26
I. Yalom, Existential psychotherapy, (New York: Basic Books, 1980).
27
K. E. Løgstrup, Metafysik II [Metaphysics II], 2nd edn (København: Gyldendal, 1975).
28
K. E. Løgstrup, Metafysik IV [Metaphysics IV], 2nd edn (København: Gyldendal, 1971).
29
K. E. Løgstrup, Metafysik IV [Metaphysics IV], 2nd edn (København: Gyldendal, 1976/1995), 247.