
Abstract
Walkability is a critical component of built environments, yet there is still diverse conceptualization and measurement of the construct. The Walk Score® metric is one measure of walkability, which is widely used in scholarly, industry, and public domains. With increased interest in the use of Walk Score® as a research tool, it is necessary to examine the operationalization and scope of the measure. This scoping review examined how researchers utilized Walk Score® in walkability research, with specific attention to identifying limitations related to health outcomes as well as the use of the metric in non-health research contexts. Findings from the review provide a novel and critically nuanced understanding of how the assumptions and limitations of Walk Score® are addressed relative to socio-ecological aspects of walkability.
Introduction
Public health researchers, policymakers, and practitioners have long acknowledged the role of our built environments on health and healthy behaviors like walking. How pedestrians interact with the built environment, as a combination of land use, urban design, and transportation, can have measurable effects not only on their walking, but their overall physical, social, and mental health (Shields et al., 2021). Walkability is an important component of built environments, however, its conceptualization and operationalization are challenging due to walkability’s position at the nexus of geography and public health (Hall & Ram, 2018). To improve walkability, we must be able to consistently conceptualize and measure it in an effort to distinguish between more and less walkable places and plot potential pathways for intervention, especially given shifting patterns in walking behaviors, for example, since the emergence of COVID-19.
Although there are multiple tools for operationalizing walkability, these tools are considered to be in the first generation of research for several reasons. First, there is a proliferation of health promoters working to advance walkability research across a wide variety of geographic landscapes (Rišová, 2020). This abundance of highly specific walkability models and applications has resulted in a lack of generalizability and transferability between research, policy, and practice settings. Second, a great deal of walkability research is rooted in expensive, time-consuming primary data collection via systematic street audits, and secondary data collection from geographic information systems and other digital databases. The prohibitive costs for either of these two options can limit the accessibility to data as well as the scale and scope of walkability work. Thirdly, health promoters focused on walkability have often failed to detail their methods in a way that facilitates transparency and replication, stalling validation of these tools, and advancement of this body of work (Rišová, 2020; Shashank & Schuurman, 2019; Shields et al., 2021; Vale et al., 2016; Wang & Yang, 2019), especially across different kinds of geographic contexts (e.g., highly urbanized vs. smaller, less urbanized environments).
The Walk Score® (Walk Score, 2022a) metric is commercially available and has offered a potential solution to improving the standard for walkability research, policy, and practice. Walk Score® was introduced by a private company in 2007 and is a calculation of walkability that can be applied to any location as it combines distance and accessibility to destinations weighted by attractiveness (e.g., grocery stores, coffee shops, parks, banks) and street connectivity (Walk Score, 2022b). Walk Score® was originally calculated on the basis of Euclidean (or straight-line) distance from a location. In 2011, Walk Score® introduced the “Street Smart Walk Score®” (hereafter referred to as “Walk Score®”), which consists of a weighted and attenuated Raw Score based on network (or street route) distances, and penalties reflecting pedestrian friendliness, namely Intersection Density (ID) and Average Block Length (ABL) (Figure 1). Walk Score® is assessed as a scale from 0 to 100 for a single location, with scores of 0 to 49 representing a location that is “car-dependent,” 50 to 69 a “somewhat walkable” location, 70 to 89 as “very walkable,” and 90 to 100 a “walker’s paradise.”
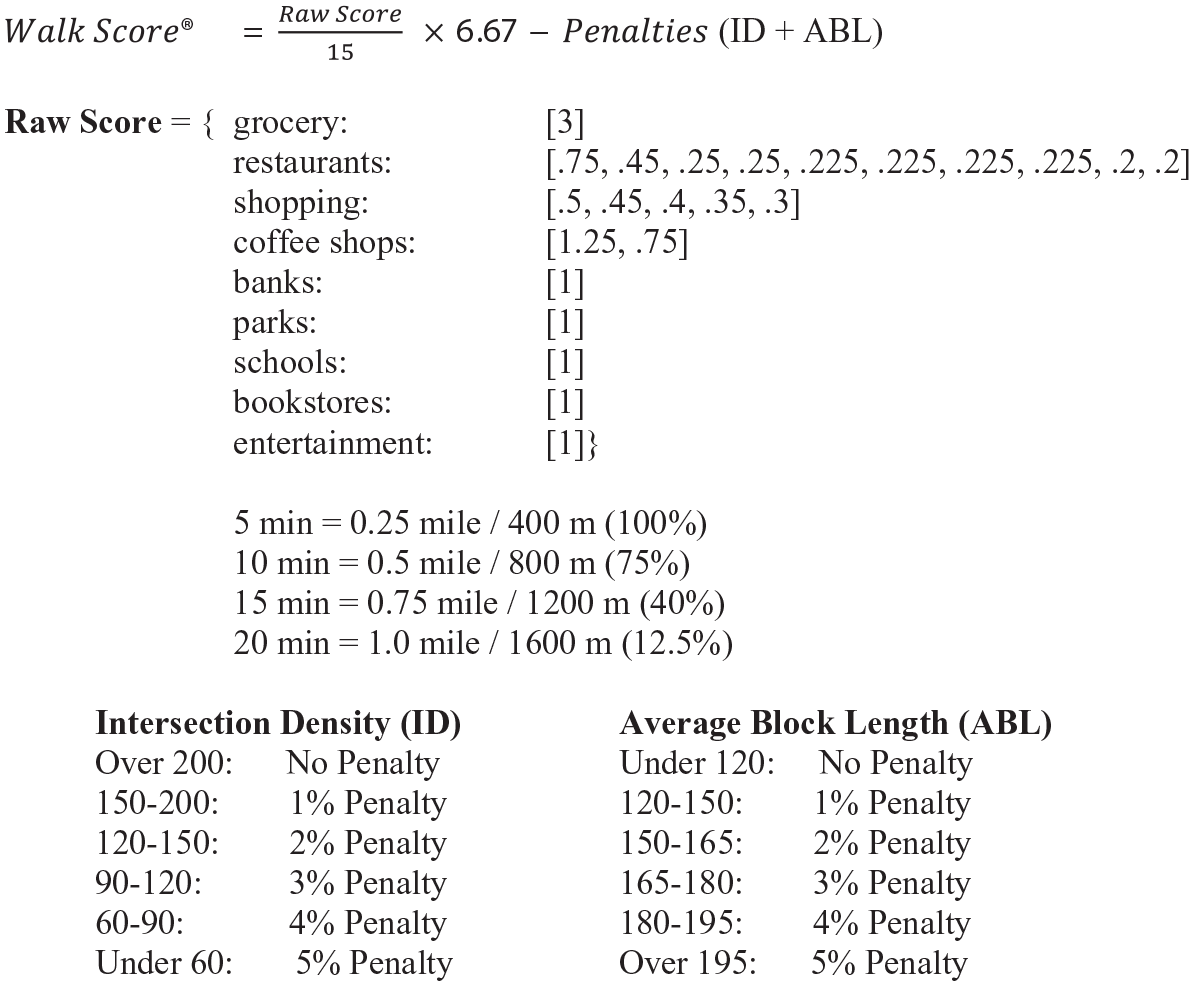
Components of the Walk Score® walkability metric formula.
Walk Score® has several advantages as a tool for assessing walkability, although many assumptions on which the metric is based may reflect conceptions of walking primarily as a derived demand for travel to a destination rather than for leisure, and it may or may not reflect how walking behaviors changed during destination restrictions and closures due the pandemic (Paydar & Fard, 2021; Salon et al., 2021). The measure is computed using information online and is available for locations throughout the United States, Canada, Australia, and New Zealand, in this way increasing the feasibility, generalizability, and transferability of research on walkability. Furthermore, the computation of Walk Score® is accessible and replicable for any location, allowing for continued refinement and tool advancement as needed to reflect the meaning and utility of walking in a changing social context. As such, researchers and knowledge users should be cognizant of the limitations and implications of using Walk Score® in the context of health promotion, by understanding its use and application during its first decade of research.
Health Promotion Implications of Walk Score® as a Research Tool
Walkability is a multidimensional construct and includes socio-demographic, built environment, individual, natural environment, and many other factors (Shields et al., 2021). Walk Score® provides an indication of walkability, but is limited in scope. Walk Score® is what is known as a destination-based walkability metric, meaning it is measured according to the number of available destinations to which pedestrians might walk from a given location (Nykiforuk et al., 2016). As such, this metric is well-suited to capturing walkability for active transportation, versus leisure time, recreational, or physical-activity based walking. As Battista and Manaugh (2018) note: “pedestrians’ social characteristics impact travel behavior independently of the built environment . . . By representing walkability through strictly physical spaces, practitioners risk ignoring generalizable social circumstances as much as resident- and neighborhood-specific particularities grounded in walkable space” (p. 53). Notably, walking behaviors changed during the height of the pandemic in unpredicted and unprecedented ways, requiring a corresponding shift in the assumptions underlying how we measure walkability in a dynamic socio-political environment (Hunter et al., 2021; Paydar & Fard, 2021). In this scoping review, we examine how researchers have operationalized Walk Score® in the context of walkability research related to health outcomes as well as the use of the metric in non-health research contexts. An understanding of how the assumptions and limitations of Walk Score® are addressed in relation to socio-ecological aspects of walkability during the first 10 years of its use will provide a critical lens to the scope of the next decade for this popular tool in the walkability sphere.
Rationale and Objectives for a Walk Score® Scoping Review
With increased interest in the use of Walk Score® as a research tool, it is necessary to outline the operationalization and scope of the measure as it has been applied during the first 10 years of its use. The accuracy of the Walk Score® metric has been field validated by two research groups working in the United States between 2010 and 2013, one working with the Euclidean version of the metric in the state of Rhode Island (Carr et al., 2010, 2011), and the other with the network version across four anonymized urbanized centers (D. T. Duncan, 2013; D. T. Duncan et al., 2011). In 2018, Koohsari et al. (2018) validated Walk Score® in rural and urban areas in Japan. Additionally, Nykiforuk et al. (2016) field validated Walk Score® in three municipalities in Alberta, Canada corresponding to small, medium, and large population centers in the Canadian census. Nykiforuk et al. along with others noted that Walk Score® omits meaningful ideas about walking as the participation in an activity space, instead “assum[ing] a contestable normative dimension, by assigning walking to the consumption of a particular set of goods and services” (p. 536). Given these considerations, our team sought to understand whether the use of Walk Score® in research grapples with these (and other) potential limitations of the metric, to understand its contribution, and areas for further consideration of the health promotion and walkability research literature that is sensitive to socio-political or other system-level changes that may influence walkability.
Despite some progress in the examination of Walk Score® in the research context, scoping review protocols have not regularly been adhered to and only a portion of the published work has been examined since the introduction of Walk Score® in 2007. In their systematic review, Hall and Ram (2018) reported on 42 articles using Walk Score® as a walkability metric up to January 2017. The authors reported a variety of study attributes, including journals of publication, countries where research took place, operationalization of walkability beyond referencing Walk Score®, whether studies employed Walk Score® alone or in combination with other walkability indicators, walking behaviors examined (transportation/purposive, leisure/recreation, or both), socio-demographic factors, types of outcomes examined, and whether research hypotheses were supported by the examined evidence. Hall and Ram focused on the results of the studies and how Walk Score® was used in these studies, and their scope was limited to active transport. The current scoping review expands on the work of Hall and Ram (2018) by adhering to scoping review reporting guidelines, by covering a greater proportion of the published literature, and by considering how assumptions underlying Walk Score® research might be reconsidered for future applications. In conducting a scoping review of peer-reviewed research using Walk Score® that adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting guidelines (Tricco et al., 2018), we aim to summarize and map this large, multidisciplinary, and heterogeneous body of literature in such a way that is transparent and replicable. More specifically, this scoping review aimed to examine the following bibliometric, geographical, and methodological questions in presenting the scope of Walk Score® research available in its first decade, that is, from 2007 to 2018:
Which researchers, funding agencies, and publications have employed Walk Score® in research studies across health and other disciplines in the 10 years since it first launched?
Where has the research using Walk Score® taken place nationally and regionally, and what are the most common geographic scales?
What kinds of analyses are being conducted with Walk Score®, in terms of the format of the metric as a variable of interest, sample populations, outcome measures, statistical testing, and other demographic variables of interest?
What are the implications of the bibliographic, geographic, and methodological characteristics of this Walk Score® research in terms of gaps and future directions for studies in a wider socio-political context (e.g., post-pandemic and other future societal shocks)?
By answering these research questions, we identify themes, limitations, and primary concepts, and unpack the implications of approximating walkability with Walk Score® in health promotion for future research, with a particular focus on research that has examined health outcomes.
Methods
Scoping Review Approach
A scoping review was selected for this research, permitting discovery of the broad coverage of research using Walk Score®, and enabling us to meet our research objectives with an overview of the volume and focus of available literature (Munn et al., 2018). In comparison with systematic reviews, scoping reviews will help to generate hypotheses, rather than summarise the evidence on a chosen topic- presenting the bibliometric characteristics, examining important concepts, and revealing potential gaps in the literature (Tricco et al., 2018). Using this approach, we were able to chart and summarize details from a heterogeneous body of knowledge, identify strengths and limitations, and draw conclusions for the planning of future research using Walk Score® data (Arksey & O’Malley, 2005) in a dynamic socio-political context. Our reporting follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews (PRISMA-ScR) (Tricco et al., 2018).
Strategy for Searching and Screening the Literature
Two comprehensive searches were conducted by a research librarian (JYK) on October 2, 2018 and updated on May 1, 2019 to identify all peer-reviewed articles published up until December 31, 2018 in Ovid MEDLINE (1946-), EMBASE (1974-), CINAHL, Scopus, Web of Science Core Collection, and Academic Search Complete, using a combination of terms to represent the Walk Score® walkability metric (e.g., sample MEDLINE search: (walk* score* OR walkscore*).mp. JYK searched Google Scholar on October 10, 2018 using the 2007 to present constraint of Walk Score® being launched, and removing patents and citations, reviewing the first 20 pages of results (exceeding standard retrieval of the first five pages to ensure a comprehensive dataset across multiple fields and disciplines). As a follow-up to these information sources, we retrieved all of the articles listed on the Walk Score® website under “Walkability Research” (https://www.walkscore.com/professional/walkability-research.php) and “Public Health Research” (https://www.walkscore.com/professional/public-health-research.php) on October 18, 2018. Drawing on its expert knowledge as walkability researchers, the research team identified additional articles not retrieved through the academic databases, Google Scholar, or Walk Score® website. Searches were limited to those available in English only. This selection of sources reflects the first 10 years of walkability research employing Walk Score® across health and other applications.
We screened all articles for inclusion by reviewing the title, abstract, and keywords, as well as conducting a text search query using the combination of terms walk* score* OR walkscore*. Articles were excluded at the first screening stage due to (a) publication in a non-English language, (b) publication prior to the launch of Walk Score® in 2007, (c) publication in a non-peer reviewed format, (d) publication in a predatory journal, and (e) publications not including the terms walk* score* OR walkscore* throughout their text. Next, the reference lists for all of the retained articles were text search queried using the combination of terms walk* score* OR walkscore*, with additional first screening conducted for new articles retrieved. The second screening involved full text review of the included articles, removing any publications which only nominally mentioned Walk Score® and therefore did not provide any data for substantive analysis or interpretation. Finally, documents were coded as health research or other research based on the target audience. A review protocol does not exist for this scoping review.
Procedures for Data Charting
Data were charted from the included sources of evidence by two independent coders (trained research assistants) using a pre-developed extraction template. Twenty documents were reviewed by both coders to ensure inter-coder reliability. Items charted were: bibliographic characteristics (i.e., type of research conducted [epidemiological, empirical, tool development, narrative review, or other], peer-reviewed journal names, years of publication, names and frequency of publication by co-authors, whether research was conducted as part of a larger study, and names of funding agencies); geographic variables (i.e., countries and sub-regions where research took place, physical scale of the research); variables of interest (i.e., sample population, size of sample populations, dependent/outcome variables, and other covariates); and analysis details (i.e., statistical analyses, additional sources of data). Notably, the research type reflects the primary topic studied, with epidemiological referring to studies with health and wellness outcomes (e.g., body mass index, physical activity levels, or chronic disease) and empirical to studies of environments, systems, or objects (e.g., transit usership or real estate prices). Tool development captured research validating walkability or other indices, reviews summarized relevant literature, and other included opinions or commentaries published in the peer-reviewed literature. Although some overlap occurred between research types, this and other charted items represented relatively discrete and comparable evidence for summarizing Walk Score® research activity with a scoping review. A critical appraisal is not required for scoping reviews, and therefore we mapped all of the sources as published, without analysis of the direction and magnitude of study results (as would be expected when employing systematic review methods) (Tricco et al., 2018).
Results
Document Searching and Screening
The process of retrieval, removal of duplicates, first screening, second screening, and categorization is documented in a PRISMA-ScR diagram (Figure 2). There were 1,245 records initially retrieved, with removal of duplicates (n = 146) resulting in 1,099 unique documents retrieved from academic databases (n = 418), Google Scholar (n = 127), the Walk Score® website (n = 64), identification by the research team (n = 3), and text search query of reference lists (n = 487). Documents were removed during the first screening for (a) publication in a non-English language (n = 5), (b) publication prior to the launch of Walk Score® in 2007 (n = 76), (c) publication in a non-peer reviewed format (n = 323), (d) publication in a predatory journal (n = 6), and (e) publications not including the walk* score* OR walkscore* throughout their text (n = 489). At the second screening stage, 28 publications were removed from the dataset for only nominally mentioning Walk Score®. A total of 172 (103 coded as health, 69 coded as other) documents retained for analysis as sources of evidence, originating from academic databases (n = 121), Google Scholar (n = 40), the Walk Score® website (n = 1), identification by the research team (n = 3), and text search query of reference lists (n = 7).
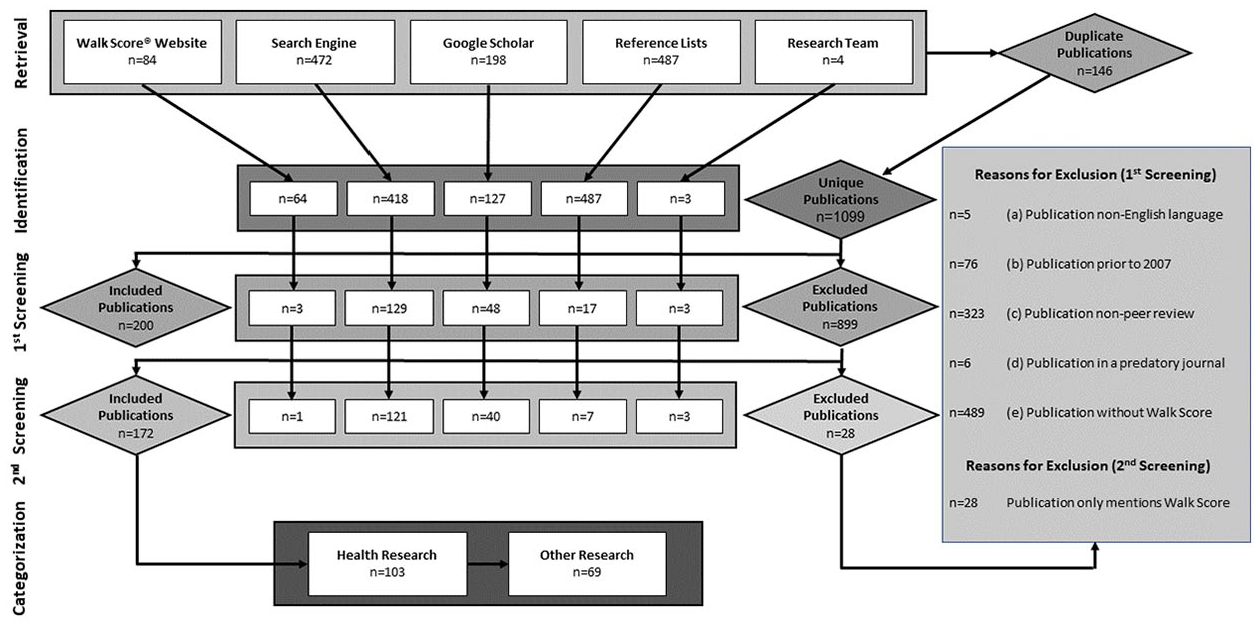
PRISMA diagram.
Summary of Data Extraction
A synthesis of our results is located in Table 1. In terms of the bibliometric characteristics of the research, the most frequent types of research conducted were epidemiological (n = 87), empirical (n = 50), tool development (n = 14), reviews (n = 6), and other (n = 15). Journals that most frequently published this research were the International Journal of Environmental Research and Public Health (n = 12), Transportation Research Record: Journal of the Transportation Research Board (n = 11), Preventive Medicine (n = 7), American Journal of Preventive Medicine (n = 6), Journal of Transport & Health (n = 5), Applied Geography (n = 5), and Health & Place (n = 5). Walk Score® publications increased year over year starting in 2009 (other research n = 1), 2010 (other research n = 2), 2011 (other research n = 5), 2012 (health research n = 3; other research n = 4), 2013 (health research n = 7; other research n = 9), 2014 (health research n = 8; other research n = 6), 2015 (health research n = 18; other research n = 12), 2016 (health research n = 21; other research n = 9), 2017 (health research n = 25; other research n = 9), 2018 (health research n = 18; other research n = 10), and in press (2019; health research n = 3; other research n = 2) (Figure 3). National research agencies were most frequently cited as funding sources, including the National Institutes of Health (NIH) (n = 33), the Canadian Institutes of Health Research (CIHR) (n = 23), the National Sciences and Engineering Council of Canada (NSERC)/Social Sciences and Humanities Research Council of Canada (SSHRC) (n = 9), and the Centers for Disease Control and Prevention (CDC) (n = 7). Other important funding sources included Michael Smith Health Research BC in Canada (n = 7), and the Robert Wood Johnson Foundation in the United States (n = 6). The most frequently published co-authors were H. A. McKay (n = 12), M. Winters (n = 11), A. M. El-Geneidy (n = 7), J. A. Hirsch (n = 7), C. Lee (n = 7), R. Wasfi (n = 7), M. J. Koohsari (n = 6), D. T. Duncan (n = 6), K. R. Evenson (n = 6), N. A. Ross (n = 6), A. M. Chudyk (n = 5), A. V. Diez Roux (n = 5), T. Hanibuchi (n = 5), K. Oka (n = 5), T. Sugiyama (n = 5), and E. Talen (n = 5). Walk Score® research was published as part of a larger study in 48 out of 172 sources. In terms of the geographic landscape, research was most frequently conducted in the United States (n = 99), Canada (n = 39), Australia (n = 6), Japan (n = 4), and China (n = 3). The most frequent geographies of studies were locations within a single metropolitan/municipal area (n = 89), locations spanning multiple jurisdictions across a single country (n = 42), and locations within a single province/state (n = 28). Socio-demographically, population sample sizes for epidemiological studies varied widely, from n = 16 to n = 3.8 million. Taken together, these bibliometric and geographic characteristics indicate how studies employing Walk Score® were generated and diffused in the first decade after its launch, with a relatively high concentration of work among a small number of researchers and funding agencies in the United States and Canada, increasingly focused on health versus other areas of research.
List of References Extracted for the Walk Score® Scoping Review (n = 172)—Column Headings A: Year; B: Co-Authors; C: Category 1 ; D: Research Type 2 ; E: Walk Score® Format 3 ; F: Larger Studies 4 ; G: Funding Sources 5 ; H: Country; I: Sub-Region; J: Population(s)/Unit(s) of Interest; K: Sample Size; L: Primary Outcome of Interest; M: Other Variables of Interest 6 ; N: Statistical Analyses. 7

Column C—Category: H: Health; O: Other.
Column D—Research Type: 1: Epidemiological; 2: Empirical; 3: Tool Development; 4: Review; 5: Other.
Column E—Walk Score® Format: C: Combination; E: Euclidean; N: Network; U: Unspecified.
Column F—Larger Studies: 1: Active Streets, Active People Study; 2: ADOPT: Accumulating Data to Optimally Predict Obesity Treatment; 3: ALERT: Alberta Older Adult Health Behavior Study; 4: BATS: Bay Area Travel Survey; 5: BEAMS: Built Environment, Accessibility, and Mobility Study; 6: CAST: Communities and Schools Together; 7: CHBE: Community Health and the Built Environment; 8: Crew 450; 9: Cuban Health Study; 10: ESUM: Analyzing Trade-Offs Between the Energy and Social performance of Urban Morphologies; 11: Family Heart Health Program: Randomized, Controlled Trial; 12: HBT: Healthy Beginnings Trial; 13: HEBEJ: Healthy Built Environment in Japan; 14: HHL: Heart Healthy Lenoir Project; 15: HPSS: Health Promoting Secondary Schools; 16: InLUT: Integration of Land Use and Transport in medium-sized cities; 17: MASALA: Mediators of Atherosclerosis in South Asians Living in America; 18: MESA: Multi-Ethnic Study of Atherosclerosis; 19: National Study of Neighborhood Parks; 20: NCHRP: National Cooperative Highway Research Program; 21: Pathways to Health Project; 22: Pedestrian Accessibility and Attractiveness Indicators: Tool for Urban Walkability Assessment and Management; 23: PSID: Panel Study of Income Dynamics; 24: RECORD: Residential Environment and CORonary heart Disease; 25: Right Size Parking Project; 26: TRACCS: Transportation-Related Activities of Childhood Cancer Survivors; 27: TRACK: Transitions and Activity Changes in Kids; 28: Walk the Talk: Transforming the Built Environment to Enhance Mobility in Seniors; 29: Washington, D.C. Cardiovascular Health and Needs Assessment; 30: Watch for Me NC; 31: WHILLS: Women’s Health Initiative Long Life Study; 32: The YMCA–Harvard Afterschool Food and Fitness Project.
Column G—Funding Sources: 1: Not specified; 2: National Institutes of Health (NIH); 3: Centers for Disease Control and Prevention (CDC); 4: Robert Wood Johnson Foundation; 5: Canadian Institutes of Health Research; 6: National Sciences and Engineering Research Council of Canada (NSERC)/Social Sciences and Humanities Research Council of Canada (SSHRC); 7: Michael Smith Health Research BC; 8: Other USA Sources; 9: Other Canada Sources; 10: Other National Sources (Country).
Column M—Other Variables of Interest: 1: Age; 2: Household Income; 3: Education; 4: Anthropometric/Adiposity Measures; 5: Marital Status; 6: Sex; 7: Gender; 8: Race; 9: Ethnicity; 10: Employment.
Column N—Statistical Analyses: 1: Descriptive Statistics; 2: Linear Regression; 3: Logistic Regression; 4: Correlation; 5: Sensitivity Analysis; 6: Chi Squared Testing; 7: Analysis of Variance (ANOVA); 8: Other.
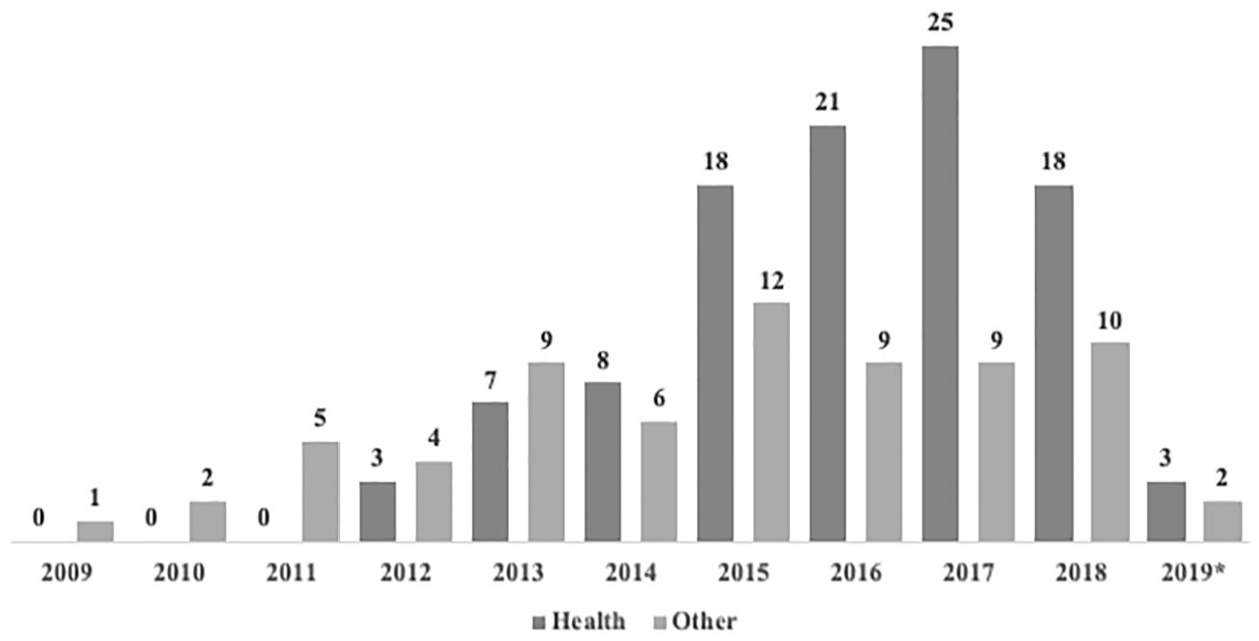
Frequency of Walk Score® publications from 2009 to 2018 by health or other categories of research included in the scoping review*.
Analytically, Walk Score® was employed as a variable of interest across studies in multiple formats: the Euclidean (traditional) measure was used in 24 studies, the network approach was used in 65 studies, and a combination of the two was used 3 times (n = 80 were unspecified or not applicable). In the “health” related articles, the most commonly studied populations were adults (n = 38), seniors/older adults (n = 15), neighborhood, region or census tracts (n = 12), adults or youth with chronic diseases or illnesses (n = 8), low income adults/older adults (n = 7), students or youth (n = 6), racial or ethnic minorities (in North America; n = 5), intersection, block or street segments (n = 2), residential/commercial addresses (n = 2), and other/not applicable populations (n = 8). In the “other” research category, samples mostly consisted of residential or commercial addresses (n = 15), neighborhoods, regions or census tracts within cities (n = 15), or samples of adults (n = 10), with other studies sampling records of home sales, mortgage interest rates or loan default frequencies (n = 5), and/or auditing intersection, block or street segments (n = 5). The most frequently assessed outcome measures were daily steps and leisure and/or purposive walking (n = 40), anthropometric measures (n = 21) (e.g., overweight and obesity, Body Mass Index [BMI], or cardiometabolic risk factors), and levels of physical activity (n = 9). The most frequently assessed demographic variables of interest across Walk Score® studies were age (n = 90), household income (n = 70), education (n = 62), anthropometric/adiposity measures (n = 47), sex (n = 46), race (n = 44), marital status (n = 36), employment (n = 31), gender (n = 27), and ethnicity (n = 19). Statistically, Walk Score® research most frequently conducted descriptive statistics (n = 125), linear regression (n = 62), logistic regression (n = 51), correlation (n = 42), Chi-squared testing (n = 18), sensitivity analysis (n = 13), Analysis of Variance (ANOVA) (n = 13), and other quantitative modeling or testing (n = 90). The analytic characteristics of the research activity indicate a primary focus on individual instead of community-level outcomes and characteristics influencing walkability, largely considered using quantitative instead of qualitative or other participatory measures and tools.
Discussion
Summary of Evidence
There was a large amount of variation in focus and scope across all of the Walk Score® publications included in our scoping review. Particularly we found a great variety in the bibliographic characteristics, the geographic landscape of research, the socio-demographics of populations studied, and the statistical analyses conducted. The publications ranged widely in sample sizes from a few with small participant groups engaged in community-based mixed methods research to others with large samples drawn from national household survey platforms. Most often studied populations were adults and seniors in the “health” research category, with some focus on individuals with illness or chronic disease. Both categories measured data at the regional, census tract, or neighborhood level, while the “other” research category sampled mostly at the residential or commercial address level or adults. Overall, the “health” research studies sampled human populations more often, while the “other” studies examined geographic characteristics, and data at the residential or commercial level. The scope of these study scales speaks to the generalizability, transferability, and accessibility of Walk Score® as a standardized walkability metric with application between diverse geographies. Unsurprisingly, most of the research was conducted in North American locations, which could simply be a product of the availability of Walk Score® in these locations. Walk Score® studies were also published as part of a larger study in many cases, demonstrating its applicability and utilization for a number of research inquiries. A few of these larger studies in the health-related research were focused on environmental (and other) correlates of chronic diseases or health status (e.g., heart disease, atherosclerosis, mobility, physical activity, safety; Barnes et al., 2016; Chudyk, McKay, et al., 2017; Hirsch et al., 2013). Some were large cohort or database studies (Brown et al., 2013, 2014; Smart, 2018), and others aimed to understand/reduce disparities in health related to race or socioeconomic status (e.g., D. T. Duncan et al., 2016; Méline et al., 2017; Taverno Ross et al., 2018). Although built environment was a common correlate in the larger studies, only two had larger goals to assess walkability (Moura et al., 2017; Slater et al., 2016). In “other” research, larger studies examined land use and travel patterns (Riggs, 2016; Rowe et al., 2013; Vale et al., 2016), obesity prevention, nutrition, and physical activity (D. T. Duncan et al., 2011; Nykiforuk et al., 2016; Schlossberg et al., 2015).
In terms of publishing trends, “other research” (e.g., real estate, policy, urban planning, business, transportation) was relatively more abundant (although still sparse) until 2014 when health research first predominated use of the Walk Score® metric—a trend that appears to be continuing. Researchers and funders are increasingly interested in Walk Score® as a proxy for walkability and the implications walkability could have on health and health behaviors; but behavioral changes during the public-health-restrictions phase of the pandemic reveal the importance of the social context of walking (Curtis et al., 2021; Paydar & Fard, 2021). This example and other system-level socio-political factors require researchers to reconsider how the metric was operationalized during the first decade of its use in research in order to apply it with a more sensitive contextual lens. Integrated into this increase in using Walk Score® to examine health related outcomes, the dependent variables or primary variables of interest along with covariates paint an important picture of research priorities and trajectories, calling into question assumptions, equity, and the limitations of the measure in context. The research picture generated in this review shows that Walk Score® researchers are increasingly interested in the relationships to health variables like physical activity and obesity, but that the intersections of critical determinants and contextual factors like privilege, gender, and socio-economic and political access are not always examined. Suggestions for future intersectional work in this area, based on the information mapped in this scoping review could help bridge these gaps in health promotion applications of Walk Score®.
Walk Score® Research Applications in a Dynamic Social Context
In examining Walk Score®, we envision researchers beginning to consider pedestrians as more active participants in the social space. For example, shifts in travel demand after the public health restriction-intensive phase of the pandemic contributed to changes in active mobility and the built environment in terms of the spatial adaptations that stay-at-home mandates, limits on social gathering, and remote options for work, shopping and other activities have encouraged (Curtis et al., 2021; Salon et al., 2021). In this scoping review, we aimed to examine the first decade of Walk Score® use in peer-reviewed studies, to map research activities and understand how the measure might better capture health and other outcomes in the next decade or more of socio-spatial adaptations in walking. Walk Score® indeed examines accessibility of destinations to walk to, but as evidenced by the inclusion of other geographic, socio-demographic, and behavioral variables, and the mixed or unexpected relationships in the literature (e.g., without critical appraisal of the evidence, we note studies finding that crime is related to higher walk scores, and others where adiposity measures are negatively related to Walk Scores®) there is clear need to include more contextual information.
In the case of physical activity as an outcome (and often a proxy for health and/or weight loss), Walk Score® has often been related to walking for transport, but not recreational walking (Chiu et al., 2015; Chudyk, Sims-Gould, et al., 2017; Collins et al., 2018; Hajna et al., 2015; Hirsch et al., 2013; Hirsch, Roux, et al., 2014; Koohsari, Sugiyama, Shibata, et al., 2018; McCormack et al., 2017; Taverno Ross et al., 2018; Thielman et al., 2015; Tuckel & Milczarski, 2015; Y. Yang & Diez-Roux, 2017) as may be expected in a measure of destination-based access. Especially given the shifts in destination-based walking during the height of the pandemic (Hunter et al., 2021; Paydar & Fard, 2021; Salon et al., 2021), these results should be considered in relation to the geographic and socio-demographic characteristics of an area (and consider system-level factors in addition to individual factors affecting the agency of pedestrians themselves). For example, residents in smaller or rural population centers may engage in less walking for transport compared to urban centres, possibly due to lack of built environment features, amenities, or personal preference (Doescher et al., 2014; Frost et al., 2010; Nykiforuk et al., 2016; Schasberger et al., 2009; Thielman et al., 2015). Indeed, some studies examining the effect of Walk Score® on total physical activity or recreational walking found positive relationships, not accounting for the quality of evidence in those studies (Han et al., 2018; Méline et al., 2017; Thielman et al., 2016; Wasfi et al., 2017). However, some studies examined only total physical activity minutes, steps, or accelerometer data, and found negative or null relationships between physical activity and Walk Score® (Reid et al., 2017; Riley et al., 2013; Thielman et al., 2015). Without charting specific sources of measurement in the studies, these inconsistent results could be an effect of physical activity measurement (e.g., self-report), but could also be due to unmeasured covariates contributing to physical activity behavior, or predominantly cross-sectional study designs. For example, Jilcott Pitts et al. (2013) found that Walk Score® was positively related to crime, BMI percentile, and heart rate, and inversely associated with moderate to vigorous physical activity among urban youth, demonstrating that a higher Walk Score® does not invariably lead to better health outcomes. Future Walk Score® research should contextualize studies by providing a thorough treatment of socio-spatial context, situating more quantitative analysis in a well-theorized representation of the pathways through which walking and walkability outcomes occur.
Reconsidering Walk Score® and the Problem of Weight Stigma
Overweight and obesity or BMI were the main outcome variable used in 18 studies, with anthropometric/adiposity measures (including BMI) as a variable of interest in 47 studies. Clearly, weight and adiposity are considered important variables in Walk Score® research. The research we reviewed was mixed regarding the relationship between Walk Score® and overweight and obesity or BMI. Some studies found no relationship (G. E. Duncan et al., 2015; Qu & Li, 2004; Sriram et al., 2016; Y. Xu et al., 2015; Y. Xu & Wang, 2015a), some a negative relationship (Chiu et al., 2015; Hirsch, Roux, et al., 2014; Jilcott Pitts et al., 2012; Koohsari, Kaczynski, et al., 2018; X. Li & Ghosh, 2018; Loo et al., 2017; Méline et al., 2017; Smart, 2018; Wasserman et al., 2014; Y. Xu & Wang, 2015b), and some found that the relationship between Walk Score® and BMI was partially mediated by physical activity (Horn et al., 2015; Koohsari et al., 2019). In a review of objectively measured walkability and active transport, results on weight related measures were inconsistent (Grasser et al., 2013). On the surface, it may seem ‘intuitive’ that more walkable neighborhoods could lead to lower body weights, but the current research does not appear to support this hypothesis. In illustration, McCormack et al. (2018) found a negative relationship between Walk Score® and waist circumference, but those in disadvantaged neighborhoods were more likely to have higher health risk due to waist circumference and BMI, compared to more advantaged neighborhoods. Interestingly, in this study those in socioeconomically disadvantaged neighborhoods had significantly higher Walk Scores® compared to advantaged neighborhoods (M = 63.0 vs. M = 56.9).
One main issue with studies examining walkability and BMI is lack of research designs capable of establishing causality. One longitudinal study found neighborhood walkability may influence BMI trajectory for men, but not women (Wasfi, Dasgupta, Orpana, et al., 2016). In the two twin studies in our review (G. E. Duncan et al., 2015; Horn et al., 2015), both identified small relationships between Walk Score®, physical activity, and BMI, but did not demonstrate a causal link between Walk Score® and BMI, showing that people with lower BMIs may choose to live in highly walkable areas and the strong link between genetics and BMI.
Public health researchers and policymakers have consistently relied on the “obesity epidemic” to justify examining overweight and obesity or BMI as research outcomes, yet the underlying assumption that lower weight equals better health is largely unfounded and potentially harmful, due to weight stigma, and lack of attention to issues like poverty and mental health that may be influencing health outcomes (Hunger & Tomiyama, 2015; Hunger et al., 2020). Health promotion researchers and practitioners have a responsibility to examine their own assumptions and how they may contribute to weight stigma and other forms of stigma that exist in our research and policies. Furthermore, establishing evaluation and design for walkable spaces can exacerbate weight stigma and exclusion of many body types in terms of the variables deemed important and environmental features such as availability and design of seating along walking routes, and path or sidewalk width (Pritchard, 2014). As noted above, walkability metrics that focus on presumably objective factors (e.g., distance and destinations) do not account for the myriad of social environmental and experiential factors that may influence the behaviors of would-be pedestrians, such as perceived safety, level of crowding and vehicle traffic (Liao et al., 2019), or what constitutes a walkable space according to socio-cultural factors. Over the next decade of Walk Score® research, greater attention to transforming social spaces for inclusivity could begin to address this issue, as we examine our assumptions about health, our environments, and walking behavior, on the whole.
Examining the Risks of Walk Score® for Socioeconomic Othering
When examining the multitude of factors that may influence the relationships between Walk Score® and health related variables, the emphasis on built environment versus social features of communities may result in interventions that benefit those already privileged while ignoring the needs of disadvantaged groups (e.g., through gentrification or displacement; Adkins et al., 2017; Knight et al., 2018). In their review of relationships between built environments and socioeconomic context, Adkins et al. (2017) note that fear of crime and lack of social support may contribute to those in disadvantaged groups walking less in supportive built environments compared to advantaged groups, and they call for walkability definitions and measurement to be inclusive of a range of social and physical barriers. Other researchers found that Walk Score® as a proxy for walkability was not as strong in less affluent neighborhoods (Koschinsky et al., 2017). Other factors may also contribute to unexpected outcomes related to Walk Score® such as automobiles acting as a status symbol, making walking for transport less attractive (Langlois et al., 2016), or attitudes towards walking (Y. Yang & Diez-Roux, 2017). Another review challenged researchers to consider adapting indicators of walkability to groups with different abilities, ages, and lifestyles (Rišová, 2020). Furthermore, Rišová (2020) suggested moving away from studying health related outcomes to improve diversity in the walkability research space. The integration and connection between health-oriented research and other research could be an important avenue for future Walk Score® applications, particularly in light of societal changes that may necessitate new consideration for the environments, systems, and technologies of walking.
Placing Walk Score® in an Intersectional Context
Intersectionality is a way of operationalizing subjectivity as resulting from an individual’s complex and overlapping identities, each subject to various structures and influences with cumulative and compounding effects (Carbado et al., 2013). Walking behaviors can be addressed in an intersectional context across a variety of indicator and outcomes. Some common outcomes related to Walk Score® in “other research” included objective or perceived neighborhood qualities (Bereitschaft, 2017b; Lo & Houston, 2018; Schlossberg et al., 2015; Talen et al., 2015; Yin & Wang, 2016), access inequality to walkable neighborhoods (Bereitschaft, 2017a; Bielik et al., 2018; Koschinsky & Talen, 2015, 2016), tool development or validation (Carr et al., 2010, 2011; D. T. Duncan et al., 2011, 2013; Koohsari, Sugiyama, Hanibuchi, et al., 2018; S. Lee et al., 2013; Nykiforuk et al., 2016), commercial or residential property value or sale prices (Boyle et al., 2014; El-Geneidy et al., 2016; Gilderbloom et al., 2015; Knight et al., 2018; Kok & Jennen, 2012; W. Li et al., 2014; Petheram et al., 2013; Pivo & Fisher, 2011; Rauterkus & Miller, 2011; M. Xu et al., 2018; L. Yang et al., 2018; Yin et al., 2015), risk of mortgage default (Gilderbloom et al., 2012; Pivo, 2014; Rauterkus et al., 2010), sustainable travel (Halat et al., 2015; Langlois et al., 2015; Manaugh & El-Geneidy, 2012; Mattson & Godavarthy, 2017), and perceptions of walkability (Bereitschaft, 2018, 2019). Some of these outcomes can certainly impact a person’s health with respect to individual behavior, financial security, or selection of a place to live or work (Glenn & Nykiforuk, 2020; Rišová, 2020). Importantly, many of the “other” research papers have already begun to address important issues related to walkability previously mentioned including equity (Knight et al., 2018; Riggs, 2016), and how walkability is defined and measured (Forsyth, 2015). By drawing on insights being developed in other research disciplines, public health researchers can develop meaningful inferences to incorporate more intersectional perspectives for further Walk Score® related research examining health related outcomes.
The Path Forward in Walkability Research Using Walk Score®
The present scoping review has demonstrated the potential of Walk Score® as a measure of accessibility and shows it may be considered a useful predictor of walking for transportation or utility. Walk Score® is accessible and presents researchers with ample data to apply in various contexts, at least in countries like the United States and Canada, where it is widely available. One limitation of this destination-based metric in health promotion research that has become apparent, however, is the broad context in which Walk Score® is used to examine behavior and health outcomes. Considering another aspect of the global COVID-19 pandemic, destinations one might usually walk to became less available to pedestrians due to closures, occupancy limits, and concern for safety and welfare, with some destinations becoming more appealing such as parks or green spaces (Curtis et al., 2021). Battista & Manaugh (2018) found that walkability instruments largely failed to account for variations in behavior and perceptions (such as occurred during and now emerging from the pandemic) and some research demonstrated that perceptions of walkability may differ from Walk Scores® overall (Bereitschaft, 2018). Some researchers have responded to these limitations by developing models of walkability that account for different pedestrian types such as children, seniors, and impaired pedestrians, although these are limited in their intersectionality as noted above (Moura et al., 2017). Others have augmented measures using the street network (which measures automobile mobility) to include subjective pedestrian attributes like safety features along school routes for children from the views of their parents (Schlossberg et al., 2015). Researchers have also noted important features like fewer parking lots and setbacks in addition to tree-coverage, which predicted walking over and above Walk Score® (Herrmann et al., 2017). Although Walk Score® includes park space as a destination in their calculation, researchers interested in the health outcomes of built environments noted the importance of green space in affecting health outcomes along different pathways than walking as measured by Walk Score® (Jia et al., 2018). While Walk Score® can be a useful metric that adds nuance to walkability research, health promotion researchers using Walk Score® should be cognizant of the limitations of the measure in addition to their own assumptions when asking research questions (Stephens, 2010), and consider it one tool among many important factors contributing to walkability in an intersectional and situated context.
Strengths and Limitations
This scoping review expanded on previous Walk Score® reviews and followed the PRISMA-ScR reporting guidelines (Tricco et al., 2018). In addition, while we did not conduct a critical analysis of articles, we excluded research from predatory journals after contacting PRISMA-ScR co-authors for guidance on this issue. Journals were deemed predatory following review by the research librarian, who evaluated questionable journal websites on several criteria from a Predatory Publishing Worksheet developed by health librarians. Although the review was limited by retrieving only literature published in English, we consider that Walk Score® research is currently produced mainly in this language, even in non-English speaking countries. The “health” and “other” categories we used suited the purpose of reviewing the literature from a public health perspective, but our categories could have been further refined to typify different health research designs and approaches, particularly for methodological and disciplinary differences. Additionally, the data extraction was created to suit the health-related studies, and therefore some of the nuances in the “other” research may have been missed. Finally, the dataset was created and analyzed prior to the COVID-19 pandemic. Shifting social patterns of individual, neighborhood, municipal, and larger-scale travel behaviors post-pandemic may have widespread effects on population health, with our research providing insight into conceptualization of Walk Score® as a research metric, prior to a major transformation in the context of walkability. However, we consider this snapshot of the first decade of operationalizing Walk Score® in research to be a valuable tool for bringing Walk Score® into the next decade—and, perhaps, growing sophistication of—walkability research, building on a comprehensive map of activities across 172 studies published from 2007 to 2018.
Conclusion
Walk Score® presents important information that supports a geographic summary of our built environments. The literature using this measure in public health applications is still limited in its predictive ability and is quite varied in terms of outcomes measured and how Walk Score® is utilized. Regardless of their research questions, approaches, and methods, researchers applying Walk Score® should be aware of the strengths and limitations of this tool to apply it with appropriate caution. Particularly, when examining physical activity, it is important to consider which types of activity are most relevant, and contributing factors from the social environment. Health outcomes related to Walk Score® could be considered more broadly than simply looking at body weight, to support analysis of intersecting physical, social, and psychological factors. Researchers should consistently examine how certain outcome variables are situated within the larger, intersectional socio-cultural context, and how important socio-demographic variables contribute and could interact with Walk Score® to draw more meaningful and less problematic conclusions about how our dynamic and transforming social and political environments impact our health.
Footnotes
Acknowledgements
The authors would like to acknowledge Hannah Mercador, Dana Tschritter, and Nathanael Skagen for their work in data extraction for analysis.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CIJN received support as an Applied Public Health Chair from the Canadian Institutes of Health Research in partnership with the Public Health Agency of Canada and Alberta Innovates—Health Solutions (2014–2019; CPP 137909). The funders had no role in the study design; collection, analysis, or interpretation of data; manuscript preparation; or decision to submit the manuscript for publication.