
Abstract
The article examines the media discourse of risk and stigma which developed in response to the COVID-19 pandemic in India, employing the theoretical frameworks of Mary Douglas and Erving Goffman. Accessing the Factiva database archive, the authors analysed a total of 139 stigma-linked media reports, using the Discourse Network Analyzer (DNA) to identify thematic groups of beliefs and related actors contributing to the risk discourse on the contagion. The results exhibit a clear difference in opinion on various stigma-related beliefs among the individuals diagnosed or assumed susceptible to COVID-19, including the issue of disclosing identities. In India, domestic actors have dominated the media discourse, particularly national government agencies, rather than intergovernmental organisations or foreign governments. The media content analysis in this article shows that new hierarchies have emerged based on confirmed or suspected contact with the disease along with reinforcement of traditional myths and superstitions, leading to discrimination against the quarantined individuals, their families, healthcare staff and socially marginalised communities.
Introduction
Risks are central to social discourse on health as they test the endurance of social cohesion. In 2020, COVID-19 poses a new risk to the world in four unique ways. First, there are still uncertainties regarding the causes and consequences of the disease. Second, the disease is highly contagious and spreads easily from one person to another. Third, a cure is presently not available, and management of the disease requires expensive facilities. Fourth, the use of facemasks, sanitisers, personal protective equipment and handwashing gets ritualised and normalised to the extent that their absence contributes to stigma. 1 Moreover, the large and increasing number of deaths attributed to COVID-19 is a significant cause of fear and anxiety. With broad implications for health and socio-economic well-being, COVID-19 has turned itself into a mega risk, which, like other infectious diseases, generates stigma based on socio-cultural representation of ‘knowledge, experience, attitudes, norms and behaviours’ (Singer, 2015: 37). During health crises, existing stereotypes and beliefs play a vital role in guiding human action (Link and Phelan, 2001: 363), which needs a cultural contextualisation of actors and organisations facilitating discourses from their respective social vantage points.
Focusing on India – which had the third-highest number of confirmed COVID-19 cases in the world by the end of the first week of July 2020 (Johns Hopkins University, 2020) – our study uses India’s diverse socio-economic profile and multipronged hierarchical structures to explore the actor-guided trajectory of risk perception and stigma generation during a novel disease encounter. Using the case of COVID-19 in India, this study investigates the actor–belief relationship of risk and stigma through three research questions: (1) What are the major stigma-linked beliefs related to COVID-19? (2) How do different actors and organisations converge in or depart from such beliefs? and (3) How are these actors and beliefs embedded in the socio-political hierarchies in India? With the established inequitable effects of socio-economic factors like wealth, caste, education, gender, religion and urban/rural residence on the health of Indian population (Subramanian et al., 2008), this study seeks to explore the associations of those factors for COVID-19, through a content-based qualitative enquiry gleaned from news media discourses. The article uses Douglas’s (1992) 2 cultural symbolic perspective of risk and blame to evaluate the agreements and disagreements with the prevalent notions of stigma, connected to one’s social position. The later sections of the article use Goffman’s (1963) interactionist perspective of stigma to identify and situate the stigma narratives within operational and emerging social hierarchies linked to risk of the virus.
Situating COVID-19 within a sociological framework of risk and stigma
COVID-19 has emerged as an unprecedented global crisis. Caused by a novel virus strain called ‘severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)’, the disease is known within the scientific community for its highly contagious nature and uncertain behaviour, giving rise to fears and suspicion among global populations (Varshney et al., 2020). With its high proliferation rate, the virus appears indiscriminate in choosing human hosts; however, studies have confirmed COVID-19’s disproportionate effects across populations based on ethnicity, race, gender, age, education, marital status, migration, minority and class (Drefahl et al., 2020; Kantamneni, 2020; Kirby, 2020; Roberto et al., 2020). Because the spread of infection is a function of ‘biological, social, cultural, and environmental factors’ (Singer, 2015: 35, 37), a social framework of risk analysis is necessary to complement the scientific enquiries for disease prevention and control. ‘Cultural theory’ (Douglas, 1992), ‘reflexive modernisation’ (Beck et al., 1994) and institutional marginalisation of the vulnerable and deprived by the attribution of ‘risk’ to its members (Lupton, 1999) are some broadly used perspectives in risk studies. As this article employs ‘stigma’ itself as a risk for society, Goffman’s (1963: 7) idea of stigma as a ‘discrediting attribute’ complemented with Douglas’s (1992) socio-political conceptualisation of risk and blame has been used to locate COVID-19 within the hierarchical social fabric of India. The inclusion of power as a tool for maintaining social hierarchies, within the framework of stigma, is expected to overcome the limitations of the ‘apolitical and ahistorical’ nature of Goffman’s work (Parker and Aggleton, 2003; Tyler and Slater, 2018).
The social configuration of stigma to an infectious disease is highly contextual. The borders created between the discredited (known stigma), the discreditable (unknown or concealed stigma) and the normal (without stigma) are contingent upon the moral norms that guide behaviour in different social situations (Goffman, 1963: 42). In the context of communicable diseases, such status ascriptions are common, and they are regulated by both formal and informal means of control, where authorised functionaries, including government, exercise the former, and the latter involve public participation in stigmatisation.
In the COVID-19 pandemic, the invisibility of the virus has played a significant role in stimulating a cultural assessment of risk by encouraging ‘trait-based attributions . . . drawn from social categories and stigma associated with outgroup members’ (Roberto et al., 2020: 372). Similarly, a close resemblance has been observed between the stigmas associated with infectious diseases such as HIV/AIDS, SARS and COVID-19 – especially with regard to conferring blame on the ‘foreign “other”’ (Eichelberger, 2007; Lichtenstein, 2008; Logie, 2020; Pescosolido and Martin, 2015: 89–91). All these cases of infectious-disease stigma rely on a binary between the ‘normal’ and the ‘other’ in the form of a culturally defined negative attribute or stigma to pass blame through social positions of power and control.
In her work on risk and blame, Douglas (1992: 8) states that ‘humans have a scope for politicised reading of danger and cognition’ in which they use blame as a tool for control. This power is exerted from dominant social positions by creating contrasting categories such as ‘clean’ and ‘unclean’ or ‘pure’ and ‘impure’ in order to maintain social order and societal stability (Douglas, 1966). For example, ‘dirt as a disorder’ is a socially constructed category and a moral code for most societies around the world. An association with ‘dirt’ invites social procedures of cleanliness or isolation, similar to Goffman’s (1963) ‘discredited’ category. Another example is the taboo of menstruation as a form of pollution in India – a stigma which myths and religion sanctify in order to reassert patriarchal domination (Narasimhan, 2011). Similarly, infection is a ‘real’ danger which invokes blame as a political tool for assigning danger to others, especially already disadvantaged groups (Douglas, 1992: 28, 34, 84). For example, HIV/AIDS patients are often assumed to have multiple sexual partners, which society does not accept. Such a conception is often used as a tool for blame, deriving from fear of infection, and labelling as ‘deviant’ and ‘anti-social’ to marginalise disease patients (Alonzo and Reynolds, 1995). In this way, the language of defining threats aims to portray and preserve existing hierarchies and power structures (Nelkin and Gilman, 1988: 376), which are deeply entrenched in Indian society.
Previous research on health and stigma in India has focused on institutions – such as caste, class and gender – influencing Indians’ health-seeking behaviour (Luke and Munshi, 2007; Nebhinani et al., 2012). The risk of social ostracisation among leprosy patients (Barrett, 2005) and HIV/AIDS patients (Bharat, 2011) in India demonstrates the infectious diseases’ profound social implications. However, the literature seldom assesses stigma and blame within a risk framework in the Indian context and there is a dearth of research based on Indian media discourse of stigma. Therefore, we analyse India’s news media in order to identify beliefs and associated actors involved in generating and transmitting stigmatising narratives. Moreover, we aim to evaluate the role of new and old social hierarchies in stigma generation. Thereby, this study not only contributes to the literature on social encounters and novel virus infection but will also help develop strategies for policies and effective risk communication during health pandemics such as the COVID-19 outbreak.
Materials and methods
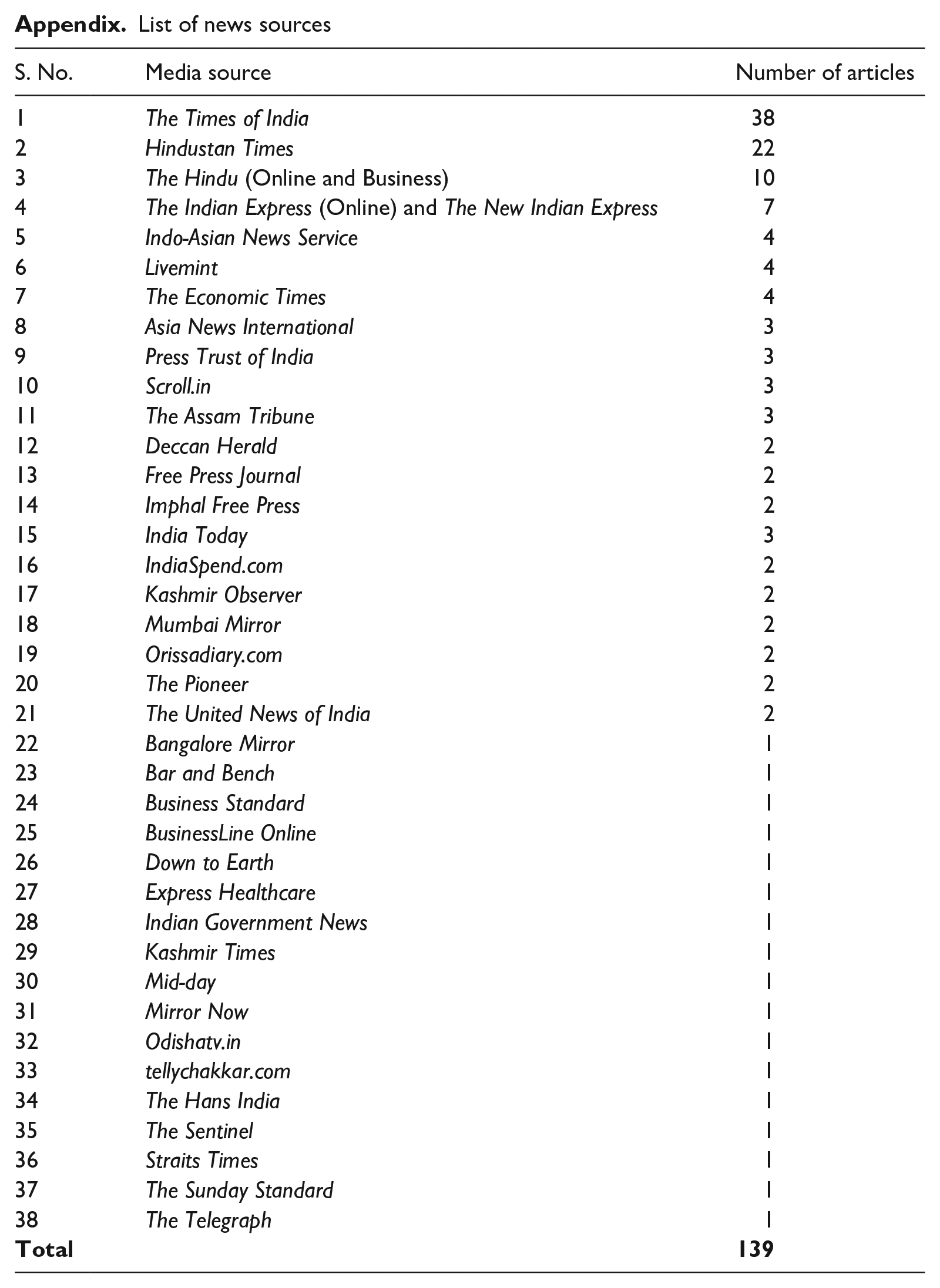
To address our primary research questions, we analysed media content and discourse network data from 38 different online news sources in India 3 (see Appendix). Some of these news sources are published across India (such as The Times of India) while others have a regional focus (such as Orissa Diary and the Kashmir Times). The data were obtained from the Factiva database of English-language online media using the keywords 4 ‘covid’ and ‘stigma’ (both words included in headlines and lead paragraphs) for the first two consecutive lockdown periods in India, between 25 March and 3 May 2020. 5 We obtained a total of 161 stigma-associated reports, which we further reduced to 139 reports after eliminating duplicates. This was followed by conducting two different levels of analysis: discourse analysis and media content analysis.
Discourse analysis was employed to extract discourse statements or belief narratives from each news report, expressing the position of a person or organisation on a COVID-19 related topic in comparison to the other identified actors, with or without any direct communication. The news articles were imported into Discourse Network Analyzer (DNA) (Leifeld, 2017), a software that uses statements as its unit of analysis (Kukkonen et al., 2017: 717). There can be multiple statements within a single article, in a paraphrased or a direct quotation form. The coding 6 of a statement used five attributes:
Person: the individual who made the statement.
Organisation: the organisational affiliation of the person.
Concept: summarise a viewpoint or belief expressed by the actors.
Dummy variable 1: indicates the person’s and/or organisation’s agreement or disagreement with the concept.
Dummy variable 2: records whether the person experienced stigma due to the pandemic or not. Based on this criterion, the article classifies the identified actors into two categories: (a) perceived-positive and (b) perceived-negative. The former category refers to the individuals positively diagnosed with COVID-19 or those facing stigmatisation due to their suspected association with the disease. The remaining actors expressing their beliefs on COVID-19, but not meeting the ‘perceived-positive’ criteria as mentioned above, were categorised as ‘perceived-negatives’.
An example of coding of a direct statement from a news report reads: Union Health Minister Dr Harsh Vardhan too acknowledged the problem posting a tweet on Tuesday evening. ‘I am deeply anguished to see reports pouring in from Delhi, Noida, Warangal, Chennai etc that doctors & paramedics are being ostracised in residential complexes & societies. Landlords are threatening to evict them fearing #COVID2019 infection. Pls don’t panic!’ (The Times of India, 2020a)
The coding was done as: (1) Dr Harsh Vardhan, (2) Union Health Ministry, (3) the concept category ‘COVID association causes stigmatisation’, (4) ‘agreement’ with the concept, (5) perceived-negative.
Two research personnel double-coded 20% of the articles independently, based on an initial corpus of concepts, to obtain inter-coder reliability. A total of 332 statements were extracted – attributing to 129 persons and 99 organisations – and coded into 13 statement categories (‘concepts’). After coding the one- and two-mode data matrix in DNA software, we exported the matrix to Visone network visualisation software (Brandes and Wagner, 2004), which creates a pictorial representation of the networks extracted from the DNA data.
The penultimate section of the article, ‘Hierarchies of COVID-19’, uses media content analysis as a method for analysing the news media data (Hainsworth et al., 2020). This method uses media discourses to generate codes, concepts and themes related to the research objectives, and analyses the resulting analogies using qualitative or quantitative interpretation. In this article, all 139 reports in the database were individually scrutinised for statements on COVID-19 stigma-based incidents and events, and categorised into observed themes: (a) traditional stigma, including codes ‘medical history’, ‘identity’, ‘myths and superstitions’; and (b) new hierarchies, including ‘marking and symbolism’, ‘lack of reverence for the dead’ and ‘severance of social ties’. The selection of stigma incidents was contingent upon media portrayal of ‘stigma’ as well as the experiences and worldview of the identified actors who perceive and label a certain event, person, or object as stigmatised.
COVID-19 related beliefs and stigmatisation in India
Every culture has unique sets of beliefs with elements of stigmatisation – ‘labelling, stereotyping, separation, status loss, and discrimination’ (Link and Phelan, 2001: 363). These elements demarcate a person’s social identity as superior or inferior, based on different social situations. Media and socio-cultural systems of information transmission – such as language, symbols and communions – play a central role in generating and strengthening beliefs, which transform into social action.
Based on the individual cases of COVID-19 reporting in Indian media, our study observed four prominent categories of stigma-based beliefs (Table 1):
1. Perceived risk-related beliefs (n = 205): contain statements which elicit cultural interpretation of risk due to fear of infection and resulting stigmatisation. An example of the most common belief under this category, ‘COVID-19 association causes stigmatisation’, reads:
. . . the villagers are scared. They think that I have brought the virus along with me. I am telling them that I have been tested three times, but they won’t listen. (Ghosh, Scroll.in, 2020)
2. Beliefs related to fear of disclosure (n = 55): encapsulate varying opinions on the preservation of the identity of COVID-19 diagnosed individuals. An example narrative of the belief ‘COVID-19 reporting to hospitals is stigmatised’ is:
‘But villagers are hiding their fever because of fear that they will be quarantined. The stigma attached to the novel coronavirus also contributes to their reluctance to consult doctors,’ said the MLA. (The Telegraph, 2020)
3. Beliefs related to traditional/existing prejudice (n = 13): reinforce the existing norms of discrimination in society at the time of pandemic. For example, a social activist from Punjab said:
There are over a hundred Gujjar families living in this area . . . A few days ago, some people made announcements from the gurdwaras and temples asking people not to buy milk from Gujjars claiming they spread the deadly virus. (The New Indian Express, 2020a)
This belief affirms the viewpoint of the villagers in Punjab, that ‘Muslims spread COVID-19 infection’.
4. Beliefs related to care and support (n = 42): the beliefs about the role and efficacy of government. The statement,
Madurai collector Dr TG Vinay said he visited the discharged patients in the city on Sunday and assured them that the administration would offer its full support in ensuring communal harmony. (Ramakrishnan, 2020)
exemplifies the concept ‘Government bodies support perceived-positives’ under this theme of ‘beliefs related to care and support’.
COVID-19 stigma-based beliefs of the perceived-positives and the perceived-negatives.
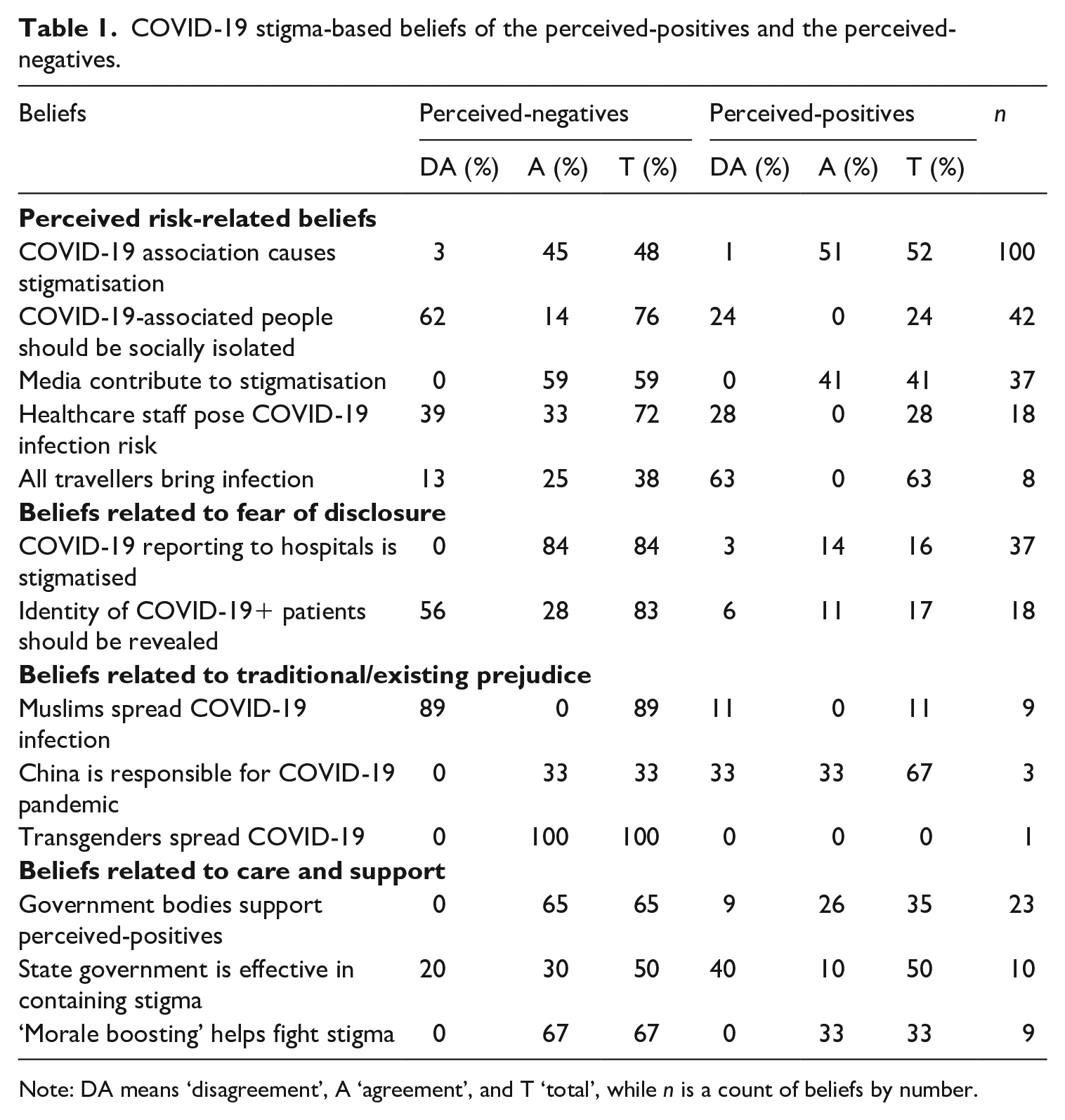
Note: DA means ‘disagreement’, A ‘agreement’, and T ‘total’, while n is a count of beliefs by number.
Our results display an interesting relationship between risk perception and stigma generation for the COVID-19 spread in India. A majority of people recognise COVID-19 association, symptom reporting in hospital and the role of media as stigmatising in nature, because all these possess a risk of disclosure of identity which might lead to social discrimination. This could be one reason why a majority (56%) of the perceived-negatives disagree with the disclosure of identities of COVID-19 patients.
Our study revealed that during the lockdown in India, social media contributed to perceived-positives’ shaming, circulating the contact information of suspected or quarantined people, vilifying them as a ‘super-spreader’ in video streams and false messages. Such stigmatising behaviour was also observed locally in state authorities’ use of ‘stickers’ on gates to mark confirmed COVID-19 cases. Some people who resisted the use of these stickers or removed them from their gates were penalised under the Epidemic Diseases Act 1897, 7 which empowers state governments to ‘take special measures and prescribe regulations as to dangerous epidemic disease’ (The Hindu Online, 2020). A study conducted on Twitter circulation of coronavirus information revealed that ‘false information is tweeted more but retweeted less than science-based evidence’ (Pulido et al., 2020: 377). Therefore, the state plays a major role in the public sphere in determining the flow of information and stigma. Our findings (Table 1) highlight that although government bodies support the perceived-positives, four out of five reported that the state governments are not efficient in containing stigma and that ‘morale boosting’ by the state can go a long way in extending support to fight stigma. India, where state bodies have maximum representation in stigma-linked media reports, promotion of identity disclosure of the confirmed patients hints at the ‘strategic deployment of stigma’ (Parker and Aggleton, 2020: 18) by the state, inciting discrimination. There was one case in agreement with the belief ‘transgenders spread COVID-19’ (Table 1). Similarly, although all reported cases in our study denied the role of Muslims in spreading infection, in congruence with other studies on COVID-19, racial discrimination against the people from northeastern India was observed due to their perceived East Asian features, particularly closer to the Chinese population, by identifying them as virus spreaders (Haokip, 2020; Kipgen, 2020). Thus, the traditional or existing prejudices in society based on religion, ethnicity and sexuality played a role in promoting stigma-based discrimination in India.
In addition to the above findings, a significant reduction in risk perception towards healthcare staff and travellers was observed by the people experiencing stigmatisation as compared to the perceived-negatives. This contrasts with the findings of Dryhurst et al. (2020: 998), who claimed that direct personal experience with the virus increases risk perception amongst the perceived-positives.
An actor-based analysis of the beliefs that emerged in the study underscores the relevance of social constructions in risk perception and assignment of blame for the perceived risk using the available socio-cultural hierarchies. This stigmatising construction and circulation of local knowledge on the novel coronavirus jeopardise timely symptom reporting at medical institutions. Goffman (1963) calls these mechanisms ‘techniques of information control’, whereby discredited or discreditable individuals obliterate or conceal stigmatising information about themselves in order to avoid discrimination. Overall, in the study, stigma’s social roots were found as the leading causes of discrimination, followed by psychological, material and economic factors. In this context, identifying the actors who were responsible for generating these stigmatising beliefs is pertinent.
Actors and risk discourses
Discourse plays a central role in risk studies, not only revealing risk perception at different stages of a risk’s proliferation but also reflecting stakeholders’ engagement at varying levels of power within a social setting. This article uses media to assess stigma-based information in order to extract relevant discourses and actor profiles and study the points of disjuncture as well as consensus between various identified groups. Our study revealed a total of nine actor categories (see Table 2): government (n = 69), hospitals (n = 29), civil society (n = 23), health institutions and associations (n = 19), business (n = 13), research organisations (n = 5), intergovernmental organisations (n = 4), political parties (n = 4) and foreign government (n = 3). These contain organisations and groups asserting their distinct standpoints about the coronavirus based on their beliefs, experiences, perceptions and knowledge.
Actors in the discourse network of COVID-19 stigma and risk-related beliefs in India.
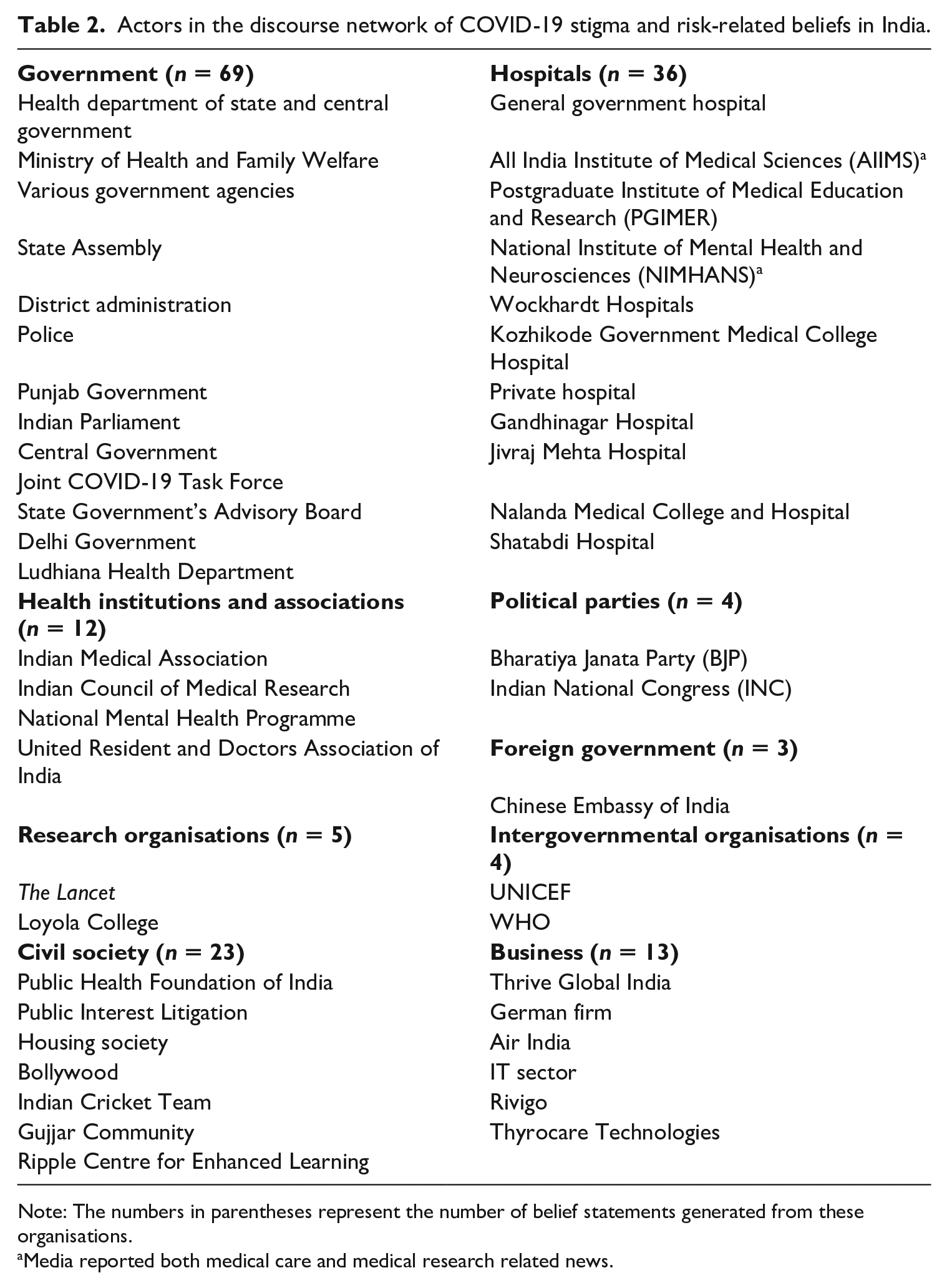
Note: The numbers in parentheses represent the number of belief statements generated from these organisations.
Media reported both medical care and medical research related news.
A discourse analysis of media reports revealed significant underreporting (4 out of total 169 cases) of international bodies, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF), which are playing an active role in risk communication about COVID-19 across the globe, as compared to the national groups and organisations. Amongst the national actors, the state government reports (n = 50), state assembly, district administration, police, state government health departments and advisory boards, etc., got more media attention as compared to the reporting from the central government actors (n = 19), the Ministry of Health and Family Welfare, Indian Parliament, Joint COVID-19 Task Force, etc. Overall, the representatives from several national health institutions belonging to the different identified categories of government (national and state ministries and health departments), hospitals, health institutions and associations, research organisations and civil societies registered the most reporting through media. Amongst hospitals, an equal representation was observed of both public and private sector professionals (such as doctors, nurses and medical testing staff) who shared their experiences and views on COVID-19 stigma. Among health institutions, the Indian Medical Association (n = 6) was most active on news media, sharing insights on issues of mental health, myth-busting and stigmatisation of healthcare workers. Similarly, within civil society, the voices of various NGOs (n = 8), lawyers (n = 6), housing societies and local communities (n = 5) and celebrities (n = 4) proliferated on several media platforms.
Stigma is a risk in itself for society because it increases the burden of a disaster for already marginalised populations. Grouping various actors together based either on commonalities in their beliefs or disagreements with the conflicting notions of other actors, especially in the context of a virus that is capable of infecting anyone, significantly explains existing and emerging polarisations in the Indian society during the crisis. This study analysed the discourse network of Indian media statements relating to COVID-19 to identify intersections and diversions in beliefs among the stakeholders. While we obtained a large consensus for the statements ‘COVID association causes stigmatisation’, ‘COVID reporting is stigmatised’ and ‘media contributes to stigmatisation’, there were four highly contentious beliefs related to stigmatisation in India (Figure 1).
First, there is the notion about healthcare staff as a potential carrier of SARS-CoV-2. In contrast to research organisations, governments, hospital authorities, civil societies and a business firm, the primary networks of healthcare staff – including housing societies and co-workers in hospitals – perceived healthcare workers as health risks (Figure 1A). The second most prominent conflict was linked to the risk of disclosure of the identities of COVID-19 patients (Figure 1B). While the state governments held mixed opinions on the concept, the actors associated with the judiciary and civil societies consider identity revelation a risk for the officially confirmed COVID-19 cases, which is in contrast to the beliefs of a business organisation and the Food and Drug Administration, which favour symbolic markers in the form stickers or notices on COVID-positive patients’ homes to protect the safety of the unaffected population. The third most conflicting opinion entailed international lobbying against China by blaming it for the global spread of the virus (Roberto et al., 2020: 369, 371). Our findings (Figure 1C) illustrate a conflict between the politicians from Bharatiya Janata Party (BJP), the ruling party of India, and the representatives of India’s Chinese Embassy regarding China’s role in facilitating the spread. Lastly, our fourth observation witnessed mixed opinions on the efficacy of the Indian government in containing the virus-related stigma. While the state governments and their bodies were positive about their performance, the association of Indian doctors and health experts, as well as research entities like The Lancet, disagreed with the notion. Members of the Indian Medical Association, a voluntary organisation of doctors in India, both agreed and disagreed with the concept.
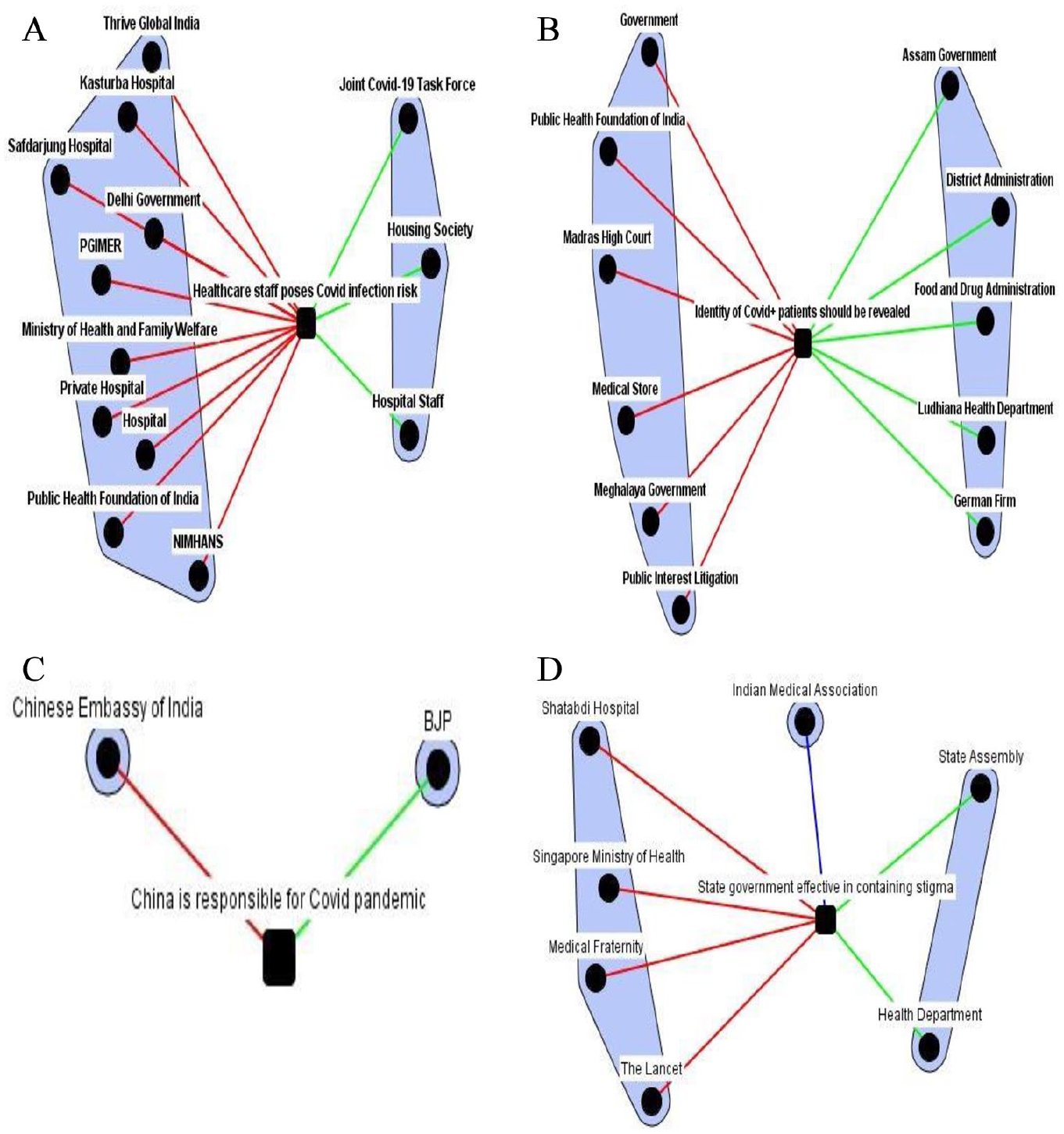
Two-mode network of organisations and beliefs regarding the four most contested beliefs.
Overall, the network-based representation of our data illustrated the presence of contrasting beliefs among the various stakeholders in India, which, when communicated from positions of power, often perpetuate discrimination at the micro-level of society. For example, our study revealed the prominence of the Indian government’s statements in the media (Table 2), which, when visualised using the most conflicting stigma discourses, show disjunctions between the national and regional governments (Figure 1). This demonstrates that stigma is not a single rigid category but rather a ‘constantly changing social process’ based on cultural and power hierarchies (Parker and Aggleton, 2003: 14).
The hierarchies of COVID-19
Reassertion of traditional stigmas
We found that the disaster emerging from the COVID-19 pandemic is amplified in the social domain via elements of traditional stigmas in India. We scrutinised our media data to identify incidents of stigma, which we then classified according to themes reflecting the prevalent causes of stigma in India. With this approach, we intended to obtain data-based categories rather than the established categories of social discrimination in India in order to avoid a biased selection. The resulting categories which we identified are: (1) medical history, (2) identity and (3) myths and superstitions.
The first category, ‘medical history’, includes cases that – due to comorbidity and a lack of scientific knowledge – enabled stigmatising interpretations and suspicious attitudes towards patients with comorbid conditions. Patients suffering from long-term illnesses, such as acquired immunodeficiency syndrome (AIDS), were largely affected (Itoo, Kashmir Times, 2020). We found the second category, ‘identity’ – which includes ascriptions and acquired affiliations gained during our lifetime – to be an important substrate of stigma generation during the COVID-19 crisis. Some of the identity-based forms of stigma were transphobia, ethnicity, religious minorities and class. The intersection of the COVID-19 crisis and ethnic roots became evident with the reporting of the first cases of COVID-19 in China. This was followed by US President Donald Trump labelling the virus ‘the Chinese virus’, forming ripples in the Indian mainland as well. First, the diaspora from India’s northeastern states faced heckling in the capital city and were reportedly asked ‘to move to China’ (The Times of India, 2020b). In a second case, Liu Bing, Counsellor of the Chinese Embassy in India, raised his voice against a member of the Legislative Assembly of India for using racially stigmatising language against the people of China (The Hans India, 2020). Such discourses often led to statements by international organisations such as the WHO to combat stigma against countries and people.
Aligning with the theme of identity, after reported outbreaks of the virus, one in five COVID-19 cases in India were linked to Tablighi Jamaat 8 (Radhakrishnan, The Hindu, 2020). The repercussions of this event extended to the Muslim pastoral Gujjar community of Uttarakhand and Punjab, whose members were accused of attending the Tablighi Jamaat conference and transmitting the virus. One such perceived-positive case from Punjab shared that villagers and a village authority accused their community of spitting in the milk they sell (The New Indian Express, 2020a). This ostracisation resulted from a risk event which, when amplified through a religious sect and circulated to a larger audience through the media, generated stigma about the religious community in general.
We also found a special role of class in determining stigma in relation to the virus. COVID-19 disrupted business across India and caused stigmatisation of people involved in unskilled jobs. A labourer having to return home expressed his agony in the following statement, I walked for 90 kilometres, but what about those who have to walk for 500 kilometres? I walked for a day, but some are taking four-five days to reach home. How will they get food and water with everything closed along the way? People will anyway die of hunger, forget coronavirus. (Ghosh, Scroll.in, 2020)
Similarly, myths and superstition also played an important role in governing risk behaviour and perceptions during the pandemic in India. In one report from Bihar, a coronavirus survivor asserted: There’s a rumour in the village that our family got into trouble because of black magic and some unseen forces. . . . I do not go out to buy grocery or vegetables to avoid the questioning gaze of people. Even the store owner does not want me to come there. (Sopam, Hindustan Times, 2020)
With the observed assertion of traditional modes of discrimination including medical history, identity and myths and superstition, a reaffirmation of beliefs propagating stigma occurred. A further analysis of the data revealed that the emergence of COVID-19 led to new categories of discrimination based on temporary associations with infection, i.e. ‘threshold people’, undergoing transition through the zones of ‘liminality’ (Turner, 1969: 95). We discuss such categories as ‘new hierarchies’ in this article.
New hierarchies
Along with reinforcing traditional stigma, three new forms of hierarchies could be identified from the data: (1) marking and symbolism; (2) lack of reverence for the dead; and (3) severance of social ties. There were three types of markings and symbolism in the data. The first comprises physical marking, whereby quarantine stickers and posters were placed on individual households, public places, or government records to mark a potential COVID-19 positive case. The action of pasting stickers was undertaken in several states, including Gujarat, Karnataka and Assam, where state municipal bodies, health departments and district administration took the lead within the ambit of the Epidemic Diseases Act of India 1897, to curb further infections. However, these actions created an atmosphere of fear and suspicion against marked people among other local residents. One perceived-positive man explained his experience of such markings as follows: The vegetable sellers have refused to give us vegetables and the milkman also does not deliver the milk to our home. . . . Weirdly so, youths gather outside our home and click selfies with the quarantine poster. When we go out in the balcony or terrace people give us looks. . . . It is upsetting. (The Times of India, 2020c)
The second type of marking was based on profession. One profession facing public prejudice was healthcare staff who, in many incidents, reported discrimination from neighbours and property owners due to their proximity with COVID-19 patients in health facilities. Incidents of neighbours tagging such workers as ‘untouchables’ were noticed. The third type of marking was by means of personal or territorial identity. In one report, an entire street was labelled as ‘coronavirus wali gali’ (coronavirus street) by the residents of nearby locations due of one confirmed COVID-19 case. In another instance, a minister from Haryana labelled people working in Delhi, a COVID-19 hotspot, as ‘corona carriers’, while in Punjab a ‘super spreader’ tag was used for a confirmed COVID-19 patient. In a further case, revelation of customers’ identities by a pharmacy in Punjab led to stigma due to fear of association with the disease. Undoubtedly, as a token of appreciation, the Government of India thanked healthcare workers by calling them ‘corona warriors’ and gave them a floral salute to boost morale, but this extra attention to a category may also lead to discrimination against them in practice.
Similarly, due to suspicion of the presence of virus in mortal remains, a number of media reports highlighted objections raised by locals against the cremation of the dead. In some cases, local administrations and health officials had to intervene, and sometimes get involved in facilitating the last rites of the deceased, leading to public outrage and hostility towards them. In another case, due to a suspicion of infection, a pregnant woman’s dead body was denied entry by the local community into a village in Odisha.
Another form of hierarchy caused the severance of social ties at the level of family and neighbourhood. In some incidents, healthcare staff faced discrimination by family members (The New Indian Express, 2020b), and in the other cases, workers faced both losing their job and discrimination due to the loss of employment during lockdown restrictions. One labourer on returning to his village said, The villagers are scared of me. They think that I have brought the virus along with me. I am telling them that I have been tested three times, but they won’t listen. . . . I have fields but how much can I earn from farming? The wheat will be harvested, fine, but to grind it, I need money. (Ghosh, Scroll.in, 2020)
Newspapers portray many such intersections of problems in the narratives of both perceived-positives and negatives. The formation of new hierarchies is a social symptom of the disease that builds on existing fear and suspicion due to the pandemic’s uncertainty.
Conclusion
Using the case of COVID-19 in India, this study has demonstrated risk perception and stigma generation as well as their effects on the population through media discourses, underpinning different actors’ beliefs within society. Research has proven that social inequities increase health disparities (Nydegger and Hill, 2020: 656; Zinn, 2020: 1087, 1088). In India, with the country’s rigidly stratified social structure and one of the lowest health expenditures, the experience of the pandemic became ‘violent, stigmatising and fatal’ due to the government’s unplanned and experimental response (Rahman, 2020: 131–139). Moreover, Douglas’s (1992: 84) assignment of a ‘real danger’ to infectious diseases and Goffman’s (1963) ascription of stigma to the ‘discredited’ offer complementary perspectives, which sociological research on stigma and risk have hardly utilised. This article has attempted to fill this gap using the relevant literature of both theorists to socially situate and visualise the risk of the coronavirus through incidents of stigma reported in online media reports during the first two consecutive lockdowns in India. The methodological novelty of our research lies in our systematic discourse analysis of 332 statements extracted from the data to identify diverse actors (129 persons and 99 organisations) and the role of their beliefs in stigma generation and proliferation.
Different studies have outlined the roles of social media (Pulido et al., 2020), government (Zinn, 2020), capitalist expansion (Matthewman and Huppatz, 2020), socio-demographic differences (Nydegger and Hill, 2020; Roberto et al., 2020) and socio-spatial interactions (James, 2020) to demonstrate different social implications of the virus. Our results have highlighted five crucial points: (1) the most popular beliefs reported in the media comprise ‘perceived risk-related beliefs’, ‘beliefs related to fear of disclosure’ and ‘beliefs related to care and support’; (2) the most contested beliefs in the media discourse are: ‘healthcare staff pose COVID-19 infection risk’, ‘identity of COVID positive patients should be revealed’, ‘China is responsible for COVID pandemic’ and ‘state government is effective in containing stigma’; (3) the major actors in the risk discourse are from the government sector, hospitals and civil society; (4) the representation of intergovernmental organisations in the media risk discourses is negligible as compared to national organisations and groups; (5) stigma perpetuates traditional as well as creates new hierarchies in relation to the risk of infection. Our study revealed that the psychosocial mechanisms of threat identification and threat elimination use socio-cultural tools to identify ‘some disapproved behaviour’ and code it ‘to give automatic, self-validating legitimacy to established law and order’ (Douglas, 1992: 29, 84). Interestingly, these mechanisms have contributed to the formation of a new hierarchy of confirmed and suspect patients and their associates, whereby perceived-positives’ primary networks at the family, neighbourhood and community levels sever social ties.
We expect this study to benefit various stakeholders by promoting cultural competence (Roberto et al., 2020: 371), and symbolic and substantive inclusivity in risk-governance (Brown, 2020: 11), trust-building (Dryhurst et al., 2020: 998), and a refocus towards managing the socio-structural risks as a strategy to combat immediate risks (Zinn, 2020: 1088). Moreover, this case study provides rich comparative literature for future research on stigma surrounding infectious diseases (de Zwart et al., 2009: 31), including secondary risk of infections (Zinn, 2020: 1083), scientific versus social methods of knowledge production and media studies. A longitudinal or in-depth evaluation of infectious diseases can be used to further explore the lifespan of the new hierarchies we have observed in order to generate better long-term policies.
Footnotes
Appendix
List of news sources
| S. No. | Media source | Number of articles |
|---|---|---|
| 1 | The Times of India | 38 |
| 2 | Hindustan Times | 22 |
| 3 | The Hindu (Online and Business) | 10 |
| 4 | The Indian Express (Online) and The New Indian Express | 7 |
| 5 | Indo-Asian News Service | 4 |
| 6 | Livemint | 4 |
| 7 | The Economic Times | 4 |
| 8 | Asia News International | 3 |
| 9 | Press Trust of India | 3 |
| 10 | Scroll.in | 3 |
| 11 | The Assam Tribune | 3 |
| 12 | Deccan Herald | 2 |
| 13 | Free Press Journal | 2 |
| 14 | Imphal Free Press | 2 |
| 15 | India Today | 3 |
| 16 | IndiaSpend.com | 2 |
| 17 | Kashmir Observer | 2 |
| 18 | Mumbai Mirror | 2 |
| 19 | Orissadiary.com | 2 |
| 20 | The Pioneer | 2 |
| 21 | The United News of India | 2 |
| 22 | Bangalore Mirror | 1 |
| 23 | Bar and Bench | 1 |
| 24 | Business Standard | 1 |
| 25 | BusinessLine Online | 1 |
| 26 | Down to Earth | 1 |
| 27 | Express Healthcare | 1 |
| 28 | Indian Government News | 1 |
| 29 | Kashmir Times | 1 |
| 30 | Mid-day | 1 |
| 31 | Mirror Now | 1 |
| 32 | Odishatv.in | 1 |
| 33 | tellychakkar.com | 1 |
| 34 | The Hans India | 1 |
| 35 | The Sentinel | 1 |
| 36 | Straits Times | 1 |
| 37 | The Sunday Standard | 1 |
| 38 | The Telegraph | 1 |
|
|
|
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.